Embed Size (px)
Citation preview

INTRODUCTION
Well-differentiated thyroid carcinomas areusually slowly growing asymptomatic tumorsthat carry an excellent prognosis when treatedproperly. Anaplastic thyroid carcinomas (ATC)are aggressive undifferentiated tumors with avery high mortality rates. They usually infiltrateinto surrounding tissues at the time of diagnosis,and have unfavorable prognosis. Among thyro-id carcinomas, ATC is the third in frequency ata rate of 1.6% after papillary and follicular car-cinomas (1,2,3). The average survival is 6-12
months with a 10-year survival of approxima-tely 3 percent (4). Most patients have localsymptoms such as dysphagia, dysphonia, stridorand neck pain. Although some series report afew cases of incidental ATC in thyroid nodules,ATC frequently appears as a rapidly growingmass in the neck. About 40% of the cases havecervical lymph node metastases, 90% directlyinvade the surrounding soft tissues and organssuch as trachea and larynx and 75% have distantmetastases. Metastases are seen most commonlyin the lungs and the brain (1,2,5).
CASE REPORT
A 50-year-old female patient had undergo-ne diagnostic fine needle aspiration biopsy(FNAB) of a nodule 1 cm in diameter localized
ABSTRACT
Anaplastic thyroid carcinoma is one of the most aggres-sive of all human malignant diseases. It has an unfavo-rable prognosis and responsible for most of the morta-lity and morbidity rates due to thyroid carcinomas. Wepresent a case of incidental anaplastic thyroid carcino-ma and discuss the epidemiology, biology, risk factors,prognostic factors of the disease and the approach totreatment, in the light of the current medical literature.The prognosis is much better in cases with incidentalcarcinoma compared to the classical type and surgicalexcision of the tumor has a favorable effect on the re-sults. Our case was followed-up for 1.5 years with noevidence of recurrence or metastasis.
Key words: Thyroid, anaplastic, carcinoma, inciden-tal, immunohistochemistry
ÖZET
Anaplastik tiroid karsinomu; insan maligniteleri içindeen agresif olan tümörlerden biridir. Kötü prognozludurve tiroid karsinomlar›na ba¤l› mortalite ve morbidite-nin önemli k›sm›n› oluflturmaktad›r. Biz bu makaledeanaplastik tiroid karsinomlu bir olgu rapor ederek epi-demiyoloji, biyoloji, risk faktörleri ve prognostik fak-törleri, tedavi yaklafl›mlar›n› literatür bilgileri eflli¤indetart›flt›k. ‹nsidental karsinomlu olgularda prognoz kla-sik tipe göre daha iyidir ve tümörün cerrahi olarak ç›-kar›lmas›, sonuçlar› olumlu etkilemektedir. Olgumuztan› sonras› 1.5 y›l takip edilmifl olup, nüks veya metas-taz saptanmam›flt›r.
Anahtar sözcükler: Tiroid, anaplastik, karsinom, insi-dental, immünhistokimya
Incidental anaplastic thyroid carcinoma: A case report
‹nsidental anaplastik tiroid karsinomu:Olgu sunumu
Pembegül GÜNEfi1, Fügen Vardar AKER1, Murat ERKAN1, Pelin DEM‹RTÜRK1, Ender DULUNDU2
Haydarpasa Numune Education and Research Hospital Department of Pathology1, 5th Surgical Clinics2, ‹STANBUL
Received: 01.11.2007Accepted: 01.01.2008Corresponding Author: Dr. Pembegül Günefl, T›bbiye Cad.Haydarpafla Numune E¤itim ve Araflt›rma Hastanesi PatolojiBölümü, 34668, Üsküdar, ‹stanbul
54
Turkish Journal of Pathology 2008;24(1):54-58

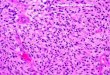
within the right lobe of the thyroid gland whichwas found to be radiologically suspicious 8months ago. FNAB had shown thyrocytes thatformed single-layer cohesive groups and colloi-dal material in the background, interpreted as a"benign colloidal nodule". She underwent bila-teral subtotal thyroidectomy 8 months later asher clinical symptoms persisted. On macrosco-pic examination, the gland was encapsulated ex-cept for one side and measured 7x5x3 cm. The-re was one nodule with a cross-section rich incolloid in the right lobe where the FNAB wasperformed while there was another nodule 2 cmin diameter which was separated from the surro-unding thyroid tissue with a thick fibrous capsu-le. Other areas were normal. Four micron thickHE stained sections obtained from routine pa-raffin blocks showed an adenomatous noduleconsisting of multi-sized follicles filled withcolloidal material detected on the microscopicexamination of the right lobe nodule. Microsco-pic examination of the 2 cm nodule in the left lo-be showed a tumor where pleomorphic cellsproliferated with a solid pattern around largeareas of necrosis surrounded by a thick fibrouscapsule (Figure 1a-b). Tumor cells consisted ofatypical cells containing a few nucleoli, withamphophilic cytoplasm, a bizarre nucleus and acoarse chromatin pattern in some areas and con-tained osteoclast-type multinuclear giant cellswhile other areas had squamoid characteristics.The component with squamoid characteristicsdid not have tumor cells forming trabeculae, fol-
licles\ nests or papillary structures, but there we-re morphological characteristics of epithelialdifferentiation. There were spindle and giantcells forming a fascicular and storiform patternin the sarcomatoid areas. All nodule was samp-led to find any concurrent well-differentiatedcarcinoma focus. There were no findings of dif-ferentiated thyroid carcinoma or extracapsularinvasion. The histopathological differential di-agnosis was between ATC, primary and metas-tatic sarcomas, insular carcinoma and metastaticcarcinomas. The palisading encirclement of thelarge central necrosis area by tumor cells andthe sarcomatous component of spindle and mul-tinuclear giant cells accompanied by undifferen-tiated epithelial areas made a diagnosis of anap-lastic thyroid carcinoma likely. We used pri-mary antibodies pancytokeratin (Neomar-kers/Biogen1/100-200), Epithelial membraneantigen (EMA) (Neomarkers/Biogen ready touse), Thyroglobulin (Neomarkers/Biogen readyto use) and Carcinoembryonic antigen (CEA)(Dako 1/25) for the immunohistochemical study(streptavidine-biotin immunoperoxidase techni-que, AEC chromogen) to determine the natureof the cells. There was strong staining withpancytokeratin and focal positive staining withEMA and CEA that excluded the possibility ofprimary and metastatic sarcomas (Figure 2). Weused thyroglobulin staining for the insular carci-noma and calcitonin for the medullary carcino-ma possibilities considered in the differential di-agnosis. Neither results were positive, excludinginsular and medullary carcinomas. Pancytokera-tin is the most important marker in the immuno-
Figure 1a. Pleomorphic cells proliferated with a solid and stori-form pattern around large areas of necrosis (HE x200). b. Thetumor was surrounded by a thick fibrous capsule (HE x100).
Figure 2. Anaplastic carcinoma showing positive reaction forkeratin in squamoid areas of the tumor (x200).
55
Incidental anaplastic thyroid carcinoma: A case report

histochemical differential diagnosis of ATCwith a staining rate of 50-100%. Thyroglobulinstaining has (8%) been rarely reported (6). Ho-wever, there was no staining in our case (Figure3). We looked for a primary focus with radiolo-gical, clinical and biochemical tests to eliminatethe possibility of a metastatic carcinoma and fo-und no primary neoplastic foci. The case was di-agnosed as an incidental anaplastic thyroid car-cinoma after evaluation of the histopathological,immunohistochemical and clinical findings.Subsequent total thyroidectomy, radiotherapyand chemotherapy were performed for treat-ment. The patient was alive 1.5 years later.
DISCUSSION
Anaplastic thyroid carcinoma is seen at arate of 1.6% in endemic goiter regions, third infrequency following papillary and follicular car-cinoma. The incidence has decreased from 5-14% in 1990s to 1.7-2% in 2000s (1,2,7,8,9).Agraval et al (10) have reported the ATC inci-dence as 7.7% between 1969 and 1973 and4.2% between 1989 and 1993. Lampertico et al(11) have reported a decrease from 11% to 5%from 1979 to 1993. On the contrary, the rate ofwell differentiated papillary carcinomas has me-anwhile increased about 3.5% during this period(10,12).
The decreased ATC incidence has beenexplained in many ways. When the hypothesisof de-differentiation of benign or malignantthyroid diseases for the etiopathogenesis of
ATC is taken into account, many benign andmalignant thyroid diseases that are risk factorsfor ATC development are now treated at anearly stage with effective surgery. It is reportedthat ATC is seen twofold in frequency in areasof endemic goiter (13). The use of prophylacticiodine in endemic areas in recent years seems tohave eliminated another important risk factor(13,14). Another factor that may explain thedecreased incidence of ATC is that many tu-mors are now correctly being diagnosed aslymphoma, undifferentiated insular carcinomaor medullary carcinoma with the increased ava-ilability of immunohistochemical studies (15). Itis therefore easy to explain the decreased inci-dence in recent years.
ATC is seen frequently in women in their6th or 7th decades. The female/male ratio is 3/1-1.2/1. The most comprehensive study on thesubject is the 134-case series of McIver et al(16) that states that the first clinical symptom isa rapidly growing mass in up to 97% of the pa-tients. Hemorrhage into the mass may cause pa-in and dysphagia. About 50% of the cases havedistant metastases at the time of diagnosis (3,13,14,17).
"Incidentaloma" can be defined as anasymptomatic tumor found incidentally duringan unrelated procedure (18). The rate of smalloccult tumors found incidentally during an au-topsy or surgical series has been reported as 0.5-13% in various articles. The rate of incidentaltumors is now increasing rapidly with the exten-sive use of ultrasound and other imaging studies(13,18). Most incidental tumors are papillarymicrocarcinomas. ATCs are rarely found inci-dentally in thyroid nodules (13,18). IncidentalATC is defined as an ATC focus in a differen-tiated tumor focus (5). This definition is closelyrelated to the etiopathogenesis. Nishiyama et al(19) have reported that when multiple samplingis performed on an ATC cases, a focus of a well-differentiated cancer is always found. Ibanez etal (11) have sampled the thyroid in 42 cases andfound a well-differentiated tumor focus in eachcase. When a well-differentiated tumor cannotbe found, it is thought that this is due to inade-quate sampling or ATC growing to a size thatdestroys all well-differentiated tumor (11). Sa-
Figure 3. There was no immunostaining with thyroglobulin intumour cells (x100).
56
Turkish Journal of Pathology 2008;24(1):54-58

bin et al (20) have found a concurrent well-dif-ferentiated carcinoma in 21-79% of ATC cases.We did not find a well-differentiated focus inour case although all nodule was sampled.
There are two etiopathogenetic theories onATC development. One is the development dueto anaplastic transformation of an accompan-ying well-differentiated tumor and the other oneis the de novo development theory (1,7,17,21).The presence of a previous or concurrent well-differentiated carcinoma is 24-89% for ATC(21). Its incidence in the elderly and in long-term tumors that have not been adequately trea-ted supports the anaplastic transformation the-ory. A study has found insular carcinoma in27% and anaplastic carcinoma in 24% of wo-men with goiter of more than 10 years duration(2). Demeter et al (22) have reported previousbenign or malignant thyroid pathology in up to76% of ATC cases and that 46% of these caseshad previous or concurrent papillary thyroidcarcinoma.
Genetic studies to understand the pathoge-nesis, progress and kinetics of tumors have in-creased recently and provided some insight intothe development of the incidental ATC (23).The loss of tumor suppressor gene p53 has beenshown in colon, lung and breast tumors and alsothyroid tumors (24). The dedifferentiation froma well-differentiated thyroid carcinoma into un-differentiated or anaplastic thyroid carcinoma isassociated with a p53 mutation. ATC casesshow a higher incidence of p53 mutation thandifferentiated thyroid carcinomas (25). Sniezeket al (24) showed loss of p21 gene expression inanaplastic and insular carcinomas. The BRAFmutation is the most common mutation in papil-lary carcinomas as shown in many recent gene-tic studies and it has been found more frequentlyin cases with dedifferentiation from well-diffe-rentiated carcinoma (4,20,23,26). The rate of aBRAF mutation in a study by Nikiforova et al(20) has been found to be 38% in papillarythyroid carcinoma, 0% in follicular and Hurtlecell carcinoma, 13% in well-differentiated car-cinoma, 10% in anaplastic carcinoma, and 0%in medullary carcinoma, Hurtle cell adenomaand hyperplastic nodules.
The prognosis of anaplastic thyroid carci-
noma depends on many factors such as age, gen-der, tumor size and resectability. Guiffride et al(27) have reported the patient's age and the ex-tent of the disease at the time of diagnosis as themost important prognostic factors. Sugino et al(13) studied 47 cases and listed the importantprognostic factors as the presence of acutesymptoms, a tumor diameter more than 5 cm,distant metastases and leucocyte counts over10.000/ml. Another study by Venkatech et al (7)reported the mean survival as 8 months for loca-lized and 3 months for metastatic disease. Whenincidental ATC and classical ATC are compa-red, there is inadequate data about better prog-nosis (13,17). Pierie et al (5) have reported a 1-3 year survival rate of 90% for incidental ATC.However, the number of incidental ATC casesin this series is not adequate to reach statisticallysignificant conclusions (5).
It is important to understand carcinogene-sis to define treatment strategies. Treatment ofATC varies as it is rare and presents at variousstages at the time of diagnosis (13). ATC is se-en more often in the elderly of poor general he-alth status. Since it is difficult to diagnose andthere is no effective treatment, it is still one ofthe most fatal tumors (14). The current treat-ment options are surgery, radiotherapy and che-motherapy. Combined treatment options areused when there is widespread metastasis withpoor prognosis, likely to be fatal within a fewmonths. The primary treatment is the surgicalremoval of the tumor. The surgical treatment forATC has changed from tracheostomy for palli-ative reasons to curative resection, if possible(17). Chemotherapy or radiotherapy is used fol-lowing surgical treatment. Pre- and postoperati-ve radiotherapy can also be used for cases sche-duled for surgery. There are many few patientswith long-term survivals and the mortality rateis reported as 70-95% (17). Sugino et al (13) ha-ve suggested adding radiotherapy to surgicaltreatment for control of local disease and founda much better prognosis for incidental ATC thanthe classical type even if incidental ATC fociare thought to be life-threatening. However, ot-her series have reported differences between theincidental type and the classical type and statedthat radiotherapy does not change 1-year survi-
57
Incidental anaplastic thyroid carcinoma: A case report

val or cumulative survival in ATC cases. Ojedaet al (21) reported a statistically favorable survi-val times in cases with focal ATC in a differen-tiated tumor or ATC limited to a single thyroidlobe in their 30-case series. The mean survivalperiod of 5 such cases was 24 months. Thisstudy emphasizes that the prognosis of ATC ac-companying a well-differentiated tumor is notdifferent from pure ATC but the prognosis isbetter when a single focus is present (21). Ourcase had ATC within a nodule limited to a sing-le lobe and survived for 1.5 years, consistentwith this study. In conclusion, a combination ofradiotherapy, chemotherapy and in resectablecases aggressive surgery may be beneficial untiltreatment options with proven efficacy are fo-und.
REFERENCES
1. Oktay MH, Smolkin MB, Williams M, Cajigas A. Me-tastatic anaplastic carcinoma of the thyroid mimickingsquamous cell carcinoma: report of a case of a challen-ging cytologic diagnosis. Acta Cytol 2006;50:201-204.
2. Are C, Shaha AR. Anaplastic thyroid carcinoma: bio-logy, pathogenesis, prognostic factors, and treatmentapproaches. Ann Surg Oncol 2006;13:453-464.
3. Kebebew E, Greenspan FS, Clark OH, Woeber KA,McMillan A. Anaplastic thyroid carcinoma. Treatmentoutcome and prognostic factors. Cancer 2005;103:1330-1335.
4. Lam KY, Lo CY, Chan KW, Wan KY. Insular andanaplastic carcinoma of the thyroid: a 45-year compa-rative study at a single institution and a review of thesignificance of p53 and p21. Ann Surg 2000;231:329-338.
5. Pierie JP, Muzikansky A, Gaz RD, Faquin WC, OttMJ. The effect of surgery and radiotherapy on outcomeof anaplastic thyroid carcinoma. Ann Surg Oncol2002;9:57-64.
6. Austin JR, el-Naggar AK, Goepfert H. Thyroid can-cers. II. Medullary, anaplastic, lymphoma, sarcoma,squamous cell. Otolaryngol Clin North Am 1996;29:611-627.
7. Venkatesh YS, Ordonez NG, Schultz PN, Hickey RC,Goepfert H, Samaan NA. Anaplastic carcinoma of thethyroid. A clinicopathologic study of 121 cases. Can-cer 1990;66:321-330.
8. Pasieka JL. Anaplastic thyroid cancer. Curr Opin On-col 2003;15:78-83.
9. Patel KN, Shaha AR. Poorly differentiated and anaplas-tic thyroid cancer. Cancer Control 2006;13:119-128.
10. Agrawal S, Rao RS, Parikh DM, Parikh HK, BorgesAM, Sampat MB. Histologic trends in thyroid cancer1969-1993: a clinico-pathologic analysis of the relati-ve proportion of anaplastic carcinoma of the thyroid. JSurg Oncol 1996;63:251-255.
11. Ibanez ML, Russell WO, Albores-Saavedra J, Lamper-tico P, White EC, Clark RL. Thyroid carcinoma biolo-gic behavior and mortality. Postmortem findings in 42cases, including 27 in which the disease was fatal. Can-cer 1966;19:1039-1052.
12. Lam AK, Lo CY, Lam KS. Papillary carcinoma ofthyroid: A 30-yr clinicopathological review of the his-tological variants. Endocr Pathol 2005;16:323-330.
13. Sugino K, Ito K, Mimura T, Nagahama M, Fukunari N,Kubo A, Iwasaki H, Ito K. The important role of ope-rations in the management of anaplastic thyroid carci-noma. Surgery 2002;131:245-248.
14. Gilliland FD, Hunt WC, Morris DM, Key CR. Prog-nostic factors for thyroid carcinoma. A population-ba-sed study of 15,698 cases from the Surveillance, Epi-demiology and End Results (SEER) Program 1973-1991. Cancer1997;79:564-573.
15. Nix PA, Nicolaides A, Coatesworth AP. Thyroid cancerreview 3: management of medullary and undifferentia-ted thyroid cancer. Int J Clin Pract 2006;60:80-84.
16. McIver B, Hay ID, Giuffrida DF, Dvorak CE, GrantCS, Thompson GB, et al. Anaplastic Thyroid Carcino-ma: 50 year experience at a single institution. Surgery2001;130:1028-1034.
17. Fortson JK, Durden FL Jr, Patel V, Darkeh A. The coe-xistence of anaplastic and papillary carcinomas of thethyroid: a case presentation and literature review. AmSurg 2004;70:1116-1119.
18. Silver RJ, Parangi S. Management of thyroid inciden-talomas. Surg Clin North Am 2004;84:907-919.
19. Nishiyama RH, Dunn EL, Thompson NW. Anaplasticspindle-cell and giant-cell tumors of the thyroid gland.Cancer 1972;30:113-127.
20. Nikiforova MN, Kimura ET, Gandhi M, BiddingerPW, Knauf JA, Basolo F, Nikiforov YE, et al. BRAFmutations in thyroid tumors are restricted to papillarycarcinomas and anaplastic or poorly differentiated car-cinomas arising from papillary carcinomas. J Clin En-docrinol Metab 2003;88:5399-5404.
21. Luis A. Pacheco-Ojeda, Ana L Martinez, Marcelo Al-verez. Anaplastic Thyroid carcinoma. Analysis ofprognostic factors. Int Surg 2001;86:117-121.
22. Demeter JG, De Jong SA, Lawrence AM, Paloyan E.Anaplastic thyroid carcinoma: risk factors and outco-me. Surgery 1991;110:956-961; discussion 961-963.
23. Stoler DL, Datta RV, Charles MA, Block AW, BrennerBM, Sieczka EM, et al. Genomic instability measure-ment in the diagnosis of thyroid neoplasms. Head Neck2002;24:290-295.
24. Sniezek JC, Holtel M. Rare tumors of the thyroidgland. Otolaryngol Clin North Am 2003;36:107-115.
25. Wallin G, Backdahl M, Tallroth Ekman E, Lundell G.Co-existent anaplastic and well differantiated thyroidcarcinomas: A nuclear DNA study. Eur J Surg Oncol1989;15:43-48.
26. Galer Davidson H, Bibbo M, Dytch HE, Gonzolez-Campore R, Fernandez A, Wied GL. Nuclear DNA inanaplastic thyroid carcinoma with a differentiatedcomponent. Histopathology 1987;11:715-722.
27. Giuffrida D, Gharib Gharib D. Anaplastic thyroid car-cinoma: current diagnosis and treatment. Ann Oncol2000;11:1083-1089.
58
Turkish Journal of Pathology 2008;24(1):54-58





![Paraneoplastic Syndromes Associated with Laryngeal Cancer...2019/03/03 · cinoma, anaplastic carcinoma, and others) [19]. Bazex’s acrokeratosis is the most frequent paraneoplastic](https://img.pdfslide.us/doc/110x75/609dc5af27661b477817a385/paraneoplastic-syndromes-associated-with-laryngeal-cancer-20190303-cinoma.jpg)