Embed Size (px)
Citation preview

The Cfflwdian ZMedical oAssociation Journal£e Journal de VAssociation medicale canadienne^June 5,1971/Volume 104, Number 11
Scintigraphy and arteriography in the diagnosisof diseases of the liver
I. Wang, D. E. Wood, m.d., f.r.c.p.[c], f.a.c.p., R. F. Colapinto, m.d., f.r.c.p.[c]and B. Langer, m.d., f.r.c.s.[c], f.a.c.s., Toronto
Summary: Arteriograms and scans performed over a five-year period on 60patients with suspect hepatic disease have been reviewed. The diagnosis was
proved in every case by biopsy, autopsy or laparotomy. Scintigraphycorrectlypredicted thepresence or absence ofdisease in 75% and arteriographyin 75% ofcases. Fifty-four ofthe patients had hepatic disease. In 81% ofthesethe accurate diagnosis ofdiffuse or localized disease was made by one or bothtechniques. Arteriography is preferred for the detection of localized lesions,but diffuse processes are more readily demonstrated by scintigraphy.
Many investigative techniques maybe employed in the diagnosis of liverdisease. Biochemical tests, thoughharmless, tend to be non-specific,while the more specific proceduressuch as needle biopsy, peritoneoscopyand laparotomy carry significant riskto the patient. Scintigraphy and arter¬iography have also been used, and thepresent study assesses the value ofthese techniques in the investigationof patients suspected of having liverdisease.
Hepatic scintigraphy, introducedby Stirrett, Yuhl and Libby1 in 1953,has become increasingly refined as
radiopharmaceuticals and in-strumentation have improved. Theiodinated human serum albumin(131IHSA) originally used was sup-planted by colloidal particles. Theseare phagocytosed by the reticuloen¬dothelial system, principally by theKupffer cells. Subsequently, 131I rose
bengal, a dye which is taken up by theparenchymal cells, was introduced.At the present time 198Au gold colloidand WmTc sulphur colloid are in mostfrequent use. Iodine-131 microaggre-gated albumin and 131mIn have also
been employed. Technetium-99m sul¬phur colloid is presently considered tobe the radiopharmaceutical ofchoice.2 Its short half-life and mono-
energetic gamma emission associatedwith the energy peak of 140 KeVpermit greater activity with subse¬quent higher count rates, more effi¬cient collimation and less radiationexposure than gold colloid.
In diffuse disease the scan oftenshows a generalized decrease in activ¬ity throughout the liver, whereas lo¬calized lesions generally appear as
"cold areas". In chronic hepatocellu-lar disease with splenomegaly, ex-
trahepatic reticuloendothelial uptakeis usually found.2 RES uptake is par¬ticularly marked in 99mTc sulphur col¬loid scans which demonstrate splenicactivity in normal subjects.
Hepatic scintigraphy has been eva-
luated extensively, and studies em-
ploying 131IHSA,3 colloidal 198Au and1311 rose bengal4'10 have been widelyreported in the literature. On the basisof five previous studies, Conn andElkington11 calculated the combinedaccuracy of hepatic scintigraphy indetecting the presence or absence of
space-occupying disease as 85%.Arteriography ofthe liver was first
described by Bierman et al.12 in 1951,but it was after the description ofpercutaneous catheterization bySeldinger13 in 1953 and Odman14 in1958 that the procedure became wide¬spread. One ofthe authors (R.F.C.)15reports that the absence or presenceof liver tumours can be shown in 91%of cases by arteriography.
Materials and methodsThe files were reviewed of 60 patientswho had both a hepatic arteriogramand a hepatic scan performed on thesame admission. All were in-patientsat the Toronto General Hospital be¬tween October 1964 and May 1969.From a search of patient records
the diagnoses which had been reachedon the basis of scintigraphy and arter¬iography were determined and com¬
pared. In every case the final diagno¬sis was made by biopsy, autopsyand/or laparotomy. Tissue materialwas available in most cases, as aresult of either biopsy (60%) or autop¬sy (22%), to permit confirmation of
1. Wang, third-year medical student, University ofToronto, Toronto, Ontario.D. E. Wood, m.d., f.r.c.p.[c], f.a.c.p., Head, Divi¬sion of Nuclear Medicine, Toronto General Hospital,Toronto, Ontario; Assistant Professor, Departmentof Medicine, University of Toronto.R. F. Colapinto, m.d., f.r.c.p.[c], Assistant Profes¬sor, Department oF Radiology, University of Toron¬to.B. Langer, m.d., f.r.c.s.[c], f.a.c.s., AssistantProfessor, Department of Surgery, University ofToronto.Reprint requests to: Dr. B. Langer, Room 124,University Wing, Toronto General Hospital, Toronto2, Ontario.
C.M.A. JOURNAL/JUNE 5, 1971 VOL. 104 989

the final diagnosis. In addition, themajority of the patients underwentlaparotomy (75%).ArteriographyCeliac and superior mesenteric arteri-ograms were obtained on 59 patients.In one case an aortogram providedvisualization ofthe hepatic vessels.A red Kifa catheter was introduced
into the femoral artery by the Seld¬inger technique and approximately 30ml. ofHypaque was injected into eachof the celiac and superior mesentericarteries. Successive films were ob¬tained in the anteroposterior projec¬tion and some were supplementedwith lateral views.
ScintigraphyAnterior scanning of the liver was
performed on 60 patients; most werealso scanned in the right lateral pro¬jection. Fifty-seven patients werescanned with colloidal 198Au using a
Nuclear-Chicago Pho-Dot scanner
(3-inch crystal, 19-hole focusing col¬limator, speed 30 to 45 cm. per min¬ute, suppression 10 to 30%). Thescan was commenced four to 24 hoursafter injection. The remaining threescans were performed using 99mTcsulphur colloid between five and 100minutes after injection (37-hole fo¬cusing collimator, speed 90 cm. perminute, suppression 10%). The ad¬ministered dosages were 1.5 uc. per
TABLE IPathological findings in 60 cases of suspected liver disease
Localized lesionsPrimary hepatic tumour 6
Hepatic cell carcinoma. 4Primary cholangiocarcinoma. 1Mixed hepatic cell and cholangiocarcinoma. 1
Secondary hepatic tumour 22Adenocarcinoma. 16Cholangiocarcinoma. 1Squamous cell carcinoma. 1Melanocarcinoma. 1Choriocarcinoma. 1Leiomyosarcoma. 1Metastases of unknown type. 1
Undetermined tumour 3Malignant tumour of unknown type. 3
Others 8Hemangioma. 2Hamartoma. 1Adenoma. 1Hydatid cyst. 2Septic abscess. 1Hematoma. 1
39Diffuse disease
Cirrhosis. 11Fatty liver. 1Zieve's syndrome with fatty liver. 1Chronic passive congestion. 1Budd-Chiari syndrome with portal vein thrombosis. 1
15
No liver pathology detected. 6
TABLE HAccuracy of scintigraphy and arteriography in detecting the presence or absenceof some hepatic abnormality and in demonstrating localized and diffuse disease
kg. body weight for gold colloid and 1mc. of technetium sulphur colloid.
ResultsThe diagnoses disclosed by surgicalor pathological examination wereclassified as: localized lesions (39cases), diffuse processes (15 cases) orlivers with no demonstrable patholo¬gy (six cases) (Table I). In each one ofthe latter group, laparotomy had beenperformed.
Comparative accuracy ofarteriography and scintigraphyThe arteriogram and scan reports ineach patient's file were used to com¬
pare the relative accuracy of arteriog¬raphy and scintigraphy in the diagno¬sis of hepatic disease (Table II). In nocase was the appearance of an en¬
larged liver considered sufficientproof that liver disease was present.The diagnosis as a result of scintigra¬phy and arteriography was consid¬ered correct: (a) if the presence orabsence of disease was detected,whether or not the stated diagnosiscorresponded in any respect to theactual disease present in the liver; (b)if, when the disease was detected, itwas correctly identified as localizedor diffuse (Table II).The following results were ob¬
tained: (a) In 45 of 60 (75%) patientswith suspected hepatic disease thepresence or absence of disease was
determined by scintigraphy. The ac¬
curacy of arteriography was also75%. (b) The demonstration of hepat¬ic disease and its identification as
localized or diffuse was accomplishedin 37 of 54 (69%) cases by scintigra¬phy and in 35 of 54 (65%) by arteriog¬raphy.
Accuracy ofarteriography andscintigraphy combinedThe accuracy of the combined tech¬niques of arteriography and scintigra¬phy in detecting the presence or ab¬sence of disease and in correctly iden-tifying the disease as localized or
diffuse was determined (Table III).By employing both techniques, dis¬ease was demonstrated and its distri¬bution correctly identified in 44 of 54patients(81%)(Figs. la, lb, 2a,2b, 3aand 3b).
Correct diagnosis by scintigraphy butnot by arteriographyArteriographic investigation failed todisclose a correct diagnosis in nine
990 C.M.A. JOURNAL/JUNE 5, 1971 VOL. 104

cases where scintigraphic investiga¬tion was successful (Table III). Sever¬al of these cases merit description.
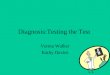
Case l. A 6-cm. mass in the left loberevealed at laparotomy proved to be a
hamartomatous bile duct malformationwith congenital hepatic cysts. Stenosisand irregularity ofthe vessels around theceliac axis noted at arteriography werebelieved to be suggestive of pancreaticmalignancy. A 6-cm. defect was visual¬ized in the left lobe by scanning (Figs. 4aand 4b).
Case 2. A case of metastatic diseasediagnosed by scintigraphy was missed byangiography owing to poor visualizationofthe liver as a result of dilated bowel.
Case 3. Cirrhosis ofthe liver was foundat laparotomy. The arteriogram hadshown intrahepatic obstruction but couldnot be more specific. The scan demon¬strated a diminution of isotope through¬out the liver.
Case 4. The arteriogram showed fillingof tumour vessels near the greater curva-ture of the stomach from the left hepaticartery. On this basis a diagnosis oftumourarising from either the stomach or theliver and invading the spleen was made, a
diagnosis erroneously implying hepaticinvolvement by the mass. The diagnosisfrom the scan was compression of a nor¬mal liver by an extrinsic mass. At laparo¬tomy a large fibrosarcoma of the spleenand a normal liver were found. At follow¬up three years later the patient was ingood health.
Correct diagnosis by arteriographybut not by scintigraphySeven cases of hepatic disease were
correctly identified by arteriographybut not by scintigraphy (Table III).Details of some of these cases are
given:Case 5. This patient had proved malig¬
nant disease ofthe liver. Multiple radiolu¬cent defects up to 6 cm. in diameter werevisualized in the hepatogram phase ofthearteriogram but no cold areas were notedon scanning.
Case 6. The arteriogram clearly de¬monstrated a small cirrhotic liver, whe¬reas the scan showed a well-defined areaofdecreased activity consistent with local¬ized disease.
Case 7. This patient with chronic chole-cystitis had a negative angiogram and a
positive scan. Metastatic disease was sus¬
pected on the basis of the scan but waslater disproved.
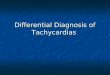
FIG.l.Hemangioma of right lobe of liver. (a) He¬patic scan shows large mass occupying most of rightlobe. (b) Celiac angiogram shows relatively avascularmass containing small persistent lakes of contrastmedium typical of hemangioma (arrows).
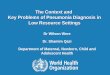
FIG. 3.Carcinoma of breast with metastases toliver. (a) Hepatic scan demonstrates irregular de¬creased activity and some splenic activity. (b) Celiacangiogram shows blush in scattered tumour nodules 1to 2 cm. in diameter throughout the liver (arrow).
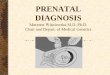
FIG. 2.(a) Hepatoma. The hepatic scan (198Au)shows a cold area 12 cm. in diameter situated on themedial aspect of the liver. (b) Celiac arteriogramdemonstrates abnormal vessels and a tumour blushtypical of hepatoma present throughout the enlargedliver.
Incorrect diagnosis by bothtechniquesIn 10 cases the diagnosis based oneither scintigraphy or arteriographywas incorrect. Several are discussedbelow.
FIG. 4.(Case 1) Hamartomatous bile duct malfor¬mation. (a) 198Au hepatic scan shows a 6-cm. defect inleft lobe. (b) Simultaneous celiac and superior me¬senteric arteriogram shows liver to be normal in sizewith no evidence of tumour.
Case 8. At laparotomy two nodules,one of which measured 4x4 cm. indiameter, were found in the liver. A tissuediagnosis of cholangiocarcinoma wasmade. The angiogram showed no evi¬dence of hepatic tumour. The uptake ofisotope was uniform, showing no evidence
C.M.A. JOURNAL/JUNE 5, 1971 VOL. 104 991

of cold areas on the scan, although theactivity throughout the organ was some¬what reduced. (Anterior view only per¬formed.)Case 9. This patient had primary bili¬
ary cirrhosis verified both at laparotomyand by biopsy. The angiogram showed a
large liver and spleen, the scan an en¬
larged liver, but aside from these findingsthe reports were negative.
Case 10. Laparotomy revealed no ab¬normal findings in the abdomen except anirregularly shaped liver with a flat leftlobe and a slightly enlarged spleen. Atangiography, enlargement ofthe left lobeof the liver by an avascular mass was
reported. The scan showed hepatomegaly;fairly localized disease ofthe left lobe wasbelieved to be present in view ofdecreasedactivity.
Additional studies"Blind" interpretation ofscintigraphyThe original interpretation of thescans was frequently made with priorknowledge of the patient's history aswell as his physical, radiological andlaboratory findings. In order to ob¬tain a more objective opinion of theirvalue, the scans were re-read by one
physician without the aid of clinicalinformation. Reporting the scans inthis manner improved the accuracy ofscintigraphy by 12% (Table IV). Thefollowing are possible explanations:
(1) When the scan was read initial¬ly, alternative interpretations were
frequently given. Unless priority wasgiven to one ofthese the diagnosis wasconsidered incorrect for the purposesof the present study. On re-readingthe scan the physician was limited to asingle opinion.
(2) Re-reading was performed in1969 when the interpretation of scanswas preceded by as long as five yearsof experience.Incidence ofvessel anomaliesAngiography is ofuse to the physiciannot only in detecting hepatic diseasebut also in displaying vessel anomal¬ies. The liver was supplied by a branchof the superior mesenteric artery innine of the 54 arteriograms in whichthat vessel was visualized (17%).Three of the branches served as sub-stitute hepatic arteries, five as acces-
sory right hepatic arteries, and one as
accessory right and left hepatic arter¬ies. Of 60 patients whose celiac arteryor celiac and superior mesenteric art¬eries were catheterized at angiogra¬phy, 11 (18%) demonstrated a leftgastric artery supplying the liver. In10 of these cases the artery was a leftauxiliary branch, and in one case
right and left auxiliary branches were
present. The splenic artery arose fromthe aorta in two patients. In four casesthe source of the left gastric arterywas an artery other than the celiac
TABLE IHAccuracy of scintigraphy and/or arteriography in demonstrating localized and
diffuse disease of the liver and normal liver
Localized, 39Diffuse, 15Total diseased, 54Normal, 16
27/39 (69)1/15 (7)
28/54 (52)2/6
3/39 (8)6/15 (40)9/54 (17)1/6
6/39 (15)1/15 (7)7/54 (13)2/6
3/39 (8)7/15 (47)10/54 (19)1/6
artery, either the hepatic artery, theaorta, the splenic artery or the superi¬or mesenteric artery. One case exhib¬ited a gastroduodenal artery arisingfrom the celiac axis.
DiscussionThe importance of hepatic scintigra¬phy and arteriography as diagnostictechniques has been extensively docu¬mented in the literature. Their valueis well estabiished. The subject oftheir combined and relative merit, onthe other hand, has received attentiononly recently.The techniques are useful in two
respects. By differentiating localizedfrom diffuse lesions of the liver theymay aid in indicating the need forsurgical intervention. They are alsouseful as adjuncts to needle biopsy.
In this series, scintigraphy correct¬ly predicted the presence or absenceof liver disease in 45 (75%) and arteri¬ography in 45 (75%) of the 60 cases
(Table II). Other studies of patientswith suspect disease report accuraciesof from 77% to 96% for scintigraphy1,7'16 and 91% for arteriography.15The techniques may be used in
combination to demonstrate local¬ized and diffuse disease. In 28 of 54(52%) cases both the scan and thearteriogram demonstrated the lesion.In an additional 16 cases, however,the disease process was shown by onlyone of the two techniques. A total of44 of 54 (81%) cases of liver diseasecould have been assigned the correctdiagnosis if both procedures had beenperformed. The increment in accura¬
cy as a result of performing bothprocedures certainly warrants theircombined use in the future.
Scintigraphy and arteriographyare therefore effective tools in combi¬nation. Together, their accuracy indetecting (but not diagnosing) space-occupying disease exceeds that ofblind needle biopsy, estimated at74%.17 Even at laparotomy (anotherprocedure involving risk to the pa¬tient) 15% of hepatic metastases mayescape detection.5 Scintigraphy andarteriography are clearly more specif¬ic than liver function tests, even
though certain tests correlate wellwith specific disease entities.18
Arteriography is slightly more reli¬able than scintigraphy in detectingspace-occupying disease (Table II).Our figures correspond with those ofother reports in which the accuracy iscited as 93% for arteriography12 and77% for scintigraphy.19 Despite these
992 C.M.A. JOURNAL/JUNE 5, 1971 VOL. 104

impressive rates, lesions as large as 6cm. in diameter escaped detection byboth methods in this series.
Diffuse disease is more readily de-tected by scintigraphy (Table II).Gheorghesco et al.20 found a "mot-tled" configuration in 70% of scans incases of diffuse disease. Rossi andGould21 cite the accuracy of arteri-ography in detecting cirrhosis as 91%,a high figure by comparison with thatobtained in the present study.
Rt.sumeLa scintigraphie el l'aru.riographiedans le diagnostic des h.patopathies
Nous avons passe en revue les art.rio-grammes et les scintigrammespratiqu.s pendant une p6riode de cinqans chez 60 malades soup.onn.s desouffrir d'une maladie h.patique. Lediagnostic a . confirm. dans tousles cas par biopsie, par laparotomie
ou & 1'autopsie. La scintigraphie, toutcomme 1'art.riographie, ont permisde pr.dire la presence ou 1'absence depathologie dans 75% des cas, parchacune des m&hodes. Une h.pato-pathie existait chez 54 malades. Chez81% d'entre eux, le diagnostic exactde maladie diffuse ou localis.e a pu&re pose par une des techniques oupar les deux. L'art.riographie estpr.f.rable pour d.ce1er les 1.sionsloca1is.es, tandis que Ia scintigraphiepermet de mettre en evidence plusfacilement les 1.sions diffuses.
References1. STIRRETT LA, YUHL ET, LIBBY RL:Surg Gynec
Obstet 96: 210, 19532. JONES EA: Gut 8: 418, 19673. STIRRETT LA, YU1-IL ET, LIBBY RL: Radiology
61: 930, 19534. BENDER MA, BLAU M: DETECTION OF LIVER
TUMORS WITH J131 Rose Bengal, in MedicalRadi-oisotope Scanning; Proceedings of SeminarJointly Organized by the International AtomicEnergy Agency and the World Health Organiza-tion, Vienna, Feb 25-27, 19S9, Vienna, Interna-tional Atomic Energy Agency, 1959, p. 83
5. OZARDAA,PICKRENJ: JNuclMed3: 149,1962
6. NAGLER, W, BENDER MA, BLAU M: Gastroen-terology 44: 36, 1963
7. GOLLIN FF,SIMsJL,CAMERoNJR: JAMA 187:111, 1964
8. MCAFEE JO, AUSE RG, WAGNER HN: ArchIntern Med(Chicago) 116: 95, 1965
9. CZERNIAK P: Dapim Refutim 26: 74, 196710. BARTLEY 0, HELANDER CO. ROSENGREN B, Ct
al: Ada Radiol [Diagn ] (Stockholm) 8:161, 196911. CONN HO, ELKINOTON SO: Gastroenterology
54: 135, 196812. BIERMAN HR, BYRON RL, KELLY KH, et al: J.
Nat Cancer Inst 12: 107, 195113. SELDINGER SI: Acta Radiol (Stockholm) 39: 368,
195314. ODMAN P: Acta Radiol (Stockholm) (suppl 159)
1, 195815. COLAPINTO RF:CanadMedAssJ99: 1175, 196816. CZERNIAK P, DEITCH M:Complete liver study by
combined RRB and 196Au examination, in Use ofRadioisotopes in A nimal Biology and MedicalSciences; Proceedings of Conference, MexicoCity, Nov 21-Dec 1, 1961, London, AcademicPress for the International Atomic Energy Agen-cy, 1962, V 2, p 303
17. WARD J, SCHIFF L, YOUNG P, et al: Gastroen-terology 27: 300, 1954
18. FENSTER LF, KLATSKIN O:AmerJ Med 31: 238,1961
19. CZERNIAK P: Scanning study of 700 livers; eva-luation of diagnostic procedures, in MedicalRadioisotope Scanning; Proceedings of Sym-posium, Athens, April 20-24. 1964, Vienna, In-ternational Atomic Energy Agency, 1964, v 2, p401
20. OHEORGHESCO B, JOVIN 0, PAVEL D, et al: RevRoum Med Intern 4:139, 1967
21. Rossi P, OOULD H R: Radiology 96: 553, 1970
Is Punishment Dead?For all its effect on the generation occupying the older side of 30, punishment,like God, is considered to be dead. It is as effective as holy water against aten-ton megaton bomb. Felons, misdemeanants, those who break the rules ofschool or university, and those who oppose their parents' fiats or flout goodtaste and decency are equally unaffected by the threat of punishment. Themilitant who captures the dean's office and hustles him out the side door andthe student who howls down as irrelevant an English professor's analysis ofBlake's poetry, unite in making punishment an anachronism, a senile maneuverat best, totally inadequate in today's scene.
Insensibly, during the past 50 years or more, crime has ceased being anevil and hence lost some of its function as whipping boy for the spirit of re-probation. Crime has become misbehaviour; this semantic change has wroughta tremendous influence on the unconscious feelings behind punishment andsoftened the moral thunderbolt hidden in it so that it appears as flat as lastnight's champagne instead of as strong as today's bitter medicine.
This changed attitude can be glimpsed at work in a secondary way in thesemantics of penology and sociology. Juvenile offenders, once called "incor-rigible children," now are classified as "wayward minors" or "beyond parentalcontrol"; chronic offenders are called "maladjusted"; jail birds are called "reci-divists"; "enemies of society" and "born criminals" are diagnosed as "chroniccharacter neuroses". Aggression in criminal areas has been democratizedand hallowed; no longer is there a criminal class from the ranks of the lowborn,the illiterate, the other-side-of-the-track citizens. "Misbehavers" carry their newdesignations as a badge of honour instead of the mark of Cain. This is espe-cially true for those whose aggression is in the service of pacifism, militantoverthrow of the educational establishment, or direct action aimed to "over-come .
The psychological fact is that lawful punishment is no longer a searing,coruscating experience to contemplate. In short the deterrent effect of punish-ment is close to zero. Here is the dilemma: law enforcement agents are essen-tial to our national life, but if punishment has lost its bite, is not this pain-staking labour of apprehending offenders and sentencing them a lost cause, amiscarriage of honest, well-meant effort?-Walter Bromberg, M.D., Amer. I.Psychiat., 127: 163, 1970.
C.M.A. JOURNAL/JUNE 5, 1971 VOL. 104 993