Embed Size (px)
Citation preview
RACHEL ZASTROW, RN, MSN, CPPS
BETTER, FASTER, SAFER:
APPLYING HUMAN
FACTORS AND PATIENT
SAFETY PRINCIPLES TO
CRITICAL CARE
AACN, June 2015
LEARNING OBJECTIVES
• To describe Safety Science Basics: Swiss cheese model, safety current state in US
• Verbalize Human factors engineering basics and examples.
• Verbalize method of investigating unexpected or undesirable events.
• Describe case study for CLABSI prevention.
• Identify root causes in simplified real-world example.
• Discussion of real-world elements of CLABSI bundle and how to ensure good engineering and compliance.
SAFETY IN U.S. HEALTHCARE
• In 1999 The Institute of Medicine estimated that 98,000 people died annually in hospitals due to medical error
• In 2013 this number was revised to 210,000-440,000
• The equivalent of a jumbo jet crashing every day for a full year
We are NOT getting better!
ELEMENTS OF PATIENT SAFETY ERRORS
• Inherently unreliable human beings
Operating within
• Unreliable processes and systems
Caring for
• Medically fragile patients, with limited capacity to recover from errors
ERRORS WHAT IS A LATENT ERROR?
http://psnet.ahrq.gov/primer.aspx?primerID=10
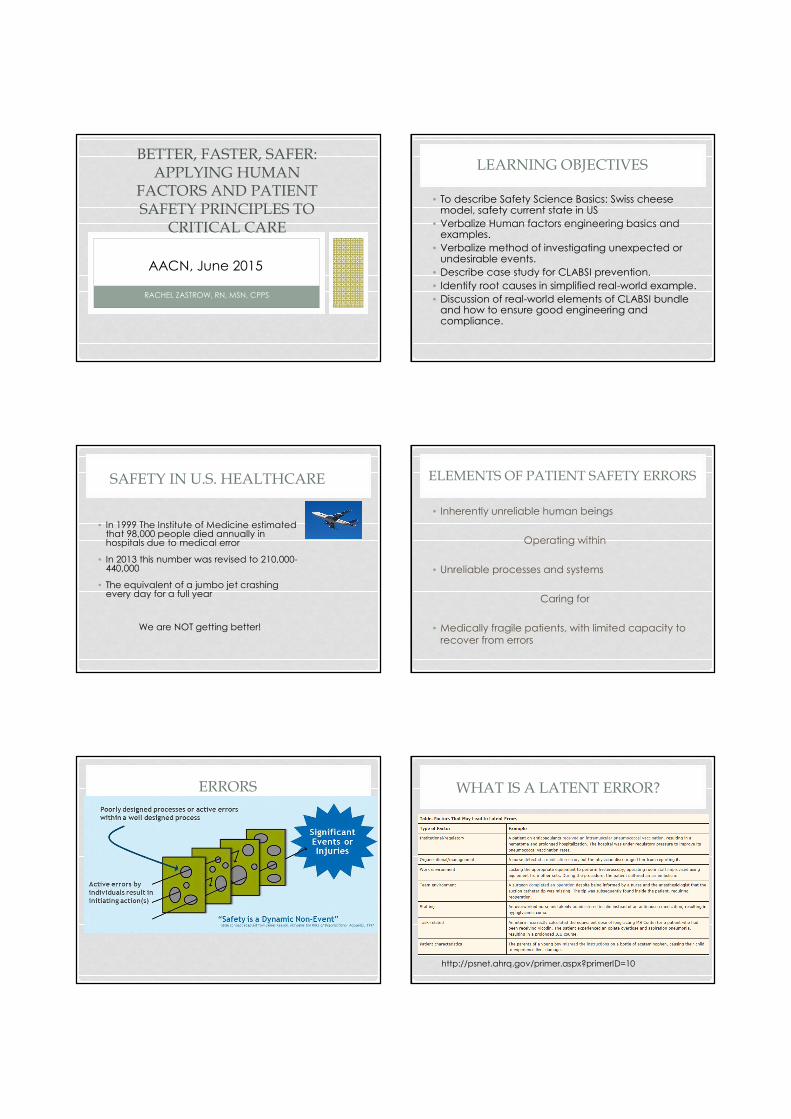
WHY SO MANY ERRORS?THE SWISS-CHEESE MODEL
Adapted from James Reason, Managing the Risks of Organizational Accidents (1997)
EVENTS ofHARM
Safety strategies
designed to stop errors
The HOLES represent
problems with the safety strategies
MEDICATION ADMINISTRATION
EVENTS ofHARM
Bar code scanning
Automated dispensing cabinet
tracking
Pharmacist
order review
Electronic
MAR
What are the safety strategies?
What are the holes in the strategies?
1. Poor wireless
connectivity
2. Med won’t scan
3. Emergency situation
4. No scanner
available
5. Scanner battery
dead
6. RN chooses not to
scan
Human FactorsWHAT IS HUMAN FACTORS?
• The science of
understanding the properties
of human capability
• The application of this
understanding to the design
and development of systems
Let’s see how many key words you can pick up…..
WHAT IS HUMAN FACTORS? INTUITIVE WORK PROCESSES
Our challenge…
To design work processes that make it easy to
do the right thing
Healthcare Performance Improvement 2014
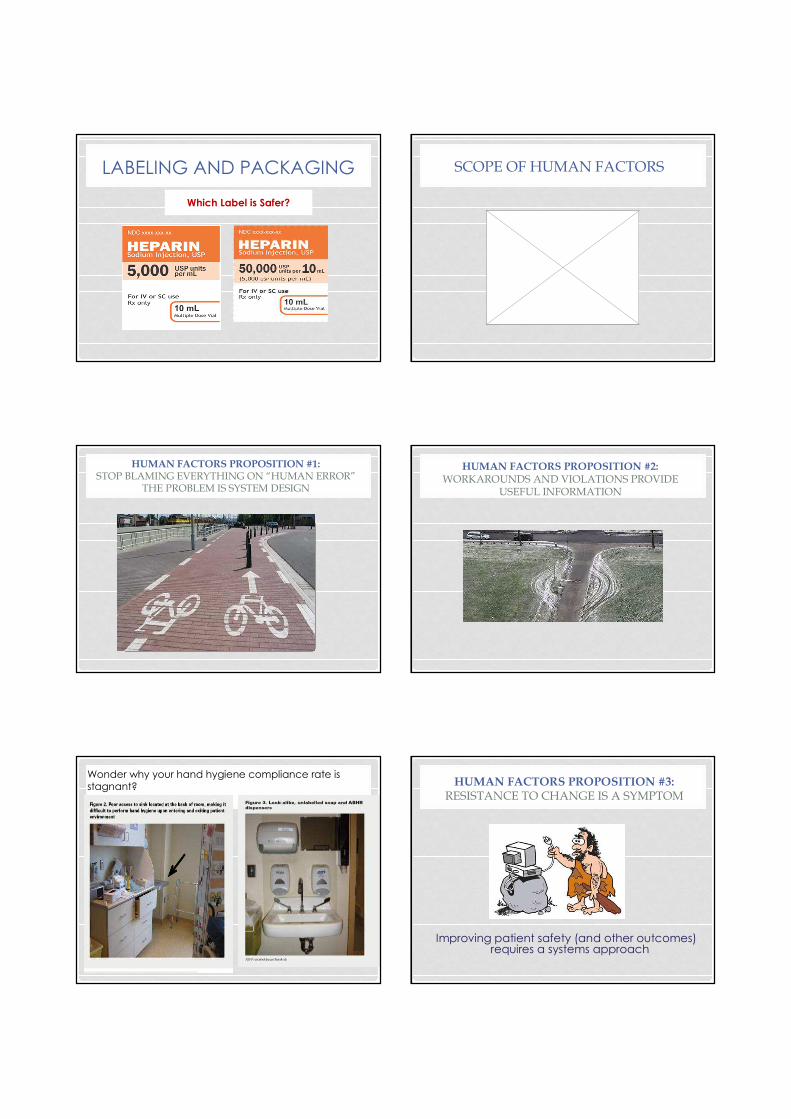
LABELING AND PACKAGING
Which Label is Safer?
SCOPE OF HUMAN FACTORS
HUMAN FACTORS PROPOSITION #1:
STOP BLAMING EVERYTHING ON “HUMAN ERROR”
THE PROBLEM IS SYSTEM DESIGN
HUMAN FACTORS PROPOSITION #2:
WORKAROUNDS AND VIOLATIONS PROVIDE
USEFUL INFORMATION
Wonder why your hand hygiene compliance rate is stagnant? HUMAN FACTORS PROPOSITION #3:
RESISTANCE TO CHANGE IS A SYMPTOM
Improving patient safety (and other outcomes) requires a systems approach
HUMAN FACTORS PROPOSITION #4:
IMPLEMENTING WELL DESIGNED AND WELL-
INTEGRATED TECHNOLOGY IS SMART
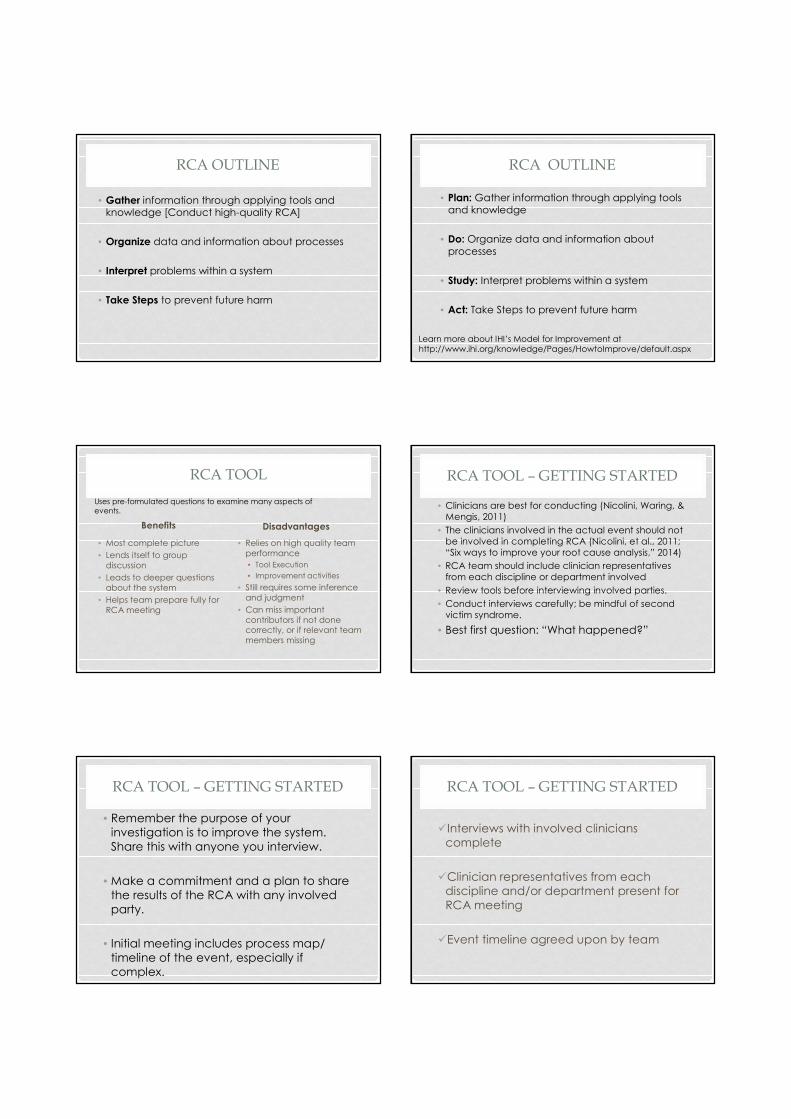
YOUR CHALLENGE:
WELL DESIGNED?
APPLYING HUMAN FACTORS
TO THE REAL WORLD…
A COMMON ICU PROBLEM
WHAT YOU NEED TO KNOW BEFORE ANY PATIENT SAFETY OR QUALITY IMPROVEMENT WORK
• The purpose of all QI work is to uncover latent and
active errors, with the purpose of correcting the system!
• The purpose is not, nor should it be, focused on targeting an individual.
THE SITUATION
• Mr. Jones has been diagnosed with a CLABSI in the intermediate care unit.
• First infection in over 12 months.
• Board has committed to elimination of healthcare acquired infections
• Long periods of success and literature indicates that virtual elimination is possible.
• Mr. Jones diagnosed with Sepsis
• ICU X 2 weeks, IMCU X 1 week before + blood cultures
• Comorbidities include
• Diabetes
• Age (78)
How will we figure out what happened?
WHAT IS A ROOT CAUSE ANALYSIS?
• Not a single unified process, but a collection of tools and knowledge that facilitates use of data and information about processes to interpret problems within a system with the goal of preventing future
harm.
RCA OUTLINE
• Gather information through applying tools and knowledge [Conduct high-quality RCA]
• Organize data and information about processes
• Interpret problems within a system
• Take Steps to prevent future harm
RCA OUTLINE
• Plan: Gather information through applying tools and knowledge
• Do: Organize data and information about
processes
• Study: Interpret problems within a system
• Act: Take Steps to prevent future harm
Learn more about IHI’s Model for Improvement at http://www.ihi.org/knowledge/Pages/HowtoImprove/default.aspx
RCA TOOL
Benefits
• Most complete picture
• Lends itself to group
discussion
• Leads to deeper questions
about the system
• Helps team prepare fully for
RCA meeting
Disadvantages
• Relies on high quality team
performance
• Tool Execution
• Improvement activities
• Still requires some inference
and judgment
• Can miss important
contributors if not done correctly, or if relevant team
members missing
Uses pre-formulated questions to examine many aspects of
events.
RCA TOOL – GETTING STARTED
• Clinicians are best for conducting (Nicolini, Waring, &
Mengis, 2011)
• The clinicians involved in the actual event should not
be involved in completing RCA (Nicolini, et al., 2011;
“Six ways to improve your root cause analysis,” 2014)
• RCA team should include clinician representatives
from each discipline or department involved
• Review tools before interviewing involved parties.
• Conduct interviews carefully; be mindful of second
victim syndrome.
• Best first question: “What happened?”
RCA TOOL – GETTING STARTED
• Remember the purpose of your
investigation is to improve the system.
Share this with anyone you interview.
• Make a commitment and a plan to share
the results of the RCA with any involved
party.
• Initial meeting includes process map/
timeline of the event, especially if
complex.
RCA TOOL – GETTING STARTED
�Interviews with involved clinicians
complete
�Clinician representatives from each
discipline and/or department present for
RCA meeting
�Event timeline agreed upon by team
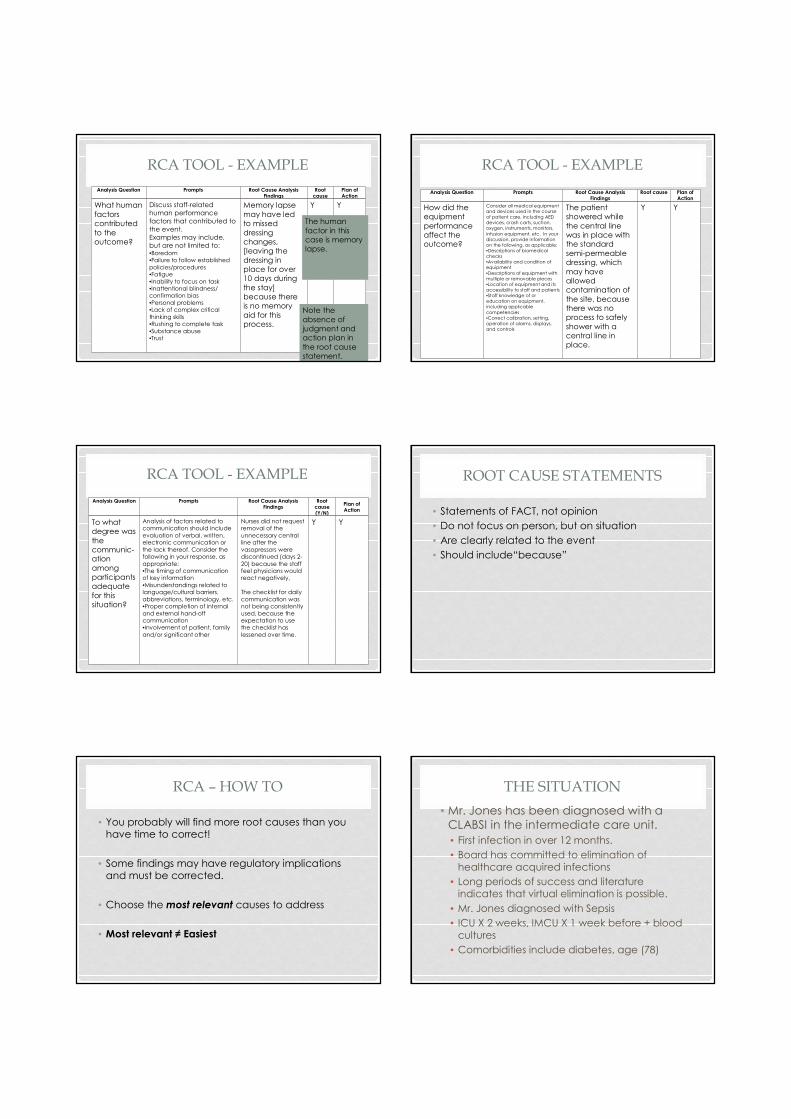
RCA TOOL - EXAMPLE
Analysis Question Prompts Root Cause Analysis Findings
Root cause
Plan of Action
What human
factors contributed
to the outcome?
Discuss staff-related
human performance
factors that contributed to
the event.
Examples may include,
but are not limited to:•Boredom•Failure to follow established
policies/procedures •Fatigue
•Inability to focus on task•Inattentional blindness/ confirmation bias
•Personal problems•Lack of complex critical
thinking skills•Rushing to complete task
•Substance abuse •Trust
Memory lapse
may have led to missed
dressing changes, [leaving the
dressing in place for over 10 days during
the stay] because there is no memory
aid for this process.
Y Y
The human
factor in this case is memory lapse.
Note the
absence of judgment and action plan in
the root cause statement.
RCA TOOL - EXAMPLE
Analysis Question Prompts Root Cause Analysis Findings
Root cause Plan of Action
How did the equipment
performance affect the outcome?
Consider all medical equipment
and devices used in the course
of patient care, including AED
devices, crash carts, suction,
oxygen, instruments, monitors,
infusion equipment, etc. In your
discussion, provide information
on the following, as applicable:
•Descriptions of biomedical
checks
•Availability and condition of
equipment
•Descriptions of equipment with
multiple or removable pieces
•Location of equipment and its
accessibility to staff and patients
•Staff knowledge of or
education on equipment,
including applicable
competencies
•Correct calibration, setting,
operation of alarms, displays,
and controls
The patient showered while
the central line was in place with the standard
semi-permeable dressing, which
may have allowed contamination of
the site, because there was no process to safely
shower with a central line in place.
Y Y
RCA TOOL - EXAMPLE
Analysis Question Prompts Root Cause Analysis Findings
Root cause (Y/N)
Plan of Action
To what degree was
the communic-ation
among participants adequate
for this situation?
Analysis of factors related to communication should include
evaluation of verbal, written, electronic communication or
the lack thereof. Consider the following in your response, as
appropriate:•The timing of communication of key information
•Misunderstandings related to language/cultural barriers,
abbreviations, terminology, etc.•Proper completion of internal
and external hand-off communication•Involvement of patient, family
and/or significant other
Nurses did not request removal of the
unnecessary central line after the
vasopressors were discontinued (days 2-
20) because the staff feel physicians would react negatively,
The checklist for daily
communication was not being consistently
used, because the expectation to use the checklist has
lessened over time.
Y Y
ROOT CAUSE STATEMENTS
• Statements of FACT, not opinion
• Do not focus on person, but on situation
• Are clearly related to the event
• Should include“because”
RCA – HOW TO
• You probably will find more root causes than you have time to correct!
• Some findings may have regulatory implications and must be corrected.
• Choose the most relevant causes to address
• Most relevant ≠ Easiest
THE SITUATION
• Mr. Jones has been diagnosed with a
CLABSI in the intermediate care unit.
• First infection in over 12 months.
• Board has committed to elimination of
healthcare acquired infections
• Long periods of success and literature indicates that virtual elimination is possible.
• Mr. Jones diagnosed with Sepsis
• ICU X 2 weeks, IMCU X 1 week before + blood
cultures
• Comorbidities include diabetes, age (78)
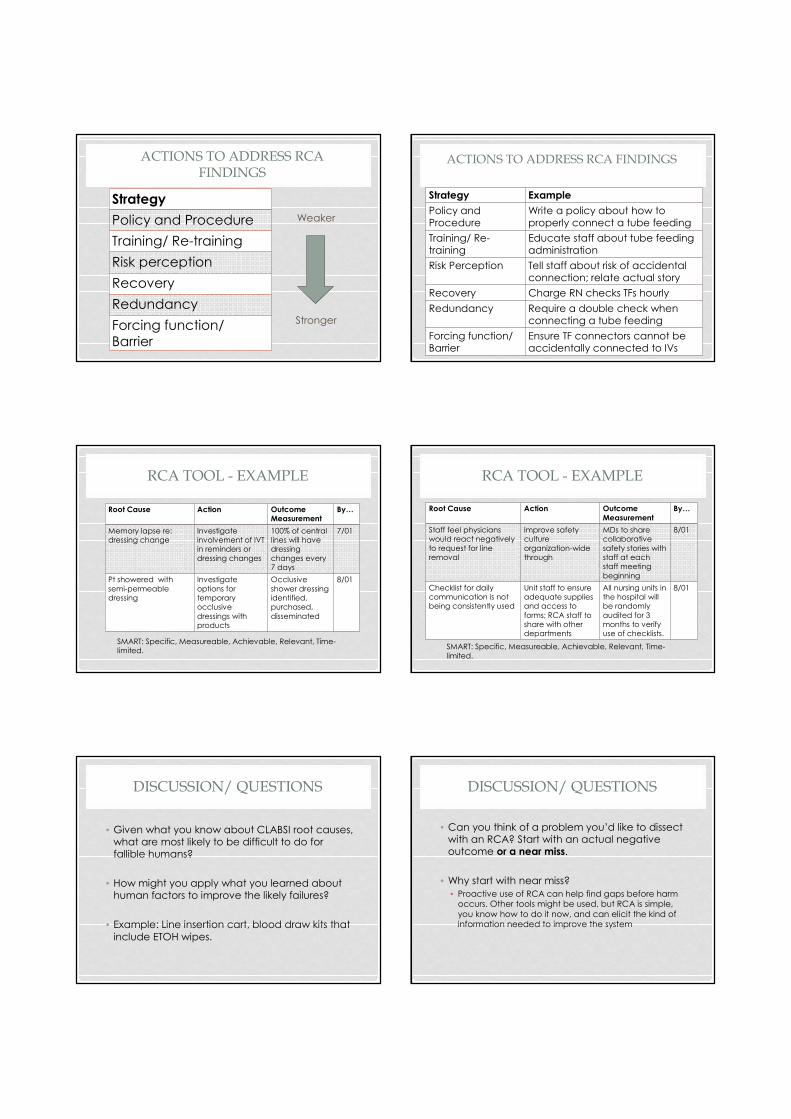
ACTIONS TO ADDRESS RCA
FINDINGS
Weaker
Stronger
Strategy
Policy and Procedure
Training/ Re-training
Risk perception
Recovery
Redundancy
Forcing function/
Barrier
ACTIONS TO ADDRESS RCA FINDINGS
Strategy Example
Policy and Procedure
Write a policy about how to properly connect a tube feeding
Training/ Re-training
Educate staff about tube feeding administration
Risk Perception Tell staff about risk of accidental connection; relate actual story
Recovery Charge RN checks TFs hourly
Redundancy Require a double check when connecting a tube feeding
Forcing function/ Barrier
Ensure TF connectors cannot be accidentally connected to IVs
RCA TOOL - EXAMPLE
Root Cause Action Outcome Measurement
By…
Memory lapse re: dressing change
Investigate involvement of IVT in reminders or
dressing changes
100% of central lines will have dressing
changes every 7 days
7/01
Pt showered with
semi-permeable dressing
Investigate
options for temporary occlusive
dressings with products
Occlusive
shower dressing identified, purchased,
disseminated
8/01
SMART: Specific, Measureable, Achievable, Relevant, Time-limited.
RCA TOOL - EXAMPLE
Root Cause Action Outcome
Measurement
By…
Staff feel physicians would react negatively
to request for line removal
Improve safety culture
organization-wide through
MDs to share collaborative
safety stories with staff at each staff meeting
beginning
8/01
Checklist for daily communication is not being consistently used
Unit staff to ensure adequate supplies and access to
forms; RCA staff to share with other departments
All nursing units in the hospital will be randomly
audited for 3 months to verify use of checklists.
8/01
SMART: Specific, Measureable, Achievable, Relevant, Time-
limited.
DISCUSSION/ QUESTIONS
• Given what you know about CLABSI root causes, what are most likely to be difficult to do for fallible humans?
• How might you apply what you learned about human factors to improve the likely failures?
• Example: Line insertion cart, blood draw kits that
include ETOH wipes.
DISCUSSION/ QUESTIONS
• Can you think of a problem you’d like to dissect with an RCA? Start with an actual negative outcome or a near miss.
• Why start with near miss?
• Proactive use of RCA can help find gaps before harm occurs. Other tools might be used, but RCA is simple,
you know how to do it now, and can elicit the kind of information needed to improve the system
RESOURCES
http://www.jointcommission.org/Framework_for_Conducting_a_Root_Cause_Analysis_and_Action_Plan/
Joint commission RCA Action Plan
Nicolini, J., Waring D., & Mengis, J. (2011). The challenges of undertaking root cause analysis in health care: a qualitative study. Journal of Health Services Research & Policy, 16 (Suppl 1) 34-41.
"6 Ways to Improve Your Root Cause Analysis." Healthcare Risk Management. AHC Media L.L.C. 2013. Retrieved March 02, 2014 from HighBeam Research: http://www.highbeam.com/doc/1G1-340759899.html
RESOURCES
http://psnet.ahrq.gov/primer.aspx?primerID=10
Patient Safety Primer: Root Cause Analysis
http://patientsafetyed.duhs.duke.edu/module_e/swiss_cheese.html
http://www.ihi.org/knowledge/Pages/HowtoImprove/default.aspx
IHI Improvement model