Embed Size (px)
Citation preview
School Immunization Programme in Malaysia
24 February to 4 March 2008
Dr Sigrun Roesel, WHO/WPRO
Dr Kaushik Banerjee, WHO/HQ
CONTENTS
Page
1. PURPOSE OF MISSION......................................................................................................................- 2 -
2. BACKGROUND ..................................................................................................................................- 2 -
3. ACTIVITIES AND FINDINGS ...........................................................................................................- 3 -
3.1 Activities ..................................................................................................................................- 3 -
3.2 Findings ...................................................................................................................................- 3 -
4. CONCLUSIONS AND RECOMMENDATIONS..............................................................................- 10 -
4.1 Conclusions............................................................................................................................- 10 -
4.2 Recommendations..................................................................................................................- 11 -
5. ACKNOWLEDGEMENTS ................................................................................................................- 11 -
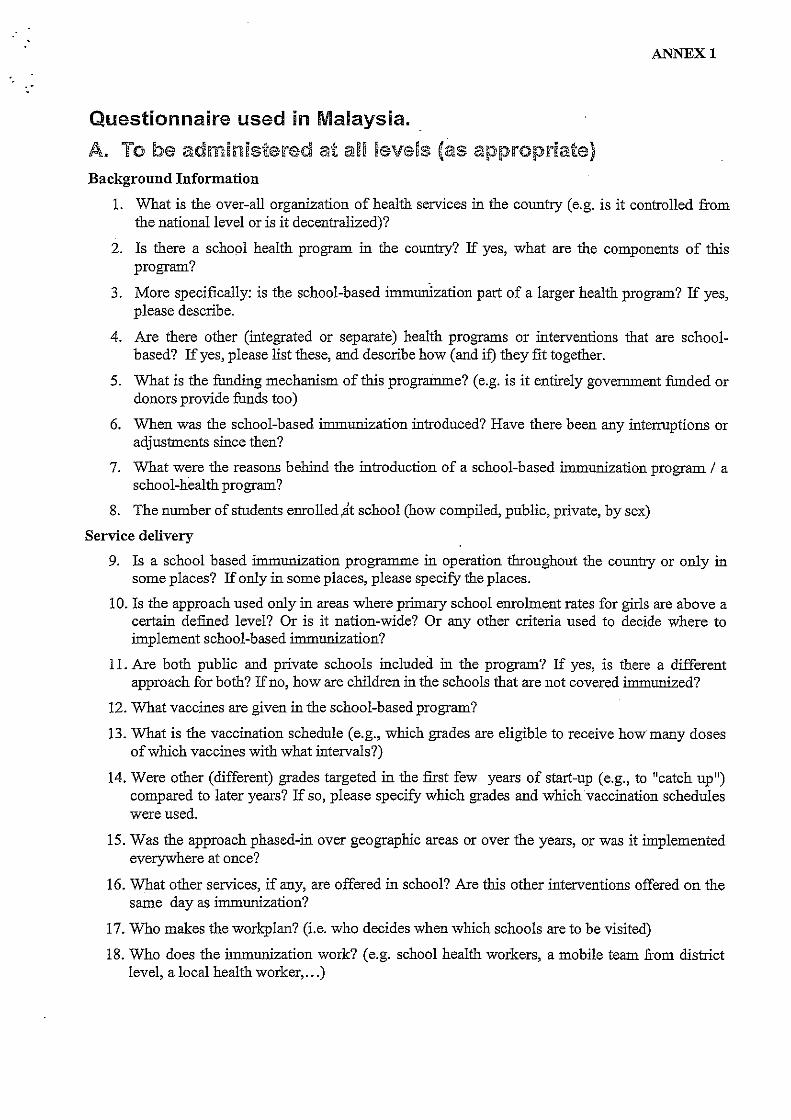
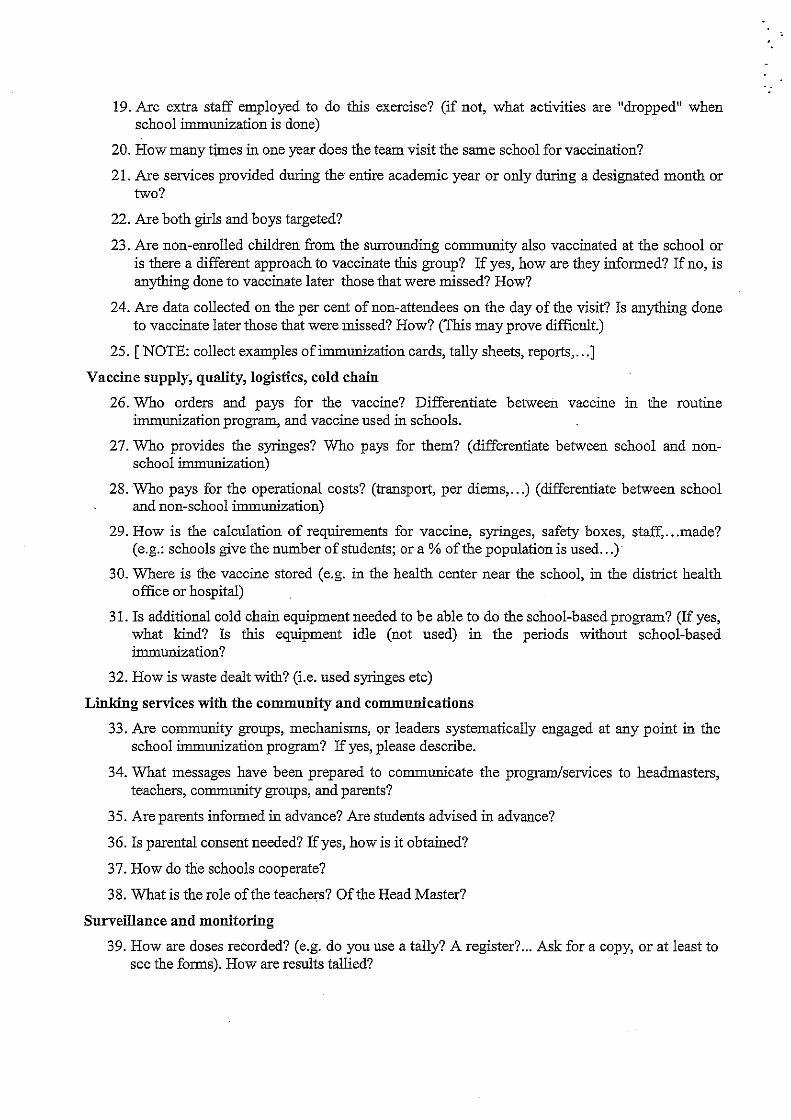
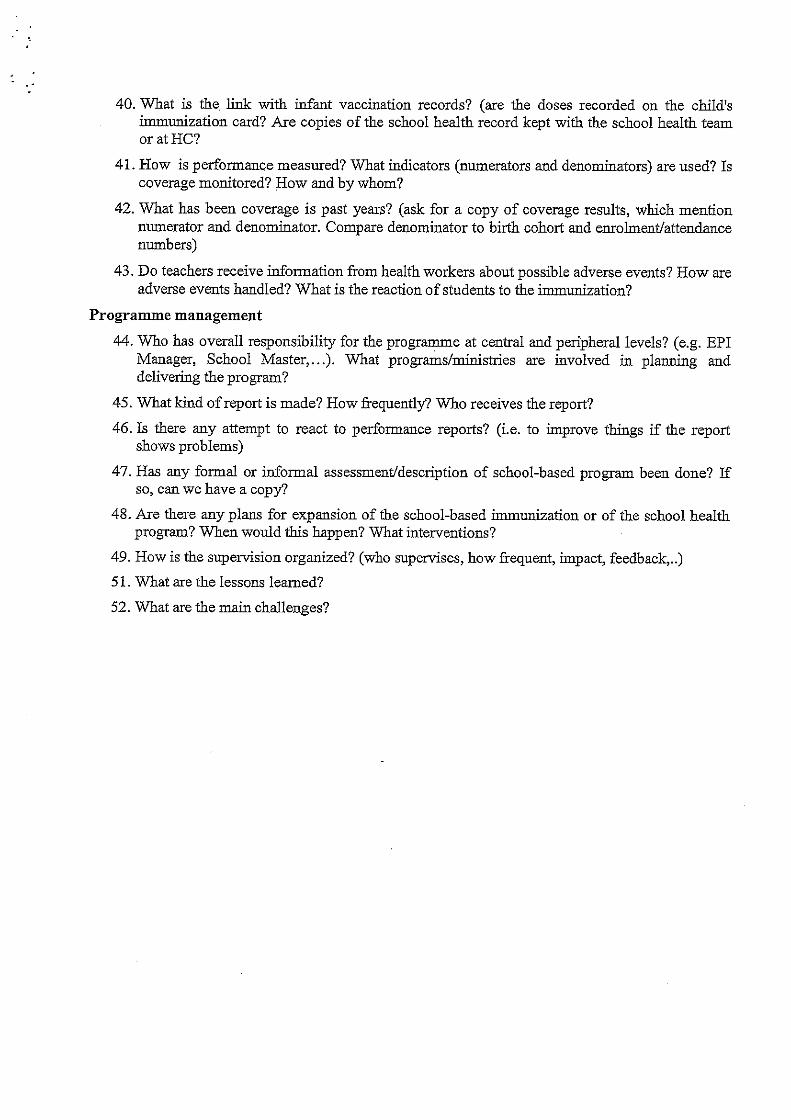
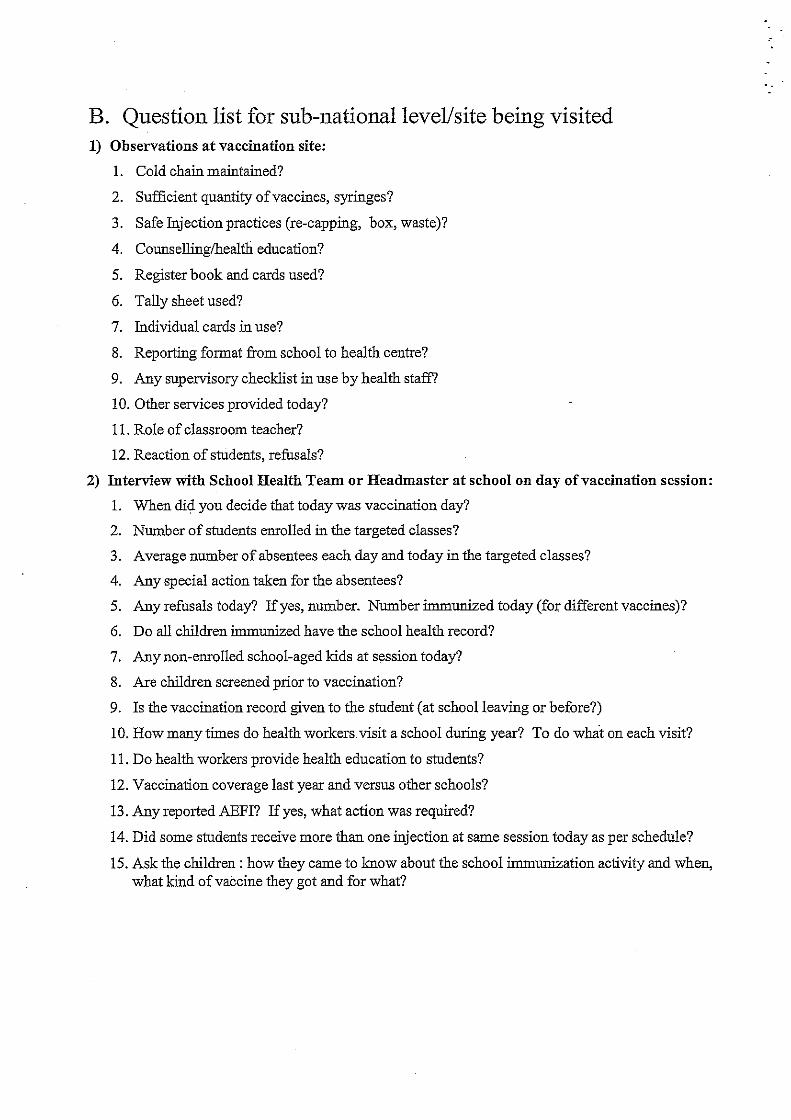
ANNEX 1 - QUESTIONNAIRE USED IN MALAYSIA
ANNEX 2 - IMMUNIZATION IN SCHOOLS – THE
MALAYSIAN EXPERIENCE
(DEBRIEFING PRESENTATION)
ANNEX 3 - REKOD KESIHATAN MURID
(SCHOOL HEALTH RECORD)
- 2 -
1. PURPOSE OF MISSION
The writers visited Malaysia from 24 February to 4 March 2008 to collaborate with the
Ministry of Health in documenting the national school-based immunization programme.
This goal was to be achieved by collecting information on the school-based immunization
programme at various levels using structured questions, reported data and observation of
processes.
The information collected from Malaysia and other selected countries will be synthesized
by WHO in order to produce a joint collaborative report on documentation of national
school-based immunization programmes.
2. BACKGROUND
The Global Immunization Vision and Strategy (GIVS) 2006–2015 was welcomed by the
WHO World Health Assembly (WHA) and UNICEF's Executive Board in 2005 as a means of
reaching the targets expressed by the United Nations Special Assembly on Children (2002).
In the first strategic area of the GIVS, which is to protect more people in a changing
world, Strategy 4 calls on countries to ''expand vaccination beyond the traditional target group''.
In this regard, it was noted that Malaysia is already implementing a national school-based
immunization programme, and it was therefore proposed to document the national system,
results, and experiences in order to guide other countries that might be interested in starting
school-based immunization.
The GIVS specifically promotes immunization of older age groups, and school-based
immunization could be one mechanism to do so. With human papilloma virus (HPV) vaccine
becoming available in the next few years, and with countries interested in introducing various
booster doses in childhood, a better understanding of school-based immunization is all the more
important.
Malaysia, together with other WHO Member States, endorsed GIVS during the 58th
session of the World Health Assembly in May 2005. The respective resolution urged all Member
States to adopt GIVS as the framework for strengthening national immunization programmes
between 2006 and 2015, with the goals of achieving greater coverage and equity in access to
immunizations, of improving access to existing and future vaccines, and of extending the
benefits of vaccination linked with other health interventions to age groups beyond infancy.
- 3 -
3. ACTIVITIES AND FINDINGS
3.1 Activities
Briefings were received at the WHO Representative's Office from Dr Nirmal Singh
(National Professional Officer) and at the Ministry of Health from Dr Saidatul Norbaya Buang
(Principal Assistant Director, School Health Unit, Family Health Development Division,
Department of Public Health) and Dr Rohana Ismail (Principal Assistant Director, Adolescence
and Child Health Unit, Family Health Development Division, Department of Public Health;
responsible for Expanded Programme on Immunization [EPI]).
The main purpose of this mission was presented to Dr Haji Ramlee bin Rahmat, Deputy-
Director General of Health (Public Health), and Mr Youssouf Oomar, UNICEF Representative to
Malaysia.
The writers then visited the school health team at the Putraya Clinic (main health centre)
and observed programme implementation for standard 1 (pupils 7 years old) at the Sekolah
Kebangsaan (SK) Putrajaya Presint 11. In Bentong District in Pahang, the writers met with the
District Health Officer, Dr Rosli Bin Ismail, and the school health team and observed programme
implementation at the SK Mempaga 2 for standards 1 and 6 (pupils 12 years old).
All discussions were guided by a structured questionnaire (after the draft version had been
slightly revised following the briefing at the WHO Office – Annex 1). Lessons learnt from
studying the school-based immunization programme in Malaysia were presented to
Dr Safurah Jafaar, Director of the Family Health Division at the Ministry of Health, and her team
at the end of the mission (Annex 2).
3.2 Findings
3.2.1 Background information
Malaysia is a confederation comprised of 13 states and the federal territories of
Kuala Lumpur, Putrajaya and Labuan Island off the eastern coast of Sabah. Each state is further
divided into several administrative districts.
Malaysia has a total population of 26 640 000 (Department of Statistics, 2006) of which
32.2% are under 15 years of age. The majority of the population is found in the peninsular
region (21.2 million), while Sabah and Sarawak account for the remaining 5.44 million of the
total population. The urban population accounts for about 63.2%, while the rural population is
about 36.8%.
The Government plays an important role as the main provider of public health services
through a national network of hospitals, clinics and other services. This is to ensure that the
objective of universal access to essential health services is attained. The efficient use of limited
resources has been achieved through an integrated national health care system that encompasses
both preventive and curative services.
The Vision for Health, which has been formulated in tandem with Malaysia’s Vision 2020,
i.e. to be a fully developed nation by the year 2020, is the country's goal. It envisages a nation of
healthy individuals, families and communities. It takes into consideration technology
- 4 -
development, cost, human values, and professional requirements to ensure a health care system
that is equitable, affordable, efficient, technologically appropriate, environmentally adaptable
and consumer-friendly. It emphasizes quality, innovation and health promotion, and stresses the
importance of individual responsibility and community participation in the enhancement of the
quality of life.
There are 128 government main and district hospitals throughout the country (Ministry of
Health, 2006). These are supported by 807 main health centres, 1919 community health clinics,
88 maternal and child health centres and 151 mobile clinics.
Public health services are delivered through various activities, which include disease
control, primary care, family health, food quality control, health education and dental services.
Child health services are rendered through a network of community and health clinics of the
public health services. In addition, urban children also utilize private medical facilities.
3.2.2 Programme management
School-based immunization in Malaysia is part of a comprehensive School Health
Programme (SHP) that was established in 1967 as a joint programme between the Ministry of
Health and the Ministry of Education after some pilot testing. Incorporation into the Maternal
and Child Health (MCH) Programme followed in 1971, and eventually, a joint committee
between the Ministry of Health and the Ministry of Education was established.
In 1995, WHO introduced the Health-Promoting School concept, based on the Ottawa
Charter for Health Promotion (1986), which was later accepted by the Ministry of Health. Some
modifications of the concept were done to strengthen the existing SHP, and the "Program
Bersepadu Sekolah Sihat" (PBSS) was officially launched in September 1997.
The aim of PBSS is to create healthy school citizens within a safe, healthy and quality
environment towards achieving Malaysia's Health Vision 2020. In order to achieve the
objectives of PBSS, six main cores have been developed (school health policy, school physical
environment, school social environment, community involvement, self-health skills, SHP).
Responsibility for implementation of the SHP lies with the Family Health Development
Division, Ministry of Health; staff at the School Health Unit include a public health physician, an
assistant medical officer, a matron and an administrative assistant.
Within the scope of the SHP, the Ministry of Health delivers primary prevention through
vaccination, health promotion, health screening, physical examination, curative and referral
services, dental health (separate team) and environmental health (assistant environmental health
officer). The Ministry of Education provides nutritional rehabilitation (school milk programme,
food supplementary programme) and health education through its curricula (physical and health
education, family life education, health across the curriculum). Both ministries allocate required
budgets accordingly.
SHP services cover all primary and secondary schools under the Ministry of Education;
private schools, less than 10% of all schools in the country, are covered upon request. As per
Ministry of Education website data, there were 7613 primary schools and 2045 secondary
schools under the Ministry of Education in 2006. School enrolment rates in Malaysia are usually
very high, as primary and secondary education are provided free of charge. Enrolment rates in
2006 were 95.6% for primary schools (6–11 years old), 87.36% for lower secondary
(12-14 years old) and 73.52% for upper secondary (15–16 years old). Problems may only exist in
areas with high numbers of migrants.
- 5 -
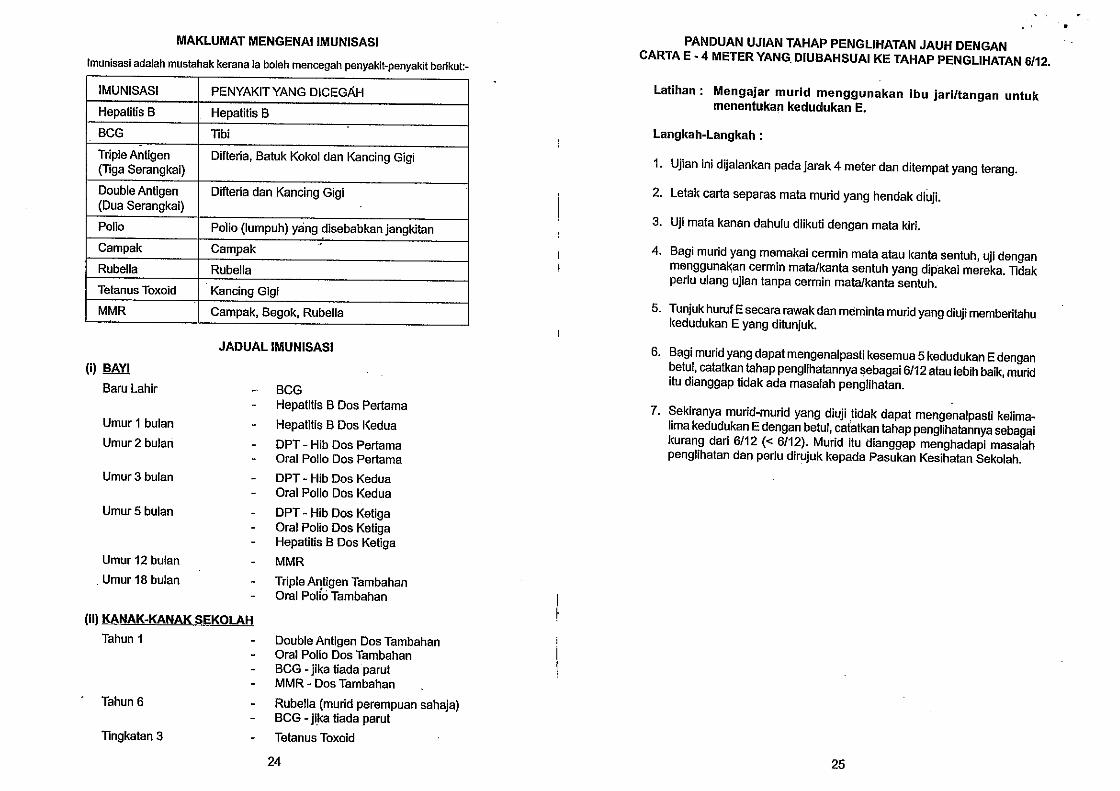
EPI saw the introduction of diphtheria-pertussis-tetanus (DPT) vaccine in Malaysia in
1958, Bacille Calmette-Guérin (BCG) vaccine in 1962, oral poliovirus vaccine (OPV) in 1972,
tetanus toxoid (TT) in 1974, measles vaccine in 1983, hepatitis B vaccine in 1989, and
Haemophilus influenzae type b (Hib) and measles-mumps-rubella (MMR) vaccines in 2002. The
uptake of MMR was relatively slow in the beginning due to vaccine supply problems, and girls
who may have missed vaccination should receive rubella vaccine. Up until 2009, all birth
cohorts should have had the opportunity to receive the vaccine.
BCG re-vaccination was stopped in 2001. In 2004, a 'catch-up' measles campaign was
conducted targeting 4.5 million children between the ages of 7 to 15 years from April through
June.
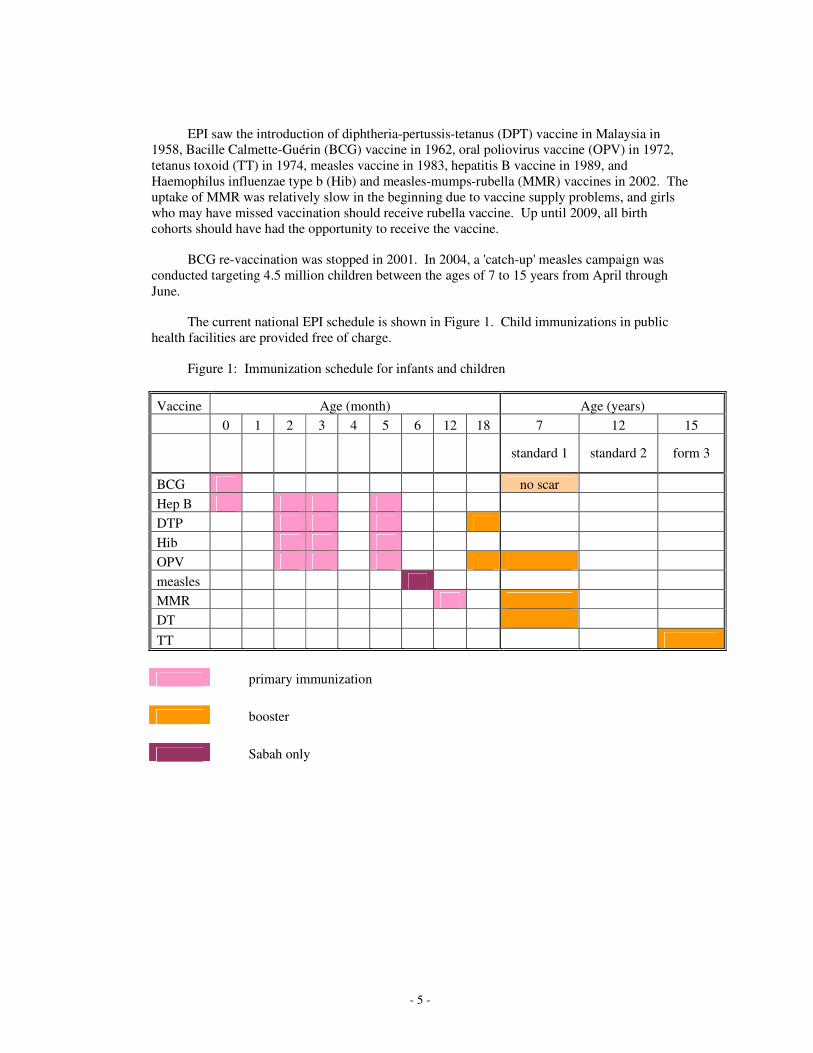
The current national EPI schedule is shown in Figure 1. Child immunizations in public
health facilities are provided free of charge.
Figure 1: Immunization schedule for infants and children
Vaccine Age (month) Age (years)
0 1 2 3 4 5 6 12 18 7 12 15
standard 1 standard 2 form 3
BCG no scar
Hep B
DTP
Hib
OPV
measles
MMR
DT
TT
primary immunization
booster
Sabah only
- 6 -
3.2.3 Service delivery
Services under the SHP, including immunization, are delivered by the school health team
based in district health offices or in health clinics, the school dental team and the inspectorate
team. A school health team is ideally composed of medical health officer, a public health nurse,
two community nurses, a nurse aide and a driver. One team should cover 3000–4000 students.
School health activities include the following:
(1) Immunization
(2) Health education
(a) physical health
(b) communicable diseases
(c) tobacco and drugs
(d) food hygiene
(e) nutrition
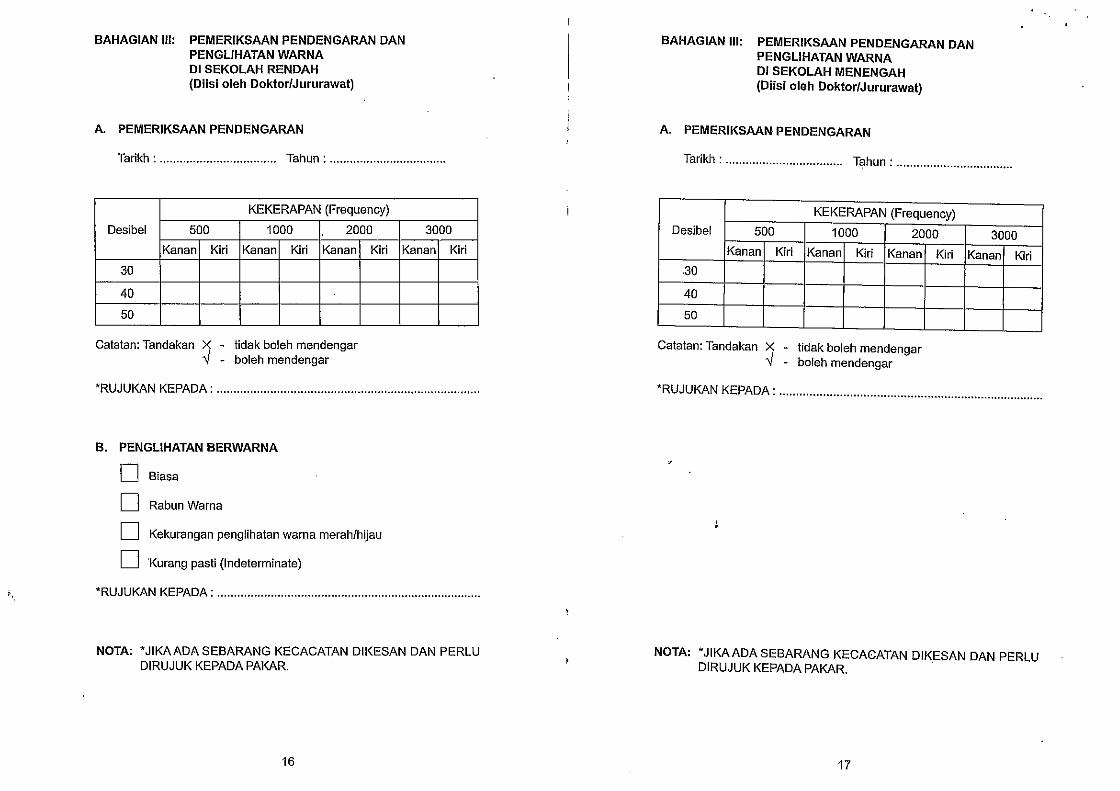
(3) Health examination
(a) hygiene
(b) anthropometry
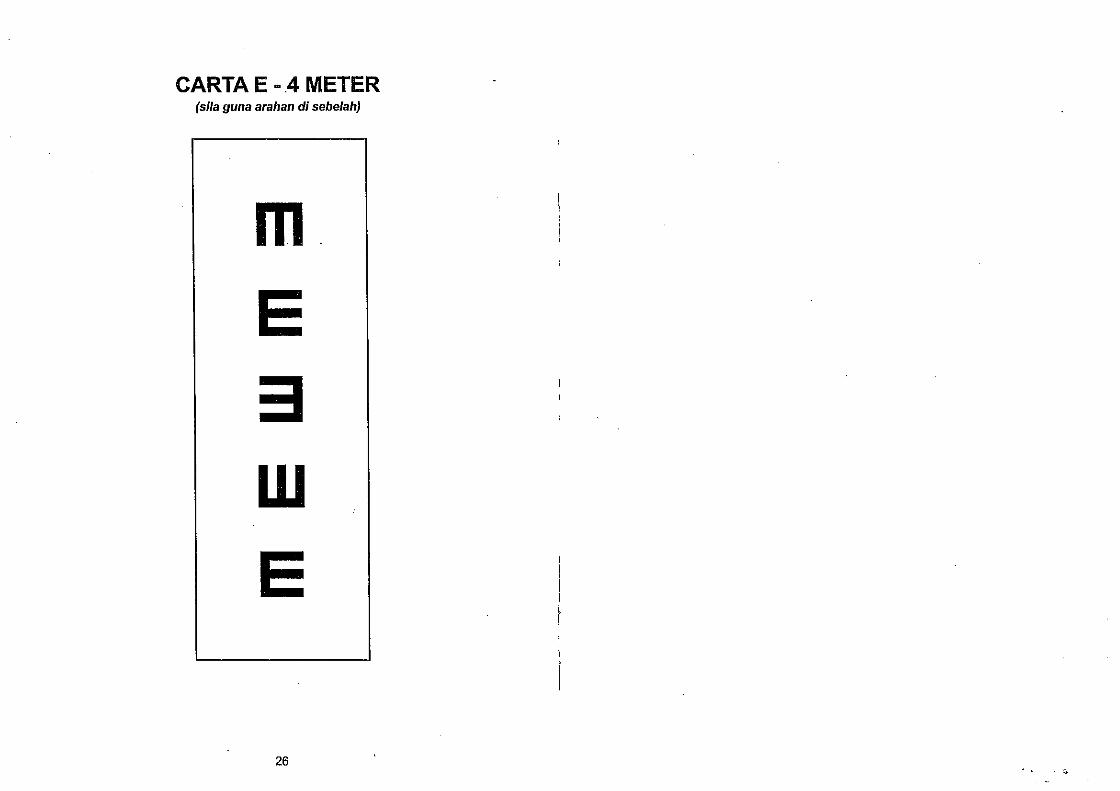
(c) visual screening
(d) hearing screening
(e) physical assessment
(4) Deworming
(5) Treatment of minor ailments
(6) Referral
(7) Peer-to-peer programme
(a) Young Doctors
(b) PROSTAR (HIV/AIDS education)
(8) School health inspections
(a) dengue vector control
(b) school canteen
(c) school environment
(9) School dental services.
- 7 -
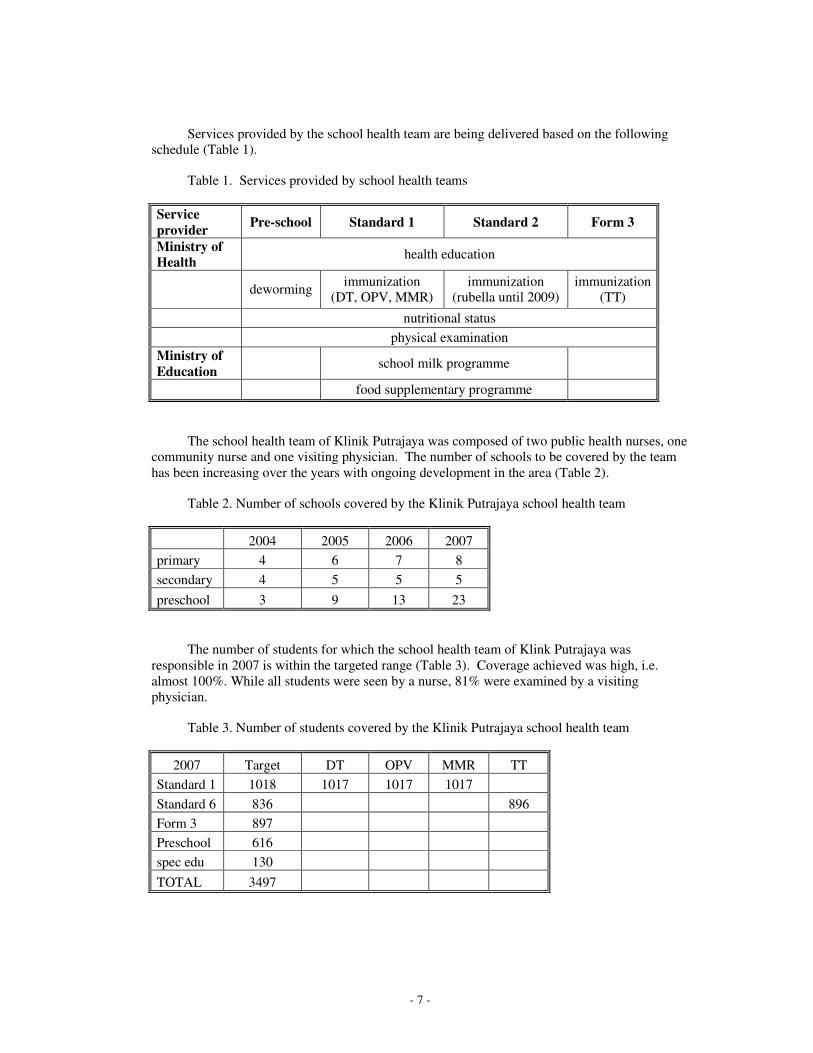
Services provided by the school health team are being delivered based on the following
schedule (Table 1).
Table 1. Services provided by school health teams
Service
provider Pre-school Standard 1 Standard 2 Form 3
Ministry of
Health health education
deworming immunization
(DT, OPV, MMR)
immunization
(rubella until 2009)
immunization
(TT)
nutritional status
physical examination
Ministry of
Education school milk programme
food supplementary programme
The school health team of Klinik Putrajaya was composed of two public health nurses, one
community nurse and one visiting physician. The number of schools to be covered by the team
has been increasing over the years with ongoing development in the area (Table 2).
Table 2. Number of schools covered by the Klinik Putrajaya school health team
2004 2005 2006 2007
primary 4 6 7 8
secondary 4 5 5 5
preschool 3 9 13 23
The number of students for which the school health team of Klink Putrajaya was
responsible in 2007 is within the targeted range (Table 3). Coverage achieved was high, i.e.
almost 100%. While all students were seen by a nurse, 81% were examined by a visiting
physician.
Table 3. Number of students covered by the Klinik Putrajaya school health team
2007 Target DT OPV MMR TT
Standard 1 1018 1017 1017 1017
Standard 6 836 896
Form 3 897
Preschool 616
spec edu 130
TOTAL 3497
- 8 -
Coverage rates achieved suggest that the number of students absent during school-based
immunization or the number of those who refused were usually low. During the activity
observed by the writers, one child of the 31 targeted was absent and the parents of another one
had refused vaccination.
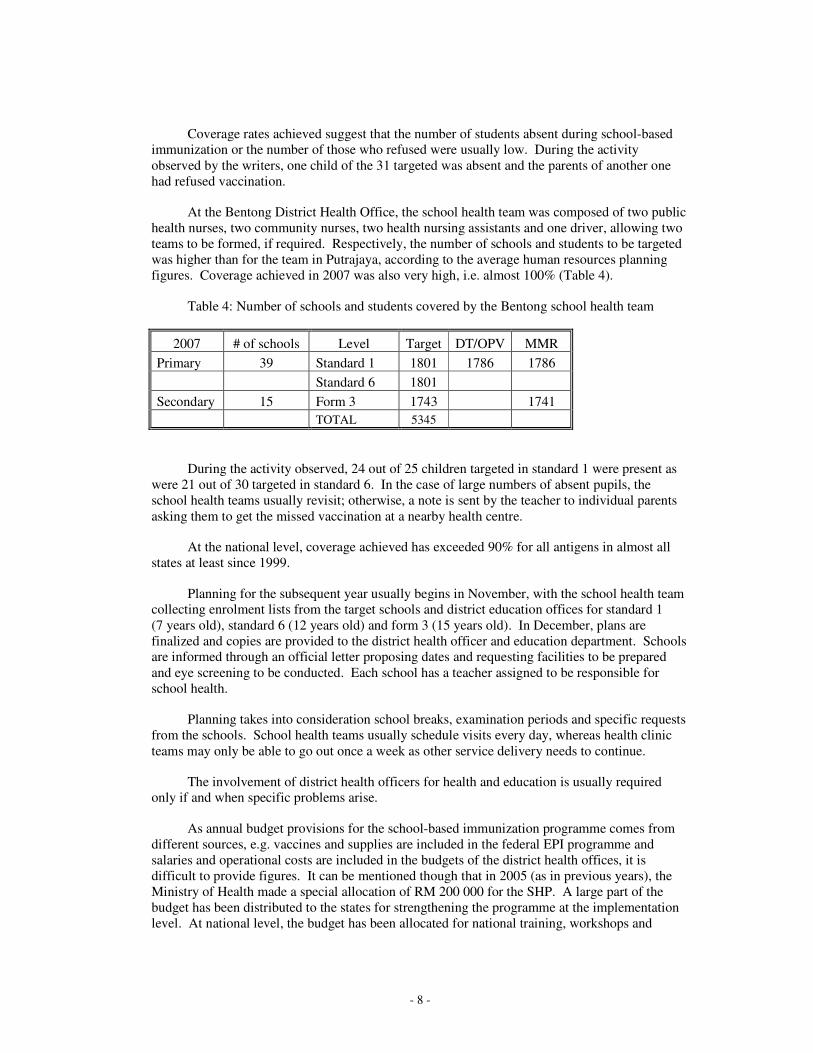
At the Bentong District Health Office, the school health team was composed of two public
health nurses, two community nurses, two health nursing assistants and one driver, allowing two
teams to be formed, if required. Respectively, the number of schools and students to be targeted
was higher than for the team in Putrajaya, according to the average human resources planning
figures. Coverage achieved in 2007 was also very high, i.e. almost 100% (Table 4).
Table 4: Number of schools and students covered by the Bentong school health team
2007 # of schools Level Target DT/OPV MMR
Primary 39 Standard 1 1801 1786 1786
Standard 6 1801
Secondary 15 Form 3 1743 1741
TOTAL 5345
During the activity observed, 24 out of 25 children targeted in standard 1 were present as
were 21 out of 30 targeted in standard 6. In the case of large numbers of absent pupils, the
school health teams usually revisit; otherwise, a note is sent by the teacher to individual parents
asking them to get the missed vaccination at a nearby health centre.
At the national level, coverage achieved has exceeded 90% for all antigens in almost all
states at least since 1999.
Planning for the subsequent year usually begins in November, with the school health team
collecting enrolment lists from the target schools and district education offices for standard 1
(7 years old), standard 6 (12 years old) and form 3 (15 years old). In December, plans are
finalized and copies are provided to the district health officer and education department. Schools
are informed through an official letter proposing dates and requesting facilities to be prepared
and eye screening to be conducted. Each school has a teacher assigned to be responsible for
school health.
Planning takes into consideration school breaks, examination periods and specific requests
from the schools. School health teams usually schedule visits every day, whereas health clinic
teams may only be able to go out once a week as other service delivery needs to continue.
The involvement of district health officers for health and education is usually required
only if and when specific problems arise.
As annual budget provisions for the school-based immunization programme comes from
different sources, e.g. vaccines and supplies are included in the federal EPI programme and
salaries and operational costs are included in the budgets of the district health offices, it is
difficult to provide figures. It can be mentioned though that in 2005 (as in previous years), the
Ministry of Health made a special allocation of RM 200 000 for the SHP. A large part of the
budget has been distributed to the states for strengthening the programme at the implementation
level. At national level, the budget has been allocated for national training, workshops and
- 9 -
printing of health education materials. The Ministry of Education provides the budget for
activities under its responsibilities (see Table 1).
3.2.4 Vaccine supply, quality, logistics
Under the Ministry of Health's central contract with a private procurement and delivery
service, vaccine orders are usually placed every four months and jointly for all EPI vaccine
requirements. If there is sufficient cold chain capacity, vaccines for infant and school
immunization are then stored separately at the district health office or clinic and the equipment
managed by the different teams. Similar ordering systems are in place for syringes and other
supplies, including safety boxes. Medical waste disposal has been outsourced to a private
company.
Quality control measures stipulate that for 10-dose vials of DT, TT and OPV only eight
doses are allowed for each vial to ensure that each child gets the adequate vaccine dosage. Data
are recorded into returns on vaccinations given, vaccine stocks and wastage into forms KKK 103
and KKK 104.
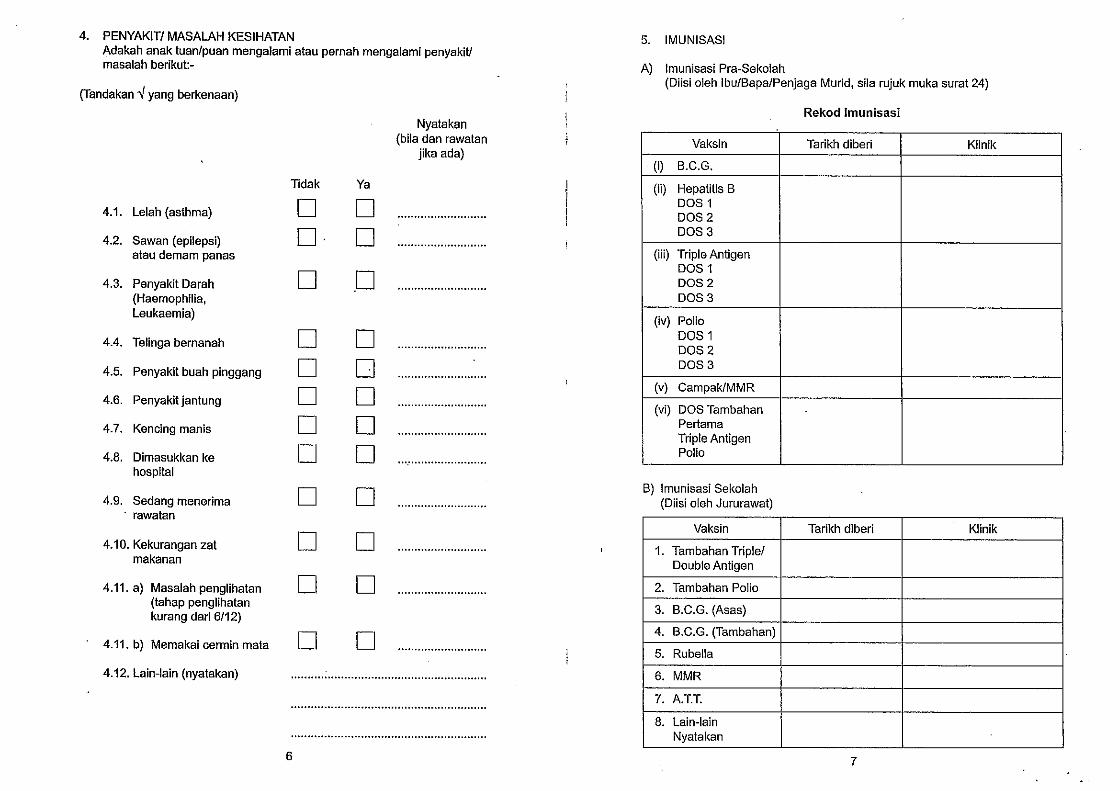
Management of adverse events following immunization (AEFI) is composed of
pre-screening for allergic reactions (documented in the school health record), referral of children
with history of allergies for observation after the vaccination, treatment of minor reactions at the
immunization site and referral to nearest health clinic or hospital, if required.
3.2.5 Linking services with the community and communications
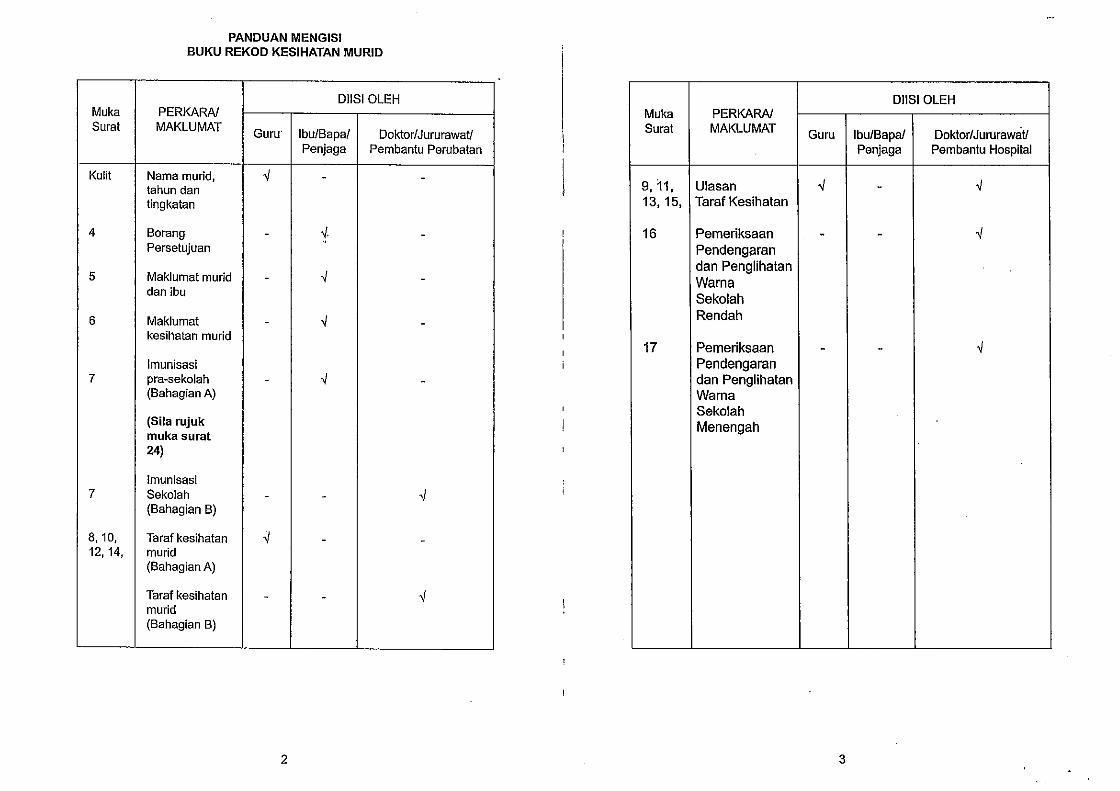
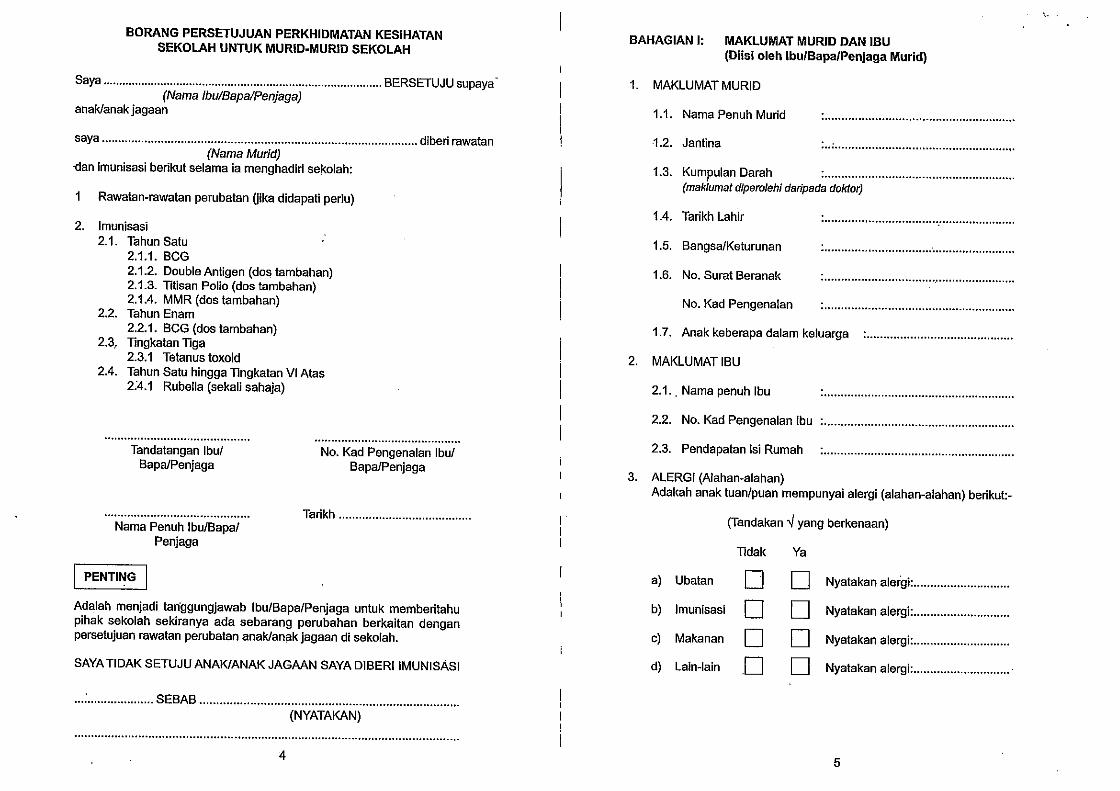
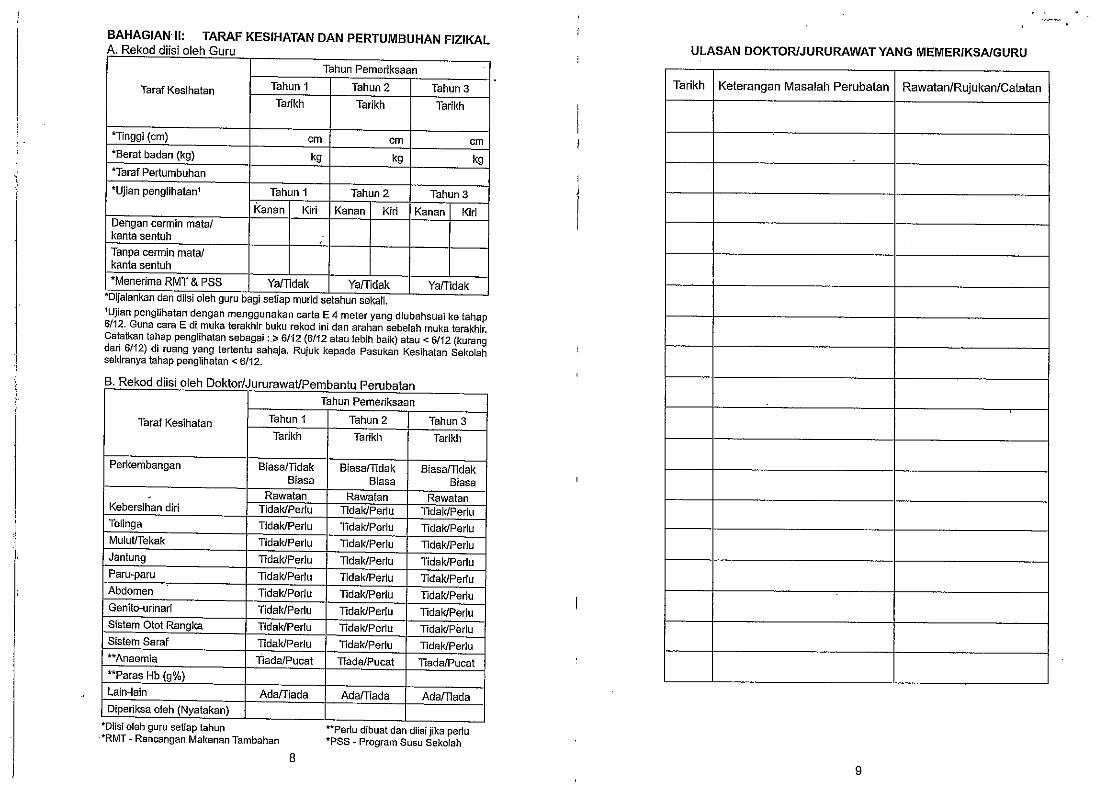
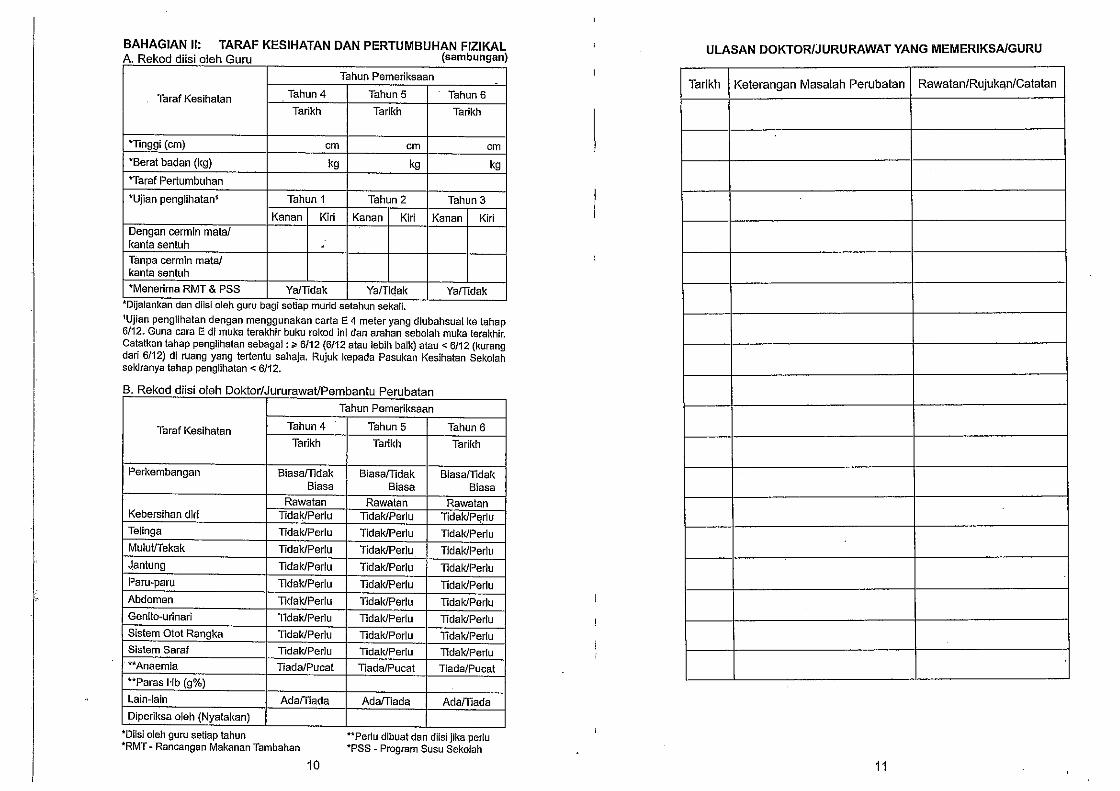
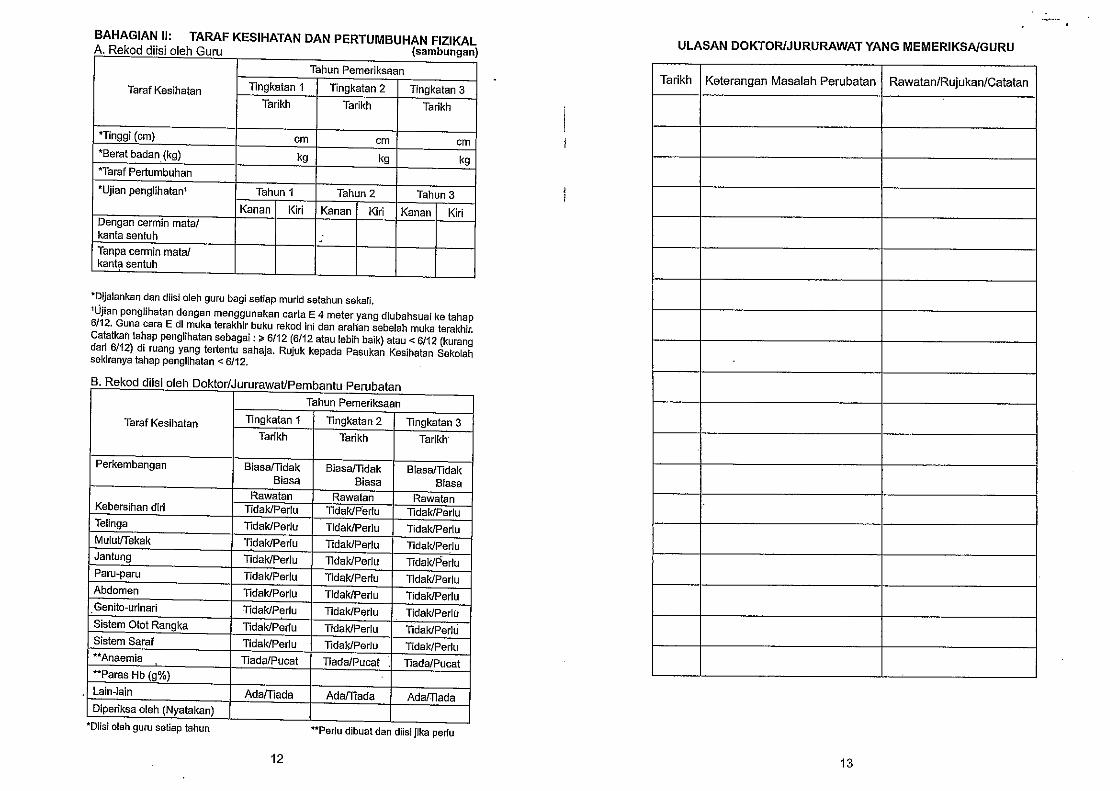
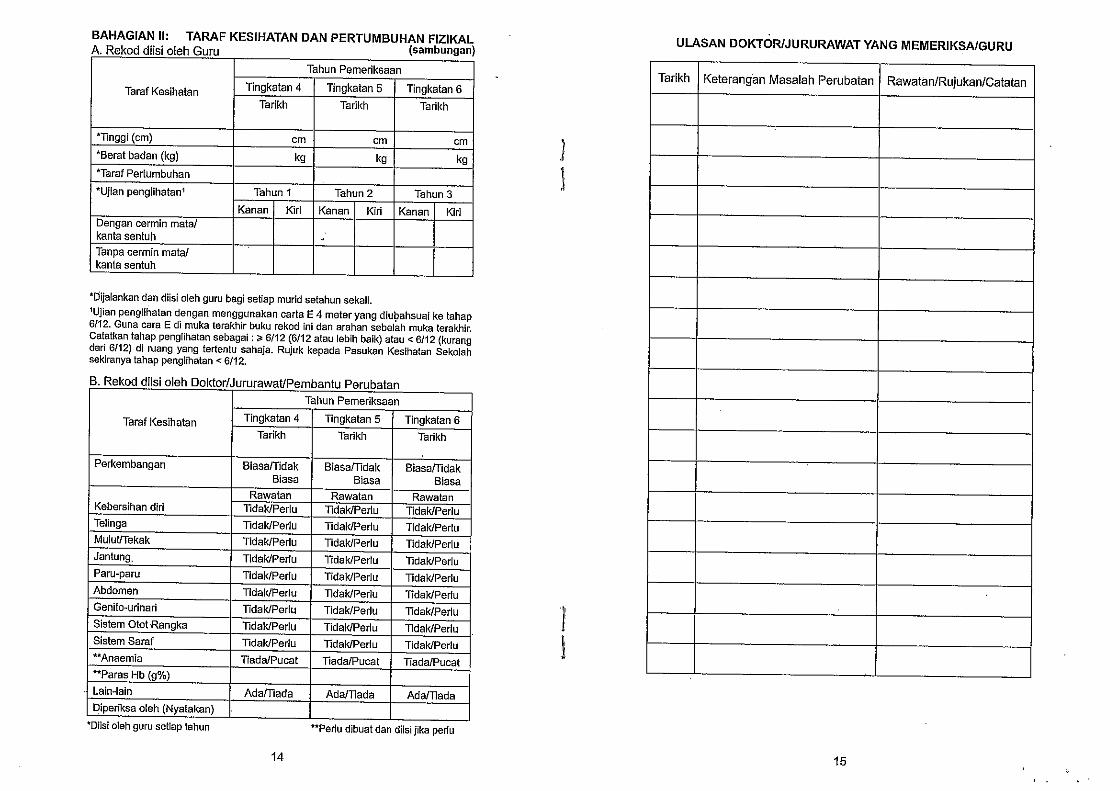
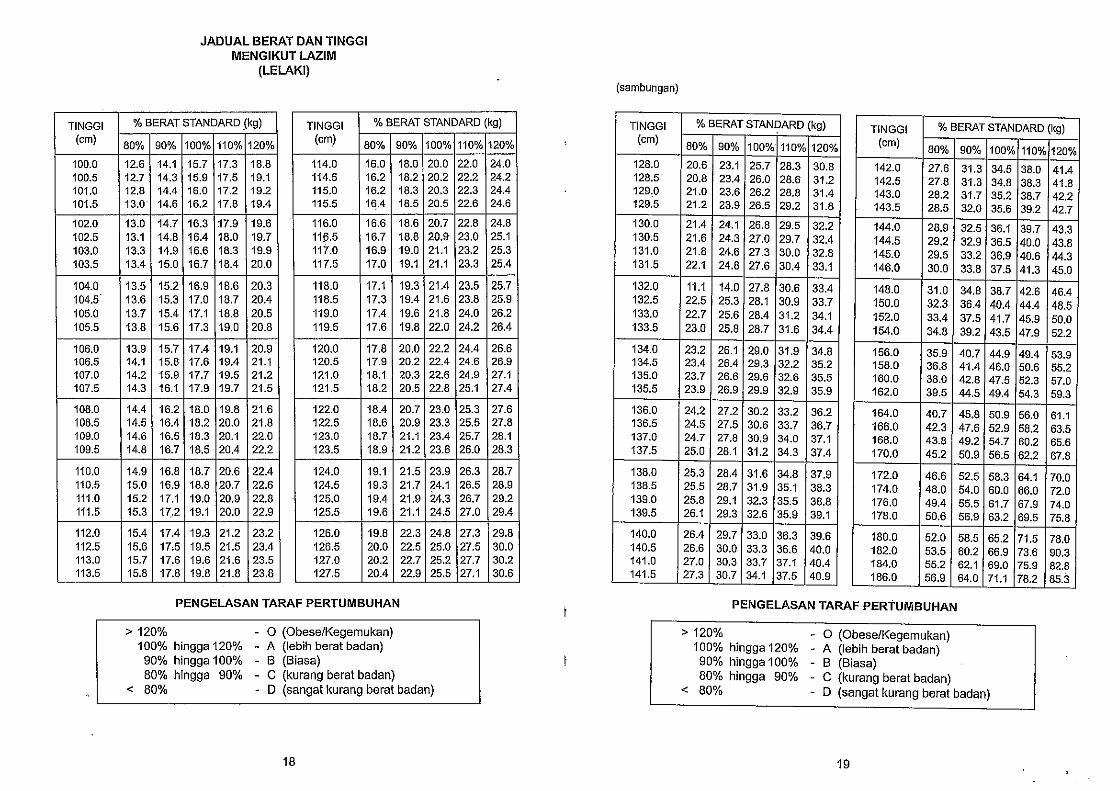
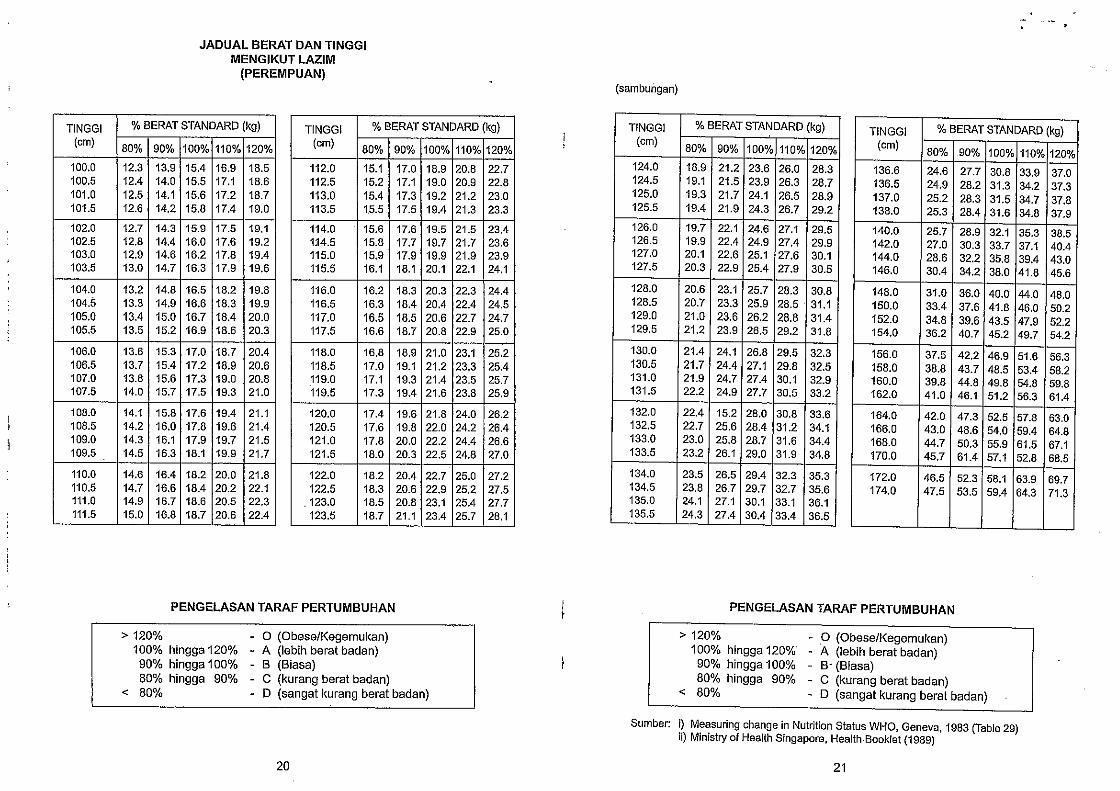
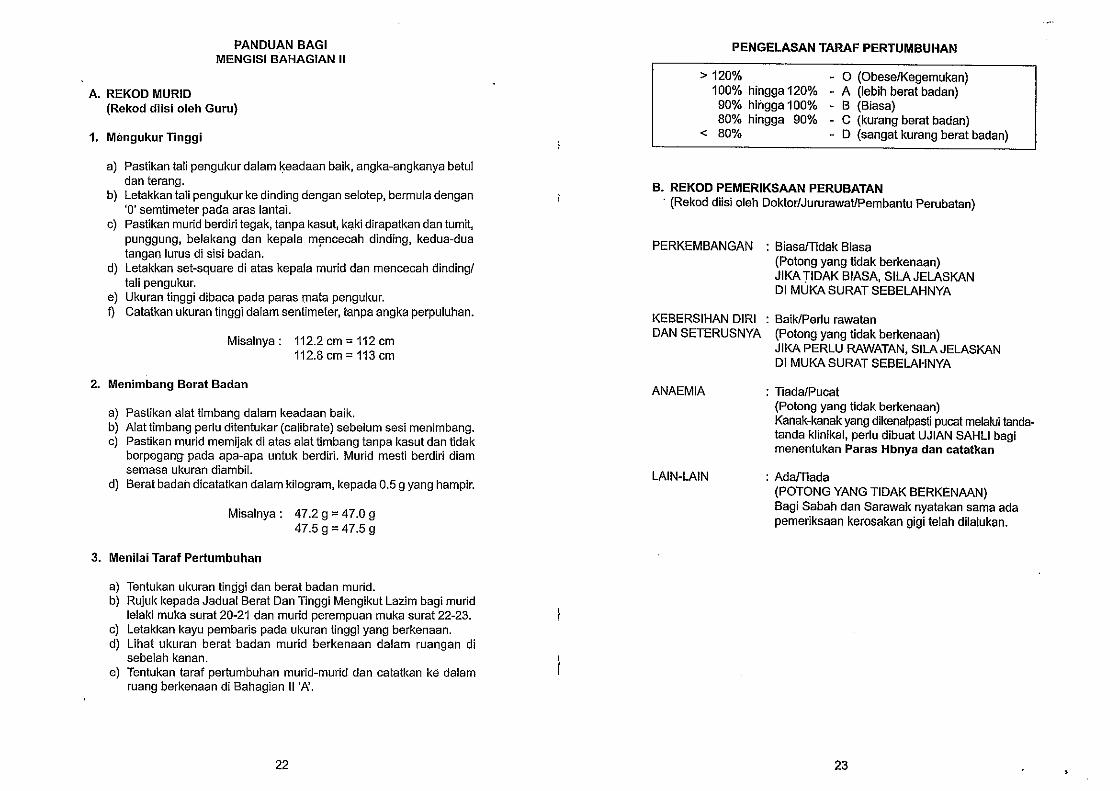
Upon first school enrolment, each child is provided with a school health record (Rekod
Kesihatan Murid, see Annex 3), which contains personal data, history (birth, diseases, and
previous immunizations), parental consent and health data (growth and development status,
vision and hearing, physical examination, school immunization, interventions carried out at
school and referrals). General parental consent in writing is only obtained at the beginning, and
based on the Education Act 1996, it is mandatory for parents to allow physical examinations. The
act is also binding for schools. However, if a student or parent refuses immunization, this is
accepted.
As the school health programme is very well established, no specific communication to
parents and communities is usually required; however, in case an issue would need to be
discussed, it could be brought to the attention of the health centre advisory panel, composed of
community members. This system was established during the mid-1990s by the then Deputy-
Director General of Health (Public Health) to establish links between the health centres and
communities.
3.2.6 Surveillance and monitoring
Data collection is, as for other health programmes, standardized, and returns follow the
following sequence: school health team or school health clinic to district health office, to state
health department to Informatics and Documentation System (IDS) unit at the Ministry of
Health; with data aggregation at each level and standardized reporting forms (KSK 101, KSK
102, KKK 103 and KKK 104) and schedules (district to state before the fifth day of the month;
state to national level before the tenth day of the month). The Ministry of Health introduced
electronic data submission in 2007, which will gradually be expanded to all services and levels
concerned.
- 10 -
Data collected include number of doses given and coverage achieved per antigen and age
group, morbidity rates for various health problems, height, weight and body mass index (BMI),
eyesight and hearing capacity and school health coverage by nurses and physicians.
As quality assurance of the school health programme, the percentage of visual defects of
schoolchildren in standard 1 is evaluated every six months. Districts with low rates of visual
defect detection (<5%) have to be further investigated.
A general evaluation of the school health programme is currently being conducted by the
Ministry of Health. The results are expected to provide future direction to the programme,
particularly in terms of cost effectiveness aspects.
4. CONCLUSIONS AND RECOMMENDATIONS
4.1 Conclusions
The school health programme in Malaysia has remained well established since its
inception in 1967, with a strong track record. It was initiated as a pilot programme and after
experience had been gained, it was extended nationwide.
While mainly managed and funded by the federal Ministry of Health, establishment as a
joint programme with the Ministry of Education has ensured close cooperation. Teachers are
involved in multiple functions (e.g. screen for vision defects, record height and weight, manage
school health records, liaise with parents if required, and organize the pupils during visits by the
school health team). Findings obtained by teachers are being assessed by the school health team
for quality control.
Strong school health teams have been created through adequate capacity-building (training
and periodic re-training, supportive supervision, etc.), and work is being guided by written
standard operating procedures, used nationwide and with infrequent operational changes, thus
ensuring universal awareness of procedures. Adequate resources are being provided, including
person power, transportation and free vaccines.
The programme targets all government schools (>90% of all schools) and also covers
private schools upon request. To include all nongovernment schools on a regular basis may be
worth exploring to achieve universally high coverage with interventions of the school health
programme. Good collaboration between the school health teams and the schools is fostered
through comprehensive planning (annual and/or monthly), thereby informing the schools in
advance of visit dates and being flexible if schedules need to be adjusted.
As the school health programme is based at the district health office, synergies with other
programmes can be exploited to ensure adequate number of school health staff, adequate
availability of transport and replenishment of vaccines and other supply stocks, if required.
Incorporating school-based immunization as part of a comprehensive school health
programme seems to facilitate the acceptance of vaccination as multiple and non-threatening
interactions take place between the members of the school health team and the pupils before
immunizations are being given. General parent consent obtained upon establishing the
individual school health records supports administration of all subsequent vaccinations. AEFI
management appears well established.
- 11 -
4.2 Recommendations
Although the objective of this mission was not an assessment of the school immunization
programme, the Ministry of Health team encouraged WHO recommendations following the
review of the programme. Hence, the writers would like to offer the following for future
consideration by the Family Health Programme:
In order to also provide long-term protection against diphtheria, a combined tetanus-
diphtheria (Td) toxoid vaccine should be given instead of TT for form 3 (15 years old students).
This is to also promote and sustain diphtheria immunity (details in WHO Position Paper on
Tetanus Vaccine, WER 2006, 81, 197-208).
Once information collected from Malaysia and other selected countries have been
synthesized by WHO into a joint collaborative report on documentation of national school-based
immunization programmes, it will be shared with the Ministry of Health of Malaysia.
If information and data from this review are used in WHO presentations, WHO will
indicate the source and state that the information was obtained through the courtesy of the
Ministry of Health, Malaysia.
5. ACKNOWLEDGEMENTS
The writers would like to express their deep sense of appreciation for the generous and
efficient support extended to them to study the school-based health and immunization
programme in Malaysia. The writers would also like to offer their sincere thanks and gratitude to
the warm hospitality received, as well as the valuable opportunity to observe and learn from a
sophisticated and energetic health programme.