Embed Size (px)
Citation preview

© Imprimis PR 2012
Indian Immunization ProgrammeA Literature Review
Imprimis Research and AdvocacyNovember 2012

Foreword
Vaccines are a strong health tool and have been cost-effective and successful in saving
children’s lives. But many areas in India still lack access to vaccines. It is therefore important that
Indian stakeholders and policy makers plan strategies to enhance the coverage of the National
Immunization Programme. Imprimis PR has launched a new Research and Advocacy wing
and we aim to embark on research in the Indian Immunization Programme to present
“Analysis, Learning and the Way Forward” in this domain. The study breaks new ground in
trying to identify a strategic action plan to increase immunization coverage. I hope practitioners
in this field and Indian strategists find this study useful. The views expressed herein should,
however, in no way be treated as the official views of Imprimis PR or its consultants.
Aman GuptaChief Executive Officer
Index
Section 1: Immunization Policy in India
1.1. Immunization Policy – History behind the programme 1
1.2. India Immunization Status 3
1.3. Role of Centre and State Government in Healthcare Financing 7
1.4. Decisive Factors Affecting Immunization 9
Section 2: Vaccination Market and Strategic Approach for India
2.1. Vaccine market and policy framework 13
2.1a.) Vaccine market 13
2.1b.) Introduction of new vaccine – Decision Making Process 14
2.2 Challenges and Strategic Action Points to improve immunization coverage 18
2.3. Conclusion 24
Section 3: Appendix and Reference (sources)
3.1. Appendix 1: India’s progress on the MDGs for 2015 27
3.2. Appendix 2 : WHO and UNICEF present country-level data on immunization status, Indian factsheet for 2010
27
3.3. Appendix 3: India reported immunization coverage 29
3.4. Appendix 4: Summary of WHO position papers - Recommendations for Routine Immunization (updated 31 May 2012)
30
Table and Figures Index 31
Frequently Used Abbreviations 31
References and Sources 32

Executive Summary
Immunizing children against vaccine-preventable diseases is a crucial instrument in saving lives, increasing productivity, and alleviating poverty. It is in this context that Imprimis Research and Advocacy has undertaken this study. We have begun with the literature review to understand the scope, development span, and role of the government and the current status for the success of the Indian Immunization Programme.
Section 1 helps in understanding the launch of the Immunization Programme in India. We have examined the history behind the programme, thereby highlighting the growth trajectory and current coverage status of the immunization programme. The study discusses the role of central and state governments in a successful campaign. We have done a review of existing studies to understand the determining factor affecting Immunization via use of regression model. Through this section we have done the ground analysis and presented the core literature in a nutshell.
Section 2 Vaccination policy, framework and authorities at work are crucial pivots in Indian Immunization Programme. We scrutinized decision making process necessary for introduction of a new vaccine in the immunization programme. There are challenges and obstacles that need to be taken care of by the policy managers and makers. The study presented the conclusion and strategic action points to reach the desired goal of UIP in India.
Section 3 supports the data points and provides extra information related to the subject. Sources are mentioned in the end for readers’ reference.



Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
1
1.1. Immunization Policy: History behind the programme
Immunization – Definition
Immunization programme is one of the essential interventions for protection of children from life-threatening diseases that are preventable. The immunization programme in India was flagged off in 1978 as Expanded Programme on Immunization (EPI). It gained impetus in 1985 as the Universal Immunization Programme (UIP) and was carried out in a phased manner to cover all districts in the country by 1989-90 (MoHFW 2006-07: 58).
In India, under the Universal Immunization Programme, vaccines for six vaccine-preventable diseases (tuberculosis, diphtheria, pertussis or whooping cough, tetanus, poliomyelitis, and measles) are available free of cost for all.
Universal Immunization Programme (UIP)
The Universal Immunization Programme (UIP), a planned strategy launched in 1985-86, aimed at systematic district-wise expansion to cover all the districts by 1989-90 (Govt. of India (GoI), MoHFW 1985; Sokhey 1985). More than 90 million pregnant women and 83 million infants were to be immunized over a five-year period under the UIP (Sokhey 1988). The programme was given the status of a National Technology Mission in 1986 (GoI 1988) to provide a sense of urgency and commitment to achieve the goals within the specified period.
UIP became a part of the Child Survival and Safe Motherhood (CSSM) Programme in 1992-93 (MoHFW 2002-03: 176). Since 1997, immunization activities have been an essential part of the National Reproductive and Child Health (RCH) Programme (MoHFW 2005-06: 54). The GoI constituted a National Technical Committee on Child Health on 11th June 2000 and launched immunization Strengthening Project on the recommendation of the Committee (MoHFW 2002-03: 173). The Department of Family Welfare established a National Technical Advisory Group on Immunization on 28th August 2001 to assist the GoI in developing a nationwide policy framework for vaccines and immunization (MoHFW 2002-03: 174).
As part of the National Health Policy, the UIP is being implemented on priority basis. The standard immunization schedule developed for the child immunization programme specifies the age at which each vaccine is to be administered and the number of doses to be given. Universal childhood immunization has been accepted by world public health leaders and stakeholders as both an affordable and cost effective strategy for promoting primary healthcare and for child survival.
Table 1: Quick Facts: Immunization:
• Immunizationhassavedmorethan20millionlivesinthelasttwodecades.
• Morethan100millioninfantsareimmunizedeachyear,saving2-3millionlivesannually.
• Globalmortalityattributed tomeaslesdeclinedby78%fromanestimated733,000deaths in2000, to164,000 in 2008.
• ImmunizationcoverageagainstHepBandHiBhasbeenincreasingsince1990–morethan160countriesnow include HepB and HiB into infant immunization schedules
Source: UNICEF/WHO, November 2011
Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
2
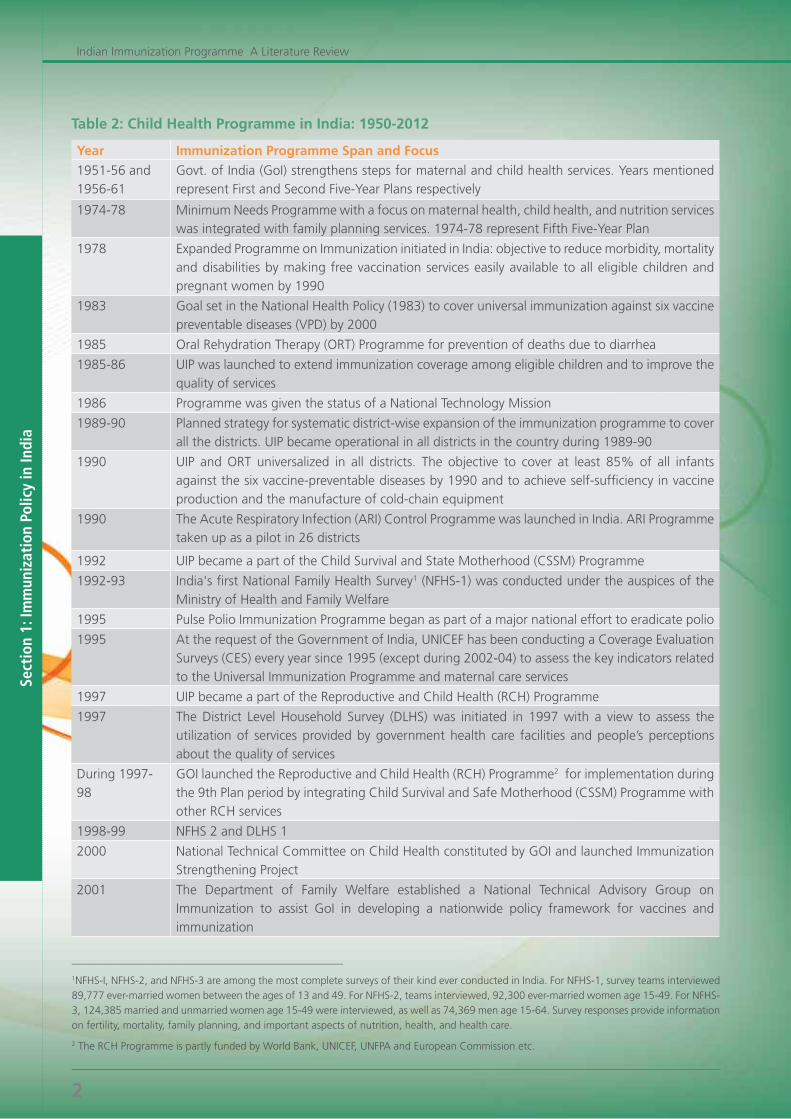
Table 2: Child Health Programme in India: 1950-2012
Year Immunization Programme Span and Focus
1951-56 and 1956-61
Govt. of India (GoI) strengthens steps for maternal and child health services. Years mentioned represent First and Second Five-Year Plans respectively
1974-78 Minimum Needs Programme with a focus on maternal health, child health, and nutrition services was integrated with family planning services. 1974-78 represent Fifth Five-Year Plan
1978 Expanded Programme on Immunization initiated in India: objective to reduce morbidity, mortality and disabilities by making free vaccination services easily available to all eligible children and pregnant women by 1990
1983 Goal set in the National Health Policy (1983) to cover universal immunization against six vaccine preventable diseases (VPD) by 2000
1985 Oral Rehydration Therapy (ORT) Programme for prevention of deaths due to diarrhea
1985-86 UIP was launched to extend immunization coverage among eligible children and to improve the quality of services
1986 Programme was given the status of a National Technology Mission
1989-90 Planned strategy for systematic district-wise expansion of the immunization programme to cover all the districts. UIP became operational in all districts in the country during 1989-90
1990 UIP and ORT universalized in all districts. The objective to cover at least 85% of all infantsagainst the six vaccine-preventable diseases by 1990 and to achieve self-sufficiency in vaccine production and the manufacture of cold-chain equipment
1990 The Acute Respiratory Infection (ARI) Control Programme was launched in India. ARI Programme taken up as a pilot in 26 districts
1992 UIP became a part of the Child Survival and State Motherhood (CSSM) Programme
1992-93 India's first National Family Health Survey1 (NFHS-1) was conducted under the auspices of the Ministry of Health and Family Welfare
1995 Pulse Polio Immunization Programme began as part of a major national effort to eradicate polio
1995 At the request of the Government of India, UNICEF has been conducting a Coverage Evaluation Surveys (CES) every year since 1995 (except during 2002-04) to assess the key indicators related to the Universal Immunization Programme and maternal care services
1997 UIP became a part of the Reproductive and Child Health (RCH) Programme
1997 The District Level Household Survey (DLHS) was initiated in 1997 with a view to assess the utilization of services provided by government health care facilities and people’s perceptions about the quality of services
During 1997-98
GOI launched the Reproductive and Child Health (RCH) Programme2 for implementation during the 9th Plan period by integrating Child Survival and Safe Motherhood (CSSM) Programme with other RCH services
1998-99 NFHS 2 and DLHS 1
2000 National Technical Committee on Child Health constituted by GOI and launched Immunization Strengthening Project
2001 The Department of Family Welfare established a National Technical Advisory Group on Immunization to assist GoI in developing a nationwide policy framework for vaccines and immunization
___________________________________________________
1NFHS-I, NFHS-2, and NFHS-3 are among the most complete surveys of their kind ever conducted in India. For NFHS-1, survey teams interviewed 89,777 ever-married women between the ages of 13 and 49. For NFHS-2, teams interviewed, 92,300 ever-married women age 15-49. For NFHS-3, 124,385 married and unmarried women age 15-49 were interviewed, as well as 74,369 men age 15-64. Survey responses provide information on fertility, mortality, family planning, and important aspects of nutrition, health, and health care.
2 The RCH Programme is partly funded by World Bank, UNICEF, UNFPA and European Commission etc.
Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
3
Year
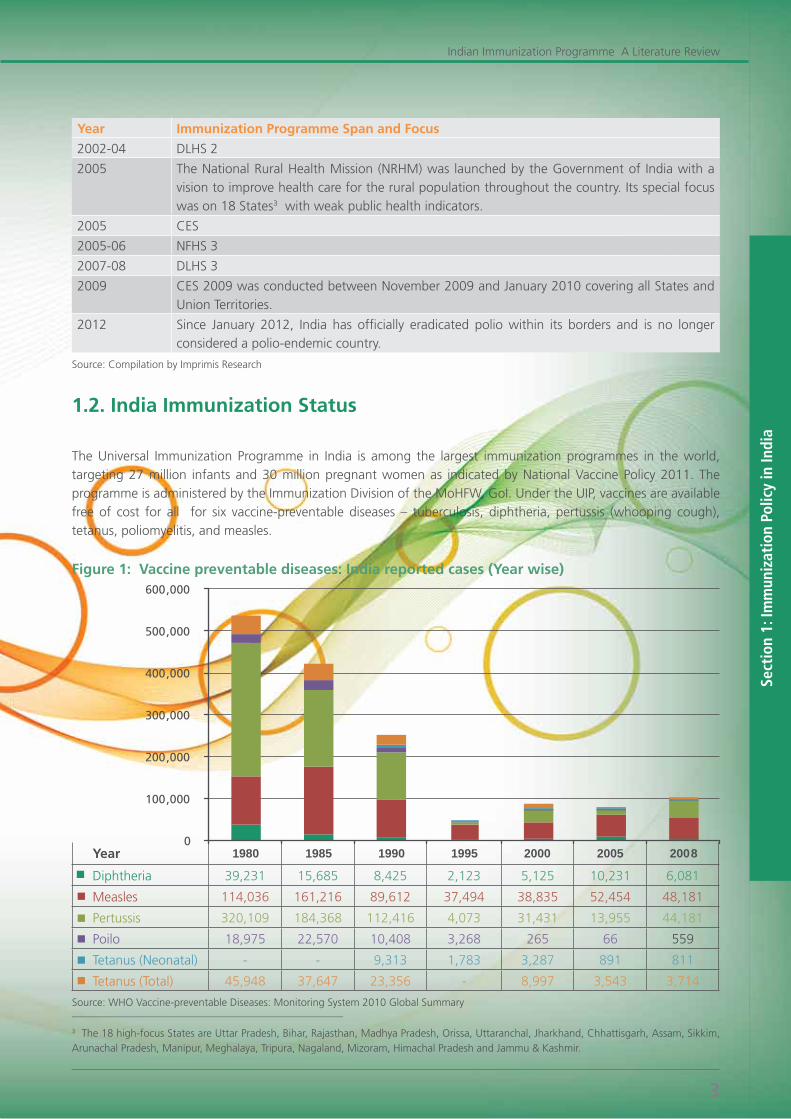
Diphtheria 39,231 15,685 8,425 2,123 5,125 10,231 6,081
Measles 114,036 161,216 89,612 37,494 38,835 52,454 48,181
Pertussis 320,109 184,368 112,416 4,073 31,431 13,955 44,181
Poilo 18,975 22,570 10,408 3,268 265 66 559
Tetanus (Neonatal) - - 9,313 1,783 3,287 891 811
Tetanus (Total) 45,948 37,647 23,356 - 8,997 3,543 3,714
Year Immunization Programme Span and Focus
2002-04 DLHS 2
2005 The National Rural Health Mission (NRHM) was launched by the Government of India with a vision to improve health care for the rural population throughout the country. Its special focus was on 18 States3 with weak public health indicators.
2005 CES
2005-06 NFHS 3
2007-08 DLHS 3
2009 CES 2009 was conducted between November 2009 and January 2010 covering all States and Union Territories.
2012 Since January 2012, India has officially eradicated polio within its borders and is no longer considered a polio-endemic country.
Source: Compilation by Imprimis Research
1.2. India Immunization Status
The Universal Immunization Programme in India is among the largest immunization programmes in the world, targeting 27 million infants and 30 million pregnant women as indicated by National Vaccine Policy 2011. The programme is administered by the Immunization Division of the MoHFW, GoI. Under the UIP, vaccines are available free of cost for all for six vaccine-preventable diseases – tuberculosis, diphtheria, pertussis (whooping cough), tetanus, poliomyelitis, and measles.
Figure 1: Vaccine preventable diseases: India reported cases (Year wise)
___________________________________________________
3 The 18 high-focus States are Uttar Pradesh, Bihar, Rajasthan, Madhya Pradesh, Orissa, Uttaranchal, Jharkhand, Chhattisgarh, Assam, Sikkim, Arunachal Pradesh, Manipur, Meghalaya, Tripura, Nagaland, Mizoram, Himachal Pradesh and Jammu & Kashmir.
Source: WHO Vaccine-preventable Diseases: Monitoring System 2010 Global Summary
0
100,000
200,000
300,000
400,000
500,000
600,000
1980 1985 1990 1995 2000 2005 2008
Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
4
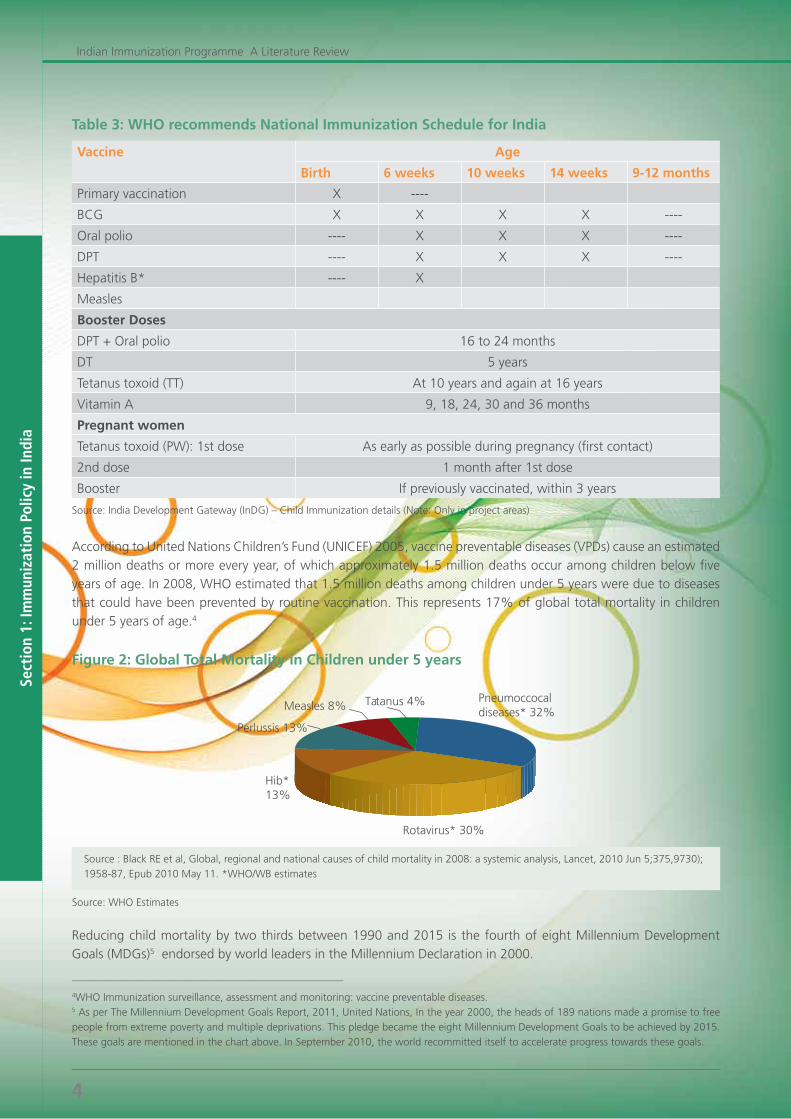
Table 3: WHO recommends National Immunization Schedule for India
Vaccine Age
Birth 6 weeks 10 weeks 14 weeks 9-12 months
Primary vaccination X ----
BCG X X X X ----
Oral polio ---- X X X ----
DPT ---- X X X ----
Hepatitis B* ---- X
Measles
Booster Doses
DPT + Oral polio 16 to 24 months
DT 5 years
Tetanus toxoid (TT) At 10 years and again at 16 years
Vitamin A 9, 18, 24, 30 and 36 months
Pregnant women
Tetanus toxoid (PW): 1st dose As early as possible during pregnancy (first contact)
2nd dose 1 month after 1st dose
Booster If previously vaccinated, within 3 years
Source: India Development Gateway (InDG) – Child Immunization details (Note: Only in project areas)
According to United Nations Children’s Fund (UNICEF) 2005, vaccine preventable diseases (VPDs) cause an estimated 2 million deaths or more every year, of which approximately 1.5 million deaths occur among children below five years of age. In 2008, WHO estimated that 1.5 million deaths among children under 5 years were due to diseases thatcouldhavebeenpreventedbyroutinevaccination.Thisrepresents17%ofglobaltotalmortalityinchildrenunder 5 years of age.4
Figure 2: Global Total Mortality in Children under 5 years
___________________________________________________
4WHO Immunization surveillance, assessment and monitoring: vaccine preventable diseases.5 As per The Millennium Development Goals Report, 2011, United Nations, In the year 2000, the heads of 189 nations made a promise to free people from extreme poverty and multiple deprivations. This pledge became the eight Millennium Development Goals to be achieved by 2015. These goals are mentioned in the chart above. In September 2010, the world recommitted itself to accelerate progress towards these goals.
Pneumoccocal diseases*32%
Rotavirus*30%
Hib* 13%
Perlussis13%
Measles8% Tatanus4%
Source: WHO Estimates
Source : Black RE et al, Global, regional and national causes of child mortality in 2008: a systemic analysis, Lancet, 2010 Jun 5;375,9730); 1958-87, Epub 2010 May 11. *WHO/WB estimates
Reducing child mortality by two thirds between 1990 and 2015 is the fourth of eight Millennium Development Goals (MDGs)5 endorsed by world leaders in the Millennium Declaration in 2000.
Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
5
The report, ‘State of the World’s Vaccines and Immunizations’ by UNICEF states that, “Immunization is one of the most powerful and cost-effective of all health interventions. It prevents debilitating illness and disability, and saves millions of lives every year. It is also key to achieving the MDGs – commitments made by world leaders in 2000 to reduce poverty and improve human development. The contribution of immunization is especially critical to achieving the goal to reduce deaths among children under five years old (MDG 4).”
India is one of the signatories committed to achieve MDGs. The realization of the MDGs goals in India is vital for attaining human development and economic growth within the country. They are critical for reaching the MDGs worldwide; given India’s enormous size, every fifth person in the world is an Indian.
To develop and implement effective strategies for improving immunization coverage, it is crucial that appropriate and accurate information about immunization coverage levels among all children and selected group, status and quality of immunization services, and bottlenecks to improving coverage levels are available.
To ensure data availability, UNICEF organized a coverage evaluation survey in 2009 (CES 2009) to assess the utilization of maternal, newborn and child health services including immunization. The Coverage Evaluation Survey 2009 -- a nationwide survey covering all the States and Union Territories of India and was conducted at the request of the Government of India.
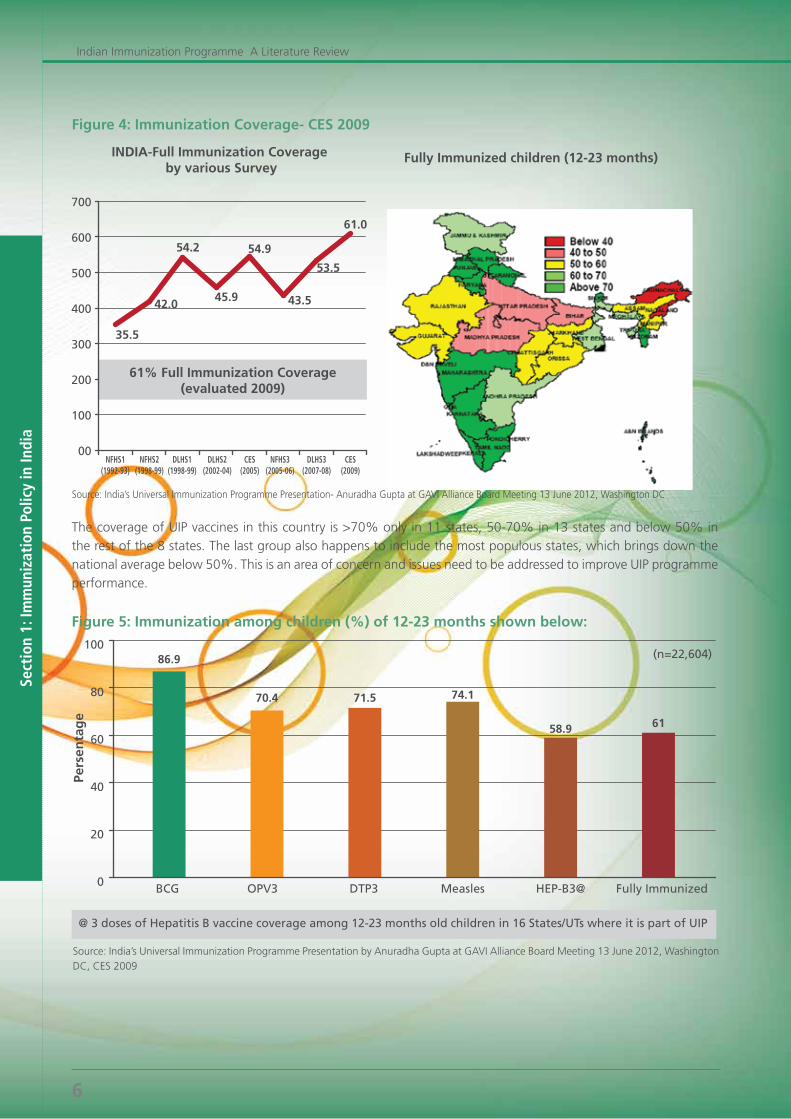
As per MoHFW presentation mentioning an overview of Universal Immunization programme in June 2012, India hasachieved61%FullImmunizationCoverageasevaluatedinCES2009.Attheall-Indialevel,61%ofchildrenaged12-23monthsreceivedfullimmunization.Thecoverageofimmunizationwashigherinurbanareas(67.4%)comparedtothatinruralareas(58.5%).Aregionwisecoverageispresentedinthefigure4.
Eradicate Extreme Hunger and Poverty
Improve Maternal Health
Achieve Universal Primary Education
Combat HIV/AIDS, Malaria and other Diseases
Promote Gender Equality and Empower Women
Ensure Environmental Sustainability
Reduce Child Mortality Develop a Global Partnership for Development
Source: UNDP in India website page - Millennium Development Goals
For more details: Refer Appendix 1: India’s progress on the MDGs for 2015 (at the end).
Figure 3: Millennium Development Goals – The Eight Goals for 2015
Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
6
ThecoverageofUIPvaccinesinthiscountryis>70%onlyin11states,50-70%in13statesandbelow50%inthe rest of the 8 states. The last group also happens to include the most populous states, which brings down the nationalaveragebelow50%.ThisisanareaofconcernandissuesneedtobeaddressedtoimproveUIPprogrammeperformance.
Figure 5: Immunization among children (%) of 12-23 months shown below:
Pers
enta
ge
@ 3 doses of Hepatitis B vaccine coverage among 12-23 months old children in 16 States/UTs where it is part of UIP
(n=22,604)
0
20
40
60
80
100
BCG
86.9
OPV3
70.4
DTP3
71.5
Measles
74.1
HEP-B3@
58.9
Fully Immunized
61
Source: India’s Universal Immunization Programme Presentation by Anuradha Gupta at GAVI Alliance Board Meeting 13 June 2012, Washington DC, CES 2009
Figure 4: Immunization Coverage- CES 2009
INDIA-Full Immunization Coverage by various Survey
35.5
54.2
45.9
54.9
42.0
00
100
200
300
400
500
600
700
NFHS1(1992-93)
NFHS3(2005-06)
NFHS2(1998-99)
DLHS1(1998-99)
DLHS2(2002-04)
DLHS3(2007-08)
CES(2005)
CES(2009)
43.5
53.5
61.0
61% Full Immunization Coverage(evaluated 2009)
Fully Immunized children (12-23 months)
Source: India’s Universal Immunization Programme Presentation- Anuradha Gupta at GAVI Alliance Board Meeting 13 June 2012, Washington DC

Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
7
Mass immunization for protection from infectious diseases is one of the greatest achievements of modern medicine and its benefits have been eloquently set out. Political and leadership factors also play roles in the success of vaccination programmes.
To strengthen the vaccine outreach in India, the Ministry of Health and Family Welfare released a draft National Vaccine Policy in April 2011. Now almost one and half years later, the policy document is a crucial reference guide for the adoption of new vaccines and formulating vaccine strategies in India. The policy, now adopted by Government of India, seeks “to develop a long-term plan to strengthen the whole vaccine programme and intends to provide broader policy guidelines and framework to guide the creation of evidence base to justify the need for R&D, production, procurement, and quality assessment of vaccines for UIP in India.” The policy also touches the aspects related to vaccine security in the country and vaccination programmes in broader framework of National Health Policy of India. Policy further underlines the significance of active Public Sector Units (PSUs); linking geographical Information System with UIP network to track delivery of vaccines and encouraging PPPs through flexible governing and grants.
Refer: Appedix ( WHO and UNICEF presents the country level data on immunization status, Indian facts for 2010 and WHO fact sheet)
1.3. Role of Centre and State Governments in Healthcare Financing
Health is a concurrent subject under the Indian constitution, but state governments are predominantly responsible for most health provisions, both curative and public health aspects. In addition to direct central government spending on specific budget items, however, there is a range of centrally mandated expenditures that are also effectively spent by state governments, as well as some joint spending6. GOI allocations for individual states are based on a weightage system, where states with the poorest health indicators get a larger share of the allocations. Generally, 85%ofthefundscomefromtheCentreandtherestfromthestates.
July 2004 working paper “Analysis of public expenditure on health using State level data” explained Centre and state roles in public healthcare expenditures. The paper7 highlights “the total public healthcare expenditure is composed of state level allocations and allocations from central government”.
The central sponsored programmes have been one key policy initiative of the Government of India to support the health sector programmes directly. The Centre provides direct and partial (matching grant) support to the states in meeting both recurring and non-recurring expenditure of programmes under this policy initiative8 . The states’ share in the total revenue expenditure has been declining. This is also a reflection of the fact that state governments are going through serious fiscal problems. The role of central support in state budgetary allocations is increasing. Still in comparison to public expenditure, the private expenditure on healthcare is increasing.
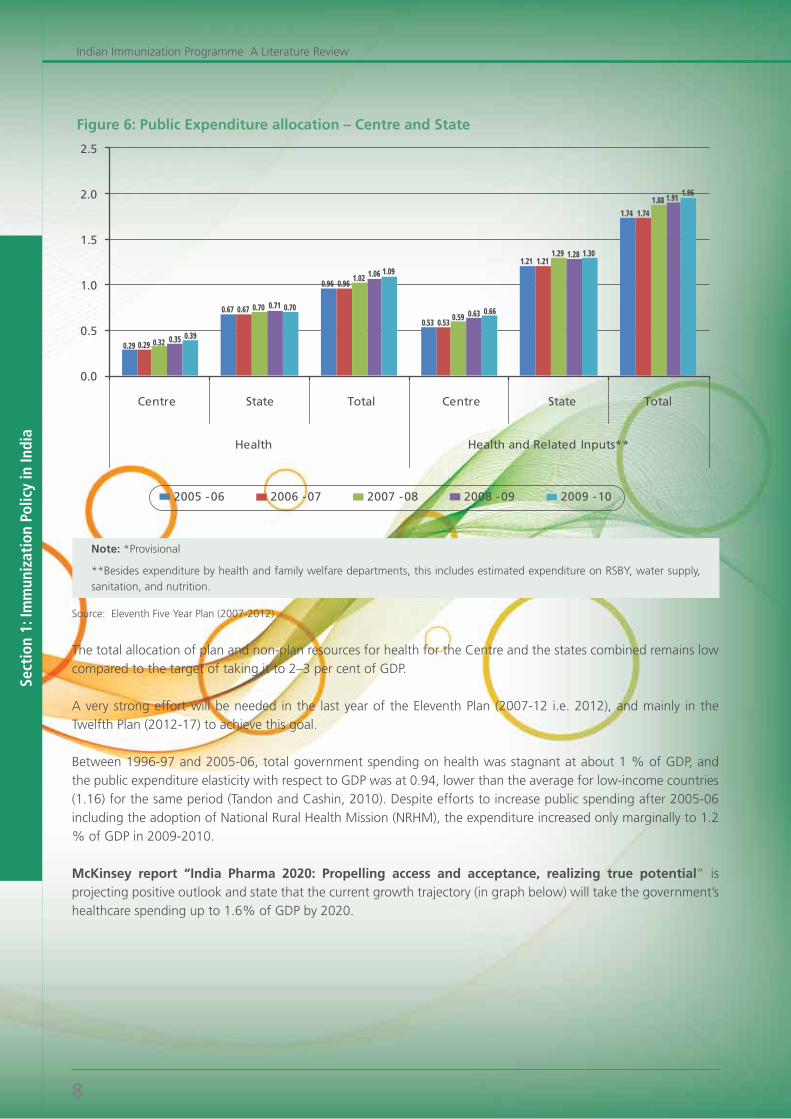
As per the 11th Five Year Plan (2007-12), “Looking at the contributions of the Centre and the states (Figure 6), the Centre’s health expenditure as percentage of GDP increased from 0.29 in 2005–06 to 0.39 in 2009–10. This is much faster than the states, where the increase was from 0.67 to 0.70 over the same period. This pattern also holds good for health-related expenditure. States, therefore, have to substantially increase their health budgets”.
___________________________________________________
6Government Health Expenditure in India: A Benchmark Study- Undertaken for the MacArthur Foundation, India, Economic Research Foundation, New Delhi- August 20067Bhat, R., “Analysis of Public Expenditure on Health Using State Level Data,” Working Paper No. WP 2004-06-08, Indian Institute of Management, Ahmedabad.8Bhat Ramesh & Jain Nishant, . “Analysis of Public Expenditure on Health Using State Level Data,” IIMA Working Papers WP2004-06-08
Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
8
Figure 6: Public Expenditure allocation – Centre and State
Note: *Provisional
**Besides expenditure by health and family welfare departments, this includes estimated expenditure on RSBY, water supply, sanitation, and nutrition.
Source: Eleventh Five Year Plan (2007-2012)
The total allocation of plan and non-plan resources for health for the Centre and the states combined remains low compared to the target of taking it to 2–3 per cent of GDP.
A very strong effort will be needed in the last year of the Eleventh Plan (2007-12 i.e. 2012), and mainly in the Twelfth Plan (2012-17) to achieve this goal.
Between1996-97and2005-06,totalgovernmentspendingonhealthwasstagnantatabout1%ofGDP,andthe public expenditure elasticity with respect to GDP was at 0.94, lower than the average for low-income countries (1.16) for the same period (Tandon and Cashin, 2010). Despite efforts to increase public spending after 2005-06 including the adoption of National Rural Health Mission (NRHM), the expenditure increased only marginally to 1.2 %ofGDPin2009-2010.
McKinsey report “India Pharma 2020: Propelling access and acceptance, realizing true potential” is projecting positive outlook and state that the current growth trajectory (in graph below) will take the government’s healthcarespendingupto1.6%ofGDPby2020.

Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
9
Figure 7: Healthcare spending by Government in India
Source: McKinsey report “India Pharma 2020: Propelling access and acceptance, realizing true potential“
As per a study done by Ernst and Young in September 2012, “Government spending on healthcare in India should beraisedtoatleast4%ofthenation’sgrossdomesticproduct(GDP)fromthecurrent1%tomeetbasichealthcarerequirements under proposed Universal Health Coverage (UHC) programme.”
1.4. Decisive Factors Affecting Immunization
Nilanjan Patra in his study paper “Universal Immunization Programme in India: The determinants of childhood immunization” analyses the effects of some select demographic and socioeconomic predictor variables on likelihood of immunization of a child for six vaccine-preventable diseases covered under UIP. His immunization coverage model is used in this study to describe the effects of the select background variables on immunization coverage.
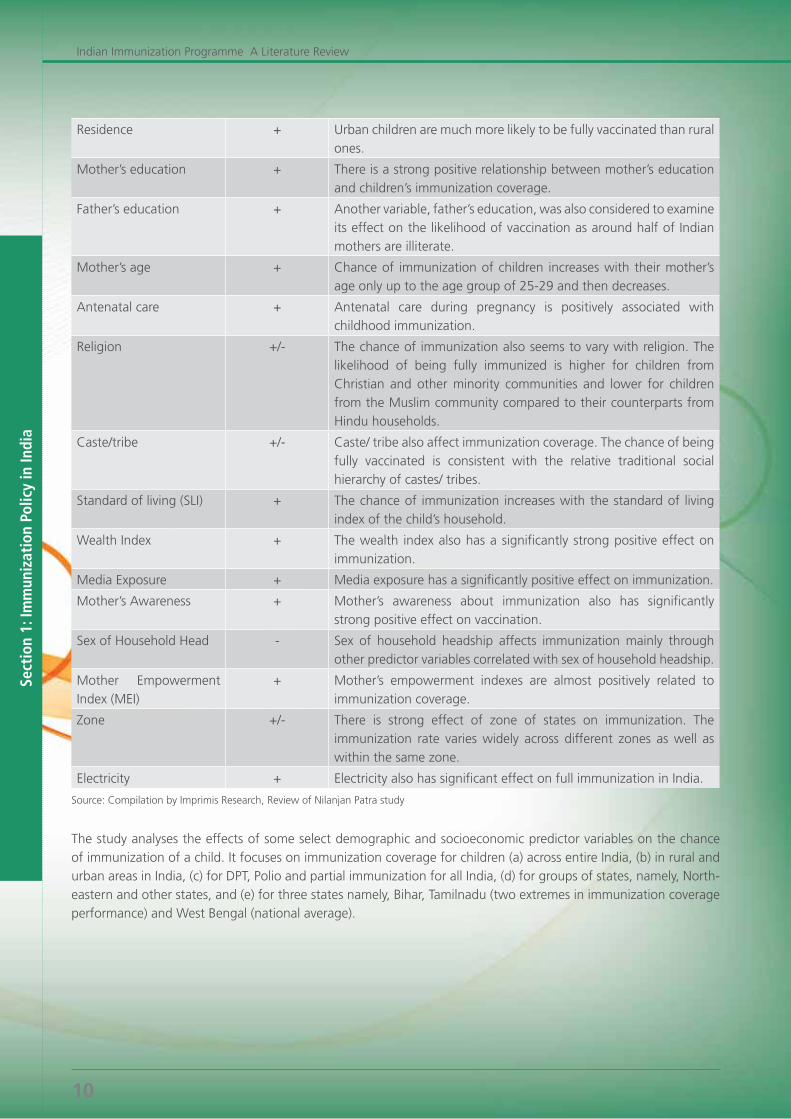
Table 4: Regression model analysis stating factors and their relationship with Immunization
Factor Relation with Immunization
Description
Education + Education is an important determinant of immunization coverage. It also affects mortality and fertility inversely.
Sex of child + Gender bias is an important obstacle against improving immunization coverage.
Birth order + There is a consistently inverse relationship between immunization coverage and birth order of a child. Majority of first-order births occur to younger women who are more likely than older women to utilize maternal and child healthcare services.
Sect
ion
1: Im
mun
izat
ion
Polic
y in
Indi
a
Indian Immunization Programme A Literature Review
10
Residence + Urban children are much more likely to be fully vaccinated than rural ones.
Mother’s education + There is a strong positive relationship between mother’s education and children’s immunization coverage.
Father’s education + Another variable, father’s education, was also considered to examine its effect on the likelihood of vaccination as around half of Indian mothers are illiterate.
Mother’s age + Chance of immunization of children increases with their mother’s age only up to the age group of 25-29 and then decreases.
Antenatal care + Antenatal care during pregnancy is positively associated with childhood immunization.
Religion +/- The chance of immunization also seems to vary with religion. The likelihood of being fully immunized is higher for children from Christian and other minority communities and lower for children from the Muslim community compared to their counterparts from Hindu households.
Caste/tribe +/- Caste/ tribe also affect immunization coverage. The chance of being fully vaccinated is consistent with the relative traditional social hierarchy of castes/ tribes.
Standard of living (SLI) + The chance of immunization increases with the standard of living index of the child’s household.
Wealth Index + The wealth index also has a significantly strong positive effect on immunization.
Media Exposure + Media exposure has a significantly positive effect on immunization.
Mother’s Awareness + Mother’s awareness about immunization also has significantly strong positive effect on vaccination.
Sex of Household Head - Sex of household headship affects immunization mainly through other predictor variables correlated with sex of household headship.
Mother Empowerment Index (MEI)
+ Mother’s empowerment indexes are almost positively related to immunization coverage.
Zone +/- There is strong effect of zone of states on immunization. The immunization rate varies widely across different zones as well as within the same zone.
Electricity + Electricity also has significant effect on full immunization in India.
Source: Compilation by Imprimis Research, Review of Nilanjan Patra study
The study analyses the effects of some select demographic and socioeconomic predictor variables on the chance of immunization of a child. It focuses on immunization coverage for children (a) across entire India, (b) in rural and urban areas in India, (c) for DPT, Polio and partial immunization for all India, (d) for groups of states, namely, North-eastern and other states, and (e) for three states namely, Bihar, Tamilnadu (two extremes in immunization coverage performance) and West Bengal (national average).


Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
13
2.1. Vaccine Market and Policy Framework
2.1A) Vaccine Market – India and Global
Vaccines are a crucial discovery of the times, essential preventive medicines for primary “healthcare” and critical component of a nation’s health security. The political will and governmental support for improving public health must be in place to make vaccination work. Oftentimes, the participation of international bodies, non-governmental organizations and other country specific agencies are critical to success. The infrastructure to support disease surveillance and vaccine delivery is essential.
Table 5: Global and International Organizations
Organization Purpose
World Bank, World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF)
These international bodies focus broadly on vaccine procurement, delivery, and monitoring. The mission of the WHO Initiative for Vaccine Research (IVR) is to guide, provide vision, enable, support, and facilitate the development, clinical evaluation and world-wide access to safe, effective and affordable vaccines against infectious diseases of public health importance, especially in developing countries.
Gates Foundation and Rotary International
Non-governmental organizations provide important knowledge and credibility in addition to crucial financial support.
Global Alliance for Vaccines and Immunization (GAVI) Alliance (launched in 2000)
Role is to ensure that new and underused vaccines are available to low-income countries at an affordable price and within a shorter time period; and then those countries are prepared and equipped to deliver them.
GAVI Partners The GAVI partners have created the Global Fund for Children’s Vaccines (GFCV) to fund poorer countries (annual per capita income less than US$1000) for new vaccines and infrastructure development.
Asian Vaccination Initiative The Asian Vaccination Initiative (AVI) of the Asian Development Bank (ADB) can offer loans for immunization programmes to countries in the region.
Global Immunization Vision and Strategy (GIVS) (launched in 2006)
GIVS is the first ever ten-year (2006-2015) framework aimed at controlling morbidity and mortality from vaccine-preventable diseases and helping countries to immunize more people, from infants to seniors, with a greater range of vaccines.
Source: Compilation by Imprimis Research
According to GBI Research Report, the overall global vaccines market was valued at US$ 28 billion in 2010 and isexpectedtoreachUS$56.7billionby2017withaCAGRof11.5%.TheimportantinternationalplayersinthevaccinesmarketareGlaxoSmithKline,Sanofi,Pfizer,NovartisAG,MerckandSP-MSD,representingaround88%ofthe total vaccine segment globally. In India companies such as Serum Institute, Shantha Biotechnics, Bharat Biotech and Panacea Biotech are poised to take greater strides in this direction.
Table 6: Authorities at work on Vaccination and Immunization in India
Organization Purpose
DCGI The vaccines licensing authority in India, i.e. the National Regulatory Authority (NRA), is the Drugs Controller General of India (DCGI), which is approved by World Health Organization (WHO).
CDSCO The Central Drugs and Standards Control Organization (CDSCO) is the National Regulatory Authority (NRA) in India. CDSCO is headed by the Drugs Controller General (India) [DCG(I)]
CLAA Licensing of products in India is by the Central Licensing Approval Authority (CLAA).

Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
14
Organization Purpose
NTAGI NTAGI advises the national government regarding the technical issues related to vaccination and immunization.
DATB The Drug Technology Advisory Board (DATB) approves introduction of vaccines into the immunization services, while all vaccine approvals and clinical trials are by the CLAA.
ICMR Good Clinical Practice (GCP) and ethical guidelines by Indian Council of Medical Research (ICMR) for approval exist.
Source: Compilation by Imprimis Research
McKinsey report titled, “India Pharma 2020: Propelling access and acceptance, realizing true potential” statedthatat2%penetration, thevaccinesmarketof India is significantlyunder-penetratedwithanestimatedturnover of around US$ 250 million, where the private segment accounts for two-thirds of the total. McKinsey expects the market to grow to US$ 1.7 billion by 2020.
AsperNationalVaccinePolicy2011,“Indiaisamajorproducerandexporterofvaccines:approximately43%ofglobal vaccine supply is provided by Indian manufacturers, primarily from the private sector. Till recently, both public and private sector vaccine producers were supplying vaccines to UIP. The Indian domestic market for UIP alone is 100 million doses; and therefore has considerable bearing on global vaccine pricing.”
As rightly stated in the WHO report on Vaccine Introduction Guidelines, the decision to add a new vaccine to an immunization programme is often influenced by social values, perceptions, and political concerns and is not just a technical one. It is the responsibility of the National Regulatory Authority (NRA) to ensure that only safe products are licensed.
For licensing of a new vaccine, the vaccine manufacturer should conduct the phase I, II, and III trials and must submit their results to NRA for its approval. There are both central and state licensing authorities. The state licensing authority inspects and grants licensing for retail.
2.1B) Introduction of New Vaccine – Decision-making process
The decision to add a new vaccine is complex. A rational decision on a vaccine requires information on: disease burden; vaccine safety and effectiveness; vaccine cost; and net impact (on immunization programme as well as health sector).
Table 7: A framework for decision-making on new vaccines: set of questions
1. Is the disease a public health problem?
2. Is immunization the best control strategy for this disease?
3. Is the immunization programme working well enough to add a vaccine?
4. What will be the net impact of the vaccine?
5. Is the vaccine a good investment?
6. How will the vaccine be funded?
7. How will the addition of the new vaccine be implemented?
Source: Assessing new vaccines for national immunization programmes, WHO 2005
Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
15
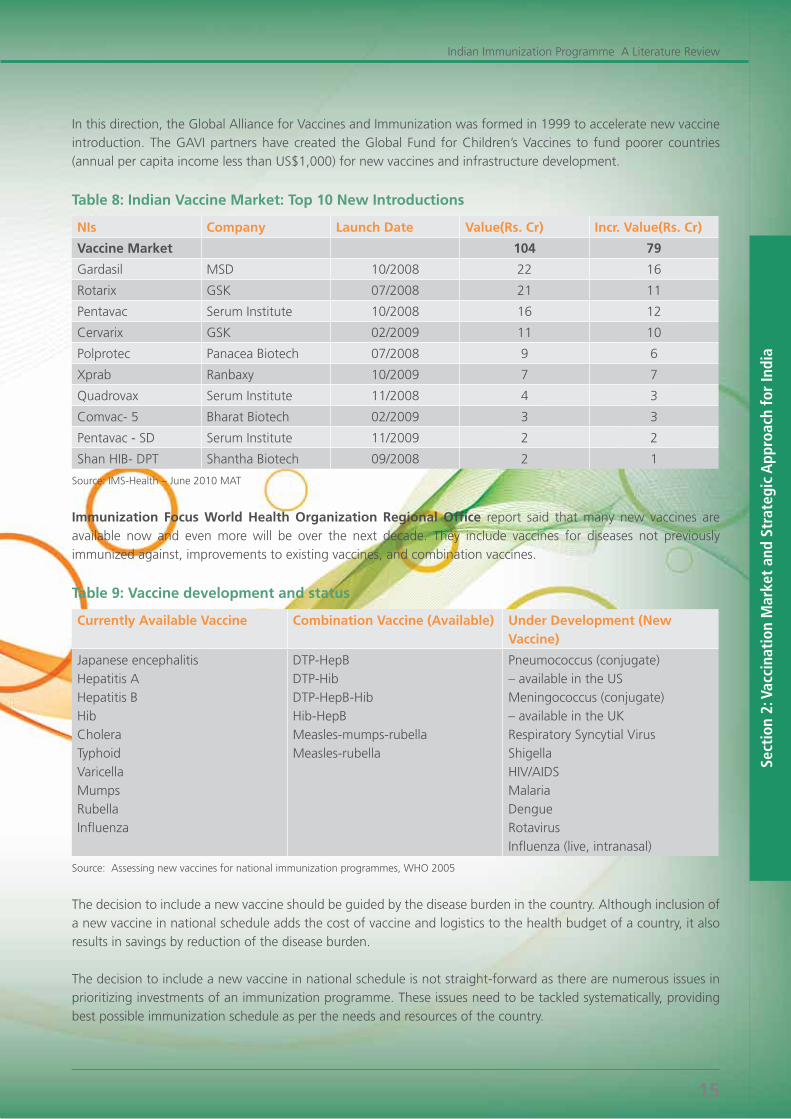
In this direction, the Global Alliance for Vaccines and Immunization was formed in 1999 to accelerate new vaccine introduction. The GAVI partners have created the Global Fund for Children’s Vaccines to fund poorer countries (annual per capita income less than US$1,000) for new vaccines and infrastructure development.
Table 8: Indian Vaccine Market: Top 10 New Introductions
NIs Company Launch Date Value(Rs. Cr) Incr. Value(Rs. Cr)
Vaccine Market 104 79
Gardasil MSD 10/2008 22 16
Rotarix GSK 07/2008 21 11
Pentavac Serum Institute 10/2008 16 12
Cervarix GSK 02/2009 11 10
Polprotec Panacea Biotech 07/2008 9 6
Xprab Ranbaxy 10/2009 7 7
Quadrovax Serum Institute 11/2008 4 3
Comvac- 5 Bharat Biotech 02/2009 3 3
Pentavac - SD Serum Institute 11/2009 2 2
Shan HIB- DPT Shantha Biotech 09/2008 2 1
Source: IMS-Health – June 2010 MAT
Immunization Focus World Health Organization Regional Office report said that many new vaccines are available now and even more will be over the next decade. They include vaccines for diseases not previously immunized against, improvements to existing vaccines, and combination vaccines.
Table 9: Vaccine development and status
Currently Available Vaccine Combination Vaccine (Available) Under Development (New Vaccine)
Japanese encephalitisHepatitis AHepatitis BHibCholeraTyphoidVaricellaMumpsRubellaInfluenza
DTP-HepBDTP-HibDTP-HepB-HibHib-HepBMeasles-mumps-rubellaMeasles-rubella
Pneumococcus (conjugate)– available in the USMeningococcus (conjugate)– available in the UKRespiratory Syncytial VirusShigellaHIV/AIDSMalariaDengueRotavirusInfluenza (live, intranasal)
Source: Assessing new vaccines for national immunization programmes, WHO 2005
The decision to include a new vaccine should be guided by the disease burden in the country. Although inclusion of a new vaccine in national schedule adds the cost of vaccine and logistics to the health budget of a country, it also results in savings by reduction of the disease burden.
The decision to include a new vaccine in national schedule is not straight-forward as there are numerous issues in prioritizing investments of an immunization programme. These issues need to be tackled systematically, providing best possible immunization schedule as per the needs and resources of the country.

Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
16
Table 10: Criterion for selection while introducing a new vaccine in UIP
The below given criteria considered for an informed decision making about the introduction of new vaccine in UIP:
• Diseaseburden(incidence/prevalence,absolutenumberofmorbidity/mortality,epidemic/pandemicpotential);
• Safetyandefficacyofthevaccineunderconsideration;
• Affordabilityandfinancialsustainabilityofthevaccinationprogram,eveniftheinitialintroductionissupportedby the external funding agency;
• Programmecapacitytointroduceanewantigen,includingcoldchaincapacity;
• Availabilityofadomesticorexternalvaccineproductioncapacity;
• Thecosteffectivenessofthevaccinationprogrammeandalsoofthealternativesotherthanvaccination.
Source: National Vaccine Policy April 2011 by Ministry of Health & Family Welfare
The potential inclusion of any new vaccine in UIP should initially be discussed by NTAGI. The NTAGI may consider various factors before giving technical recommendation for introducing any new vaccine in the programme. The technical decision of NTAGI should be considered by immunization division for implementation.
Advocacy and communication efforts are as important for community acceptance of the new vaccine as also for maintaining their confidence in the existing vaccines.
According to WHO report on “Vaccine Introduction Guidelines – Adding a vaccine to a national immunization programme: decision and implementation” 2005 paper, outlines the key issues to be considered before deciding to introduce a vaccine. This report aims to help country-level decision-makers decide whether to add a new vaccine to the national immunization programme and national immunization programme managers to implement the operational steps to add the vaccine.
While deciding to introduce a vaccine, examination of the key elements for programmatic planning and for monitoring the impact of the additional vaccine is required. The emphasis is on two parametric issues:
- Policy issues as first (where high level decision-makers to agree on whether the introduction of a particular vaccine is acceptable from an immunization policy perspective by doing assessment of public health priority and candidate vaccine)
- Second as Programmatic Issues (addressing the feasibility of the vaccine introduction from a technical perspective).
Although it is recommended that each issue is addressed in a fully informed decision-making process, some aspects of the flowchart may outweigh the other considerations, depending on the specific circumstances. The Flowchart outlines the key issues to be considered before deciding to introduce a vaccine.
Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
17
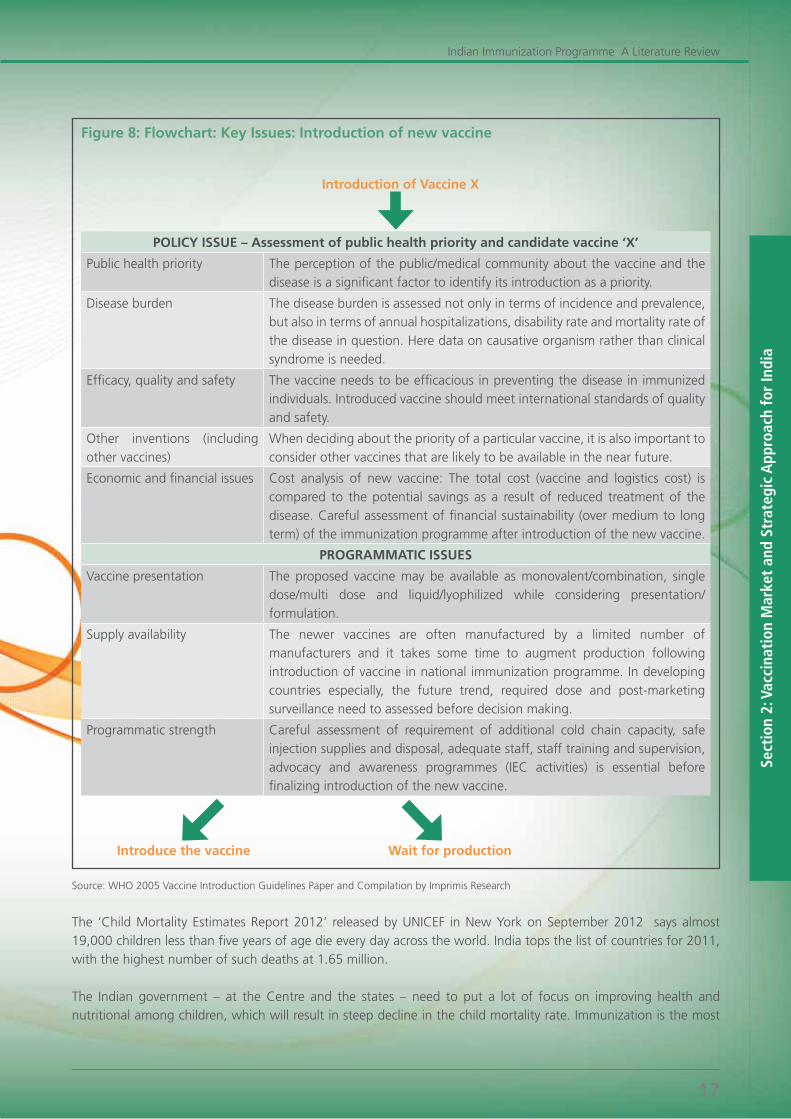
Figure 8: Flowchart: Key Issues: Introduction of new vaccine
Introduction of Vaccine X
POLICY ISSUE – Assessment of public health priority and candidate vaccine ‘X’
Public health priority The perception of the public/medical community about the vaccine and the disease is a significant factor to identify its introduction as a priority.
Disease burden The disease burden is assessed not only in terms of incidence and prevalence, but also in terms of annual hospitalizations, disability rate and mortality rate of the disease in question. Here data on causative organism rather than clinical syndrome is needed.
Efficacy, quality and safety The vaccine needs to be efficacious in preventing the disease in immunized individuals. Introduced vaccine should meet international standards of quality and safety.
Other inventions (including other vaccines)
When deciding about the priority of a particular vaccine, it is also important to consider other vaccines that are likely to be available in the near future.
Economic and financial issues Cost analysis of new vaccine: The total cost (vaccine and logistics cost) is compared to the potential savings as a result of reduced treatment of the disease. Careful assessment of financial sustainability (over medium to long term) of the immunization programme after introduction of the new vaccine.
PROGRAMMATIC ISSUES
Vaccine presentation The proposed vaccine may be available as monovalent/combination, single dose/multi dose and liquid/lyophilized while considering presentation/formulation.
Supply availability The newer vaccines are often manufactured by a limited number of manufacturers and it takes some time to augment production following introduction of vaccine in national immunization programme. In developing countries especially, the future trend, required dose and post-marketing surveillance need to assessed before decision making.
Programmatic strength Careful assessment of requirement of additional cold chain capacity, safe injection supplies and disposal, adequate staff, staff training and supervision, advocacy and awareness programmes (IEC activities) is essential before finalizing introduction of the new vaccine.
Introduce the vaccine Wait for production
Source: WHO 2005 Vaccine Introduction Guidelines Paper and Compilation by Imprimis Research
The ‘Child Mortality Estimates Report 2012’ released by UNICEF in New York on September 2012 says almost 19,000 children less than five years of age die every day across the world. India tops the list of countries for 2011, with the highest number of such deaths at 1.65 million.
The Indian government – at the Centre and the states – need to put a lot of focus on improving health and nutritional among children, which will result in steep decline in the child mortality rate. Immunization is the most

Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
18
cost-effective public health intervention in India. The effective immunization coverage largely depends on political will, funding, strategic initiative and execution of the planned policies..
2.2. Challenge and Strategic Action Points to Improve Immunization Coverage
India was one of the first countries to adopt the World Health Organization’s Expanded Programme of Immunization (EPI). The programme began globally in 1974 and was initiated in India in 1978. Since its inception, considerable progress has been made in terms of reduction in disease burden. Despite these achievements and tremendous advances in economic and technological spheres in recent years, the burden of vaccine-preventable diseases remains unacceptably high, in comparison to developed nations and also many developing countries9 . One of the obvious reasons for this could be that the level of coverage with individual vaccines does not meet the target of sustained high coverage required to control/eradicate the disease.
We have seen two main coverage issues vis-à-vis the Indian Immunization Programme : - There is a high level of disparity in vaccination coverage in different states. The traditionally poor preforming
states have greater inequities; however, there is significant inequity even among better performing states.
- There are considerable inequities in childhood vaccination by various individual (gender, birth order), family (area of residence, wealth, parental education), social (religion, caste), and societal (access to healthcare, community literacy level) characteristics.
Coverage of immunization is affected by demand and supply side factors highlighted well in CES 2009 report: Figure below
Figure 9 Reasons for partial or no Immunization (multiple responses)
05 10 15 20 25 30
Did not feel need
Not knowing about vaccines
Not knowing where to go for immunization
Time not convenint
Fear of side effects
Do not have time
Wrong advice by someone
Cannot afford the cost
Vaccine not available
Place not convenient
ANM absent
Long waiting time
Place too far
Service not available
Others
(n=9,375)
Sup
ply
sid
e Is
sues
Percentage
Dem
and
Sid
e Is
sues
Source: CES 2009
___________________________________________________
9World Health Organization; World Health Statistics 2011
Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
19
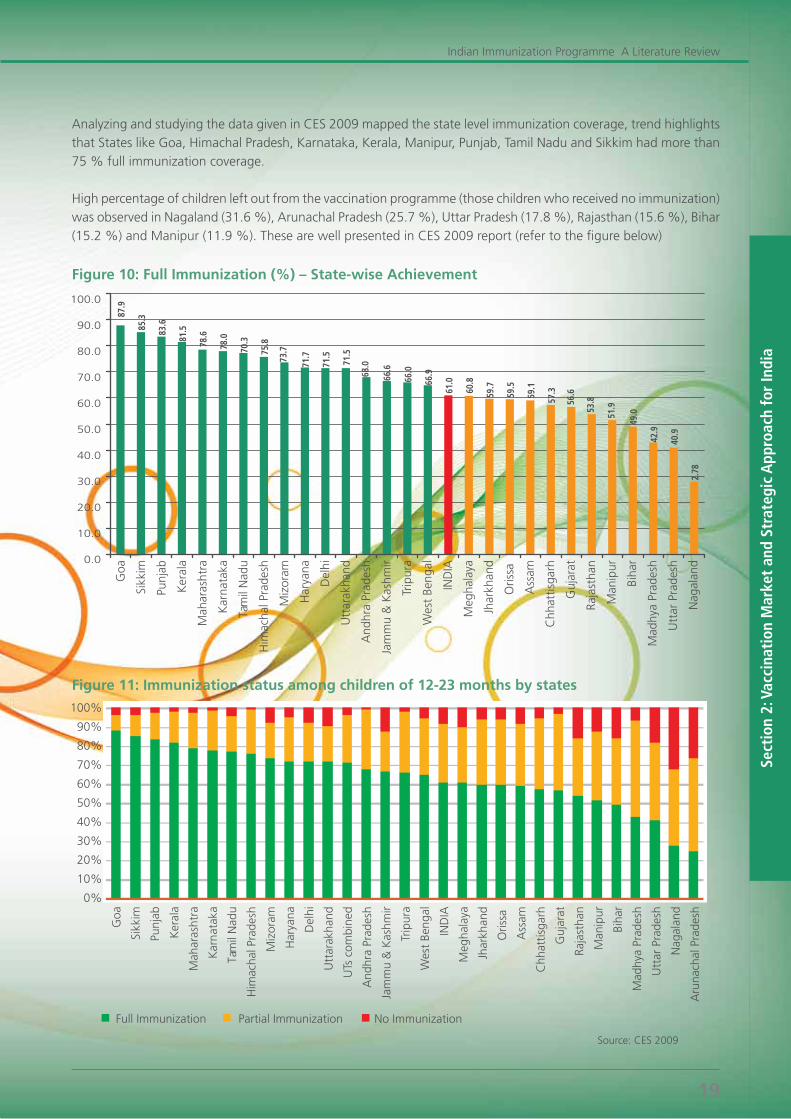
Analyzing and studying the data given in CES 2009 mapped the state level immunization coverage, trend highlights that States like Goa, Himachal Pradesh, Karnataka, Kerala, Manipur, Punjab, Tamil Nadu and Sikkim had more than 75%fullimmunizationcoverage.
High percentage of children left out from the vaccination programme (those children who received no immunization) wasobservedinNagaland(31.6%),ArunachalPradesh(25.7%),UttarPradesh(17.8%),Rajasthan(15.6%),Bihar(15.2%)andManipur(11.9%).ThesearewellpresentedinCES2009report(refertothefigurebelow)
Figure 10: Full Immunization (%) – State-wise Achievement
Figure 11: Immunization status among children of 12-23 months by states
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Goa
Sikk
im
Punj
ab
Ker
ala
Mah
aras
htra
Kar
nat
aka
Tam
il N
adu
Him
acha
l Pra
desh
Miz
oram
Har
yana
Del
hi
Utt
arak
hand
UTs
com
bine
d
And
hra
Prad
esh
Jam
mu
& K
ashm
ir
Trip
ura
Wes
t Be
ngal
IND
IA
Meg
hala
ya
Jhar
khan
d
Oris
sa
Ass
am
Chh
attis
garh
Guj
arat
Raja
stha
n
Man
ipur
Biha
r
Mad
hya
Prad
esh
Utt
ar P
rade
sh
Nag
alan
d
Aru
nach
al P
rade
sh
Full Immunization Partial Immunization No Immunization
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
87.9
85.3
83.6
81.5
78.6
78.0
70.3
75.8
73.7
71.7
71.5
71.5
68.0
66.6
66.0
66.9
61.0
60.8
59.7
59.5
59.1
57.3
56.6
53.8
51.9
49.0
42.9
40.9
2.78
Goa
Sikk
im
Punj
ab
Ker
ala
Mah
aras
htra
Kar
nata
ka
Tam
il N
adu
Him
acha
l Pra
desh
Miz
oram
Har
yana
Del
hi
Utt
arak
hand
And
hra
Prad
esh
Jam
mu
& K
ashm
ir
Trip
ura
Wes
t Be
ngal
IND
IA
Meg
hala
ya
Jhar
khan
d
Oris
sa
Ass
am
Chh
attis
garh
Guj
arat
Raja
stha
n
Man
ipur
Biha
r
Mad
hya
Prad
esh
Utt
ar P
rade
sh
Nag
alan
d
Source: CES 2009
Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
20
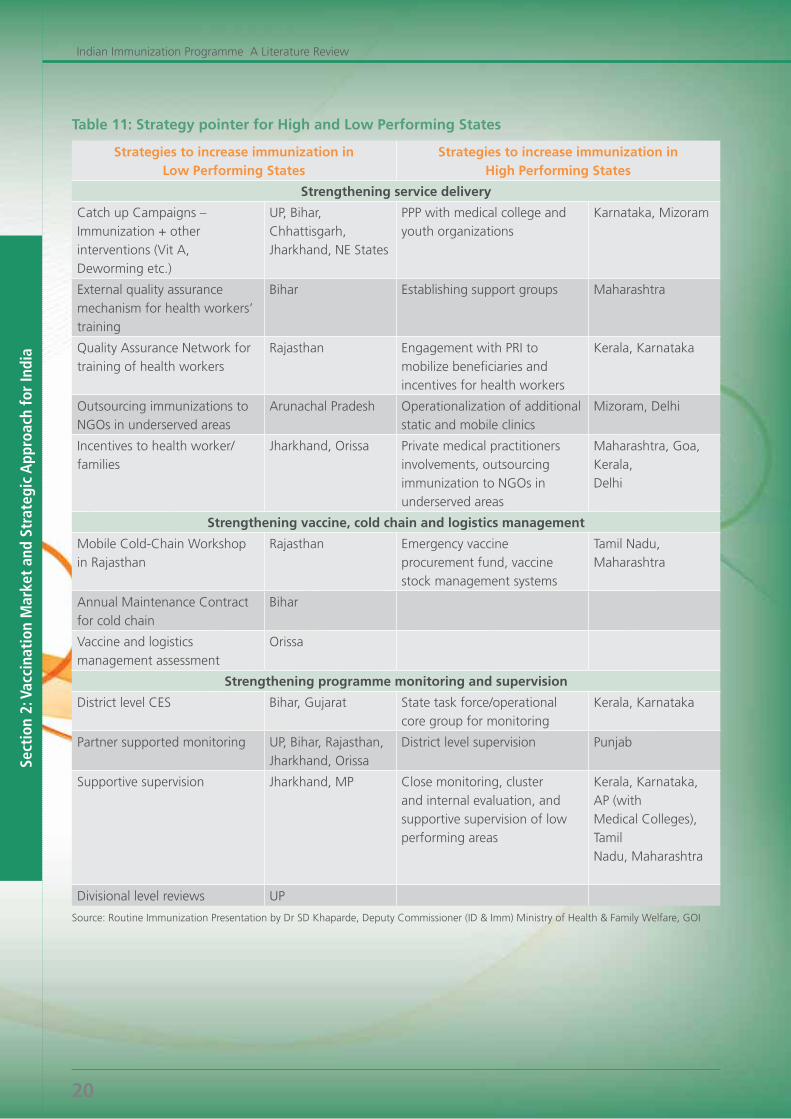
Table 11: Strategy pointer for High and Low Performing States
Strategies to increase immunization inLow Performing States
Strategies to increase immunization inHigh Performing States
Strengthening service delivery
Catch up Campaigns – Immunization + other interventions (Vit A, Deworming etc.)
UP, Bihar, Chhattisgarh, Jharkhand, NE States
PPP with medical college and youth organizations
Karnataka, Mizoram
External quality assurance mechanism for health workers’ training
Bihar Establishing support groups Maharashtra
Quality Assurance Network for training of health workers
Rajasthan Engagement with PRI to mobilize beneficiaries and incentives for health workers
Kerala, Karnataka
Outsourcing immunizations to NGOs in underserved areas
Arunachal Pradesh Operationalization of additional static and mobile clinics
Mizoram, Delhi
Incentives to health worker/ families
Jharkhand, Orissa Private medical practitioners involvements, outsourcing immunization to NGOs in underserved areas
Maharashtra, Goa, Kerala,Delhi
Strengthening vaccine, cold chain and logistics management
Mobile Cold-Chain Workshop in Rajasthan
Rajasthan Emergency vaccine procurement fund, vaccine stock management systems
Tamil Nadu, Maharashtra
Annual Maintenance Contract for cold chain
Bihar
Vaccine and logistics management assessment
Orissa
Strengthening programme monitoring and supervision
District level CES Bihar, Gujarat State task force/operational core group for monitoring
Kerala, Karnataka
Partner supported monitoring UP, Bihar, Rajasthan, Jharkhand, Orissa
District level supervision Punjab
Supportive supervision Jharkhand, MP Close monitoring, cluster and internal evaluation, and supportive supervision of low performing areas
Kerala, Karnataka, AP (withMedical Colleges), TamilNadu, Maharashtra
Divisional level reviews UP
Source: Routine Immunization Presentation by Dr SD Khaparde, Deputy Commissioner (ID & Imm) Ministry of Health & Family Welfare, GOI
Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
21
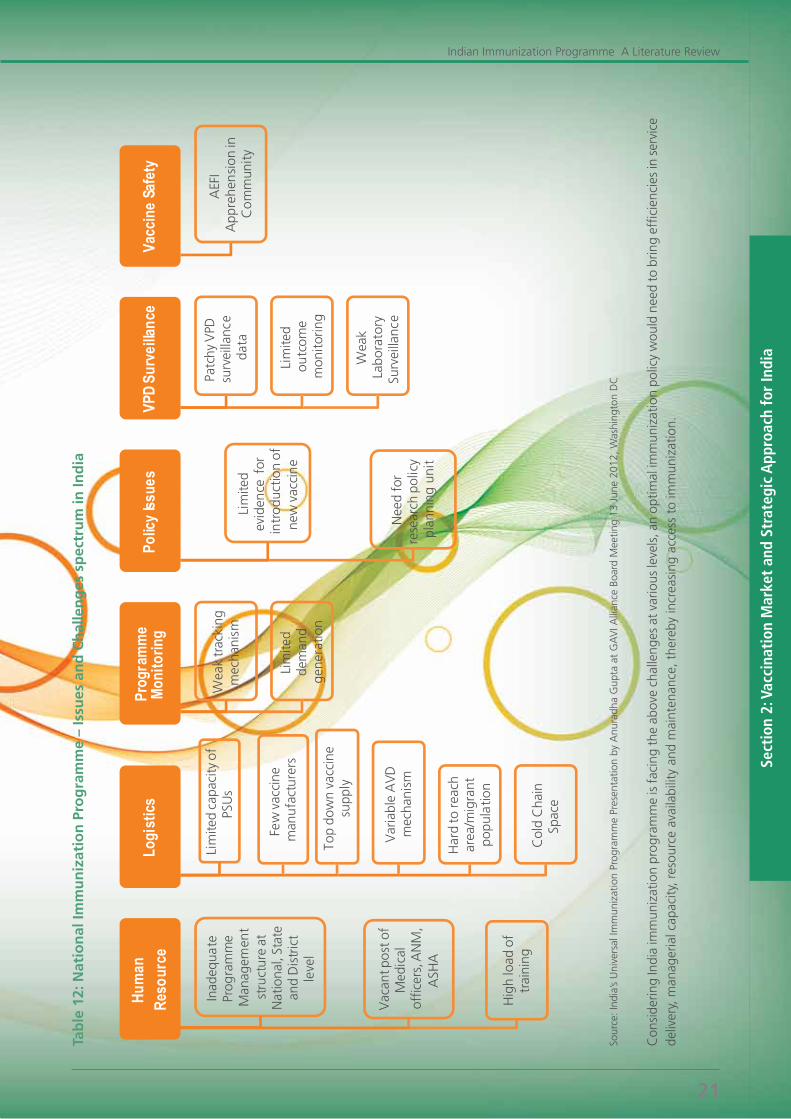
Tab
le 1
2: N
atio
nal
Imm
un
izat
ion
Pro
gra
mm
e –
Issu
es a
nd
Ch
alle
ng
es s
pec
tru
m in
Ind
ia
Sour
ce: I
ndia
’s U
nive
rsal
Imm
uniz
atio
n Pr
ogra
mm
e Pr
esen
tatio
n by
Anu
radh
a G
upta
at
GA
VI A
llian
ce B
oard
Mee
ting
13 J
une
2012
, Was
hing
ton
DC
Con
side
ring
Indi
a im
mun
izat
ion
prog
ram
me
is f
acin
g th
e ab
ove
chal
leng
es a
t va
rious
leve
ls, a
n op
timal
imm
uniz
atio
n po
licy
wou
ld n
eed
to b
ring
effic
ienc
ies
in s
ervi
ce
deliv
ery,
man
ager
ial c
apac
ity, r
esou
rce
avai
labi
lity
and
mai
nten
ance
, the
reby
incr
easi
ng a
cces
s to
imm
uniz
atio
n.
Hum
an
Reso
urce
Inad
equa
te
Prog
ram
me
Man
agem
ent
stru
ctur
e at
N
atio
nal,
Stat
e an
d D
istr
ict
leve
l
Vac
ant p
ost
of
Med
ical
of
ficer
s, A
NM
, A
SHA
Hig
h lo
ad o
f tr
aini
ng
Logi
stics
Lim
ited
capa
city
of
PSU
s
Few
vac
cine
m
anu
fact
urer
s
Top
dow
n va
ccin
e su
pply
Var
iabl
e A
VD
m
echa
nism
Har
d to
rea
ch
area
/mig
rant
po
pula
tion
Col
d C
hain
Sp
ace
Prog
ram
me
Moni
torin
g
Wea
k tr
acki
ng
mec
hani
sm
Lim
ited
dem
and
ge
nera
tion
Polic
y Iss
ues
Lim
ited
evid
ence
for
in
trod
uctio
n of
ne
w v
acci
ne
Nee
d fo
r re
sear
ch p
olic
y pl
anni
ng u
nit
VPD
Surv
eilla
nce
Patc
hy V
PD
surv
eilla
nce
data
Lim
ited
outc
ome
mon
itor
ing
Wea
k La
bora
tory
Su
rvei
llanc
e
Vacc
ine
Safe
ty
AEF
I A
ppre
hen
sion
in
Co
mm
unit
y
Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
22
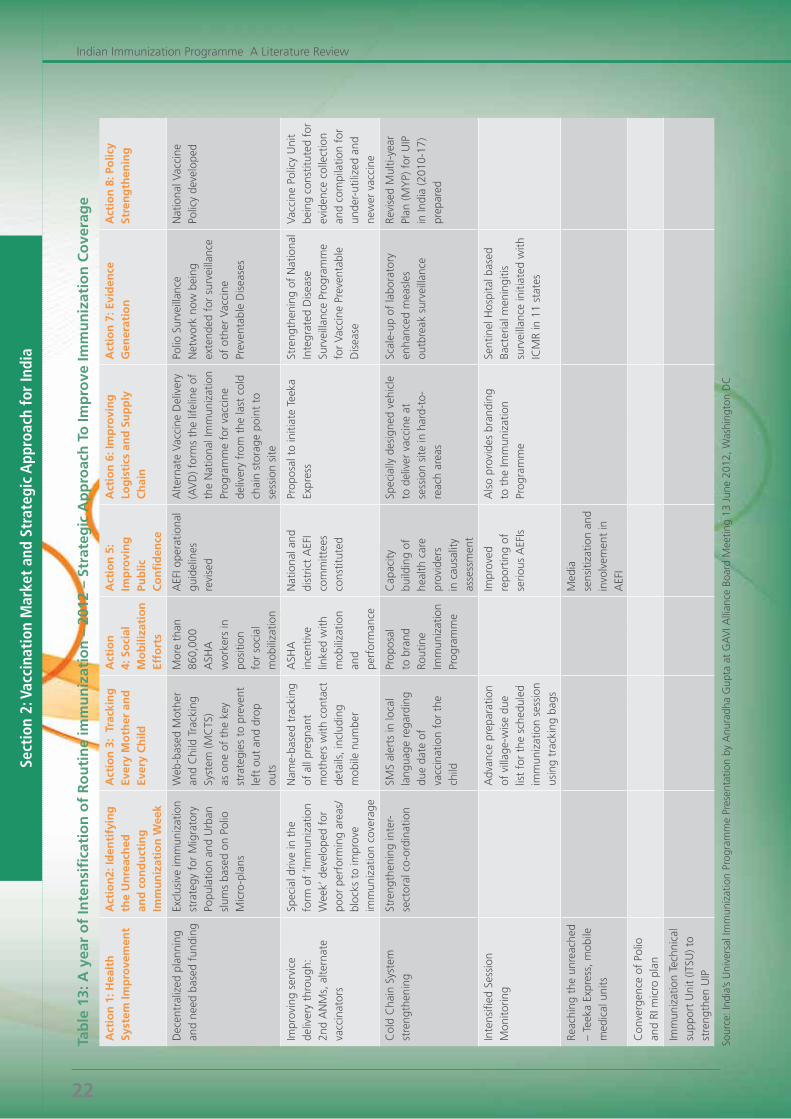
Tab
le 1
3: A
yea
r o
f In
ten
sifi
cati
on
of
Ro
uti
ne
imm
un
izat
ion
– 2
012
– St
rate
gic
Ap
pro
ach
To
Imp
rove
Imm
un
izat
ion
Co
vera
ge
Act
ion
1: H
ealt
h
Syst
em Im
pro
vem
ent
Act
ion
2: Id
enti
fyin
g
the
Un
reac
hed
an
d c
on
du
ctin
g
Imm
un
izat
ion
Wee
k
Act
ion
3:
Trac
kin
g
Ever
y M
oth
er a
nd
Ev
ery
Ch
ild
Act
ion
4:
So
cial
M
ob
iliza
tio
n
Effo
rts
Act
ion
5:
Imp
rovi
ng
Pu
blic
C
on
fid
ence
Act
ion
6: I
mp
rovi
ng
Lo
gis
tics
an
d S
up
ply
C
hai
n
Act
ion
7: E
vid
ence
G
ener
atio
nA
ctio
n 8
: Po
licy
Stre
ng
then
ing
Dec
entr
aliz
ed p
lann
ing
and
need
bas
ed f
undi
ngEx
clus
ive
imm
uniz
atio
n st
rate
gy f
or M
igra
tory
Po
pula
tion
and
Urb
an
slum
s ba
sed
on P
olio
M
icro
-pla
ns
Web
-bas
ed M
othe
r an
d C
hild
Tra
ckin
g Sy
stem
(MC
TS)
as o
ne o
f th
e ke
y st
rate
gies
to
prev
ent
left
out
and
dro
p ou
ts
Mor
e th
an
860,
000
ASH
A
wor
kers
in
posi
tion
for
soci
al
mob
iliza
tion
AEF
I ope
ratio
nal
guid
elin
es
revi
sed
Alte
rnat
e Va
ccin
e D
eliv
ery
(AV
D) f
orm
s th
e lif
elin
e of
th
e N
atio
nal I
mm
uniz
atio
n Pr
ogra
mm
e fo
r va
ccin
e de
liver
y fr
om t
he la
st c
old
chai
n st
orag
e po
int
to
sess
ion
site
Polio
Sur
veill
ance
N
etw
ork
now
bei
ng
exte
nded
for
sur
veill
ance
of
oth
er V
acci
ne
Prev
enta
ble
Dis
ease
s
Nat
iona
l Vac
cine
Po
licy
deve
lope
d
Impr
ovin
g se
rvic
e de
liver
y th
roug
h:
2nd
AN
Ms,
alte
rnat
e va
ccin
ator
s
Spec
ial d
rive
in t
he
form
of
‘Imm
uniz
atio
n W
eek’
dev
elop
ed f
or
poor
per
form
ing
area
s/bl
ocks
to
impr
ove
imm
uniz
atio
n co
vera
ge
Nam
e-ba
sed
trac
king
of
all
preg
nant
m
othe
rs w
ith c
onta
ct
deta
ils, i
nclu
ding
m
obile
num
ber
ASH
A
ince
ntiv
e lin
ked
with
m
obili
zatio
n an
d pe
rfor
man
ce
Nat
iona
l and
di
stric
t A
EFI
com
mitt
ees
cons
titut
ed
Prop
osal
to
initi
ate
Teek
a Ex
pres
sSt
reng
then
ing
of N
atio
nal
Inte
grat
ed D
isea
se
Surv
eilla
nce
Prog
ram
me
for
Vacc
ine
Prev
enta
ble
Dis
ease
Vacc
ine
Polic
y U
nit
bein
g co
nstit
uted
for
ev
iden
ce c
olle
ctio
n an
d co
mpi
latio
n fo
r un
der-
utili
zed
and
new
er v
acci
ne
Col
d C
hain
Sys
tem
st
reng
then
ing
Stre
ngth
enin
g in
ter-
sect
oral
co-
ordi
natio
nSM
S al
erts
in lo
cal
lang
uage
reg
ardi
ng
due
date
of
vacc
inat
ion
for
the
child
Prop
osal
to
bra
nd
Rout
ine
Imm
uniz
atio
n Pr
ogra
mm
e
Cap
acity
bu
ildin
g of
he
alth
car
e pr
ovid
ers
in c
ausa
lity
asse
ssm
ent
Spec
ially
des
igne
d ve
hicl
e to
del
iver
vac
cine
at
sess
ion
site
in h
ard-
to-
reac
h ar
eas
Scal
e-up
of
labo
rato
ry
enha
nced
mea
sles
ou
tbre
ak s
urve
illan
ce
Revi
sed
Mul
ti-ye
ar
Plan
(MY
P) f
or U
IP
in In
dia
(201
0-17
) pr
epar
ed
Inte
nsifi
ed S
essi
on
Mon
itorin
gA
dvan
ce p
repa
ratio
n of
vill
age-
wis
e du
e lis
t fo
r th
e sc
hedu
led
imm
uniz
atio
n se
ssio
n us
ing
trac
king
bag
s
Impr
oved
re
port
ing
of
serio
us A
EFIs
Als
o pr
ovid
es b
rand
ing
to t
he Im
mun
izat
ion
Prog
ram
me
Sent
inel
Hos
pita
l bas
ed
Bact
eria
l men
ingi
tis
surv
eilla
nce
initi
ated
with
IC
MR
in 1
1 st
ates
Reac
hing
the
unr
each
ed
– Te
eka
Expr
ess,
mob
ile
med
ical
uni
ts
Med
ia
sens
itiza
tion
and
invo
lvem
ent
in
AEF
I
Con
verg
ence
of
Polio
an
d RI
mic
ro p
lan
Imm
uniz
atio
n Te
chni
cal
supp
ort
Uni
t (IT
SU) t
o st
reng
then
UIP
Sour
ce: I
ndia
’s U
nive
rsal
Imm
uniz
atio
n Pr
ogra
mm
e Pr
esen
tatio
n by
Anu
radh
a G
upta
at
GA
VI A
llian
ce B
oard
Mee
ting
13 J
une
2012
, Was
hing
ton
DC

Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
23
India has declared 2012 as the year of intensification of routine immunization. The present full immunization coverageofchildrenis61%.Thekeyobjectiveofthiscampaignistoimprovefullimmunizationcoverageandreachall children, particularly in remote, inaccessible and backward areas as well as in urban slums. The strategies that are being deployed under this include:
• Updatingofmicroplanstocoverallvillagesandhamletsinthecountry;
• Specialimmunizationdrivesinpocketsoflowimmunizationcoverage;
• Intensificationofimmunizationactivitybyobservingimmunizationweeksinlowperformingstates;
• IECrelatedactivitiesfordemandgenerationtowardsimmunization;
• Deploymentofadequatenumberofhealthworkers;
• Prioritizationofareaswithexclusivestrategyfor200poorperformingdistricts;
• Specialfocusonmigrantandmobilepopulations.
As per WHO “Assessing new vaccines for national immunization programmes a framework to assist decision makers – 2005”, today HIV/AIDS, tuberculosis (TB), malaria, respiratory and gastrointestinal infections form the bulk of infectious disease burden in developing countries. Many of these infections are potentially vaccine-preventable and vaccine development studies are accelerating. New vaccines present numerous issues in prioritizing investments of a national immunization programme.
The revolutionary new way of developing a vaccine is through Advance Market Commitment (AMC) (explained below).
Table 14: Advance Market Commitments – The new trend in Vaccination Industry
A new approach to public health funding, Advance Market Commitments (AMCs) are designed to stimulate the development and manufacture of vaccines specifically for developing countries. The pilot AMC is for a new vaccine to target pneumococcal disease. The donor commitments provide vaccine makers with the incentive they need to invest the considerable sums required to conduct research, train staff and build manufacturing facilities.
As part of the AMC, participating companies also make binding commitments to supply the vaccines at lower and sustainable prices after the donor funds made available for the initial fixed price are used up. Ultimately, developing country governments are able to budget and plan for immunization programmes, knowing that vaccines will be available in sufficient quantity, at a price they can afford, for the long term.
Pneumococcal disease takes the lives of 1.6 million people each year – including up to one million children before theirfifthbirthday.Morethan90%ofthesedeathsoccurindevelopingcountries.Itisestimatedthatthispilotproject could prevent more than seven million childhood deaths by 2030.
In June 2009, after two years of preparatory work, GAVI, the World Bank, WHO and UNICEF, five national governments and the Bill & Melinda Gates Foundation signed legal documents to formally kick-off the first-ever AMC, designed to accelerate access to vaccines against pneumococcal disease.
In March 2010, GlaxoSmithKline (GSK) and Pfizer Inc. became the first two companies to make long-term commitments to supply new vaccines for the Pneumo AMC. The two participating firms committed to supply 30 million doses each year for a 10-year period.
GAVI hopes to assist up to 60 of the world’s poorest countries to introduce these vaccines by 2015. Lessons learnt from this first AMC will help in the planning of other AMCs to tackle diseases such as HIV/AIDS, malaria and tuberculosis.
Source: GAVI Alliance: Advance Market Commitment
Sect
ion
2: V
acci
nati
on M
arke
t an
d St
rate
gic
App
roac
h fo
r In
dia
Indian Immunization Programme A Literature Review
24
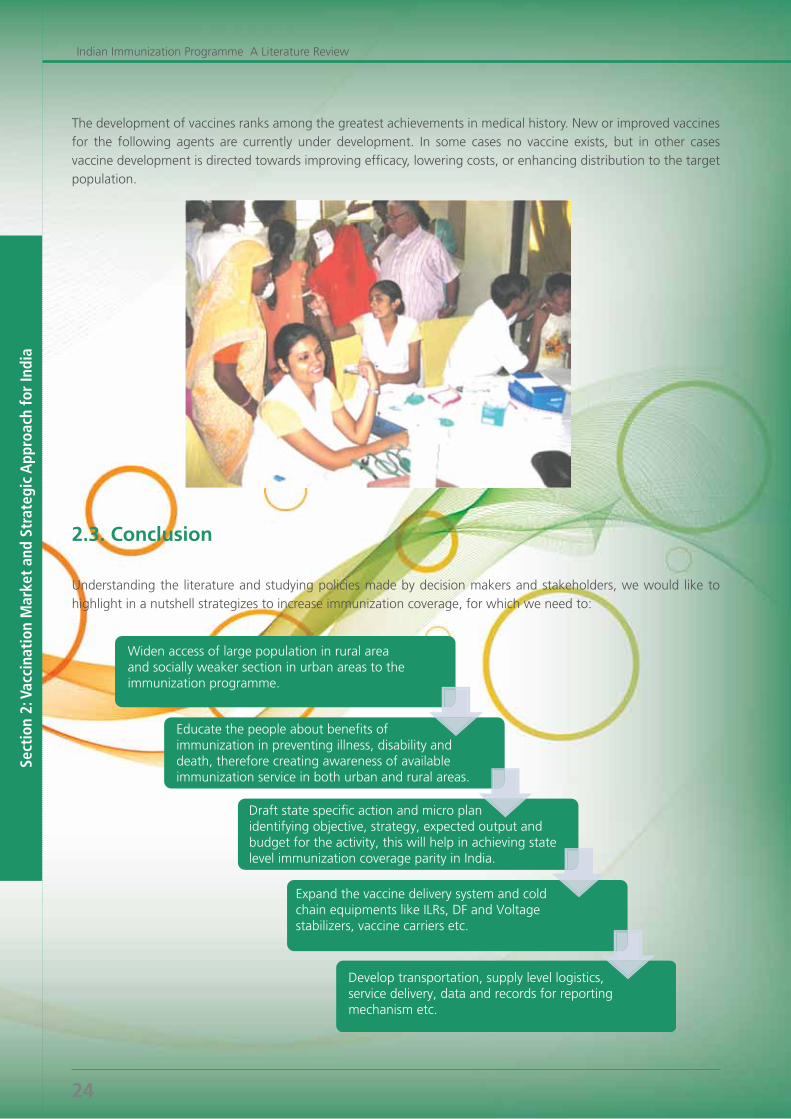
The development of vaccines ranks among the greatest achievements in medical history. New or improved vaccines for the following agents are currently under development. In some cases no vaccine exists, but in other cases vaccine development is directed towards improving efficacy, lowering costs, or enhancing distribution to the target population.
2.3. Conclusion
Understanding the literature and studying policies made by decision makers and stakeholders, we would like to highlight in a nutshell strategizes to increase immunization coverage, for which we need to:

Sect
ion
3: A
ppen
dix
and
Refe
renc
e
Indian Immunization Programme A Literature Review
27
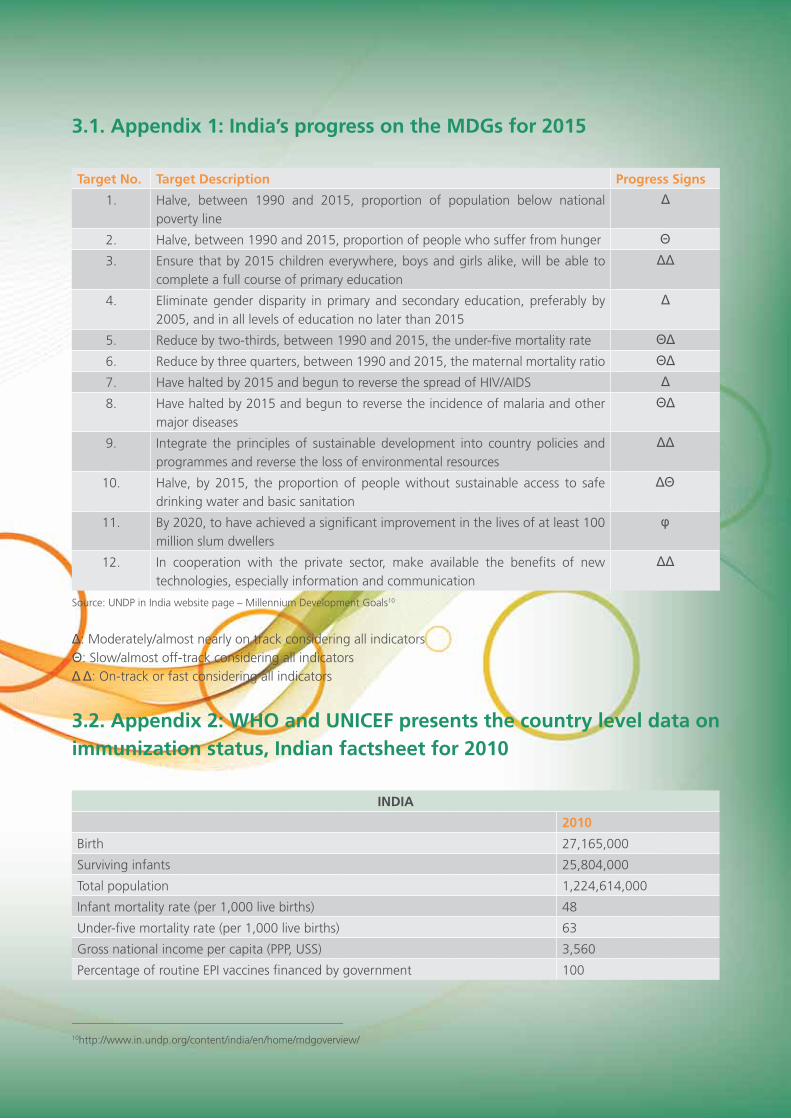
3.1. Appendix 1: India’s progress on the MDGs for 2015
Target No. Target Description Progress Signs
1. Halve, between 1990 and 2015, proportion of population below national poverty line
Δ
2. Halve, between 1990 and 2015, proportion of people who suffer from hunger Θ3. Ensure that by 2015 children everywhere, boys and girls alike, will be able to
complete a full course of primary education
ΔΔ
4. Eliminate gender disparity in primary and secondary education, preferably by 2005, and in all levels of education no later than 2015
Δ
5. Reduce by two-thirds, between 1990 and 2015, the under-five mortality rate ΘΔ6. Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio ΘΔ7. Have halted by 2015 and begun to reverse the spread of HIV/AIDS Δ8. Have halted by 2015 and begun to reverse the incidence of malaria and other
major diseases
ΘΔ
9. Integrate the principles of sustainable development into country policies and programmes and reverse the loss of environmental resources
ΔΔ
10. Halve, by 2015, the proportion of people without sustainable access to safe drinking water and basic sanitation
ΔΘ
11. By 2020, to have achieved a significant improvement in the lives of at least 100 million slum dwellers
φ
12. In cooperation with the private sector, make available the benefits of new technologies, especially information and communication
ΔΔ
Source: UNDP in India website page – Millennium Development Goals10
Δ: Moderately/almost nearly on track considering all indicatorsΘ: Slow/almost off-track considering all indicatorsΔ Δ: On-track or fast considering all indicators
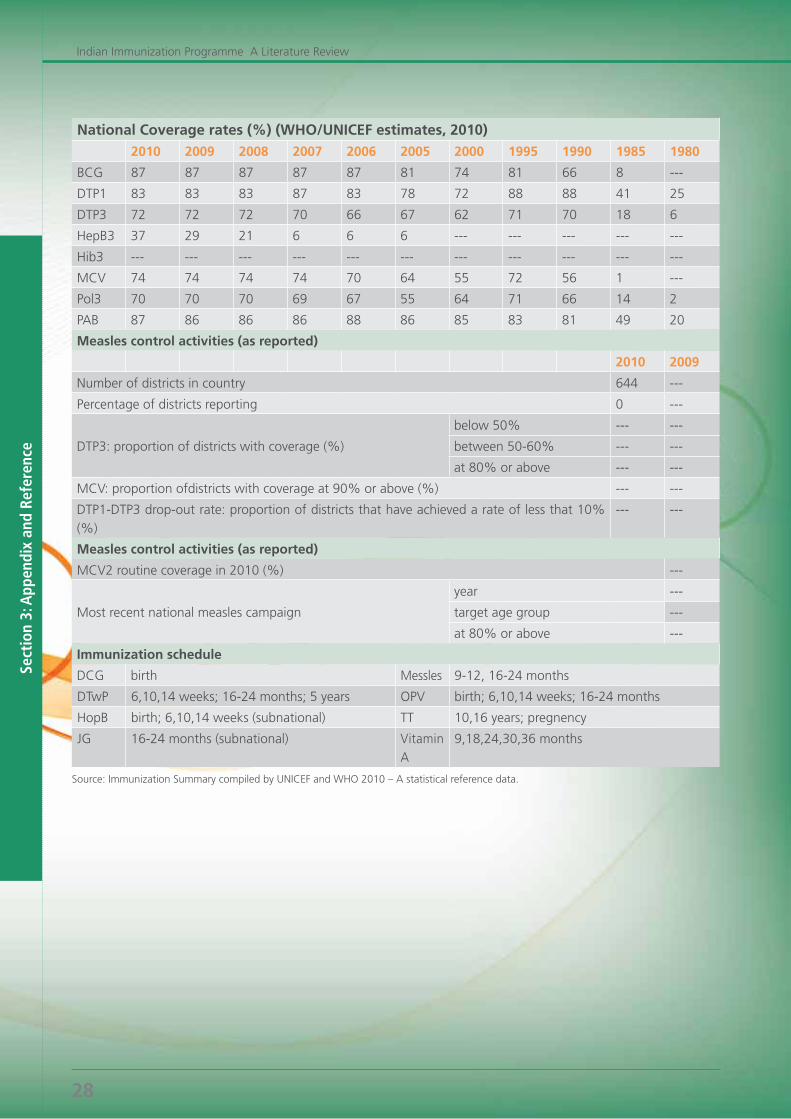
3.2. Appendix 2: WHO and UNICEF presents the country level data on immunization status, Indian factsheet for 2010
INDIA
2010
Birth 27,165,000
Surviving infants 25,804,000
Total population 1,224,614,000
Infant mortality rate (per 1,000 live births) 48
Under-five mortality rate (per 1,000 live births) 63
Gross national income per capita (PPP, USS) 3,560
Percentage of routine EPI vaccines financed by government 100
___________________________________________________
10http://www.in.undp.org/content/india/en/home/mdgoverview/
Sect
ion
3: A
ppen
dix
and
Refe
renc
e
Indian Immunization Programme A Literature Review
28
National Coverage rates (%) (WHO/UNICEF estimates, 2010)
2010 2009 2008 2007 2006 2005 2000 1995 1990 1985 1980
BCG 87 87 87 87 87 81 74 81 66 8 ---
DTP1 83 83 83 87 83 78 72 88 88 41 25
DTP3 72 72 72 70 66 67 62 71 70 18 6
HepB3 37 29 21 6 6 6 --- --- --- --- ---
Hib3 --- --- --- --- --- --- --- --- --- --- ---
MCV 74 74 74 74 70 64 55 72 56 1 ---
Pol3 70 70 70 69 67 55 64 71 66 14 2
PAB 87 86 86 86 88 86 85 83 81 49 20
Measles control activities (as reported)
2010 2009
Number of districts in country 644 ---
Percentage of districts reporting 0 ---
DTP3:proportionofdistrictswithcoverage(%)
below50% --- ---
between50-60% --- ---
at80%orabove --- ---
MCV:proportionofdistrictswithcoverageat90%orabove(%) --- ---
DTP1-DTP3drop-outrate:proportionofdistrictsthathaveachievedarateoflessthat10%(%)
--- ---
Measles control activities (as reported)
MCV2routinecoveragein2010(%) ---
Most recent national measles campaign
year ---
target age group ---
at80%orabove ---
Immunization schedule
DCG birth Messles 9-12, 16-24 months
DTwP 6,10,14 weeks; 16-24 months; 5 years OPV birth; 6,10,14 weeks; 16-24 months
HopB birth; 6,10,14 weeks (subnational) TT 10,16 years; pregnency
JG 16-24 months (subnational) Vitamin A
9,18,24,30,36 months
Source: Immunization Summary compiled by UNICEF and WHO 2010 – A statistical reference data.
Sect
ion
3: A
ppen
dix
and
Refe
renc
e
Indian Immunization Programme A Literature Review
29
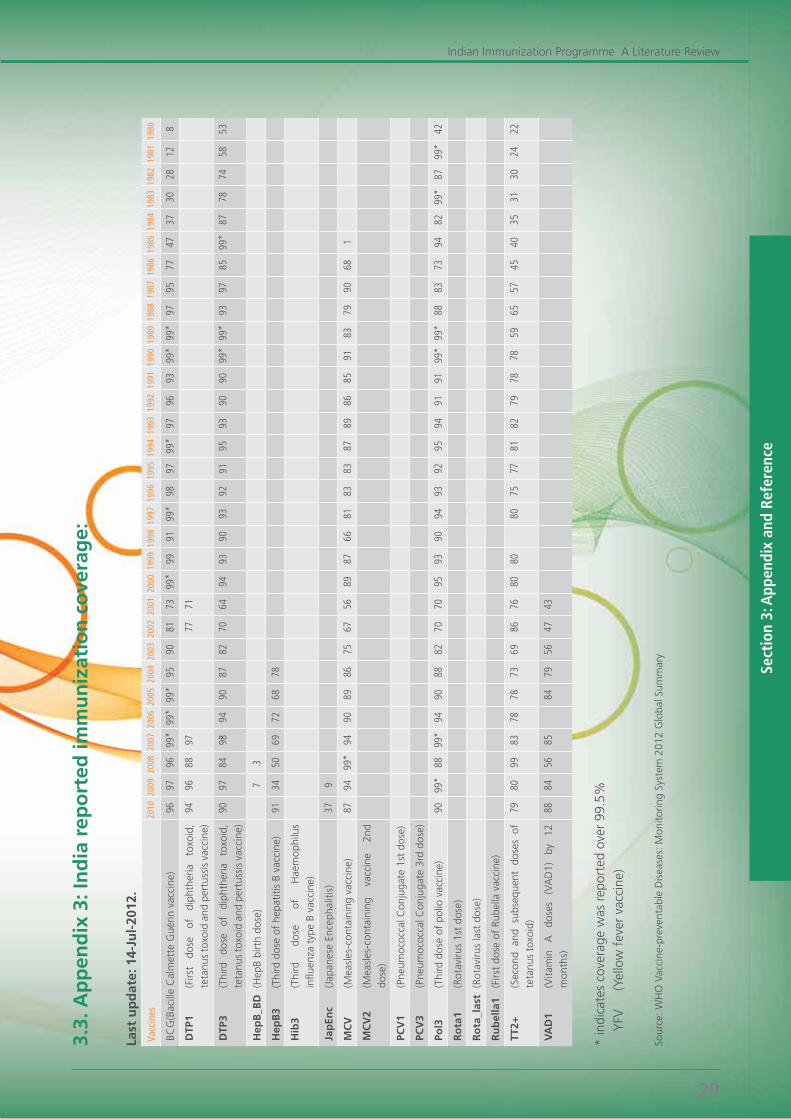
3.3.
Ap
pen
dix
3: I
nd
ia r
epo
rted
imm
un
izat
ion
co
vera
ge:
Last
up
dat
e: 1
4-Ju
l-20
12.
Vacc
ines
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
1989
1988
1987
1986
1985
1984
1983
1982
1981
1980
BCG
(Bac
ille
Cal
met
te G
uérin
vac
cine
) 96
97
96
99
* 99
* 99
* 95
90
81
73
99
* 99
91
99
* 98
97
99
* 97
96
93
99
* 99
* 97
95
77
47
37
30
28
12
8
DTP
1 (F
irst
dose
of
di
phth
eria
to
xoid
, te
tanu
s to
xoid
and
per
tuss
is v
acci
ne)
94
96
88
97
77
71
DTP
3
(T
hird
do
se
of
diph
ther
ia
toxo
id,
teta
nus
toxo
id a
nd p
ertu
ssis
vac
cine
)
90
97
84
98
94
90
87
82
70
64
94
93
90
93
92
91
95
93
90
90
99*
99*
93
97
85
99*
87
78
74
58
53
Hep
B_B
D
(Hep
B bi
rth
dose
)
7 3
Hep
B3
(Thi
rd d
ose
of h
epat
itis
B va
ccin
e)
91
34
50
69
72
68
78
Hib
3 (T
hird
do
se
of
Hae
mop
hilu
s in
fluen
za t
ype
B va
ccin
e)
Jap
Enc
(Jap
anes
e En
ceph
aliti
s)
37
9
MC
V
(Mea
sles
-con
tain
ing
vacc
ine)
87
94
99
* 94
90
89
86
75
67
56
89
87
66
81
83
83
87
89
86
85
91
83
79
90
68
1
MC
V2
(Mea
sles
-con
tain
ing
vacc
ine
2nd
dose
)
PCV
1 (P
neum
ococ
cal C
onju
gate
1st
dos
e)
PCV
3 (P
neum
ococ
cal C
onju
gate
3rd
dos
e)
Pol3
(T
hird
dos
e of
pol
io v
acci
ne)
90
99*
88
99*
94
90
88
82
70
70
95
93
90
94
93
92
95
94
91
91
99*
99*
88
83
73
94
82
99*
87
99*
42
Ro
ta1
(Rot
aviru
s 1s
t do
se)
Ro
ta_l
ast
(Rot
aviru
s la
st d
ose)
Ru
bel
la1
(Firs
t do
se o
f Ru
bella
vac
cine
)
TT2+
(S
econ
d an
d su
bseq
uent
dos
es o
f te
tanu
s to
xoid
)
79
80
99
83
78
78
73
69
86
76
80
80
80
75
77
81
82
79
78
78
59
65
57
45
40
35
31
30
24
22
VA
D1
(Vita
min
A
do
ses
(VA
D1)
by
12
m
onth
s)
88
84
56
85
84
79
56
47
43
*in
dica
tes
cove
rage
was
rep
orte
dov
er9
9.5%
YFV
(
Yello
w f
ever
vac
cine
)
Sour
ce: W
HO
Vac
cine
-pre
vent
able
Dis
ease
s: M
onito
ring
Syst
em 2
012
Glo
bal S
umm
ary
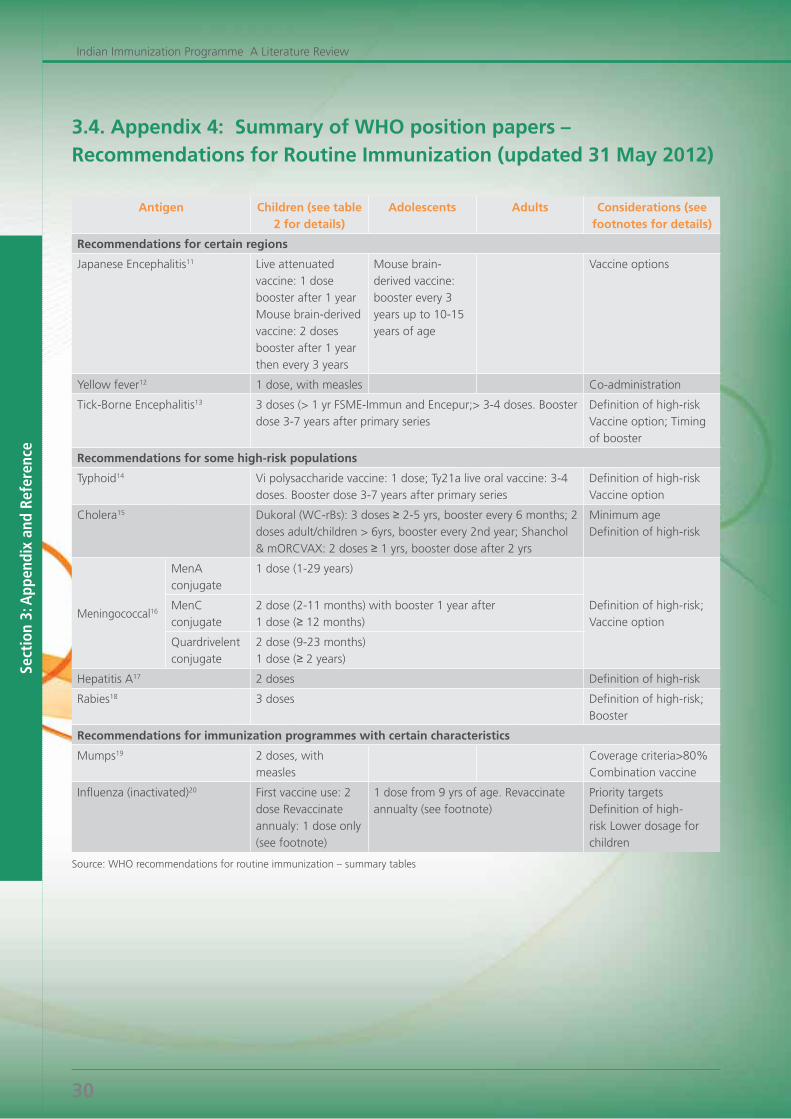
Sect
ion
3: A
ppen
dix
and
Refe
renc
e
Indian Immunization Programme A Literature Review
30
3.4. Appendix 4: Summary of WHO position papers – Recommendations for Routine Immunization (updated 31 May 2012)
Antigen Children (see table 2 for details)
Adolescents Adults Considerations (see footnotes for details)
Recommendations for certain regions
Japanese Encephalitis11 Live attenuated vaccine: 1 dose booster after 1 year Mouse brain-derived vaccine: 2 doses booster after 1 year then every 3 years
Mouse brain-derived vaccine: booster every 3 years up to 10-15 years of age
Vaccine options
Yellow fever12 1 dose, with measles Co-administration
Tick-Borne Encephalitis13 3 doses (> 1 yr FSME-Immun and Encepur;> 3-4 doses. Booster dose 3-7 years after primary series
Definition of high-risk Vaccine option; Timing of booster
Recommendations for some high-risk populations
Typhoid14 Vi polysaccharide vaccine: 1 dose; Ty21a live oral vaccine: 3-4 doses. Booster dose 3-7 years after primary series
Definition of high-risk Vaccine option
Cholera15 Dukoral (WC-rBs): 3 doses ≥ 2-5 yrs, booster every 6 months; 2 doses adult/children > 6yrs, booster every 2nd year; Shanchol & mORCVAX: 2 doses ≥ 1 yrs, booster dose after 2 yrs
Minimum age Definition of high-risk
Meningococcal16
MenA conjugate
1 dose (1-29 years)
Definition of high-risk; Vaccine option
MenC conjugate
2 dose (2-11 months) with booster 1 year after1 dose (≥ 12 months)
Quardrivelent conjugate
2 dose (9-23 months)1 dose (≥ 2 years)
Hepatitis A17 2 doses Definition of high-risk
Rabies18 3 doses Definition of high-risk; Booster
Recommendations for immunization programmes with certain characteristics
Mumps19 2 doses, with measles
Coveragecriteria>80%Combination vaccine
Influenza (inactivated)20 First vaccine use: 2 dose Revaccinate annualy: 1 dose only (see footnote)
1 dose from 9 yrs of age. Revaccinate annualty (see footnote)
Priority targets Definition of high-risk Lower dosage for children
Source: WHO recommendations for routine immunization – summary tables
Sect
ion
3: A
ppen
dix
and
Refe
renc
e
Indian Immunization Programme A Literature Review
31
Tables and Figures Index
Tables Table 1: Quick Facts: ImmunizationTable 2: Child Health Programme in India: 1950-2012Table 3 : WHO recommends National Immunization Schedule for India Table 4: Regression model analysis stating factors and their relationship with ImmunizationTable 5: Global and International Organizations Table 6: Authorities at work on Vaccination and Immunization in India Table 7: A framework for decision-making on new vaccines: set of questionsTable 8: Indian Vaccine Market: Top 10 New IntroductionsTable 9: Vaccine development and statusTable 10: Criterion for selection while introducing a new vaccine in UIP Table 11: Strategy pointer for High and Low Performing StatesTable 12: National Immunization Programme – Issues and Challenges Spectrum in India Table 13: A year of Intensification of Routine Immunization : 2012 – Strategic Approach To Improve Immunization CoverageTable 14: Advance Market Commitments – The new trend in Vaccination Industry
FiguresFigure 1: Vaccine preventable diseases: India reported cases (Year wise).Figure 2: Global Total Mortality in Children under 5 yearsFigure 3: Millennium Development Goals – The Eight Goals for 2015Figure 4: Immunization coverage – CES 2009 Figure5:Immunizationamongchildren%of12-23monthsFigure 6: Public Expenditure allocation – Centre and StateFigure 7: Healthcare spending by Government in IndiaFigure 8: Flowchart: Key Issues: Introduction of new vaccineFigure 9: Reasons for partial or no ImmunizationFigure10:FullImmunization(%)–State-wiseAchievementFigure 11: Immunization status among children of 12-23 months by states
Frequently Used Abbreviations
GoI Government of IndiaUNICEF United Nations Children’s FundUNDP United Nations Development ProgrammeUNFPA United Nations Population FundWHO World Health OrganizationNRA National Regulatory AuthorityMoHFW Ministry of Health & Family WelfareNRHM National Rural Health MissionMDG Millennium Development GoalsGAVI Global Alliance for Vaccines and Immunization
AllianceGIVS Global Immunization Vision and StrategyGFCV Global Fund for Children’s VaccinesAVI Asian Vaccination InitiativeADB Asian Development Bank EPI Expanded Programme on ImmunizationUPI Universal Immunization ProgrammeFYP Five Year PlanMYP Multi Year PlanCSSM Child Survival and State MotherhoodRCH Reproductive and Child HealthNFHS National Family Health SurveyDLHS District Level Household SurveyCES Coverage Evaluation Survey
UHC Universal Health Coverage GDP Gross Domestic ProductORT Oral Rehydration TherapyDCGI Drugs Controller General of India CDSCO Central Drugs and Standards Control
OrganizationCLAA Central Licensing Approval AuthorityNTAGI National Technical Advisory Group on
ImmunizationDATB Drug Technology Advisory Board GCP Good Clinical PracticeICMR Indian Council of Medical ResearchVPD Vaccine Preventable DiseasesAVD Alternate Vaccine DeliveryBCG Bacille Calmette Guérin VaccineDTP Diphtheria Toxoid, Tetanus Toxoid and Pertussis
VaccinePSUs Public Sector UnitsASHAs Accredited Social Health ActivistsAEFI Adverse Events Following ImmunizationITSU Immunization Technical Support UnitMCTS Mother and Child Tracking SystemAMC Advance Market CommitmentsIEC Information, Education and Communication

Sect
ion
3: A
ppen
dix
and
Refe
renc
e
Indian Immunization Programme A Literature Review
32
1. http://www.who.int/entity/gho/publications/world_health_statistics/EN_WHS2011_Full.pdf. Accessed on 27 December 2011..
2. Nilanjan Patra (2009) When Will They Ever Learn?’: The Great Indian Experience of Universal Immunisation Programme
3. Ministry of Health and Family Welfare. Government of India - District Level Household and. Facility Survey. All India Fact sheet- 2007-08. India.
4. Global, regional, and national causes of child mortality in. 2008: a systematic analysis. Robert E Black, Simon Cousens, Hope L Johnson, Joy E Lawn, Igor Rudan, Diego G Bassani, Prabhat Jha, Harry Campbell, Christa Fischer Walker, Richard Cibulskis, Thomas Eisele, Li Liu, Colin Mathers, for the Child Health Epidemiology Reference Group of WHO and UNICEF* May 2010 (http://wwwlive.who.int/immunization_monitoring/diseases/Lancet_2010_withAppendix.pdf)
5. Ajay Tandon and Cheryl Cashin (2010), Assessing Public Expenditure on Health from a Fiscal Space Perspective. (The International Bank for Reconstruction and Development / The World Bank)
6. Routine Immunization. Dr SD Khaparde Deputy Commissioner (ID & Imm) Ministry of Health & Family Welfare, Government of India
7. Coverage Evaluation Survey 2009 – National Fact Sheet.8. National Vaccine Policy April 2011 by Ministry of Health &
Family Welfare 9. Licensing procedure and inclusion of a vaccine in the National
Immunization Programme (NIP) of a country. IAP Guide Book on Immunization
10. WHO (December 2000) Assessing New Vaccines for National Immunization Programmes. A Framework to Assist Decision Makers.
11. Bhat Ramesh & Jain Nishant, Analysis of Public Expenditure on Health Using State Level Data, IIMA Working Papers WP2004-06-08
12. WHO, UNICEF, World Bank. State of the world’s vaccines and immunization, 3rd ed. Geneva, World Health Organization, 2009
13. 2012: Year of Intensification of Routine Immunization in the South-East Asia Region: Framework for increasing and sustaining coverage, Regional Committee document, 2011
14. Universal Immunization Programme. Progress, Challenges and steps to. Expand Coverage. Dr. Ajay Khera. Deputy Commissioner & Pubic Health Expert Child Health & Immunization Ministry of Health & Family Welfare, Government of India, 2011
15. Ministry of Health & Family Welfare, Govt. of India. An Overview. India’s Universal Immunization Programme. GAVI Alliance Board Meeting, Anuradha Gupta, 2011
16. McKinsey & Company’s report, India Pharma 2020: Propelling access and acceptance, realizing true potential.
17. Mid-Term Appraisal of Eleventh Five Year Plan 2007-2012, Planning Commission, Yojana Bhawan, Government of India.
18. WHO – Global Immunization Data. May 201219. UNICEF: Coverage Evaluation Survey Report 2009 (CES-2009):
All India Report20. Paul Wilson (2010) Giving developing countries the best shot:
An overview of vaccine access and R&D.21. UNICEF (2005): Immunization Summary – 2005: A Statistical
Reference.
22. World Health Organization (http://www.who.int).23. WHO (2004): ‘Economics of Immunization: A Guide to
the Literature and other Resources’, Dept. of Vaccines and Biologicals, (http://www.who.int/vaccines-documents/).
24. Universal Immunisation Programme in India: The Determinants of Childhood. Immunisation (2005)- Nilanjan Patra
25. Health Care Financing Reforms in India. M. Govinda Rao and Mita Choudhury. Working Paper No: 2012-100. March- 2012. National Institute of Public Finance and Policy
26. WHO (2005) – Vaccine Introduction Guidelines – Adding a vaccine to a national immunization programme: decision and implementation
27. Government Health Expenditure in India: A Benchmark Study – Undertaken for the MacArthur Foundation, India, Economic Research Foundation, New Delhi – August 2006
28. “Immunization in India: An Equity-Adjusted Assessment” With Abdo Yazbeck (World Bank) Health Nutrition and Population Paper Series, March 2006.
29. Summary of WHO Position Papers – Recommendations for Routine Immunisation Tables (updated: 31 May 2012)
30. UNICF/WHO, November 201131. WHO vaccine-preventable diseases: monitoring system 2010
global summary32. India Development Gateway (InDG) – Child Immunization
details 33. IMS-Health – June 2010 MAT34. GAVI Alliance: Advance Market Commitment35. WHO vaccine-preventable diseases: monitoring system 2012
global summary36. Assessing New Vaccines For National Immunization
Programmes: A framework to assist decision-makers, WHO (http://www.path.org/vaccineresources/files/wpro-new-vaccines.pdf)
37. Vaccine Development: current status and future needs. A report from the American Academy of Microbiology – October 2005
38. UNDP in India website page – Millennium Development Goals: http://www.in.undp.org/content/india/en/home/mdgoverview/)
39. Immunization Summary compiled by UNICEF and WHO 2010 – A statistical reference data.
40. http://kotharionindia.blogspot.in/2012/04/india-policy-action-for-achieving.html
41. http://www.in.undp.org/content/india/en/home/mdgoverview/42. http://www.who.int/immunization_monitoring/diseases/en/43. http://fr.gavialliance.org/vision/in_financing/amcs/index.php44. (http://www.path.org/vaccineresources/files/VaccineDev_ASM.
pdf)45. http://www.unicef.org/india/health_5578.htm46. http://www.unicef.org/immunization/index_coverage.html47. http://www.unicef.org/immunization/files/SOWVI_full_report_
english_LR1.pdf48. http://www.unicef.org/india/health_6679.htm49. http://ssrn.com/abstract=88122450. http://www.indg.in/india51. http://whqlibdoc.who.int/hq/2005/WHO_IVB_05.18.pdf52. http://www.unicef.org/immunization/index_43911.html53. h t t p : / / b i o s p e c t r u m i n d i a . c i o l . c o m / c o n t e n t /
CoverStory/11205112.asp
References and Sources:
IMPRIMIS RESEARCH AND ADVOCACY WING
Imprimis Research and Advocacy is the research analysis arm of Imprimis PR – India’s fastest growing public relations and communications consultancy.
Research is a systematic search for an answer to a question or a solution to a problem. Our key differentiator is our ability to understand issues, design customized approaches and perform analysis and deliver the results in time. Our company develops the best research techniques and specialized analytical methods, adopts data collection technology and provides business/market intelligence knowledge to our clientele.
We are a full-service research and advocacy consultancy with a nationwide network of offices and two parallel Headquarters in New Delhi and Mumbai providing a strong backbone with specialized support function. We hold unparalleled domain experience in working closely with healthcare providers, pharmaceuticals companies, biotechnology, healthcare retailing, FMCG sector, agriculture boards, foods and commodity organizations.
Our company develops the best research techniques and specialized analytical methods, adopts data collection technology and provides business/market intelligence knowledge to our clientele.
With the integrated research approach, innovative research tools and expert knowledge base, we provide quality research services to our esteemed clients. We adopt a mix of both primary and secondary tools as part of a research and analytical model.
Neha JindalResearch Lead
With a post graduation degree in M.A. (Economics) from Delhi School of Economics, Neha has more than six years of experience in research, analysis and feasibility studies. Currently working as a lead for Research and Advocacy team, she brings with her expertise and experience in conducting primary and secondary research analysis, market intelligence to analyze present industry trends and 360-degree plan for research execution.






























