Embed Size (px)
Citation preview

SCLEROSING PAPILLARY PROLIFERATIONS IN T H E FEMALE BREAST
A Benign Lesion Often Mistaken for Carcinoma
CECILIA FENOGLIO, MD,” AND RAFFAELE LATTES, MD+
The occurrence of foci of fibrosis in benign intraductal papillary proliferations in the female mammary gland can lead t o extreme distortion with a pseudo- invasive pat tern tha t is still of ten mistaken for carcinoma. The histologic diagnostic criteria which differentiate between this benign lesion and t rue carcinoma are described in detail in this report . In a series of 30 cases with adequa te followup, the benign na tu re of this lesion was confirmed.
ENIGN INTRADUCTAL PAPILLARY PROLIFERA- B tions in the mammary gland may un- dergo sclerosis and distortion, leading to a pseudoinvasive pattern. This can be, and often is, mistaken for carcinoma. Most of the experienced surgical pathologists have learned how to avoid this diagnostic pitfall. Yet these lesions remain a diagnostic dilemma to those who are unfamiliar with the phenomenon.
From the Division of Surgical Pathology, Depart- ment of Pathology, Columbia IJniversity, College of Physicians and Surgeons, 630 W. 168th Street, New York, N.Y. 10032.
* Trainee in Surgical Pathology (NIH #STOlCA-
t Professor of Surgical Pathology. T h e authors wish to thank the following colleagues
who provided the followup information on the pa- tients included in this study: Giles Allard, St. Joseph Hospital, Stamford, Conn.; Stuart Anderson, Hacken- sack Hospital, Hackensack, N.J.; John Duffy, Nassau County Medical Center, East Meadow, N.Y.; Charles Findlay, Columbia Presbyterian Medical Center, N.Y.; William Green, Valley Hospital, Ridgewood, N.J.; C. D. Haagensen, Columbia Presbyterian Medical Center, N.Y.; E. J. Hayes, Good Samaritan Hospital and Medical Center, Portland, Oregon; Sven Kister, Columbia Presbyterian Medical Center, N.Y.; Eric Liban, Kaplan Hospital, Rehovot, Israel; H. L. Mame- lock, T h e Elizabeth A. Horton Memorial Hospital, Middletown, N.Y.; Alfred Markowitz, Columbia Pres- byterian Medical Center, N.Y.; David Nelligan, Lawrence and Memorial Hospitals, New London, Conn.; Vincent Palladino, Nassau County Medical Center, East Meadow, N.Y.; Arthur Patchefsky, Thomas Jefferson University Hospital, Philadelphia, Pa.; E. C. H. Schmidt, T h e Memorial Hospital at Easton, Pa.; H. Schriver, John F. Kennedy Community Hospital, Edison, N.J.; Stumpf, Overlook Hospital, Summit, N.J.; Paul Tamura, Castle Memorial Hos- pital, Kailua, Hawaii; Victor Tchertkoff, Metropolitan Hospital Center, N.Y.; Robert Totten, Presbyterian University Hospital, Pittsburgh, Pa.; Philip Wiedel, Columbia Presbyterian Medical Center, N.Y.; and Edward Zaino, Mercy Hospital, Rockville Centre, N.Y. Most of the photographic work was done with the help of Dr. Gordon Kaye.
051 07- 11).
Received for publication July 3, 1973.
This is reflected in the frequency with which practicing pathologists seek a consultant’s advice because of their uncertainty as to the nature of this lesion. Unfortunately, radical or modified mastectomies are still occasionally performed because a distorted sclerosed be- nign papillary proliferation was misinter- preted as a carcinoma, especially on frozen section.
This problem has previously been briefly referred to in the literature.1,2~~-~ However, no detailed description of the histology or the clinical followups has been published. The files of the Division of Surgical Pathology of Columbia-Presbyterian Medical Center con- tain numerous examples of this condition. We therefore undertook the following study to describe in detail the histology of this le- sion and to document i ts benign course through careful postoperative clinical fol- lowup.
MATERIALS AND METHODS
One hundred forty-two papillary breast le- sions were reviewed which were variously listed in our diagnostic files as “intraductal papilloma with fibrosis,” “papilloma with pseudocancer,” “papillomatosis with scle- rosis,” “sclerosing papilloma,” “papilloma- tosis with distortion secondary to fibrosis,” “papillomatosis with pseudoinvasive features,” “papilloma distorted by scarring,” “papilloma with atypical features,” and “papillomatosis with pseudomalignant features.” These r e p resented local hospital cases as well as those cases received for consultation from other in- stitutions.
From these 142 cases, 54 were chosen which
69 1

692 CANCER March 1974 Vol. 33
we felt met our diagnostic criteria for scleros- ing papillomas or papillomatosis of the breast. As outlined below, 15 of these were local hospital cases, and the remaining 39 were received in consultation. The hospital charts of the local cases were reviewed; if the pa- tient was a private patient, the private physi- cian was contacted for additional followup in- formation not available in the hospital chart. Of the local cases, 4 were lost to followup.
In the remaining 39 cases, letters request- ing the followup were sent to the physicians who had submitted them for consultation. We obtained information in 19 patients. Thus, we have adequate followup information on 30 patients, of which 11 are local cases and 19 are consultation cases. I t is these 30 pa- tients which are the basis of this study.
RESULTS
Histologic features: On low power examina- tion, the sclerosing papillary lesions fre- quently have a characteristic stellate form of central fibrosis which merges in a radial way with the peripheral non-sclerosed portion of
the papillomatous growth (Figs. 1-3). This central sclerotic portion is composed of dense, often hyalinized and poorly cellular fibrous tissue in which small trapped epithelial structures can be found. T h e latter often take the form of small groups of cells which are generally arranged in a glandular fashion. In other cases, or in other areas of the same case, the epithelial structures trapped in the dense fibrous tissue have a more obvious papillary pattern. On higher power examina- tion one can generally see that both the small tubular structures and the partly papillary ones are lined by a double row of regularly arranged normochromic cells, a feature sel- dom seen in true carcinomas (Fig. 4).
Occasionally, deposits of heniosiderin and liemosiderin-laden macrophages are seen in the central area, surrounded by mononuclear inflammatory cells. These foci are associated with the sclerotic process. In these instances the stroma is usually more cellular and some- times even resembles granulation tissue.
As already mentioned, at its periphery, the sclerotic process tends to merge with the complex glandular pattern normally associ-
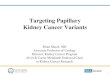
FIG. 1 . Sclerosing papillary lesion. Low power view of the fibrosing process, with entrapment of distorted ductules. At the periphery, remnants of benign papillomatosis can be seen. Note absence of extension into the intralobular fat (H & E. ~ 4 3 ) .

No. 3 SCLEROSING PAPILLARY PROLIFERATIONS - Fenoglio and Lattes
FIG. 2. Sclerosing papillary lesion of another patient. Here, the benign duct papillomatosis is more obvious, associated with the pseudo-invasive pattern of the ducts distorted by fibrosis. Also here, the process does not extend into the interlobular fat (H & E, ~ 4 3 ) .
693
FIG. 3. Same case as Fig 1. ScIerosing papillary lesion. The findings are similar to those in Figs. 1 and 2, but the stellate cicatricial pattern is more striking (H & E, X43).

694 CANCER March 1974 VOl. 33
FIG. 4. Same case as in Figs. 1 and 3. Sclerosing papillary lesion. A higher power view of a pseudo-invasive area, showing that most ductules exhibit a double row of epithelial cells with lack of anaplasia, and that the fibrous tissue is definitely cicatricial in type (H & E, ~ 1 7 0 ) .
FIG. 5 . Sclerosing papillary lesion. Here the benign duct papillomatosis is only slightly distorted by the fibrosing process (H & E, ~ 1 0 0 ) .

No. 3 SCLEROSING PAPILLARY PROLIFERATIONS - Fenoglio and Lat tes
FIG. 6. Sclerosing papillary lesion. A higher power view of same case as in Fig. 5, showing the clearly benign nature of the epithelial proliferation (H & E, ~ 1 5 0 ) .
FIG. 7. A solitary intraductal papilloma with marked fibrosis which in the right side of the field leads to a pseudo-invasive pattern of the entrapped epithelial structures (H & E, ~ 4 3 ) .
695

696 CANCER March 1974 VOl. 33
FIG. 8. A higher power view of the area referred to in Fig. 7 (H & E, ~ 1 0 0 ) .
ated with benign mammary papillary lesions. This is one of the important clues in the differential diagnosis with invasive ductal or tubular carcinoma. In these peripheral areas where they are more easily recognized as such, the papillomas or duct papillomatosis show fronds lined by a double row of normochro- mic cells which may be supported by connec- tive tissue stroma (Figs. 1-3). No small nests or cords of cells or small tubular structures are ever seen extending into areas away from the sclerotic process, especially into the inter- lobular fat, as one would expect in a truly malignant and invasive tumor. In addition, the papillary growths do not have the well- known features of papillary carcinoma (Figs.
The surrounding breast tissue usually shows adenosis, other foci of papillomatosis, epithelial hyperplasia, apocrine metaplasia, and cysts. It is not unusual to find foci of sclerosing adenosis in proximity to the scle- rosed papillomas.
The clinical correlations are summarized in Table 1. The most common presenting symptom was a palpable mass in the breast. The nature of the mass was either cystic disease, or adenosis, or a combination of both.
1-3, 9-11).
The patients’ ages ranged from 15 to 67 years. As would be statistically expected, foci of true carcinoma can coexist occasionally else- where in the same breast which contains the pseudocarcinomatous sclerosing papillary le- sions. In fact, areas of typical lobular neo- plasia in situ (lobular carcinoma in sit^)^ were found in Case 28, and in Case 27 there was a separate small focus of non-invasive intraductal carcinoma as well as areas of lobular neoplasia in situ. In addition, in Case 20, a focus of lobular neoplasia in situ was found at the time of a second operation done in order to remove recurrent benign sclerosed papillomatosis.
In five cases, major surgery was done be- cause of an original diagnosis of carcinoma. Three of these, when seen in consultation (Cases 10, 12, 19) were subsequently recog- nized as sclerosing papillary lesions. The other two, as already mentioned in the pre- ceding paragraph, contained also separate small foci of non-invasive intraductal carci- noma and lobular neoplasia in situ in one (Case 27) and lobular neoplasia in situ in another (Case 28).
In four cases, the sclerosing papillomatosis was part of a pattern of recurrent and/or

No. 3 SCLEROSING PAPILLARY PROLIFERATIONS - Fenoglio and L a t tes
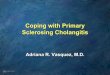
FIG. 9. A true carcinoma, tubular type, with invasion of the intralobular fat (H & E, xl00).
FIG. 10. Another area of same case as in Fig. 9, with invasion of the intralobular fat (H & E, ~ 1 0 0 ) .
697

698 CANCER March 1974 VOI. 33
FIG. 11 . A classical papillary adenocarcinoma, with well differentiated intraductal, and less well differentiated invasive components (XIOO).
multiple papillomatosis. All of these patients are alive and well without further breast problems except for one who died of heart disease.
One patient was pregnant at the time of surgery and another has had two successful uneventful pregnancies since the lesion was removed. No information regarding intake of estrogenic compounds was available in any of these cases.
DISCUSSION
We believe that it is important to bring to the pathologist’s attention the potential diagnostic pitfall represented by these scle- rosed benign papillary proliferations with a pseudo-invasive pattern. Clinically, although there is no characteristic feature, these are generally middle-aged females, whose main complaint is a small poorly outlined mass which is sometimes associated with nipple discharge. Occasionally, the fibrosing process can cause their fixation to the skin (Case 18), thus justifying an increased suspicion as to their possible malignant nature. On frozen
section, as in all papillary lesions of the breast in general, a differential diagnosis be- tween benign sclerosed papillary prolifera- tions and carcinoma may be difficult. For this reason, in all papillary lesions of the breast it is our rule to defer the diagnosis until multiple permanent paraffin sections are available.?
Pathologically, the characteristic features which help in differentiating this benign le- sion from invasive ductal, tubular, or papil- lary carcinoma with invasion are:
1. A low power architecture frequently suggesting a contracted scar which has oc- curred in an area of intraductal papillary proliferation (Figs. 1-3).
2. The papillary proliferations associated with the lesion are obviously morphologically benign, featuring either the pattern of duct papillomatosis or that of a solitary benign intraductal papilloma on a stalk (Figs. 1-8).
3. T h e small epithelial nests and glands which at first may suggest an invasive desmo- plastic carcinoma are made up of cytologically benign cells, and where they are arranged in

No. 3 SCLEROSING PAPILLARY PROLIFERATIONS - Fenoglio and Lattes 699
TABLE 1. Summary of Clinical Correlations ~~
Pathology Other findings Case no. Ane Clinical findings Treatment Previous Synchronous Subsequent Followup
-
1
2
3
4
5
6
7
8
9
10
1 1
12
13
14
15
16
1 7
18
19
20
21
22
23
24
25
26
27
28
29
30
B 52582
B 47344
B 66517
B 66245
B 44363
A 59723
A 93640
B 56840
P & s 84150
P s 83110
P & s a4280
P & S 80329
P & S 19944
P & S 73082
P & S 16225
P & s 78844
P & S 78292
P & S 68154
P & S 61131
P & S 75881
P & S 84365
P & s 83202
B ass52
A 14077
C 22663
P & S 84562
P & S 65745
P & S 67967
P & S 81334
B 99316
36 lump*
47 lump*
49 lump*
44 painful lump*
41 recurrent lump*
46 recurrent lump*
35 lump*
55 lump*
19 lump*
38 lump*
38 recurrent lump*
49 lump*
15 lump*
45 local tenderness
41 lump*
53 bloody nipple discharge
45 lump*
65 lump with skin
42 lump*
fixation*
local excision
local excision
local excision
local excision
local excision
local excision
local excision
local excision
local excision
simple mastectomy
local excision
simple mastectomy
local excision
local excision
local excision
local excision
local excision
local excision
radical mastectomy
none
none
none
CD
papillomat osis
papillomatosis
none
none
none
sillicone prosthesis 11 yrs. prev.
papillomatosis
none
none
none
none
none
none
none
none
67 intracystic mass* local excision none
41 not known local excision none
33 lump* local excision none
50 lump* local excision LN
47 not known local excision none
42 lump* local excision none
50 lump* local excision none
52 lump* radical mastectomy none
48 lump* modified radical none
28 lump* local excision none
64 lump* local excision CA opposite
mastectomy
breast 13 years Drevious
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
none
recurrence S P 4- CD
CD + papill.
none
none
none
none
5 years
6 years
5 years
3 years
6 years
12 years
10 years
6 years
4 years
9 years
CD 4 years
CD contralateral 7 years breast
none 7 years
none 2 years
none 8 years
none 1 years
none 8 years
none 1 1 years
none 11 years
none
none
none
none
none
none
none
intraductdl CA + LN
none
none
none
none
none
none
none
none
none
Microscopic intraductal CA opposite breast
none
LN
none
recurrent S P LN same breast
1 1 years
4 years
5 years
4 months
1 year
4 years
3 yearst
12 years
1 1 years
6 years
2 years
* In all cases, the palpable lump was caused by either cystic disease or adenosis. or a combination of both. t Died 3 years later of cardiovascular disease. LN-lobular neoplasia (lobular carcinoma in situ) ; CD-cyst ic disease; SP-sclerosing papillomatosis.
glandular fashion, they almost always show the double row of cells characteristic of be- nign (normal or hyperplastic) mammary epi- thelium. Rather than an invasion of the epithelial elements in the stroma, there is an “invasion” of fibrous reparative tissue in a pre-existing papillary proliferation, possibly following hemorrhage. The epithelial ele-
ments become trapped in this scar tissue and this is what leads to the pseudoinvasive pattern. 4. The “pseudoinvasion” is limited to the
immediate peri-ductal zone. Involvement of the interlobular fat should suggest a true carcinoma (Figs. 9, 10).
The importance of recognizing the mis-

700 CANCER March 1974 VOl. 33
leading histologic features of this benign this reaon that we decided to describe in lesion is obvious, in order to avoid unneces- detail this condition and to document its sary and unjustified major surgery. It is for benign clinical course.
REFERENCES
1. Evans, W. P.: Histological Appearance of T u - mors, 2nd ed. London, E. & S. Livingstone Ltd., 1966; p. 822.
2. Haagensen, C. D.: Diseases of the Breast, 2nd ed. Philadelphia, W. B. Saunders Co., 1971; p. 260.
3. Haagensen, C. D., Lane, N., and Lattes, R.: Neoplastic proliferations of the epithelium of the mammary lobules. Surg. Clin. North Am. 52:497-524, 1972.
4. Haagensen, C. D., Stout, A. P., and Phillips, J. S.: The papillary neoplasms of the breast. Ann. Surg.
133: 18-36, 1951. 5. Kraus, F. T., and Neubecker, R. D.: The differ-
ential diagnosis of papillary tumors of the breast. Cancer 15:444455, 1962.
6. McDivitt, R. W., Stewart, F. W., and Berg, J. W.: Tumors of the breast. Atlas of Tumor Pathology. 2nd series, fasc. 2. Washington, D.C., Armed Forces Institute of Pathology, 1967.
7. Nakazawa, H., Rosen, P., Lane, N., and Lattes, R.: Frozen section experience in S O 0 0 cases. Am. J . Clin. Pathot. 49:41-51, 1968.