Embed Size (px)
Citation preview
SAFE STEMI for Seniors: a PASSION proof of concept study
Predictable And SuStainable Implementation Of National CardioVascular Registries Thinktank(PASSION CV Registries Thinktank)
SAFE STEMI for Seniors: a PASSION proof of concept study
Predictable And SuStainable Implementation Of National CardioVascular Registries Thinktank(PASSION CV Registries Thinktank)
October 15, 2014October 15, 2014
Proof of Concept vs. Leap of Faith?
Proof of Concept vs. Leap of Faith?
NCRI Data InfrastructureNCRI Data Infrastructure
Internal Randomization Integrated EMR->NCDR->EDC data EDC data collection for supplemental research
data (e.g. study drug admin, efficacy details) Consistent application of data validation rules Data output using CDISC SDTM 21CFR11 Compliant

NCRI WorkflowNCRI Workflow
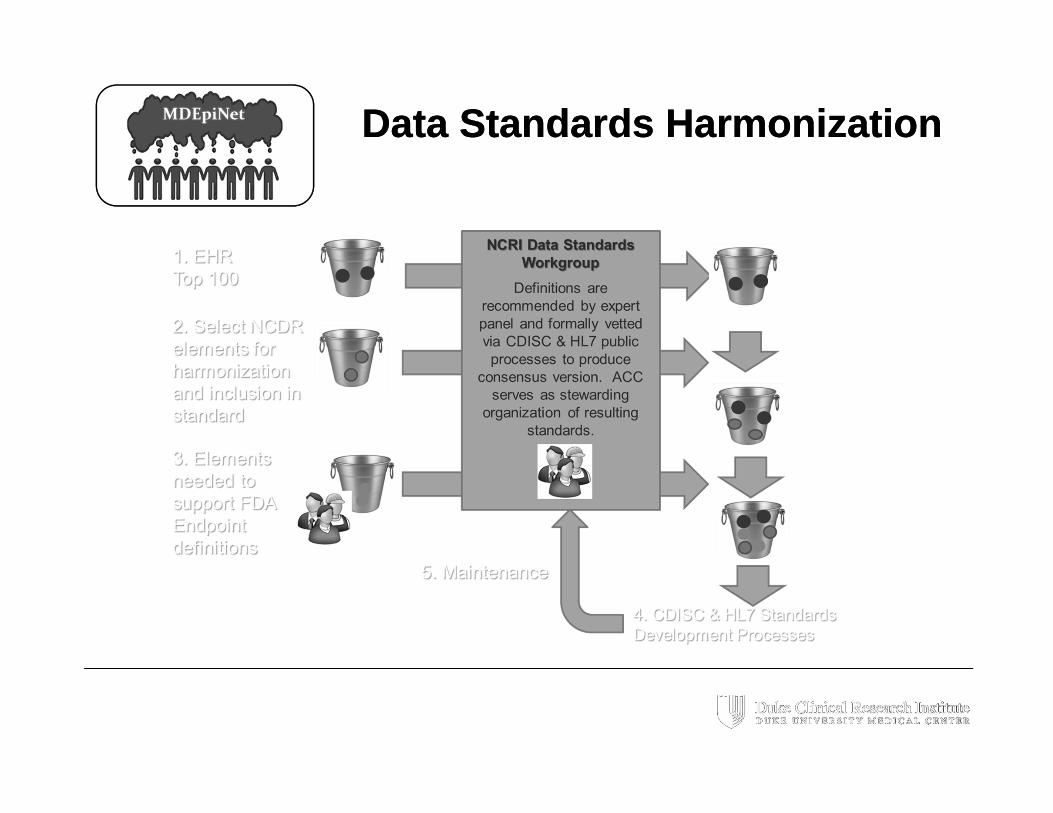
Data Standards HarmonizationData Standards Harmonization
Initial Proof of ConceptInitial Proof of Concept
Randomized open-label trial of women undergoing PCI Hypothesis: Compared with femoral, the radial approach is:
Superior with respect to bleeding and vascular complications Non-inferior with respect to procedural failure
Protocol standardized “Best” background medical therapy to minimize bleeding risk and ischemic complications
Bivalirudin Prasugrel for ACS patients < 75 years old, no prior stroke, body
weight > 60 kg; clopidogrel otherwise GP IIb/IIIa inhibitors at operators’ discretion, intention specified
prior to randomization Arteriotomy management
Patent hemostasis mandated for radial patients Femoral closure devices allowed at operator discretion
Randomized open-label trial of women undergoing PCI Hypothesis: Compared with femoral, the radial approach is:
Superior with respect to bleeding and vascular complications Non-inferior with respect to procedural failure
Protocol standardized “Best” background medical therapy to minimize bleeding risk and ischemic complications
Bivalirudin Prasugrel for ACS patients < 75 years old, no prior stroke, body
weight > 60 kg; clopidogrel otherwise GP IIb/IIIa inhibitors at operators’ discretion, intention specified
prior to randomization Arteriotomy management
Patent hemostasis mandated for radial patients Femoral closure devices allowed at operator discretion
Initial Proof-of-Concept: TREATT / SAFE-PCIInitial Proof-of-Concept: TREATT / SAFE-PCI
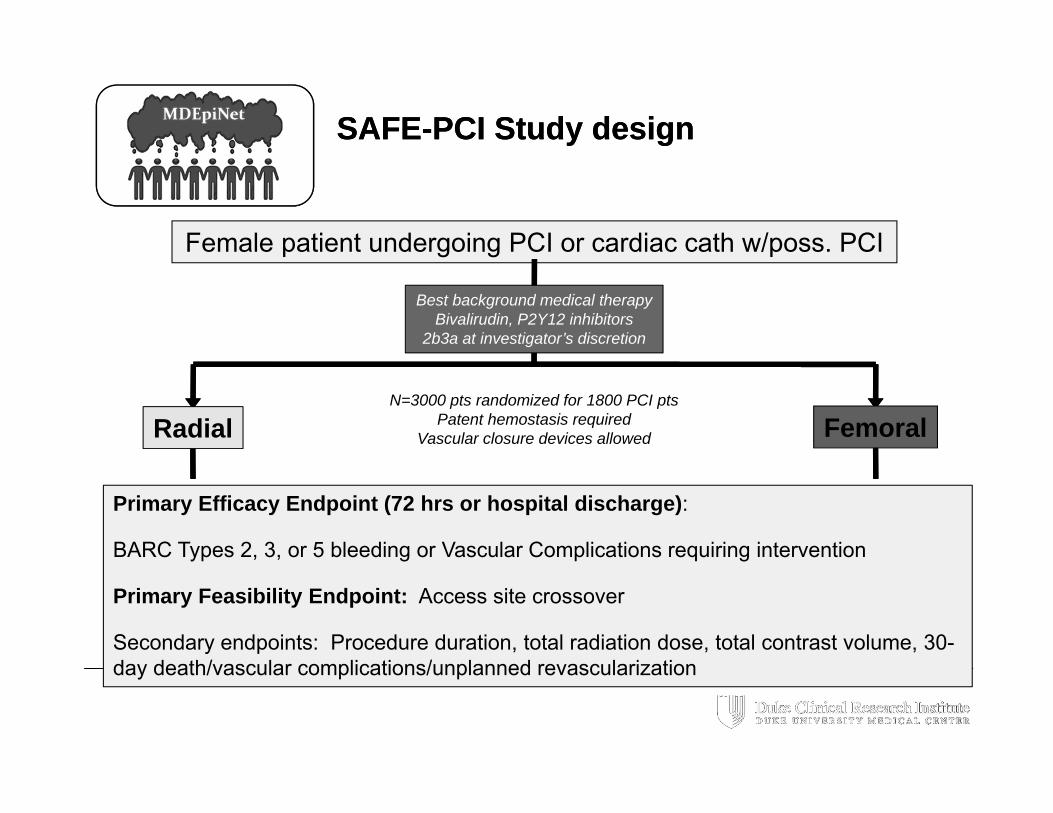
SAFE-PCI Study designSAFE-PCI Study design
Female patient undergoing PCI or cardiac cath w/poss. PCI
Best background medical therapyBivalirudin, P2Y12 inhibitors
2b3a at investigator’s discretion
N=3000 pts randomized for 1800 PCI ptsPatent hemostasis required
Vascular closure devices allowed
Primary Efficacy Endpoint (72 hrs or hospital discharge):
BARC Types 2, 3, or 5 bleeding or Vascular Complications requiring intervention
Primary Feasibility Endpoint: Access site crossover
Secondary endpoints: Procedure duration, total radiation dose, total contrast volume, 30-day death/vascular complications/unplanned revascularization
Radial Femoral
NCRI and TREATT / SAFE-PCINCRI and TREATT / SAFE-PCI
As the first registry-based randomized trial in the US, the SAFE-PCI for Women trial demonstrated a new paradigm for conducting efficient pragmatic clinical trials using a National Cardiovascular Research Infrastructure
1787 women randomized at 60 US sites 96.7% of sites enrolled ≥ 1 subject 70.9% of sites enrolled ≥ 10 subjects
High quality data; Adjudication possible
CFR Part 11 compliant – IND and IDE applications
Faster enrollment, Reduced site workload by ~ 30%
Reduced costs (total budget ~ $5 million)
As the first registry-based randomized trial in the US, the SAFE-PCI for Women trial demonstrated a new paradigm for conducting efficient pragmatic clinical trials using a National Cardiovascular Research Infrastructure
1787 women randomized at 60 US sites 96.7% of sites enrolled ≥ 1 subject 70.9% of sites enrolled ≥ 10 subjects
High quality data; Adjudication possible
CFR Part 11 compliant – IND and IDE applications
Faster enrollment, Reduced site workload by ~ 30%
Reduced costs (total budget ~ $5 million)
Proof of ConceptProof of Concept
Study of Access site For Enhancing PCI in STEMI for Seniors(SAFE-STEMI for Seniors)
Study of Access site For Enhancing PCI in STEMI for Seniors(SAFE-STEMI for Seniors)
Next stage in proofs-of-concept
Public health focus: Senior population (both genders, age >= 65 years)
NCDR registry prospectively linked with claims data for long term (1-year) follow up
Randomization with factorial design radial vs. femoral access Single IRA only vs. IFR guided multivessel
intervention
Next stage in proofs-of-concept
Public health focus: Senior population (both genders, age >= 65 years)
NCDR registry prospectively linked with claims data for long term (1-year) follow up
Randomization with factorial design radial vs. femoral access Single IRA only vs. IFR guided multivessel
intervention
SAFE-STEMI for SeniorsSAFE-STEMI for Seniors
Data to evaluate therapeutic strategy and support two independent IDEs
Hypotheses: Superior bleeding and clinical outcome (NACE) at 1
year associated with radial vs. femoral vascular access
Superior death, re-MI & refractory angina associated with iFR guided multi-vessel PCI vs. IRA-only
1 year MACE performance goal for second generation DES
Data to evaluate therapeutic strategy and support two independent IDEs
Hypotheses: Superior bleeding and clinical outcome (NACE) at 1
year associated with radial vs. femoral vascular access
Superior death, re-MI & refractory angina associated with iFR guided multi-vessel PCI vs. IRA-only
1 year MACE performance goal for second generation DES
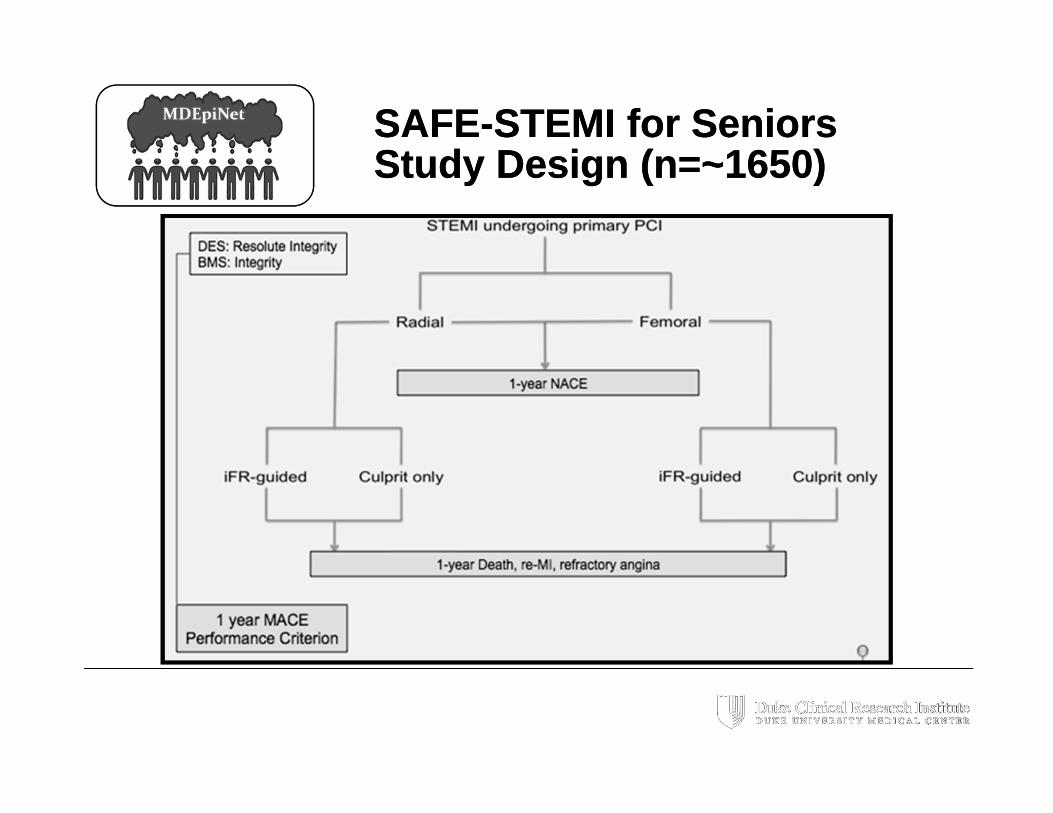
SAFE-STEMI for SeniorsStudy Design (n=~1650)SAFE-STEMI for SeniorsStudy Design (n=~1650)
Key ChallengesKey Challenges
Data Specifications Atomic definitions Timing Qualifiers Observed vs explicit
response
Parallel Workflows Patient Care Clinical Research QI Registry
Systems Interfaces More interfaces Validation purpose
Data Specifications Atomic definitions Timing Qualifiers Observed vs explicit
response
Parallel Workflows Patient Care Clinical Research QI Registry
Systems Interfaces More interfaces Validation purpose
Opportunity: ReusabilityOpportunity: Reusability
Beyond the horizonBeyond the horizon
Reusable infrastructure may facilitate opportunities for informative registry-based studies and simultaneous evaluation of treatment strategies
Consistent data standards and workflows create downstream efficiencies for future investigations
Integration with EHR initiatives will evaporate the distinction between source documents and CRFs
Reusable infrastructure may facilitate opportunities for informative registry-based studies and simultaneous evaluation of treatment strategies
Consistent data standards and workflows create downstream efficiencies for future investigations
Integration with EHR initiatives will evaporate the distinction between source documents and CRFs