Embed Size (px)
Citation preview

CONCLUSIONS
BACKGROUND
ABSTRACT
SCD1 is a novel target in Anaplastic Thyroid Carcinoma
Christina A. von Roemeling1, Laura Marlow1, Robert C. Smallridge2, John A. Copland1
1Department of Cancer Biology, Mayo Clinic Florida, Jacksonville, Florida; 2Division of Endocrinology-Internal Medicine, Mayo Clinic Florida, Jacksonville, Florida.
October 19, 2013: Abstract 1756663
FUTURE DIRECTIONS
RESULTS
REFERENCES
A
pt. 1
36
PTC
FA
FTC-low
B Normal match to FA
ATC
pt.
306
pt. S
DAR
1
FTC-high
pt. 4
93
H = 172.9 ± 25.2, n=7
H = 123.8 ± 22.2, n=8 H = 37.9 ± 20.5, n=7
H = 105.1 ± 18.1, n=8
H = 50.2 ± 13.2, n=7 H = 48.1 ± 10.4, n=8
C
01020304050607080
THJ1
00N
THJ1
16N
THJ1
67N
THJ2
95T
THJ1
00T
THJ1
16T
THJ3
35T
EAM
136
KTC
1TP
C1
K1
LAM
1TH
J306
TS
DAR
1FT
C13
3M
L1TT
2609
-102
CG
THW
1S
DAR
2S
DAR
3W
RO
THJ2
1TTH
J11T
THJ1
6TTH
J29T FF
1FR
OK
TC2
normal FA PTC FTC ATCC
ell S
CD
1 m
RN
A
D
SCD1
β-actin
THJ1
6T
THJ2
9T
FTC
133
SD
AR
1
THJ3
06T
ML1
EA
M13
6
TPC
1
KTC
1
LAM
1
ATC NT FA PTC FTC
KTC
2
THJ1
03T
THJ2
95T
THJ1
00T
THJ1
67N
THJ1
16N
THJ1
00N
Cak
i1 (+
)
THJ1
16T
A B
C
IC50 (nM) THJ100T NA THJ295T NA THJ13T NA
IC50 (nM) THJ100N NA THJ167N NA THJ116N NA
D
IC50 (nM) SDAR1 NR FTC133 NR ML1 NR EAM306 NR THJ103T NR
IC50 (nM) LAM1 1000 TPC1 5000 KTC1 NR LAM136 NR THJ116T NR
0
20
40
60
80
100
120
140
DMSO 1 10 100 1000 10000
PTC
hi P
rolif
erat
ion
A939572 (nM)
LAM1TPC1KTC1EAM136TTHJ116T 0
20
40
60
80
100
120
140
DMSO 1 10 100 1000 10000
FTC
Pro
lifer
atio
n
A939572 (nM)
SDAR1FTC133ML1THJ306TTHJ103T
E
IC50 (nM) THJ29T 50 KTC2 100 THJ16T 90
F
0
20
40
60
80
100
120
140
THJ29T THJ16T KTC2
Prol
ifera
tion
DMSO BSA DMSO OAA939572 BSA A939572 OA
* * *
A
B
β-actin
S-XBP1
CHOP
PARP
- + - - + - - + -
THJ29T THJ16T KTC2
A939572 DMSO
OA-BSA BSA
+ - + + - + + - + + - - + - - + - - - + + - + + - + +
c-PARP
C
THJ2
9T
control A939572 A939572 + OA
THJ1
6T
*
0
10
20
30
40
50
control A939572 A939572+OA
THJ2
9T m
RN
A
GADD45aDDIT3HERPUD1
1647
13
5
05
101520253035
control A939572 A939572+OA
THJ1
6T m
RN
A
GADD45aDDIT3HERPUD1
00.5
11.5
22.5
33.5
44.5
control A939572 A939572+OA
KTC
2 m
RN
A
GADD45aDDIT3HERPUD1*
* *
*
*
*
* *
*
C 0 1 2 5 10
0
20
40
60
80
100
120
0 10 25 50 100
Carfilzomib (nM)
THJ1
6T P
rolif
erat
ion
A939572 (nM)
A939572A939:CarfCarfilzomib
0 1 2 5 10
0
20
40
60
80
100
120
0 1 10 25 50
Carfilzomib (nM)
THJ2
9T P
rolif
erat
ion
A939572 (nM)
A939572A939:CarfCarfilzomib
0 1 2 5 10
0
20
40
60
80
100
120
0 10 25 50 100
Carfilzomib (nM)
KTC
2 Pr
olife
ratio
n
A939572 (nM)
A939572A939:CarfCarfilzomib
0 0.2 0.4 0.6 0.8 1.00
0.3
0.6
0.9
1.2
Effect
Fa-CI plot
CI
a939:car CI = 1.0
1
2
34
0 0.2 0.4 0.6 0.8 1.00
0.5
1.0
1.5
Effect
Fa-CI plot
CI
a939:car CI = 1.0
1
234
0 0.2 0.4 0.6 0.8 1.00
0.5
1.0
1.5
2.0
2.5
Effect
Fa-CI plot
CI
a939:car CI = 1.0
1
2
34
a939 (nM) car (nM) Effect CI 1 10 1 0.88296 0.821 2 20 2 0.829304 1.031 3 30 5 0.460784 0.201 4 50 10 0.359008 0.224
a939 (nM) car (nM) Effect CI 1 10 1 0.973655 1.241 2 20 2 0.6348 0.587 3 30 5 0.332251 0.569 4 50 10 0.19198 0.708
a939 (nM) car (nM) Effect CI 1 10 1 0.985186 2.227 2 20 2 0.895403 1.026 3 30 5 0.600466 0.532 4 50 10 0.354651 0.512
THJ29T KTC2 THJ16T
0 1 2 4 6
020406080
100120140
0 10 25 50 100
Bortezomib (nM)
THJ1
6T P
rolif
erat
ion
A939572 (nM)
A939572A939:BortBortezomib
0 1 2 4 6
0
20
40
60
80
100
120
0 1 10 25 50
Bortezomib (nM)
THJ2
9T P
rolif
erat
ion
A939572 (nM)
A939572A939:BortBortezomib
0 1 2 4 6
0
20
40
60
80
100
120
0 10 25 50 100
Bortezomib (nM)
KTC
2 Pr
olife
ratio
n
A939572 (nM)
A939572A939:BortBortezomib
0 0.2 0.4 0.6 0.8 1.00
0.5
1.0
1.5
Effect
Fa-CI plot
CI
a939:bor CI = 1.0
1
23
4
0 0.2 0.4 0.6 0.8 1.00
0.5
1.0
1.5
Effect
Fa-CI plot
CI
a939:bor CI = 1.0
1
2
34
0 0.2 0.4 0.6 0.8 1.00
0.3
0.6
0.9
1.2
Effect
Fa-CI plot
CI
a939:bor CI = 1.0
1
234
a939 (nM) bort (nM) Effect CI 1 10 1 0.999 1.224 2 20 2 0.879913 0.767 3 30 5 0.484603 0.888 4 50 10 0.226386 1.188
a939 (nM) bort (nM) Effect CI 1 10 1 0.988699 1.351 2 20 2 0.849721 1.151 3 30 5 0.351924 0.897 4 50 10 0.134336 0.883
a939 (nM) bort (nM) Effect CI 1 10 1 0.72516 1.156 2 20 2 0.368839 0.498 3 30 5 0.227396 0.552 4 50 10 0.166951 0.639
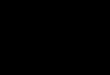
Figure 1: Expression Analysis of SCD1 in Thyroid Cancer
Figure 2: A939572 Inhibits ATC Cell Proliferation
Figure 3: A939572 Induces ER Stress in ATC
Figure 4: A939572 / Proteosome Inhibitor Synergy in ATC
D E
A
Introduction: Anaplastic Thyroid Carcinomas (ATC) are aggressive, undifferentiated tumors for which there currently is no cure. Although ATC accounts for a mere 1.7 percent of all thyroid cancers in the United States, it is disproportionately responsible for a large fraction of thyroid cancer related deaths. Patients diagnosed with ATC have grim prognoses, with a median survival rate of 5 months. ATC not only is resistant to traditional radio and chemotherapeutics, but targeted applications as well. Furthermore, due to its highly invasive nature, surgical resection is often not an option. Clearly, new therapies for ATC are sorely needed. Stearoyl-CoA Desaturase 1 (SCD1) is a fatty acid metabolism enzyme whose expression has been implicated in pro-tumor survival of several subsets of cancer. Methods: SCD1 expression patterns were examined in patient samples of normal thyroid, follicular adenoma (FA), papillary thyroid carcinoma (PTC), high grade follicular thyroid carcinoma (FTC), and ATC via quantitative real-time PCR as well as by immunohistochemistry. Activity of the SCD1 inhibitor A939572 was tested in representative patient derived cell lines. Results: SCD1 demonstrates high levels of expression in papillary thyroid carcinoma (PTC), high grade follicular thyroid carcinoma (FTC), and ATC. Application of an SCD1 inhibitor (A939572) surprisingly yielded strong anti-tumor proliferation and induction of apoptosis specifically in ATC cell lines, but had little to no activity among the other subtypes of thyroid carcinomas. In addition, A939572 induced the endoplasmic reticulum (ER) stress pathway, leading to endoplasmic reticulum associated degradation (ERAD) activation- a proteasome mediated survival response to ER stress. Sequential application of a proteasome inhibitor with A939572 led to synergistic anti-tumor activity in ATC cell lines. Conclusions: We propose that administration of an SCD1 inhibitor concomitantly with a proteasome inhibitor is a novel course of treatment that may provide a clinical benefit for patients presenting with ATC.
ATC: • The origin of ATC is unknown, but is thought to arise from less aggressive pre-existing
thyroid cancers such as the papillary variant • ATC progresses rapidly, and requires immediate medical intervention once diagnosed • Mean survival rate of 3 to 9 months post diagnosis, with less than 10-15% of patients surviving
2+ years • 20-50% of patients present with distant metastasis at time of diagnosis, and 25% develop new
metastasis during disease progression • ATC is classified as stage IV regardless of tumor size or presence of lymph node or distant
metastasis (American Joint Committee on Cancer) • Radical tumor resection of ATC confers a substantial survival benefit, with complete
resection identified as a prognostic factor for survival • Common mutations reported in ATC include p53 (55%), RAS (22%), BRAF (26%), β-catenin
(38%), PIK3CA (17%), Axin (82%), APC (9%), PTEN (12%) SCD1:
• SCD1 is a fatty acid metabolism enzyme belonging to a family of fatty acyl desaturases, whose role is to catalyze the biosynthesis of ∆9 monounsaturated fatty acids (MUFA), oleic and palmitoleic acid, from the saturated fatty acids (SFA) stearic and palmitic acid
• SCD1 has been proposed as a therapeutic target in other aggressive cancers including renal, breast , prostate, lung, and ovarian carcinomas
• Inhibition of SCD1 activity has been shown to induce the ER stress response in cancer cells Treatment:
• Currently there is no defined standard of care therapy for patients with ATC • ATC does not respond to radioiodine therapy or TSH suppression with thyroxine • Treatment includes combination of radiotherapy with chemotherapy (cisplatin, doxorubicin,
paclitaxil, carboplatin) and targeted therapy • Targeted therapies under investigation in ATC: Anti-angiogenic therapy (Pazopanib), vascular
disrupting agents (Combretastatin A4 phosphate), Tyrosine kinase inhibitors (Imatinib, Sorafenib), Histone deacetylase inhibitors (valproic acid), and PPARϒ agonists (Efatutazone)
1. Roongta UV, Pabalan JG, Wang X, Ryseck RP, Fargnoli J, Henley BJ, et al. Cancer cell dependence on unsaturated fatty acids implicates stearoyl-CoA desaturase as a target for cancer therapy. Mol Cancer Res. 2011;9:1551-61. 2. Fleming ID, Phillips JL, Menck HR, Murphy GP, Winchester DP. The National Cancer Data Base report on recent hospital cancer program progress toward complete American Joint Committee on Cancer/TNM staging. Cancer. 1997;80:2305-10. 3. Kebebew E, Greenspan FS, Clark OH, Woeber KA, McMillan A. Anaplastic thyroid carcinoma. Treatment outcome and prognostic factors. Cancer. 2005;103:1330-5. 4. Smallridge RC, Copland JA. Anaplastic thyroid carcinoma: pathogenesis and emerging therapies. Clin Oncol (R Coll Radiol). 2010;22:486-97. 5. Perri F, Lorenzo GD, Scarpati GD, Buonerba C. Anaplastic thyroid carcinoma: A comprehensive review of current and future therapeutic options. World J Clin Oncol. 2011;2:150-7. 6. Rusinek D, Szpak-Ulczok S, Jarzab B. Gene expression profile of human thyroid cancer in relation to its mutational status. J Mol Endocrinol. 2011;47:R91-103. 7. Smallridge RC, Copland JA, Brose MS, Wadsworth JT, Houvras Y, Menefee ME, et al. Efatutazone, an oral PPAR-gamma agonist, in combination with paclitaxel in anaplastic thyroid cancer: results of a multicenter phase 1 trial. J Clin Endocrinol Metab. 2013;98:2392-400. 8. Deshpande HA, Roman S, Sosa JA. New targeted therapies and other advances in the management of anaplastic thyroid cancer. Curr Opin Oncol. 2013;25:44-9. 9. Brown RF, Ducic Y. Aggressive surgical resection of anaplastic thyroid carcinoma may provide long-term survival in selected patients. Otolaryngol Head Neck Surg. 2013;148:564-71. 10. von Roemeling CA, Marlow LA, Wei JJ, Cooper SJ, Caulfield TR, Wu K, et al. Stearoyl-CoA desaturase 1 is a novel molecular therapeutic target for clear cell renal cell carcinoma. Clin Cancer Res. 2013;19:2368-80.
• SCD1 demonstrates elevated expression patterns in PTC, advanced FTC, and ATC subtypes of thyroid carcinoma when compared to normal and benign thyroid tissue
• Presence of SCD1 protein does not dictate response to anti-SCD1 therapy • ATC cells uniquely demonstrate decreased proliferation and induction of
apoptosis in response to SCD1 inhibition (A939572) • SCD1 inhibition in ATC induces the ER stress response, leading to up-regulation
of transcriptional inhibitors, molecular chaperones, and ERAD • ATC cells are sensitive to mono-therapeutic inhibition of proteosome activity
using the inhibitors carfilzomib and bortezomib • Complementary targeted inhibition of the proteosome degradation pathway
using either carfilzomib or bortezomib in addition to SCD1 inhibition results in the synergistic inhibition of ATC proliferation
• Our hypothesized molecular mechanism of drug synergy between A939572 and a proteosome inhibitor is mediated by blockage of ERAD induction and survival caused by SCD1 inhibition
• SCD1 and proteosome activity present as novel therapeutic targets in ATC
0
20
40
60
80
100
120
0 1 10 100 1000
Gro
wth
(% D
MSO
ctr
l)
Carfilzomib (nM)
THJ29TKTC2THJ16T
bortezomib IC50 (nM) THJ29T 6 KTC2 6
THJ16T 7
carfilzomib IC50 (nM) THJ29T 10 KTC2 4
THJ16T 15
B
• Development of an orthotopic preclinical model of ATC to examine effects of drug treatment on tumor growth, local invasion, and metastasis
• Validation of mono-therapeutic activity of an SCD1 inhibitor and a proteosome inhibitor in a preclinical model of ATC
• Validation of combinatorial therapy using an SCD1 inhibitor together with a proteosome inhibitor in a preclinical model of ATC
• Pharmacokinetic and pharmacodynamics assessment of combinatorial therapy • Investigation of efficacy of SCD1/proteosome inhibitor combinatorial drug
therapy in other aggressive tumor models and in cases of refractory disease • Initiation of a phase I clinical trial investigating tumor response to combinatorial
therapy in patients with ATC
A) mRNA transcript levels of SCD1 in patient thyroid tissues including normal, follicular adenoma (FA), PTC, FTC, and ATC . Values are represented as fold change induction normalized to normal thyroid tissue expression of SCD1. B) Immunohistochemistry of SCD1 protein expression in patient thyroid tissues. The FTC variant is sub-divided into low grade and high-grade cases. Stain intensity is quantified by H-score. C) mRNA transcript levels of SCD1 in cells derived from patient thyroid tissues. Values are represented as fold change induction normalized to normal thyroid cell expression of SCD1. D) Western blot of SCD1 expression in cells derived from patient thyroid tissues.
Drug dose response of thyroid cells including (A) normal, (B) follicular adenoma (FA), (C) PTC, (D) FTC, and (E) ATC cells to A939572, a small molecule selective inhibitor of SCD1 activity. (F) Target specificity was confirmed by rescue of cell proliferation in A939572 treated (IC50 dose) ATC cells with oleic acid (OA), the primary product of SCD1 .
Evaluation of ER stress induction in ATC cells treated with A939572 by (A) QPCR analysis of three ER stress genes (GADD45a , DDIT3 (CHOP), HERPUD1) and (B) Western blot for protein expression of CHOP and spliced-XBP1. (C) Western blot for PARP cleavage (c-PARP) indicating programmed cell death. (D) Representative phase-contrast microscopy of ATC cells treated with A939572 +/- OA rescue demonstrating cell death (decreased cell density and cell detachment) and subsequent rescue with oleic acid.
(A) Proposed model of SCD1 inhibitor and proteosome inhibitor drug synergy. Drug dose response of ATC cells to proteosome inhibitors (B) carfilzomib (targets 20S proteosome subunit) and (C) bortezomib (targets 26S proteosome subunit). Mono and combinatorial dose response and synergy curves of (C) THJ29T, (D) THJ16T, and (E) KTC2 ATC cells treated with A939572 and either carfilzomib or bortezomib. Synergy is indicated indicated by the combination index (CI) determined using CalcuSyn® where synergistic values are CI<0.9 (green highlight), additive values are 0.9-1.1 (yellow highlight), and agonistic values are 1.1<CI.

![TRIF-dependent Toll-like receptor signaling suppresses Scd1 … · [poly(I:C)] suppressed the increase in SCD1 abundance ind uced by palmitic acid or an HFD and subsequently prevented](https://img.pdfslide.us/doc/110x75/5e6e4023df96fd6fa13818a2/trif-dependent-toll-like-receptor-signaling-suppresses-scd1-polyic-suppressed.jpg)