Embed Size (px)
Citation preview
SAMO Master Class
Colorectal Cancer
Roger von MoosRoger von Moos
Kantonsspital Graubünden
12.9.2014
Potential conflict of interest and otherPotential conflict of interest and otherstatementsstatements
Thanks to Bernhard Pestalozzi to share some slidesThanks to Bernhard Pestalozzi to share some slides
Advisory board: Amgen, Merck, Roche, Sanofi, PfizerAdvisory board: Amgen, Merck, Roche, Sanofi, Pfizer Advisory board: Amgen, Merck, Roche, Sanofi, PfizerAdvisory board: Amgen, Merck, Roche, Sanofi, Pfizer
Unrestricted research grant: Amgen, Merck, RocheUnrestricted research grant: Amgen, Merck, Roche
Speaker: Amgen, Roche, BayerSpeaker: Amgen, Roche, Bayer
IncidenceIncidence
2012 4472012 447‘‘000 new cases000 new cases
Second most frequent cancerSecond most frequent cancer
Responsible for 215Responsible for 215‘‘000 deaths000 deaths Responsible for 215Responsible for 215‘‘000 deaths000 deaths
25% of patients presents with metastases25% of patients presents with metastases
50% will develop metastasis50% will develop metastasis
5 year survival rate 60%5 year survival rate 60%
Van Cutsem, Annals of Oncol, 2014
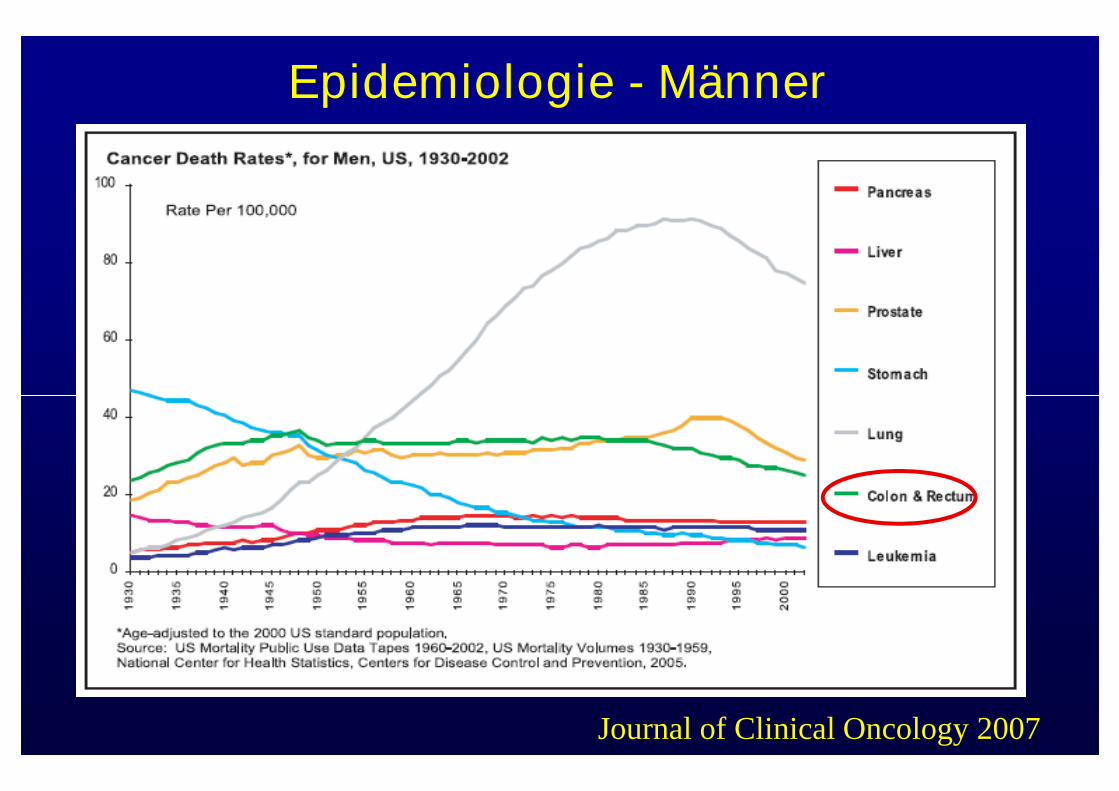
Epidemiologie - Männer
Journal of Clinical Oncology 2007
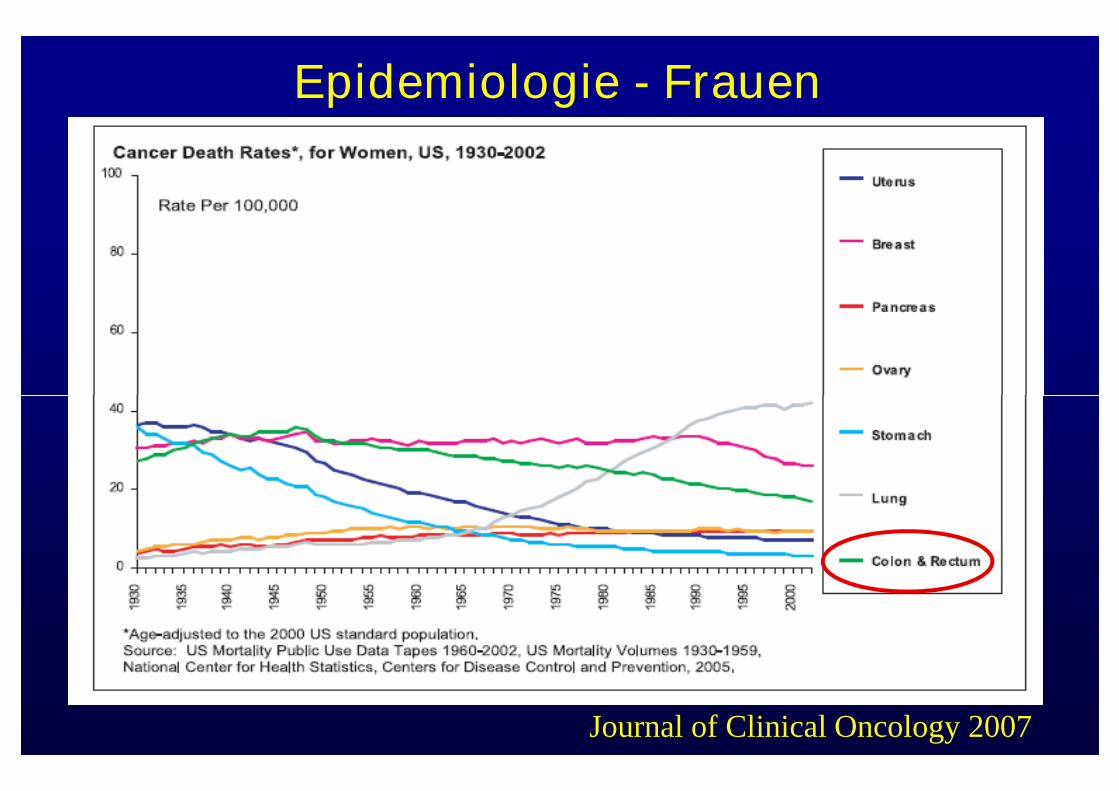
Epidemiologie - Frauen
Journal of Clinical Oncology 2007
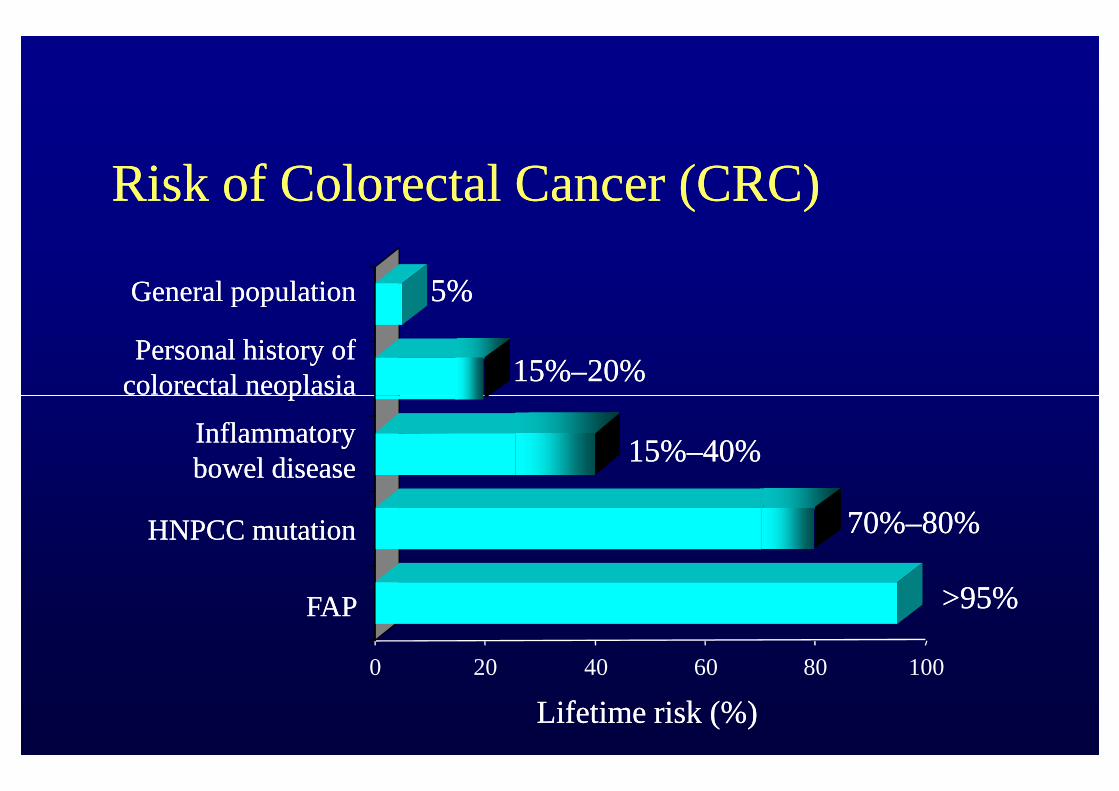
Risk of Colorectal Cancer (CRC)Risk of Colorectal Cancer (CRC)
General populationGeneral population
Personal history ofPersonal history ofcolorectal neoplasiacolorectal neoplasia
5%5%
15%15%––20%20%
0 20 40 60 80 100
colorectal neoplasiacolorectal neoplasia
InflammatoryInflammatorybowel diseasebowel disease
HNPCC mutationHNPCC mutation
FAPFAP
15%15%––40%40%
70%70%––80%80%
>95%>95%
Lifetime risk (%)Lifetime risk (%)
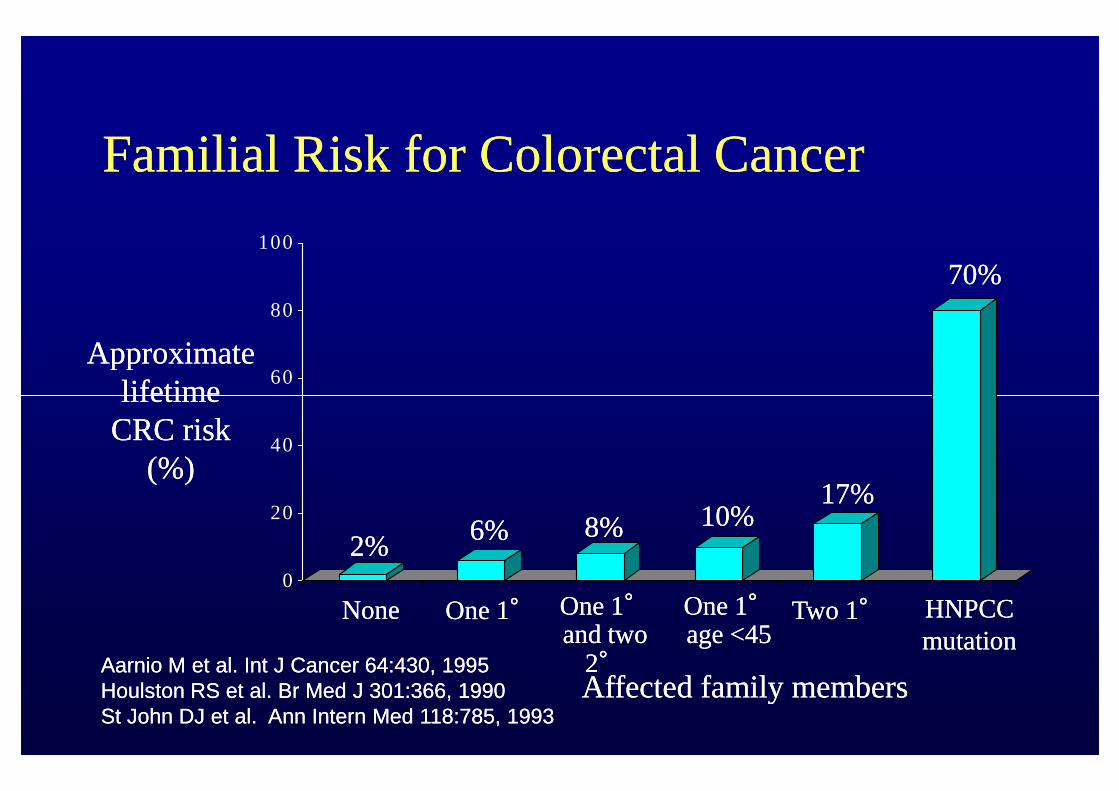
Familial Risk for Colorectal CancerFamilial Risk for Colorectal Cancer
ApproximateApproximatelifetimelifetime
60
80
100
70%70%
lifetimelifetimeCRC riskCRC risk
(%)(%)
Affected family membersAffected family members
0
20
40
NoneNone One 1One 1°° One 1One 1°°and twoand two
22°°
One 1One 1°°age <45age <45
Two 1Two 1°° HNPCCHNPCCmutationmutation
2%2%6%6% 8%8% 10%10%
17%17%
Aarnio M et al.Aarnio M et al. Int J CancerInt J Cancer 64:430, 199564:430, 1995Houlston RS et al.Houlston RS et al. Br Med JBr Med J 301:366, 1990301:366, 1990St John DJ et al.St John DJ et al. Ann Intern MedAnn Intern Med 118:785, 1993118:785, 1993
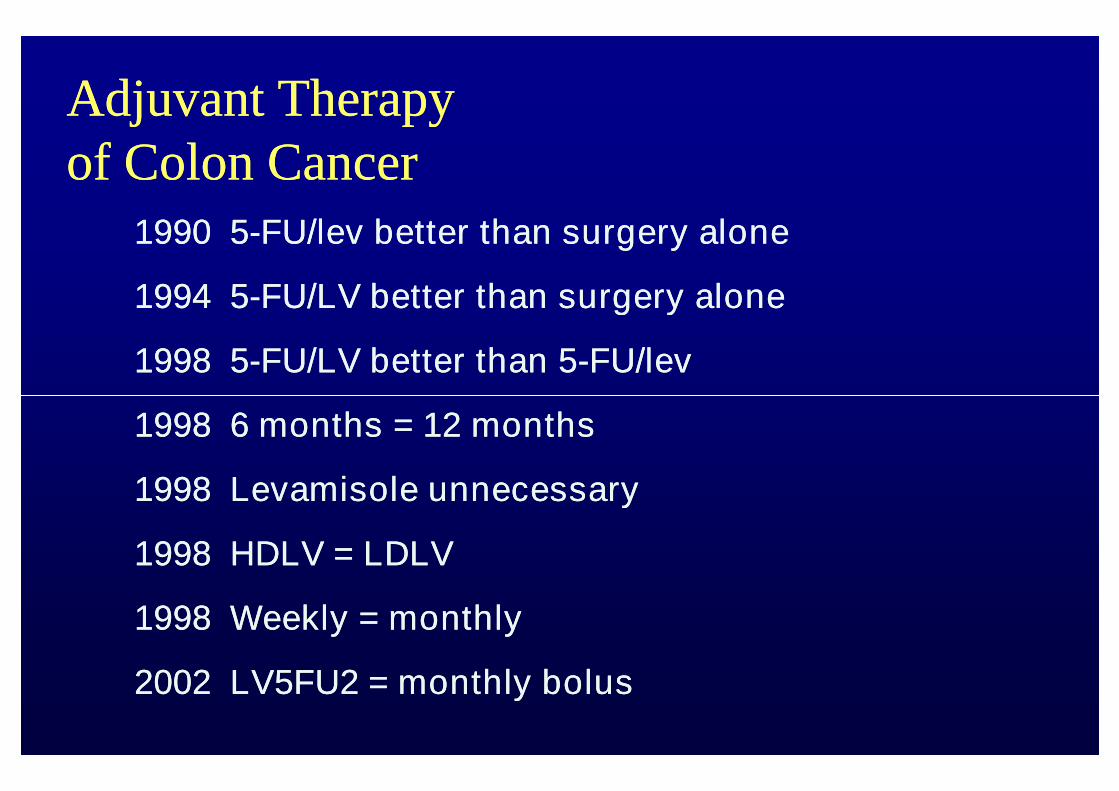
Adjuvant TherapyAdjuvant Therapyof Colon Cancerof Colon Cancer
19901990 55--FU/lev better than surgery aloneFU/lev better than surgery alone
19941994 55--FU/LV better than surgery aloneFU/LV better than surgery alone
19981998 55--FU/LV better than 5FU/LV better than 5--FU/levFU/lev
19981998 6 months = 12 months6 months = 12 months
19981998 Levamisole unnecessaryLevamisole unnecessary
19981998 HDLV = LDLVHDLV = LDLV
19981998 Weekly = monthlyWeekly = monthly
20022002 LV5FU2 = monthly bolusLV5FU2 = monthly bolus
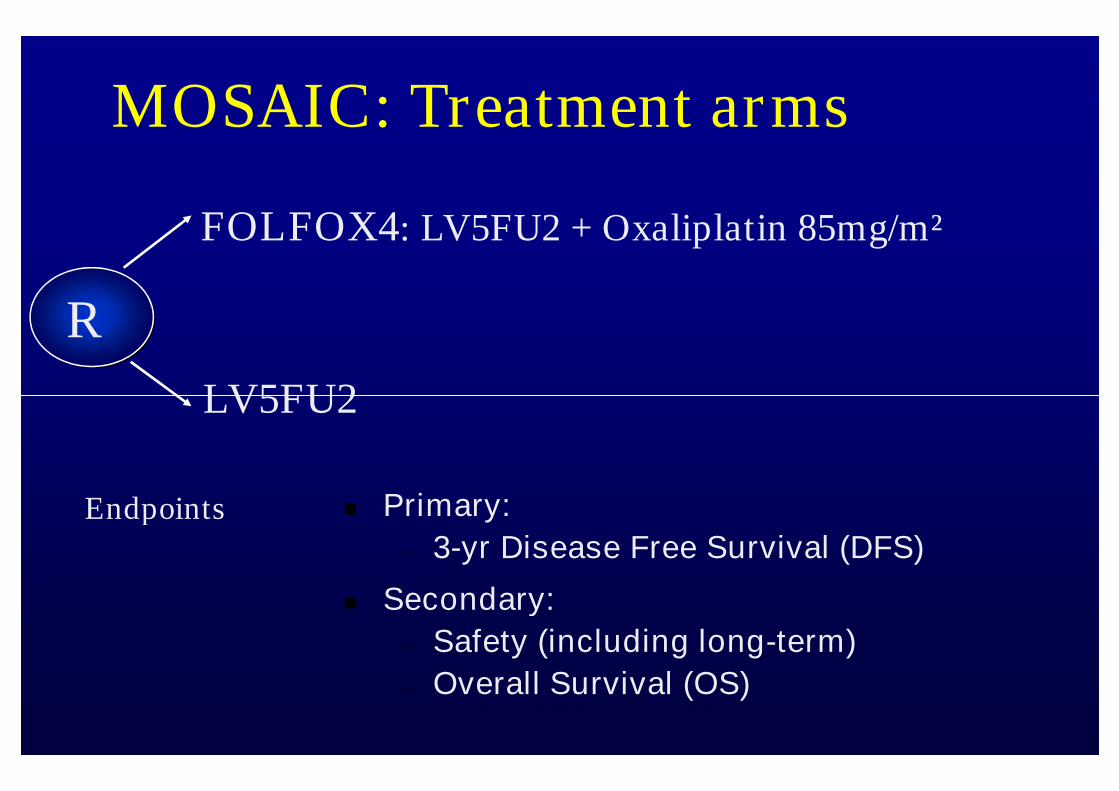
MOSAIC: Treatment arms
R
LV5FU2
FOLFOX4: LV5FU2 + Oxaliplatin 85mg/m²
LV5FU2
Primary:
– 3-yr Disease Free Survival (DFS)
Secondary:
– Safety (including long-term)
– Overall Survival (OS)
Endpoints
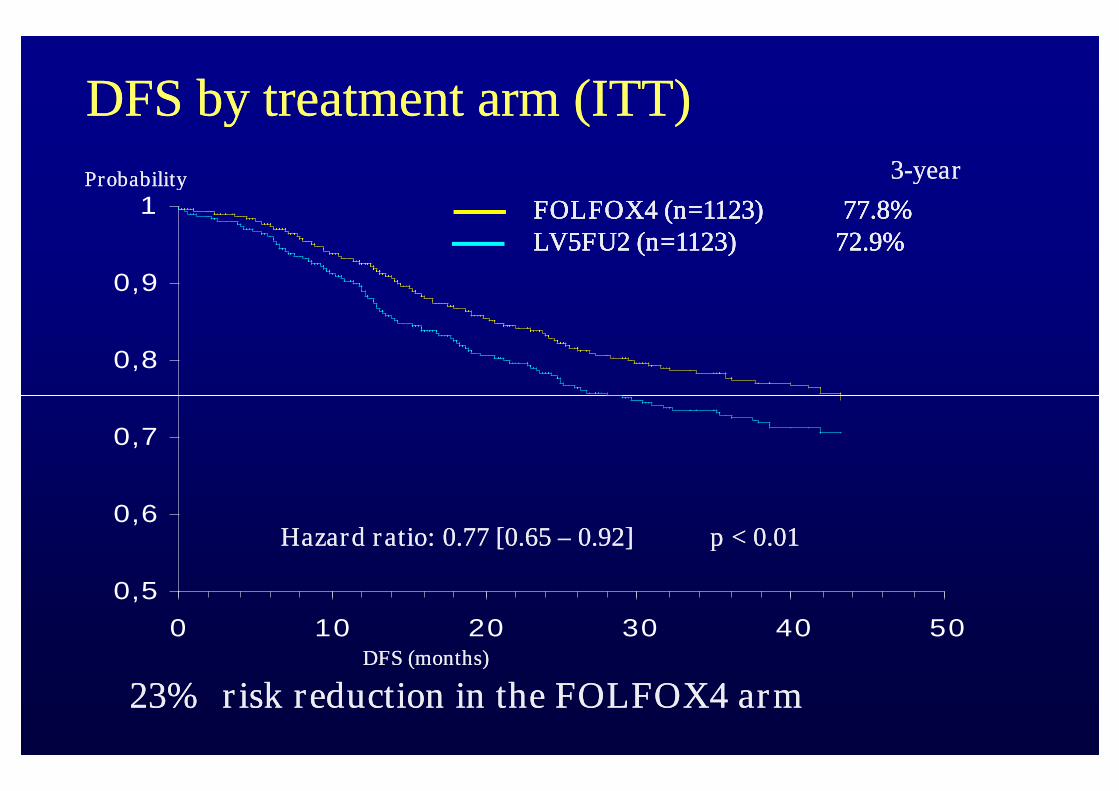
DFS by treatment arm (ITT)DFS by treatment arm (ITT)
0,8
0,9
1ProbabilityProbability
FOLFOX4 (n=1123)FOLFOX4 (n=1123) 77.8%77.8%LV5FU2 (n=1123) 72.9%LV5FU2 (n=1123) 72.9%FOLFOX4 (n=1123)FOLFOX4 (n=1123) 77.8%77.8%LV5FU2 (n=1123) 72.9%LV5FU2 (n=1123) 72.9%
33--yearyear
0,5
0,6
0,7
0 10 20 30 40 50DFS (months)DFS (months)
Hazard ratio: 0.77 [0.65Hazard ratio: 0.77 [0.65 –– 0.92]0.92] p < 0.01p < 0.01
23% risk reduction in the FOLFOX4 arm23% risk reduction in the FOLFOX4 arm
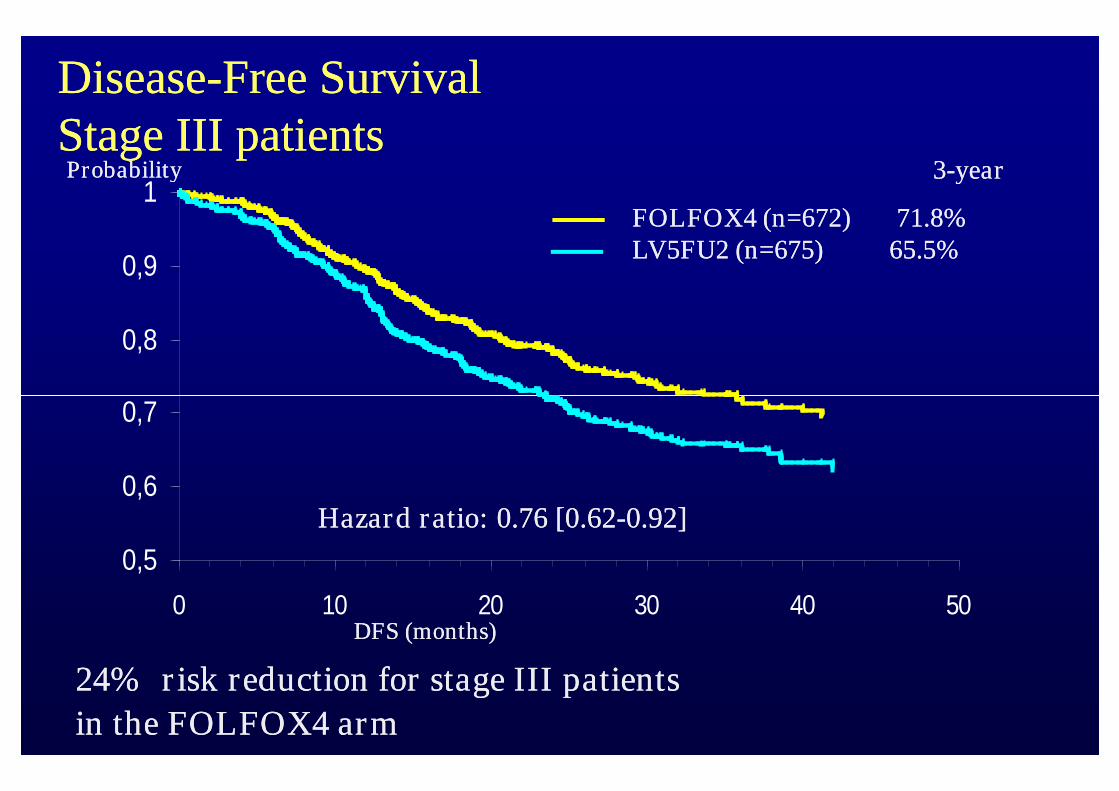
DiseaseDisease--Free SurvivalFree SurvivalStage III patientsStage III patients
0,7
0,8
0,9
1ProbabilityProbability
FOLFOX4 (n=672) 71.8%LV5FU2 (n=675) 65.5%FOLFOX4 (n=672) 71.8%LV5FU2 (n=675) 65.5%
33--yearyear
0,5
0,6
0,7
0 10 20 30 40 50DFS (months)DFS (months)
24% risk reduction for stage III patients24% risk reduction for stage III patients
in the FOLFOX4 armin the FOLFOX4 arm
Hazard ratio: 0.76 [0.62Hazard ratio: 0.76 [0.62--0.92]0.92]
ConclusionConclusion
Initial data showed DFS improvment (77.8 vsInitial data showed DFS improvment (77.8 vs72.9%)72.9%)
Follow up after 6 years no OS benefit for allFollow up after 6 years no OS benefit for all Follow up after 6 years no OS benefit for allFollow up after 6 years no OS benefit for allpatientspatients
Stage III subset 72.9 vs 68.7% stat significantStage III subset 72.9 vs 68.7% stat significant(HR 0.80; 0.65(HR 0.80; 0.65--0.97)0.97)
More neutropenia and more neurotoxicityMore neutropenia and more neurotoxicity
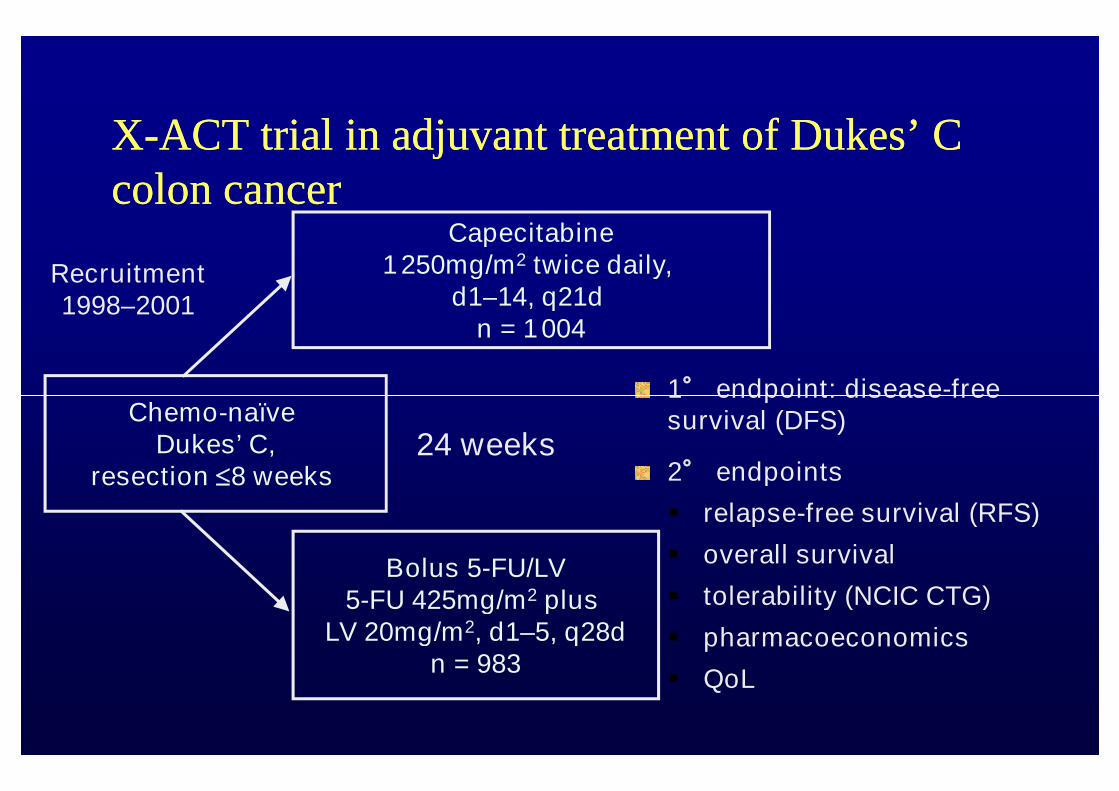
XX--ACT trial in adjuvant treatment of DukesACT trial in adjuvant treatment of Dukes’’ CCcolon cancercolon cancer
1° endpoint: disease-free
Capecitabine1250mg/m2 twice daily,
d1–14, q21dn = 1004
Recruitment1998–2001
1° endpoint: disease-freesurvival (DFS)
2° endpoints
relapse-free survival (RFS)
overall survival
tolerability (NCIC CTG)
pharmacoeconomics
QoL
Chemo-naïveDukes’ C,
resection 8 weeks
Bolus 5-FU/LV5-FU 425mg/m2 plus
LV 20mg/m2, d1–5, q28dn = 983
24 weeks
XX--ACT powered to establish at least equivalenceACT powered to establish at least equivalenceof capecitabine to bolus 5of capecitabine to bolus 5--FU/LVFU/LV
Primary endpoint DFSPrimary endpoint DFS
80% power for at least equivalence80% power for at least equivalence
if upper limit of 95% CI for HR <1.25, then primary endpointif upper limit of 95% CI for HR <1.25, then primary endpointmetmetmetmet
DFS = RFS + all deaths from other causesDFS = RFS + all deaths from other causes
RFS:RFS: relapses/new colon cancer + all deaths due to colon cancerrelapses/new colon cancer + all deaths due to colon canceror treatmentor treatment
All analyses shown were prospectively plannedAll analyses shown were prospectively planned
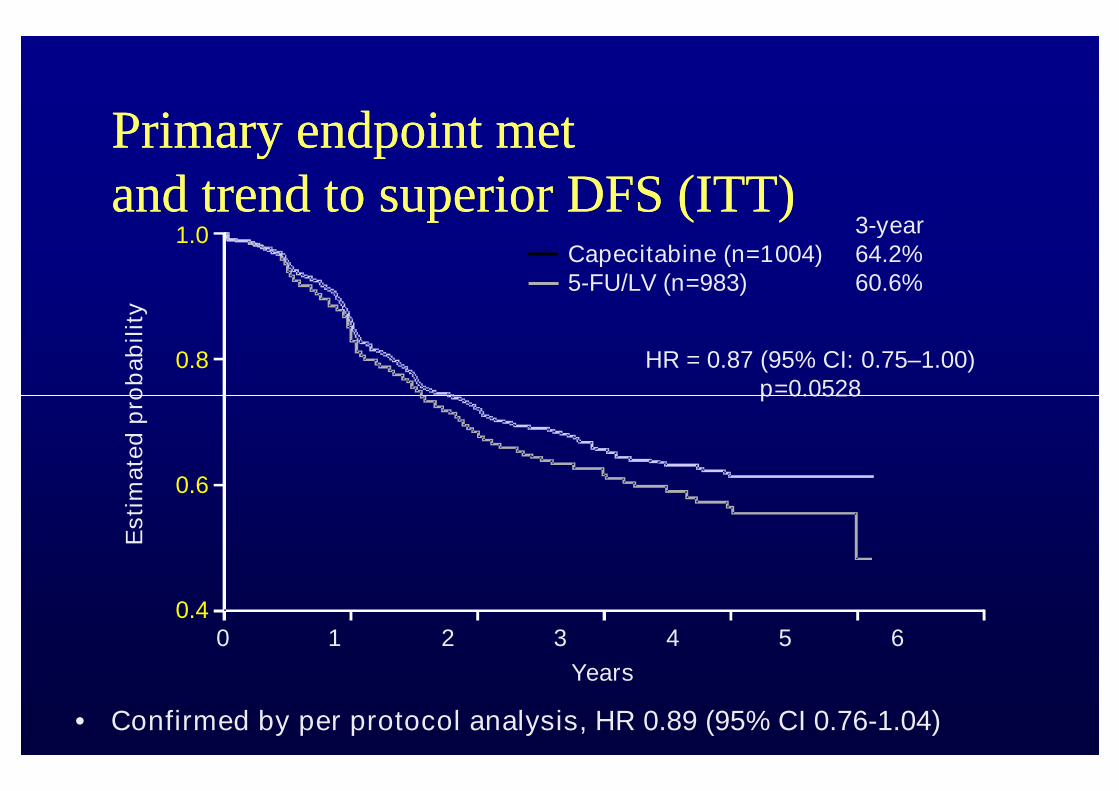
Primary endpoint metPrimary endpoint metand trend to superior DFS (ITT)and trend to superior DFS (ITT)
1.0
0.8
Esti
mate
dp
rob
ab
ilit
y
HR = 0.87 (95% CI: 0.75–1.00)p=0.0528
3-yearCapecitabine (n=1004) 64.2%5-FU/LV (n=983) 60.6%
• Confirmed by per protocol analysis, HR 0.89 (95% CI 0.76-1.04)
0.6
0.40 1 2 3 4 5 6
Years
Esti
mate
dp
rob
ab
ilit
y
p=0.0528
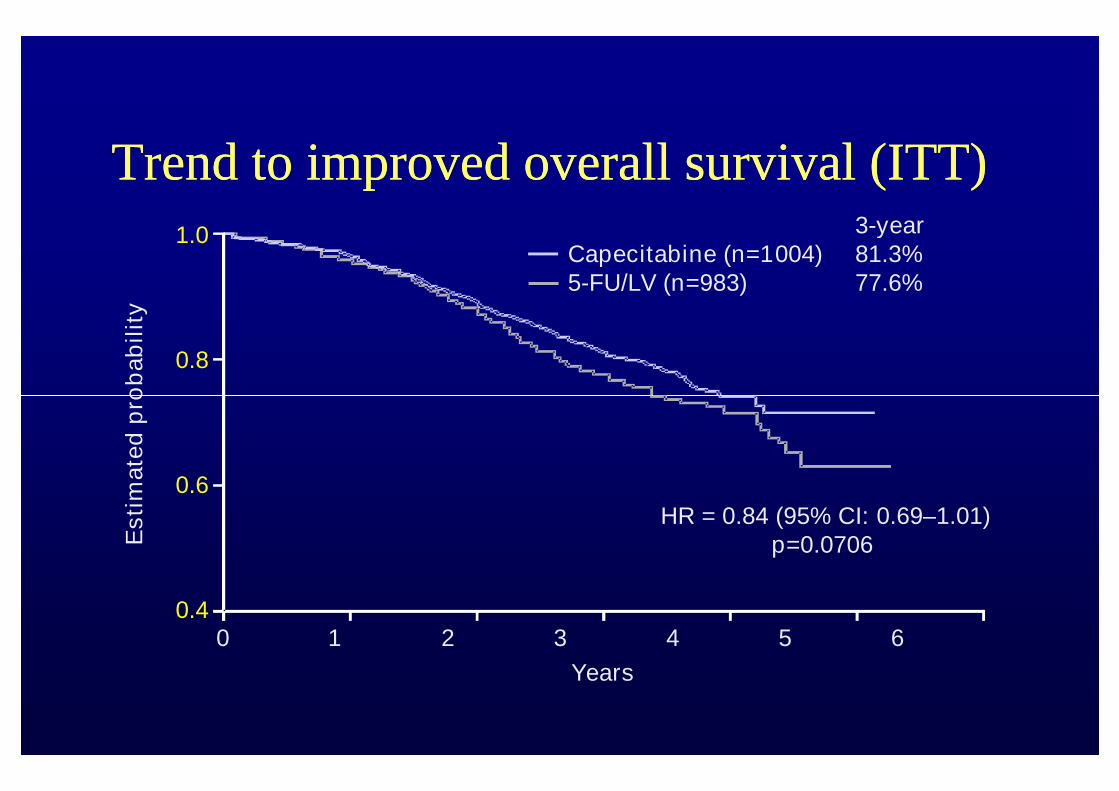
Trend to improved overall survival (ITT)Trend to improved overall survival (ITT)E
sti
mate
dp
rob
ab
ilit
y
1.0
0.8
3-yearCapecitabine (n=1004) 81.3%5-FU/LV (n=983) 77.6%
Esti
mate
dp
rob
ab
ilit
y
0 1 2 3 4 5 6
Years
HR = 0.84 (95% CI: 0.69–1.01)p=0.0706
0.6
0.4
XX--ACT study conclusionsACT study conclusions
DFS at 3 years equivalent to 5FU/LVDFS at 3 years equivalent to 5FU/LV
HFS and hyperbilirubinemia more often,HFS and hyperbilirubinemia more often,diarhoea, nausea and vomiting, stomatitis anddiarhoea, nausea and vomiting, stomatitis anddiarhoea, nausea and vomiting, stomatitis anddiarhoea, nausea and vomiting, stomatitis andneutropenia significantly lessneutropenia significantly less
In 57% of patients required dose modificationIn 57% of patients required dose modification
Capecitabine is the standard todayCapecitabine is the standard today
Metastatic colorectal cancerMetastatic colorectal cancer
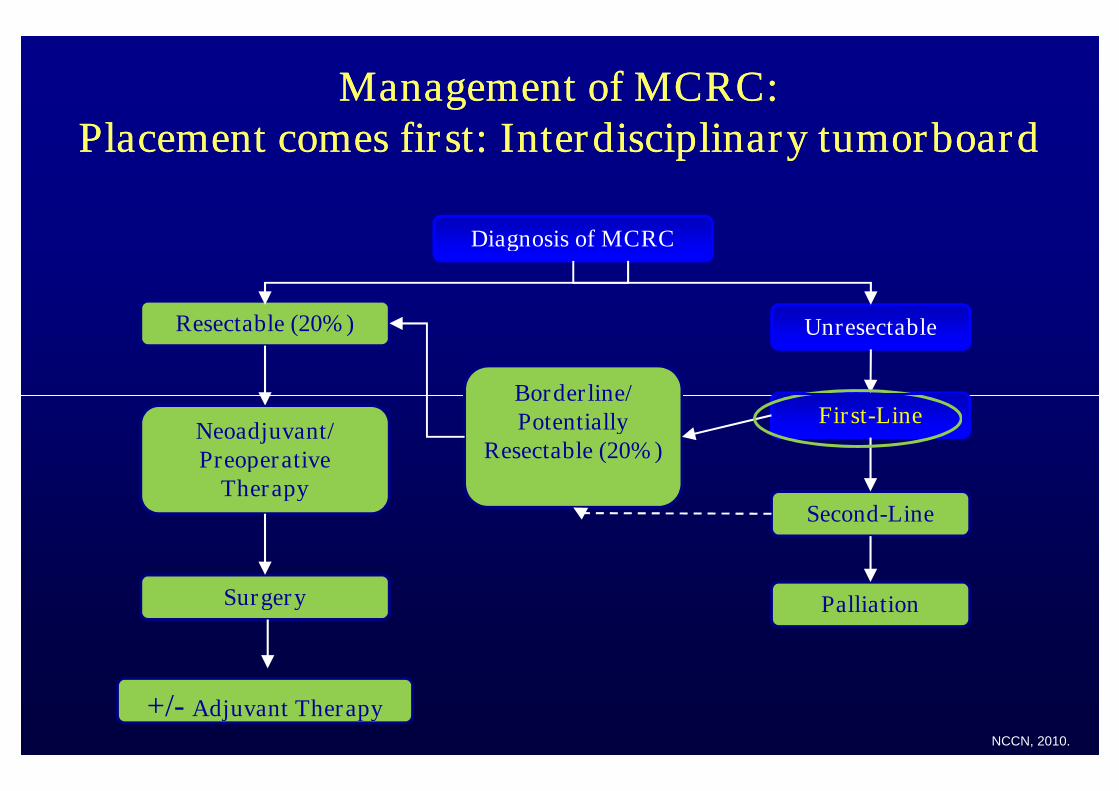
Management of MCRC:Management of MCRC:Placement comes first: Interdisciplinary tumorboardPlacement comes first: Interdisciplinary tumorboard
Diagnosis of MCRC
Resectable (20%) Unresectable
Borderline/
+/- Adjuvant Therapy
Surgery
Neoadjuvant/Preoperative
Therapy
First-Line
Second-Line
Palliation
Borderline/Potentially
Resectable (20%)
NCCN, 2010.
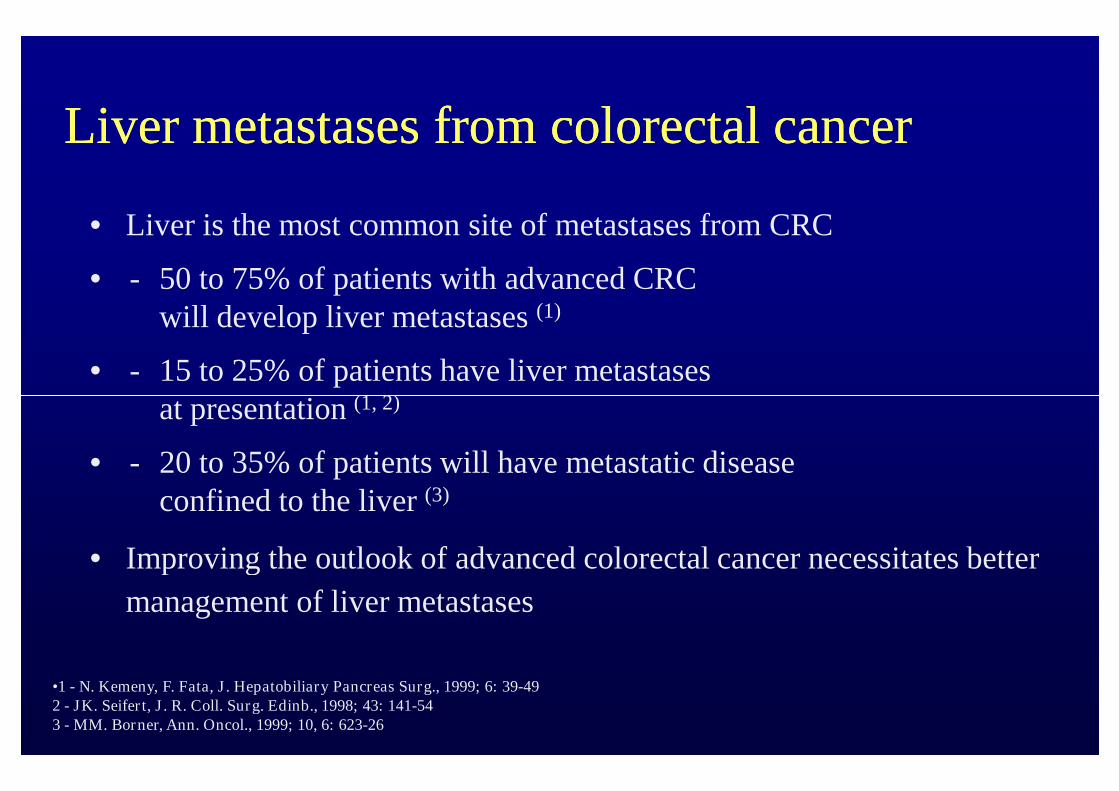
Liver metastases from colorectal cancerLiver metastases from colorectal cancer
• Liver is the most common site of metastases from CRC
• - 50 to 75% of patients with advanced CRCwill develop liver metastases (1)
• - 15 to 25% of patients have liver metastasesat presentation (1, 2)
•1 - N. Kemeny, F. Fata, J. Hepatobiliary Pancreas Surg., 1999; 6: 39-492 - JK. Seifert, J. R. Coll. Surg. Edinb., 1998; 43: 141-543 - MM. Borner, Ann. Oncol., 1999; 10, 6: 623-26
at presentation (1, 2)
• - 20 to 35% of patients will have metastatic diseaseconfined to the liver (3)
• Improving the outlook of advanced colorectal cancer necessitates better
management of liver metastases
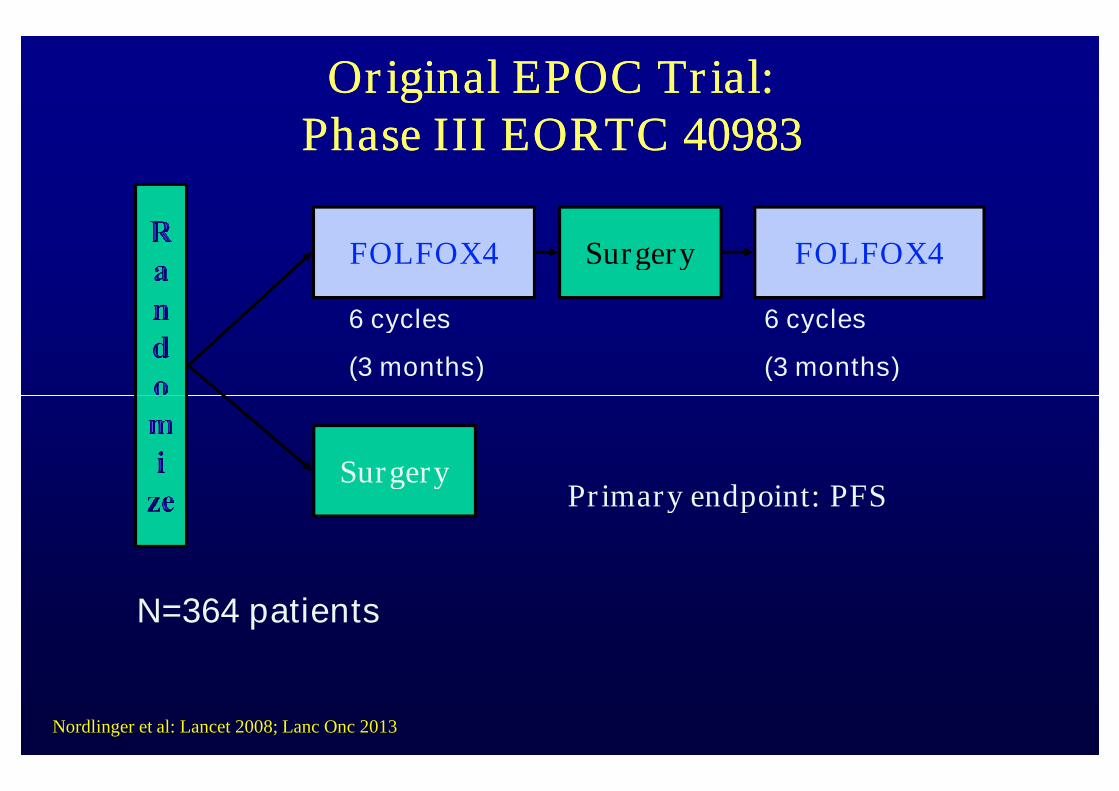
Original EPOC Trial:Original EPOC Trial:Phase III EORTC 40983Phase III EORTC 40983
SurgeryFOLFOX4 FOLFOX4
6 cycles
(3 months)
6 cycles
(3 months)
Surgery
N=364 patients
Primary endpoint: PFS
Nordlinger et al: Lancet 2008; Lanc Onc 2013
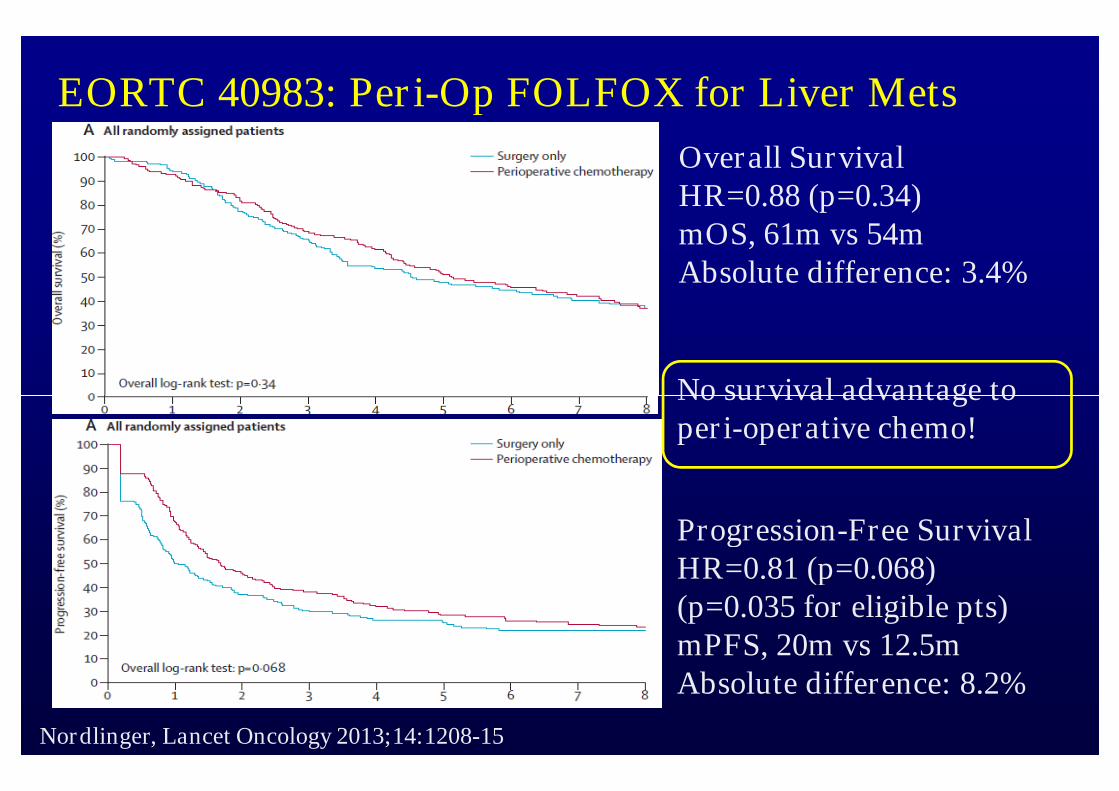
EORTC 40983: Peri-Op FOLFOX for Liver Mets
Overall SurvivalHR=0.88 (p=0.34)mOS, 61m vs 54mAbsolute difference: 3.4%
No survival advantage to
Nordlinger, Lancet Oncology 2013;14:1208-15
Progression-Free SurvivalHR=0.81 (p=0.068)(p=0.035 for eligible pts)mPFS, 20m vs 12.5mAbsolute difference: 8.2%
No survival advantage toperi-operative chemo!
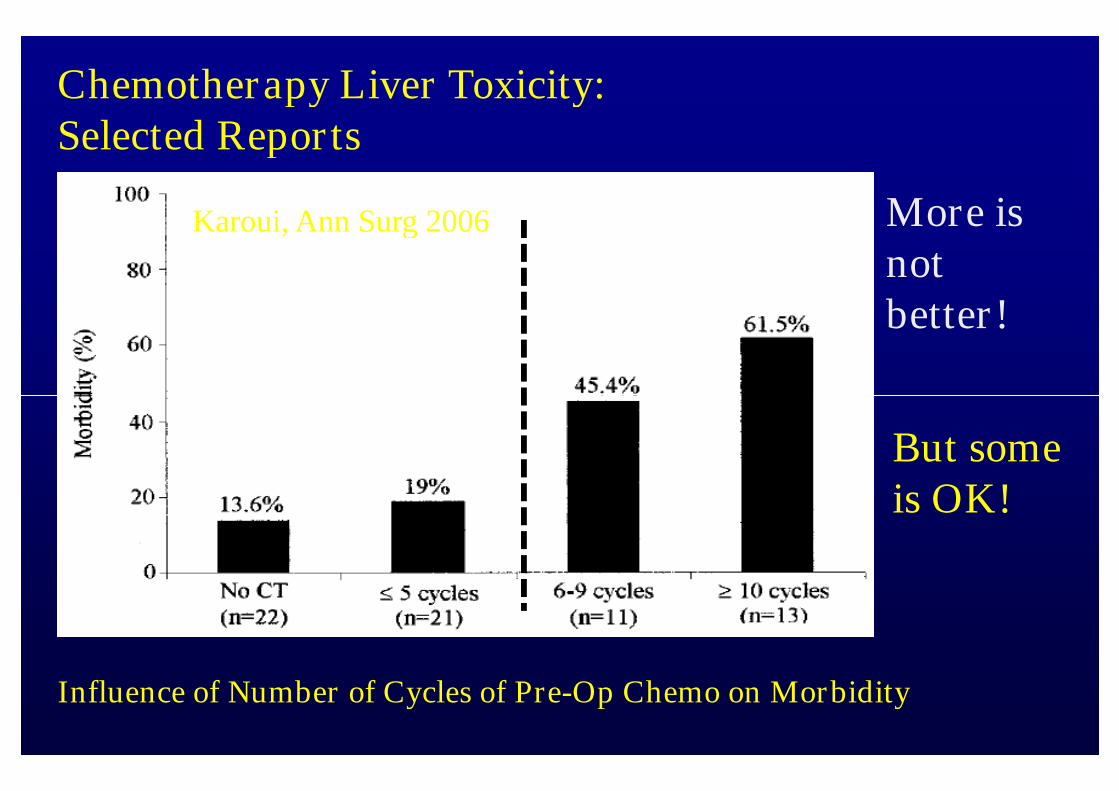
Chemotherapy Liver Toxicity:Selected Reports
Karoui, Ann Surg 2006 More isnotbetter!
Influence of Number of Cycles of Pre-Op Chemo on Morbidity
But someis OK!
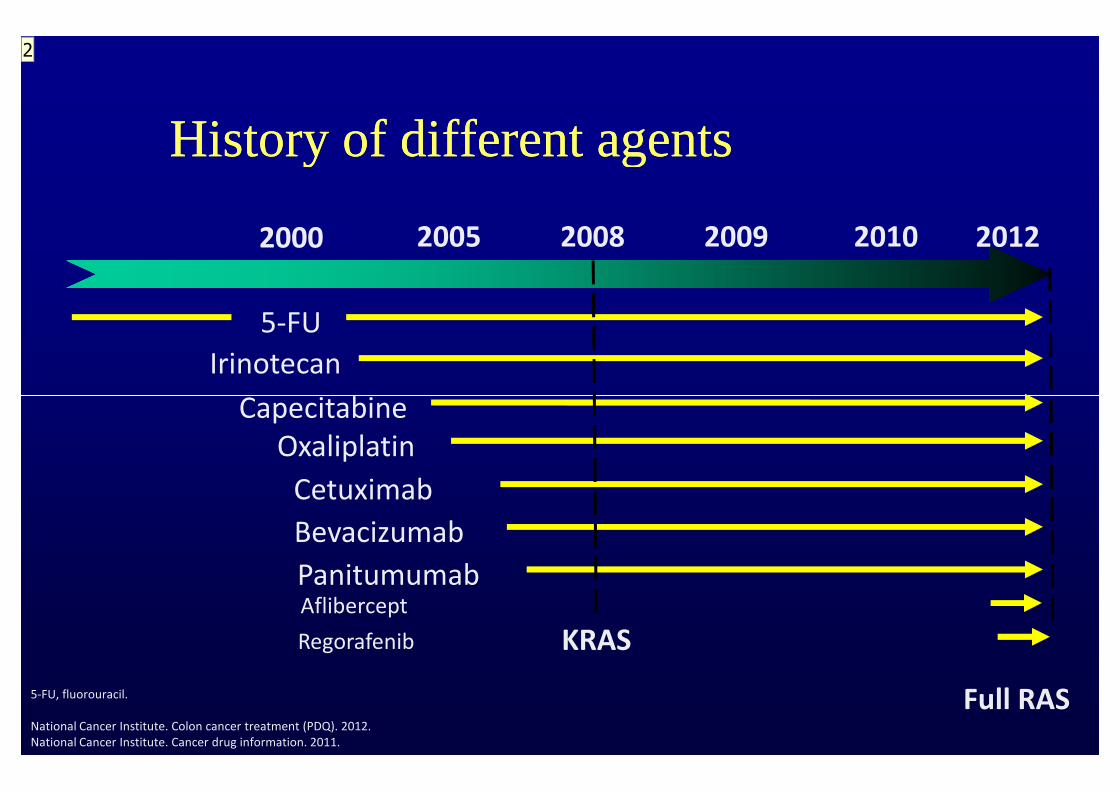
History of different agentsHistory of different agents
2000 2005 2008 2009 2010
Capecitabine
Irinotecan
5-FU
2012
CapecitabineOxaliplatin
Cetuximab
Panitumumab
Bevacizumab
KRAS
5-FU, fluorouracil.
National Cancer Institute. Colon cancer treatment (PDQ). 2012.National Cancer Institute. Cancer drug information. 2011.
Aflibercept
Regorafenib
Full RAS
2
Slide 24
2 Würde Zeitachse um 2012 ergänzen und Targeted therapies wegennehmen, erstens englisch zweitens müsste sonst die Klammer Afliberceptund Regorafenib auch umfassenRoger von Moos; 13.10.2013
RAS Wild type, what is the standard treatment ?RAS Wild type, what is the standard treatment ?
Selection for EGFR wild typSelection for EGFR wild typ PRIME data (phase III disadvantage for panitumumab in KRASPRIME data (phase III disadvantage for panitumumab in KRAS
mutant)mutant)
Data to use EGFR antibodies or Bevacizumab inData to use EGFR antibodies or Bevacizumab in Data to use EGFR antibodies or Bevacizumab inData to use EGFR antibodies or Bevacizumab infirst line in wild type patients ?first line in wild type patients ?
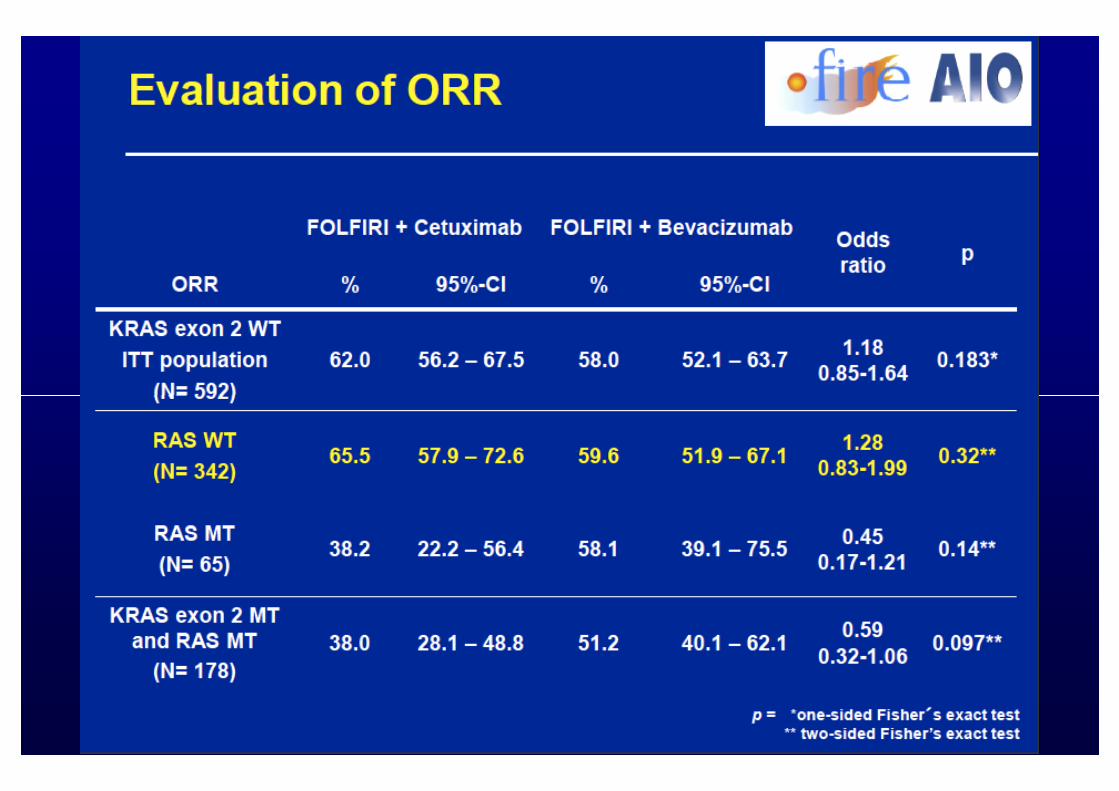
FIREFIRE--33
PEAK (not shown)PEAK (not shown)
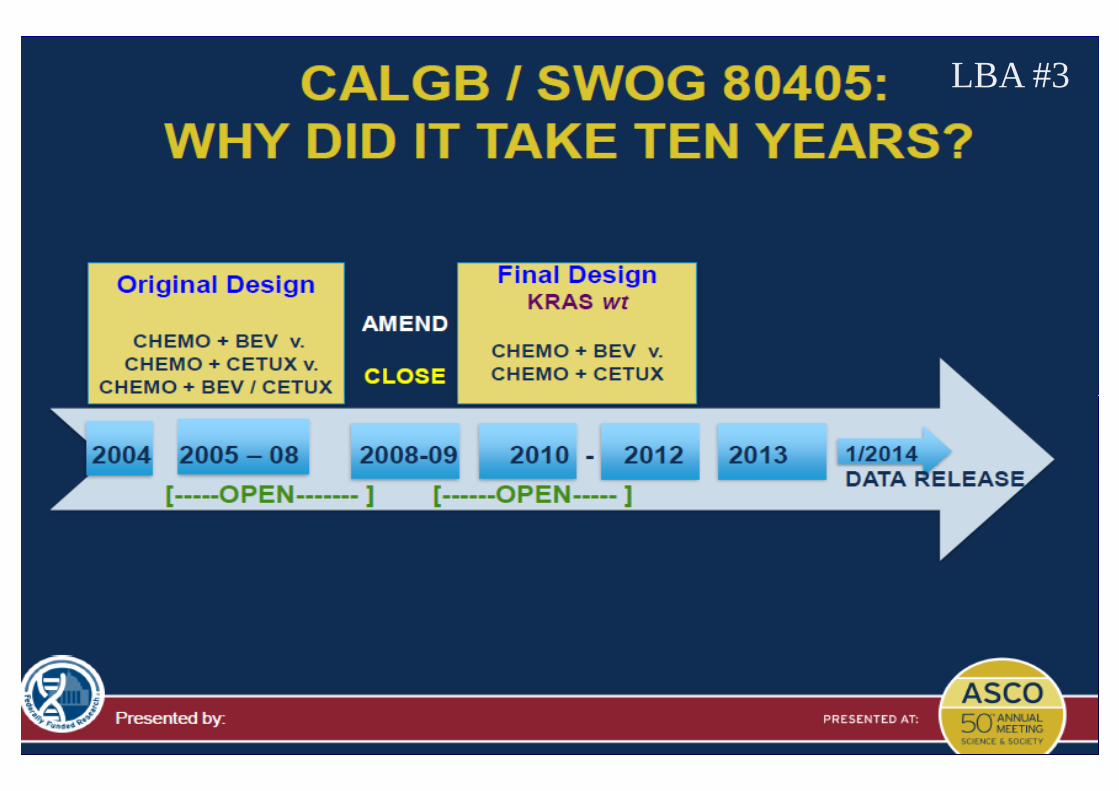
CALGB 80405CALGB 80405
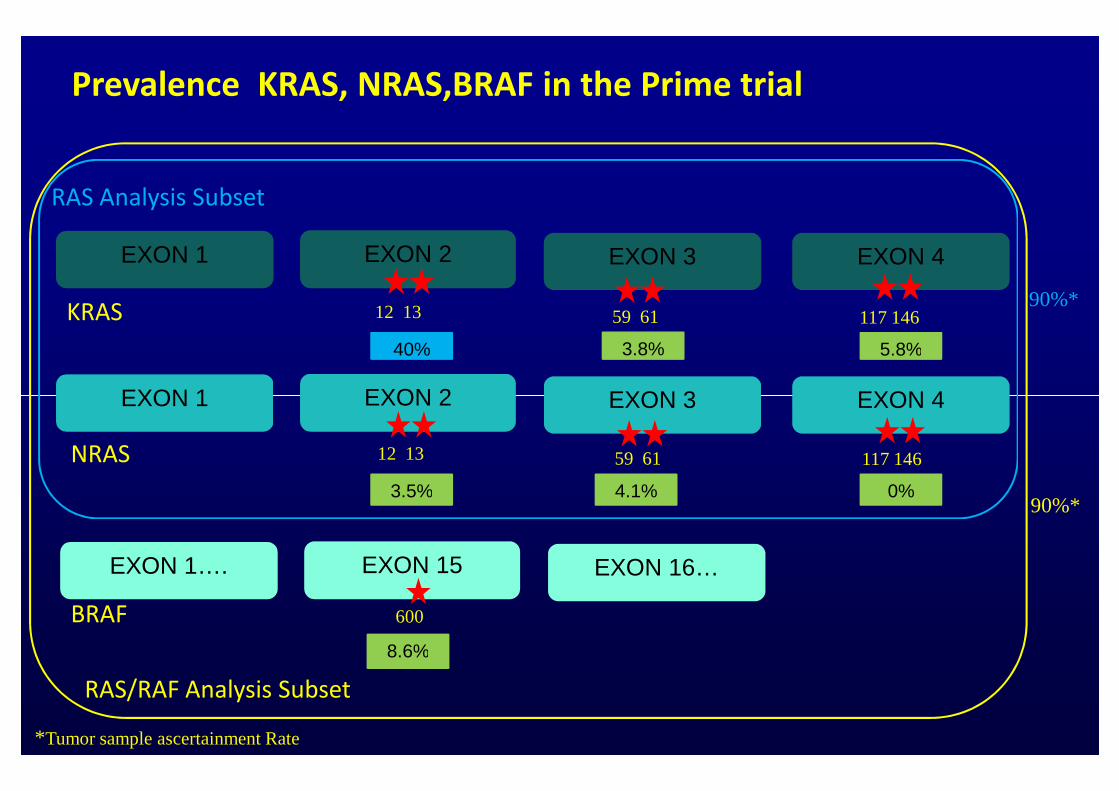
Prevalence KRAS, NRAS,BRAF in the Prime trial
EXON 1 EXON 2 EXON 4EXON 3
EXON 1 EXON 2 EXON 4EXON 3
RAS Analysis Subset
KRAS90%*
40% 5.8%3.8%
12 13 59 61 117 146
EXON 1 EXON 2 EXON 4EXON 3
EXON 1…. EXON 15 EXON 16…
NRAS
BRAF
RAS/RAF Analysis Subset
90%*3.5% 0%4.1%
8.6%
12 13 59 61 117 146
600
*Tumor sample ascertainment Rate
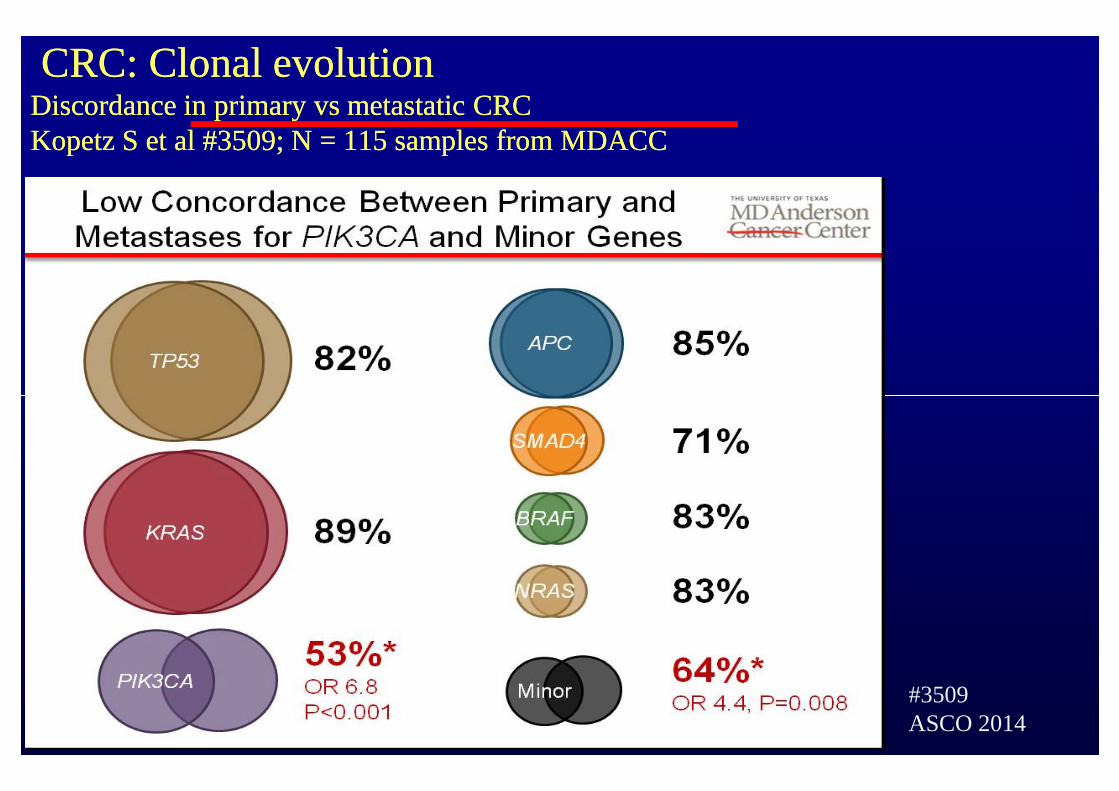
CRC: Clonal evolutionCRC: Clonal evolutionDiscordance in primary vs metastatic CRCDiscordance in primary vs metastatic CRCKopetz S et al #3509; N = 115 samples from MDACCKopetz S et al #3509; N = 115 samples from MDACC
Pestalozzi PostASCO June 12, 2014
#3509ASCO 2014
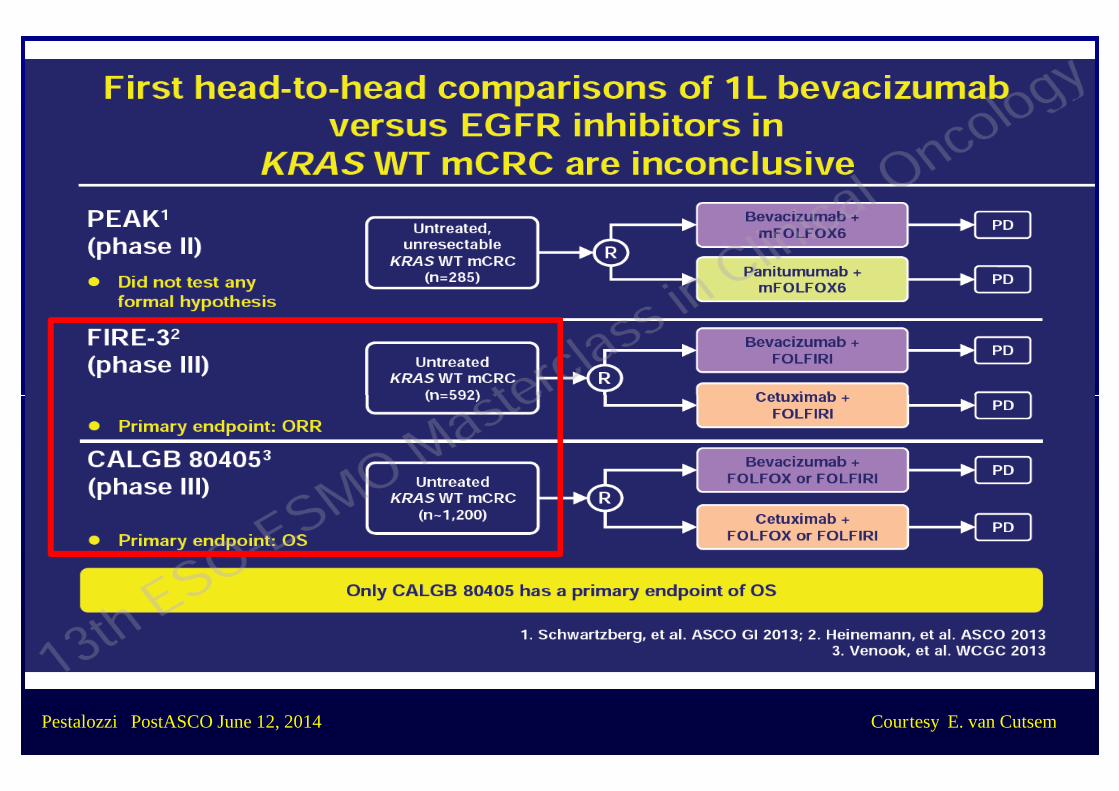
Pestalozzi PostASCO June 12, 2014 Courtesy E. van Cutsem
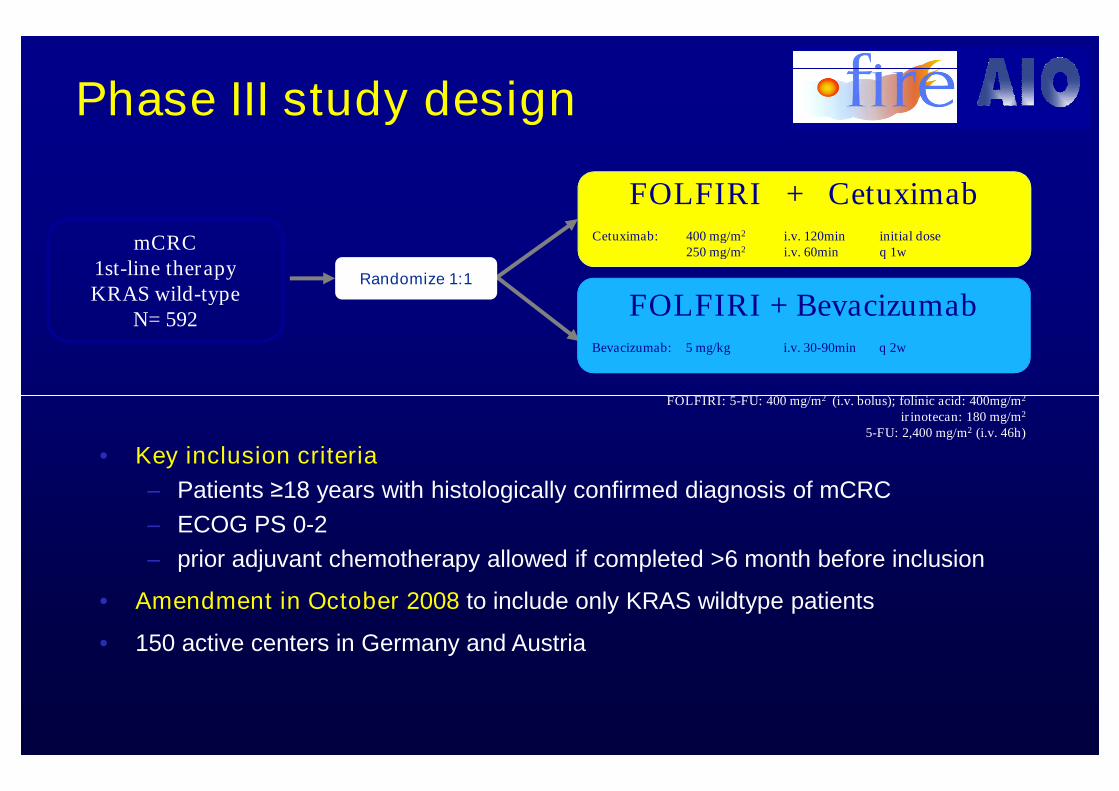
Phase III study design
FOLFIRI + CetuximabCetuximab: 400 mg/m2 i.v. 120min initial dose
250 mg/m2 i.v. 60min q 1w
FOLFIRI + BevacizumabBevacizumab: 5 mg/kg i.v. 30-90min q 2w
mCRC1st-line therapyKRAS wild-type
N= 592
Randomize 1:1
FOLFIRI: 5-FU: 400 mg/m2 (i.v. bolus); folinic acid: 400mg/m2
• Key inclusion criteria
– Patients ≥18 years with histologically confirmed diagnosis of mCRC
– ECOG PS 0-2
– prior adjuvant chemotherapy allowed if completed >6 month before inclusion
• Amendment in October 2008 to include only KRAS wildtype patients
• 150 active centers in Germany and Austria
FOLFIRI: 5-FU: 400 mg/m2 (i.v. bolus); folinic acid: 400mg/m2
irinotecan: 180 mg/m2
5-FU: 2,400 mg/m2 (i.v. 46h)
Primary endpoint
• ORR (mRECIST 1.0, investigators‘ read)
Secondary endpoints
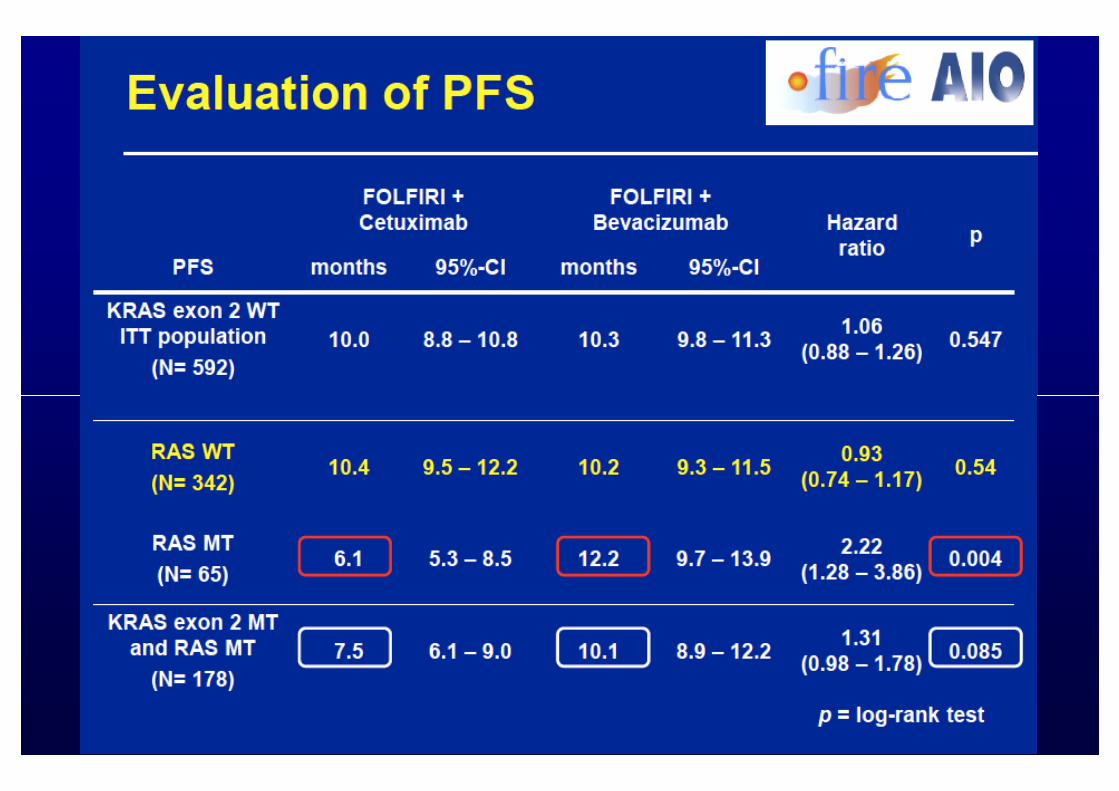
• Progression-free survival (PFS)
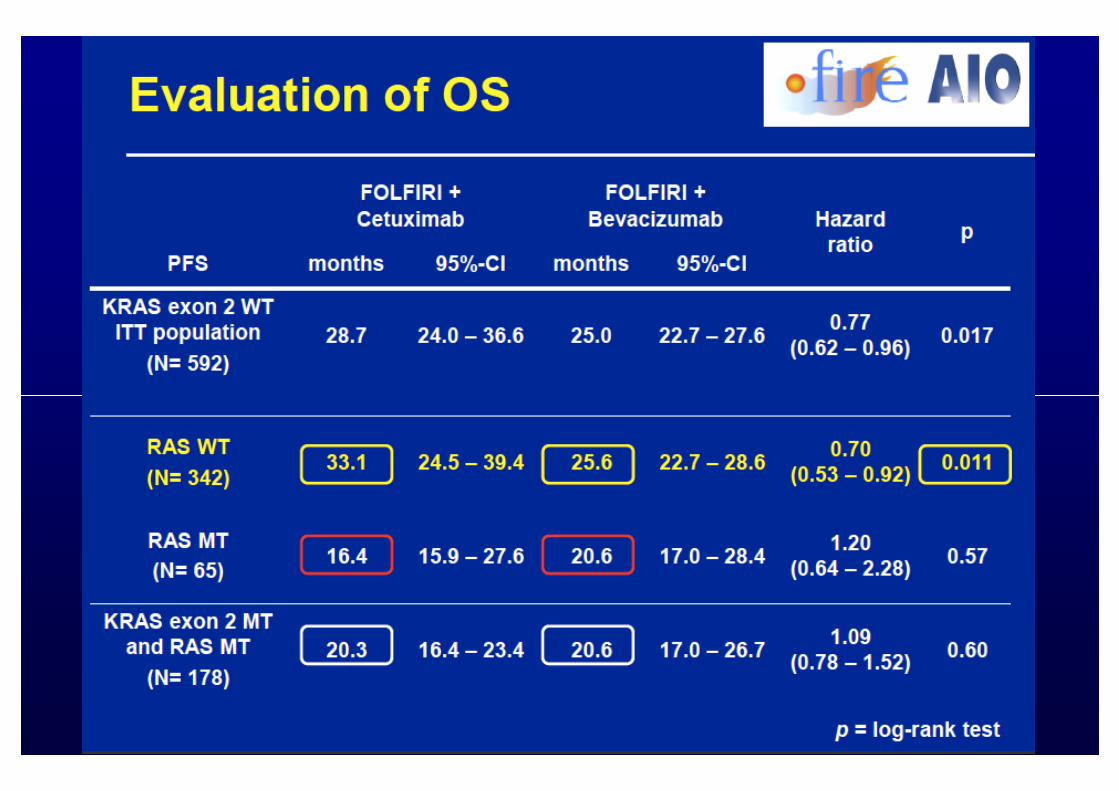
• Overall survival (OS)
Endpoints
• Overall survival (OS)
• Time to failure of strategy (time to failure of 1st-line therapy) (TFS)
• Deepness of response (percent of tumor shrinkage compared to baseline)
• Secondary resections of liver metastases with potentially curative intention
• Safety and tolerability according to NCI-CTCAE criteria
analyses were performed in the ITT and assessable for response population
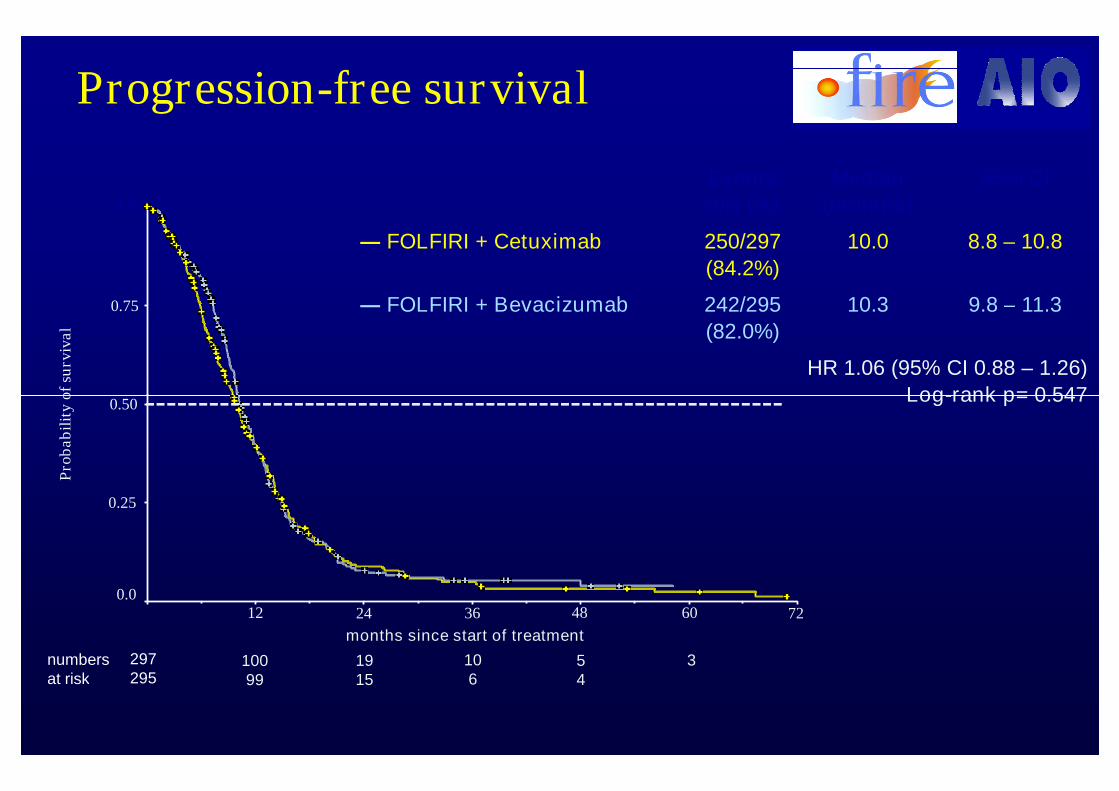
Progression-free survival
0.75
1.0
0.50
Pro
bab
ilit
yof
surv
ival
Events
n/N (%)
Median
(months)
95% CI
― FOLFIRI + Cetuximab 250/297
(84.2%)
10.0 8.8 – 10.8
― FOLFIRI + Bevacizumab 242/295
(82.0%)
10.3 9.8 – 11.3
HR 1.06 (95% CI 0.88 – 1.26)
Log-rank p= 0.5470.50
0.25
12 24 36 48 60 72
months since start of treatment
297295
numbersat risk
10099
1915
106
54
3
0.0
Pro
bab
ilit
yof
surv
ival
Log-rank p= 0.547
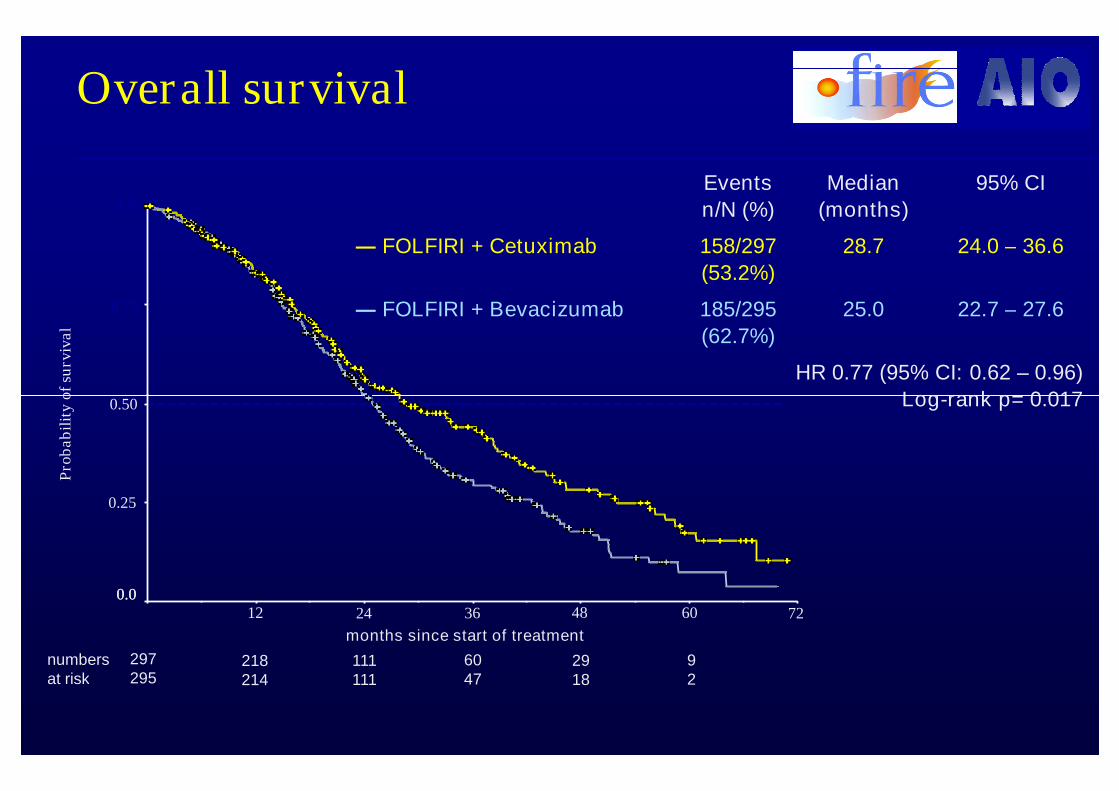
Overall survival
Events
n/N (%)
Median
(months)
95% CI
― FOLFIRI + Cetuximab 158/297
(53.2%)
28.7 24.0 – 36.6
― FOLFIRI + Bevacizumab 185/295
(62.7%)
25.0 22.7 – 27.6
HR 0.77 (95% CI: 0.62 – 0.96)
Log-rank p= 0.017
0.75
1.0
0.50
Pro
bab
ilit
yof
surv
ival
Log-rank p= 0.017
0.012 24 36 48 60 72
months since start of treatment
297295
numbersat risk
218214
111111
6047
2918
92
0.50
0.25
0.0
Pro
bab
ilit
yof
surv
ival
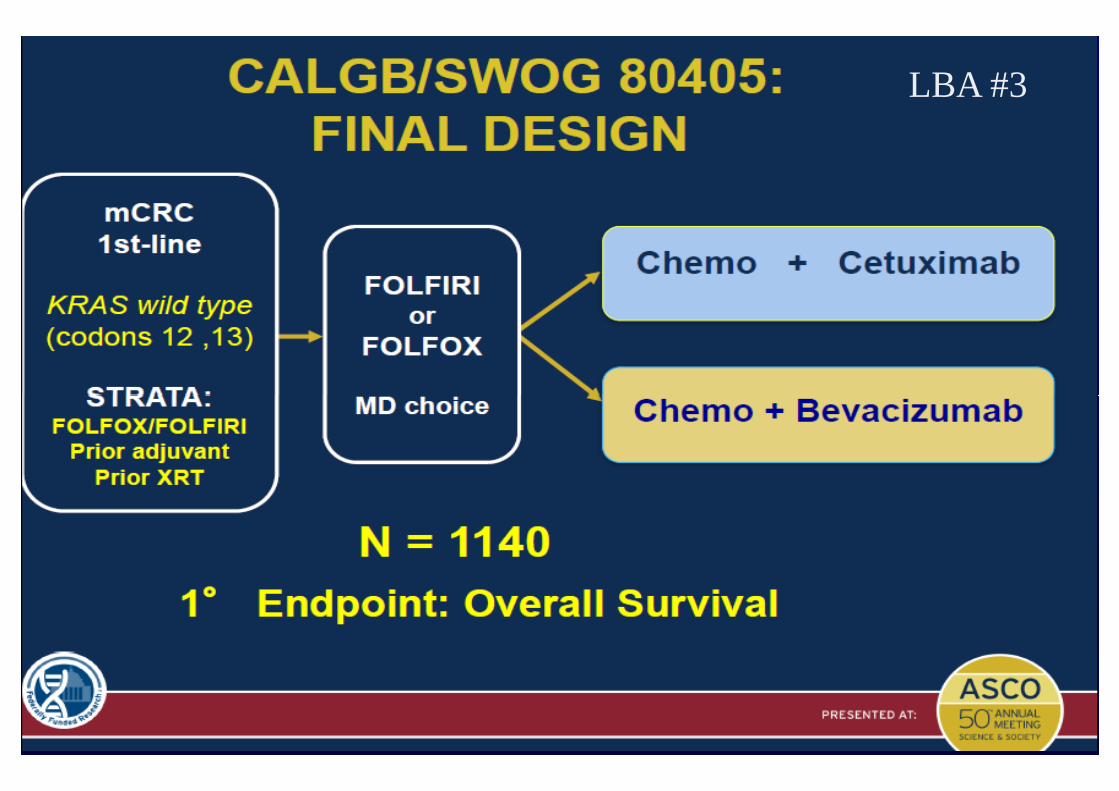
CALGB/SWOG 80405: ConclusionCALGB/SWOG 80405: ConclusionVenook A et al LBA3, Plenary SessionVenook A et al LBA3, Plenary Session
LBA #3LBA #3
Pestalozzi PostASCOJune 12, 2014
36
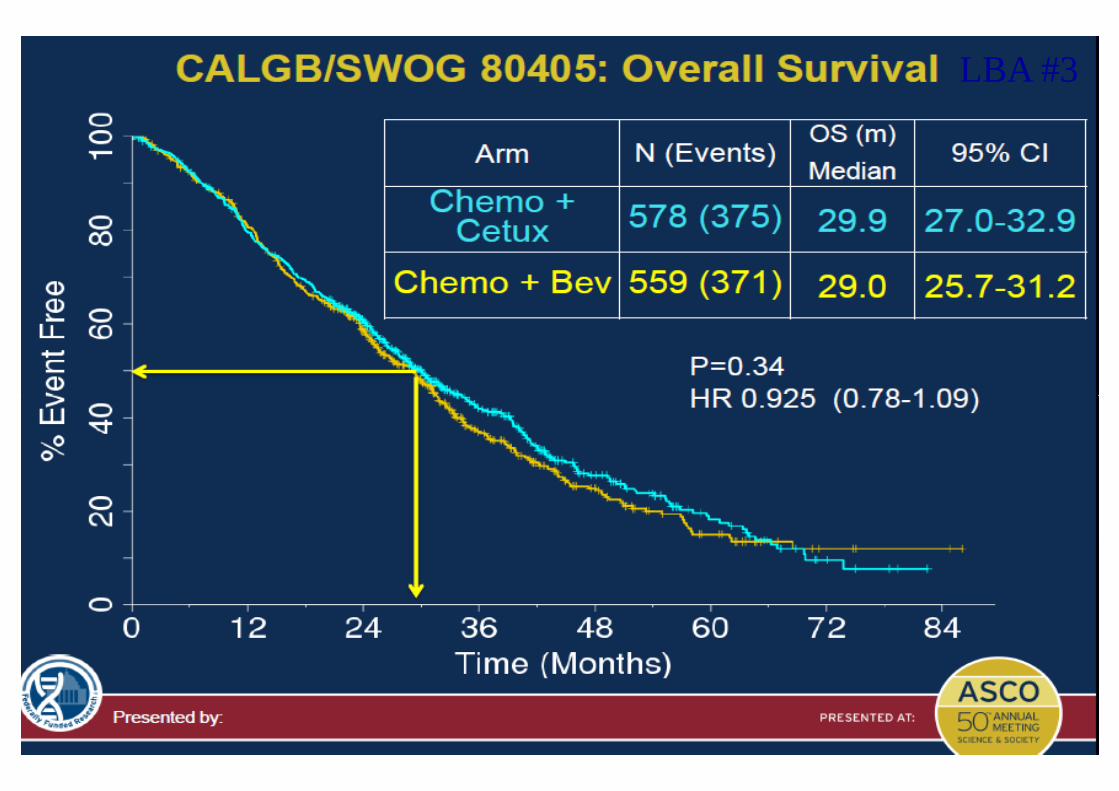
CALGB/SWOG 80405: ConclusionCALGB/SWOG 80405: ConclusionVenook A et al LBA3, Plenary SessionVenook A et al LBA3, Plenary Session
LBA #3
37
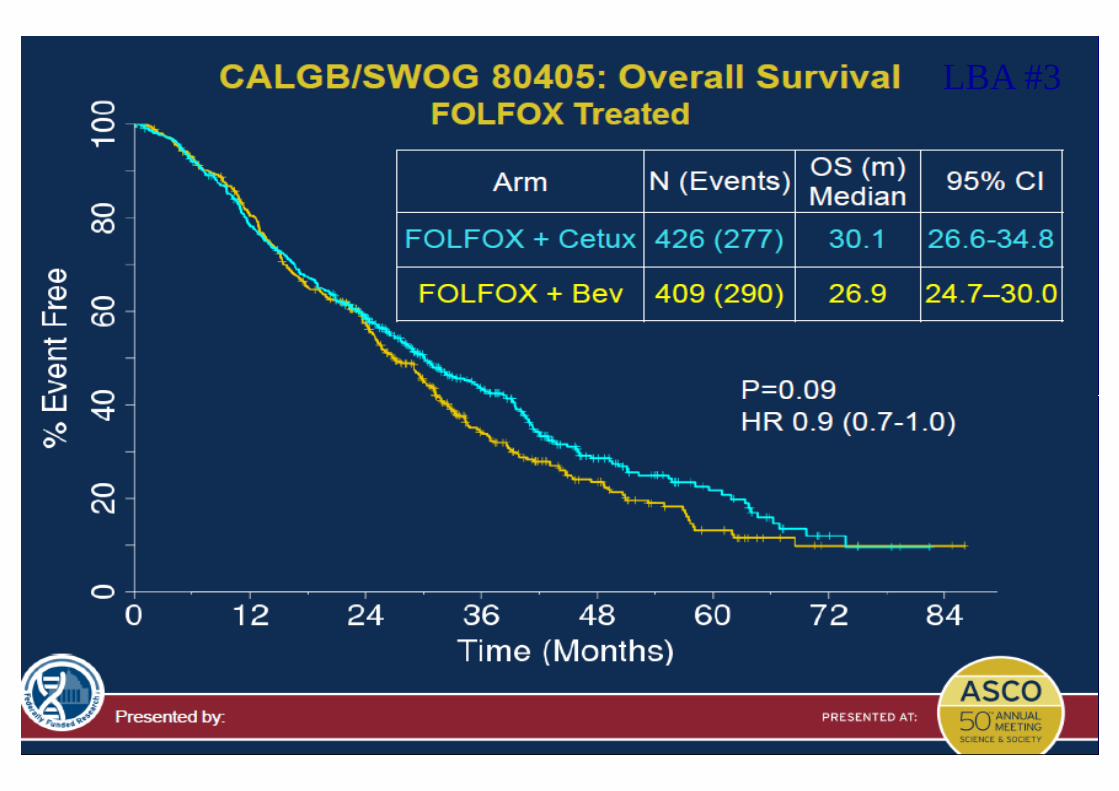
CALGB/SWOG 80405: ConclusionCALGB/SWOG 80405: ConclusionVenook A et al LBA3, Plenary SessionVenook A et al LBA3, Plenary Session
LBA #3
38
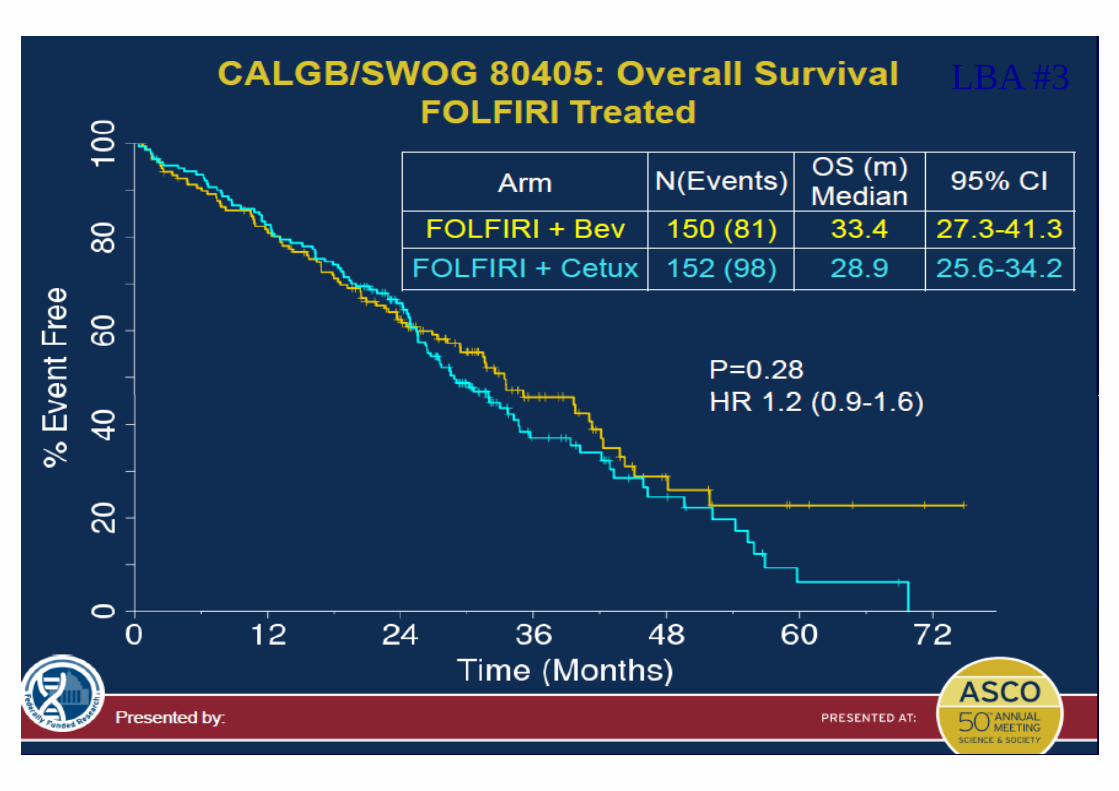
CALGB/SWOG 80405: ConclusionCALGB/SWOG 80405: ConclusionVenook A et al LBA3, Plenary SessionVenook A et al LBA3, Plenary Session
LBA #3
39
CALGB/SWOG 80405: ConclusionCALGB/SWOG 80405: ConclusionVenook A et al LBA3, Plenary SessionVenook A et al LBA3, Plenary Session
LBA #3
40
Second Line DataSecond Line Data
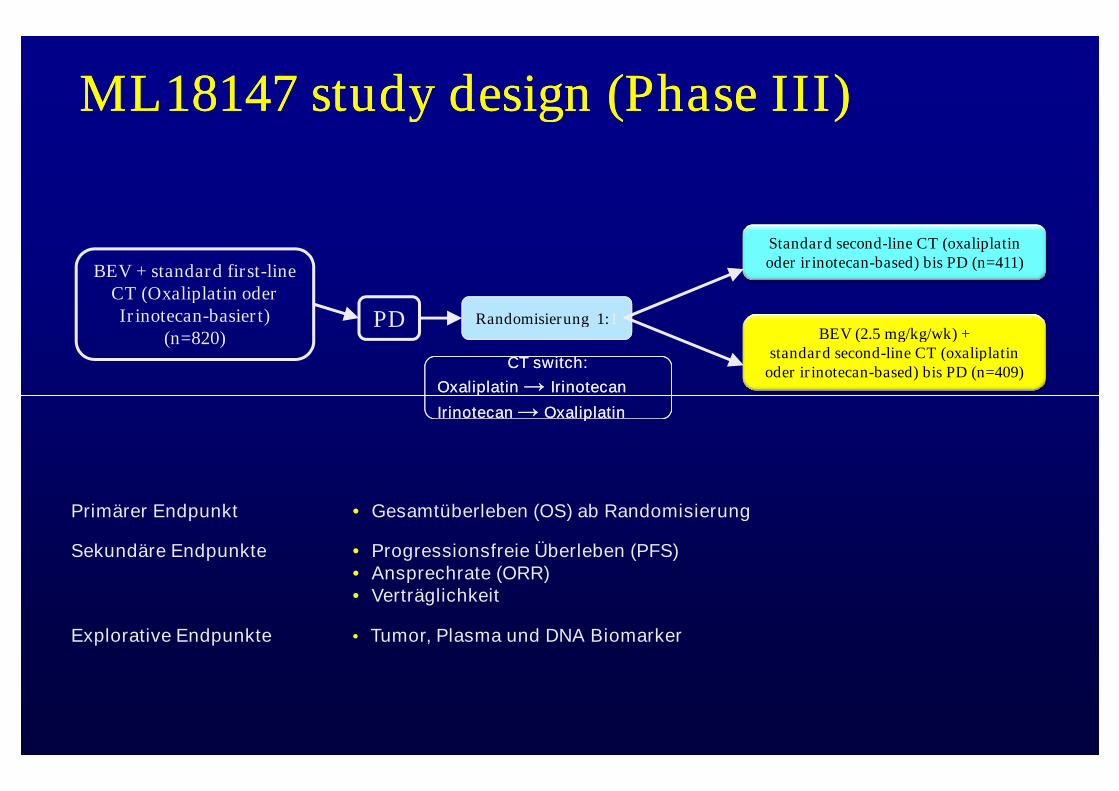
BEV + standard first-lineCT (Oxaliplatin oderIrinotecan-basiert)
(n=820)Randomisierung 1:1
Standard second-line CT (oxaliplatinoder irinotecan-based) bis PD (n=411)
BEV (2.5 mg/kg/wk) +standard second-line CT (oxaliplatin
oder irinotecan-based) bis PD (n=409)
PD
ML18147 study design (Phase III)ML18147 study design (Phase III)
CT switch:
Oxaliplatin → Irinotecan
CT switch:
Oxaliplatin → IrinotecanOxaliplatin → Irinotecan
Irinotecan → Oxaliplatin
Oxaliplatin → Irinotecan
Irinotecan → Oxaliplatin
Primärer Endpunkt • Gesamtüberleben (OS) ab Randomisierung
Sekundäre Endpunkte • Progressionsfreie Überleben (PFS)• Ansprechrate (ORR)• Verträglichkeit
Explorative Endpunkte • Tumor, Plasma und DNA Biomarker
OS
OS
esti
ma
te
1.0
0.8
0.6
PFS
PF
Ses
tim
ate
1.0
0.8
0.6
CT (n=410)BEV + CT (n=409)
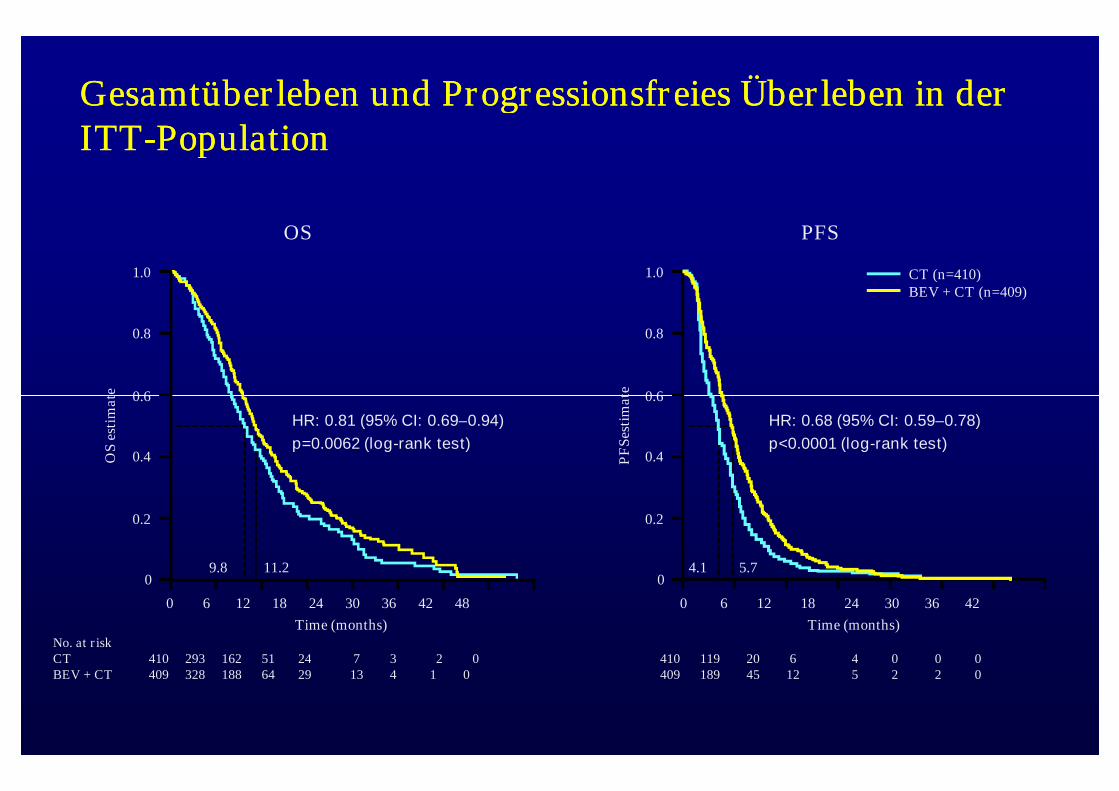
Gesamtüberleben und Progressionsfreies Überleben in derGesamtüberleben und Progressionsfreies Überleben in derITTITT--PopulationPopulation
0 6 12 18 24 30 36 42 48
OS
esti
ma
te
Time (months)
0.6
0.4
0.2
0
No. at riskCT 410 293 162 51 24 7 3 2 0BEV + CT 409 328 188 64 29 13 4 1 0
9.8 11.2
HR: 0.81 (95% CI: 0.69–0.94)
p=0.0062 (log-rank test)
PF
Ses
tim
ate
Time (months)
0.6
0.4
0.2
0
410 119 20 6 4 0 0 0409 189 45 12 5 2 2 0
4.1 5.7
HR: 0.68 (95% CI: 0.59–0.78)
p<0.0001 (log-rank test)
0 6 12 18 24 30 36 42
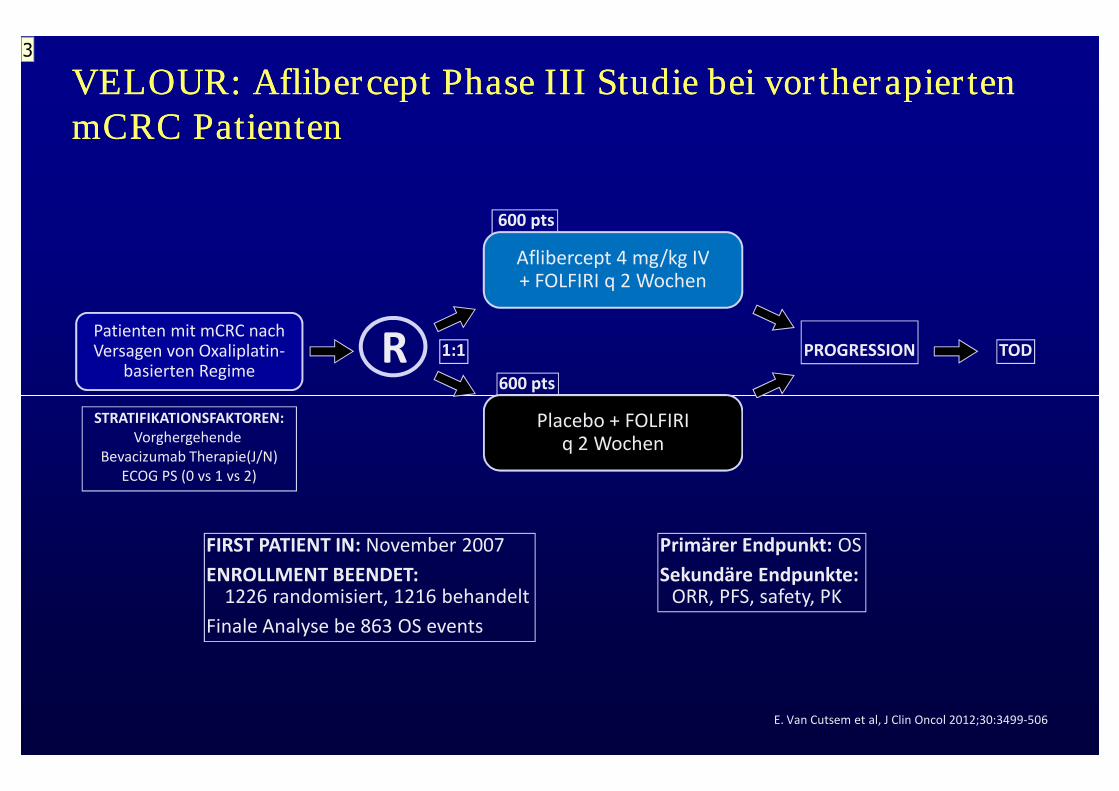
VELOUR: Aflibercept Phase III Studie bei vortherapiertenVELOUR: Aflibercept Phase III Studie bei vortherapiertenmCRC PatientenmCRC Patienten
1:1 PROGRESSION TODPatienten mit mCRC nachVersagen von Oxaliplatin-
basierten RegimeR
600 pts
Aflibercept 4 mg/kg IV+ FOLFIRI q 2 Wochen
600 pts
Primärer Endpunkt: OS
Sekundäre Endpunkte:ORR, PFS, safety, PK
FIRST PATIENT IN: November 2007
ENROLLMENT BEENDET:1226 randomisiert, 1216 behandelt
Finale Analyse be 863 OS events
STRATIFIKATIONSFAKTOREN:Vorghergehende
Bevacizumab Therapie(J/N)ECOG PS (0 vs 1 vs 2)
Placebo + FOLFIRIq 2 Wochen
E. Van Cutsem et al, J Clin Oncol 2012;30:3499-506
3
Slide 44
3 UebersetzungRoger von Moos; 13.10.2013
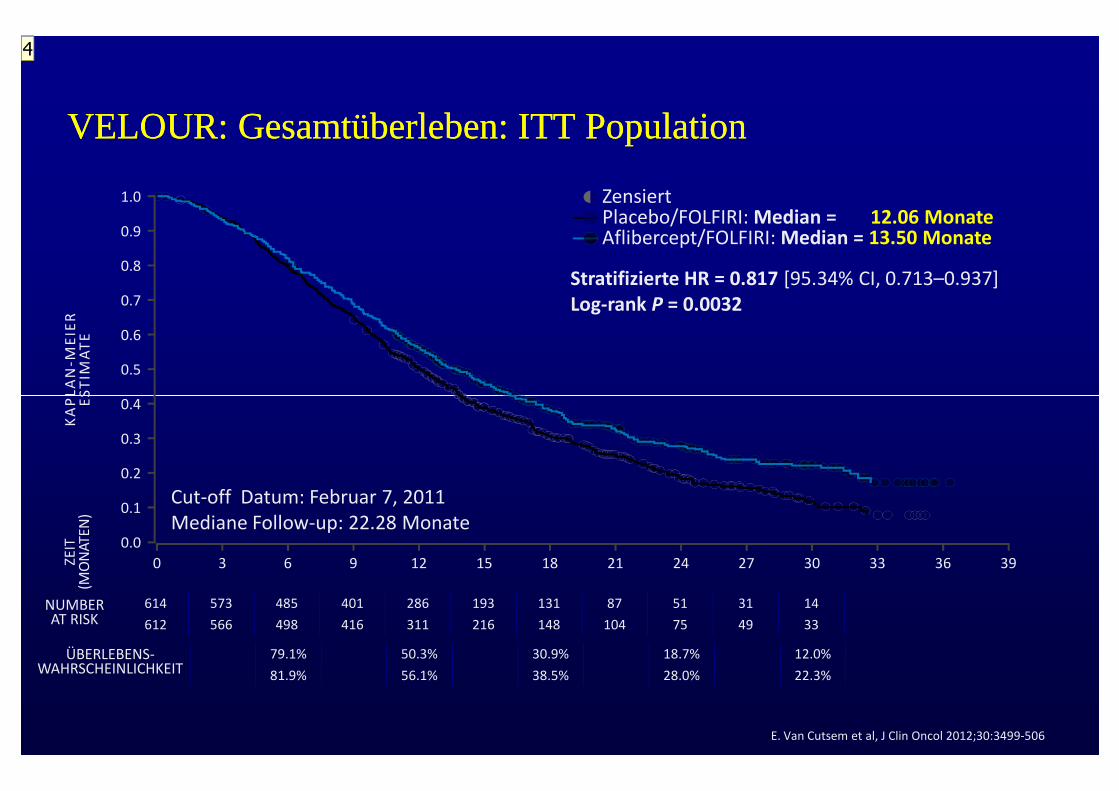
VELOUR: Gesamtüberleben: ITT PopulationVELOUR: Gesamtüberleben: ITT Population
1.0
0.9
0.8
0.7
0.6
0.5
0.4
KA
PL
AN
-ME
IER
ES
TIM
AT
E
Stratifizierte HR = 0.817 [95.34% CI, 0.713–0.937]Log-rank P = 0.0032
Zensiert
Aflibercept/FOLFIRI: Median = 13.50 MonatePlacebo/FOLFIRI: Median = 12.06 Monate
614 573 485 401 286 193 131 87 51 31 14
612 566 498 416 311 216 148 104 75 49 33
0 3 6 9 12 15 18 21 24 27 30 33 36 39
0.4
0.3
0.2
0.1
0.0
KA
PL
AN
ES
TIM
AT
E
NUMBERAT RISK
ZEIT
(MO
NAT
EN)
Cut-off Datum: Februar 7, 2011Mediane Follow-up: 22.28 Monate
79.1% 50.3% 30.9% 18.7% 12.0%
81.9% 56.1% 38.5% 28.0% 22.3%
ÜBERLEBENS-WAHRSCHEINLICHKEIT
E. Van Cutsem et al, J Clin Oncol 2012;30:3499-506
4
Slide 45
4 Hier müssten Farben angepasst werden und UebersetzungRoger von Moos; 13.10.2013
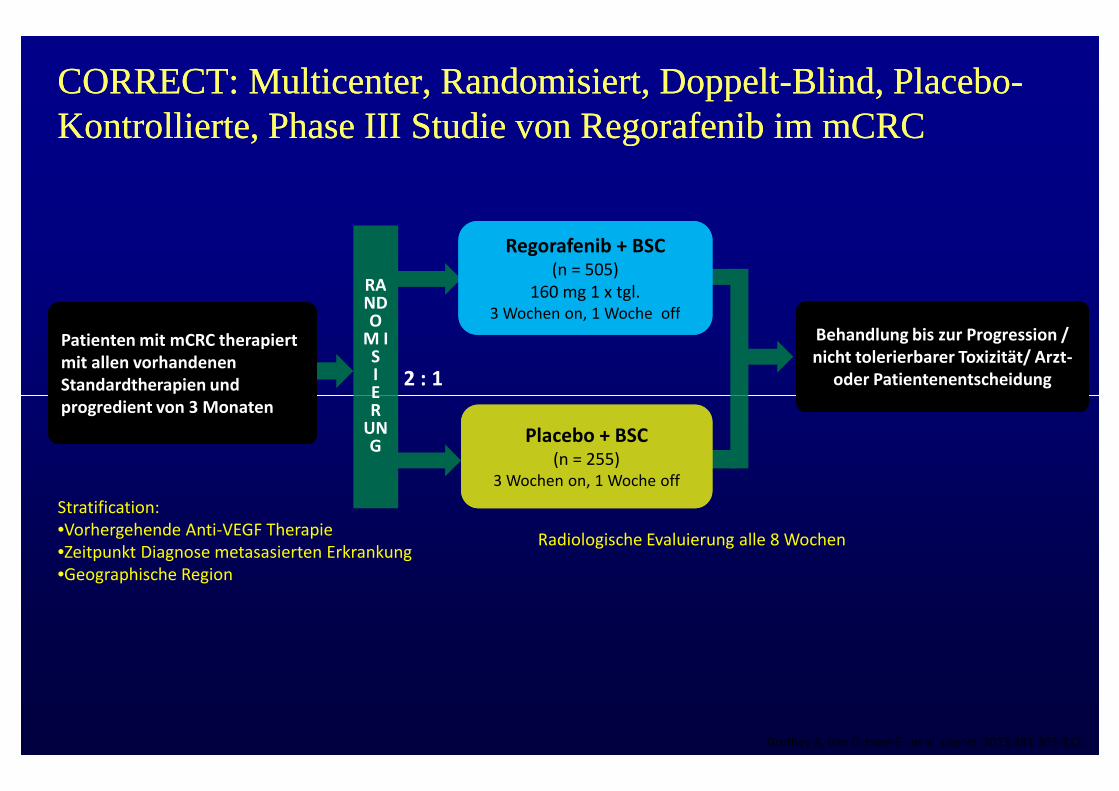
CORRECT: Multicenter, Randomisiert, DoppeltCORRECT: Multicenter, Randomisiert, Doppelt--Blind, PlaceboBlind, Placebo--Kontrollierte, Phase III Studie von Regorafenib im mCRCKontrollierte, Phase III Studie von Regorafenib im mCRC
Behandlung bis zur Progression /nicht tolerierbarer Toxizität/ Arzt-
oder Patientenentscheidung
Behandlung bis zur Progression /nicht tolerierbarer Toxizität/ Arzt-
oder Patientenentscheidung2 : 1
Regorafenib + BSC(n = 505)
160 mg 1 x tgl.3 Wochen on, 1 Woche off
Regorafenib + BSC(n = 505)
160 mg 1 x tgl.3 Wochen on, 1 Woche off
RANDO
M ISIE
Patienten mit mCRC therapiertmit allen vorhandenenStandardtherapien undprogredient von 3 Monaten
Patienten mit mCRC therapiertmit allen vorhandenenStandardtherapien undprogredient von 3 Monaten
Radiologische Evaluierung alle 8 Wochen
Grothey A, Van Cutsem E , et al. Lancet. 2013;381:303-312..
Placebo + BSC(n = 255)
3 Wochen on, 1 Woche off
Placebo + BSC(n = 255)
3 Wochen on, 1 Woche off
ER
UNG
progredient von 3 Monatenprogredient von 3 Monaten
Stratification:•Vorhergehende Anti-VEGF Therapie•Zeitpunkt Diagnose metasasierten Erkrankung•Geographische Region
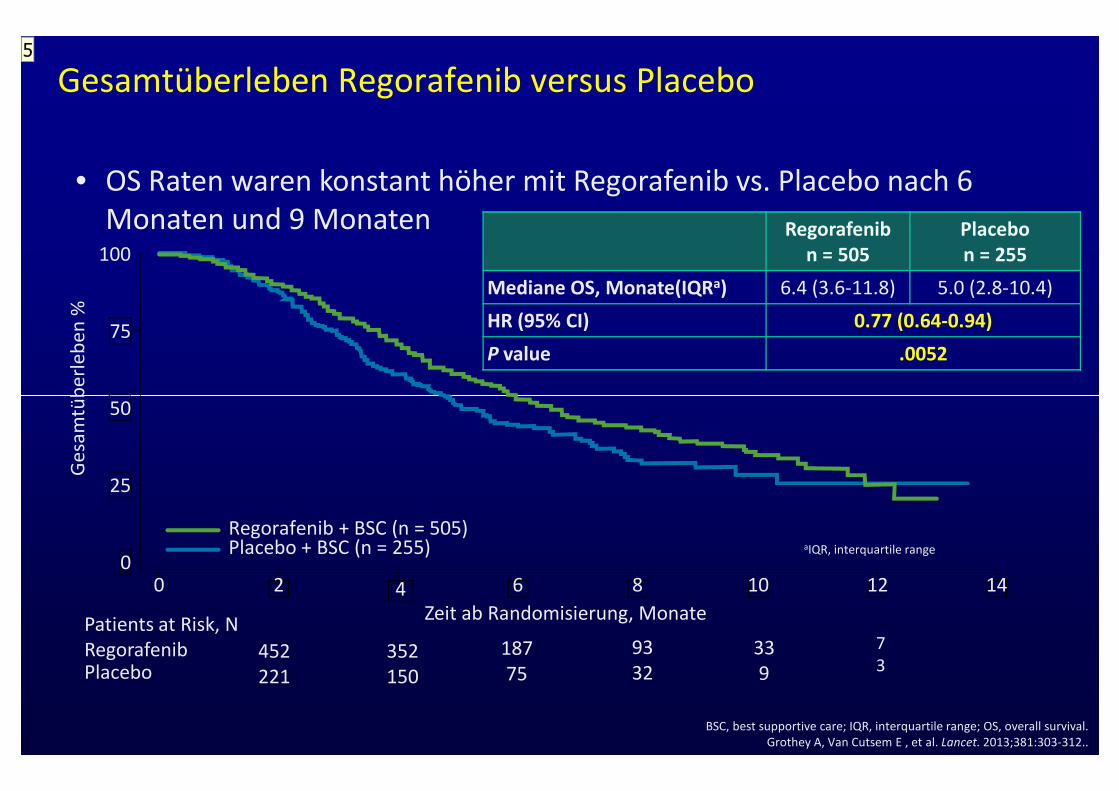
Regorafenibn = 505
Placebon = 255
Mediane OS, Monate(IQRa) 6.4 (3.6-11.8) 5.0 (2.8-10.4)
HR (95% CI) 0.77 (0.64-0.94)
P value .0052
100
75
50
Ge
sam
tüb
erl
eb
en
%Gesamtüberleben Regorafenib versus Placebo
• OS Raten waren konstant höher mit Regorafenib vs. Placebo nach 6Monaten und 9 Monaten
PlaceboRegorafenibPatients at Risk, N
452221
352150
18775
9332
339
73
Zeit ab Randomisierung, Monate
aIQR, interquartile range0
0 6 10 14842 12
Regorafenib + BSC (n = 505)Placebo + BSC (n = 255)
50
25
Ge
sam
tüb
erl
eb
en
%
BSC, best supportive care; IQR, interquartile range; OS, overall survival.Grothey A, Van Cutsem E , et al. Lancet. 2013;381:303-312..
5
Slide 47
5 Bitte alles auf deusch übersetzenRoger von Moos; 13.10.2013
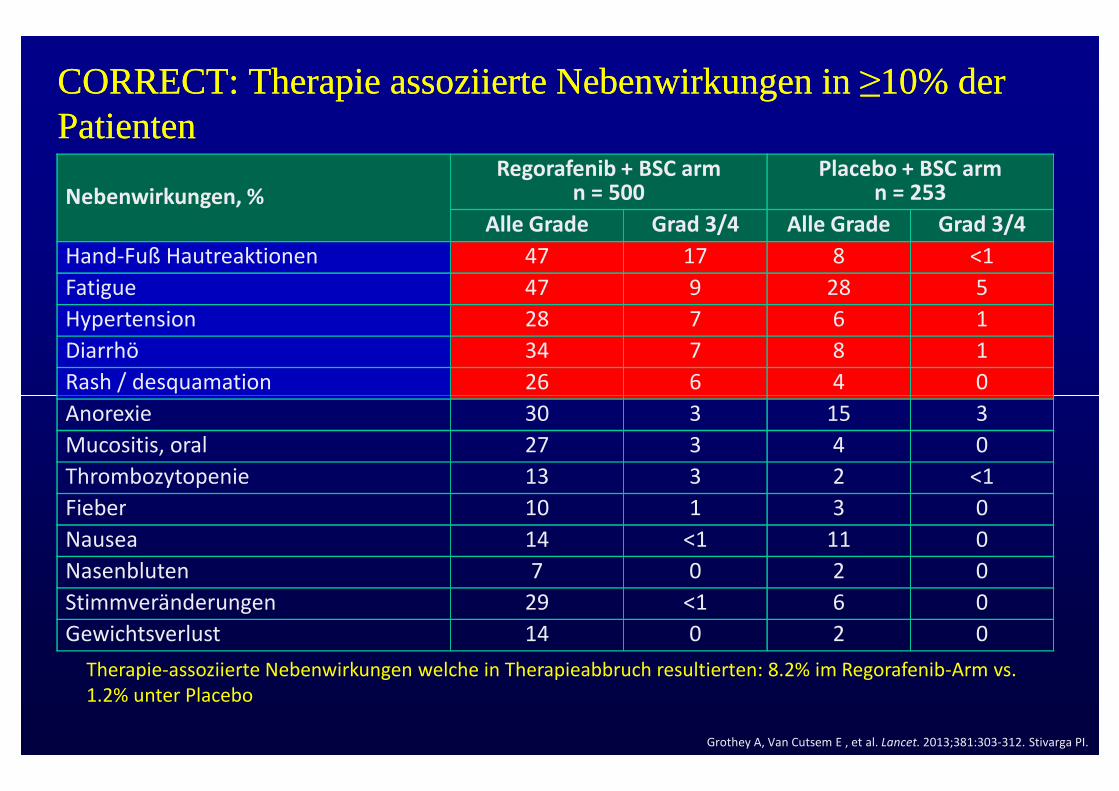
CORRECT: Therapie assoziierte Nebenwirkungen in ≥10% derCORRECT: Therapie assoziierte Nebenwirkungen in ≥10% derPatientenPatienten
Nebenwirkungen, %Regorafenib + BSC arm
n = 500Placebo + BSC arm
n = 253
Alle Grade Grad 3/4 Alle Grade Grad 3/4
Hand-Fuß Hautreaktionen 47 17 8 <1
Fatigue 47 9 28 5
Hypertension 28 7 6 1
Diarrhö 34 7 8 1
Rash / desquamation 26 6 4 0
Anorexie 30 3 15 3
Mucositis, oral 27 3 4 0
Thrombozytopenie 13 3 2 <1
Fieber 10 1 3 0
Nausea 14 <1 11 0
Nasenbluten 7 0 2 0
Stimmveränderungen 29 <1 6 0
Gewichtsverlust 14 0 2 0
Grothey A, Van Cutsem E , et al. Lancet. 2013;381:303-312. Stivarga PI.
Therapie-assoziierte Nebenwirkungen welche in Therapieabbruch resultierten: 8.2% im Regorafenib-Arm vs.1.2% unter Placebo
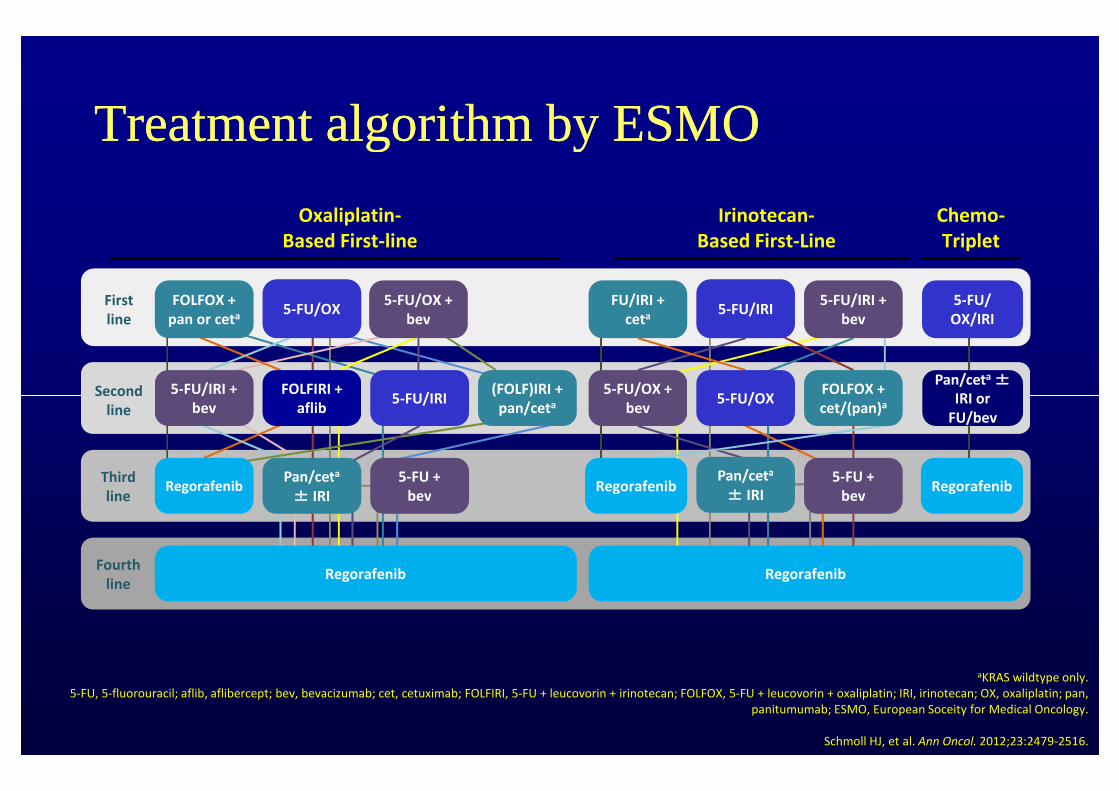
Treatment algorithm by ESMOTreatment algorithm by ESMO
Oxaliplatin-Based First-line
Irinotecan-Based First-Line
Chemo-Triplet
5-FU/IRI + 5-FU/OX +
5-FU/OX +bev
FOLFOX +pan or ceta
(FOLF)IRI +
FU/IRI +ceta5-FU/OX
5-FU/OX5-FU/IRI
5-FU/IRI5-FU/OX/IRI
Pan/ceta ±IRI or
FOLFIRI +
Firstline
Second
5-FU/IRI +bev
FOLFOX +
Regorafenib
Regorafenib RegorafenibPan/ceta
± IRI5-FU +
bev5-FU +
bev
5-FU/IRI +bev
5-FU/OX +bev
(FOLF)IRI +pan/ceta 5-FU/OX5-FU/IRI IRI or
FU/bev
FOLFIRI +aflib
Secondline
Thirdline
Fourthline
Regorafenib
FOLFOX +cet/(pan)a
aKRAS wildtype only.5-FU, 5-fluorouracil; aflib, aflibercept; bev, bevacizumab; cet, cetuximab; FOLFIRI, 5-FU + leucovorin + irinotecan; FOLFOX, 5-FU + leucovorin + oxaliplatin; IRI, irinotecan; OX, oxaliplatin; pan,
panitumumab; ESMO, European Soceity for Medical Oncology.
Schmoll HJ, et al. Ann Oncol. 2012;23:2479-2516.
Pan/ceta
± IRI
Regorafenib
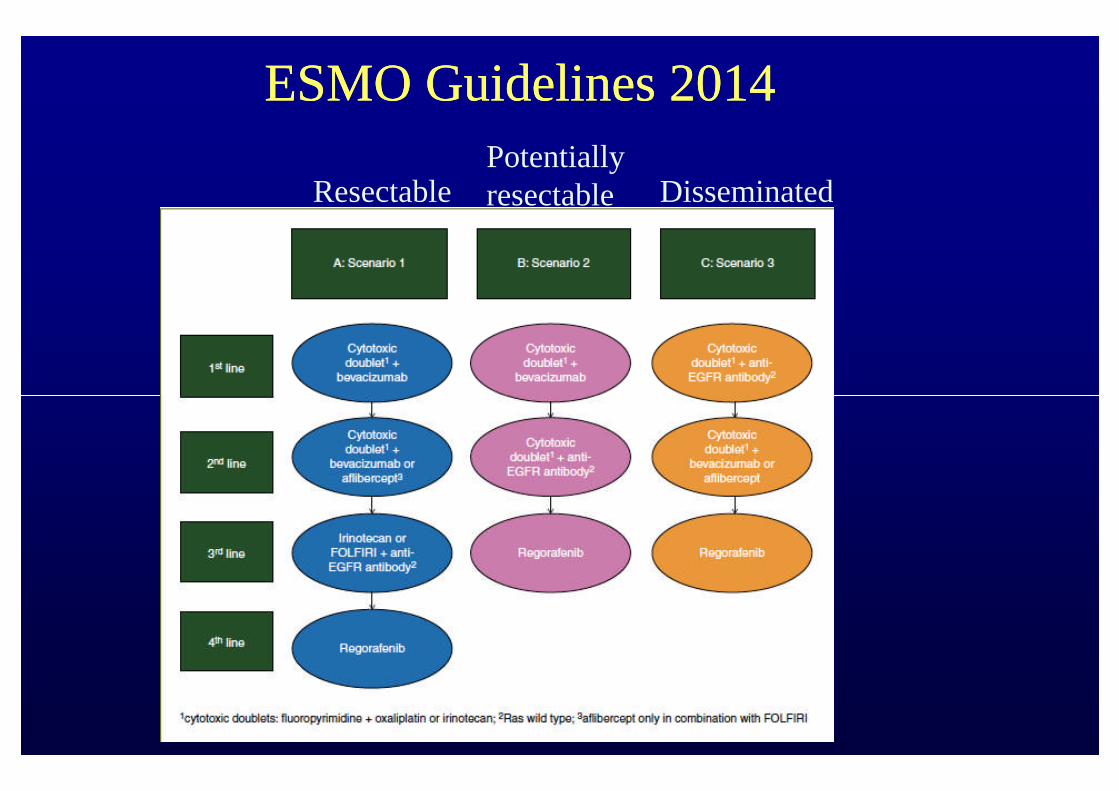
ESMO Guidelines 2014ESMO Guidelines 2014
ResectablePotentiallyresectable Disseminated
ConclusionConclusion Full RAS and BRAF analysis is necessary in all patients who are candidate forFull RAS and BRAF analysis is necessary in all patients who are candidate for
systemic treatmentsystemic treatment
Irinotecan and Oxaliplatin regimens are both effective in first and second lineIrinotecan and Oxaliplatin regimens are both effective in first and second line
Capecitabine as monotherapy is an alternative for patients not tolerating aCapecitabine as monotherapy is an alternative for patients not tolerating acombination chemotherapycombination chemotherapy
In RAS wild type patients, EGFR antibodies seems to be more effective thanIn RAS wild type patients, EGFR antibodies seems to be more effective thanbevacizumab (lets wait for new data at ESMO in 2 weeks)bevacizumab (lets wait for new data at ESMO in 2 weeks)
Good data for Bevacizumab are available for RAS mutant, and second lineGood data for Bevacizumab are available for RAS mutant, and second linetreatmenttreatment
The TML showed a survival benefit for patients treated with Bevacizumab inThe TML showed a survival benefit for patients treated with Bevacizumab infirst and second linefirst and second line
Aflibercept has shown acitivity in second line therapyAflibercept has shown acitivity in second line therapy
Patients in good condition are candidates for further line treatment withPatients in good condition are candidates for further line treatment withRegorafenibRegorafenib

![Welcome [] · Pronzato. SAMO 2013, Nice. Thierry Mara SAMO 2016, Reunion Island, Université de La Réunion, celebrating the 90th birthday of Ilya M. Sobol’](https://img.pdfslide.us/doc/110x75/5eb4fbbdf6f27f19976506a1/welcome-pronzato-samo-2013-nice-thierry-mara-samo-2016-reunion-island-universit.jpg)