Embed Size (px)
Citation preview

Insights into to the 2003 Federal Health Savings
Account Law from Minnesota’s Consumer Driven Health Plans
(CDHPs)Stephen T. Parente, Ph.D.
Assistant ProfessorCarlson School of Management
University of Minnesota
Testimony before the Minnesota State SenateFebruary 3, 2004
For more information: [email protected]

Presentation OverviewWhat are Health Savings Accounts?How are they related to the Consumer
Driven Health Plans (CDHPs) in use by the University of Minnesota and Medtronic employees?
What are the findings from Minnesota employees?
Who is choosing them? What is the cost and use impact?
What is the downside to this law?What is the possible upside to the law?

Health Savings AccountsIntroduced in the 2003 Medicare Reform
LawWhat it enables:
• U.S. citizen can create a ‘qualified’ HSA account.
• Qualification is• Must have ‘catastrophic health insurance’ with
minimum deductible of $2,000. Max is $10,000 for a family contract.
• Individuals or employers can make annual pre-tax contribution to an HSA, separate from the insurance policy, of 100% of the deductible (max of $5,150).

Why Would Anyone Want such a Wacky Thing?
Compare & ContrastOld Way for Family to Buy Coverage:Buy family policy from BCBSPolicy cost: $8,460Plan has $500 deductible Deductible applied per personDeductible capped at $1,000Cost if healthy: $8,460Cost if 1 person sick: $8,960Cost if 2+ people sick: $9,460
The New HSA Way: Buy BCBS ‘qualified’ plan
from BCBS. Qualified plans costs: $3,936 Plan has $2,500 deductible Deductible applied per
person Deductible capped at $5,000 Cost of healthy: $3,936 Cost if 1 person sick: $6,436 Cost if 2+ people sick:
$8,936

How Wound This Work and Who Would Buy It?
Medical Savings Accounts (MSAs) as AncestorsHSAs are really another form of Medical Savings Accounts.Since ’96 Medical Savings Accounts have been tax-advantaged.Very little enrollment because of restrictions to only small firms.
Consumer Driven Health Plans as Self-insured Employer Analog:Since 2000, CDHPs have taken off.Major insurers offer version of CDHPs.Structured similar/identical to HSAs.

Issues Driving CDHP CreationPatients
Dissatisfaction with provider access Patient incentives are to consume Limited choices of benefits and providers Combative relationship with managed care companies
Providers Loss of autonomy Erosion of physician/patient relationship Misalignment of physician reimbursement and incentives
Employers Plan costs are increasing Employees are not happy Increase of employer administration burdens

Early CDHPs in Operation
– Definity•Concept developed in 1998, Funded in April, 2000•Minnesota based•Clear first mover & dot-bomb survivor•300,000+ subscribers in 2004, from 0 in 2000.
– Lumenos•Started in 2000•Based in Virgina•Havard B-School inspired (Regina Herzlinger)
– Destinty•Operating as Medical Savings Account model•In operation for 10 years in South Africa

Definity Health as CDHP Model
Definity Definity HealthHealthCareCare
AdvantageAdvantage
Web- and Web- and Phone-Phone-Based Based ToolsTools
Health ToolsHealth Toolsand Resourcesand Resources
Health Tools and Resources• Care management
program• Extensive easy-to-use
information and services
Health Coverage• Preventive care covered
100%• Annual deductible• Expenses beyond the
PCA• Nationwide provider
access• No referrals required
Personal Care Account (PCA)• Employer allocates PCA1
• Member directs PCA• Section 213(d) “scope”• Roll over at year-end • Apply toward deductible2
Annual Annual DeductibleDeductible
Annual Annual DeductibleDeductible
Pre
ven
tive
Care
10
0%
Pre
ven
tive
Care
10
0%
Health Health CoverageCoverage
An
nu
al
Ded
uct
ible
1 Employer selects which expense apply toward the Health Coverage annual deductible.2 Paid out of employer’s general assets.
PCAPCAPCAPCA
$$

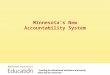
HSA Mechanics
Health Coverage• Purchased by ‘Qualified’
Plans• Annual deductible• Expenses beyond the
HSA• No managed care
provisions• Nationwide provider
access• No referrals required
Health Care Account (HSA)• Consumer/Employer allocates
HSA• Consumer directs HSA• Owned by consumer and
portable• Roll over at year-end• Many deposited pre-tax• Consumer can withdrawal
with penalty• Can apply toward deductible
Annual Annual DeductibleDeductible
Annual Annual DeductibleDeductible
Health Health CoverageCoverage
An
nu
al
Ded
uct
ible
HSAHSAHSAHSA
$$

New RWJ-Funded Research
Key Research Questions1. Is there an ‘adverse selection’ problem?
Traditionally, adverse selection is defined as the situation when healthy individuals choose Definity leaving the sick in a traditional plan that will soon implode its premiums because of disproportionate share of sick individuals in the insurance pool.
2. What is the impact on cost and utilization? Definity has been chosen as a response to rising premium prices in an attempt to make the consumer ‘drive the market’ be examining price variations and constraining their personal consumption, if possible.

Research Design– 2 Year study (11/1/2002 - 10/31/2004)– Six employers examined:
• University of Minnesota, MN• Medtronic, National• Ridgeview Medical Center, MN• Hannaford Bros, New England• Welch-Allyn, Upstate NY (tentative)• Raytheon (New England or South Atlantic firm)
– Data collected• Claims data of all utilization for all health plan choices, pre (2001)
and post (2002-2003) Definity.• Employer info on flexible spending accounts and employee income
• Survey information on Definity choices in 2002 & 2003 from U of M.

Early Results #1:
Who is Choosing a CDHP and is there Adverse
Selection?

U of MN Health Plan Choices
1. Health Partners: Staff model HMO with direct capitation contracting at a limited number of group practices.
2. Patient Choice: A ‘Tiered-direct contracting’ descendent of Minnesota’s Buyers Health Care Action Group health benefit design experiment.
3. Definity Health: Consumer-driven Health Plan 4. Preferred One: Preferred Provider
Organization

UPlan Options/Enrollment
Total CostLess UM
contributionEmployee
contribution EnrollmentHealthPartners Classic $137.84 $137.84 $0.00 5,027Patient Choice Cost Group I $137.84 $137.84 $0.80 Patient Choice Cost Group II $147.15 $137.84 $9.31 2,091Patient Choice Cost Group III $157.90 $137.84 $20.06PreferredOne National $189.51 $137.84 $51.77 731
Definity Health Option 1 $150.52 $137.84 $12.68 349Definity Health Option 2 $150.48 $137.84 $12.64
Total 8,198
Employee-only coverage
Total CostLess UM
contributionEmployee
contribution EnrollmentHealthPartners Classic $344.59 $323.92 $20.67 3,967Patient Choice Cost Group I $329.60 $323.92 $20.67Patient Choice Cost Group II $351.30 $323.92 $39.23 2,808Patient Choice Cost Group III $376.80 $323.92 $65.73PreferredOne National $448.40 $323.92 $143.91 997
Definity Health Option 1 $353.00 $323.92 $51.63 346Definity Health Option 2 $327.50 $323.92 $51.55
Total 8,118Single & Family Total 16,316
Family coverage

Early UM Definity ExperienceYear 2002
54%46%Option 1Option 2 51%49% Family
Single
49% 51% FemaleMale
51%49%Employee
Dependents

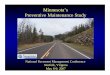
Definity Age/Gender Distribution
2002 University of Minnesota
0
10
20
30
40
50
60
70
<25 25-34 35-44 55-64 >65
Definity Male
Definity Total
Other Plans

All RespondentsSatisfaction with Plan
OverallYes No
How would you rate your overall experience with your health plan in 2002? (1=worst possible, 10=best possible)
Definity 7.47 7.41 7.50Other Plans 7.55 7.64 7.49
For Definity respondents, would you recommend Definity to a friend, family member or colleague? (%)
Yes 85.0 87.4 83.6No 12.4 9.3 14.1
Don't know/refused 2.6 3.3 2.2
By Whether Respondent or Dependent Has Chronic Condition

Health Plan Features Most Preferred
50
36.7
29.8
6.9312
1516
46.4
76.44
0 20 40 60 80 100
My doctors in health plan
No referral authorizations
Has preventive care
National provider panel
PCA balance rolls over
Small out-of-pocket $$
Small paycheck deduction
No copayments
Online tools
Percent agreement
Other Health Plans Definity

Results: Health Status and Other Employee Characteristics
• No evidence of CDHP adverse selection (after multivariate plan choice analysis).
• If anything, there is adverse selection to the PPO.
• Higher income employees chose Definity or Choice Plus, suggesting these plans may evolve as favorites of the ‘well-to-do’
• Older employees chose PreferredOne or Choice Plus

Early Results #2:
What are the Effects of CDHPs on Utilization and
Cost?

Study Setting
• Health plan choices by employees:– HMO, 2000-2002– PPO, 2000-2002– CDHP, 2001-2002
• Variation in cost sharing by contract• Take-up of CDHP approximately 15%. • General caveat: Each of the six employers’
experience can be quite different due to:– Alternatives offered– Plan design– Communications with employees– Sponsor’s objectives for the plan

What was the ADJUSTED impact on provider and patient
payment?
NOTE: These are results from a restricted continuously enrolled sample of 50% to 60% of the total employee population and are not a reflection of the plans’ full PMPM expenditures. Also note: 1) Patient expenditures from the Personal Care Account (PCA) are included in the employer payment category. 2) Consumer payment reflects deductibles, copayments, and coinsurance expenses.
Health Plan Cohorts Mean Mean Mean
CDHP Cohort N=531Total Expenditure 5,555.57$ 6,456.57$ 7,988.80$ Employer Expenditure 5,119.68$ 6,242.51$ 7,707.16$ Employee Expenditure 488.89$ 613.91$ 702.30$
HMO Cohort N=1,551Total Expenditure 6,574.79$ 7,552.76$ 8,170.57$ Employer Expenditure 6,162.39$ 7,012.36$ 7,373.04$ Employee Expenditure 458.35$ 580.92$ 755.15$
PPO Cohort N=1,554Total Expenditure 6,324.16$ 7,542.66$ 8,472.59$ Employer Expenditure 5,727.73$ 6,847.41$ 7,466.26$ Employee Expenditure 582.79$ 674.94$ 864.38$
2000 2001 2002

What was the ADJUSTED impact on provider & patient payment by different
services?
NOTE: These are results from a restricted continuously enrolled sample of 50% to 60% of the total employee population and are not a reflection of the plans’ full PMPM expenditures.
Health Plan Cohorts MeanDeviationMean MeanDeviation
CDHP Cohort N=531Hospital Expenditure 1,721.23$ 1,982.79$ 3,224.46$ Physician Expenditure 2,590.43$ 3,058.93$ 3,411.27$ Pharmacy Expenditure 1,086.11$ 1,072.45$ 1,229.97$
HMO Cohort N=1,551Hospital Expenditure 2,284.27$ 1,957.99$ 2,077.66$ Physician Expenditure 2,899.45$ 3,263.15$ 3,452.05$ Pharmacy Expenditure 1,266.97$ 1,533.62$ 1,717.15$
PPO Cohort N=1,554Hospital Expenditure 2,100.61$ 2,045.69$ 2,238.25$ Physician Expenditure 2,658.17$ 2,997.35$ 3,305.93$ Pharmacy Expenditure 1,135.19$ 1,481.71$ 1,690.24$
Year 2000 Year 2001 Year 2002

Was ADJUSTED service use different for CDHPs?
NOTE: These are results from a restricted continuously enrolled sample of 50% to 60% of the total employee population and are not a reflection of the plans’ full admissions and prescription drug experience.
Health Plan Cohorts Mean Mean Mean
CDHP Cohort N=531Physician Visits 6.54 4.87 4.63Hospital Admission Rate 0.07 0.13 0.14Prescriptions Filled 21.23 21.21 22.80
HMO Cohort N=1,551Physician Visits 7.49 7.60 7.46Hospital Admission Rate 0.08 0.07 0.09Prescriptions Filled 21.06 22.67 31.54
PPO Cohort N=1,554Physician Visits 6.31 6.36 6.48Hospital Admission Rate 0.08 0.07 0.07Prescriptions Filled 22.43 22.43 22.96
2000 2001 2002

What Share of CDHP Enrollees Had Money Left
in Their Accounts?PCA MAP 2001 2002Under PCA Limit 40% 28%Ended Within Gap 13% 15%Above Deductible 47% 57%
Continuously enrolled population

Conclusions (To Date)• CDHPs adopter are not that different from other
employees. • Income is a driver in adoption, though not exclusively.• CDHP is lower cost, but the trajectory is not great.• Critical caveat: Benefit design will drive expenditure
results.
‘Draconian’ benefit design for family contract:• $1,0000 PCA, $4,000 Deductible, 20% co-insurance after
deductible
Current industry standard design for family contract:• $2,000 PCA, $4,000 Deductible, 10% to 15% co-insurance after
deductible
Generous benefit design for family contract:• $2,000 PCA, $3,000 Deductible, 0% co-insurance after deductible

Policy Opportunities What is the Upside to the
Law?• Innovative means to bring consumer choice into the medical marketplace as well as consumer awareness of the trade-offs of liberal medical insurance coverage policies.
• Creates foundations for infrastructure for personal, portable health care coverage.
• Hybrid variants could be crafted to serve low income, part time workers and possibly the uninsured through tax credits and vouchers.

Policy ConundrumsWhat is the Downside to the
Law?• What if HSAs/CDHPs accelerate the
consumer’s burden of health care spending ‘too’ quickly?
• Not much incentives for managed care’s proven assets (e.g., disease management) to play a role. get involved.

Federal versus State Issues that Need to be Considered
Does the HSA law supercede state health insurance commissioners?• Partially – They legitimize the national market for such insurance
similar to Medicare Medigap policies. Can a qualified plan be offered to a Minnesota from an out-of-
state insurer?• No – State/federal larger question – Why not other than history?
Can an ERISA-exempt self-insurer employer role employees into their own account?• Very loaded issue as it not clear how employers account for unused
employee PCA dollars. For these plans, what is there for a state health insurance
commission/commissioner to do?• Unknown – Seems like only approve the premium and not weigh in on
design. How are unfunded mandates treated?
• Should be the same as an individual policy and determined by the State.