Embed Size (px)
Citation preview

J Plast Surg Hand Surg, 2012; 46: 335–338©2012 Informa HealthcareISSN: 2000-656X print / 2000-6764 onlineDOI: 10.3109/2000656X.2012.718281
ORIGINAL ARTICLE
Salvage for pectoralis major myocutaneous flap failure in head and neckreconstruction by microvascular flap
Chen-Ling Tang1, Yi-Chia Wu2, Ching-Hung Lai2, Chung-Sheng Lai2,3, Chih-Lung Lin3,4, Sin-Daw Lin2 & Kao-Ping Chang2,3
1Department of Surgery, 2Division of Plastic and Reconstructive Surgery, Department of Surgery, Kaohsiung Medical University Hospital,Kaohsiung, Taiwan, 3Department of Surgery, Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan and4Division of Neurosurgery, Department of Surgery, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
AbstractThe pectoralis major myocutaneous pedicled flap (PMMPF) – the “workhorse” for head and neck reconstruction – is associated with a highincidence of complications in certain cases. This study presents free tissue transfer as an alternative salvage technique after PMMPF failure in headand neck reconstruction. It includes seven consecutive patients who underwent free tissue salvage after PMMPF failure in head and neckreconstruction from January 2008 to September 2010 at Kaohsiung Medical University Hospital, Taiwan. Four vertical rectus abdominismyocutaneous (VRAM) flaps were applied for tongue and mouth floor defects, while three anterolateral thigh (ALT) flaps were used for mouthfloor, buccal, and cheek defects. All flaps survived uneventfully, and normal oral feeding was achieved without major complications. Free tissuetransfer has several advantages and can be successfully employed in head and neck reconstruction, and it is also a reliable salvage procedure afterPMMPF failure in such cases.
Key Words: Free tissue transfer, salvage, head and neck, pectoralis major myocutaneous flap, failed flap
IntroductionThe pectoralis major myocutaneous pedicled flap (PMMPF) isconsidered the “workhorse” flap for head and neck reconstruc-tion operations after its introduction in 1979 by Ariyan [1–4].Despite advancements in microsurgery, this flap continues to bethe primary reconstructive choice for several reasons, such asgood coverage, readily identifiable and reliable bloody supply,reduced operative time, simple technical aspects, lower patientcomorbidity, and proximity to the head and neck region [3,5–8].It is also considered a versatile, robust, reliable, and safe optionfor head and neck reconstruction [6–8].
However, the disadvantages of the PMMPF include cosmeticdeformity, flap bulkiness, lack of arc rotation, morbidity asso-ciated with donor and recipient sites, and a high incidence ofcomplications [2,9,10]. The high incidence of complications isassociated with smoking, diabetes, previous radiotherapy, obe-sity, and an inexperienced surgeon; it can be further increased byinfection and wound dehiscence [2,6,11]. In these situations, asecondary operation is required, with the incidence of suchsecondary operations ranging from 10%–50% [11–14]. How-ever, few studies have reported the management of PMMPFfailure. Here, we describe our experience with using free tissuetransfer as a salvage technique after PMMPF failure in head andneck reconstruction.
Patients and methodsIn this study, we included seven patients who had free tissuesalvage after PMMPF failure in head and neck reconstructionbetween January 2008 and September 2010 at the Kaohsiung
Medical University Hospital, Taiwan. The medical records ofthese patients were reviewed. All patients were referred from theDepartment of Otorhinolaryngology. The indication for previ-ous PMMPF reconstruction was immediate reconstruction afterhead and neck tumour operation. Debridement and free flapreconstruction were performed simultaneously in every salvageoperation by plastic surgeons. However, the time interval fromPMMPF to free flap varied and depended upon the referral date.All salvage operations were completed within 1 week afterreferral consultation. Patient demographics, adjuvant therapy,tumour data, flap details, and the complications for each case ofreconstruction were analysed.
ResultsAll seven patients were men with a mean age of 45.2 years(range 39–52). Each patient had free tissue salvage afterPMMPF failure for head and neck reconstruction. Of these,six patients had stage IV squamous cell carcinoma (SCC), andone had stage II SCC. None of them had previously receivedadjuvant radiotherapy or chemotherapy. Four of them receivedthe vertical rectus abdominis myocutaneous (VRAM) flap as thesalvage flap for tongue (Figure 1) and mouth floor defects, whilethe remaining three received the anterolateral thigh (ALT) flapfor a buccal (Figure 2), cheek, and mouth floor (Figure 3) defecteach. The superior thyroid artery was used as the recipient arteryin all cases. Only one patient suffered from minor wounddehiscence and the wound was left for secondary healing.All flaps survived well with OPD follow-up ranging from7–25 months. All patients had fair swallowing function to
Correspondence: Kao-Ping Chang, MD, PhD, Division of Plastic and Reconstructive Surgery, Kaohsiung Medical University Hospital, 100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan. Tel: 886-7-3121101 Ext 7675. Fax: 886-7-3111482. E-mail: [email protected](Accepted 21 May 2012)
Jour
nal o
f Pl
astic
Sur
gery
and
Han
d Su
rger
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
9/24
/12
For
pers
onal
use
onl
y.

tolerated regular oral intake well and their communicationfunction was also acceptable (Table I).
DiscussionAlthough the PMMPF has been widely used in head and neckreconstruction since its first introduction by Ariyan in 1979[1–4], many studies have revealed the reliability of free tissuetransfer since the 1980s. Therefore, the role of the PMMPF inhead and neck reconstruction has been supplanted by freetissue transfer in several situations [3,4,9]. However, free tissue
transfer requires a specialised team since it is a complexoperation entailing rigorous postoperative care; it is thus expen-sive and not available in many hospitals [7]. Moreover, theadvantages of PMMPF include relatively easy technique, prox-imity of the head and neck region, readily identifiable andreliable blood supply, abundant soft tissue volume for goodcoverage, protection of the great vessels in the neck, unchangedpatient position during harvest and use of the flap, and reducedoperating time as compared with that for the free flap technique[3,6,7,15,16]. Therefore, the PMMPF remains an excellent
a b
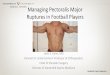
Figure 1. (a, b) A 45-year-old man with tongue carcinoma, T2N2M0 Stage II, had a wide excision with mandibulectomy and functional neckdissection. The defect was reconstructed using a PMMPF flap. However, progressive partial necrosis was noted. At 26 days after the firstoperation, a VRAM flap was used to salvage the failed PMMPF.
a b
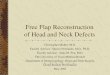
Figure 2. (a, b) A 39-year-old man with right buccal squamous cell carcinoma, T4N0M0 Stage IVa, had a wide excision with maxillectomy,segmental mandibulectomy, and right radical neck dissection, with PMMPF being used for reconstruction. Congestion was noted in the flap onpostoperative day 2. Exploration was performed but no obvious cause was found; therefore, an ALT flap was used to salvage the failed PMMPF.
a b
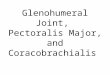
Figure 3. (a, b) A 41-year-old man with tongue carcinoma, T2N0M0 Stage II, had a wide excision with mandibulectomy and functional neckdissection. The defect was reconstructed using a PMMPF flap. However, necrotic flap with tongue and mouth floor defect were notedpostoperatively. At 17 days after the initial operation, an ALT flap was used to salvage the failed PMMPF.
336 C.-L. Tang et al.
Jour
nal o
f Pl
astic
Sur
gery
and
Han
d Su
rger
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
9/24
/12
For
pers
onal
use
onl
y.

reconstructive choice in head and neck reconstruction, espe-cially in high-risk patients (elderly, significant comorbidity,advanced tumour, previous extended head and neck operation,and radiation) and in developing countries that need cost-effective care [7,11,17]. Another common (~ 25%) and impor-tant indication for PMMPF reconstruction is salvage procedureafter free flap failure [5,17].
Reconstructions comprise donor site disfigurement, exces-sive bulk, restricted arc of rotation, gravitational displacementwith time, technical difficulties in women, and high compli-cation rates [2,4,10,15,17]. Its complications include wounddehiscence, infection, fistula formation, and partial and totalflap loss; the incidence of such high-risk complications variesfrom 14% [18] to 69% [1]. The incidence of partial flap loss,complete flap loss, and salivary fistulas ranges from 4%–29%,0%–16%, and 5%–20%, respectively [1,6,7,16,17]. Moreover, asecondary operation is required in 10%–50% of cases [11-14].Liu et al. [17] reported that 17% of flap necrosis cases requiredanother flap for salvage, while Milenovic et al. [16] reportedthat only 2% of those who required surgical interventionfor postoperative complications received a new flap. McLeanet al. [14] showed that 7% (1/15) of patients who received asecondary operation required contralateral PMMPF reconstruc-tion. In our hospital, the failure rate of complete PMMPF losswas about 10%. Smoking and an inexperienced surgeon wereregarded as the main causes of flap failure. Further, severalauthors have reported significant donor site morbidity, includ-ing neck pain (33%), sensory loss (65%), limited lateral flexionaway from the operation site, impaired neck mobility, limitedrange of motion of shoulder, and impairment of arm strength[4,19,20]. Because of these critical morbidities, using thecontralateral PMMPF for salvaging a failed PMMPF can causefurther grievous disability. However, the use of a free flapfor salvaging a failed PMMPF would reduce neighbouringtissue contracture and preserve the function of the oppositeshoulder. Therefore, in this study, we proposed using free flaptransfer as an alternative method for salvaging failed PMMPFreconstruction.
Wei et al. [21] reported the next reconstructive ladder afterfailed free flap transfer, considering a secondary free tissuetransfer as an effective and reliable procedure after free flapreconstruction failure in head and neck reconstruction, with theonly contraindication being the deteriorating condition of thepatient. Further, they mentioned that regional flaps used inthe head and neck region had higher complication rates than
secondary free flaps, with one-third of them requiring substi-tution by another free flap. As compared with free flap failure,PMMPF failure has certain advantages, such as recognisableand good-quality recipient vessels that would aid in successfulsecondary surgery involving free flap reconstruction.
Secondary free tissue transfer for PMMPF failure in headand neck reconstruction entails certain challenges, e.g., thecommonly used cervical vessels are often buried in the scar,the defect itself is frequently scarred, and the failed flap isassociated with tissue oedema, inflammation, vascular trauma,malnutrition, or infection, all of which would delay woundhealing [22]. Adequate debridement to remove devitalisedtissue, including removal of failed flap and residual debris,is thus a necessity for ensuring bacterial control [21]. The besttime for secondary reconstruction by the free flap was recom-mended once when the flap failure was noted, the patient hasrecovered from previous operation, and infection was undercontrol. Further, the PMMPF is generally used in advancedoral cancer patients with large skin and mucosal loss, total orsubtotal glossectomies, and removal of the muscles in theoral floor [11]. Therefore, the secondary flap needs to havegood vascularity, a long pedicle, and bulky volume. Althougha pedicled latissimus dorsi flap has good vascularity and bulkyvolume, the difficulties associated with its relatively shortarc should be considered. Further, although the radial forearmfree flap has a long and relatively large vascular pedicle vessel,its volume is usually insufficient to restore function andcosmesis [23].
Based on these considerations, we regard the free VRAM andALT flaps as good choices in salvage procedures after PMMPFfailure owing to their long pedicle vessels, as well as the lowfunctional loss at the donor site noted in our patient series.However, VRAM and ALT flaps have drawbacks similar toother free flap operations, such as the need for an experiencedsurgical and postoperative care team, expensive instruments,and longer operating time and higher expense as compared withPMMPF reconstruction. Despite these disadvantages, we con-sider immediate free tissue transfer as a reliable salvage alter-native for PMMPF failure, except in elderly patients or thosewith significant comorbidity.
In conclusion, the high complication rate, especially total flaploss, associated with the use of PMMPF in head and neckreconstruction, often requires secondary reconstruction. In thissituation, free VRAM and ALT flaps are robust and reliablereconstructive strategies in non-high-risk patients.
Table I. Details of patients.
Case no.Age/sex
Tumoursite
Tumourstage
Adjuvanttherapy
Day of secondaryreconstruction
Flap used inreconstruction Recipient vessels Complication
Patient’ssatisfaction
1 39/M Buccal T4N0M0 Nil 6 ALT Superior thyroid a No Good2 45/M Tongue T2N2M0 Nil 26 VRAM Superior thyroid a No Good3 41/M Tongue T2N0M0 R/T 17 ALT Superior thyroid a No Good4 42/M Mouth floor T4N1M0 Nil 15 VRAM Superior thyroid a Minor wound
dehiscenceGood
5 47/M Mouth floor T4N1M0 Nil 14 VRAM Superior thyroid a No Good6 51/M Cheek T4N2M0 Nil 10 ALT Superior thyroid a No Good7 52/M Tongue T4N1M0 Nil 8 VRAM Superior thyroid a No GoodALT = anterolateral thigh flap; VRAM = vertical rectus abdomins myocutaneous flap; Superior thyroid a = Superior thyroid artery.
Salvage for failed PM flap by free flap 337
Jour
nal o
f Pl
astic
Sur
gery
and
Han
d Su
rger
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
9/24
/12
For
pers
onal
use
onl
y.

AcknowledgementWe thank the Department of Otorhinolaryngology for all thetumour ablations that they performed.
Declaration of interest: The authors report no conflicts ofinterest. The authors alone are responsible for the contentand writing of the paper.
References[1] Corten EM, Schellekens PP, Hag JJ, Kon M. Clinical outcome
after pedicled segmental pectoralis major island flaps for headand neck reconstruction. Ann Plast Surg 2009;63:292–6.
[2] O’Neill JP, Shine N, Eadie PA, et al. Free tissue transfer versuspedicled flap reconstruction of head and neck malignancydefects. Ir J Med Sci 2010;179:337–43.
[3] Yeh JT, Chen HC, Laverty LA, et al. Conversion from pedicledto free flap for salvage of the compromised pectoralis majormyocutaneous flap in head and neck reconstruction. PlastReconstr Surg 2004;114:152–7.
[4] Moukarbel RV, Fung K, Franklin JH, et al. Neck and shoulderdisability following reconstruction with the pectoralis majorpedicled flap. Laryngoscope 2010;120:1129–34.
[5] Avery CM, Crank ST, Neal CP, et al. The use of the pectoralismajor flap for advanced and recurrent head and neck malignancyin the medically compromised patient. Oral Oncol 2010;46:829–33.
[6] Liu R, Gullane P, Brown D, Irish J. Pectoralis major myocu-taneous pedicled flap in head and neck reconstruction: retro-spective review of indications and results in 244 consecutivecases at the Toronto General Hospital. J Otolaryngol 2001;30:34–40.
[7] Vartanian JG, Carvalho AL, Carvalho SM, et al. Pectoralismajor and other myofascial/myocutaneous flaps in head andneck cancer reconstruction: experience with 437 cases at a singleinstitution. Head Neck 2004;26:1018–23.
[8] Koh KS, Eom JS, Kirk I, et al. Pectoralis major musculocuta-neous flap in oropharyngeal reconstruction: revisited. PlastReconstr Surg 2006;118:1145–50.
[9] Mallet Y, El Bedoui S, Penel N, et al. The free vascularized flapand the pectoralis major pedicled flap options: comparativeresults of reconstruction of the tongue. Oral Oncol 2009;45:1028–31.
[10] Chaturvedi P, Pai PS, Pathak KA, et al. Simultaneousreconstruction of large skin and mucosal defect following
head and neck surgery with a single skin paddle pectoralismajor myocutaneous flap. J Laryngol Otol 2005;119:303–5.
[11] El-Marakby HH. The reliability of pectoralis major myocuta-neous flap in head and neck reconstruction. J Egypt Natl CancInst 2006;18:41–50.
[12] von Biberstein SE, Spiro JD. The pectoralis major myocuta-neous flap in reconstructive head and neck surgery revisited:a recent experience. Conn Med 1994;58:711–14.
[13] Righi PD, Weisberger EC, Slakes SR, et al. The pectoralis majormyofascial flap: clinical applications in head and neck recon-struction. Am J Otolaryngol 1998;19:96–101.
[14] McLean JN, Carlson GW, Losken A. The pectoralis majormyocutaneous flap revisited: a reliable technique for headand neck reconstruction. Ann Plast Surg 2010;64:570–3.
[15] Bianchi B, Ferri A, Ferrari S, et al. Free and locoregionalflap associations in the reconstruction of extensive headand neck defects. Int J Oral Maxillofac Surg 2008;37:723–9.
[16] Milenovic A, Virag M, Uglesic V, Aljinovic-Ratkovic N. Thepectoralis major flap in head and neck reconstruction: first500 patients. J Craniomaxillofac Surg 2006;34:340–3.
[17] Liu HL, Chan JY, Wei WI. The changing role of pectoralismajor flap in head and neck reconstruction. Eur Arch Otorhi-nolaryngol 2010;267:1759–63.
[18] Talesnik A, Markowitz B, Calcaterra T, et al. Cost and outcomeof osteocutaneous free-tissue transfer versus pedicled soft-tissuereconstruction for composite mandibular defects. Plast ReconstrSurg 1996;97:1167–78.
[19] van Wilgen CP, Dijkstra PU, van der Laan BF, et al. Shoulderand neck morbidity in quality of life after surgery for head andneck cancer. Head Neck 2004;26:839–44.
[20] Nowak P, Parzuchowski J, Jacobs JR. Effects of combinedmodality therapy of head and neck carcinoma on shoulderand head mobility. J Surg Oncol 1989;41:143–7.
[21] Wei FC, Demirkan F, Chen HC, et al. The outcome of failed freeflaps in head and neck and extremity reconstruction: what is nextin the reconstructive ladder? Plast Reconstr Surg 2001;108:1154–62.
[22] Iseli TA, Yelverton JC, Iseli CE, et al. Functional outcomesfollowing secondary free flap reconstruction of the head andneck. Laryngoscope 2009;119:856–60.
[23] de Bree R, Reith R, Quak JJ, et al. Free radial forearm flap versuspectoralis major myocutaneous flap reconstruction of oral andoropharyngeal defects: a cost analysis. Clin Otolaryngol 2007;32:275–82.
338 C.-L. Tang et al.
Jour
nal o
f Pl
astic
Sur
gery
and
Han
d Su
rger
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
9/24
/12
For
pers
onal
use
onl
y.