Embed Size (px)
Citation preview

The Journal of Applied Research • Vol. 4, No. 4, 2004 635
females and 11 males, with a medianage of 64 years (range 37-80 years).Histology was adenocarcinoma in 23patients and neuroendocrine tumor in 2patients. One patient had resectedtumor, 3 patients were resected withpositive margins, 1 patient wasresectable with poor performance statusprohibiting resection, and 20 patientshad unresected locally advanced dis-ease. Median dose of capecitabine con-current with radiation was 1500mg/m2/day (600-1600 mg/m2/day) givenorally in two divided doses, 5 days perweek on days of treatment with radia-tion therapy. Patients received a medi-an total radiation dose of 5040 cGy(4500-5040 cGy) over 6 weeks. Elevenpatients were continued on capecitabinecycles after treatment with concurrentcapecitabine and irradiation. The medi-an number of cycles completed was 3,with one patient completing 8 cycles.Median survival was 14 months, with 18patients surviving through the end ofthe study period. Median overall pri-mary tumor response over the studyperiod was –2% (-100%-100%). Fivepatients were taken to laparotomy after
Retrospective Analysis ofCapecitabine and RadiationTherapy in the Treatment ofPancreatic CancerM. Wasif Saif, MDM. Joseph, MDS. Tang, PhDSelwyn Vickers, MDB. Plants, MDS. Russo, MD
University of Alabama at Birmingham Comprehensive Cancer Center, Birmingham, Alabama
KEY WO R D S : pancreatic cancer,capecitabine (Xeloda), r a d i o t h e r a p y,thymidine phosphorylase
ABSTRACTPurpose: To report our clinical experi-ence with 25 patients receiving concur-rent capecitabine and irradiation in thetreatment of locally advanced or resect-ed pancreatic cancer.
Methods and Materials: We reviewedthe medical records of patients withpancreatic cancer who received treat-ment with capecitabine and irradiationfor pancreatic cancer and receivedcapecitabine 1200 to 1600 mg/m2 orallytwice daily Monday through Friday withconcurrent radiation (5040-5400 cGy,180 cGy, 5 days/week), followed by a 4-week rest, then 6 to 8 cycles ofcapecitabine alone 2000 to 2500 mg/m2
twice daily for 14 days every 3 weeks(surgically resected), and capecitabine2000 to 2500 mg/m2 BID for 14 daysevery 3 weeks until progressive disease(unresected).
Results: The population consisted of 14
Saif#2-vol4no4 12/6/05 6:53 PM Page 635

Vol. 4, No. 4, 2004 • The Journal of Applied Research636
treatment based on radiographicresponse and two patients were success-fully resected. By the end of the studyperiod, there were 4 complete remis-sions, 2 partial remissions, 6 stable dis-ease, and 13 progressive disease. Grade3 or 4 toxicity was observed mainly withgastrointestinal symptoms includingnausea, vomiting, diarrhea, and anorex-ia. Three patients had G3 hand-footsyndrome, 1 patient had G3 peripheralneuropathy, 1 patient had G4 gastroin-testinal bleed, and 1 patient had G3radiation enteritis. There was one deathdirectly related to treatment secondaryto uncontrolled GI bleeding.
Conclusion: In patients with locallyadvanced pancreatic cancer, concurrentcapecitabine and radiation had goodsurvival response in patients and goodtumor response. Toxicity of oralcapecitabine was well tolerated.
INTRODUCTIONStandard treatment for locally advancedpancreatic cancer for several decadeshas been rapid infusion 5-fluorouracil(5-FU) delivered in conjunction withirradiation (XRT).1 Both abdominalradiotherapy and 5-FU treatment areassociated with gastrointestinal symp-toms including diarrhea, nausea, vomit-ing, and intestinal fibrosis, sometimesleading to bowel obstruction. Regimensbased on gemcitabine have been offeredas an alternative to fluorouracil basedtreatment in this stage of malignancy,with recent studies indicating improvedclinical response with gemcitabine.2
However subsequent analysis of experi-ences with gemcitabine and concurrentirradiation shows a significant toxicity,arguing for ongoing pursuit of therapeu-tic regimens in the treatment of locallyadvanced, unresectable pancreatic can-cer.3 A recent meta-analysis of treat-ment for locally advanced pancreaticcancer proposes that 5-FU in conjunc-
tion with irradiation is the preferredchemotherapeutic agent, with gemc-itabine viewed as an acceptable alterna-tive. The preferred delivery of 5-FU,whether infusional or bolus, however,was not well established by the studiesanalyzed.4
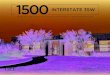
Capecitabine (Xeloda; RocheLaboratories, Nutley, NJ), a pro-drug of5-FU, is an oral fluoropyrimidine thathas recently been shown in a phase IIstudy to have activity in advanced andmetastatic pancreatic cancer.5 The con-version to 5-FU occurs in a 3-stepprocess, the last of which may providefor tumor selectivity (Figure 1). The finalconversion to 5-FU occurs throughthymidine phosphorylase (TP). Thisanti-angiogenic enzyme, which is alsoknown as the platelet-derived endothe-lial cell growth factor, tends to be foundin higher concentrations in tumor tissuethan in surrounding normal tissue2. Thisdifferential creates the potential fortumor selectivity and enhanced thera-peutic index, which is demonstrated invivo.6 Additionally, thymidine phospho-rylase has been shown to be upregulatedin irradiated human tissue.7 Since TP isdifferentially expressed in tumors versusnormal tissue, it is anticipated that treat-ment-related toxicity may be diminishedby the use of concurrent capecitabinewith radiotherapy, further enhancing thetherapeutic index of radiation.
Use of capecitabine as a radiationsensitizer offers several other theoreticaladvantages. Capecitabine is wellabsorbed orally and offers the possibilityof continuous tumor exposure to tissue.A phase III study comparingcapecitabine to 5-FU in colorectal can-cer showed similar incidence of gastroin-testinal side effects, decreased incidenceof stomatitis, alopecia, and grade 3/4neutropenia but increased incidence ofhand-foot syndrome and uncomplicatedhyperbilirubinemia. Efficacy was similarwith both drugs.8 An added advantage to
Saif#2-vol4no4 12/6/05 6:53 PM Page 636

The Journal of Applied Research • Vol. 4, No. 4, 2004 637
oral capecitabine is the elimination ofcatheter-related complications and con-venience of oral administration. Thesedata suggest that oral capecitabine maybe an equally efficacious and a more tol-erable treatment for locally advancedpancreatic cancer.
We report a retrospective analysis ofthe efficacy and toxicity of concurrentcapecitabine and radiation in 25 patientswith locally advanced (resected or unre-sectable) pancreatic cancer treated atthe University of Alabama atBirmingham (UAB) during April 2002through September 2003.
METHODS AND MATERIALSThis study was approved by theInstitutional Review Board (IRB) at theUniversity of Alabama at Birmingham,Birmingham, Alabama. We reviewedrecords of 25 patients with locallyadvanced or resected pancreatic cancerwho were treated with capecitabine andconcurrent radiation therapy. Patientswere seen from April 2002 throughSeptember 2003. Twenty-four patientsreceived treatment at the University ofAlabama at Birmingham; one patientwas initially seen at the University ofAlabama at Birmingham, but receivedtreatment at an outside facility. Patientswere identified by medical oncologists atthe University of Alabama atBirmingham. Information regarding
patient characteristics, treatment dura-tion and dosage, toxicity, and survivalwas obtained from medical charts andthrough the tumor registry at theUniversity of Alabama at Birmingham.
CapecitabinePatients received a 6-week course oforal capecitabine, divided in two dailydoses on days of radiation, Mondaythrough Friday, for 6 weeks’ durationwith concurrent radiation therapy.Patients received capecitabine doses of1200 to 1600 mg/m2/day in two divideddoses per day (median dose 1600mg/m2/day). Capecitabine was roundedto the nearest dose, which allowed fordosing with standard 150 mg and 500 mgtablets. This 6-week chemoradiation wasfollowed by a 4-week rest period.Patients who responded to capecitabinewith radiation (responded either stabledisease or response) were treated withthen 6 to 8 cycles of capecitabine 2000 to2500 mg/m2 orally twice daily for 14 daysevery 3 weeks for the surgically resectedpatients, and capecitabine 2000 to 2500mg/m2 orally, twice daily for 14 daysevery 3 weeks (with 2 weeks on medica-tion, 1 week off) until progressive dis-ease for unresected patients.
Radiation therapyCT image-based three-dimensionaltreatment planning was utilized to opti-
Figure 1. The enzymatic conversion of capecitabine to 5-FU occurs in a three-step process.
Saif#2-vol4no4 12/6/05 6:53 PM Page 637

Vol. 4, No. 4, 2004 • The Journal of Applied Research638
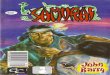
mize radiation treatment by facilitatingidentification of the target volume andsurrounding normal structures (Figure2). Attempts were made to minimizeradiation dose to surrounding normaltissues while ensuring adequate dose tothe target volume. CT simulation was
performed with IV and oral contrastmaterial to assist in localizing kidneys,liver, stomach, and intestines.Anatomical structures were contouredfor dose-volume histogram (DVH)analysis. The intestines were defined asthe contents within the peritoneal cavity,
Figure 2. Three-dimensional treatment plan with color wash dose distributions identifying dose oftumor delivered to tumor volume and surrounding normal anatomical structures.
Saif#2-vol4no4 12/6/05 6:53 PM Page 638

The Journal of Applied Research • Vol. 4, No. 4, 2004 639
excluding the stomach, spleen, liver, kid-neys, aorta, and gross target volume(GTV) to allow for organ motion.
The maximum extent of the tumorand involved nodal areas (gross tumorvolume, GTV), or tumor bed (markedwith clips placed at the time of surgery),plus adjacent loco-regional nodes (celi-ac, peripancreatic, and portal), and para-aortic nodal areas at risk for residualmicroscopic diseases (clinical target vol-ume, CTV) were also defined by CT.
Radiatherapy began on the first dayof week 1 of capecitabine therapy. Theinitial target volume received 1.8 Gy/daydelivered Monday through Friday for 25fractions (45 Gy). Typically, the edges ofthe initial fields were defined superiorly1.5 cm above the CTV, inferiorly tocover the para-aortic nodes to the L3-4intervertebral space, laterally and anteri-orly with a 1.5 cm margin around theCTV, and posteriorly by splitting theanterior vertebral bodies in half. After45 Gy, an additional three to five 1.8 Gyfraction was delivered to the GTV ortumor bed with a 1.5 cm margin for atotal dose of 50.4 to 54 Gy. Externalbeam radiation therapy was deliveredfrom high-energy linear acceleratorswith 15 MV photon beams. Patientsreceived 4500 to 5040 cGy, median dose5040 cGy to the tumor bed. Treatmentfields were irradiated once daily, 5 daysper week, at 180 cGy per fraction, overthe course of 6 weeks.
Response AssessmentSurvival was measured from date oftreatment initiation. Disease responsewas measured according to the RECISTcriteria. Assessments of tumor dimen-sions were performed prior to treat-ment, after treatment with capecitabineand radiation (6 weeks of chemoradio-therpy + 4-week rest) and then everythree cycles (9 weeks). Response crite-ria were as follows: complete response,disappearance of all target lesions; par-
tial response, at least 30% decrease inlongest diameter; progressive disease, atleast 20% increase in longest diameter;and stable disease, response fallingbetween partial response and progres-sive disease.9
Toxicity AssessmentPatients were assessed weekly duringchemo-radiation and every 3 weeks dur-ing capecitabine monotherapy. Acute£90 days from the start of radiation, sideeffects were documented using the NCICommon Toxicity Criteria (CTC) ver-sion 2.0.10 Late (>90 days from the startof radiation side effects were evaluatedand graded according to RTOG LateRadiation Morbidity Scoring Scale.
Statistical MethodsPatient characteristics were analyzedwith frequency tables with groupingsassigned respective percentage of theentire data set. Toxicity was analyzedwith frequency tables with groupingsassigned respective percentage of theentire data set. Survival was assessedwith Kaplan-Meier survival analysis.Survival was measured from date of diag-nosis until date of death or until the endof the study period for patients survivingthrough the end of the study period.
RESULTSPatient CharacteristicsTable 1 summarizes the patient charac-teristics. Twenty-five patients consistingof 14 females and 11 males, with locallyadvanced or resected pancreatic cancer,treated with capecitabine and irradiationwere identified. Median age of thepatient population was 64 years, range37 to 80 years. Twenty-three patientshad adenocarcinoma and 2 had neu-roendocrine tumor of the pancreas. Onepatient had resected tumor, 3 patientswere resected with positive margins, 1patient was resectable with poor per-formance status prohibiting resection,
Saif#2-vol4no4 12/6/05 6:53 PM Page 639

Vol. 4, No. 4, 2004 • The Journal of Applied Research640
Table 1. Patient CharacteristicsCharacteristic No (%)Age
<65 years 13 (52)≥65 years 12 (48)
RaceWhite 23 (92)African-American 2 (8)
GenderFemale 14 (56)Male 11 (44)
HistologyAdenocarcinoma 23 (92)Neuroendocrine 2 (8)
Stage I 2 (8)IVA 23 (92)
Resection statusResected with (-) margins 1 (4)Resected with (+) margins 3 (8)Resectable, but inoperable d/t
poor performance status 1 (4)Locally advanced 20 (84)
Primary siteHead 20 (80)Body 3 (12)Neck 1 (4)Periampulla 1 (4)
Performance statusECOG 0 9 (36)ECOG 1 13 (52)ECOG 2 2 (8)ECOG 3 1 (4)
Weight loss grade0 11 (44)1 9 (36)2 4 (16)3 1 (4)
Pain grade0 9 (36)1 13 (52)2 2 (8)3 1 (4)
New onset diabetesNo 23 (92)Yes 2 (8)
CA 19-90-10 5 (20)11-100 5 (20)101-1000 6 (24)>1000 7 (28)
Prior therapyNone 22 (88)Surgical resection 1 (4)Chemotherapy for prior malignancy 2 (8)
Saif#2-vol4no4 12/6/05 6:53 PM Page 640

The Journal of Applied Research • Vol. 4, No. 4, 2004 641
and 20 patients had unresected locallyadvanced disease due to vascularinvolvement. Most patients were of per-formance status 0 to 1, with grade 0 to 1weight loss and grade 0 to 1 pain associ-ated with disease. Tumor marker CA19-9 ranged with a relatively even distri-bution among different log ranges. Mostpatients did not have prior treatment formalignancy, but two patients did haveprior treatment for breast cancer, bothwith chemotherapy, and one with hor-monal therapy.
Treatment Delays and ModificationsTwenty of 25 patients completed the full6 week course of capecitabine-radiother-apy at the intended dose without a breakor dose reduction of therapy. Tw opatients mistakenly took half a dose forthe first 3 weeks, and were then correctedby the treating physician to the intendeddose for the last 3 weeks. One patientdid not complete the intended 6-weekcourse because of prolonged hospitaliza-tion secondary to malignancy related bil-iary obstruction. Two patients had breaksin treatment: one patient had capecitabineheld for 3 days due to diarrhea, and onepatient had capecitabine held for 2 weeksdue to hyperbilirubinemia.
Eleven patients were continued oncapecitabine monotherapy after conclu-sion of capecitabine-radiation. Mediannumber of cycles completed was 3, withrange from 1 to 8. Eight cycles (intend-ed full course) were completed by onepatient. Of the 11 patients who receivedcapecitabine cycles, 7 patients had cyclesheld: 3 had cycles held due to diarrhea, 3had cycles held due to grade 3 hand-footsyndrome, and 1 had capecitabine cyclelength shortened due to physician deci-sion. Capecitabine cycles were heldfrom 1 to 4 weeks with resolution ofsymptoms. Of the 11 patients whoreceived capecitabine cycles, 4 had dosesdecreased for symptoms: 3 patients forgrade 3 hand-foot syndrome and 1patient for grade 3 diarrhea, grade 2mucositis, and grade 2 hand-foot syn-drome.
Capecitabine was continued astreatment until certain endpoints werereached. Sixteen patients had progres-sive disease or inadequate response totreatment, including both patients withneuroendocrine histology, and weretherefore discontinued on capecitabineand changed to an alternate treatmentregimen. Most common agents usedafter failing capecitabine included gemc-
Table 2. Number and Percentage of Patients with Capecitabine Toxicity
Grade 1 Grade 2 Grade 3 Grade 4Toxicity No. (%) No. (%) No. (%) No. (%)Anemia 11 (44) 2 (8) 0 (0) 0 (0)Neutropenia 2 (8) 1 (4) 0 (0) 0 (0)Thrombocytopenia 0 (0) 0 (0) 0 (0) 0 (0)Nausea 12 (48) 1 (4) 3 (12) 0 (0)Vomiting 7 (28) 0 (0) 3 (12) 0 (0)Diarrhea 10 (40) 1 (4) 4 (16) 0 (0)Anorexia 2 (8) 4 (16) 0 (0) 2 (8)Weight loss 6 (24) 4 (16) 0 (0) 0 (0)Mucositis 1 (4) 1 (4) 0 (0) 0 (0)Hand-foot syndrome 2 (8) 1 (4) 3 (12) 0 (0)Peripheral nervous 0 (0) 1 (4) 1 (4) 0 (0)GI bleeding 0 (0) 0 (0) 1 (4) 1 (4)Radiation enteritis 1 (4) 0 (0) 1 (4) 0 (0)
Saif#2-vol4no4 12/6/05 6:53 PM Page 641

Vol. 4, No. 4, 2004 • The Journal of Applied Research642
itabine as a single agent (> 70%), combi-nation of gemcitabine with other agentssuch as irinotecan. Six patients were notstopped during the study period, and 2of these 6 patients completed theintended 8 total capecitabine cycles.Two patients were discontinued oncapecitabine due to physician decision inanticipation of side effects. One patientdied due to disease before capecitabinecycle discontinuation.
ToxicityTable 2 summarizes the toxicity ofcapecitabine when given with XRT. G3-4 toxicity was reported in 10 patients,related to vomiting, diarrhea, and hand-foot syndrome. Most common toxicitiesincluded G1-2 gastrointestinal sideeffects and G1-2 anemia.Gastrointestinal toxicity comprised ofnausea, vomiting, diarrhea, weight loss,and anorexia. Most of patients devel-oped G1-2 nausea or vomiting, while 12patients developed cases of G3-4 nau-sea, vomiting, diarrhea, and anorexia.There were 10 cases of G1-2 weight lossbut no G3-4 weight loss was noted.There were 3 cases of G3 hand-foot syn-drome, 2 of which required holding doseof capecitabine. Hematologic toxicityconsisted of 13 cases of G1-2 anemiaand 3 cases of G1-2 neutropenia. Nocases of thrombocytopenia were report-ed. Other toxicity included 3 instancesof G1-2 hand-foot syndrome, 2 cases ofG1-2 mucositis, and 2 cases of peripheralneuropathy. Peripheral neuropathy wasof G3 in one patient manifested as gaitataxia, and G2 in the second presentingas perioral numbness and tingling ofupper extremity. Both these patientshad their symptoms resolved withoutdiscontinuation of capecitabine.11 Onecase of G4 gastrointestinal bleedingoccurred on capecitabine, requiringangiographic embolization. One case ofG3 radiation enteritis is also reportedhere, though not directly related to
capecitabine therapy.Capecitabine was held in 7 patients
(3 due to diarrhea, 3 due to grade 3hand-foot syndrome, and 1 instance forG4 bleeding). Other delays or alterationin therapy were unrelated to toxicity. Sixpatients were hospitalized for sideeffects related to capecitabine; one hos-pitalization was for G4 bleeding notedabove, the rest were for gastrointestinalside effects. Toxicity was controlled withsymptomatic treatment on outpatientbasis.
One possible treatment-relateddeath occurred and was attributable touncontrolled GI bleeding. This bleedingoccurred within the radiation port as alate complication, while the patient wasreceiving post-radiation capecitabinemonotherapy (approximately 3 monthsfollowing completion of capecitabine-radiotherapy).
RESPONSE AND SURVIVALChemo-radiotherapyAfter initial treatment with capecitabineand radiation (6-week chemo-radiother-apy), 2 of 20 patients with unresected,locally advanced tumor were convertedto radiographically resectable disease (2complete response). Two other patientswith locally advanced unresectable dis-ease exhibited a partial response of 29%and 42%, respectively. Eight patientsexhibited stable disease, and 10 patientsexhibited progressive disease, of whom 1showed an increase in tumor size by100%, the other 9 exhibited metastaticdisease in the liver. All the patients withresected tumor (either negative or posi-tive margins) had no radiological evi-dence of recurrent disease at the end of6-week chemo-radiotherapy.
Mono-chemotherapyEleven patients received further treat-ment with capecitabine cycles alone.With continued capecitabine therapy, 3patients with locally advanced unre-
Saif#2-vol4no4 12/6/05 6:53 PM Page 642

The Journal of Applied Research • Vol. 4, No. 4, 2004 643
sectable tumor were thought to be radi-ologically converted to a resectable dis-ease. Of these 3 patients, only 1 wassuccessfully taken for possible resectionafter careful evaluation of the scans by ateam composed of a radiologist, radia-tion oncologist, medical oncologists, andsurgical oncologists. Four patients hadstable disease during treatment withcapecitabine cycles alone, and 5 patientsexhibited progressive disease, comprisedof 2 recurrences after resection with (+)margins, 2 progressions to metastatic dis-ease, and 1 patient with an increase intumor size by 28%. However, in spite ofa 28% increase in size, the patient’stumor was converted to resectable, andthe patient was taken to laparotomy.
Surgical ResectionOf the 20 patients with locally advanced,unresected disease, 5 had radiographicimprovement of disease sufficient totake patients to laparotomy for tumorresection. Only 2 of the 5 patientstaken to laparotomy were successfully
resected. The other 3 patients were notresected due to intraoperative findingsprohibiting resection, including inflam-matory adhesions in one and residualdisease encasing vasculature in the rest.Operative findings in the former patientshowed extensive fibrosis primarily atthe tumor sites, but not in the surround-ing normal tissues.
Overall ResponseOverall response to therapy was 4 com-plete remissions, 2 partial remissions, 6stable disease, and 13 progressive disease.Average duration of treatment withineach group was 7.3 months (range 2.2-13.0 months) for the complete remis-sions, 5.4 months (range 2.2-8.5 months)for the partial remissions, 5.2 months(range 2.3-9.0 months) for the stable dis-ease group, and 4.1 months (range 2.0-14.0 months) for the progressive diseasegroup, respectively. One patient withstage I resected disease remained incomplete remission over 13 months oftreatment. Two patients with resected
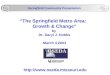
Figure 3. Kaplan-Meier survival curve for 25 patients treated with capecitabine and irradiation.
Saif#2-vol4no4 12/6/05 6:53 PM Page 643

Vol. 4, No. 4, 2004 • The Journal of Applied Research644
disease but positive margins progressedwith treatment after 6.2 and 14 months,respectively. Five patients with unre-sectable locally advanced disease wereconverted to resectable disease andtaken to resection. Of these, only 1 wassuccessfully resected.
SurvivalSurvival was measured from date of ini-tial treatment until date of death or untilthe end of the study period. Figure 3depicts the Kaplan-Meier survival curvefor the population. Median survival was14 months, with 50% of patients reach-ing the endpoint of death at 14 months.Survival ranged from 3.75 months to 17months. Average survival was 10.3months, with a standard deviation of 3.5months. Seven of the 25 patientsreviewed expired before the end of thestudy period, indicating that median andmean survival times are underestima-tions of actual survival.
DISCUSSIONPancreatic adenocarcinoma is the fourthmost common cause of adult cancerdeath. About 50% of patients presentwith metastatic disease, 20% withresectable disease and the remaining30% of patients are diagnosed withincurable, locally advanced unresectablebut nonmetastatic pancreatic cancer.1,4
Earle et al recently performed a system-atic review of the literature includingMEDLINE, CANCERLIT, andCochrane Library databases to evaluatethe current evidence regarding treat-ment of incurable, locally advanced,unresectable but nonmetastatic pancre-atic cancer and produced an evidence-based practice guideline.4 Eightrandomized trials were obtained thatmet the inclusion criteria. Current rec-ommendations are to offer combinedchemotherapy and radiotherapy to suit-able patients. The preferred chemothera-peutic agent to combine with
radiotherapy is bolus or infusional 5-flu-orouracil, but the optimal mode andduration of 5-fluorouracil delivery isunclear. Chemotherapy alone with gem-citabine is an acceptable alternative.Survival in the series of patients treatedwith fluoropyrimidine is similar to treat-ment with capecitabine in our patients.Fisher et al report a median survival of 7months in patients with locally advancedpancreatic cancer treated with infusional5-FU.12 Moertel et al report a mediansurvival of 7.5 months.1 Median survivalwith treatment with concurrentcapecitabine and irradiation was 14months. In our study, among 20 patientswith unresected tumor and who wereotherwise eligible candidates for resec-tion, 5 patients sustained a radiologicalresponse indicating laparotomy forresection. Of these, 1 patient was suc-cessfully resected. One patient who wassuccessfully resected with negative mar-gins maintained complete remissionthrough the end of the study period foran overall survival of 17 months.
The major benefit of capecitabinelies in its favorable toxicity profile. Aretrospective analysis of capecitabine inthe treatment of a series of gastrointesti-nal malignancies recently showed inci-dence of gastrointestinal toxicity andhand-foot syndrome to be comparableto that infusional 5-FU. This studyreviewed a number of different tumortypes, and the treatment period withcapecitabine was during radiation onlywithout analyzing ongoing treatmentwith cycles of capecitabine monothera-py.13 Our study also indicated that mosttoxicities were gastrointestinal, with rel-atively no grade 3/4 hematologic toxici-ties. However, over 50% of the patientsdid experience grade 1/2 anemia. Animportant consideration of oral therapyis vomiting sufficient to prevent absorp-tion of oral medication. In this series,12% of patients had grade 3/4 vomitingduring treatment, but patients were able
Saif#2-vol4no4 12/6/05 6:53 PM Page 644

The Journal of Applied Research • Vol. 4, No. 4, 2004 645
to maintain oral capecitabine. Toxicitycomparisons of 5-FU and capecitabineare perhaps best analyzed by looking atexperiences with other malignancies,namely colorectal malignancies. Aphase III study comparing oralcapecitabine to 5-FU in colorectal can-cer showed significantly less diarrhea,stomatitis, nausea, alopecia, and grade3/4 neutropenia with capecitabine,although grade 3 hand-foot syndromeand grade 3/4 hyperbilirubinemia weremore frequent with capecitabine.14 Thisis in comparison with a similar study inwhich gastrointestinal side effects weresimilar with capecitabine and 5-FU.5
Secondly, a phase II study has evalu-ated the efficacy of capecitabine inpatients with metastatic or unresectable,locally advanced pancreatic cancer.5Forty-two patients were treated withoral capecitabine 1,250 mg/m2 adminis-tered twice daily (2,500 mg/m2/d) asintermittent therapy in 3-week cyclesconsisting of 2 weeks of treatment fol-lowed by 1 week without treatment. Ten(24%) of 42 patients experienced a clini-cal benefit response (95% confidenceinterval [CI], 12.1% to 39.5%) as evi-denced by improvement in pain intensi-ty, analgesic consumption, and/orKarnofsky performance status. Three(7.3%) of the 41 patients with measura-ble disease had an objective response(partial). The median time to objectiveresponse was 85 days (range, 47 to 91days) and duration of response was 208,260, and 566 days for the 3 respondingpatients. One patient with nonmeasur-able but assessable disease hadimproved residual disease with a posi-tive clinical benefit response, for a totalof 4 responses among the 42 assessablepatients, for an overall response rate of9.5% (90% CI, 3.3% to 20.5%).Capecitabine was generally well tolerat-ed.5
Thirdly, there is also evidence thatthat ionizing radiation may increase the
therapeutic index of capecitabine. Datafrom human cancer xenograft studiessuggest that radiation upregulates TP intumor tissue.7 A single fraction of radia-tion (2.5 to 5 Gy) resulted in significantincrease in TP at 6, 9, and 18 days afterexposure in 4 of 5 xenograft models. A9.4 fold increase in tumor TP levels wasobserved after whole body irradiation,but no increase in liver TP levels wasfound. An increase in tumor levels ofTumor Necrosis Factor-alpha, anotherknown upregulator of TP, was alsoobserved to precede the increase intumor TP levels, suggesting that thismechanism is involved. The investigatorsalso demonstrated the effects of com-bined capecitabine-XRT on tumorgrowth using a WiDr human colon can-cer models, which is known to be refrac-tory to 5-FU due to low TP levels. Thetumor regrowth delay aftercapecitabine-XRT appeared to be morethan additive. In contrast, the tumorregrowth delay after 5-FU-XRT was lessthan additive.7
The major pitfall, as related to anyoral agent, is in patients controlling theirmedication. In this study, 2 patientsmade mistakes in dosing, which werecorrected 3 weeks into their 6-weekcourse of treatment. A close diary wasfollowed on each visit in which patientswere asked to write down the time theytake their capecitabine and sign. Arecent retrospective analysis of receiptof treatment for locally advanced pan-creatic cancer indicated that only 44%of patients in a series of 1,696 patientsreceived treatment.15 It is not clear thatoral treatment for pancreatic cancerwould significantly raise the number ofpatients treated as the risk factors citedin that study would not necessarily becorrected by an oral treatment.
In conclusion, capecitabine can besafely and conveniently administeredwith concurrent radiotherapy in thetreatment of locally advanced and
Saif#2-vol4no4 12/6/05 6:53 PM Page 645

Vol. 4, No. 4, 2004 • The Journal of Applied Research646
resected pancreatic cancer. Oralcapecitabine has good bioavailability,did not have problems associated withintolerance of oral medication, and hada tolerable side effect profile. Tumorresponse and survival were comparableif not better to standard treatment withinfusional 5-FU, although to test this rig-orously, a phase III trial comparing thetwo treatment routes would have to bestudied. Additionally, capecitabine hasthe convenience of oral administrationand avoidance of catheter related prob-lems. We are currently performing aphase I/II study to determine if TP isupregulated by administering radiationprior to capecitabine in locally advancedunresectable pancreatic cancer.16 Wealso aim to evaluate the role of TNF-alpha, if there is any.
REFERENCES1. Moertel CG, Frytak S, Hahn RG, et al.
Therapy of Locally Unresectable PancreaticCarcinoma: A Randomized Comparison ofHigh Dose (6000 Rads) Radiation Alone,Moderate Dose Radiation (4000 Rads + 5-Fluorouracil), and High Dose Radiation + 5-Fluorouracil. Cancer. 1981;48:1705-1710.
2. Burris HA III, Moore MJ, Andersen J, et al.Improvements in survival and clinical benefitwith gemcitabine as first-line therapy forpatients with advanced pancreas cancer: arandomized trial. J Clin Oncol. 1997;15:2403-2413.
3. Crane CH, Janjan NA, Evans DB, et al.Toxicity and efficacy of concurrent gemc-itabine and radiotherapy for locally advancedpancreatic cancer. Int J Pancreatol. 2001;29:9-18.
4. Earle CC, Agboola O, Maroun J, et al. Thetreatment of locally advanced pancreatic can-cer: a practice guideline. Can J Gastroenterol.2003;17:161-167.
5. Cartwright TH, Cohn A, Varkey JA, et al.Phase II study of oral capecitabine in patientswith advanced or metastatic pancreatic can-cer. J Clin Oncol. 2002;20:160-164.
6. Miwa M, Ura M, Nishida M, et al. Design of anovel oral fluoropyrimidine carbamate,capecitabine, which generates 5-fluorouracilselectively in tumours by enzymes concen-trated in human liver and cancer tissue. Eur JCancer. 1998;34:1274-1281.
7. Sawada N, Ishikawa T, Sekiguchi F, et al. X-ray irradiation induces thymidine phosphory-lase and enhances the efficacy of capecitabine(Xeloda) in human cancer xenografts. ClinCancer Res. 1999;5:2948-2953.
8. Van Cutsem E, Twelves C, Cassidy J, et al.Oral capecitabine compared with intravenousfluorouracil plus leucovorin in patients withmetastatic colorectal cancer: results of a largephase III study. J Clin Oncol. 2001;19:4097-4106.
9. Therasse P, Arbuck SG, Eisenhauer EA, et al.New guidelines to evaluate the response totreatment in solid tumors. EuropeanOrganization for Research and Treatment ofCancer, National Cancer Institute of theUnited States, National Cancer Institute ofCanada. J Natl Cancer Inst. 2000;92:205-216.
10. Cancer Therapy Evaluation Program.Common Toxicity Criteria, Version 2.0.DCTD, NCI, NIH, DHHS. March 1998.
11. Saif MW, Wood TE, McGee PJ, Diasio RB.Peripheral neuropathy associated withcapecitabine. Anticancer Drugs. 2004;15:767-771.
12. Fisher BJ, Perera FE, Kocha W, et al. Analysisof the clinical benefit of 5-fluorouracil andradiation treatment in locally advanced pan-creatic cancer. Int J Radiat Oncol Biol Phys.1999;45:291-295.
13. Vaishampayan UN, Ben-Josef E, Philip PA,Vaitkevicius VK, et al. A single-institutionexperience with concurrent capecitabine andradiation therapy in gastrointestinal malig-nancies. Int J Radiat Oncol Biol Phys.2002;53:675-679.
14. Hoff PM, Ansari R, Batist G, et al.Comparison of oral capecitabine versus intra-venous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastaticcolorectal cancer: results of a randomizedphase III study. J Clin Oncol. 2001;19:2282-2292.
15. Krzyzanowska MK, Weeks JC, Earle CC.Treatment of locally advanced pancreaticcancer in the real world: population-basedpractices and effectiveness. J Clin Oncol.2003;21:3409-3414.
16. Saif MW, Eloubeidi M, Thornton J, et al. Up-regulation of thymidine phosphorylase (TP)by radiotherapy (RT): A phase I study ofcapecitabine (CAP) with concurrent RT forpts with locally advanced (LA) pancreaticcancer (Pan Ca). J Clin Oncol. 2004;22(suppl14S):4104.
Saif#2-vol4no4 12/6/05 6:53 PM Page 646