Embed Size (px)
Citation preview

ANATOMY OF OESOPHAGUS
Presented by: Anshul Mel

Contents
• Introduction• Development of esophagus• Histology of esophagus• Anatomy of esophagus• Applied aspects• Conclusion• References

Introduction

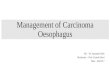
Development of the oesophagus
• At a very early period the stomach is separated from pharynx by a mere constriction from primitive pharynx. This constriction is future esophagus.

• Previous to this elongation the trachea and oesophagus form a single structure.
• This becomes divided into two by the in growth of two lateral septa, which fuse giving rise to trachea in front and oesophagus behind.
• At this stage the oesophagus becomes converted into a solid rod of cells, losing its tubular nature.
• This eventually becomes
canalised to form a tube.

ESOPHAGUS HISTOLOGY

•The esophageal mucosa contains nonkeratinized stratified squamous epithelium. At the esophageal stomach junction the epithelium changes to simple columnar epithelium.

•The submucosa contains mucus secreting glands. As a bolus moves through the esophagus, it compresses these glands, causing them to secrete mucus which aids in the movement of food.

•The muscularis externa is skeletal muscle in its superior third, a mixture of skeletal and smooth muscle in its middle third, and entirely smooth muscle in its inferior third.

•The serosa is entirely connective tissue which blends with surrounding structures along its route.

ESOPHAGUS ANATOMY
•The esophagus is a muscular tube about 25 cm long which connects the pharynx with the stomach. The esophagus takes a straight course through the mediastinum of the thorax and pierces the diaphragm at the esophageal hiatus to enter the abdomen and the stomach.
ESOPHAGUS

Oesophagus
• A muscular tube; 25 cm in length – Collapsed at rest,– Flat in upper 2/3 & rounded in lower 1/3
• Commences at the lower border of the cricoid cartilage.(C6).
• Descends along the front of the spine, through the posterior mediastinum, passes through the Diaphragm, and, entering the abdomen, terminates at the cardiac orifice of the stomach, opposite the eleventh dorsal vertebra.
• In the newborn Upper limit at the level of 4th or 5th CerVertb and it ends at 9th Dorsal

• Length at birth: 8-10 cm, end of Ist Yr: 12cm, 5th Yr.:16cm 15th: 19cm
• Diameter: Varies whether bolus of food/ fluid passing thru or not.– At rest in adults 20 mm but can
stretch up to 30 mm– At birth it is 5mm at 5 yrs it is 15mm

General direction of the oesophagus is vertical • Presents two or three
slight curvatures • At commencement, in the
median line • Inclines to the left side at
the root of the neck • Gradually passes to the
middle line• Again deviates to the left

• The oesophagus also presents an antero-posterior flexure, corresponding to the curvature of the cervical and thoracic portions of the spine.

• In the neck, the oesophagus is in relation, – in front, with the trachea; and, at
the lower part of the neck, where it projects to the left side, with the thyroid gland and thoracic duct;
– behind, it rests upon the vertebral column and Longus colli muscle; on each side, it is in relation with the common carotid artery (especially the left, as it inclines to that side), and part of the lateral lobes of the thyroid gland; the recurrent laryngeal nerves ascend between it and the trachea.

• In the thorax, it is at first situated a little to the left of the median line: it passes across the left side of the transverse part of the aortic arch, descends in the posterior mediastinum, along the right side of the aorta, until near the Diaphragm, where it passes in front and a little to the left of this vessel, previous to entering the abdomen.

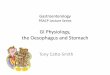
• Oesophagus is the narrowest region of alimentary tract except vermiform appendix. During its course it has three indentations:– At 15 cm from incisor teeth is
crico-pharyngues sphincter (normally closed) (UES)
– At 25 cm aortic arch and left main bronchus
– At 40 cms where it pierces the diaphragm where a physiological sphincter is sited (LES)

Oesophagus divided into functional sphincters
• Upper Oesophageal Sphincter: It is a 2-3 mm zone of elevated pressure between pharynx & oesophagus. It relates to cricopharyngeal muscle
• Lower Oesophageal Sphincter: The LES is located at the junction between the esophagus and stomach, usually localized at or just below the diaphragmatic hiatus. Despite its distinct physiological function, it is not easily distinguished anatomically.

ESOPHAGUS ANATOMY
•The pharynx propels food into the esophagus through the upper esophageal sphincter.
Upper esophagealsphincter

ESOPHAGUS ANATOMY
•The bolus of food is propelled within the esophagus by peristalsis.

ESOPHAGUS ANATOMY

ESOPHAGUS ANATOMY

Unusual! Arterial supply derived from vessels feeding mainly other organs – thyroid,
trachea & stomachCervical Oesophagus: Right & Left superior & inferior thyroid arteries. Thoracic Oesophagus: Upto tracheal bifurcation Right & Left inferior thyroid Artery direct supply from aorta (tracheo-bronchial tree) Abdominal Oesophagus 11 branches off L gastric artery and Branches of splenic artery posteriorly

Venous Relations• Intra-oesophageal
(Intrinsic) Drainage– Longitudinally arranged
in Submucosa • Extra-oesophageal
(Extrinsic) Drainage into locally corresponding veins – Inf. thyroid (into
innominate vein),– Azygos, hemiazygos – L gastric & splenic

• The venous supply is also segmental. • From the dense submucosal plexus the venous
blood drains into the superior vena cava. The veins of the proximal and distal esophagus drain into the azygous system. Collaterals of the left gastric vein, a branch of the portal vein, receive venous drainage from the mid-esophagus.
• The submucosal connections between the portal and systemic venous systems in the distal esophagus form esophageal varices in portal hypertension. These submucosal varices are sources of major hemorrhage in conditions such as cirrhosis.

lymphatics drainage
• In the proximal third of the esophagus, lymphatics drain into the deep cervical lymph nodes,
• In the middle third, drainage is into the superior and posterior mediastinal nodes.
• The distal-third lymphatics follow the left gastric artery to
the gastric and celiac lymph nodes

Nerve Supply
• Parasympathetic – Vagus – motor to muscular coats & secretomotor to
glands
• Sympathetic – From cervical & thoracic sympathetic chain – Contraction of sphincters, wall relaxation, peristalsis

Atresia, and TEF
Congenital anomaly

• Oesophago-tracheal fistula – Commonest type – Newborn has violent
fits of vomiting & coughing on swallowing
• Partial Obstruction of Oesophaugs– Stricture – Atresia– newborn salivates
excessively, becomes cyanotic and vomits
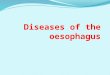
Source: http://www.nature.com/gimo/contents/pt1/fig_tab/gimo6_F10.html
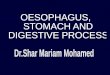
Common Congenital Tracheo-esophageal anomalies

Oesophageal atresia and/or tracheoesophageal (TE)
fistulaAetiology: A= 8% (atresia), C= 87% (atresia +distal TEF),
Incomplete fusion of the tracheo-oesophagel septum.

Atresia & distal TEF: Management
Clinical Picture:1. Choking2. Regurgitation.
Investigations:1. A rubber catheter : not pass along 2. X-ray : increased inhaled air in stomach.3. X-ray with aqueous contrast like di-ionosil blind pouch
and connection if spill-over occurs.

Atresia & distal TEF: Management
Treatment:
Immediate: any delay will ↑ mortality.
end-to-end anastomosis of the oesophagus,

FB Lodgment

Oesophagus: Foreign Bodies
Aetiology: Accidental in children and insane Suicidal in adults.
Pathology: The commonest FB is a coin Bolus of food, Dentures, Fish bones, Safety pinUsually at the inlet of the or anywhere

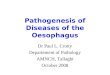
These areas are where most oesophageal
foreign bodies become entrapped.• The most common site of oesophageal
impaction is at the thoracic inlet • Defined as the area between the
clavicles on chest radiograph, this is the site of anatomical change from the skeletal muscle to the smooth muscle of the oesophagus. The cricopharyngeus sling at C6 is also at this level and may "catch" a foreign body.
• About 70% of blunt foreign bodies that lodge in the oesophagus do so at this location.

• Another 15% become lodged at the mid oesophagus, in the region where the aortic arch and carina overlap the oesophagus on chest radiograph.
• The remaining 15% become lodged at the lower oesophageal sphincter (LES) at the gastroesophageal junction.

Oesophagus: Foreign Bodies
Clinical Picture:Dysphagia, Regurgitation, Salivation,
Investigation:X-ray show the coin or bones or metal FB
Complications:Oesophagitis, Ulceration, Perforation, Mediastinits.

Oesophagus: Foreign Bodies
Treatment:1. Endoscopic removal: Hypopharyngoscope
or oesophagoscope2. Sharp FB need special instruments.3. Approach via the neck or thorax: failure
of endoscopic or if the FB migrates outside the oesophagus.

GERD
Reflux

Gastro-Esophageal Reflux Disease "GERD“ : Definition
Frequent transient relaxation of the LES Reflux of gastric contents to the oesophagus Gastric fumes may reach pharynx or larynx.
It is a common disease especially above 40.
LPR: laryngo-pharyngeal reflux
Aetiology: Unknown

Gastro-Esophageal Reflux Disease "GERD“; Clinical Picture
Burning: 1. Burning and sense of FB in throat with
frequent trials of throat clearing. 2. Retro-sternal burning, but this is usually
absent.Hoarseness and chronic irritative cough
and sometimes choking attacks.

Gastro-Esophageal Reflux Disease "GERD“; Investigations
Oesophagoscopy: multiple superficial oesophageal ulceration
Oesophageal motility tracing and 24-hour pH monitoring are
diagnostic.NB: 5-10 mm Hg: Normal resting LES
pressure40-60 mm Hg is characteristic for achalasia

Gastro-Esophageal Reflux Disease "GERD"
Complications
Chronic pharyngitis. "GERP"
Chronic laryngitis. "GERL"
Oesophageal ulcerations
Cancer oesophagus and larynx.

Gastro-Esophageal Reflux Disease "GERD“: TreatmentMedical instructions: Bed position: anti-trendlenberg 15 degree.Avoid: tight belts, and corset. Avoid eating two
hours before bed time. Avoid eating: spicy or fatty foods, or drinking citrus, coffee, alcohol, at night. Quit smoking.
Medical treatment:H2 histamine receptor antagonist: Prokinetic
drugs: Domperidone, Proton pump inhibitors: Surgical: Nissen's fundoplication: failure of medical treatment.

Oesophagoscopy
Procedure

Oesophagoscopy
Flexible: By using fibreoptic oesophagoscope, May be done with or without sedation. For diagnosis and biopsy, Sclerotheray:
varicesRigid:
By using rigid oesophagoscope, Always done under GA

Oesophagoscopy

Rigid Oesophagoscopy: Indications
Diagnostic: For diagnosis and biopsy taking
Therapeutic: 1. FB extraction, 2. Non-malignant stricture dilatation, and 3. Sauttar's tube application in advanced
cancer oesophagus

Oesophageal FB

Rigid Oesophagoscopy: Contraindications
1. Severe Kyphosis
2. Acute corrosive oesophagitis,
3. Aortic aneurysm,
4. Oesophageal Varices.

Rigid Oesophagoscopy: Complications
Injury:
Teeth, lip, tongue, Perforation of the pharynx, and Perforation of the Oesophagus, Injury of the varices leading to bleeding.
Anaesthetic complications

Oesophageal Prforation: endotracheal intubation
Abscess: ↑ prevertebral ST + air

Conclusion

Questions????

References
• Gray’s anatomy 39th edition• Human anatomy - B.D.Chaurasia 3rd edition• Oral and maxillofacial surgery Volume 1- Laskin• McMinn`s colour atlas for Human Anatomy 5th
edition.• Snell`s Clinical anatomy by regions 8th edition• Harcourt, Burket’s oral medicine,11th edition

THANK YOUTHANK YOU