Embed Size (px)
Citation preview

Il trattamento dell’infarto miocardico acuto ad ST spraslivellato: dal territorio al laboratorio di emodinamica
Il punto sulla terapia antitrombotica nelle sindromi coronariche acute
Santa Margherita LigureTIGULLIO CARDIOLOGIA 2012
16-17 Febbrajo 2012
Diego ArdissinoParma

Divisione di CardiologiaParma
Antithrombotic therapy in ACS
Aggressiveness of Antithrombotic therapy
Ischemic Risk
Bleeding Risk
Ischemic vs Bleeding Risk in ACS
Today’s practiceOptimal practice
Risk

Divisione di CardiologiaParma

Divisione di CardiologiaParma
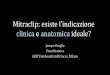
Aspirin in Acute Myocardial InfarctionCumulative vascular mortality in days 0 - 35
Cum
ulat
ive n
umbe
r of v
ascu
lar d
eath
s
Days from randomisation0 7 14 21 28 35
0
100
200
300
400
500
600Placebo
Streptokinase + aspirin
Streptokinase
The Lancet 1988
Aspirin

ESC/ EACTS Guidelines on myocardial revascularization 2010Antithrombotic treatment options in myocardial revascularization
Options for anticoagulation include UFH 60 IU/Kg iv boluswith GPIIb/IIIa inhibitor or UFH 100 IU/Kg iv bolus withoutGPIIb/IIIa inhibitor, (I C) or bivalirudin 0.75 mg/Kg bolusfollowed by 1.75 mg/kg/h (I B). Antithrombins can be stoppedafter PCI for STEMI.

EUROPEAN SOCIETY OF CARDIOLOGY GUIDELINESMANAGEMENT OF ACUTE MYOCARDIAL INFARCTION
Unfractionated heparin is standard anticoagulant therapy duringPCI.
• i.v. bolus: 100 U/Kg (60 U/Kg if GP IIb/IIIa antagonists are used)•target ACT during procedure: 250-350 seconds (200-250 seconds if GP IIb/IIIaantagonists are used)
CLASS I EVIDENCE C
ANTITHROMBOTIC THERAPY IN PRIMARY PCI

EUROPEAN SOCIETY OF CARDIOLOGY GUIDELINESMANAGEMENT OF ACUTE MYOCARDIAL INFARCTION
CLASS IIa EVIDENCE A
ANTITHROMBOTIC THERAPY IN PRIMARY PCI
Abiciximab can be administered in primary PCI.•i.v. bolus: 0.25 mg/kg
•Infusion: 0.125 mcg/Kg/min (maximum 10 mcg/min for 12 hours)

Abciximab as Adjunctive Therapy to Reperfusion in STEMI30-day mortality
Divisione di CardiologiaParma�De Luca G. et al, JAMA 2005; 293: 1759-65
RAPPORTISAR-2ADMIRALCADILLACPetronio et alZorman et alACEPetronio et alASSENT-3ENTIRE-TIME 23GUSTO VPrimary PCIFibrinolysis
Overall
P Value
0.750.240.160.490.360.100.79
> 0.990.150.790.430.0470.95
0.61
0.1 101Abciximab better Control better
Odds Ratio (95% CI)

Abciximab as Adjunctive Therapy to Reperfusion in STEMILong-term (6 and 12 month) mortality
Divisione di CardiologiaParma�De Luca G. et al, Jama 2005; 293: 1759-65
P Value
0.830.330.130.830.150.040.040-090.990.010.41
0.98
0.1 101Abciximab better Control better
Odds Ratio (95% CI)
RAPPORTISAR-2ADMIRALCADILLACPetronio et alZorman et alACEASSENT-3GUSTO VPrimary PCIFibrinolysis
Overall

Abciximab vs Placebo in Primary PCIDeath or re-infarction over 3 years of follow-up
Divisione di CardiologiaParma
Time
Surv
ival d
istrib
utio
n fu
nctio
n
0 400 600 1000
Montalescot G. et al, Eur Heart J 2007; 28: 443-449
200 800
Trials: ACE, ADMIRAL and ISAR
0.80
0.85
0.90
0.95
1
P = 0.008
AbciximabPlacebo

ESC/ EACTS Guidelines on myocardial revascularization 2010Antithrombotic treatment options in myocardial revascularization
CLASS III EVIDENCE B
….the controversial literature data, the negative outcome of theonly prospecitve RCT and the beneficial effects of faster acting andmore efficacious ADP receptor blockers in primary PCI do notsupport pre-hospital or pre-catheterization use of GPIIb/IIIainhibitors.
UPSTREAM GP IIb/IIIa INHIBITORS

0
2
4
6
8
10
12
14
16
Facilitated PCI in Patients with STEMIThe FINESSE trial
Divisione di CardiologiaParma
Days
Patie
nts w
ith P
rimar
y Com
posit
eEn
d Po
int p
erce
nt
0 30 60 90
Ellis SG. et al, N Engl J Med 2008; 358: 2205-17
Primary PCIAbciximab-facilitated PCICombination-facilitated PCI
P = NS

0
5
10
15
20
25
30
Divisione di CardiologiaParma
TIMI Bleeding through Discharge/Day 7
Perc
enta
ge
TIMI major TIMI minor TIMI major or minor
Facilitated PCI in Patients with STEMIThe FINESSE trial
2.64.1 4.8 4.3
6
9.7
6.9
10.1
14.5
P < 0.001
P < 0.001
P = 0.025
P = 0.127P = 0.547
P = 0.141
P = 0.006P = 0.025
P = 0.008
Primary PCI with in Lab Abciximab ( n = 795 )Abciximab facilitated PCI ( n = 805 )Abciximab/Reteplase facilitated ( n = 814 )
Ellis SG. et al, N Engl J Med 2008; 358: 2205-17

STEMIplanned for 1° PCI
ENOXAPARIN IV0.5 mg/kg
(± GP IIb/IIIa inhibitor)
UFH IV50 – 70 IU/kg if GP IIb/IIIa
70 – 100 IU/kg if no GP IIb/IIIaDose adjusted to ACT
Randomization (N = 850)
1° PCI and stenting1° EP: Death, complication of MI, procedure failure
or non-CABG major bleeding at 30 daysMain 2° EP: Death, MI, refractory ischemia, urgent revasc.
6-month follow-upPatients who have already received UFH or LMWH or any other anticoagulant are excluded.
All concomitant drugs accepted, except lytics; cross-over to other anticoagulant NOT accepted.
Enoxaparin vs UFH in primary PCIATOLL Study Design
Divisione di CardiologiaParma
Montalescot, ESC 2010

Divisione di CardiologiaParma
28
33,7
0
10
20
30
40
Montalescot, ESC 2010
RRR=17% P=0.07
Per
cent
of p
atie
nts
Enoxaparin vs UFH in primary PCIATOLL trial Primary endpoint
Death, complication of MI, procedure failure or maior bleeding

ESC/ EACTS Guidelines on myocardial revascularization 2010Antithrombotic treatment options in myocardial revascularization
CLASS I EVIDENCE B
….a recent study suggested bivalirudin monotherapy as analterantive to UFH plus a GPIIb/IIIa inhibitor.
ANTICOAGULATION

0
3
6
9
12
15
Bivalirudin During Primary PCI in STEMIThe HORIZONS-AMI trial
Divisione di CardiologiaParma
Days
Net A
dver
se C
linica
l Eve
nts p
erce
nt
0 10 20 30
�Stone GW. et al, N Engl J Med 2008; 358: 2218-30
5 15 25
Net adverse clinical events
Heparin plus GP IIB/IIIaBivalirudin alone P = 0.006
12.2
9.3

0
1
2
3
4
5
6
7
8
Bivalirudin During Primary PCI in STEMIThe HORIZONS-AMI trial
Divisione di CardiologiaParma
Days
Majo
r Adv
erse
card
iova
scul
arEv
ents
per
cent
0 10 20 30
Stone GW. et al, N Engl J Med 2008; 358: 2218-30
5 15 25
Major adverse cardiovascular events
Heparin plus GP IIB/IIIaBivalirudin alone
P = 0.985.5
5.5

0
3
6
9
12
Bivalirudin During Primary PCI in STEMIThe HORIZONS-AMI trial
Divisione di CardiologiaParma
Days
Majo
r Blee
ding
per
cent
0 10 20 30
�Stone GW. et al, N Engl J Med 2008; 358: 2218-30
5 15 25
Major bleeding
Heparin plus GP IIB/IIIaBivalirudin alone P < 0.0001
8.4
5.0

0
1
2
3
4
5
Bivalirudin During Primary PCI in STEMIThe HORIZONS-AMI trial
Divisione di CardiologiaParma
Days
Deat
h pe
rcen
t
0 10 20 30
Stone GW. et al, N Engl J Med 2008; 358: 2218-30
5 15 25
Death from cardiac and non cardiac causes
Heparin plus GP IIB/IIIaBivalirudin alone
P = 0.032.9
1.8
0.3
0.2
Cardiac
Noncardiac

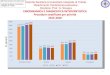
Bivalirudin During Primary PCI in STEMIThe HORIZONS-AMI trial 3-years follow up
Divisione di CardiologiaParmaStone GW. et al, TCT 2010
0.1 0.5 1.0 1.5 2.0
Major bleeding
All-cause mortality
Cardiac mortality
Reinfarction
6.9
5.9
2.9
6.2
10.5
7.7
5.1
8.2
0.64 (0.51-0.80)
0.75 (0.58-0.97)
0.56 (0.40-0.80)
0.76 (0.59-0.92)
<0.001
0.03
0.001
0.04
Endpoint Bival HR (95% CI) pHep+GP IIb/IIIa(%) (%)

ANTITHROMBOTIC THERAPY IN STEMIAbciximab vs bivalirudin
Divisione di CardiologiaParma
High ischemic risk
High bleeding risk
AGGRESSIVENESS OF ANTITHROMBOTIC THERAPY
Abciximab
+Heparin
Biva
lirud
in
Heparin

ESC/ EACTS Guidelines on myocardial revascularization 2010Antithrombotic treatment options in myocardial revascularization
Dual antiplatelet therapy consists of aspirin 150-300mg per os or 250-500 mg bolus iv followed by 75-100 mg daily, and prasugrel 60 mgloading dose, followed by 10 mg daily, or ticagrelor 180 mg loadingdose, followed by 90 mg twice daily, depending on drug availability.
Clopidogrel 600 mg loading dose, followed by 75 mg daily should beused primarily if the more effective ADP receptor blockers arecontroindicated or unavailable.
STEMI ANTITHROMBOTIC THERAPY

012345
6789
1011
COMMIT / CCS-2In-hospital death
Divisione di CardiologiaParma
Time since randomization (up to 28 days)
Deat
h pe
rcen
t
0 14
COMMIT Collaborative Group Lancet 2005; 366: 1607-21
7 14 21
Placebo + ASA: 1845 deaths (8.1%)Clopidogrel + ASA: 1726 deaths (7.5%)
7 % (SE) relative risk reduction (2P = 0.03)

Divisione di CardiologiaParma
Hours prior to PCI of study drug loading doseSteirhubl SR et al Circulation 2003;108:374
MACE
5 150 10 20 25
PlaceboClopidogrel
p = 0.02for treatment/timing interaction
Prevention of Myocardial Infarction During PCIEffect of Clopidogrel 300 mg Loading Dose

Divisione di CardiologiaParmaFefer P et al. Am J Cardiol 2009; 104: 514-518
Patie
nts (
%)
Clopidogrel 600 mg Clopidogrel 300 mg n=116 n=80 n=97 n=64
p<0.01
Primary composite endpoint at 30 days ( death, recurrent ACS, stent thrombosis, CHF)
Impact of pre-treatment with clopidogrel on outcome in STEMI

ESC/ EACTS Guidelines on myocardial revascularization 2010Antithrombotic treatment options in myocardial revascularization
CLASS I EVIDENCE B
Prasugrel is superior to clopidogrel in reducing combinedischaemic endpoints and stent thrombosis in STEMI patientswithout increasing the risk of severe bleeding.

Prasugrel vs clopidogrel in primary PCI TRITON TIMI-38
Primary endpoint: Cardiovascular death, non-fatal MI, non-fatal stroke
0
5
10
15
Montalescot G et al, Lancet 2009; 373: 723-31Divisione di Cardiologia
Parma
Cum
ulat
ive in
ciden
ce (%
)
50 150 250 350 450
Days from randomization
p=0.0017 p=0. 0221
ClopidogrelPrasugrel

0
5
10
15TIMI major bleeding
TRITON TIMI-38Prasugrel vs clopidogrel in primary PCI
Montalescot G et al, Lancet 2009; 373: 723-31Divisione di Cardiologia
Parma
Days from randomization50 150 250 350 450
p=0.3359 p=0. 6451
Cum
ulat
ive in
ciden
ce (%
) ClopidogrelPrasugrel

Net Clinical BenefitBleeding Risk Subgroups Post-hoc Analysis
YesNo
≥ 75< 75
< 60 Kg≥ 60 Kg
Overall
+54-16
-1-16
+3-14
-13
0.5 1 2
Pinter = 0.36
HRPrasugrel better Clopidogrel better
Risk percent
PriorStroke / TIA
Age
Wgt
Pinter = 0.18
Pinter = 0.006
Divisione di CardiologiaParma

CLASS I EVIDENCE B
…A predefinite subgroup analysis has demonstrated that STEMIpatients referred to PCI significantly benefit from ticagrelor vsclopidogrel, with similar bleeding rates.
ESC/ EACTS Guidelines on myocardial revascularization 2010Antithrombotic treatment options in myocardial revascularization

Divisione di CardiologiaParma
Greater and More Consistent IPAwith AZD6140 than Clopidogrel
Final Extent
Mean
per
cent
inhi
bitio
n
Hours
AZD6140 100 mg bd
0
20
40
60
80
100
0 2 4 8 12 242 4 8 12Day 1 Day 14
Hours
Clopidogrel
0
20
40
60
80
100
0 2 4 8 12 242 4 8 12Day 1 Day 14

0123456789
101112
Divisione di CardiologiaParma
Months
Cum
ulat
ive in
ciden
ce (%
)
0 1 3 5 7 9 12
Clopidogrel
Ticagrelor
2 4 6 8 10
T 3752 3476 3424 3331 2687 2049 1675
C 3792 3501 3438 3356 2726 2097 1679
11
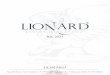
Ticagrelor vs clopidogrel in STEMI treated with primary PCIPrimary efficacy endpoint
Steg PG et al, Circulation 2010, 122:2131-2141
HR 0.87 95%CI 0.75-1.01 p=0.07

0123456789
101112
Divisione di CardiologiaParma
Months
Cum
ulat
ive in
ciden
ce (%
)
0 1 3 5 7 9 12
Clopidogrel
Ticagrelor
2 4 6 8 10
T 3752 3581 3539 3461 2812 2154 1766
C 3792 3614 3580 3511 2872 2216 1773
11
Ticagrelor vs clopidogrel in STEMI treated with primary PCICardiovascular death
Steg PG et al, Circulation 2010, 122:2131-2141
HR 0.83 95% CI 0.67-1.02 p=0.07

0
1
2
3
4
5
6
7
8
9
10
Divisione di CardiologiaParma
Months
Cum
ulat
ive in
ciden
ce (%
)
0 1 3 5 7 9 12
Clopidogrel
Ticagrelor
HR 0.98 95%CI 0.83-1.14 p=0.76
2 4 6 8 10 11
Ticagrelor vs clopidogrel in STEMI treated with primary PCI
Steg PG et al, Circulation 2010, 122:2131-2141
Major bleeding according to PLATO definition
T 3719 3079 2920 2812 2183 1592 1459
C 3752 3092 2972 2850 2202 1624 1471

Divisione di CardiologiaParma
Pre-hospital vs. In-hospital initiation of ticagrelor therapy in STEMIATLANTIC study design
Primary endpoint: TIMI flow grade 3 of MI culprit vessel at initial angiography; ST-segment resolution up to pre PCI >70%
Secondary endpoint: 30-days death, MI, urgent revascularization, stent thrombosis, life threatening bleeding, major and minor bleeding
(n = 1.770)
Pre-hospital Ticagrelor loading dose (180 mg) followed by in-hospital matching placebo
Randomized, Parallel-group, Double blind, Placebo controlled phase IV trial
STEMI patients planned for primary PCI(symptom onset < 6 hours)
R
Pre-hospital placebo followed by in-hospital Ticagrelor loading dose (180mg)

Primary Efficacy Endpoint: CV death, MI or strokePrimary Safety Endpoint: TIMI major Bleeding
Follow up VisitsQ4 mos for 1st ys, then Q6 mos
(n = 21,000)
Ticagrelor 90 mg BID Placebo
Divisione di CardiologiaParma
History of MI 1-3 years prior +
Randomize double blind
* Age≥ 65yrs, diabetes, 2nd prior MI, multivessel CAD, PAD or chronic non-end stage renal dysfunction
PEGASUS TIMI 54 Study design
Min 12 mos and average 24 mos follow-up
Event driven trial
Standard background care (ASA 75-100 mg recommended)
Ticagrelor 60 mg BID
> 1 additional atherothrombosis risk factor

Divisione di CardiologiaParma
The cycle of continuous quality improvement
Concept
Clinical Trials
Guidelines
PerformanceIndicators
Outcomes
Performance
Califf RM et al. JACC 2002;40:1895-901