-
7/25/2019 Catheter Ablation
1/16
Catheter Ablation
Overview
Background
Radiofrequency (RF) catheter ablation (RFCA) has revolutionized
treatmentfor tachyarrhythmias and has become first-line therapy for
some tachycardias
Althou!h developed in the "#$%s and widely applied in the
"##%s& formalized!uidelines for its use in clinical practice
were not developed until some yearslater'"& & & *+
Catheters were first used for intracardiac recordin! and
stimulation in the late"#,%s& but sur!ical treatment for
refractory tachyarrhythmias was themainstay of nonpharmacolo!ic
therapy until it was superseded by catheterablation he initial
ener!y source used was direct current (.C) from astandard e/ternal
defibrillator A shoc0 was delivered between the distalcatheter
electrode and a cutaneous surface electrode1 however& this
hi!h-volta!e dischar!e was difficult to control and could cause
e/tensive tissuedama!e
RF ener!y& a low-volta!e& hi!h-frequency form of
electrical ener!y familiar tophysicians from its use in sur!ery
(e!& electrocautery)& quic0ly supplanted .Cablation he
relative safety of RF ener!y has contributed to the
widespreadadoption of catheter ablation as a therapeutic
modality
RF ener!y produces small& homo!eneous& necrotic lesions
by heatin! tissue2esion size is influenced& in part& by the
len!th of the distal ablation electrodeand the type of catheter
(standard vs saline-cooled) 3ith typical powersettin!s and !ood
catheter contact pressure with cardiac tissue& lesions
areminimally about 4-5 mm in diameter and -4 mm in depth
Future directions
A curative procedure for atrial fibrillation (AF) is a ma6or
!oal in clinical cardiacelectrophysiolo!y 7uccess has been achieved
in patients with paro/ysmal
lone AF by eliminatin! conduction from the pulmonary veins to
the left atrium&as many of these episodes are tri!!ered by
rapid electrical activity arisin!from tissue near the pulmonary
vein ostia or from muscle sleeves surroundin!the pro/imal veins
Other forms of AF may require some de!ree of substrateablation
(e!& linear transmural lesions in the left atrium)
-
7/25/2019 Catheter Ablation
2/16
echniques are evolvin! to address the challen!e of a
catheter-based cure forall forms of AF hree-dimensional
electroanatomic maps& overlaid onma!netic resonance ima!in!
(8R9) or computed tomo!raphy (C) scans ofthe left atrium& can
facilitate navi!ation of the catheter and mappin! of
thearrhythmo!enic substrate 9ntracardiac echocardio!raphy may also
help inavoidin! collateral dama!e to the pulmonary veins or
esopha!us& ensurin!adequate endocardial contact& and
monitorin! for complications (e!&pericardial effusion and
thrombus development)
Alternative ener!y sources are bein! investi!ated in the
ablation of AF (e!&balloon-based technolo!ies usin!
cryoablation&'4+ ultrasound& and laser) 9naddition&
robotic catheter navi!ation is now available to deliver RFCA
Research is also focused on developin! better methods and tools
for catheterablation of ventricular tachycardia(:)& and even
ventricular fibrillation (:F)&
in patients with structural heart disease ;picardial
electrophysiolo!y viasub/iphoid pericardial puncture is a
relatively new frontier1 sometachyarrhythmia substrates (especially
: in nonischemic cardiomyopathy)cannot be reached from the
endocardium
Indications
here are three class 9 indications for catheter ablation he
first issymptomatic supraventricular tachycardia (7:) due to
atrioventricular (A:)nodal reentrant tachycardia (A:s
preference
he second indication is AF with lifestyle-impairin! symptoms and
inefficacy orintolerance of at least one antiarrhythmic
a!ent',& + ?oth left atrial ablation forrestoration of sinus
rhythm and A: 6unction ablation for rate control are class
9indications& dependin! on the circumstance
he third indication is symptomatic :'5+ Catheter ablation is
first-line therapy
in idiopathic : if that is the patient>s preference 9n
structural heart disease&catheter ablation is !enerally
performed for dru! inefficacy or intolerance or asad6unctive
therapy in patients with an implantable
cardioverter-defibrillator(9C.) who are e/periencin! frequent 9C.
dischar!es
@ncommon indications for catheter ablation include the
followin!
http://emedicine.medscape.com/article/159075-overviewhttp://emedicine.medscape.com/article/162245-overviewhttp://emedicine.medscape.com/article/162245-overviewhttp://emedicine.medscape.com/article/159075-overviewhttp://emedicine.medscape.com/article/162245-overviewhttp://emedicine.medscape.com/article/162245-overview
-
7/25/2019 Catheter Ablation
3/16
7ymptomatic dru!-refractory (inefficacy or intolerance)
idiopathic sinus
tachycardia
2ifestyle-impairin! ectopic beats
7ymptomatic 6unctional ectopic tachycardia
RFCA has been applied to most clinical tachycardias& even to
polymorphic :and :F in preliminary studies 7uccess rates are
hi!hest in patients withcommon forms of 7:& namely A:
-
7/25/2019 Catheter Ablation
4/16
tri!!erin! event monitor 7ome patients require the use of
previouslyineffective antiarrhythmic dru!s to maintain success
Supraventricular tachyarrhythmias
he common forms of 7: (e!& A:
-
7/25/2019 Catheter Ablation
5/16
For patients with structural heart disease and stable :& the
potential benefitof catheter ablation before implantation of an 9C.
was demonstrated in the:entricular achycardia Ablation in Coronary
Beart .isease (:ACB) study'#+ his prospective& randomized&
controlled international trial in "%* patientsfound that time to
recurrence of : or :F was lon!er in the ablation !roup(median&
"$, months) than in the control !roup (4# months) At
years&estimates for survival free from : or :F were *5 in the
ablation !roup and# in the control !roup
-
7/25/2019 Catheter Ablation
6/16
=eriprocedural Care
Preprocedural planning
he preprocedural evaluation always includes a thorou!h history
and physicale/amination& as well as a review of
electrocardio!rams (;CDs1 "-lead& ifavailable) obtained durin!
the tachycardia and in sinus rhythm At a minimum&preprocedural
blood wor0 typically includes a complete blood count and
anassessment of renal function and electrolyte levels
An echocardio!ram is frequently obtained to e/clude structural
heart diseaseOther tests that are indicated in specific situations
include e/ercise testin!
with or without cardiac ima!in! (especially for
e/ercise-inducedtachyarrhythmias)& and cardiac
catheterization
he patient should fast overni!ht before the procedure Cardiac
medicationswith electrophysiolo!ic effects (e!& beta
bloc0ers& calcium channel bloc0ers&di!o/in& and class 9
and 999 antiarrhythmic dru!s) are often tapered ordiscontinued
before the procedure 3arfarin may or may not be held prior tothe
procedure For e/ample& performin! left atrial ablation for
atrial fibrillationon warfarin may reduce thromboembolic
complications'"%+
Patient preparation
Catheter ablation typically requires that the patient be under
conscioussedation with intravenous tranquilizers and narcotics
Deneral anesthesiaisused in children and selected adults
Monitoring and follow-up
After !eneric supraventricular tachcardia (7:) ablation or
idiopathicventricular tachycardia (:) ablation& some physicians
empirically treatpatients with * wee0s of aspirin therapy with the
aim of potentially reducin!the ris0 of thromboembolic sequelae
Anticoa!ulation with warfarin or one of the newer a!ents is
typically employedfor at least " month after ablation for patients
presentin! in persistent atrialflutter and for months after left
atrial ablation for patients with AF
http://emedicine.medscape.com/article/1271543-overviewhttp://emedicine.medscape.com/article/1271543-overview
-
7/25/2019 Catheter Ablation
7/16
;chocardio!raphy is not routinely performed unless a
complication (e!&pericardial effusion) may have occurred
=ostprocedural electrophysiolo!ictestin! is not routinely performed
unless recurrent tachyarrhythmias aresuspected
echniqueApproach considerations
ypically& two to five electrode catheters are percutaneously
inserted via thefemoral or internal 6u!ular veins and are
positioned within the left heart& theri!ht heart& or both
8ultiple catheters are needed to induce and map
varioustachyarrhythmias before radiofrequency (RF) catheter
ablation (RFCA)
Cannulation of the coronary sinus is helpful to map left-sided
accessorypathways or evaluate other left-sided tachyarrhythmia
substrates
For left-heart catheterization& one of the followin! two
approaches may beta0en
ransseptal catheterization via the interatrial septum
Retro!rade catheterization across the aortic valve
he latter is typically reserved for ventricular tachycardia (:)
ablations oraccessory pathway ablations
Anticoa!ulation with intravenous (9:) heparin is used to reduce
the ris0 ofperiprocedural thromboembolism
Atrial fibrillation
RFCA of the atrioventricular (A:) 6unction is the simplest
catheter ablationprocedure performed in patients with atrial
fibrillation (AF) A: nodalmodification is less effective and is not
frequently performed e/cept in anattempt to avoid pacema0er
implantation ?oth of these approaches are usedto achieve !ood rate
control in AF& but unli0e ablation techniques in
atrialtissue& neither one restores normal sinus rhythm 9n
addition& A: 6unction
ablation mandates permanent pacema0er implantation
Catheter ablation of atrial tissue to cure AF continues to
evolve heprocedure is technically demandin! and is both more ris0y
and lesssuccessful than A: 6unction ablation
-
7/25/2019 Catheter Ablation
8/16
e/citement that this common tachyarrhythmia may be amenable to a
curativecatheter procedure
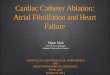
For catheter ablation of atrial tissue for AF& the most
commonly usedtechnique is a wide circumferential ablation around
the pulmonary veins (see
the ima!e below) he !oal is to electrically isolate rapid
electrical activityarisin! from inside the veins& or ad6acent
to the pulmonary vein ostia& from therest of the left
atrium
;lectroanatomic map of posterior
left atrium& illustratin! pulmonary veins ri!ht superior
pulmonary vein (R7=:)& ri!htinferior pulmonary vein (R9=:)&
left superior pulmonary vein (27=:)& and left inferiorpulmonary
vein (29=:) Red circles represent actual discrete radiofrequency
(RF)applications& predominantly delivered in circumferential
pattern around the pulmonaryveins his ablation strate!y can isolate
pulmonary vein foci that initiate atrial fibrillation(AF) or alter
substrate of left atrium to inhibit fibrillatory activity due to
reentry 9ma!ecourtesy of American Colle!e of Cardiolo!y
Foundation
-
7/25/2019 Catheter Ablation
9/16
curin! AF in all comers& re!ardless of chronicity or whether
structural heartdisease is present he best success rates with left
atrial catheter ablation arein patients with paro/ysmal AF and
hearts that are not too structurallyabnormal
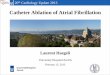
Atrial flutter
Atrial flutteris most commonly due to a lar!e reentrant circuit
in the ri!htatrium& involvin! an isthmus of tissue between the
tricuspid valve annulus andthe inferior vena cava 8ost
commonly& reentry proceeds countercloc0wise upthe atrial septum
and down the lateral wall of the ri!ht atrium&
inscribin!inverted (ie& sawtooth) flutter waves in the inferior
leads and upri!ht = wavesin :"(see the ima!es below)
7chema of common variety of atrial flutterReentry circuit is
confined to ri!ht atrium and circulates as
countercloc0wisemacroreentrant circuit proceedin! superiorly over
atrial septum and inferiorly over lateralatrial wall 3ave front
circulates throu!h narrow isthmus of tissue between tricuspid
valve annulus and inferior vena cava 2inear ablation across this
isthmus (cavotricuspidisthmus) cures this common form of atrial
flutter
http://emedicine.medscape.com/article/151210-overviewhttp://emedicine.medscape.com/article/151210-overview
-
7/25/2019 Catheter Ablation
10/16
ypical countercloc0wise atrialflutter (most common form of
atrial flutter in patients who have not had prior ablation)Cardinal
features are perfectly re!ular atrial rhythm with inverted = waves
inferiorly thathave positive overshoot& upri!ht = waves in
:"& and inverted = waves in :,
Cloc0wise reentry usin! this same circuit can also occur&
!ivin! upri!ht =waves inferiorly and inverted = waves in :" 2inear
ablation of thecavotricuspid isthmus cures these common forms of
atrial flutter (7ee the
video below)
hree-dimensional electroanatomic map of cavotricuspid isthmus
flutter Colorspro!ress from red to purple and represent relative
conduction time in ri!ht atrium (earlyto late) Ablation line (red
dots) has been created from tricuspid annulus to inferior venacava
his interrupts flutter circuit
-
7/25/2019 Catheter Ablation
11/16
.ia!rammatic schema of typicaltype of atrioventricular (A:)
nodal reentrant tachycardia (A:
-
7/25/2019 Catheter Ablation
12/16
and retro!rade = wave is hi!hly specific for atrioventricular
(A:) nodal reentranttachycardia (A:
-
7/25/2019 Catheter Ablation
13/16
7chema of orthodromicreciprocatin! tachycardia (OR)
Atrioventricular (A:) node serves as antero!rade limb&whereas
accessory pathway (A: connection) serves as retro!rade limb
7upraventricular tachycardia(7:) in patient with orthodromic
reciprocatin! tachycardia (OR) due to concealedpathway
-
7/25/2019 Catheter Ablation
14/16
olff-Parkinson-hite syndrome
3hereas OR uses an accessory pathway in the retro!rade
direction& 3=3syndrome by definition indicates an accessory
pathway capable ofantero!rade conduction and is manifest by
pree/citation (delta waves) on the
sinus rhythm ;CD
AF in 3=3 syndrome may result in life-threatenin!ly fast
antero!radeconduction over the accessory pathway& manifested by
an irre!ular wide-comple/ (pree/cited) tachycardia that can
sometimes de!enerate toventricular fibrillation (:F) AF in 3=3
syndrome may be tri!!ered by OR
Ablation of the accessory pathway cures 3=3 syndrome&
eliminatin! OR& aswell as AF& in the ma6ority of
patients
!nifocal atrial tachycardia
@nifocal atrial tachycardia& which can arise from either
atrium or thenoncoronary cusp of the aorta& is somewhat more
challen!in! to ablate thanthe more common forms of !eneric
supraventricular tachycardia (7:) Forthose tachycardias ori!inatin!
from the left atrium& transseptal catheterizationvia a patent
foramen ovale or transseptal puncture is usually required
"entricular tachycardia
9diopathic : most commonly arises from the ri!ht ventricular
outflow tractand less commonly ori!inates in the inferoseptal left
ventricle about two thirds
of the way toward the ape/ from the base of the left ventricle
hese forms of: are amenable to catheter ablation& thou!h
success rates are somewhatlower than those for the common forms of
7:
: in structural heart disease is also amenable to ablation 7ome
form ofthree-dimensional electroanatomic mappin! is employed for
these comple/ablations to identify the scar that contributes to the
anatomic substrate forreentry 9ntracardiac echocardio!raphy durin!
the procedure andpreprocedural ima!in! with ma!netic resonance
ima!in! (8R9) or computedtomo!raphy (C) are also used in some
instances Anatomy from
such ima!in! can be inte!rated with the electroanatomic map
ifnecessary 7ome : substrates& especially : in
nonischemiccardiomyopathy& are not reachable from the
endocardium 9n these instances&percutaneous epicardial mappin!
and ablation are necessary
Complications
-
7/25/2019 Catheter Ablation
15/16
he radiation ris0 from catheter ablation is low& but it may
e/ceed the ris0 fromcommon radiolo!ic procedures he avera!e ris0 of
!enetic defects has beencomputed at " case per million births he
avera!e ris0 of fatal mali!nanciesran!es from % to deaths per "%%%
cases for every ,% minutes offluoroscopy'"+ 8any ablation
procedures require less than ,% minutes offluoroscopy
8a6or complications occur in appro/imately of patients who
under!oablation procedures& includin! thromboembolism in fewer
than " (hi!her insome AF ablation series) and death in %"-% of all
procedures heincidence of cardiac complications varies accordin! to
the site and type ofablation Cardiac complications include the
followin!
Bi!h-!rade A: bloc0
Cardiac tamponade (hi!hest in AF ablation& up to ,)
Coronary artery spasmIthrombosis
=ericarditis
:alve trauma
:ascular complications& which occur in appro/imately -* of
procedures&include the followin!
Retroperitoneal bleedin!
Bematoma
:ascular in6ury
ransient ischemic attac0Istro0e
Bypotension
hromboembolism or air embolism
=ulmonary complications include the followin!
=ulmonary hypertension& with or without hemoptysis
(secondary to
pulmonary vein stenosis)
=neumothora/
8iscellaneous complications include the followin!
2eft atrialGesopha!eal fistula
Acute pyloric spasmI!astric hypomotility
=hrenic nerve paralysis
Radiation- or electricity-induced s0in dama!e
9nfection at access site
9nappropriate sinus tachycardia
-
7/25/2019 Catheter Ablation
16/16
=roarrhythmia