-
8/6/2019 sbo1- patho
1/11
SBO: PATHOLOGY ~~ CELLULAR INJURY AND CELL DEATH, CELL GROWTH
AND DIFFERENTIATION
***1. DESCRIBE THE PATHOGENIC MECHANISMS INVOLVED AND THE
PROTOTYPE EXAMPLES OF EACH OF THE FOLLOWING
TYPES OF NECROSISTYPE OF
NECROSISCOAGULATION
NECROSISLIQUEFACTION
NECROSISENZYMATIC FAT
NECROSISCASEOUS NECROSIS
GANGRENOUSNECROSIS
DESCRIPTION form of necrosis in
which thearchitecture of deadtissues is preservedfor a span of
at leastsome days
digestion of the dead
cells
focal areas of fat
destruction
caseous (cheeselike);
encountered most oftenin foci of tuberculousinfection
serious and potentially
life-threateningcondition that ariseswhen a considerablemass of
body tissuedies
CHARACTERISTIC
tissues exhibit a firmtexture
tissue into a liquidviscous mass; creamyyellow because of
thepresence of deadleukocytes (pus)
visible chalky-whiteareas (fatsaponification)Histologic
exam:form of foci of shadowyoutlines of necrotic fatcells, with
basophilic
calcium deposits,surrounded by aninflammatory reaction
friable white appearanceHistologic exam:collection of
fragmentedor lysed cells andamorphous granulardebris enclosed
within adistinctive inflammatory
border (granuloma)
affected areas turningblack and/or greenand/or
yellowishbrown
MECHANISM denatures not onlystructural proteins butalso enzymes
and soblocks the proteolysisof the dead cells; as aresult,
eosinophilic,anucleate cells maypersist
microbes stimulatethe accumulation ofleukocytes and
theliberation of enzymesfrom these cells
release of activatedpancreatic lipases intothe substance of
thepancreas and theperitoneal cavity(acute pancreatitis);pancreatic
enzymesleak out of acinar cellsand liquefy the
membranes of fat cellsin the peritoneum. Thereleased lipases
splitthe triglyceride esterscontained within fatcells. The fatty
acids,so derived, combinewith calcium.
a form of coagulativenecrosis, in that noliquefaction
hasoccurred, butmicroscopically theaffected tissue
appearscompletely structureless,under the microscopeand exhibits a
greater
than usual affinity foracidic dyes such as eosin
reduced blood supplyto the affected tissues,which resultsin cell
death
http://en.wikipedia.org/wiki/Cell_(biology)http://en.wikipedia.org/wiki/Cell_(biology)
-
8/6/2019 sbo1- patho
2/11
EXAMPLES
COAGULATIVE NECROSIS:Gross: Image of the heart fromthis case,
note the area of freshmyocardial infarction (arrows)in the anterior
portion of theleft ventricle and extending intothe anterior portion
of theinterventricular septum. Notethat the walls of the left
and
LIQUEFACTION NECROSIS:Gross: the cerebral infarction atthe upper
left heredemonstrates liquefactivenecrosis. Eventually, theremoval
of the dead tissueleaves behind a cavity.
Histology: Liquefactive necrosis(arrow). The necrotic
braintissue is
-
8/6/2019 sbo1- patho
3/11
ENZYMATIC FAT NECROSIS:Gross: a mesentery that has becomegorged
with necrotic fat; some relativelynormal white fat is visible and
necrotic fatin the middle of the mass
Histology: As with any necrotic condition,
inflammation will occur in fat necrosis,reflected by the large
numbers of
ENZYMATIC FAT NECROSIS:Gross: On closer inspection,
thegranulomas have areas of caseousnecrosis. This is very
extensivegranulomatous disease. This
pattern of multiple caseatinggranulomas primarily in the
upperlobes is most characteristic ofsecondary
(reactivation)tuberculosis. However, fungalgranulomas
(histoplasmosis,
GANGRENOUS NECROSIS:
Histology: intestinal gangrene:extensive necrosis of the
entireintestinal wall. HE stain.
Gross: Seen here is the lower legfrom a below the knee
amputation.The affected skin is dark red toblack and there is a
large area of
-
8/6/2019 sbo1- patho
4/11
2. GIVE THE 3 GROUPS OF CELLS BASED ON THEIR REGENERATIVE
CAPACITY, THE PROTOTYPE OF EACH AND THE CLINICALSIGNIFICANCE OF
EACH CATEGORY
a. Labile cells (continuously dividing cells)- continue to
multiply throughout life under normal physiologic conditions.Eg:
surface epithelial cells of epidermis, alimentary tract,
respiratory tract, urinary tract, vagina, cervix, uterine
endometrium,hematopoietic cells of bone marrow, cells of lymph
nodes and spleen
b. Stabile cells (quiescent cells)- decrease/lose their ability
to proliferate after adolescence but retain the capacity to
multiply inresponse to stimuli throughout adult life.Eg:
parenchymal cells of organs like liver, pancreas, kidneys, adrenal
and thyroid; mesenchymal cells like smooth muscle cells,
fibroblasts, vascular endothelium, bone and cartilage cellsc.
Permanent cells- lose their ability to proliferate around the time
of birth.Eg: neurons of nervous system, skeletal muscle and cardiac
muscle cells
3. DEFINE AND GIVE AT LEAST ONE ILLUSTRATIVE EXAMPLE OF EACH OF
THE FOLLOWING TYPES OF CELLULARADAPTATIONS OF GROWTH AND
DIFFERENTIATION
TYPE OFCELLULAR
ADAPTATION
ATROPHYHYPERTROP
HY
HYPERPLASIA
METAPLASIA DYSPLASIAPHYSIOLOGIC PATHOLOGIC
DESCRIPTION
decrease incell size
increase in cellsize
increase in the number of cells when a differentiated cellof a
certain type is
replaced by another celltype, which may be
lessdifferentiated
abnormalchanges in
cellularshape, size,and/ororganization
1. Compensatory
hyperplasia-permits tissueand organregeneration
Eg: epithelial cells ofthe epidermis and intestine, liver
hepatocytes, bone marrow cells,and fibroblasts
2. Hormonalhyperplasia-occurs mainly in
organs thatdependon estrogen
Eg: estrogen-dependentuterine cells undergohyperplasia
andhypertrophy followingpregnancy
abnormal increase in cell
divisionEg: endometriosis
http://en.wikipedia.org/wiki/Cellular_differentiationhttp://en.wikipedia.org/wiki/Cellular_differentiation
-
8/6/2019 sbo1- patho
5/11
EXAMPLES
ATROPHY:The atrophic glands have
scant cytoplasm and hyperchromatic
nuclei with occasional punctate
nucleoli. The basal cell layer is
fragmented but still present as
HYPERTROPHY: Myocardial CellHypertrophyCompare the nuclei of
these hugemyocardial cells to the little endothelialcell nuclei
that lie between them.Obviously these have more than 92chromosomes
(normal for a sedentaryperson's heart).Athletic hypertrophy is
good, but
-
8/6/2019 sbo1- patho
6/11
PHYSIOLOGIC HYPERPLASIA:Endometrial mucosa: normalendometrial
gland in theproliferative phase of themenstrual cycleRecall that
the proliferative phase ofthe cycle is an estrogen primed
event.
Estrogen is a growth promoter andcauses the endometrial
glandular cells
PATHOLOGIC HYPERPLASIA: Endometrial mucosa:pathologic
endometrial hyperplasia due to unopposedestrogen stimulationWhen
comparing this slide above, it is apparent that far moreglands are
present and they are crowded together. This occurs
when a woman has too much estrogen and not enoughprogesterone,
the latter a hormone that causes endometrialglands to undergo
atrophy. Examples of unopposed estrogeninclude a postmenopausal
woman who is taking estrogen withoutprogesterone to prevent
osteoporosis or an obese woman, who
METAPLASIA: SquamousMetaplasia
The physiologic, normal processwhereby columnar epithelium
maturesinto squamous epithelium. Squamousmetaplasia typically
occupies part ofthe transformation zone. At thesquamocolumnar
junction it appears asa "ghost white" or white-blue film withthe
application of acetic acid. It isusually sharply demarcated toward
the
-
8/6/2019 sbo1- patho
7/11
**1. ENUMERATE THE COMMON CAUSES OF CELL INJURY AND THE
MECHANISMS INVOLVED IN EACH
a. Depletion of ATP -> Na pump failure -> water enters
cell -> cells swellb. Mitochondrial damage -> can cause
apoptosisc. Influx of calcium and loss of calcium homeostasis
d. Accumulation of oxygen-derived free radicals (oxidative
stress)e. Defects in membrane permeability -> water enters cell
-> cell swells and even deathf. Damage to DNA -> DNA and RNA
changes (inherited/ acquired) -> if enzymes deficient ->
substrate accumulates -> cells
swellDamage to proteins -> enzymatic and structural proteins
are not synthesized -> cells swell
2. GIVE THE MOLECULAR MECHANISMS RESPONSIBLE FOR CELL INJURY
LEADING TO NECROSIS
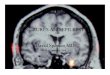
DYSPLASIA: Immunohistochemicallocalization of phospho-Akt
inhuman bronchial biopsiesSections from human bronchialbiopsies
were incubated withantibodies specific for thephosphorylated form
(ser473) of Akt,color developed with nickel-DAB(black) and
counterstained withnuclear fast red. Representative stains
-
8/6/2019 sbo1- patho
8/11
-
8/6/2019 sbo1- patho
9/11
3. DEFINITION OF TERMS:
a. NECROSIS- (from the Greek , "dead", , "death, the stage of
dying, the act of killing") is thepremature death of cells and
living tissue.
b. AUTOLYSIS- The term derives from the Greek words ("self") and
("splitting"). More commonly known as self-digestion,refers to the
destruction of a cell through the action of its own enzymes. It may
also refer to the digestion of an enzyme by anothermolecule of the
same enzyme.
c. HETEROLYSIS- If enzymatic digestion is accomplished by
enzymes derived from cells other than the dead or dying ones;
mayoccur as a result of endocytosis, in the course of which
phagocytes ingest portions of dead or dying cells and segregate
them intophagocytic vacuoles (phagosomes).
d. KARYOLYSIS-dissolution of the cell nucleus with loss of its
affinity for basicstains sometimes occurring normally but usually
in necrosis
e. PYKNOSIS-a degenerative condition of a cell nucleus marked by
clumping ofthe chromosomes, hyperchromatism, and shrinking of the
nucleus
f. KARYORRHEXIS-a degenerative cellular process involving
fragmentation of thenucleus and the breakup of the chromatin into
unstructured granules
INITIAL STIMULUS:
Interference with energy metabolism Glycolysis
modification of the function of the plasma membraneSIGNALLING
PATHWAYS:
mitochondrial respiration and oxidative phosphorylation are
rapidlyaffected (stimulates anaerobic glycolysis)
lack of ATP
rapid increase of Ca (activation of other signalling
mechanismsincluding kinases: early gene transcription; modify
cytoskeletal
-
8/6/2019 sbo1- patho
10/11
g. APOPTOSIS- also known as programmed cell death; the
elimination of unwanted cells with minimum disruption of the
surroundingtissue.
h. HYPOPLASIA- the failure of development of an organ to its
full mature sizei. APLASIA- the complete failure of development of
an organ, commonly seen in paired organs e.g. kidney, adrenal,
gonads.
j. AGENESIS- lack or failure of developmentk. ATRESIA- absence
or closure of a normal body orifice or tubular passage
*1. GIVE THE 3 BASIC MECHANISMS INVOLVED IN THE PATHOGENESIS OF
INTRACELLULAR ACCUMULATION OF THE 3
CATEGORIES OF STOCKPILED SUBSTANCES AND EXAMPLES OF EACH3
CATEGORIES OFSTOCKPILED SUBSTANCES
(1) a normal cellular constituentaccumulated in excess, suchas
water, lipids, proteins,and carbohydrates
(2) an abnormal substance,either exogenous, such as amineral or
products ofinfectiousagents, or endogenous, such asa product of
abnormal synthesisor metabolism
(3) a pigment, such as melanin,hemosiderin,
lipofuscin,bilirubin
GENERAL MECHANISMS disordered homeostasis: uptake from exogenous
source, endogenous synthesis,or breakdown or transport from
cell
insolubility of accumulated material in water
2. DESCRIBE THE MECHANISMS INVOLVED IN THE FOLLOWING SUBCELLULAR
ALTERATIONSa. LYSOSOMAL HETEROPHAGY AND AUTOPHAGY
i. Lysosomal heterophagy1. The cell takes up particles or
molecules by the process of endocytosis, engulfing them in
membrane-bounded vesicles or vacuoles that are
formed at the cell surface.
2. The endocytosed material enters lysosomes via intermediate
membrane-bounded compartments known as endosomes.3. In higher
animals, heterophagy is most prominently used by leukocytes and
macrophages. These specialized cells endocytose
invasive microorganisms and use endocytosis in clearing debris
and disposing of dead or senescent cells.
ii. Lysosomal autophagy1. Cells segregate regions of their own
cytoplasm within compartments that come to be bounded by single
membranes and to receive lysosomal
enzymes.
2. Autophagic lysosomes take part in the remodeling of cells as
part of the processes of development and during stressful
circumstances.
3. They also participate, along with nonlysosomal enzymes and
heterophagic lysosomes, in normal turnover of the body's
constituentsthebalanced synthesis and destruction through which
most molecules of most cells are replaced by new molecules.
b. HYPERTROPHY OF SMOOTH ENDOPLASMIC RETICULUM
i. Eg: an exogenous metabolic demand on the liver cell by
administering drugs that must be detoxified by the mixed-function
oxidase system.
1. Cytochrome P450 and other enzymes of this drug-metabolizing
system reside in the smooth endoplasmicreticulum. The liver cell
responds to the metabolic demand of detoxification by increasing
the amount of smoothendoplasmic reticulum, with consequent
hypertrophy of the cell.
c. MITOCHONDRIAL ALTERATIONSi. Causes:
1. increases of cytosolic Ca2+
2. reactive oxygen species
http://humpath.com/spip.php?article10268http://humpath.com/spip.php?article15000http://humpath.com/spip.php?article8585http://humpath.com/spip.php?article8585http://humpath.com/spip.php?article10268http://humpath.com/spip.php?article15000http://humpath.com/spip.php?article8585http://humpath.com/spip.php?article8585
-
8/6/2019 sbo1- patho
11/11
3. oxygen deprivation4. injurious stimuli, including hypoxia and
toxins5. mutation in mitochondrial genes
ii. Mechanisms:
1. formation of a high-conductance channel in the mitochondrial
membrane, called the mitochondrial permeabilitytransition pore
a. leads to the loss of mitochondrial membrane potential,
resulting in failure of oxidative phosphorylation andprogressive
depletion of ATP, culminating in necrosis of the cell.
2. sequester between their outer and inner membranes several
proteins that are capable of activating apoptoticpathwaysa. these
include cytochrome c and proteins that indirectly activate
apoptosis inducing enzymes called
caspases (leads to apoptosis ~~ remember embryology?? Hehehe ^_^
).
3. GIVE EXAMPLES OF ABNORMALITIES OF CYTOSKELETON AND MEMBRANE
SKELETON
a. Plasma membrane alterations: blebbing, blunting, loss of
microvillib. Mitochondrial changes: swelling , appearance of small
amorphous densitiesc. Endoplasmic reticulum: dilation, detachment
of polysomes, intracytoplasmic myelin figuresd. Nucleus:
disaggregation of granular and fibrillar elements
katemendoza2014summarized this from robbins and cotran 8th ed +
internet sources
read your books for more info ~1st tranx for 2nd yr....happy
studying! Sorry kng kulang ah, d ko kasi alam sagot dun..haha!!
kinig nlng tau lec nila doc tpos sulat nyo
nlng s free space ung tamang sagot.... ^_^