Embed Size (px)
Citation preview

How should CLL with del 17pbe treated?
SAMO InterdisciplinaryWorkshop on Lymphoma,
14th and 15th November 2014,Hotel Hermitage, Lucerne
be treated?
Michael Gregor
Division of Hematology

Selection of initial therapy for symptomaticor advanced chronic lymphocytic leukemiaHigh-risk disease: del(17p) or TP53 mutations
“The appropriate treatment for patients withdel(17p) remains undefined at this time.”

Outline
• del 17p and TP53 mutation
• prognosis of patients with deletion 17p / TP53mut
• results of current conventional treatments
– FCR, Alemtuzumab, Ofatumumab– FCR, Alemtuzumab, Ofatumumab
– allogeneic stem cell transplantation
• new treatment options
– Ibrutinib, Idelalisib, ABT199
• how to treat patients with deletion 17p / TP53mut

Deletion 17p, TP53 mutation, p53 protein.
Tumor protein p53, also known as p53, is a protein that isencoded by the TP53 genein humans . TP53 gene is locatedon the short arm of chromosome 17 (17p13.1).
The p53 protein is crucial in multicellular organismsregulating the cell cycle. P53 has been called "the guardianregulating the cell cycle. P53 has been called "the guardianof the genome" because of its role in conserving geneticstability by preventing genome mutation.
If p53 function is lost, tumor suppression is compromised.
Tumors with p53 dysfunction frequently have bad prognosisdue to poor response to antineoplastic treatment.

TP53 mutation and deletion 17p.
Zenz T et al. Chronic lymphocytic leukemia and treatment resistance in cancer: the role of the p53 pathway.Cell Cycle. 2008; 7:3810-4.

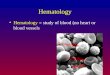
Expansion of TP53 mutated subclones.
Dearden C. CLLonal selection: survival of the fittest? Blood. 2014 ; 123:2130-1
.
Clonal selection and expansion of TP53-mutated subclones during the clinicalcourse of CLL. Yellow circles indicate the TP53-mutated CLL cell which expandsthrough the disease course from below the level of conventional detectionmethods at diagnosis to become the dominant population in refractory disease.Blue circles indicate the non-TP53–mutated CLL cell which is the dominant cloneat diagnosis but is subsequently replaced by the TP53-mutated subclone.
CLL patients with TP53 mutations or deletion 17p probably shouldn’tbe treated with standard chemo- or chemoimmunotherapy!

TP53 mutation and deletion 17p.
Patients with CLL needing treatment should be tested for
- Deletion 17p by FISHAND
- TP53 mutation (variety of methods, mutation should beconfirmed by Sanger sequencing)*
Patients with CLL and deletion 17p and / or TP53 mutation(probably) shouldn’t have treatment with standardchemotherapy or chemoimmunotherapy.
* Pospisilova S et al. ERIC recommendations on TP53 mutation analysis in chronic lymphocytic leukemia.Leukemia 2012; 26, 1458-1461.

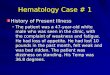
CLL: FISH and Prognosis
Döhner H et al. Genomic aberrations and survival in chronic lymphocytic leukemia.N Engl J Med 2000;343:1910-6.
CLL patients with deletion 17p are arather small group with a poor prognosis!

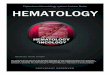
CLL: TP53 and Prognosis
• GCLLSH CLL4 (F vs. FC)
• TP53 mutations in 8.5% of patients (28 of 328 patients).
• None of the patients with TP53 mutation had a CR.
del 17p (N=15)TP53 mut, no del 17p (N=13)
Zenz T. et al. TP53 Mutation and Survival in Chronic Lymphocytic Leukemia.J Clin Oncol 2010; 28: 4473-4479.
TP53 mut, no del 17p (N=13)neither (N=260)
CLL patients with TP53 mutations have the same poor prognosis withchemotherapy like patients with deletion 17p!

Genetic risk groups in CLL8
GCLLSG CLL8: FC vs. FCR first-line in fit patients
FC FCR
Hallek M et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocyticleukaemia: a randomised, open-label, phase 3 trial. Lancet 2010; 376: 1164–74.
.
Also patients with deletion 17p profit from the addition of rituximab.But they still have a poor response (ORR FC 34%, FCR 68%; CR FC0%, FCR 5%; PFS@3y FC 0%, FCR 18%; OS@3y FC 37%, FCR 38%.)

Alemtuzumab in CLL 1st-lineRCT: 297 patients, 149 alemtuzumab (A) and 148 chlorambucil (Clb).ORR: A 83% (24% CR) versus Clb 55% (2% CR) (P <0.0001).PFS: A 14.6 months versus Clb 11.7 months (P = 0.0001).TTNT: A 23.3 months versus Clb 14.7 months (HR 0.54; P <0.0001).
Hillmen P et al. Alemtuzumab Compared With Chlorambucil As First-Line Therapy for Chronic LymphocyticLeukemia. J Clin Oncol 2007; 25: 5616-5623
Patients with deletion 17p:Alemtuzumab (N=11) ORR 64%, PFS 10.7mChlorambucil (N=10) ORR 20%, PFS 2.2months

Alemtuzumab s.c. in rel/refr CLLPhase II: 109 patients, no response to F or relapse within 6 months.ORR 34% (CR 4%). PFS median 7.7 months. OS median 19.1 months.
del 11q(N=20)del 17p (N=31)other (N=49)
Stilgenbauer S et. al. Subcutaneous Alemtuzumab in Fludarabine-Refractory Chronic Lymphocytic Leukemia:Clinical Results and Prognostic Marker Analyses From the CLL2H Study of the German Chronic Lymphocytic
Leukemia Study Group. J Clin Oncol 2009; 27: 3994-4001.
Patients with F-refractory CLL treated with alemtuzumab have the sameprognosis independent of cytogenetic subgroup.

Alemtuzumab + HDMPPhase II: 39 patients with TP53-deleted CLL (17 untreated and 22previously treated) up to 16 weeks alemtuzumab 30 mg i.v./s.c. TIWand methylprednisolone 1.0g/m2 i.v. x 5d every 5 weeks.
All patients: ORR 85%, CR 36%, 11.8 months, and 23.5untreated: ORR 88%, CR 65%, PFS 18.3 months, OS 38.9 months,treated: ORR 77%, CR 14%, PFS 6.5 months, OS 19.5 months.
Pettitt AR et al. Alemtuzumab in Combination With Methylprednisolone Is a Highly Effective Induction Regimenfor Patients With Chronic Lymphocytic Leukemia and Deletion of TP53: Final Results of the National Cancer
Research Institute CLL206 Trial. J Clin Oncol 2012; 30: 1647-1655. .
treated: ORR 77%, CR 14%, PFS 6.5 months, OS 19.5 months.

Alemtuzumab + HDMP
Pettitt AR et al. Alemtuzumab in Combination With Methylprednisolone Is a Highly Effective Induction Regimenfor Patients With Chronic Lymphocytic Leukemia and Deletion of TP53: Final Results of the National Cancer
Research Institute CLL206 Trial. J Clin Oncol 2012; 30: 1647-1655. .
Grade 3 to 4 hematologic and glucocorticoid-associated toxicityoccurred in 67% and 23% of patients, respectively. Grade 3 to 4infection occurred in 51% of the overall cohort and in 29% of patientsless than 60 years of age. Treatment-related mortality was 5%.
Alemtuzumab plus methypredisolone is the most effective inductionregimen reported in TP53-deleted CLL but associated with toxicity.

Alemtuzumab s.c. + Dexa
131 patients in three cohorts: 17p- 1st line, 17p- relapsed (notrefractory) and refractory to F-based therapy or similar.Alemtuzumab s.c. (30mg, 3x weekly) + Dexa (40 mg d 1-4 and 15-18),prophylactic pegfilgrastim 6 mg on days 1 and 15,3 cycles, followed by either allo-SCT or A maintenance (30mg q2w).
Parameter 17p- 1st line 17p- relapsed F-refractory
Stilgenbauer S et al. Alemtuzumab Combined with Dexamethasone, Followed By Alemtuzumab Maintenanceor Allo-SCT in “ultra High-risk” CLL: Final Results from the CLL2O Phase II Study. ASH 2014 abstract 1991.
Parameter 17p- 1st line 17p- relapsed F-refractory
Number of patients 42 28 61
Median age (yrs) 66.5 64 66
17p- (%) 100 100 49
Prior lines (median) n.a. 2 3
Prior rituximab (%) n.a. 71 93
ORR (%) 97 79 69
CR (%) 21 4 3
Median PFS (mo) 32.8 10.3 9.7
Median OS (mo) >60.0 21.4 17.3

Alemtuzumab s.c. + Dexa
Toxicity was variable depending on line of therapy and pretreatment.Although CMV reactivation ocurred, CMV infection wasn’t frequent.
Grade III / IV adverse events:
Parameter 17p- 1st line 17p- relapsed F-refractory
Number of patients 42 28 61
Stilgenbauer S et al. Alemtuzumab Combined with Dexamethasone, Followed By Alemtuzumab Maintenanceor Allo-SCT in “ultra High-risk” CLL: Final Results from the CLL2O Phase II Study. ASH 2014 abstract 1991.
Number of patients 42 28 61
All AEs (%) 36 43 50
Neutropenia (%) 24 36 67
Anemia (%) 14 36 21
Thrombocytopenia (%) 12 39 31
Non-CMV infection (%) 19 36 36
CMV infection (%) 7 0 2

Alemtuzumab s.c. + Dexa
Stilgenbauer S et al. Alemtuzumab Combined with Dexamethasone, Followed By Alemtuzumab Maintenanceor Allo-SCT in “ultra High-risk” CLL: Final Results from the CLL2O Phase II Study. ASH 2014 abstract 1991.
The combination of Alemtuzumab and Dexamethasone, followedby maintenance or allo-SCT showed high response rates in “ultra high-risk” CLL with expected toxicity. For 17p- 1st line treatment, the resultscompare favorably to FCR (CLL8: ORR 68%, median PFS 11.3 mo).Allo-SCT appears to offer superior disease control in eligible patientsdespite prior A exposure. Overall, this trial may serve as a benchmarkfor comparison of novel agents in “ultra high-risk” CLL.

Ofatumummab in rel/refr CLLPhase II: 138 patients with Fludarabine and Alemtuzumab-refractoryCLL (n=59) and bulky Fludarabine-refractory CLL (n=79).
Wierda WG et al. Ofatumumab As Single-Agent CD20 Immunotherapy in Fludarabine-Refractory ChronicLymphocytic Leukemia. J Clin Oncol 2010; 28: 1749-1755.
Patients with del 17p:FA-ref N=17 ORR 41% . BF-ref N=14 ORR 14%.
ORR FA-ref 58% and BF-ref 47%.PFS FA-ref 5.7 months and BF-ref 5.9 months.OS FA-ref 13.7 months and BF-ref 15.5 months.

Allogeneic SCT in CLL
Dreger P et al. Allogeneic stem cell transplantation provides durable disease control in poor-risk chroniclymphocytic leukemia: long-term clinical and MRD results of the GCLLSG CLL3X trial.
Blood. 2010;116:2438-2447.
Allogeneic SCT is a curative therapy in CLL patients, independent of del17p. At transplnat the disease shouldn’t be bulky or refractory.

Allogeneic SCT in CLL
Dreger P et al. Managing high-risk chronic lymphocytic leukemia during transitionto a new treatment era: Stem cell transplantation or novel agents?
Blood. doi:10.1182/ blood-2014-07-586826 (Prepublished online October 9, 2014)
Results of allogeneic SCT in CLL:Relapse 35-40%, PFS @ 5-6y 40%, OS @5-6y 55%.

Allogeneic SCT in CLL
Dreger P et al. Managing high-risk chronic lymphocytic leukemia during transitionto a new treatment era: Stem cell transplantation or novel agents?
Blood. doi:10.1182/ blood-2014-07-586826 (Prepublished online October 9, 2014)
Results of allogeneic SCT in CLL:Early death low!, NRM 20%, extensive cGvHD 21-56%.

Situation in 2012
• Patients with del 17p and TP53 mutation have apoor response (low ORR, few CRs, short PFS, shortOS) with conventional chemotherapy, chemo-immunotherapy or monoclonal antibodies.
• Best ORR with alemtuzumab + high-dose steroids.
• Allogeneic stem cell transplantation is a curativeoption for eligible patients with donor.
• Toxicity is a major problem for alemtuzumab +high-dose steroids and for allogenic stem celltransplantation.

Treatment of CLL
Hallek M Blood 2012; 119 (22):5059

New Agents and their targets in CLL
Tausch E et al. Advances in treating chronic lymphocytic leukemia. F1000Prime Rep. 2014 Aug 1;6:65.

Idelalisib+R vs R in relapsed CLL
Idelalisib is a selective, oral inhibitor of PI3Kδ.Combination with Rituximab may be additive orsynergistic.
Phase 3 study 220 patients Idelalisib + R vs. placebo + R
Idelalisib 150mg BID or placebo continuously
Rituximab 375mg/m2 500mg/m2 (8 doses/24 weeks)
Primary endpoint was progression-free survival (PFS).
Furman RR et al. Idelalisib and Rituximab in Relapsed Chronic Lymphocytic Leukemia.N Engl J Med 2014;370:997-1007.

Idelalisib+R vs R in relapsed CLL
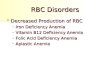
Furman RR et al. Idelalisib and Rituximab in Relapsed Chronic Lymphocytic Leukemia.N Engl J Med 2014;370:997-1007.
• ORR Idelalisib+R 81%, R-mono 13% (p<0.001).PFS not reached vs. 5.5. monthsOS@12m 92% vs. 80% (hazard ratio for death 0.28; P = 0.02).
• “Improvement in PFS was observed not only in the overall studypopulation but also in all subgroups, including patients with poorprognostic features, such as 17p deletion or TP53 mutations.” ?

Idelalisib+R vs R in relapsed CLL
Sharman JP et al. Second Interim Analysis of a Phase 3 Study of Idelalisib (ZYDELIG®) Plus Rituximab (R) forRelapsed Chronic Lymphocytic Leukemia (CLL): Efficacy Analysis in Patient Subpopulations with Del(17p) and
Other Ad-verse Prognostic Factors. ASH 2014 abstract 330.
IDELA+R demonstrated statistically significant improvement overPBO+R in PFS@12m (66% vs. 13%), ORR (77% vs. 15%), and OS (HR0.28) with an acceptable safety profile.These results show a comparable efficacy of IDELA+R across all riskgroups, including those with high-risk genomic markers like del(17p),TP53 mutations, and del(11q).

Ibrutinib vs Ofatumumab inrelapsed or refractory CLL
391 patients with relapsed or refractory CLL.Ibrutinib p.o. 420mg once daily until progression.Ofatumumab i.v. 300mg / 2000mg weekly / monthly for 6 months.ORR with Ibrutinib 43% (+20% PR with lymphocytosis),with Ofatumumab 4% (p<0.001).
Byrd JC et al. Ibrutinib versus Ofatumumab in Previously Treated Chronic Lymphoid Leukemia.N Engl J Med 2014;371:213-23..

Ibrutinib vs Ofatumumab inrelapsed or refractory CLL
Byrd JC et al. Ibrutinib versus Ofatumumab in Previously Treated Chronic Lymphoid Leukemia.N Engl J Med 2014;371:213-23..
• PFS@ 6 months Ibrutinib 88%, Ofatumumab 60%.OS @ 12 months Ibrutinib 90%, Ofatumumab bei 81%(Hazard ratio for death 0.41, p = 0.005).
• “The positive effect of ibrutinib was observed in subgroups ofpatients with a high-risk chromosome 17p13.1 deletion and withresistance to previous purine analogue therapy.” ?

Ibrutinib in relapsed/refractory CLL
O'Brian S et al. Independent evaluation of ibrutinib efficacy 3 years post-initiation of monotherapy in patientswith chronic lymphocytic leukemia/small lymphocytic leukemia including deletion 17p disease.
ASCO 2014 abstract 7014.
BCR-signalling inhibitor Idelalisib (+Rituximab) and Ibrutinib are activein patients with relapsed and refractory CLL with del17p.Nevertheless a significant number of patients with del 17p relapses.

ABT199 phase 1 Trial in R/R CLL
ABT-199 is a selective, potent, orally bioavailable, small molecule Bcl-2inhibitor that can trigger apoptosis of CLL cells in vitro
The primary objectives of this phase I, dose-escalation study in patients withR/R CLL/SLL after ≥ 1 standard therapy were to evaluate the safety,pharmacokinetics (PK), determine a maximum tolerated dose, and arecommended phase 2 dose of ABT-199.recommended phase 2 dose of ABT-199.
Seymour J et al. ASH Annual Meeting Abstracts 2013: 528.

ABT199 phase 1 Trial in R/R CLL
ABT-199 showed activity in patients with R/R CLL with a response rate of84%, including 20% CR/Cri, independent of del 17p.
Phase 2 studies in relapsed patients as monotherapy or as combinationeither with rituximab or obinutuzumab are ongoing / planned.
Seymour J et al. ASH Annual Meeting Abstracts 2013: 528.

How to treat patients with CLL anddeletion 17p / TP53mut?
Dreger P et al. Managing high-risk chronic lymphocytic leukemia during transitionto a new treatment era: Stem cell transplantation or novel agents?
Blood. doi:10.1182/ blood-2014-07-586826 (Prepublished online October 9, 2014)

How to treat patients with CLL anddeletion 17p / TP53mut?
• Recommended options:
– Ibrutinib
– Idelalisib + Rituximab
– Alemtuzumab + steroids*
• Consider and discuss allogeneic SCT in eligiblepatients taking into account transplant-relatedrisk-factors, patient’s preferences and todaysuncertainties (e.g. results of allogeneic SCT afterfailure of one or more novel agents).
* steroid may be omitted in patients with high-risk for steroid-associated side effects (e.g.diabetes mellitus) and non-bulky disease

Take home messages
• Before each line of CLL treatment testing fordeletion 17p and TP53 mutation is recommended.
• Novel agents have a good activity with low toxicityin CLL with deletion 17p / TP53 mutation, butin CLL with deletion 17p / TP53 mutation, butthere are few CRs and probably no cure.
• Patients with deletion 17p / TP53 mutationcontinue to relapse on novel agents.
• Uncertainty which patients should have anallogeneic SCT and when.

Thank you for your attention!Thank you for your attention!