Embed Size (px)
Citation preview
Safe and Effective Use of Insulin in the Hospital Setting
1

Recommended Glycemic TargetsRecommended Glycemic Targets in the Hospital Setting
2009 AACE and ADA Joint Consensus Statement
8 /dLICU
140‐180 mg/dL(Lower target may be appropriate in select patients, but targets < 110 mg/dL are NOT recommended)
Non‐critically ill patients
Premeal < 140 mg/dLRandom < 180 mg/dL
AACE, American Association of Clinical Endocrinologists; ADA, American Diabetes Association; ICU, intensive care unit.
Moghissi ES, et al. Endocr Pract. 2009;15(4):1‐17.Moghissi ES, et al. Diabetes Care. 2009 32(6):1119‐1131.
Summary:For critically-ill patients, the AACE and ADA recommend: Initiation of insulin at a threshold of no greater than 180 mg/dLMaintain a glucose range of 140 to 180 mg/dL
For Non-Critically ill patients, the recommendations are:Premeal BG target < 140 mg/dL in conjunction with a random BG target of < 180 mg/dL (provided they can be achieved safely)< 180 mg/dL (provided they can be achieved safely)More stringent targets may be appropriate in stable patients with previous tight glycemic controlLess stringent targets may be appropriate in terminally ill or those with severe comorbidities
ReferencesMoghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract. 2009;15:353-369.Moghissi ES, Korytkowski MT, DiNardo M, Einhorn D, Hellman R, Hirsch IB, Inzucchi SE, Ismail-Beigi F, Kirkman MS, Umpierrez GE; American Association of Clinical Endocrinologists; American Diabetes Association. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient
2
Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009 Jun;32(6):1119-1131

Methods for Managing g gHyperglycemia in
Hospitalized PatientsContinuous variable‐rate intravenous (IV) insulin drip
– Regular insulin
Basal/bolus therapy (MDI ‐multiple daily injections)
– Long‐acting and rapid‐acting insulin analogs
– Regular human insulin and NPH
NPH, Neutral Protamine Hagedorn insulin
Moghissi ES, et al. Endocr Pract. 2009;15(4):1‐17.Moghissi ES, et al. Diabetes Care. 2009 32(6):1119‐1131.
SummaryInsulin therapy is the preferred method of glycemic control in the majority of hospitalized patients because of its rapid half-life, its powerful glucose-lowering ability, and the ease by which it can be titrated to adjust to the changing medical status of hospitalized patients. In the intensive care units, intravenous infusion of insulin is the preferred route of administration. Outside of critical care units, subcutaneous insulin administration is a more common method of insulin delivery.
ReferencesMoghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract. 2009;15:353-369.Moghissi ES, Korytkowski MT, DiNardo M, Einhorn D, Hellman R, Hirsch IB, Inzucchi SE, Ismail Beigi F Kirkman MS Umpierrez GE; American Association of ClinicalIsmail-Beigi F, Kirkman MS, Umpierrez GE; American Association of Clinical Endocrinologists; American Diabetes Association. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009 Jun;32(6):1119-1131.
3

Limitations of Oral Agents inLimitations of Oral Agents in the Hospital Setting
Metformin is contraindicated in patients with renal failure
Thiazolidinediones must be discontinued in any Thiazolidinediones must be discontinued in any patient with congestive heart failure
Long‐acting secretagogues (sulfonylureas, glinides) can cause profound hypoglycemia and are not easily titrated
Moghissi ES, et al. Endocr Pract. 2009;15(4):1‐17.Moghissi ES, et al. Diabetes Care. 2009;32(6):1119‐1131.
SummaryEach of the major classes of non-insulin glucose-lowering drugs has significant limitations for inpatient use and thus, they are generally not recommended. These agents provide little flexibility or opportunity for titration in a setting where acute changes in patient status often demand such action. Despite the shortcomings for use of these agents in the inpatient setting, for patients whose glycemia was well controlled on oral agents prior to admission, transition to oral agents in the day or t i t di h i fttwo prior to discharge is often necessary.
ReferencesMoghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract. 2009;15:353-369.M hi i ES K tk ki MT DiN d M Ei h D H ll R Hi h IB I hi SEMoghissi ES, Korytkowski MT, DiNardo M, Einhorn D, Hellman R, Hirsch IB, Inzucchi SE, Ismail-Beigi F, Kirkman MS, Umpierrez GE; American Association of Clinical Endocrinologists; American Diabetes Association. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009 Jun;32(6):1119-1131.
4
Barriers to Effective HyperglycemiaBarriers to Effective Hyperglycemia Control in the Inpatient Setting
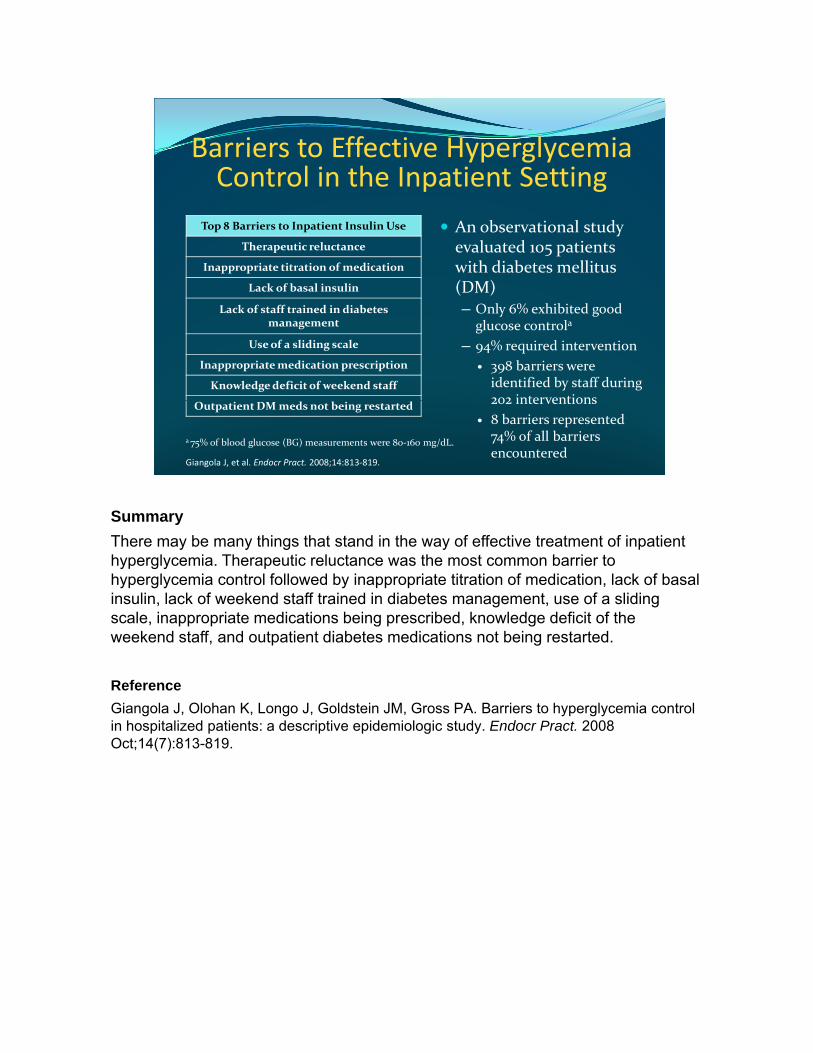
An observational study evaluated 105 patients with diabetes mellitus
Top 8 Barriers to Inpatient Insulin Use
Therapeutic reluctance
Inappropriate titration of medication
(DM)─ Only 6% exhibited good
glucose controla
─ 94% required intervention398 barriers were identified by staff during 202 interventions
Lack of basal insulin
Lack of staff trained in diabetes management
Use of a sliding scale
Inappropriate medication prescription
Knowledge deficit of weekend staff202 interventions8 barriers represented 74% of all barriers encountered
Outpatient DM meds not being restarted
a 75% of blood glucose (BG) measurements were 80‐160 mg/dL.
Giangola J, et al. Endocr Pract. 2008;14:813‐819.
SummaryThere may be many things that stand in the way of effective treatment of inpatient hyperglycemia. Therapeutic reluctance was the most common barrier to hyperglycemia control followed by inappropriate titration of medication, lack of basal insulin, lack of weekend staff trained in diabetes management, use of a sliding scale, inappropriate medications being prescribed, knowledge deficit of the weekend staff, and outpatient diabetes medications not being restarted.
ReferenceGiangola J, Olohan K, Longo J, Goldstein JM, Gross PA. Barriers to hyperglycemia control in hospitalized patients: a descriptive epidemiologic study. Endocr Pract. 2008 Oct;14(7):813-819.
Some Indications for Intravenous Insulin Therapyin the Hospital
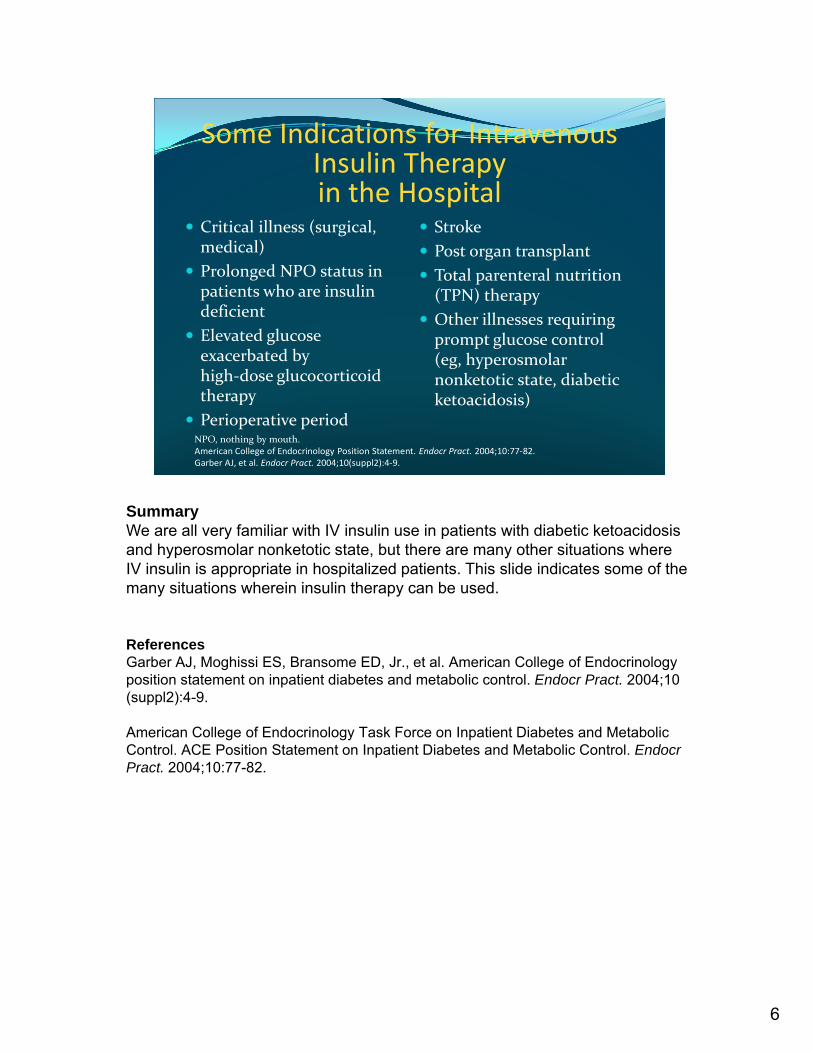
Critical illness (surgical, medical)Prolonged NPO status in
StrokePost organ transplant Total parenteral nutrition Prolonged NPO status in
patients who are insulin deficient Elevated glucose exacerbated by high‐dose glucocorticoid therapy
Total parenteral nutrition (TPN) therapyOther illnesses requiring prompt glucose control (eg, hyperosmolar nonketotic state, diabetic ketoacidosis)therapy
Perioperative periodketoacidosis)
NPO, nothing by mouth.American College of Endocrinology Position Statement. Endocr Pract. 2004;10:77‐82.Garber AJ, et al. Endocr Pract. 2004;10(suppl2):4‐9.
SummaryW ll f ili ith IV i li i ti t ith di b ti k t id iWe are all very familiar with IV insulin use in patients with diabetic ketoacidosis and hyperosmolar nonketotic state, but there are many other situations where IV insulin is appropriate in hospitalized patients. This slide indicates some of the many situations wherein insulin therapy can be used.
ReferencesGarber AJ, Moghissi ES, Bransome ED, Jr., et al. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Pract. 2004;10 (suppl2):4-9.
American College of Endocrinology Task Force on Inpatient Diabetes and Metabolic Control. ACE Position Statement on Inpatient Diabetes and Metabolic Control. Endocr Pract. 2004;10:77-82.
6

Subcutaneous InsulinSubcutaneous Insulin Therapy in the Hospital
Principles are borrowed from outpatient therapyProvide standing insulin orders– Basal / Prandial / Supplemental (correction)Assess insulin needs in the context of intercurrent stress / medications affecting glucoseDo not omit doses for good control or mild hypoglycemiaReview glucose results and adjust insulin dailyReview chart for unusual circumstancesReview chart for unusual circumstances– Missed meals, hypoglycemia treatment, late insulin
Korytkowski M. ACP Hospitalist. 2009;12(suppl):15‐23. http://www.acphospitalist.org/archives/2009/12/hyperglycemia.pdf.Accessed November 15, 2010; Expert Opinion, Evidence Level C.
SummaryThe principles of subcutaneous insulin therapy in the hospital setting are borrowed from outpatient therapy and revolve around physiologic insulin replacement. Scheduled SC insulin that includes an intermediate or long-acting insulin preparation (basal insulin) in combination with short- or rapid-acting insulin (bolus) is the preferred method of glycemic management for most patients with a history of diabetes or new-onset hyperglycemia in non–
iti l h it l tticritical care hospital settings.
ReferenceKorytkowski M. Treatment options for safely achieving glycemic targets in the hospital. ACP Hospitalist. 2009;12(suppl):15-23. Available at: http://www.acphospitalist.org/archives/2009/12/hyperglycemia.pdf.
7
Subcutaneous Insulin TherapySubcutaneous Insulin Therapy Definitions
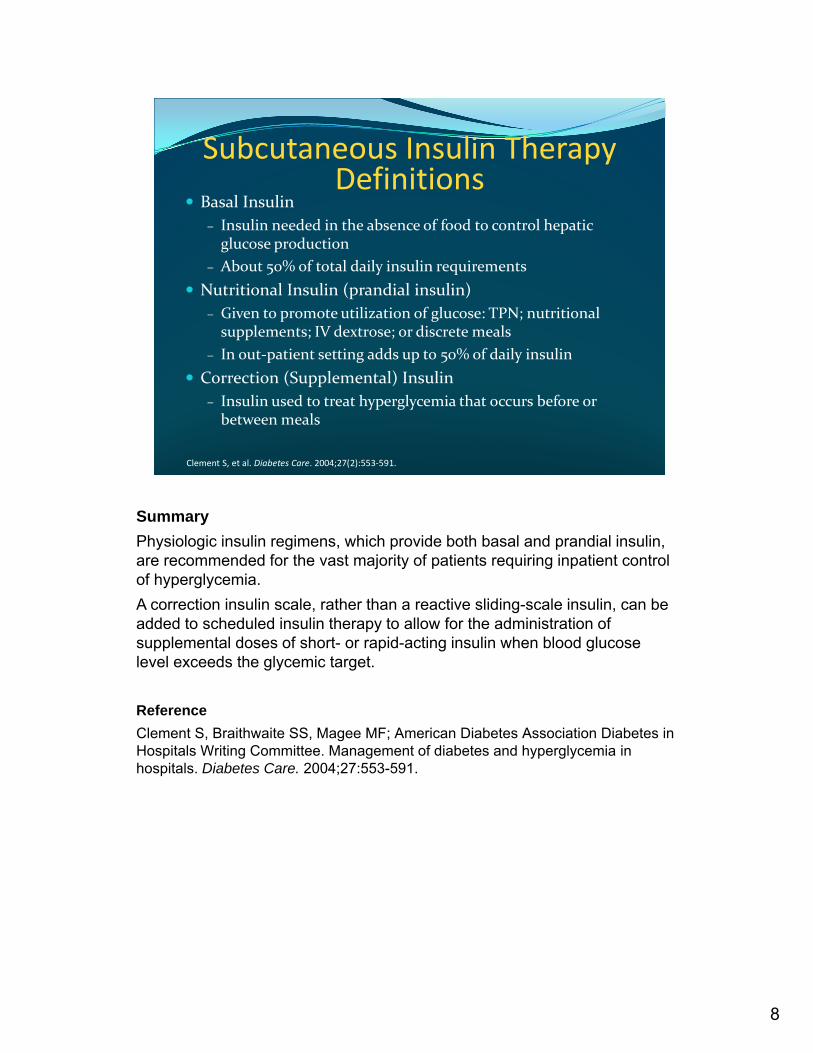
Basal Insulin – Insulin needed in the absence of food to control hepatic glucose production
– About 50% of total daily insulin requirementsNutritional Insulin (prandial insulin) – Given to promote utilization of glucose: TPN; nutritional supplements; IV dextrose; or discrete meals
– In out‐patient setting adds up to 50% of daily insulinCorrection (Supplemental) Insulin
Insulin used to treat hyperglycemia that occurs before or – Insulin used to treat hyperglycemia that occurs before or between meals
Clement S, et al. Diabetes Care. 2004;27(2):553‐591.
SummaryPhysiologic insulin regimens, which provide both basal and prandial insulin, are recommended for the vast majority of patients requiring inpatient control of hyperglycemia.A correction insulin scale, rather than a reactive sliding-scale insulin, can be added to scheduled insulin therapy to allow for the administration of supplemental doses of short- or rapid-acting insulin when blood glucose level exceeds the glycemic target.
ReferenceClement S, Braithwaite SS, Magee MF; American Diabetes Association Diabetes in Hospitals Writing Committee. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
8
Maintaining Physiologic InsulinMaintaining Physiologic Insulin Delivery in the Hospital:
Basal Bolus
Supplemental or
Breakfast Lunch Dinner BedtimeBasal insulin
Mealtime insulin(bolus)
Supplemental or Correction insulin
Insulin
Breakfast Lunch Dinner Bedtime
Clement S, et al. Diabetes Care. 2004;27(2):553‐591.
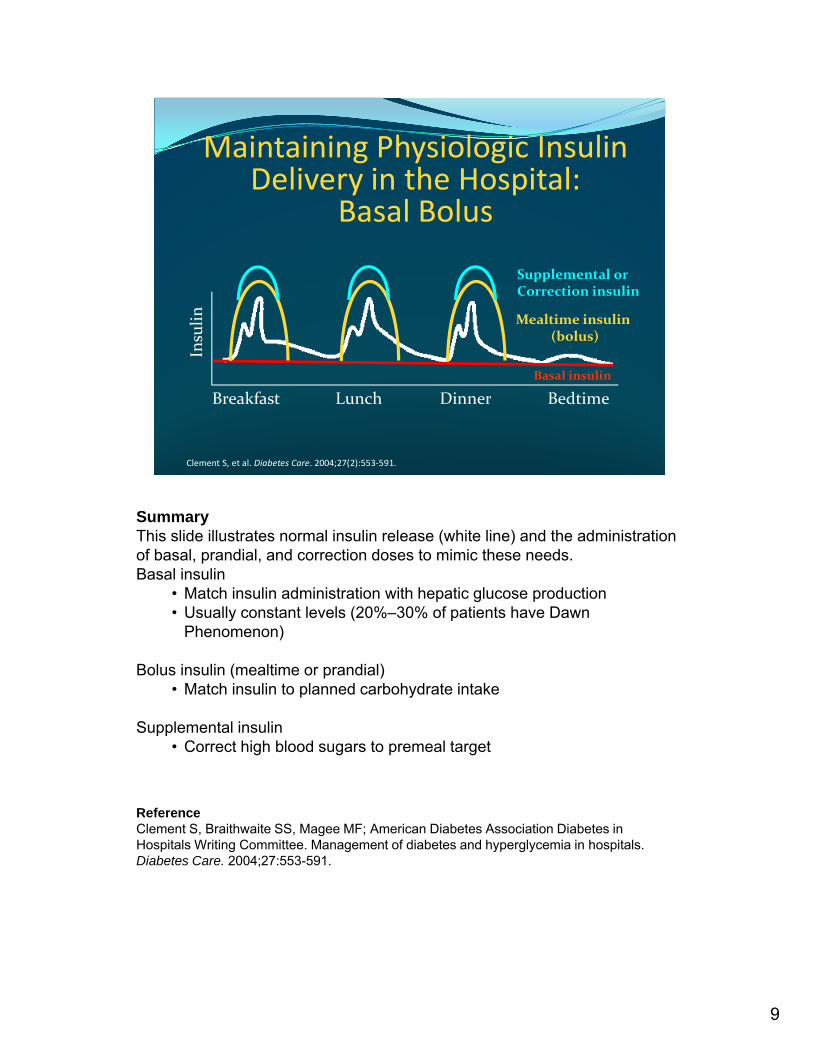
SummaryThis slide illustrates normal insulin release (white line) and the administration of basal, prandial, and correction doses to mimic these needs.Basal insulin
• Match insulin administration with hepatic glucose production• Usually constant levels (20%–30% of patients have Dawn
Phenomenon)
Bolus insulin (mealtime or prandial)• Match insulin to planned carbohydrate intake
Supplemental insulin• Correct high blood sugars to premeal target
ReferenceClement S, Braithwaite SS, Magee MF; American Diabetes Association Diabetes in Hospitals Writing Committee. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
9
Options forOptions forBasal and Prandial Insulin
Analogs Analogs
Options for basal insulin (controlling BG in fasting state)
Options for nutritional insulin (controlling BG when there is caloric intake)
AnalogsAnalogs– Detemir
– Glargine
Human– NPH
Analogs– Aspart– Glulisine– Lispro
Human– Regular
Analogs1. Altered Absorption
Characteristics
2. More Physiologic Approach
3. Alleviate the inconvenience and problems with traditional preparations
Clement S, et al. Diabetes Care. 2004;27(2):553‐591.
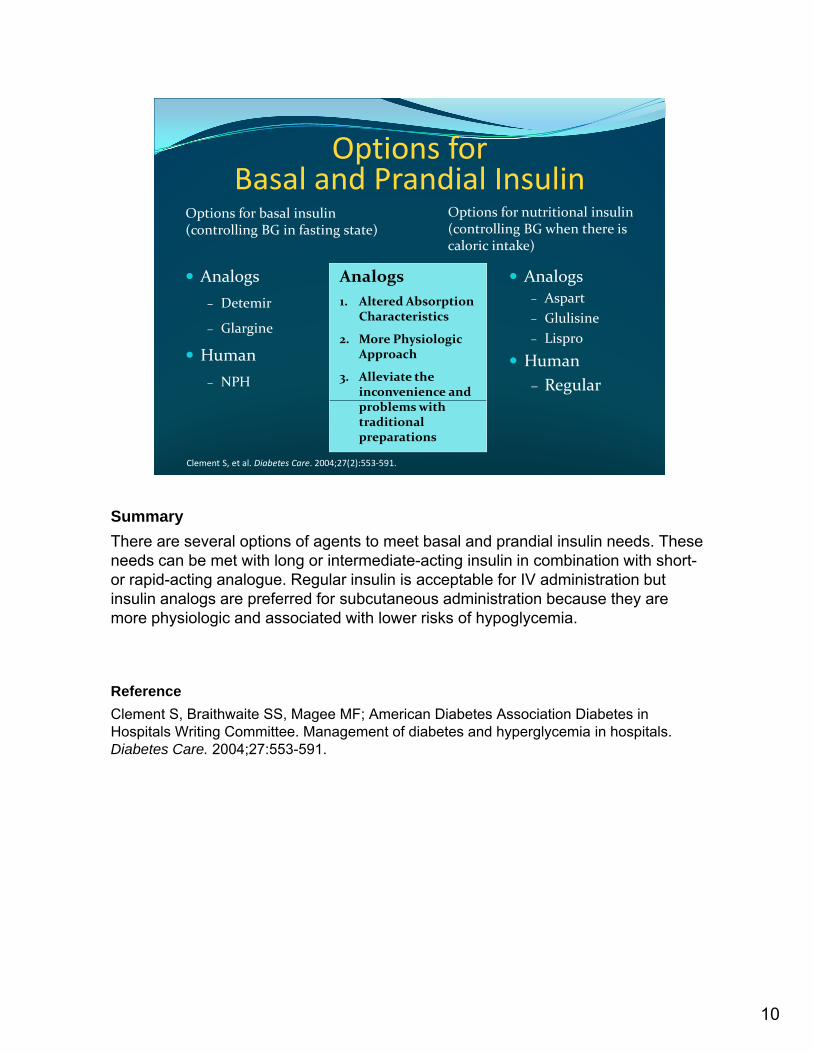
SummaryThere are several options of agents to meet basal and prandial insulin needs. These needs can be met with long or intermediate-acting insulin in combination with short-or rapid-acting analogue. Regular insulin is acceptable for IV administration but insulin analogs are preferred for subcutaneous administration because they are more physiologic and associated with lower risks of hypoglycemia.
ReferenceClement S, Braithwaite SS, Magee MF; American Diabetes Association Diabetes in Hospitals Writing Committee. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553-591.
10
Use of “Sliding‐Scale” InsulinUse of Sliding‐Scale Insulin Alone is Discouraged
Evidence does not support this technique without basal insulin
Hazards of sliding scale insulin use exceed the Hazards of sliding‐scale insulin use exceed the advantages of its convenience
Leads to rapid changes in BG levels resulting in exacerbation of both hyperglycemia and hypoglycemia
Possible iatrogenic diabetic ketoacidosis in hospitalized patients with T1DMpatients with T1DM
Moghissi ES, et al. Endocr Pract. 2009;15(4):1‐17.Moghissi ES, et al. Diabetes Care. 2009;32(6):1119‐1131.
SummaryUnfortunately, sliding-scale insulin, which is reactive and not a proactive physiologic approach, remains the treatment of choice for clinicians at many institutions.
Sliding scale insulin regimens are not recommended because they may result in unacceptably high rates of hyperglycemia, hypoglycemia, and i t i di b ti k t id i i h it li d ti t S h d l d di liatrogenic diabetic ketoacidosis in hospitalized patients. Scheduled prandial insulin doses should be given in relation to meals and should be adjusted according to point-of-care BG levels.
ReferencesMoghissi ES Korytkowski MT DiNardo M et al American Association of ClinicalMoghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract. 2009;15:353-369.Moghissi ES, Korytkowski MT, DiNardo M, Einhorn D, Hellman R, Hirsch IB, Inzucchi SE, Ismail-Beigi F, Kirkman MS, Umpierrez GE; American Association of Clinical Endocrinologists; American Diabetes Association. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control Diabetes Care 2009 Jun;32(6):1119 1131
11
on inpatient glycemic control. Diabetes Care. 2009 Jun;32(6):1119-1131
Pitfalls of Sliding‐Scale InsulinIs reactive, rather than proactive
Often mismatched with changes in patient’s insulin sensitivityinsulin sensitivity
Does not meet physiologic needs
Can lead to ‘insulin stacking’
– When several boluses are given in a short period of time; insulin action overlaps, which may cause h l ihypoglycemia
Hirsch IB. JAMA. 2009;301:213‐214.
SummarySSI traditionally would include regular insulin or a rapid-acting analog provided to treat hyperglycemia after it had already occurred, making it a reactive rather than proactive strategy. Another fundamental problem is that the traditional SSI regimen assumes that all patients have similar insulin sensitivities or no change in insulin sensitivity during different stages of acute illness, which is not true. Insulin stacking is when insulin doses are injected at times too close together, resulting in an overlap of action of the insulin.
R fReferenceHirsch IB. Sliding scale insulin—time to stop sliding. JAMA. 2009;301:213-214.
12
Sliding‐Scale Insulin Is Inferior to Basal Bolus Insulin Treatment forBasal‐Bolus Insulin Treatment for
Inpatient Hyperglycemia (m
g/dL
)
180
200
220
240
* * *† †
††
No differences in the rate of hypoglycemia or hospital LOS.
Days of Therapy
Mea
n BG (
100
120
140
160
180
Admit 1
SSI
Basal‐bolus
2 3 4 5 6 7 8 9 10
†
*P <.01; †P <.05. Error bars denote standard deviation. Insulin glargine + glulisine: 0.4 units/kg for BG 140‐200 mg/dL; 0.5 units/kg for BG 201‐400 mg/dL (1/2 daily dose given as glargine).SSI = regular insulin 4 times daily for BG > 140 mg/dL. LOS, length of stay.Umpierrez GE, et al. Diabetes Care. 2007;30:2181‐2186.
yp g y p
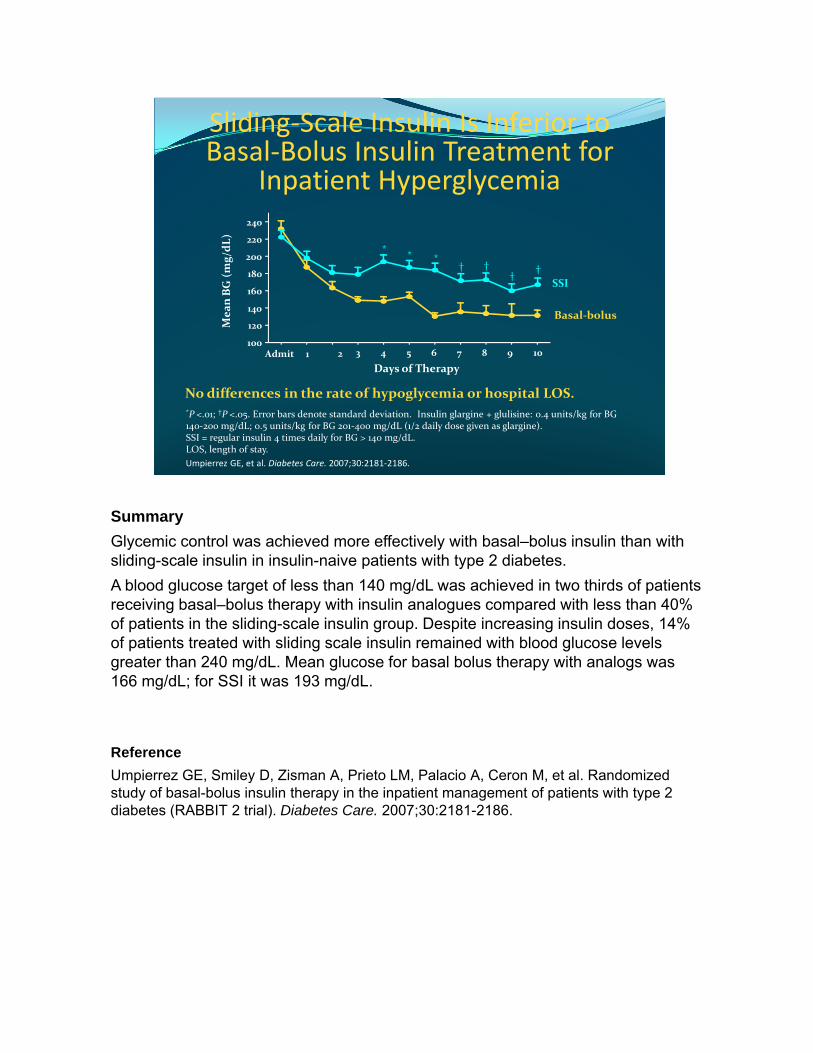
SummaryGlycemic control was achieved more effectively with basal–bolus insulin than with sliding-scale insulin in insulin-naive patients with type 2 diabetes.A blood glucose target of less than 140 mg/dL was achieved in two thirds of patients receiving basal–bolus therapy with insulin analogues compared with less than 40% of patients in the sliding-scale insulin group. Despite increasing insulin doses, 14% of patients treated with sliding scale insulin remained with blood glucose levels greater than 240 mg/dL. Mean glucose for basal bolus therapy with analogs was 166 mg/dL; for SSI it was 193 mg/dL.
ReferenceUmpierrez GE Smiley D Zisman A Prieto LM Palacio A Ceron M et al RandomizedUmpierrez GE, Smiley D, Zisman A, Prieto LM, Palacio A, Ceron M, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care. 2007;30:2181-2186.
Sliding Scale Insulin Is Associated withSliding‐Scale Insulin Is Associated with Higher Glucose Levels and Poorer
Clinical OutcomesOdds Ratio 95% CI230250
Blood glucose (mg/dL)Ratio
CV complications or death
1.86 0.99–3.49
Sepsis or ICU admission 4.98 2.38–10.42
113
0501001502005
Regularlyscheduledinsulin
Sliding‐scaleinsulin
P < .0001
Patients admitted with pneumonia. CI, confidence interval; CV, cardiovascular.
Becker T, et al. Diabetes Res Clin Pract. 2007;78:392‐397.
insulin
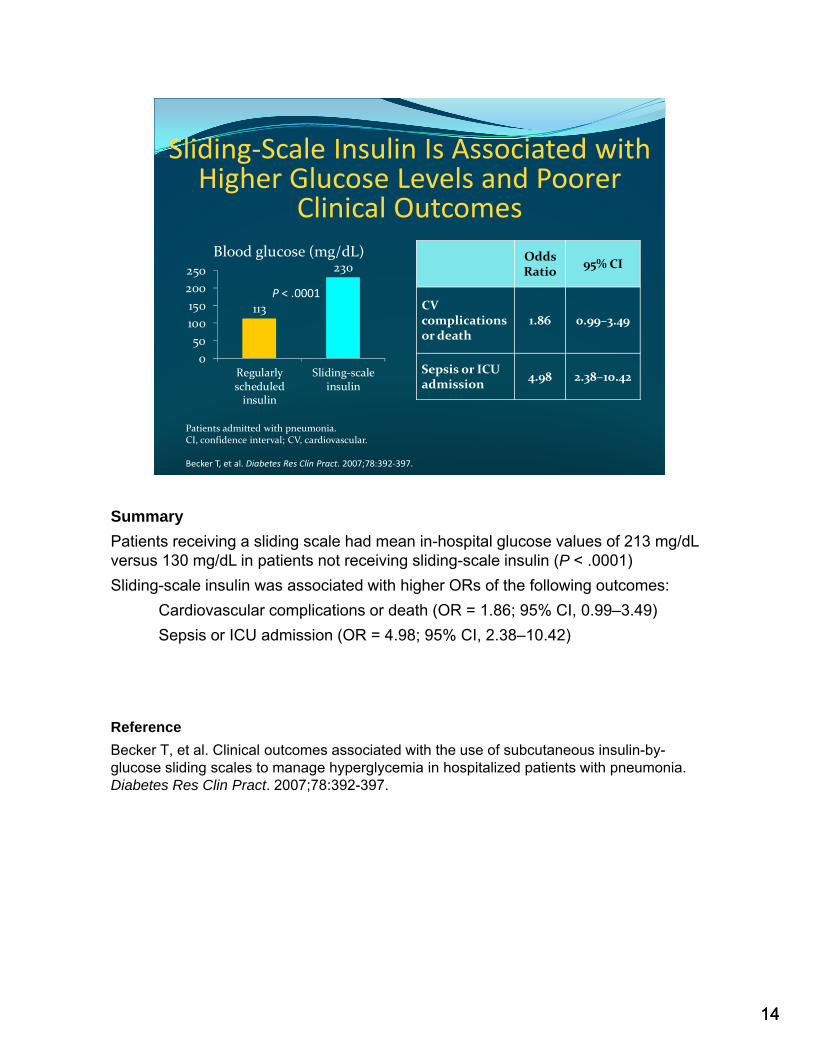
SummaryPatients receiving a sliding scale had mean in-hospital glucose values of 213 mg/dL versus 130 mg/dL in patients not receiving sliding-scale insulin (P < .0001)Sliding-scale insulin was associated with higher ORs of the following outcomes:
Cardiovascular complications or death (OR = 1.86; 95% CI, 0.99–3.49)Sepsis or ICU admission (OR = 4.98; 95% CI, 2.38–10.42)
ReferenceBecker T, et al. Clinical outcomes associated with the use of subcutaneous insulin-by-glucose sliding scales to manage hyperglycemia in hospitalized patients with pneumonia. Diabetes Res Clin Pract. 2007;78:392-397.
1414
Subcutaneous CorrectionSubcutaneous Correction Insulin Algorithms
Does NOT replace scheduled insulin
– Rather it corrects for changing needs
d h l f hBased on the insulin sensitivity of the patient
– Total daily insulin requirement
– Weight/BMI
Utilize rapid‐acting analogs
– Need rapid onset and short duration of action– Need rapid onset and short duration of actionBMI, body mass index.
Korytkowski M. ACP Hospitalist. 2009;12(suppl):15‐23. http://www.acphospitalist.org/archives/2009/12/hyperglycemia.pdf.Expert Opinion, Evidence Level C.
SummaryThe ultimate insulin regimen should address the 3 components of insulin requirement: basal (what is required in the fasting state to maintain normal metabolism), nutritional (what is required for peripheral glucose disposal), and correctional (what is required for unexpected glucose elevations). Distinctions between correction insulin and sliding scale insulin include: 1) The use of rapid-acting insulin analogs with correction insulin. If a patient’s blood glucose is elevated, an agent with a rapid onset to correct the hyperglycemia and short duration to minimize the risk of delayed hypoglycemia is needed 2.) Correction insulin is given in addition to schedule basal and nutritional/prandial insulin not instead of scheduled insulin. 3.) Correction insulin is determined by the insulin sensitivity rather than using the same dose for all.
ReferenceKorytkowski M. Treatment Options for safely achieving glycemic targets in the hospital.ACP Hospitalist. 2009;12(suppl):15-23. http://www.acphospitalist.org/archives/2009/12/hyperglycemia.pdf.
15
Transition From IV to SC InsulinIncorporate estimate of insulin dose from most recent insulin infusion rate
Typically a percentage (usually 75% 80%) of the total – Typically, a percentage (usually 75% – 80%) of the total daily IV infusion dose is proportionately divided into basal and prandial components
Some overlap of IV infusion is needed to avoid recurrence of hyperglycemia until subcutaneous (SC) insulin takes effect
ACE/ADA Task Force on Inpatient Diabetes. Endocr Pract. 2006;12:458‐468.McDonnell M, et al. ACP Hospitalist. 2009;12(suppl):24‐30.http://www.acphospitalist.org/archives/2009/12/hyperglycemia.pdf.
Summary
The daily insulin requirement can be calculated from the insulin infusion rate and the amount of dextrose the patient is receiving.Typically, a percentage (usually 75% – 80%) of the total daily IV infusion dose is proportionately divided into basal and prandial components.Subcutaneous insulin should be administered one to two hours beforeSubcutaneous insulin should be administered one to two hours before discontinuation of the insulin infusion. This allows sufficient time for the subcutaneous insulin to be absorbed and take effect such that there is a reduced risk of significant hyperglycemia during the transition period.
ReferenceMcDonnell M, Donahue M. Transitioning patients along the continuum of care—intravenous to subcutaneous insulin, inpatient to outpatient settings: practical considerations. ACP Hospitalist. 2009;12(suppl):24-30.
16

Subcutaneous Insulin DosingSubcutaneous Insulin Dosing Without Prior Intravenous Insulin
Calculate the estimated total daily dose (TDD) of insulin
Type 2 DM: 0 5 0 7 unit/kg– Type 2 DM: 0.5‐0.7 unit/kg
– Type 1 DM: 0.3‐0.5 unit/kg
– Unknown: 0.3‐0.5 unit/kg
Divide TDD of insulin into 50% basal as long‐acting analog and 50% prandial as rapid‐acting analog i liinsulin
– Divide prandial insulin into 3 equal doses
DeSantis AJ, et al. Endocr Pract. 2006;12:491‐505.
SummaryNote that patients with type 2 diabetes are generally more insulin resistant and will require larger insulin doses.
ReferenceReferenceDeSantis AJ, Schmeltz LR, Schmidt K, O'Shea-Mahler E, Rhee C, Wells A, Brandt S, Peterson S, Molitch ME. Inpatient management of hyperglycemia: the northwestern experience. Endocr Pract. 2006 Sep-Oct;12(5):491-505.
17
Daily Dose AdjustmentDetermine yesterday’s total insulin dose actually administered Review yesterday’s glycemic controly y g yCalculate today’s scheduled insulin dose – Some BG < 90 mg/dL → 80% of yesterday’s total
– BGs 90–179 mg/dL → 100% of yesterday’s total
– Some BG ≥ 180 mg/dL, no BG < 90 mg/dL → 110% of yesterday’s total
Expert Opinion, Evidence Level C.
SummaryBG monitoring will dictate what changes need to be made. The slide shows that if blood glucose levels are in the target range, then no dose adjustment is required; however adjustments should be made for levels above or below target ranges to maintain recommended blood glucose levels.
18
The Balancing Act:
HyperglycemiaHypoglycemia
SummaryThese recent recommended targets per the 2009 AACE/ADA consensus statement reflect a balanced approach for treating hyperglycemia while avoiding hypoglycemia.
19
Inpatient Hypoglycemia Is Associated with Increased Morbidity/Mortalitywith Increased Morbidity/Mortality
in Non‐ICU SettingsInpatient Mortality
nt D
ecea
sed
Adm
ission (%)
8
12
16
Postdischarge Mortality
ent D
ecea
sed
1 Ye
ar (%
)
40
60
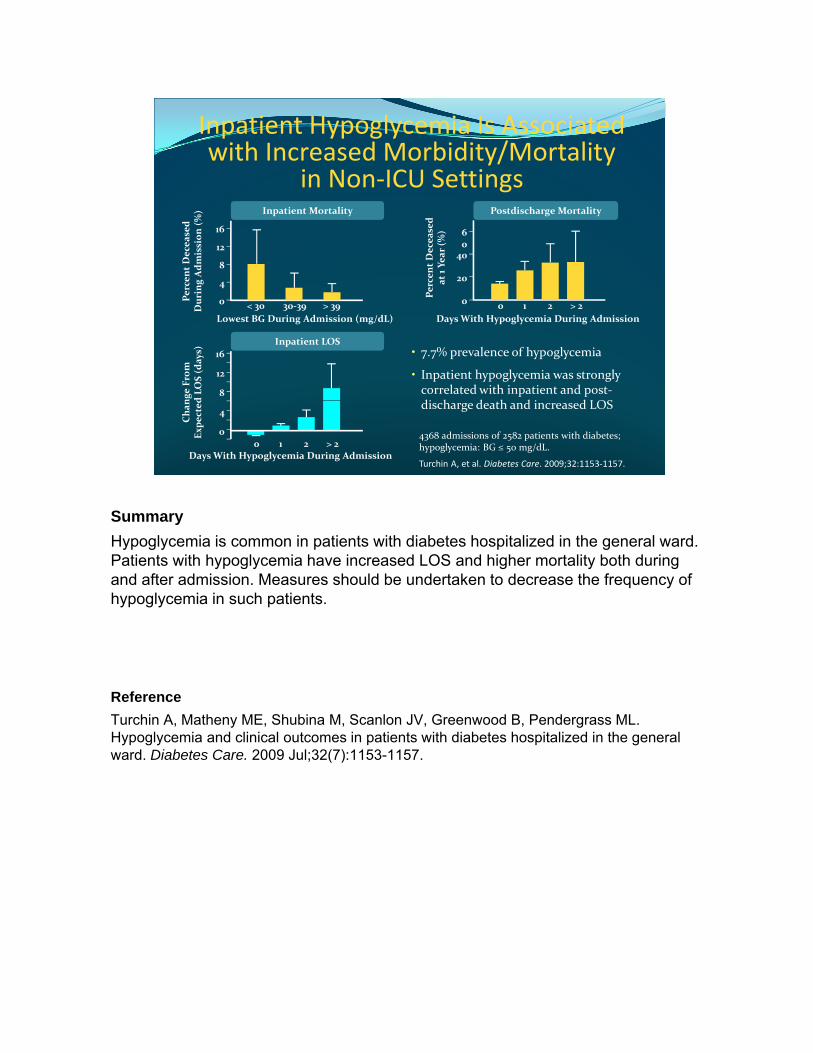
• 7.7% prevalence of hypoglycemia
• Inpatient hypoglycemia was strongly correlated with inpatient and post‐di h d h d i d LOS
Lowest BG During Admission (mg/dL)< 30 30‐39 > 39
Percen
Dur
ing A
0
4
0 1 2 > 2Days With Hypoglycemia During Admission
Perce
at
0
20
Inpatient LOS
nge From
d LO
S (d
ays)
8
12
16
4368 admissions of 2582 patients with diabetes; hypoglycemia: BG ≤ 50 mg/dL.
Turchin A, et al. Diabetes Care. 2009;32:1153‐1157.
discharge death and increased LOS
Days With Hypoglycemia During Admission
Cha
nEx
pected
0
4
0 1 2 > 2
SummaryHypoglycemia is common in patients with diabetes hospitalized in the general ward. Patients with hypoglycemia have increased LOS and higher mortality both during and after admission. Measures should be undertaken to decrease the frequency of hypoglycemia in such patients.
ReferenceTurchin A, Matheny ME, Shubina M, Scanlon JV, Greenwood B, Pendergrass ML. Hypoglycemia and clinical outcomes in patients with diabetes hospitalized in the general ward. Diabetes Care. 2009 Jul;32(7):1153-1157.
Essential Part of Insulin Therapy:Essential Part of Insulin Therapy:Hypoglycemia Protocol
Clear Definition of Hypoglycemia – (BG < 70 mg/dL)
Nursing Order to Treat Without Delayg y– Stop insulin infusion (if patient is on one)– Oral glucose (if patient is able to take oral)– IV dextrose or glucagon (if patient is unable to take oral)– Repeat blood glucose monitoring 15 min after treatment for hypoglycemia
and repeat treatment if blood sugar not up to target– Directions for when and how to restart insulin
Look for the cause of hypoglycemia and determine if other Look for the cause of hypoglycemia and determine if other treatment changes are needed
Moghissi ES, et al. Endocr Pract. 2009;15(4):1‐17.Moghissi ES, et al. Diabetes Care. 2009;32(6):1119‐1131.
SummaryThere should be a clear definition of hypoglycemia. Severe hypoglycemia in hospitalized patients has been defined by many clinicians as a BG of < 40 mg/dL, although this value is lower than the approximate 50–70 mg/dL level at which cognitive impairment begins in normal persons. Hypoglycemia should be defined as any BG value of < 70 mg/dL.
Hypoglycemia should be treated promptlyHypoglycemia should be treated promptly.
Hypoglycemic events can be minimized with improvement in, standardization of, and careful implementation of protocols.
ReferencesM hi i ES K tk ki MT DiN d M t l A i A i ti f Cli i lMoghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract. 2009;15:353-369.
Moghissi ES, Korytkowski MT, DiNardo M, Einhorn D, Hellman R, Hirsch IB, Inzucchi SE, Ismail-Beigi F, Kirkman MS, Umpierrez GE; American Association of Clinical Endocrinologists; American Diabetes Association. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on
21
Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009 Jun;32(6):1119-1131.

Clinical Scenarios Prompting Increased Monitoring and PossibleIncreased Monitoring and Possible
Decreases in Insulin Doses
Patient is switched to NPO status
Reduction in oral intake of food
Discontinuation of enteral feeding or of total parenteral nutrition Discontinuation or reduction in IV dextrose
Timing of premeal insulin if meal disrupted due to medical procedures or patient transport
Reduction in corticosteroid administration
Clement S, et al. Diabetes Care. 2004;27:553‐591.
SummaryThis slide summarizes situations in which adjustment of insulin doses and/or increased monitoring of glucose levels may be warranted.
ReferenceReferenceClement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27(2):553-591.
2222
Common Risk FactorsCommon Risk Factors for Insulin Errors
Lack of dose verification
Mix‐up between insulin and heparin vials
Sliding‐scale ordersHandwritten and no carbon required ordersand heparin vials
Use of the abbreviation “U” in place of “units”
Wrong infusion rates programmed into infusion pump
qDangerous abbreviations and dose designationsVerbal ordersAmbiguous ordersHold orders
infusion pump
Cohen M. Am J Health Syst Pharm. 2010;67(16)(suppl8):S17‐21.
SummaryInsulin is a drug with a low therapeutic index, and it bears a heightened risk of causing significant patient harm when used in error, making it a high-alert medication. The use of sliding-scale insulin can lead to hyperglycemia and hypoglycemia and is confusing and prone to error; it is not recommended. Any ambiguous insulin therapy orders should be clarified in writing prior to administration.
ReferenceCohen MR. Pharmacists' role in ensuring safe and effective hospital use of insulin. Am J Health Syst Pharm 2010 Aug;67(16 Suppl 8):S17-21Health Syst Pharm. 2010 Aug;67(16 Suppl 8):S17 21.
23
Recommendation: StandardizeRecommendation: Standardize Pharmacy Procedures
Prepare all insulin infusions within the pharmacy
Use a standard insulin infusion concentration throughout institutionthroughout institution
Double‐check all insulin preparations against original order prior to dispensing
Verify diagnosis and indication for insulin
Cohen M. Am J Health Syst Pharm. 2010;67(16)(suppl8):S17‐21.
SummaryThe use of standard insulin order sets for scheduled subcutaneous insulin administration and standard concentrations for IV insulin are recommended to ensure the safe use of this medication. Preparation of all insulin infusions should occur within the pharmacy. Pharmacists can contribute to the safe use of insulin in the inpatient setting by minimizing the likelihood of medication errors related to prescribing, transcription, dispensing, administration, storage, and communication.
ReferenceCohen MR. Pharmacists' role in ensuring safe and effective hospital use of insulin. Am J Health Syst Pharm 2010 Aug;67(16 Suppl 8):S17-21Health Syst Pharm. 2010 Aug;67(16 Suppl 8):S17 21.
24
Recommendation: Standardize Operations of Pharmacist andOperations of Pharmacist and
Pharmacy StaffStore insulin in high‐alert bins, away from other drugs
Separate different types of insulin
Alert staff about insulin‐containing IV solutions by brightly labeling bag
Utilize preprinted insulin order sets
Consider use of insulin pen devices for subcutaneous insulin administration
Consider information technology issues
Cohen M. Am J Health Syst Pharm. 2010;67(16)(suppl8):S17‐21.Kelly JL. Am J Health Syst Pharm. 2010;67(16)(suppl8):S9‐16.
SummarySafe insulin storage practices are recommended to reduce the risk for insulin error. Insulin pen delivery devices may be used in hospitals, but safe use depends on ongoing oversight by a multidisciplinary committee, introduction of one device at a time, and initial and regular follow-up education of nurses, including agency nurses and those who work part-time. Computerized prescriber order entry can assist in the appropriate ordering of insulin therapy. For example, it can prompt the prescriber to
d i t b t i li i d k it diffi ltorder an appropriate subcutaneous insulin regimen and make it difficult or impossible for the prescriber to order sliding scale insulin.
ReferencesCohen MR. Pharmacists' role in ensuring safe and effective hospital use of insulin. Am J g pHealth Syst Pharm. 2010 Aug;67(16 Suppl 8):S17-21.
Kelly JL. Ensuring optimal insulin utilization in the hospital setting: role of the pharmacist.Am J Health Syst Pharm. 2010 Aug;67(16 Suppl 8):S9-16.
25

Summary:Management of Hyperglycemia andManagement of Hyperglycemia and Hypoglycemia in the Hospital is a
Patient Safety ConcernAppropriately start insulin therapy, but only in patients >140‐180 mg/dL consistently. Level A (randomized controlled trial/meta‐analysis).In general, target ADA/AACE guideline glucose levels1, but evidence in non‐ICU
i i lli L l B ( h id )settings is not yet compelling. Level B (other evidence).Flag charts in high risk patients such as elderly, renal dialysis, active CV disease, dementia, etc. Level C (consensus/expert opinion).Standardize pharmacy procedures and orders for insulin therapy.Avoid severe hypoglycemia in all patients. (If occurs treat promptly and reassess for causes). Level C (consensus/expert opinion).Implement standardized hypoglycemia treatment protocol. Level B (other evidence).)Properly educate staff about the above. Level C (consensus/expert opinion).Errors occur: evaluate causes and reassess areas of concern/process improvement. Level C (consensus/expert opinion).
SummaryM t f i ti t h l i i ti t tManagement of inpatient hyperglycemia may improve patient outcomes.Insulin protocols and procedures may:
–Decrease confusion regarding medication orders–Increase monitoring for hypoglycemia–Provide specific triggers for intervention–Improve outcomesE h li ith dit ti i t ( J i t C i i )–Enhance compliance with accreditation requirements (eg, Joint Commission)
Staff education may:–Involve staff in curriculum development–Develop internal support–Improve decision-making–Address concerns and overcome barriersReview principles of inpatient insulin management–Review principles of inpatient insulin management–Increase internal protocol adherence
Key Takeaway
Reference• Level A (randomized controlled trial/meta-analysis): High-quality randomized controlled trial (RCT) that considers all important outcomes. High-quality meta-analysis (quantitative systematic review) using comprehensive search strategies. • Level B (other evidence): A well-designed, nonrandomized clinical trial. A nonquantitative systematic review with appropriate search strategies ( ) g q y pp p gand well-substantiated conclusions. Includes lower quality RCTs, clinical cohort studies and case-controlled studies with nonbiased selection of study participants and consistent findings. Other evidence, such as high-quality, historical, uncontrolled studies, or well-designed epidemiological studies with compelling findings, is also included. • Level C (consensus/expert opinion): Consensus viewpoint or expert opinion. Each label should include the letter rating (A, B, C), followed by the specific type of study for that reference. For example, following a level B rating, include one of these descriptors: (1) nonrandomized clinical trial; (2) nonquantitative systematic review; (3) lower quality RCT; (4) clinical cohort study; (5) case-controlled study; (6) historical uncontrolled study; (7) epidemiological study.
26
Thank You
Thank you for participating in this activity.Thank you for participating in this activity.
Click the button below to proceed to the post‐test
27





























