Embed Size (px)
Citation preview

Sa1592Improved Visualization of Small Bowel Lesions by CapsuleEndoscopy Using Flexible Spectral Imaging Color Enhancement(FICE) SystemYasushi Sato*, Masahiro Hirakawa, Hiroyuki Ohnuma, Kohichi Takada,Tsutomu Sato, Koji Miyanishi, Rishu Takimoto, Masayoshi Kobune,Junji KatoSapporo Medical University, School of Medicine, Sapporo, JapanBackground and Aim: Computed virtual chromoendoscopy with flexible spectralimaging color enhancement (FICE) offers improved detection andcharacterization of the gastrointestinal tract lesions and are applied widely inclinical practice at gastroscopy and colonoscopy; however, its clinical usefulnessin capsule endoscopy remain to be firmly established. The aim of this study wasto evaluate the clinical usefulness of the FICE-enhanced capsule endoscopysystem comparing with conventional, white light images. Methods: Threeexperienced endoscopists compared FICE images with correspondingconventional images of 232 lesions obtained from 151 patients who underwentvideo CE at our hospital between January 2009 and November 2011.The lesionswere classified as angioectasia, erosion/ulceration, or tumor, and these imageswere viewed using white light and 3 different sets of FICE images (ie, setting 1:red 595 nm, green 540 nm, blue 535 nm; setting 2: red 420 nm, green 520 nm,blue 530 nm; setting 3: red 595 nm, green 570 nm, blue 415 nm). Endoscopistsrated the visibility of the lesions on FICE images as follows: �2 (markedimprovement), �1 (modest improvement), 0 (remain the same as conventionalimages), �1 (slight decrease), and �2 (marked decrease). Scores for each lesionwere totaled per FICE setting and evaluated. Inter-observer agreement was alsoexamined. The time taken to interpret the capsule videos was also determined.Results: With FICE setting 1, the mean visibility score was 4.7�0.4 forangioectasia images, 2.7�0.4 for erosion/ulceration images, and 0.8�0.2 fortumor images. With setting 2, the mean visibility scores were 4.3�0.4, 3.0�0.9,and �0.4�0.4, respectively. With setting 3, the mean visibility scores were0.8�0.2, 0.3�0.4, and �2.8�0.4, respectively. The inter-observer agreement wasgood (mean weighted kappa � 0.79). Interpretation times were 36�6.9 min,33�5.4 min, 35�2.8, and 36�5.2 with conventional CE, CE-FICE setting 1,setting 2, and setting 3, respectively, and there was no significant differenceamong the 4 groups (P � 0.05). Conclusions: FICE imaging adds valuableinformation to conventional CE imaging and enables better diagnostic utility forsmall-bowel lesions of angioectasia or erosion/ulceration, especially with the useof FICE setting 1 or 2.
Sa1593The Optimal Staining Regimen for Colonic EndocytoscopyCould Be 1.0% Methylene Blue for 3 Minutes: An In Vivo PilotStudyKatsuro Ichimasa*1, Shin-Ei Kudo1, Nobunao Ikehara1,Kunihiko Wakamura1, Yuichi Mori1, Yoshiki Wada1,Makoto Kutsukawa1, Yasuharu Maeda1, Kenichi Takeda1,Akira Yokoyama1, Noriyuki Ogata1, Hirotaka Nishiwaki1,Hideyuki Miyachi1, Fuyuhiko Yamamura1, Kazuo Ohtsuka1,Haruhiro Inoue1, Shigeharu Hamatani21Digestive Disease Center, Showa University Northern YokohamaHospital, Yokohama, Japan; 2Department of Pathology, ShowaUniversity Northern Yokohama Hospital, Yokohama, JapanIntroduction and Objectives: Endocytoscopy (EC) with 450� ultra-magnificationenables the observation of living cells in the gastrointestinal tract. For ECobservation, vital staining provides the information of gland formation andnuclei. Methylene blue (MB), toluidine blue (TB), and crystal violet (CV) havebeen reported to be useful for ex vivo EC staining. The aim of this study was todetermine the optimal in vivo staining regimen for EC. Methods: The subjectswere five patients (mean age 59�11 years, all males) with rectal hyperplasticpolyps. Integrated-type EC scope was used in this study. Each normal rectalmucosa was stained with five dyes (1.0%MB, 0.5%TB, 1.0%TB,0.05%CV�0.5%MB, and 0.05%CV�0.5%TB), and they were assessed afterdifferent exposure times (15 and 30 seconds, and 1, 2, 3, 4, and 5 minutes).Endoscopic images were stored electronically and randomly allocated to fourexaminers who were blinded to the subjects. Each image was scored by addingup the following two parameters: gland formation (clearest, 4; clear, 3; obscure,2; not identified, 1) and nuclei (clearest, 4; clear, 3; obscure, 2; not identified, 1).Added scores were categorized as poor: �3; good: �3 to �8; or excellent: �8.STUDY1: In order to identify the optimal staining regimen, the average of all thescores for each five staining was calculated and compared. STUDY2: In order todefine the reliability of the present method, inter- and intraobserver agreementwith the EC image evaluation (poor, good, or excellent) were calculated amongthe four examiners at intervals of two weeks. Results: STUDY1: The averagescore and the best staining time for each dye were described in the table below.1.0%MB showed the highest score among the five dyes. The best exposure timeto staining was 3-4 minutes for all dyes. STUDY2: Moderate inter- andintraobserver agreement was obtained, with kappa scores of 0.412 (95%
confidence interval, 0.31-0.52) and 0.502 (0.10-0.90), respectively. Conclusion: A3-minute exposure to 1.0% MB was shown to provide the appropriate stainingfor colonic EC with feasible reliability. Reference: S.Kodashima.et al. Ex-vivostudy of high-magnification chromoendscopy in the gastrointestinal tract todetermine the optimal staining conditions for endoscopy. Endoscopy. 2006;38(11): 1115-1121.
1.0%MB0.05%CV �
0.5%MB 1.0%TB 0.5%TB0.05%CV �
0.5%TB
score 6.2 5.5 4.8 4.8 4.195%CI 5.4-7.0 4.8-6.2 4.4-5.3 4.1-5.4 3.5-4.7best exposure timeto staining
3 minutes 3 minutes 4 minutes 4 minutes 3 minutes
Sa1594Endoscopic Screening of Proximal Colon Adenomas:Conventional Imaging Versus Chromoendoscopy With IndigoCarmine DyeSerguei Mouzyka*Endoscopy, LISSOD Hospital, Kiev, UkraineIntroduction: The adenoma-carcinoma sequence developed is accepted inprinciple for colorectal cancer. Small proximal adenomas (above the splenicflexure) are commonly missed during screening colonoscopy. The aim of ourstudy was to assess the detection rate of proximal colon adenomas by comparingchromocolonoscopy with standard white light colonoscopy. Methods: In oneinstitution, 519 asymptomatic patients (F329, M190; mean age 51,5) participatedin study of screening video colonoscopy, performed by a single endoscopist.Informed consents were obtained in all cases. Patients were excluded if thebowel preparation was inadequate, if they had an earlier diagnosed colorectalneoplasia or inflammation, or if they were receiving anticoagulant medication.All endoscopic examinations were performed after obtaining permissions frompatients. Patients received intravenous propofol prior to intubation of thecolonoscope. Complete colonoscopy was performed in 517 (99,6%) cases.Conventional white light colonoscopy was performed in 169 patients. A further350 patients were examined using pancolonic 0,2% solution indigo carmine dye.All lesions identified during screening colonoscopy in both groups wereremoved completely by cold forceps or snare polypectomy. The two groupswere similar with regard to age, gender and rate of complete colonoscopy.Mann-Whitney U Tests were used to determine differences between conventionalcolonoscopy and chromoendoscopy. Results: There was not anythingcomplications after colonoscopy. Totally 151 proximal adenomas (84 patients)were detected during colonoscopy in both groups, with flat lesions 112 (74%)and protuberant lesions 39 (26%). Results of proximal colon lesions detection areshown in Table, the difference between two groups was significant (p value lessthan 0.05). Conclusion: The results of our comparative study show that for thedetection of proximal lesions in asymptomatic patients chromocolonoscopy issuperior to standard colonoscopy. Chromoendoscopy with indigo carmineimproves the detection rate of proximal colon adenomas.
Patients withproximal
adenomasonly
Patients withproximaladenoma
totalProximal
adenoma/patient
Conventionalcolonoscopy
4,7% 9% 0,16
Chromoendoscopy 10,3% 19,7% 0,35P � 0,005 � 0,005 � 0,005
Sa1595A Preliminary Feasibility Study of Using a Novel Narrow BandImaging System With Dual Focus Magnification Capability inBarrett’s Oesophagus: Is the Time Ripe to Abandon RandomBiopsies?Rajvinder Singh*1,2, William Tam1,2, Mahesh Jayanna1,Nazree Nordeen1, Biju George1, Garry Nind1
1Gastroenterology, Division of Medicine, Lyell McEwin Hospital,Adelaide, SA, Australia; 2Department of Medicine, University ofAdelaide, Adelaide, SA, AustraliaIntroduction: The utility of a novel Narrow Band Imaging (NBI) system with dualfocus magnification (DF) in patients with Barrett’s Oesophagus (BE) presentingfor surveillance endoscopy or whom were referred for further assessment ofdysplasia was assessed. Methods: All procedures were performed with aprototype 190 series Exera III NBI system (Olympus Co. Ltd, Japan) with DF
Abstracts
www.giejournal.org Volume 75, No. 4S : 2012 GASTROINTESTINAL ENDOSCOPY AB213
capability. The NBI image has been brightened by 150% and the DF functionenables magnification of upto 70X. Both are push button techniques. Each BEsegment was first evaluated with NBI on the overview mode. Suspicious(darkened/brown) and normal/unsuspicious areas (4 quadrants, every 2cm) werethen recorded. These areas were further assessed with NBI-DF. Histology wasthen predicted in real time based on the mucosal morphology patterns on NBI-DF which was classified as: a) regular pit/ microvasculature (no dysplasia-ND),b) irregular pit/ microvasculature (high grade dysplasia: HGD) and c) regular/absent pits with dilated microvasculature but no change in the calibre of themicrovessels (low grade dysplasia (LGD)/inflammation). Targeted biopsies ofeach suspicious and unsuspicious area were then performed followed by blindedhistopathological analysis. The primary endpoint was the Sensitivity (Sn),Specificity (Sp), Positive Predictive Value (PPV) and Negative Predictive Value(NPV) of NBI-DF in the prediction of HGD. The secondary endpoint was theNPV of NBI-DF in the prediction of areas which did not harbour any dysplasia.Results: 147 separate areas in 21 patients [16 males, mean age (range): 61.8 (27-85) years, mean BE length (range): 4.2 (1-10) cm] were assessed in thispreliminary study. 27 areas appeared suspicious on NBI overview. NBI-DF wasable to correctly discriminate 2 areas as HGD and 22 as LGD/Inflammation. Onearea which was called as HGD only demonstrated inflammation and another 2which were abnormal on NBI overview were correctly diagnosed as harbouringND based on NBI-DF. The other 120 ’normal’ areas on NBI overview whichwere assessed with NBI-DF demonstrated a regular pattern and targeted biopsiesdid not reveal any dysplasia. The Sn, Sp, PPV, NPV in the prediction HGD was100%, 99.3%, 66.7% and 100% respectively. The NPV of NBI-DF in correctlypredicting areas which did not harbour any dysplasia was 100%. Hence, 120biopsies (81.6%) could have been avoided. Conclusion: The novel NBItechnology in the overview mode may be the ideal red flag technique. Furthercharacterisation of abnormal areas with NBI-DF can then be used. Thistechnique could potentially lead to a paradigm shift of how patients with BE aresurveyed where abnormal areas on overview mode are further evaluated withNBI-DF. Irregular areas can be resected, areas which are equivocal, biopsied and’normal/unsuspicious’ areas left behind.
Sa1596Vessels Within Epithelial Circle (VEC) Pattern, As Visualized byMagnifying Endoscopy With Narrow-Band Imaging (ME-NBI), Isa Useful Marker for the Diagnosis of Papillary Adenocarcinoma:A Case-Control StudyTakao Kanemitsu*1, Kenshi Yao2, Shoko Fujiwara1, Takashi Nagahama1,Toshiyuki Matsui1, Hiroshi Tanabe3, Atsuko Ota3, Akinori Iwashita3
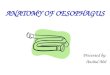
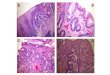
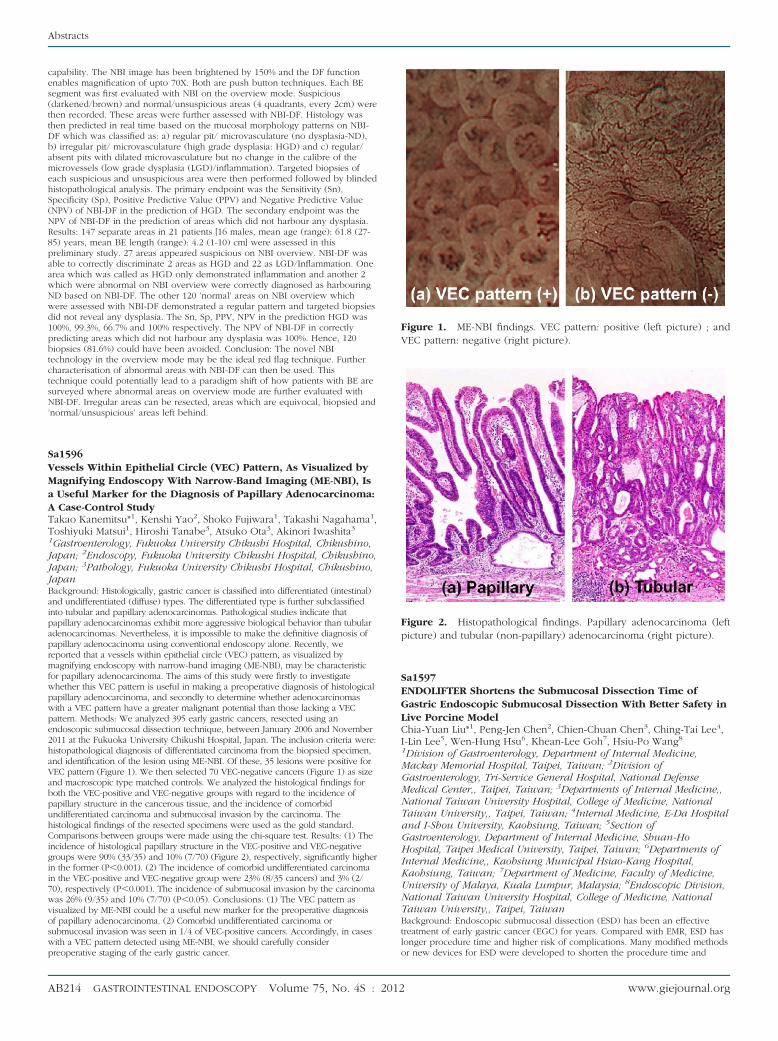
1Gastroenterology, Fukuoka University Chikushi Hospital, Chikushino,Japan; 2Endoscopy, Fukuoka University Chikushi Hospital, Chikushino,Japan; 3Pathology, Fukuoka University Chikushi Hospital, Chikushino,JapanBackground: Histologically, gastric cancer is classified into differentiated (intestinal)and undifferentiated (diffuse) types. The differentiated type is further subclassifiedinto tubular and papillary adenocarcinomas. Pathological studies indicate thatpapillary adenocarcinomas exhibit more aggressive biological behavior than tubularadenocarcinomas. Nevertheless, it is impossible to make the definitive diagnosis ofpapillary adenocacinoma using conventional endoscopy alone. Recently, wereported that a vessels within epithelial circle (VEC) pattern, as visualized bymagnifying endoscopy with narrow-band imaging (ME-NBI), may be characteristicfor papillary adenocarcinoma. The aims of this study were firstly to investigatewhether this VEC pattern is useful in making a preoperative diagnosis of histologicalpapillary adenocarcinoma, and secondly to determine whether adenocarcinomaswith a VEC pattern have a greater malignant potential than those lacking a VECpattern. Methods: We analyzed 395 early gastric cancers, resected using anendoscopic submucosal dissection technique, between January 2006 and November2011 at the Fukuoka University Chikushi Hospital, Japan. The inclusion criteria were:histopathological diagnosis of differentiated carcinoma from the biopsied specimen,and identification of the lesion using ME-NBI. Of these, 35 lesions were positive forVEC pattern (Figure 1). We then selected 70 VEC-negative cancers (Figure 1) as sizeand macroscopic type matched controls. We analyzed the histological findings forboth the VEC-positive and VEC-negative groups with regard to the incidence ofpapillary structure in the cancerous tissue, and the incidence of comorbidundifferentiated carcinoma and submucosal invasion by the carcinoma. Thehistological findings of the resected specimens were used as the gold standard.Comparisons between groups were made using the chi-square test. Results: (1) Theincidence of histological papillary structure in the VEC-positive and VEC-negativegroups were 90% (33/35) and 10% (7/70) (Figure 2), respectively, significantly higherin the former (P�0.001). (2) The incidence of comorbid undifferentiated carcinomain the VEC-positive and VEC-negative group were 23% (8/35 cancers) and 3% (2/70), respectively (P�0.001). The incidence of submucosal invasion by the carcinomawas 26% (9/35) and 10% (7/70) (P�0.05). Conclusions: (1) The VEC pattern asvisualized by ME-NBI could be a useful new marker for the preoperative diagnosisof papillary adenocarcinoma. (2) Comorbid undifferentiated carcinoma orsubmucosal invasion was seen in 1/4 of VEC-positive cancers. Accordingly, in caseswith a VEC pattern detected using ME-NBI, we should carefully considerpreoperative staging of the early gastric cancer.
Sa1597ENDOLIFTER Shortens the Submucosal Dissection Time ofGastric Endoscopic Submucosal Dissection With Better Safety inLive Porcine ModelChia-Yuan Liu*1, Peng-Jen Chen2, Chien-Chuan Chen3, Ching-Tai Lee4,I-Lin Lee5, Wen-Hung Hsu6, Khean-Lee Goh7, Hsiu-Po Wang8
1Division of Gastroenterology, Department of Internal Medicine,Mackay Memorial Hospital, Taipei, Taiwan; 2Division ofGastroenterology, Tri-Service General Hospital, National DefenseMedical Center,, Taipei, Taiwan; 3Departments of Internal Medicine,,National Taiwan University Hospital, College of Medicine, NationalTaiwan University,, Taipei, Taiwan; 4Internal Medicine, E-Da Hospitaland I-Shou University, Kaohsiung, Taiwan; 5Section ofGastroenterology, Department of Internal Medicine, Shuan-HoHospital, Taipei Medical University, Taipei, Taiwan; 6Departments ofInternal Medicine,, Kaohsiung Municipal Hsiao-Kang Hospital,Kaohsiung, Taiwan; 7Department of Medicine, Faculty of Medicine,University of Malaya, Kuala Lumpur, Malaysia; 8Endoscopic Division,National Taiwan University Hospital, College of Medicine, NationalTaiwan University,, Taipei, TaiwanBackground: Endoscopic submucosal dissection (ESD) has been an effectivetreatment of early gastric cancer (EGC) for years. Compared with EMR, ESD haslonger procedure time and higher risk of complications. Many modified methodsor new devices for ESD were developed to shorten the procedure time and
Figure 1. ME-NBI findings. VEC pattern: positive (left picture) ; andVEC pattern: negative (right picture).
Figure 2. Histopathological findings. Papillary adenocarcinoma (leftpicture) and tubular (non-papillary) adenocarcinoma (right picture).
Abstracts
AB214 GASTROINTESTINAL ENDOSCOPY Volume 75, No. 4S : 2012 www.giejournal.org