Embed Size (px)
Citation preview

S. Banai, M.D.
PCI and platelet activation
The early response to arterial wall injury is platelet activation and deposition over the injured arterial surface, creating the substrate for thrombosis
Stent implantation appears to be associated with greater platelet activation than balloon angioplasty alone
The magnitude of platelet activation is associated with an increased risk for adverse clinical events after coronary intervention
Kabbani SS: Circulation. 2002;104:181–186
S. Banai, M.D.
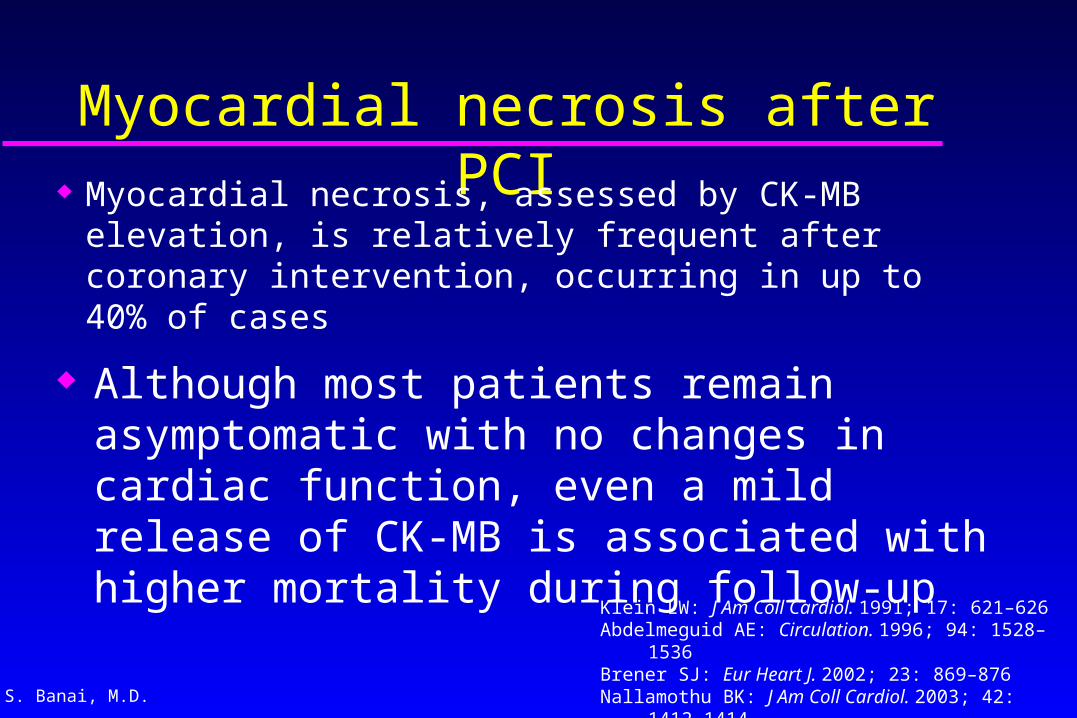
Myocardial necrosis after PCI Myocardial necrosis, assessed by CK-MB
elevation, is relatively frequent after coronary intervention, occurring in up to 40% of cases
Klein LW: J Am Coll Cardiol. 1991; 17: 621–626Abdelmeguid AE: Circulation. 1996; 94: 1528–1536Brener SJ: Eur Heart J. 2002; 23: 869–876Nallamothu BK: J Am Coll Cardiol. 2003; 42: 1412–1414Ioannidis JPA: J Am Coll Cardiol. 2003; 42: 1406–1411
Although most patients remain asymptomatic with no changes in cardiac function, even a mild release of CK-MB is associated with higher mortality during follow-up

S. Banai, M.D.
PCI-related myocardial injury
The most frequent complication after PCI
Can be significantly reduced and outcome improved with appropriate pharmacological treatment before PCI

S. Banai, M.D.
The ARMYDA Study
Randomized, placebo-controlled trial to evaluate the effect of pretreatment with atorvastatin (40mg) started 1 week before elective PCI on the release of markers of cardiac damage (CK-MB, troponin I, and myoglobin) in patients with stable angina
Pasceri V: Circulation 2004;110:674-678
Atorvastatin for Reduction of MYocardial Damage during
Angioplasty

S. Banai, M.D.Pasceri, V. et al. Circulation
2004;110:674-678
Incidence of postprocedural increase of CK-MB and troponin
I >1, 2 to 5, and >5 times above upper normal limit (UNL)
Conclusions: Pretreatment with atorvastatin significantly reduces procedural myocardial injury in
elective PCI
Peak values of CK-MB, troponin I, and myoglobin in statin vs placebo group

S. Banai, M.D.
To evaluate whether aggressive antiplatelet therapy
with clopidogrel in patients undergoing PCI will reduce periprocedural MI and improve outcome
The ARMYDA-2 Study Antiplatelet therapy for Reduction of MYocardial
Damage during Angioplasty
Patti, G. et al. Circulation 2005;111:2099-2106

S. Banai, M.D.
255 pts with stable CAD or non-ST ACS, randomized to 300 or 600 mg of Clopidogrel 4-8 h before PCI
Primary end point: A composite of death, MI or TVR at 30 days
non-ST-elevation MI - 25% complex lesions - 75%DES - 20% IIb/IIIa blockers - 13%
Patti, G. et al. Circulation 2005;111:2099-2106
ARMYDA-2 StudyAntiplatelet therapy for Reduction of Antiplatelet therapy for Reduction of
Myocardial Damage during AngioplastyMyocardial Damage during Angioplasty

S. Banai, M.D.
ARMYDA-2: Number of events
EventClopidogrel 300 mg
Clopidogrel 600 mg
Death 00
Target vessel revascularization
01
MI 15 5

S. Banai, M.D.Patti, G. et al. Circulation 2005;111:2099-2106
ARMYDA-2 STUDY Results: ARMYDA-2 STUDY Results: 30-day occurrence of death, MI, or TVR in patients receiving 600-mg versus the
300-mg loading regimen of clopidogrel
The primary end points occurred in: 4% of pts with 600
mg versus 12% with 300 mg
S. Banai, M.D. Patti, G. et al. Circulation 2005;111:2099-2106
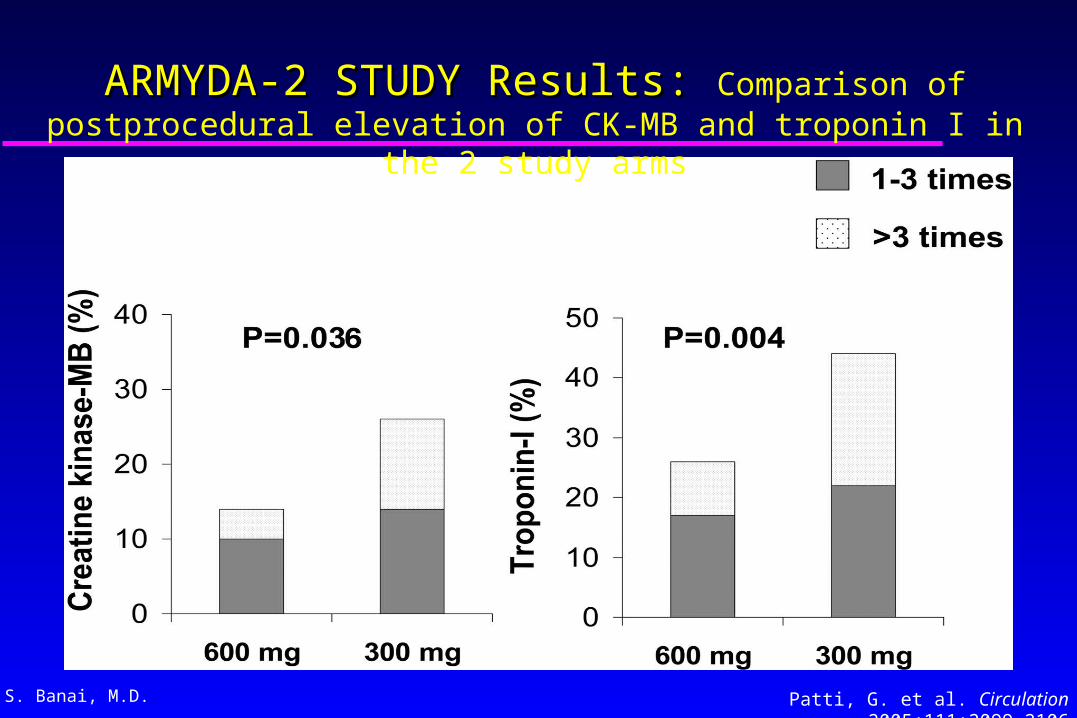
ARMYDA-2 STUDY Results: ARMYDA-2 STUDY Results: Comparison of postprocedural elevation of CK-MB and troponin I in the 2
study arms

S. Banai, M.D. Patti, G. et al. Circulation 2005;111:2099-2106
ARMYDA-2 STUDY Results: ARMYDA-2 STUDY Results: Baseline and peak values of CK-MB, troponin I, and myoglobin

S. Banai, M.D.
Pretreatment with 600-mg loading dose of clopidogrel significantly reduced the risk of periprocedural MI (OR 0.48; 95% CI 0.15 to 0.97; P=0.044)
Patti, G. et al. Circulation 2005;111:2099-2106
ARMYDA-2 STUDY Results: ARMYDA-2 STUDY Results: Multivariable analysis

S. Banai, M.D.
Percentage of patients with any elevation of CKMB/troponin I
Marker Clopidogrel 300 mg(%)
Clopidogrel 600 mg(%)
p
CKMB26140.036
Troponin I
44260.004

S. Banai, M.D.
Bleeding events
EventClopidogrel 300 mg
Clopidogrel 600 mg
Major bleed (Hgb>5g/dL)
00
Minor bleed (Hgb<5g/dL)
1) 0.8%(1) 0.8%(

S. Banai, M.D.
The ARMYDA-2 trial Conclusions:
Pretreatment with a 600-mg loading dose of clopidogrel given 6 hours before the procedure is safe and, as compared with the 300-mg dose, reduces periprocedural MI and improves short-term prognosis in patients undergoing PCI
The low risk of this pharmacological regimen may support its routine use in patients before planned coronary angioplasty and may influence practice patterns with regard to antiplatelet
therapy before PCI

S. Banai, M.D.
CLOPIDOGREL
ASA COX
ADP
ADP
C
GPllb/llla(Fibrinogen receptor)
Collagen thrombinTXA
2Activation
TXA 2
COX (cyclo-oxygenase)ADP (adenosine diphosphate)TXA2 (thromboxane A2)
Jarvis B, Simpson K. Drugs 2000; 60: 347–77
The active metabolite exerts its antiplatelet effect by noncompetitive inhibition of the platelet ADP receptor
subtype P2Y12
Clopidogrel: An inactive prodrug requires in vivo conversion in the liver
by the cytochrome P450 (CYP) 3A4 enzyme system

S. Banai, M.D.
A prodrug that needs to be metabolized to an active compound that targets the platelet Gi-coupled adenosine diphosphate
(ADP) P2Y12 receptor Clopidogrel is oxidized in a cytochrome P450 (CYP)
monooxygenase-dependent way to 2-oxo-clopidogrel, an intermediate metabolite that is further hydrolyzed to the active thiol metabolite of clopidogrel
The active metabolite irreversibly binds to the P2Y12 receptor
The major circulating metabolite of clopidogrel is a carboxylic acid derivate that completely lacks antiaggregatory activity
The thienopyridine clopidogrel

S. Banai, M.D.
Absorption (oral): rapid, not affected by food or
antacids
Metabolism: rapid and extensive hepatic metabolism
Half-life: 8 hours (but has an irreversible effect on
platelets, with a lifespan of approximately 7–10 days)
Excretion: 50% in urine and 46% in feces, after 5 days
Pharmacology of Clopidogrel
Jarvis B, Simpson K. Drugs 2000; 60: 347–77

S. Banai, M.D.
Clopidogrel Dosing1977: The 75-mg once-daily dose was approved by the FDA after the CAPRIE trial showed superior reduction of adverse cardiovascular events with clopidogrel versus aspirin
The 75-mg once-daily dose had been used in CAPRIE
because it produced inhibition of platelet aggregation equivalent to that produced by ticlopidine 250 mg administered twice daily
2002: FDA approval for the 300-mg loading dose in patients with ACS after the CURE trial demonstrated a reduction of adverse cardiovascular events with dual antiplatelet therapy versus aspirin

S. Banai, M.D.
Loading Dose Without a loading dose, clopidogrel 75 mg daily induces inhibition of ADP-induced platelet aggregation as early as 2 hours after the first dose but requires 3 to 7 days to achieve maximal inhibition of platelet aggregation
The 3- to 7-day delay can be shortened to 6 hours with a loading dose of 300 mgWith 600 mg loading (as compared with the 300-mg
dose):the maximal platelet inhibition is achieved at 2
hoursthe level of inhibition of platelet aggregation is
increasedthe number of low responders decreased
Bates ER: Circulation 2005;111:2557-2559
Hochholzer W: Circulation 2005;111:2560-2564

S. Banai, M.D.
The benefit of a higher loading doseThe advantage of using the higher loading dose is the maximal drug effect during the periprocedural period when pretreatment has not been given, a common occurrence with ad hoc PCI
The clinical benefit is measured by lower biomarker-defined periprocedural MI rates, as has been seen with periprocedural platelet inhibition with GP IIb/IIIa inhibitor agents, and with the 600 mg Clopidogrel pre-treatment in the ARMYDA-2 trial

S. Banai, M.D.
Should patients who are on chronic clopidogrel therapy receive the 600 mg pretreatment
regimen?
Many patients presenting for PCI are already treated with clopidogrel. Should these patients receive the 600-mg pretreatment regimen?
The answer is yes!
Additional, significant inhibition of platelet aggregation is achieved when a 600-mg dose is administered to patients already receiving clopidogrel 75 mg daily

S. Banai, M.D.
Further platelet inhibition can be achieved with 600-mg Re-loading in patients with chronic clopidogrel
therapy
Adnan Kastrati Circulation. 2004;110:1916-1919
In both groups, 600 mg clopidogrel loading significantly inhibited ADP-induced expression of GP IIb/IIIa and P-selectin receptors
In the chronic therapy group, loading with 600 mg clopidogrel
yielded further inhibition of platelet aggregation in addition to that achieved by the maintenance dose of 75 mg/d, from 52±14% to 33±12% (P<0.001)

S. Banai, M.D.
Abciximab offers no additional benefit in the setting of Clopidogrel pretreatment
Kastrati A: N Engl J Med 2004;350:232-238

S. Banai, M.D.
Study design and objectives
2159 patients with CAD who underwent a PCI:
All patients were pretreated with a 600-mg dose of clopidogrel at least two hours before the procedure
N=1079 - abciximab N=1080 - placebo
Primary end point: Composite of death, MI, and urgent TVR within 30 days
Kastrati A: N Engl J Med 2004;350:232-238

S. Banai, M.D.
Results: 4% event rate in both patient groups
Kastrati A: N Engl J Med 2004;350:232-238

S. Banai, M.D.
conclusion
In patients at low and intermediate risk who undergo elective PCI after pretreatmentwith a 600-mg loading dose of clopidogrel at leasttwo hours before the procedure, the additional use of abciximab is associated with no clinically measurable benefit within the first 30 days
Kastrati A: N Engl J Med 2004;350:232-238

S. Banai, M.D.
Randomized Clinical Trial of Abciximab in Diabetic Patients Undergoing Elective PCI After Treatment With a High Loading
Dose of Clopidogrel
Julinda Mehilli, Circulation. 2004;110:3627-3635
Abciximab offers no additional benefit in the setting of Clopidogrel pretreatment in Diabetics
Study: 701 diabetic patients with CAD who underwent elective PCI after pretreatment with a 600-mg dose of clopidogrel >2 hours before the procedure
351 patients - abciximab
350 patients - placebo
Primary end point: composite of death and MI at 1 year

S. Banai, M.D.
There is no significant impact of abciximab on the risk of death and MI in diabetic patients undergoing PCI after pretreatment with a 600-mg loading dose of clopidogrel at least 2 hours before the procedure
Conclusions:
Mehilli J, Circulation 2004;110:3627-3635

S. Banai, M.D.
How High Should We Go?Absorption, Metabolization, and Antiplatelet Effects
of 300, 600, and 900-mg Loading Doses of Clopidogrel:
Results of the ISAR-CHOICE (Intracoronary Stenting and Antithrombotic Regimen: Choose Between 3 High Oral Doses
for Immediate Clopidogrel Effect) Trial
Nicolas von Beckerath: Circulation 2005;112: 2946 - 2950
Primary end point:
Maximal ADP-induced (5 µmol/L) platelet aggregation 4 hours after administration of
clopidogrel

S. Banai, M.D.
Antiplatelet Effects of 300-, 600-, and 900-mg Loading Doses of Clopidogrel
Sixty patients with suspected or documented CAD admitted for coronary angiography were included
They were allocated to clopidogrel loading doses of 300, 600, or 900 mg in a double-blinded, randomized manner
Plasma concentrations of the active thiol metabolite, unchanged clopidogrel, and the
inactive carboxyl metabolite of clopidogrel were determined before and serially after drug administration Nicolas von Beckerath: Circulation 2005;112: 2946 - 2950

S. Banai, M.D.von Beckerath, N. et al. Circulation 2005;112:2946-2950
Plasma concentrations
Loading with 600 mg resulted in higher plasma concentrations of active metabolite, clopidogrel, and carboxyl metabolite compared with loading with 300 mg (P 0.03)
With 900 mg, no further increase in plasma concentrations of active
metabolite and clopidogrel (P 0.38) was achieved
active metabolite
clopidogrel
carboxyl metabolite
300 mg (blue)600 mg (red)
900 mg (cyan)

S. Banai, M.D.
Maximal ADP-induced platelet aggregation 4 hours after administration of a 300-, 600-, and 900- mg
loading dose
von Beckerath, N. et al. Circulation 2005;112:2946-2950
An increase of the clopidogrel loading dose from 600 to 900 mg does not result in further suppression of platelet aggregation caused by a failed increase in plasma concentration of the drug
This suggests that intestinal absorption becomes the bottleneck when single doses exceeding 600 mg are administered

S. Banai, M.D.
Should we split the high dose?
Administering 900 mg Clopidogrel in 2 separate doses may allow more complete absorption and, consequently, additional platelet inhibition compared with 600 mgHowever, the practicability of such an approach as a pretreatment before PCI is limited
Nicolas von Beckerath Circulation. 2005;112:2946-2950

S. Banai, M.D.
What can we reasonable conclude about antiplatelet therapy and PCI?
1. augmenting aspirin with additional antiplatelet therapy reduces myonecrosis after PCI
2. according to the information currently available, if clopidogrel is selected, the dose should be 600 mg and the drug should be administered at least 2 hours before PCI
3. for the types of patients evaluated thus far, intravenous GP IIb/IIIa inhibitors appear unnecessary when clopidogrel has been administered
4. if circumstances restrict clopidogrel pretreatment, intravenous GP IIb/IIIa is a reasonable alternative
S. Banai, M.D.
Thank You