Embed Size (px)
Citation preview

N E W S A N D V I E W S
1018 VOLUME 13 | NUMBER 9 | SEPTEMBER 2007 NATURE MEDICINE
muscle-specific ring finger protein-1 and atrogin-1. Therefore, these data indicate that ribosomal S6 protein and eIF4B do not mediate the muscle hypertrophic effects of S6K1 and that the loss of muscle size in the absence of S6K1 is not a consequence of increased protein degradation rates, or at least not through these catabolic systems.
Although much remains to be understood about the effects of S6K1 on skeletal-muscle hypertrophy, the data from these studies provide strong evidence that S6K1 modu-lates muscle growth together with AMPK,
acting as an integrator of fuel availability and spending. Exquisitely regulated, the fine balance between muscle-energy sens-ing and spending likely has additional con-trol switches that have yet to be discovered, which will certainly have an impact in our understanding of the regulatory circuitry of the cell.
COMPETING INTERESTS STATEMENTThe author declares no competing financial interests.
1. Glass, D.J. Int. J. Biochem. Cell Biol. 37, 1974–1984 (2005).
2. Nader, G.A. Int. J. Biochem. Cell Biol. 37, 1985–1996 (2005).
3. Bodine, S.C. et al. Nat. Cell Biol. 3, 1014–1019 (2001).
4. Mieulet, V. et al. Am. J. Physiol. Cell Physiol. 293, C712–C722 (2007).
5. Kahn, B.B., Alquier, T., Carling, D. & Hardie, D.G. Cell Metab. 1, 15–25 (2005).
6. Bolster, D.R., Crozier, S.J., Kimball, S.R. & Jefferson, L.S. J. Biol. Chem. 277, 23977–23980 (2002).
7. Chan, A.Y., Soltys, C.L., Young, M.E., Proud, C.G. & Dyck, J.R. J. Biol. Chem. 279, 32771–32779 (2004).
8. Inoki, K., Zhu, T. & Guan, K.L. Cell 115, 577–590 (2003).
9. Aguilar, V. et al. Cell Metab. 5, 476–487 (2007).10. Ohanna, M. et al. Nat. Cell Biol. 7, 286–294
(2005).
Schizophrenia drug says goodbye to dopamineDaniel R Weinberger
A drug that activates glutamate receptors offers promise for a new class of anti-psychotic therapeutics and sheds light on the pathophysiology of this devastating disease (pages 1102–1107).
All psychiatric drugs in common use today are derivatives of treatments that were originally discovered by accident. None were developed based on a scientific understanding of the causes or pathophysiology of mental illness. The modern era of clinical psychopharma-cology began over 50 years ago with the ser-endipitous observation by Henri Laborit, a French surgeon, that a new antihistamine called chlorpromazine had unusual tranquil-izing effects which, he proposed, could treat psychosis without major sedation. Subsequent studies confirmed his suspicion and suggested that chlorpromazine’s mechanism of action involved reducing dopamine neurotransmis-sion1, particularly dopamine D2–receptor signaling, in the brain2. Many follow-up drugs with slight variations in pharmacologic proper-ties and side-effect profiles have been marketed for the treatment of psychotic symptoms (for example, hallucinations and delusions), but all have been based on this antidopaminergic principle.
The finding that every available antipsy-chotic drug is antidopaminergic spawned the dopamine hypothesis of schizophrenia, an operational and enduring theory that psycho-sis is related to excessive dopaminergic activity
in the brain1. Despite the clinical benefits and antidopaminergic properties of these agents, convincing evidence that patients with schizo-phrenia have a primary abnormality of dopa-mine metabolism or receptor signaling has not been found.
In this context, the report of Patil et al.3 in this issue of Nature Medicine represents a potential sea change in the pharmacological approach to schizophrenia. Based on more recent evidence that glutamate neurotransmis-sion may be a key element in the pathology of schizophrenia, Patil et al. designed and tested a novel class of drugs that activate so-called group II metabotropic glutamate receptors (mGluR2 and mGluR3), which bind gluta-mate and signal through G proteins and cyclic mononucleotides. They report the first credible evidence of an effective antipsychotic drug that does not target dopamine.
An editorial in Nature4 referred to schizo-phrenia as “arguably the worst disease affect-ing mankind, even AIDS not excepted.” The disorder has a devastating and usually lifelong impact on an individual’s capacity to function in society. Schizophrenia typically emerges dur-ing young adulthood without specific warning signs, and it affects major aspects of cognition, perception and behavior. The classic symptoms of hallucinations, delusional ideas and thought disorganization tend to wax and wane with acute episodes of illness. There are also more stable and enduring deficits, such as problems with attention and memory, and these tend to predict overall social and vocational function.
Daniel R. Weinberger is at the Clinical Brain
Disorders Branch, Intramural Research Program,
National Institute of Mental Health, National
Institutes of Health, Bethesda, Maryland 20892,
USA.
e-mail: [email protected]
Presynaptic cell
Postsynaptic cell
Astrocyte
Glu
Glu
Glu
Glu
Glu
AMPANMDA
mGluR3
Glial glutamatetransportermGluR
Glutamate
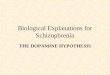
Figure 1 The novel compound for treating schizophrenia described in the study by Patil et al. is a specific agonist of the so-called group II metabotropic glutamate receptors, mGlurR2 and mGluR3. These receptors are found primarily on presynaptic neurons and regulate the release of neurotransmitters, especially glutamate. mGluR3 is also found on glia. On astrocytes, it regulates the expression of the glial glutamate transporter, which removes extracellular glutamate to modulate glutamate neurotransmitter signaling. Pharmacological targeting of mGluR2/3 is thought to be therapeutic for schizophrenia because it modulates glutamate synaptic activity.
Kat
ie R
is-V
icar
i
©20
07 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine

N E W S A N D V I E W S
NATURE MEDICINE VOLUME 13 | NUMBER 9 | SEPTEMBER 2007 1019
The drugs currently used to treat schizophrenia are more effective at controlling the florid psy-chotic symptoms than they are at improving cognitive deficits and social role performance.
Until very recently, almost nothing was known about the molecular pathophysiology of schizophrenia. Archival twin and adop-tion studies strongly suggested that genetic variation accounts for the lion’s share of indi-vidual risk, and epidemiologic studies have consistently found subtle abnormalities of early development as antecedents of the ill-ness5. Although these studies have suggested that schizophrenia arises from defects in brain maturation, likely because of interact-ing genetic and environmental factors, most research has been phenomenological, based on characterizing differences in behavior and in biological measures between patients and con-trols. But schizophrenia research has taken on a decidedly different aura of late, having been catapulted into the age of molecular medicine as a result of the discovery of putative suscep-tibility genes6 and the first objective clues to molecular mechanisms of the disorder7.
One of these candidate genes is GRM3, which encodes mGluR3 (ref. 8). The other group II receptor, mGluR2, is very similar in terms of DNA sequence and protein homol-ogy to GRM3, which has made it difficult to fully characterize the receptors individually, and to develop specific ligands for each of them. Nevertheless, mGluRs regulate syn-aptic concentrations of glutamate and other neurotransmitters, including dopamine, γ-aminobutyric acid (GABA) and serotonin, by inhibiting neurotransmitter release on the presynaptic neuron (Fig. 1). mGluR3 also is expressed on glia, particularly on astrocytes that straddle neuronal synapses, where it reg-ulates the reuptake of extracellular glutamate and the inactivation of glutamate synaptic signaling9.
Several other potential schizophrenia sus-ceptibility genes are related to glutamate neu-rotransmission, particularly signaling via the glutamate N-methyl-D-aspartic acid (NMDA) receptor ion channel5. The NMDA receptor had been previously implicated in schizophre-nia, when antagonists of the glutamate NMDA receptor were shown to induce abnormal men-tal states similar to schizophrenia10. It has been proposed that schizophrenia may be a genetic disorder of subtle abnormalities in glutamate synaptic function.
Knowing this, Patil et al. targeted the schizophrenia-associated glutamate recep-tors mGluR3 and mGluR2 with the amino acid analog known as the LY2140023 compound3. LY2140023 binds mGluR3 and mGluR2 with high affinity and stimulates their activity. Patil
et al. found that the mGluR2/3 agonist treat-ment in mice reduced the hyperlocomotion induced by NMDA antagonism3. This combi-nation of genetic, pharmacological and ani-mal data suggests that targeting mGluR3 and mGluR2 may be therapeutically valuable.
Patil et al.3 studied the clinical effects of LY2140023 in 97 patients with chronic schizo-phrenia, comparing their outcome after 4 weeks of treatment to that of 62 patients treated with placebo and 34 patients treated with a popular antipsychotic drug, olanzapine. The protocol was a randomized, double-blind, parallel fixed-dose study and was completed at ten clinical sites in Russia. To determine efficacy, the investigators measured comple-tion rates and improvement of schizophre-nia symptoms, including so-called ‘positive’ symptoms such as hallucinations, delusions and thought disorganization, and ‘negative’ symptoms such as emotional blunting, lack of motivation and paucity of thought.
Treatment with LY2140023 led to statisti-cally significant improvement in all primary outcome measures compared to placebo at the 4-week endpoint, and it was well tolerated. Importantly, individuals taking LY2140023 showed none of the typical side effects associ-ated with antidopaminergic treatment, such as parkinsonian motor signs or elevated serum prolactin. Moreover, in contrast to drugs such as olanzapine, which have negative meta-bolic side effects associated with weight gain, LY2140023 resulted in a net weight loss. These results are striking and potentially impor-tant.
The results of the phase 2 trial of Patil et al.3 provide tantalizing evidence that effec-tive antipsychotic therapy can ignore dopa-mine and directly target glutamate. There are, however, a number of issues raised by this trial that require further study. That this new compound is more effective than placebo over 4 weeks does not establish that it can stand on its own as a treatment for schizo-phrenia. Currently available drugs are woe-fully inadequate in restoring psychological and cognitive function, and for more than half of the patients who receive them they do not provide adequate relief10.
The small study of Patil et al.3 does not establish that this new drug will do any bet-ter. In fact, LY2140023 may not be as effective as olanzapine. The discontinuation rate was almost three times greater than that of olan-zapine, apparently because of lack of efficacy. Also, individuals on the new drug tended to experience a smaller reduction in positive symptoms than those taking olanzapine, even though the dose of olanzapine used in this study was lower than the standard doses10.
LY2140023 itself was originally developed to treat anxiety, and the possibility that its acute behavioral benefits are related to antianxiety rather than antipsychotic effects will need to be further examined.
Though it is designed to target the gluta-mate pathway, this new pharmacotherapeutic approach may be closer to the more tradi-tional antidopaminergic treatments than it first appears. Dopamine tunes the excitability of glutamate and GABA neurons in part by regulating the activity of glutamate NMDA channels and the availability of glutamate α-amino-3-hydroxy-5-methylisoxazole-4-pro-pionic acid (AMPA) receptors (Fig. 1). This changes the signal-to-noise characteristics of neurons in the prefrontal cortex, a cell popu-lation and brain area prominently implicated in schizophrenia12. Perhaps the antipsychotic actions of traditional antidopaminergic drugs fine tuned these glutamate-regulated cortical microcircuits. It will be important to deter-mine whether an mGluR2/3 agonist improves cortical function in psychosis any better than a dopamine antagonist does.
Antipsychotic drugs marketed within the past decade were originally heralded as major advances in terms of tolerability and efficacy, but such claims have increasingly been ques-tioned by more objective studies11. Time, clinical experience and the results of phase 3 clinical trials will provide important infor-mation about the ultimate clinical utility of this new approach to treating schizophrenia. Although the jury is out, there is reason for optimism. The days of designing new drugs for schizophrenia based on a half-century-old accident are numbered. Treatments based upon scientific insights about genetic etiol-ogy and pathophysiologic mechanisms have to be a better way to go.
COMPETING INTERESTS STATEMENTThe author declares no competing financial interests.
1. Carlsson, A. & Lindquist, M. Acta Pharmacol. Toxicol. (Copenh.) 20, 140–144 (1963).
2. Creese, I., Burt, D.R. & Snyder, S.H. Science 192, 481–483 (1976).
3. Patil, S.T. et al. Nat. Med. 13, 1100–1105 (2007).
4. Anonymous. Nature 336, 95–96 (1998).5. Ross, C.A., Margolis, R.L., Reading, S.A., Pletnikov,
M., & Coyle, J.T. Neuron 52, 139–153 (2006).6. Harrison, P.J. & Weinberger, D.R. Mol. Psychiatry 10,
40–68 (2005).7. Tan, W. et al. J. Biol. Chem. 282, 24343–24351
(2007).8. Egan, M.F. et al. Proc. Natl. Acad. Sci. USA 101,
12604–12609 (2004).9. Aronica, E. et al. Eur. J. Neurosci. 17, 2106–2118
(2003).10. Krystal, J.H. et al. Arch. Gen. Psychiatry 51, 199–
214 (1994).11. Lieberman, J.A. et al. N. Engl. J. Med. 353, 1209–
1223 (2005).12. Winterer, G. & Weinberger, D.R. Trends Neurosci. 27,
683–690 (2004).
©20
07 N
atur
e P
ublis
hing
Gro
up
http
://w
ww
.nat
ure.
com
/nat
urem
edic
ine