Embed Size (px)
Citation preview
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 1/54
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 2/54
2340 ( 4350)
(.)
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 3/54
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 4/54
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 5/54
This video is intended for Doctors ONLYفق
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 6/54
Here are some tips before you start
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 7/54
Tips
• RVP is very useful and very serious.• If you are careful enough, it will become a piece of cake with
time!• In the first few RVPs, an anesthetist should be around (they
know it better).• Practice being talkative and funny. It is necessary to help the
patient overcoming the pain associated with RVP.• In the first RVPs select your patient carefully.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 8/54
TipsThis is the ideal patient for a beginner doctor:
• A young patient, but not very young (e.g. 40s but not 20s)• A patient who is generally fit (no cardiac, pulmonary or serious
systemic disorders).• A patient who has a very serious local foot problem, preferably
one who has been advised to have below or above kneeamputation. These patients tolerate pain of RVP much betterthan others because they have a stronger motivation.
• A patient who has severe pain in the foot (ischemic orneuropathic) as these patients will have better complicanceafter the pain is abolished by RVP.
• A patient who has a stronger family support, as these patientswill have better overall results.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 9/54
What does “RVP” stand for?
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 10/54
RVP = Retrograde Venous Perfusion
It is a therapeutic method where aperipheral vein is used to provide the limb
with necessary medications instead of the
Artery.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 11/54
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 12/54
Eighty years later (1988), it was re-discovered as apotential therapy for foot disorders by Ferreira fromBrasil.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 13/54
Many doctors around the world used RVP forfoot problems (infection, ischemia, ulcers ..etc).
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 14/54
In 1997 Dr Sarky presented his results of RVP in “International Surgery”, the official journal of the “International College of Surgeons”.
Since then, Dr Sarky became the world’s leaderin this technique.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 15/54
What are the scientificbasis for RVP?
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 16/54
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 17/54
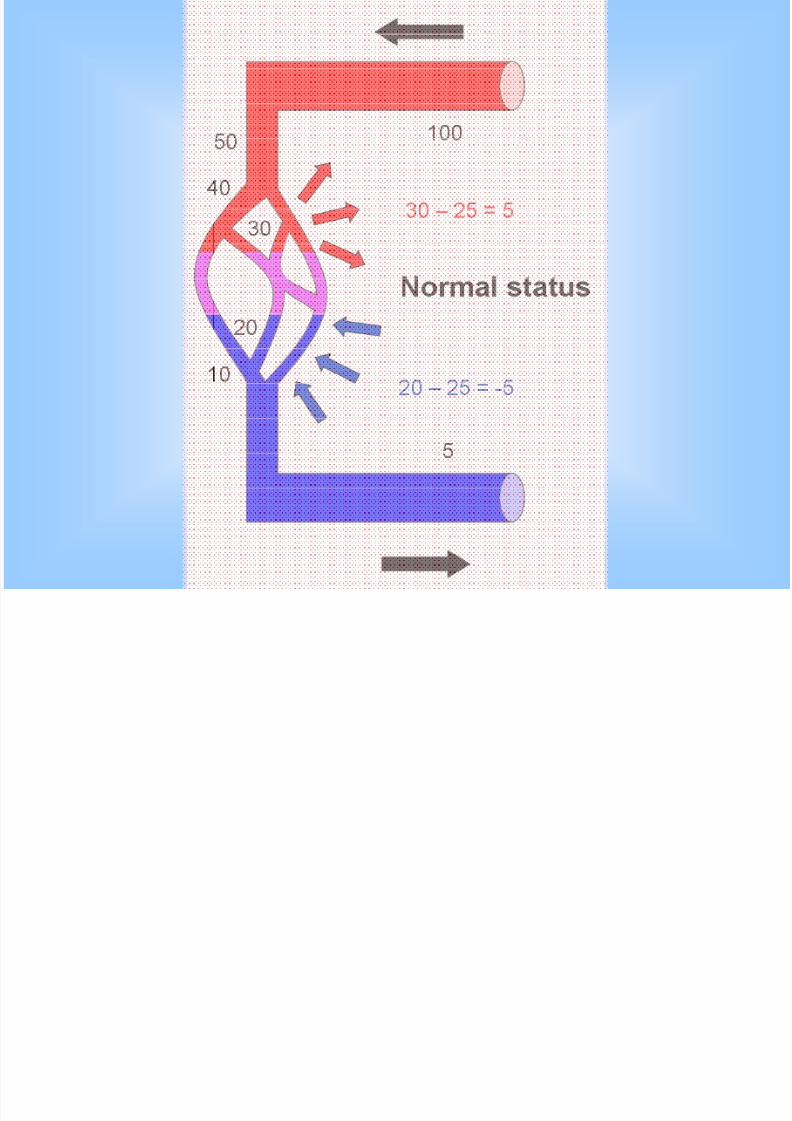
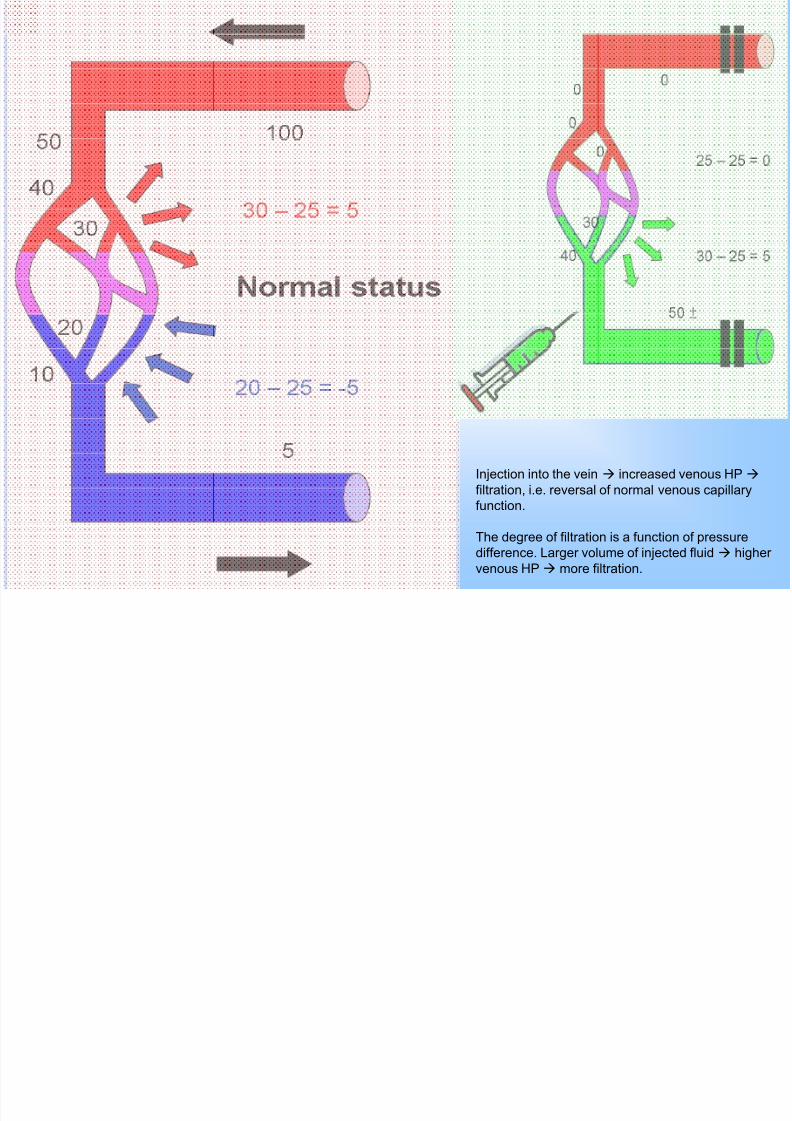
Injection into the vein increased venous HP
filtration, i.e. reversal of normal venous capillary
function.
The degree of filtration is a function of pressure
difference. Larger volume of injected fluid higher venous HP more filtration.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 18/54
Is RVP really effective?
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 19/54
RVP results in high tissue concentration
of administered drugs.
Tissue concentration of 99 mTc labelled human
serum albumin after RVP was:
. 3 times higher than after intra-arterial
. 7 times higher than after systemic i.v. injection
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 20/54
When is RVP a must?
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 21/54
• Severe acute infections – Diffuse, with no definite localization.
– Anerobic.
– Intense necrotizing reactions or secondary gangrene.
• Critical limb ischemia– Only for occlusions below the knee
– Only when surgical intervention is not feasible• Long, tight occlusions with no distal run-offs
• Refusal of the patient.
• Complicated peripheral neuropathyWhen medical treatments gives no effects.
– Recurrent ulcers.
– Severe intolerable pain.
– Charcot disease.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 22/54
When is RVP considered
as an adjunctive therapy?

7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 23/54
• Complementary to surgery for allother conditions that require surgicalintervention.
• Chronic non-healing wounds andulcers.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 24/54
When is RVP better avoided?
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 25/54
• Severe systemic disorders
– Advanced cardio-pulmonary disease.– Multiple organ-system failure.
• Psychological or emotional instability
• Rapidly progressive local disordersWhen RVP is not associated with rapid control of disease
threat of patient’s life (here amputation is a must).
– Expanding gangrene
– Infection extending to or above the knee.
– medical treatments gives no effects.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 26/54
What is the value of RVP?
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 27/54
85% of amputations for diabetic foot are avoidable
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 28/54
Direct access to sick tissues
RVP bypasses blocked arteries and delivers medications intotarget tissues despite the blocked arterial system. Patients withPAD benefit the least from medications because diseased limbgets the least amounts of the drugs.
RVP also focuses drugs into lesions more than 3 times betterthan neighboring tissues of the limb. This is due to the “rinsingeffect”.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 29/54
Beating the time factor
RVP allows a superdose (very high concentrations) of drugs intarget tissues over a very short time dramatic effects(infection control, ischemia combating, healing of wounds etc).
The rapid effect versus time • Preventing continuous damage by pathology.• Avoiding patient’s non-compliance or negligence.• Avoiding side-effects of long-term use of medications.• Reduction in costs.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 30/54
Avoiding systemic effects of drugs
RVP avoids systemic side-effects and toxicity of some of theused drugs by focusing them into target tissues. Also, when thedrug is expensive, it is not wasted on healthy organs.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 31/54
How can I do RVP?
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 32/54
Requirements
1) One doctor, aware of the procedure.2) Two trained assistants.
• One for observing cuff pressure and control timing.• One for assisting in simultaneous intervention.
3) Room, wide and equipped.4) Bed, better designed for elevation of foot side.5) Special cuffs: long, wide, double inflated parts.6) Blood pressure device.7) Blood sugar meter.8) Tourniquet.
9) Syringes (10 and 20 cc).10) Canulas (22, 24).
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 33/54
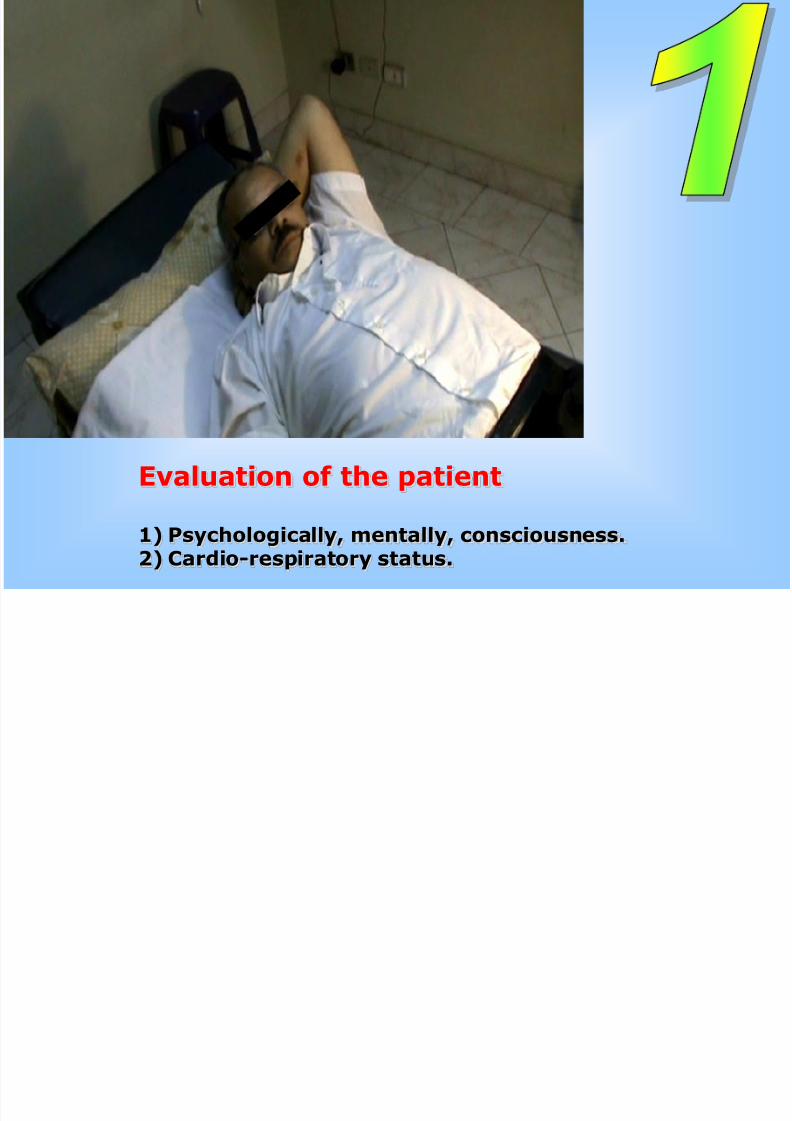
Evaluation of the patient
1) Psychologically, mentally, consciousness.
2) Cardio-respiratory status.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 34/54
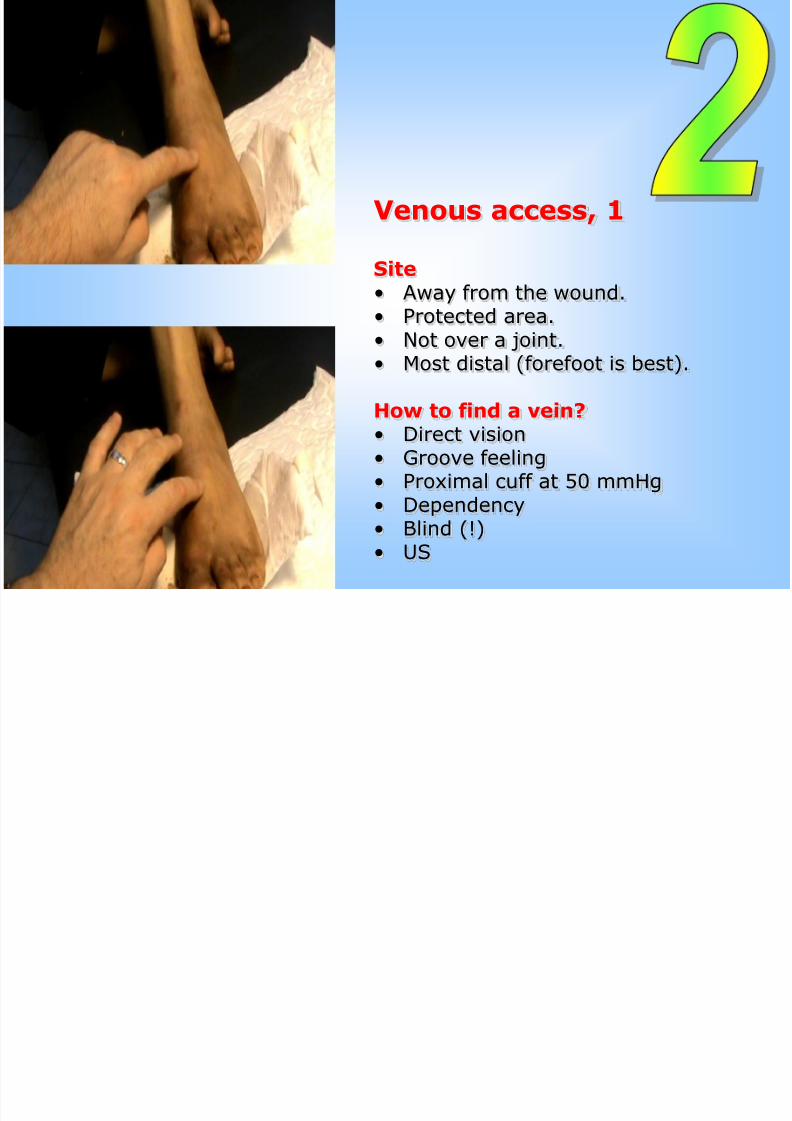
Venous access, 1
Site• Away from the wound.• Protected area.• Not over a joint.• Most distal (forefoot is best).
How to find a vein?• Direct vision• Groove feeling• Proximal cuff at 50 mmHg• Dependency• Blind (!)
• US
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 35/54
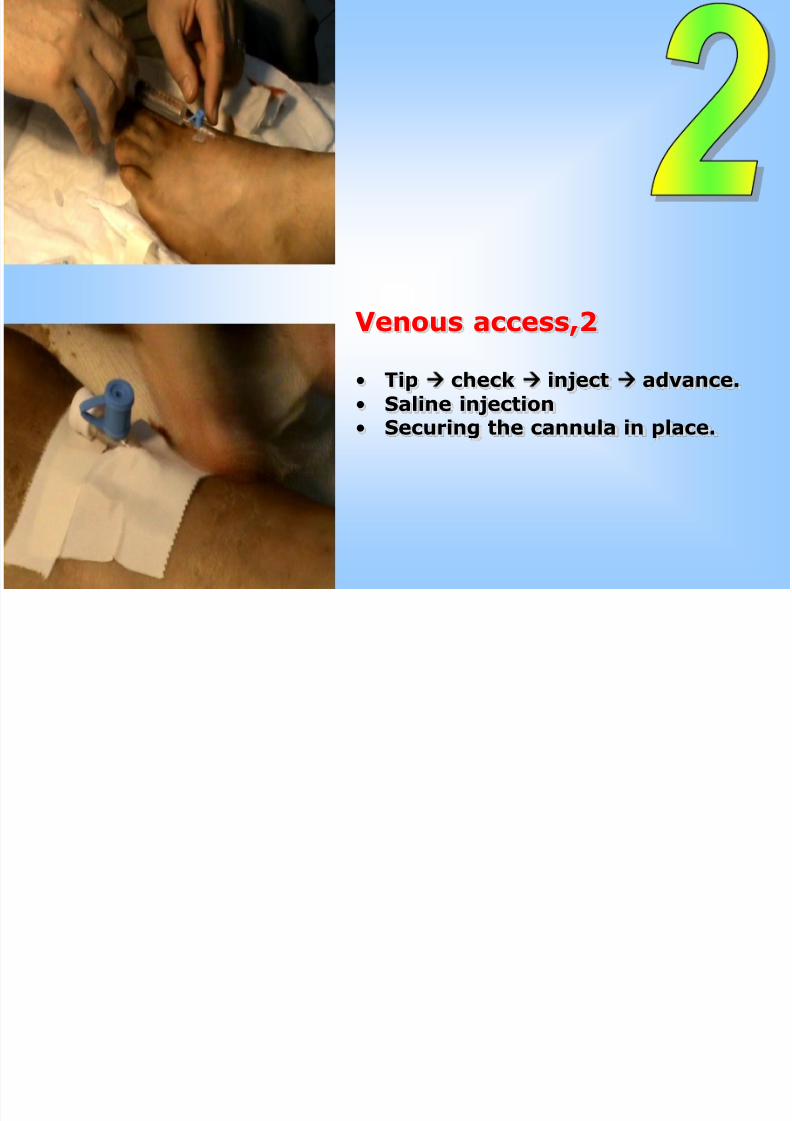
Venous access,2
• Tip check inject advance.
• Saline injection• Securing the cannula in place.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 36/54
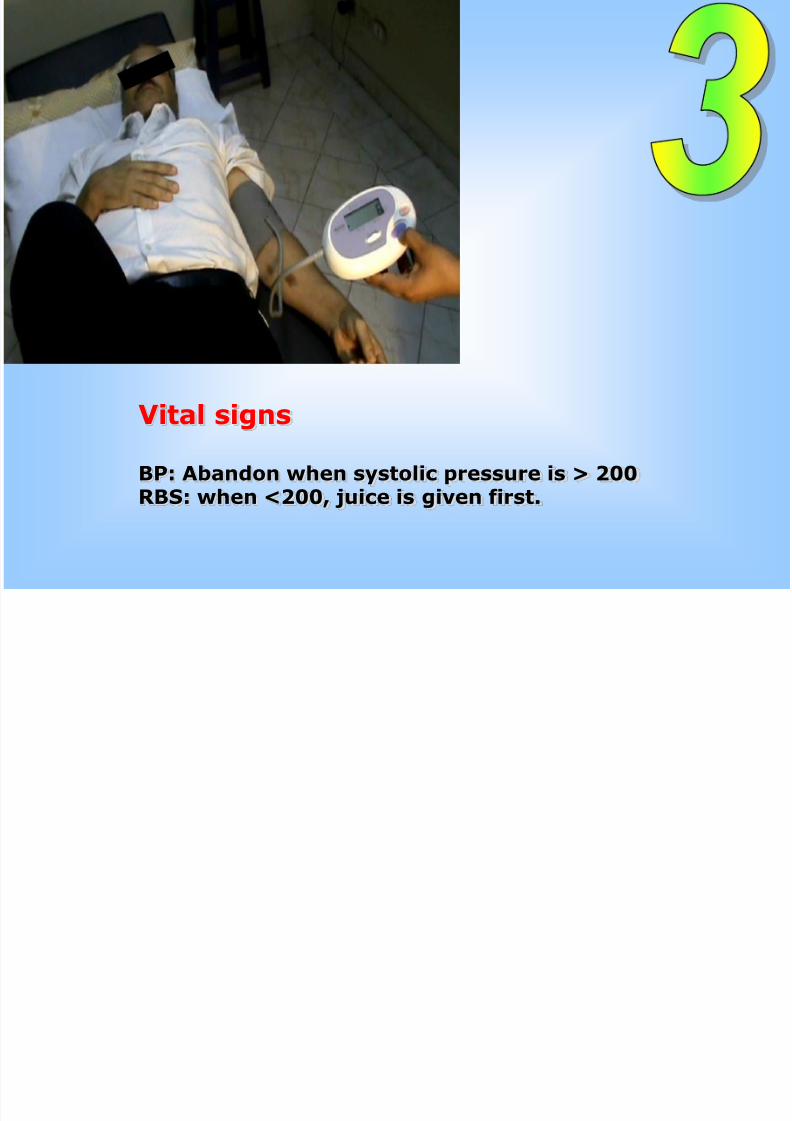
Vital signs
BP: Abandon when systolic pressure is > 200RBS: when <200, juice is given first.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 37/54
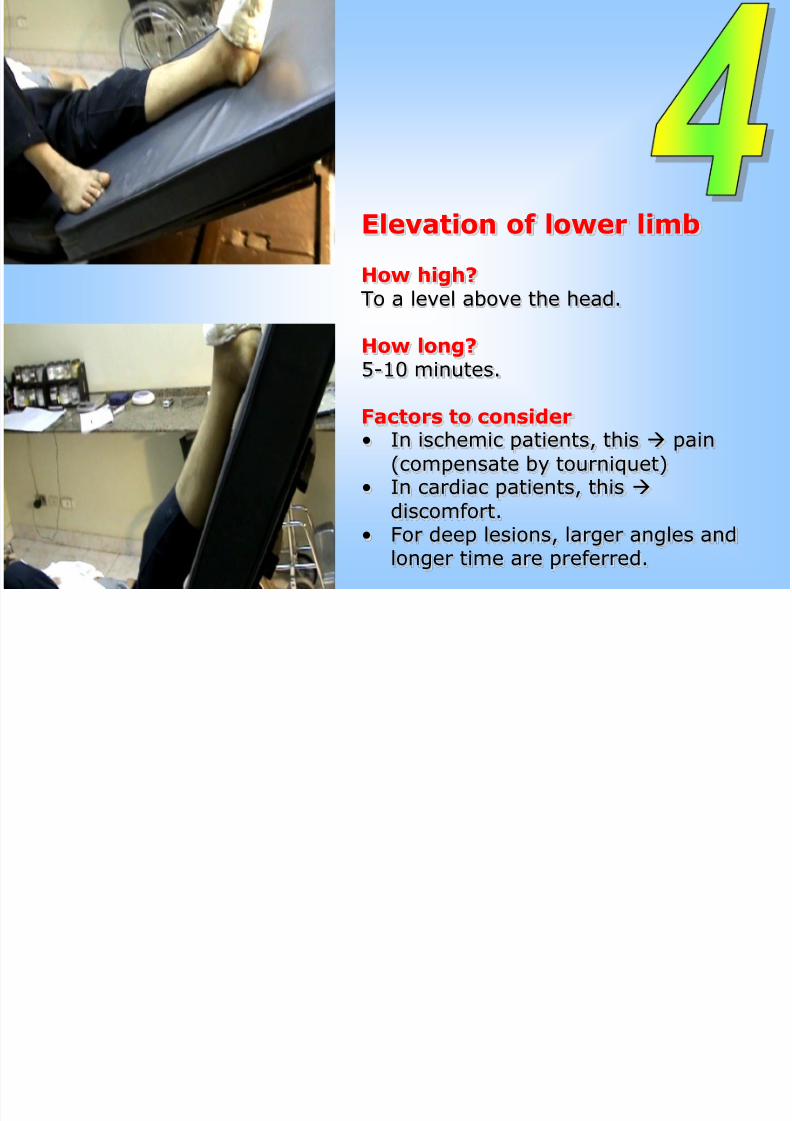
Elevation of lower limb
How high?To a level above the head.
How long?5-10 minutes.
Factors to consider• In ischemic patients, this pain
(compensate by tourniquet)• In cardiac patients, this
discomfort.• For deep lesions, larger angles and
longer time are preferred.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 38/54
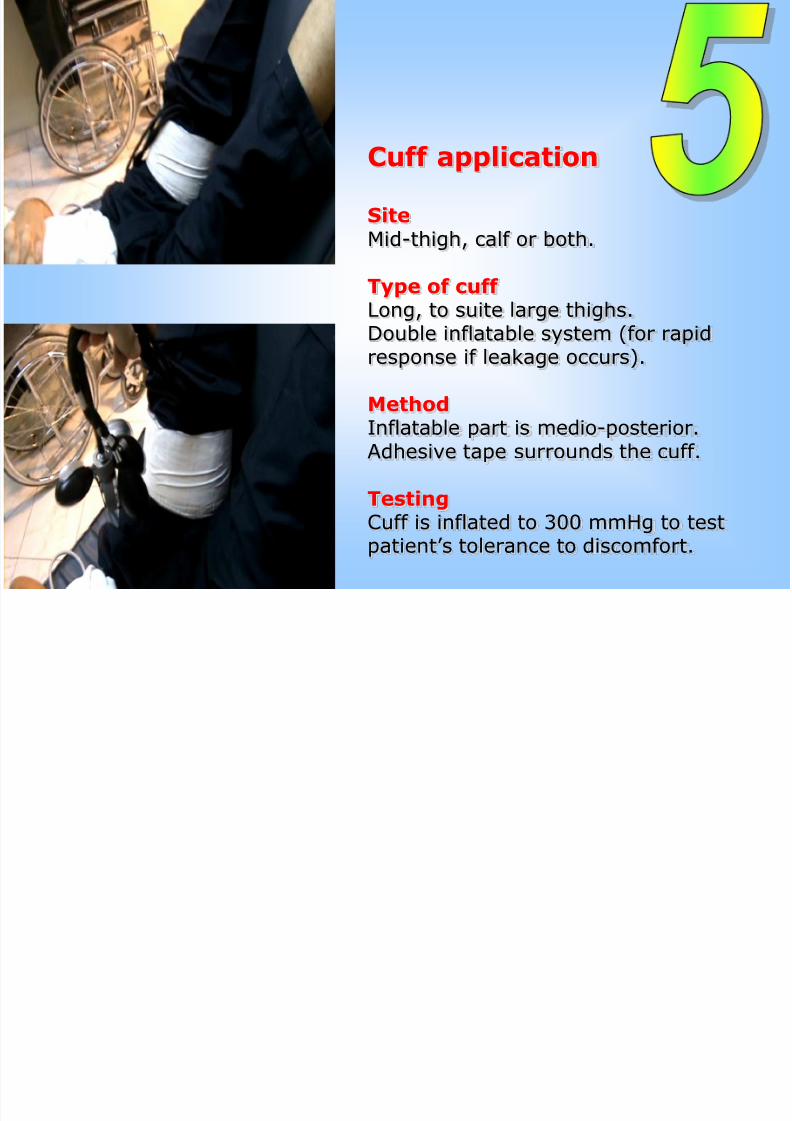
Cuff application
SiteMid-thigh, calf or both.
Type of cuff Long, to suite large thighs.Double inflatable system (for rapidresponse if leakage occurs).
Method
Inflatable part is medio-posterior.Adhesive tape surrounds the cuff.
TestingCuff is inflated to 300 mmHg to testpatient’s tolerance to discomfort.

7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 39/54
Preparing Injected fluids
Amount120-260 cc saline, depending on:• Size and age of the patient.• Cardiovascular status.• Syringe back-flow during injection.
• Number of drugs used (the more the more).
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 40/54
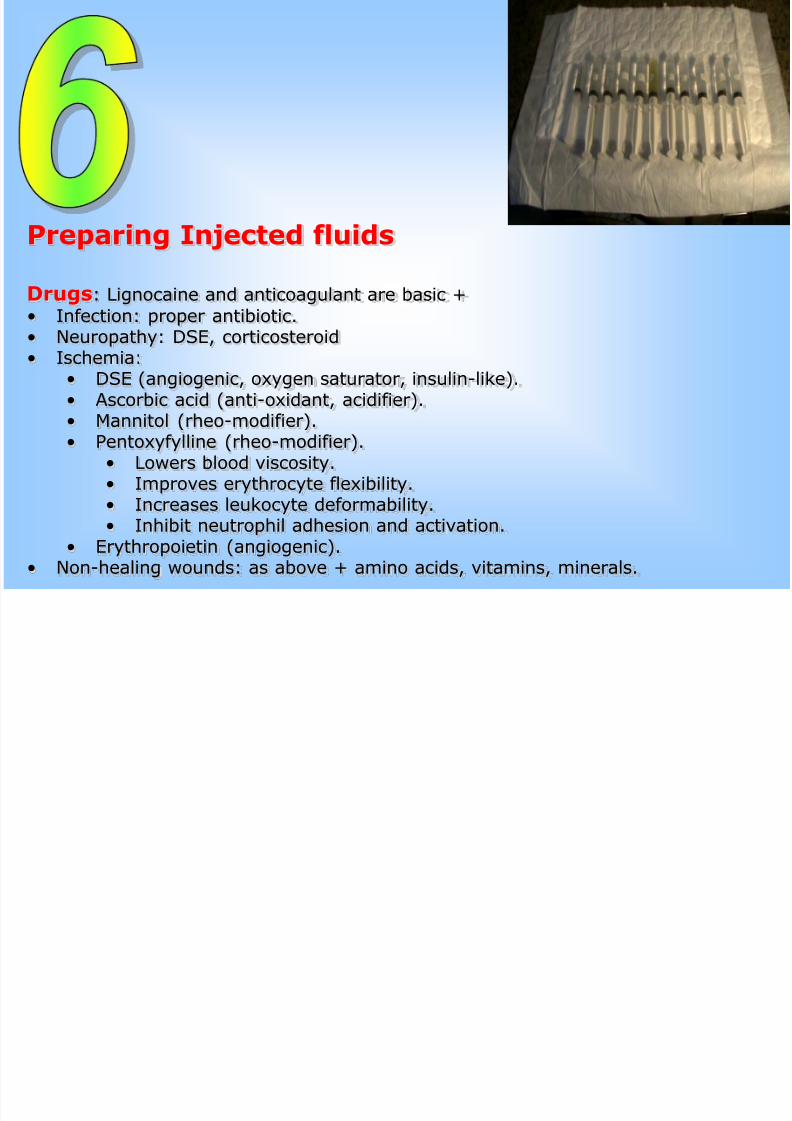
Preparing Injected fluids
Drugs: Lignocaine and anticoagulant are basic +
• Infection: proper antibiotic.• Neuropathy: DSE, corticosteroid• Ischemia:
• DSE (angiogenic, oxygen saturator, insulin-like).• Ascorbic acid (anti-oxidant, acidifier).
• Mannitol (rheo-modifier).• Pentoxyfylline (rheo-modifier).
• Lowers blood viscosity.• Improves erythrocyte flexibility.• Increases leukocyte deformability.• Inhibit neutrophil adhesion and activation.
• Erythropoietin (angiogenic).• Non-healing wounds: as above + amino acids, vitamins, minerals.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 41/54
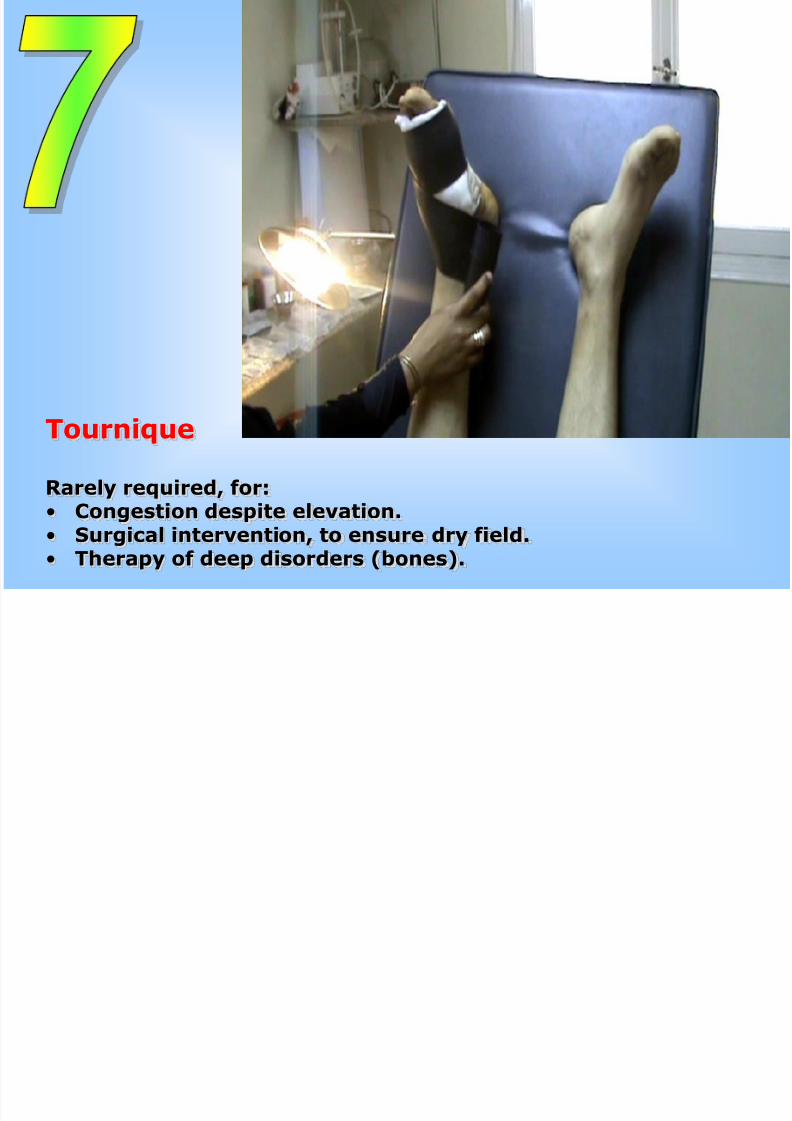
Tournique
Rarely required, for:• Congestion despite elevation.• Surgical intervention, to ensure dry field.
• Therapy of deep disorders (bones).
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 42/54
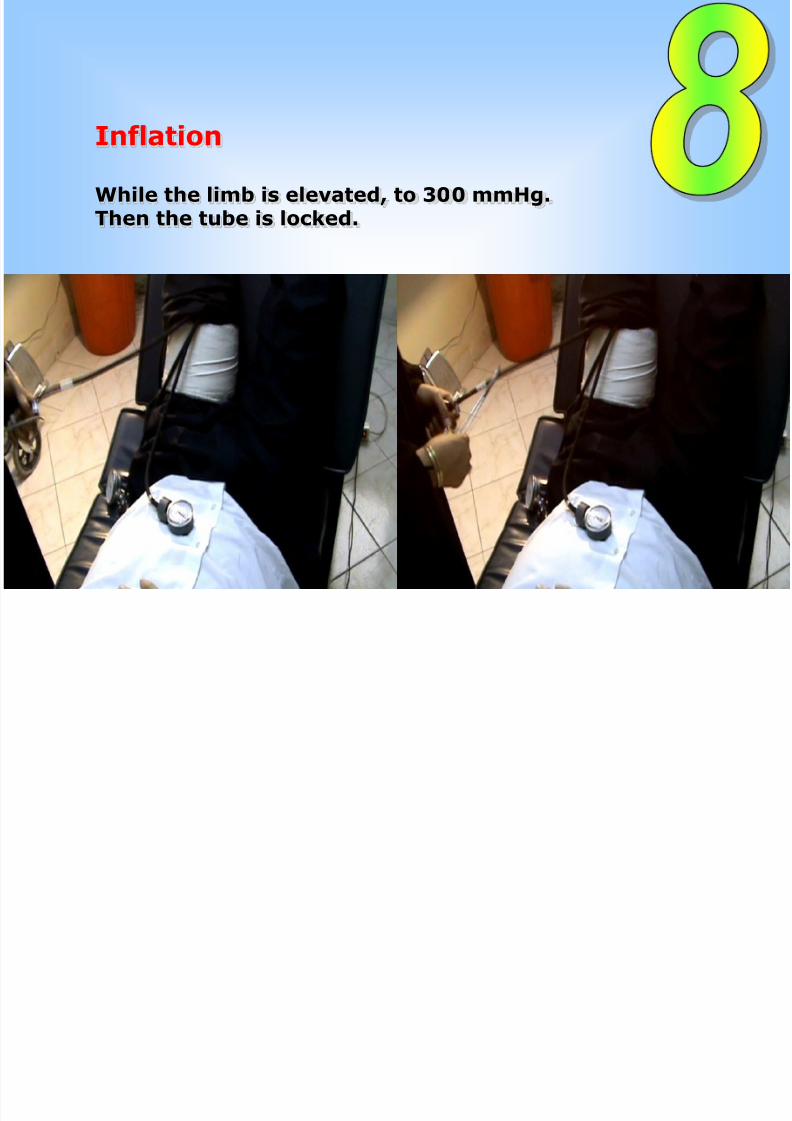
Inflation
While the limb is elevated, to 300 mmHg.Then the tube is locked.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 43/54
Lowering the limb

7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 44/54
Injection
Order• Start with Lignocaine• Alternate others• End with heparin.
SpeedThe higher the risk, the slower the speed.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 45/54
Observation
• Vital signs q 5 minutes
• Degree of consciousness• Attitude• Talking with the patient to pick any deterioration rapidly.• Tolerance to cuff pressure.• Symptoms of lignocaine toxicity: cirumoral numbness
and tingling, tinnitus, chest oppression ..
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 46/54
Manipulation
Surgical intervention or wound dressingis done as planned.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 47/54
Deflation
After a minimum of 25 minutes and a maximum of 60
minutes (longer durations are better avoided).
Preceded by a final measuring of vital signs.
Pressure is released very slowly, particularly in the
subdiastolic range of pressure.
When surgery is associated, release is made a bit faster inthe subdiastolic range to avoid excessive bleeding, nulessthis constitutes a risk to the patient.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 48/54
Post-procedural Observation
Duration30 minutes after RVP.120 minutes, when surgery is associated.
ParametersThe same as observation during the procedure + watching for
bleeding from the wound.
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 49/54
How many times will RVP be required?
General rule
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 50/54
RVP is repeated daily until the target is reached, e.g.• Infection: clinical evidence of control of infection
• No more fever.• Less or no pain.• No clinical manifestations of sepsis (malaise, disturbed consciousness).• No septic discharge of the wound.
• No foul smell in anerobic infection.• No progressive sloughing of tissues.• No extension of infection proximally.
• Ischemia: clinical evidence of improved arterial perfusion to the level of safety• No extension of gangrene after testing surgical intervention.• Appearance of line of demarcation.
• Appearance of granulation tissue.• Less sloughing.• Less pain.• Hyperemic wound.• Bleeding surfaces.• Improved capillary circulation of skin.• Spontaneous separation of sloughed parts.
• Neuropathy
• Restored sensations.• Better ability to walk and ascend the stairs.• Less pain to tolerability level.
Estimated number of sessions• Infection: 3-5
• Ischemia: 10-15• Neuropathy: 5-7
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 51/54
Can I be a diabetic foot doctorwithout practicing RVP?
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 52/54

7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 53/54
7/28/2019 Sarky - RVP
http://slidepdf.com/reader/full/sarky-rvp 54/54


















![Tramites rvp 02_registro[1]](https://img.pdfslide.us/doc/110x75/58ef6a4a1a28ab80278b4617/tramites-rvp-02registro1.jpg)








