Embed Size (px)
Citation preview

Clinical pathology group assignment BY KULA JILO 2015
1 | P a g e
1. SEROLOGY
1.1 What does mean by serology?
Serology is the scientific study of serum and other bodily fluids. In practice, the term usually refers to
the diagnostic identification of antibodies in the serum. Such antibodies are typically formed in
response to an infection (against a given microorganism), against other foreign proteins (in response,
for example, to a mismatched blood transfusion), or to one's own proteins (in instances of
autoimmune disease).Serological tests may be performed for diagnostic purposes when an infection is
suspected, in rheumatic illnesses, and in many other situations, such as checking an individual's type.
Serology blood tests help to diagnose patients with certain immune deficiencies associated with the
lack of antibodies, such as X-linked gamma globulinemia. In such cases, tests for antibodies will be
consistently negative.
There are several serology techniques that can be used depending on the antibodies being
studied. These include:
ELISA
agglutination
precipitation
complement-fixation and
Fluorescent antibodies.
Some serological tests are not limited to blood serum, but can also be performed on other
bodily fluids such as semen and saliva, which have (roughly) similar properties to serum.
Serological tests may also be used forensically, specifically for a piece of evidence (e.g.,
linking a rapist to semen sample).
1.2 How can we get the sample of serum from the blood sample?
Blood is centrifuged to remove cellular components. Anti-coagulated blood yields plasma containing
fibrinogen and clotting factors. Coagulated blood (clotted blood) yields serum without fibrinogen,
although some clotting factors remain.

Clinical pathology group assignment BY KULA JILO 2015
2 | P a g e
1.3 For what types of tests we use serum samples? Please list all possible
test performed in the clinical laboratory used in the analysis of serum.
Don’t miss to specify the purpose (objectives) of each test
Any of several laboratory procedures carried out on a sample of blood serum, the clear liquid that
separates from the blood when it is allowed to clot. The purpose of such a test is to detect serum
antibodies or antibody-like substances that appear specifically in association with certain diseases.
The various types of serological tests include:
1) Flocculation tests:
The complement-fixation tests are the most common. They are based on the precipitation,
or flocculation, that takes place when antibody and specially prepared antigens are mixed
together.
2) Neutralization tests:
Depend on the capacity of antibody to neutralize the infectious properties of the
infectious organisms.
3) Hemagglutinin-inhibition tests:
Which make use of the finding that certain viruses will cause the red blood cells of certain
animal species to agglutinate (congeal, or clump together) and that this agglutination will be
prevented by antibody.
4) Enzyme linked immuono sorbent assay (ELISA)
Its objectives are:
To evaluate either the presence of antigen or the presence of antibody in a sample and
determining serum antibody concentrations.
ELISA test has a wide application in the detection of antigens and antibodies of different
diseases.
It is a helpful diagnostic tool to detect diseases and determining the presence of allergen in
food.
ELISA testing is a double antibody ―sandwich‖ immunoassay, which employs specific antibodies
against the disease to be tested: monoclonal antibody immobilized at the bottom of the microtiter
wells, and polyclonal antibodies coupled with horseradish peroxidase as the conjugate solution.
During the assay, existing antigens in the specimen will react with the antibodies to form an

Clinical pathology group assignment BY KULA JILO 2015
3 | P a g e
―antibody-antigen-antibody-HRP‖ immuno-complex. After the unbound material is washed off
during the assay procedure, substrate is applied to indicate the test result.
5) Immuno fluorescent antibody technique (IFAT):
To evaluate an immunofluorescence antibody test (IFAT) for diagnosis of
schistosomiasis in non-immune travellers and immigrants from endemic areas.
It used to detect serum antibodies and immune complexes in tissues and microorganisms
in specimens from patients with infectious diseases (IDFAT).
Utilizing a fluorochrome conjugated to an antibody, which is added directly to a tissue or
cell suspension for the detection of a specific antigen (DFAT) and
To examine tissue fluorescence microscope.
6) Radio immuno assay (RIA):
Immunoassay is the method of choice for measuring analyses normally present at very low
concentrations that cannot be determined accurately by other less expensive tests.
It uses for measurement of drugs, hormones, specific proteins, tumor markers and markers of
cardiac injury.
Qualitatively it used to detect antigens on infectious agents and antibodies that the body
produces to fight them. For example, immunoassays are used to detect antigens on
Hemophilus, Cryptococcus and Streptococcus organisms in the cerebrospinal fluid (CSF) of
meningitis patients.
To detect antigens associated with organisms that are difficult to culture, such as hepatitis B
virus and Chlamydia trichomatis.
7) Agglutination tests:
Determination of blood types or antibodies to blood group antigens and to assess bacterial
infections
Determination of blood types or antibodies to blood group antigens.
To assess bacterial infections. Example , typhoid fever
To detect the presence and relative amount of specific antibody in a patient’s serum.
8) Complement fixation tests (CFT):
Looking for evidence of infection tests for the presence of either specific antibody or specific
antigen in a patient's serum

Clinical pathology group assignment BY KULA JILO 2015
4 | P a g e
for the aid of diagnosis of infectious disease
9) Precipitation tests:
For the detection of immunoglobulin levels in the serum of a patient
10) Serum neutralization tests (SNT):
11) Toxin-antitoxin test:
12) Determination of the protective value of an ant serum in an animal:
2. HEMOCYTOMETER
2.1 What is hemocytometer?
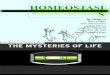
Hemocytometer is a device used to count cells. It was originally designed for the counting of
blood cells. It consists of a thick glass microscope slide with a rectangular indentation that
creates a chamber. This chamber is engraved with a laser-etched grid of perpendicular lines. The
device is carefully crafted so that the area bounded by the lines is known, and the depth of the
chamber is also known. It is therefore possible to count the number of cells or particles in a
specific volume of fluid, and thereby calculate the concentration of cells in the fluid overall.
To use the hemocytometer, first make sure that the special coverslip provided with the counting
chamber is properly positioned on the surface of the counting chamber. When the two glass
surfaces are in proper contact Newton's rings can be observed. If so, the cell suspension is
applied to the edge of the coverslip to be sucked into the void by capillary action which
completely fills the chamber with the sample. The number of cells in the chamber can be
determined by direct counting using a microscope, and visually distinguishable cells can be
differentially counted. The number of cells in the chamber is used to calculate the concentration
or density of the cells in the mixture the sample comes from. It is the number of cells in the
chamber divided by the chamber's volume, which is known from the start, taking account of any
dilutions and counting shortcuts:

Clinical pathology group assignment BY KULA JILO 2015
5 | P a g e
Fig.1. parts of hemocytometer
2.2 How many squares does hemocytometer have? Whether the squares
are used for counting or not? Consider the size.
hemocytometer is composed of nine equally sized bigger squares. The central one is different
from the other ones because it is divided into 25 smaller squares, while the ones in the
corners are divided into 16 smaller squares. The rest of squares are not used. In addition, the
smaller squares inside the central square are subdivided into 16 even smaller squares each.
This allows counting very tiny cells with the same precision level as larger ones (but with a
higher magnification).
Dimensions
Area
Volume at 0.1 mm depth
1 x 1 mm 1 mm2 100 nL
0.25 x 0.25 mm 0.0625 mm2 6.25 nL
0.25 x 0.20 mm 0.05 mm2 5 nL
0.20 x 0.20 mm 0.04 mm2 4 nL
0.05 x 0.05 mm 0.0025 mm2 0.25 nL
Table.1 dimension, areas and volume of hemocytometer.
The proportion of the cells counted applies if not all inner squares within a set square are
counted (i.e., if only 4 out of the 20 in a corner square are counted, then this term will equal
0.2).The parts of the hemocytometer (as viewed from the side) are identified. For most

Clinical pathology group assignment BY KULA JILO 2015
6 | P a g e
applications, the four large corner squares are only used. The cells that are on or touching the
top and left lines are counted, but the ones on or touching the right or bottom lines are
ignored.
2.3 How many squares used for RBC in one hemocytometer?
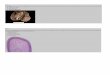
The central square, each of the 25 smaller squares will be 1 mm/5 = 0.2 mm in width and 0.2
mm x 0.2 mm = 0.04 mm2 in area (or 1 mm 2/25 = 0.04 mm2). In turn, each of the 25
smaller squares contains 16 even smaller squares which measure: 0.2 mm/4 = 0.05 mm in
width and 0.05 mm x 0.05 mm = 0.0025 mm2 = 2500 μm2 (or 0.04 mm2/16 = 0.0025 mm2).
Cells that are 10 μm or smaller should be counted in the central square – sometimes even in
one of the smaller squares inside the central square. Typically you would count red blood
cells, platelets, most types of yeast, and sperm cells.
Fig.2 centeral squares used to count RBC.
2.4 How many squares used for WBC counting in one hemocytometer?
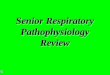
The four corner squares are further divided into sixteen smaller squares and are used for
WBC counting. Four corner squares are meant for WBC counting. Total = 64 small squares
Counting procedures of WBCs on hemacytometers Count cells starting in the upper the left
top large corner square. Move to the upper right corner square, bottom right corner square,
and end in the bottom left corner square. Count cells touching the left and top side lines.
Count all cells that touch any of the right and bottom lines, do not count any cell that touches
the upper and left boundary lines.

Clinical pathology group assignment BY KULA JILO 2015
7 | P a g e
Each of the 16 smaller squares will be 1 mm/4 = 0.25 mm in width and 0.25 mm x 0.25 mm
= 0.0625 mm2 in area (or 1 mm2/16 = 0.0625 mm2). Therefore, cells that are 10 μm or more
should be counted in these corner squares (although it doesn’t hurt if you also include a count
from the central square). For example, white blood cells (leukocytes).
Fig.3 corner squares (labeled by ―W‖ used for WBC count.
2.5 Why not those squares used for WBC counting is also used for RBC
counting and vice versa?
White blood cells: because they’re bigger, we are going to count those in the four corner
squares. We should establish a rule for the cells that are touching the peripheral lines: we can
count the ones touching the top and left and skip the ones on the bottom and right, or any
other combinations of two consecutive lines that we want. We have to note down our counts
(discriminating between live and dead if we added a dye).
Red blood cells: zoom into the central square, where smaller squares have been drawn. Count
the cells in the four small corner squares and the small central square, and do as with the
counts of the WBC
3. DIFFERENTIAL CELL COUNTING
3.1Define differential cell counting
A blood differential test, also called a white blood cell count differential, measures the
number of each of the five types of white blood cells present in blood. The blood differential
test measures the percentage of each type of white blood cell (WBC) in blood. It also reveals

Clinical pathology group assignment BY KULA JILO 2015
8 | P a g e
if there are any abnormal or immature cells and can diagnose an infection, inflammation,
leukemia, or an immune system disorder. It helps to tell the difference between various types
of white blood cells. Five types of white blood cells, also called leukocytes, normally appear
in the blood: Neutrophils, Lymphocytes (B cells and T cells), Monocytes, eosinophil and
Basophils.
3.2 Which test is used for differential cell counting?
It helps reveal abnormal white blood cell populations (e.g., blasts, immature granulocytes, or
circulating lymphoma cells in the differential totals the number of each type and determines
if the cells are present in normal proportion to one another, if one cell type is increased or
decreased, or if immature cells are present. This information is useful in helping to diagnose
the specific cause of an illness, such as:
Infections caused by bacteria, viruses, fungi or parasites
Inflammation
Allergies, asthma
Immune disorders (e.g., autoimmune disorders, immune deficiency)
Leukemia (e.g., chronic myeloid leukemia, chronic lymphocytic leukemia)
Myelodysplastic syndrome
Myeloproliferative neoplasms (e.g., myelofibrosis) the peripheral blood).
Some diseases trigger a response by the immune system that causes an increase in certain
types of WBCs. A differential may give clues to the specific cause of that immune response.
For example, it may help determine whether an infection is caused by bacteria or by viruses.
Other conditions affect the production of certain WBCs by the bone marrow or their survival
in the circulation, resulting in either an increase or decrease in their number. A differential
informs the healthcare provider as to which type of WBC is low or high. An abnormal
differential result may be followed by other tests such as a blood smear, bone marrow biopsy,
chromosome analysis, or immunopheno typing (e.g., flow cytometry). These tests can reveal
the presence of abnormal and/or immature populations of WBCs.

Clinical pathology group assignment BY KULA JILO 2015
9 | P a g e
Type of WBC
Abbreviations
Examples of causes of
a high count
Examples of causes
of a low count
Neutrophils
(Absolute neutrophil
count, percent
neutrophils)
Neu, Polys, PMNs,
ANC, % Neu
Known as
neutrophilia
Acute bacterial
infections and also
some infections
caused by viruses and
fungi
Inflammation (e.g.,
inflammatory bowel
disease, rheumatoid
arthritis)
Tissue death
(necrosis) caused by
trauma, major
surgery, heart attack,
burns
Physiological
(stress, rigorous
exercise)
Pregnancy—last
trimester or during
labor
Chronic leukemia
(e.g., myelogenous
leukemia
Known as
neutropenia
Myelodysplastic
syndrome
Severe,
overwhelming
infection (e.g.,
sepsis--neutrophils
are used up)
Reaction to drugs
(e.g., penicillin,
ibuprofen, phenytoin,
etc.)
Autoimmune
disorder
Chemotherapy
Cancer that
spreads to the bone
marrow
Aplastic anemia
Lymphocytes
(Absolute
Lymphs, lym, ly,
ALC, % lymphs
Known as
lymphocytosis
Known as
lymphopenia or

Clinical pathology group assignment BY KULA JILO 2015
10 | P a g e
lymphocyte count,
percent lymphocytes
Acute viral
infections (e.g.,
hepatitis, chicken
pox, cytomegalovirus
(CMV), Epstein-Barr
virus (EBV), herpes,
rubella)
Certain bacterial
infections (e.g.,
pertussis (whooping
cough), tuberculosis
(TB))
Lymphocytic
leukemia
Lymphoma
lymphocytopenia
Autoimmune
disorders (e.g., lupus,
rheumatoid arthritis)
Infections (e.g.,
HIV, TB, hepatitis,
influenza)
Bone marrow
damage (e.g.,
chemotherapy,
radiation therapy)
Immune
deficiency
Eosinophils
(Absolute eosinophil
count, percent
eosinophils)
Eos, AEC, % eos Known as
eosinophilia
Asthma, allergies
such as hay fever
Drug reactions
Inflammation of
the skin (e.g., eczema,
dermatitis)
Parasitic infections
Inflammatory
disorders (e.g., celiac
disease, inflammatory
bowel disease)
Certain
Known as
eosinopenia
This is often difficult
to determine because
numbers are
normally low in the
blood. One or an
occasional low
number is usually not
medically significant

Clinical pathology group assignment BY KULA JILO 2015
11 | P a g e
malignancies/cancers
Hypereosinophilic
myeloid neoplasms
Basophils (Absolute
basophil count,
percent basophils
Baso, ABC, % baso Known as basophilia
Rare allergic
reactions (e.g., hives,
food allergy)
Inflammation
(rheumatoid arthritis,
ulcerative colitis)
Some leukemias
(e.g., chronic myeloid
leukemia
Known as basopenia
As with eosinophils,
numbers are
normally low in the
blood; usually not
medically significant
Table.2 Possible Causes of High and Low WBC Differential Results
3.3 Why differential cell count is preferred than total white blood cell
count?
A white blood cell (WBC) count determines the concentration of white blood cells in the
patient's blood. A differential determines the percentage of each of the five types of mature
white blood cells. The white blood cell differential is often used as part of a complete blood
count (CBC) as a general health check. It may be used to help diagnose the cause of a high or
low white blood cell (WBC) count, as determined with a CBC. It may also be used to help
diagnose and/or monitor other diseases and conditions that affect one or more different types
of WBCs.
4. WHY THE SHAPE OF RBC IS BICONCAVE? EXPLAIN BRIEFLY.
Because their biconcave shape gives blood cell a larger surface area which increases the
ability to absorb oxygen. They are tiny and flexible; therefore they can squeeze through the
narrowest of blood capillaries to deliver oxygen. Red blood cells or Erythrocytes are

Clinical pathology group assignment BY KULA JILO 2015
12 | P a g e
biconcave because they do not contain nucleus. They are a-nucleated. This provides the cell
to attain large surface area to accommodate and maximum space for hemoglobin. And also
use for the subsequent accumulation of non-coding DNA in the genome. Efficient gas
transport requires erythrocytes to pass through very narrow capillaries, and this constrains
their size. In the absence of nuclear elimination, the accumulation of repeat sequences is
constrained by the volume occupied by the nucleus, which increases with genome size.
Generally Red blood cells, or erythrocytes, are biconcave for two reasons.
First, erythrocytes have no nucleus or internal membranes.
Second, erythrocytes have an unusual cytoskeleton.