Embed Size (px)
Citation preview
Prepared by the Health and Safety Laboratory, the Institute of Occupational Medicine and Imperial College London for the Health and Safety Executive 2012
Health and Safety Executive
The burden of occupational cancer in Great BritainMelanoma
RR860Research Report
Charlotte YoungHealth and Safety LaboratoryHarpur Hill, BuxtonDerbyshire SK17 9JN
John Cherrie, Martie Van TongerenInstitute of Occupational MedicineResearch Avenue NorthRiccartonEdinburgh EH14 4AP
Léa Fortunato, Sally Hutchings, Lesley Rushton Department of Epidemiology and BiostatisticsImperial College LondonNorfolk PlaceLondon W2 1PG
The aim of this project was to produce an updated estimate of the current burden of cancer for Great Britain resulting from occupational exposure to carcinogenic agents or exposure circumstances. The primary measure of the burden of cancer was the attributable fraction (AF) being the proportion of cases that would not have occurred in the absence of exposure; and the AF was used to estimate the number of attributable deaths and registrations. The study involved obtaining data on the risk of the cancer due to the exposure of interest, taking into account confounding factors and overlapping exposures, as well as the proportion of the target population exposed over the relevant exposure period. Only carcinogenic agents, or exposure circumstances, classified by the International Agency for Research on Cancer (IARC) as definite (Group 1) or probable (Group 2A) human carcinogens were considered. Here, we present estimates for melanoma that have been derived using incidence data for calendar year 2004, and mortality data for calendar year 2005.
The estimated total (male and female) AF for melanoma of the eye related to overall occupational exposure is 1.56% (95%Confidence Interval (CI)= 0.30-3.62), which equates to 1 (95%CI= 0-3) death and 6 (95%CI= 1-15) registrations, all of which were attributable to occupational exposure to ultraviolet radiation from welding.
This report and the work it describes were funded by the Health and Safety Executive (HSE). Its contents, including any opinions and/or conclusions expressed, are those of the authors alone and do not necessarily reflect HSE policy.
The burden of occupational cancer in Great BritainMelanoma
HSE Books
Health and Safety Executive

© Crown copyright 2012
First published 2012
You may reuse this information (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view the licence visit www.nationalarchives.gov.uk/doc/open-government-licence/, write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email [email protected].
Some images and illustrations may not be owned by the Crown so cannot be reproduced without permission of the copyright owner. Enquiries should be sent to [email protected].
ACKNOWLEDGEMENTS
Funding was obtained from the Health and Safety Executive (HSE). Andrew Darnton from the HSE was responsible for the work on mesothelioma. The contributions to the project and advice received from many other HSE and Health and Safety Laboratory staff is gratefully acknowledged. Two workshops were held during the project bringing together experts from the UK and around the world. We would like to thank all those who participated and have continued to give advice and comment on the project. We would also like to thank Helen Pedersen and Gareth Evans for their help in editing and formatting the reports.
ii
EXECUTIVE SUMMARY The aim of this project was to produce an updated estimate of the current burden of cancer for Great Britain resulting from occupational exposure to carcinogenic agents or exposure circumstances. The primary measure of the burden of cancer used in this project was the attributable fraction i.e. the proportion of cases that would not have occurred in the absence of exposure; this was then used to estimate the attributable numbers. This involved obtaining data on the risk of the disease due to the exposure of interest, taking into account confounding factors and overlapping exposures, and the proportion of the target population exposed over the period in which relevant exposure occurred. Estimation was carried out for carcinogenic agents or exposure circumstances classified by the International Agency for Research on Cancer (IARC) as definite (Group 1) or probable (Group 2A) human carcinogens. Here, we present estimates for melanoma that have been derived using incidence data for calendar year 2004, and mortality data for calendar year 2005. Solar radiation has been classified by the IARC as a definite human carcinogen for melanoma skin cancer. However, the risk for malignant melanoma of the skin caused by occupational exposure to solar radiation is uncertain due to difficulties in classifying solar exposure as occupational or recreational. Both positive and negative associations have been found giving no overall increase in risk. The attributable fraction and numbers of deaths and registrations due to occupationally related solar radiation has therefore not been estimated for melanoma of the skin. Ultraviolet radiation from artificial sources has been classified by IARC as a probable human carcinogen for melanoma, particularly of the eye. Evidence of high intensity exposure in welding is particularly strong. Due to assumptions made about cancer latency and working age range, only cancers in ages 25+ in 2005/2004 could be attributable to occupation. For Great Britain in 2005, there were 39 total deaths in men aged 25+ and 44 in women aged 25+ from melanoma of the eye; in 2004 there were 198 total registrations for melanoma of the eye in men aged 25+ and 185 in women aged 25+. The estimated total (male and female) attributable fraction for melanoma of the eye is 1.56% (95%Confidence Interval (CI)=0.30-3.62), which equates to 1 (95%CI=0-3) death and 6 (95%CI=1-15) registrations, all of which were attributable to occupational exposure to ultraviolet radiation from welding.
iii
iv
CONTENTS
1 INCIDENCE AND TRENDS 1 1.1 Melanoma of the Skin 1 1.2 Melanoma of the Eye 3
2 OVERVIEW OF AETIOLOGY 5 2.1 Exposures for Melanoma of the Skin 9
2.1.1 Solar Radiation 9 2.1.2 Ultraviolet Radiation from Artificial Sources 14
2.2 Exposures for Melanoma of the eye 16 2.2.1 Solar Radiation 16 2.2.2 Ultraviolet Radiation from Artificial Sources 18
2.3 Occupation as an Exposure 19 3 ATTRIBUTABLE FRACTION ESTIMATION 30
3.1 General Considerations 30 3.2 Solar Radiation 32 3.3 Ultraviolet Radiation from artificial sources 35
4 OVERALL ATTRIBUTABLE FRACTION 38 4.1 Exposure Map 38 4.2 Summary of Results 38 4.3 Exposures by Industry/Job 40
5 BIBLIOGRAPHY 41 6 STATISTICAL APPENDIX 45
v

vi
1 INCIDENCE AND TRENDS
The cells that become cancerous in melanoma are called ‘melanocytes’ (Cancer Research UK 2008). They are mainly found between the dermis and epidermis, but are also found in many other places, including the hair and the lining of internal organs, such as the eye. The melanocytes produce a dark-coloured pigment called melanin, which is responsible for the colouring of the skin. The pigment helps to protect the body from the ultraviolet (UV) light of the sun, which can cause burns. 1.1 MELANOMA OF THE SKIN
Melanoma of the skin, also called cutaneous melanoma or malignant melanoma (ICD-10 C43; ICD-9 172) accounted for 160,000 new cases, and 41,000 deaths, worldwide in 2002 (Parkin et al. 2005). There were slightly more cases in women than men, however, there were more deaths in men. This type of tumour is particularly common in white populations living in sunny climates. High incidence rates are found in Australia, New Zealand, North America and Northern Europe. Rapid increases in incidence and mortality are being observed in both males and females in many countries, including countries where rates are typically low, such as Japan. Survival from melanoma is relatively high in developed areas (81% in Europe). In contrast, survival is lower in developing countries (typically around 40%); this is partly due to late diagnosis, and the majority of tumours being acral melanoma (located on the soles of the feet), which have a poorer prognosis than other melanoma types. There are four main types of cutaneous melanoma: superficial spreading melanoma, nodular melanoma, lentigo maligna melanoma and acral lentiginous melanoma (Cancer Research UK 2008). Superficial spreading melanoma is the most common, accounting for about 70% of cases. This type of melanoma tends to grow outwards initially, then downward into the deeper layers of the skin. Approximately 25% of UK melanomas are nodular; these develop quickly and grow down into the skin, usually on infrequently exposed parts of the body. Lentigo maligna melanoma appears in areas of skin that get a lot of sun exposure and is largely restricted to the head and neck, especially the face. Acral lentiginous melanoma, by definition, is found on the skin of the palms of the hands and more commonly on the soles of the feet. Melanoma of the skin arises in different anatomic sites in men and women. The trunk (back, abdomen and chest) is the most common in men, accounting for 38%. Melanoma is most commonly found on the legs (including the hips and thighs) in women, accounting for 42%. Sun exposure is the main cause of cutaneous melanoma, or more specifically solar UV radiation (Gruber and, Armstrong 2006). Benign acquired nevi (those that develop after 6 months of age) and atypical nevi are also well-established risk factors for melanoma of the skin. Nevi are most likely to be associated with superficial spreading melanoma rather than other types. Congenital nevi (those present immediately at birth) are categorised by size, which corresponds to the malignant potential, thus cutaneous melanoma arising in small congenital nevi is rare. In the UK and Ireland in the 1990s, melanoma of the skin accounted for 1 in 50 diagnosed cases of cancer and 1 in 100 cancer deaths (Gavin and Walsh 2005). Overall, the age-standardised incidence rates were 7.7 and 9.7 per 100,000 in males and females, respectively. Although there was a higher incidence rate for females, the mortality rates were similar. The age-standardised mortality rate was 2.5 per 100,000 in males and 2.0 per 100,000 in females. Currently cutaneous melanoma is the seventh most common cancer in the UK; sixth in women and tenth in men. In Great Britain, the numbers diagnosed have been steadily increasing from approximately 5,500 cases each year to in excess of 8,500 (Table 1). Nearly 2,000 people die from
1
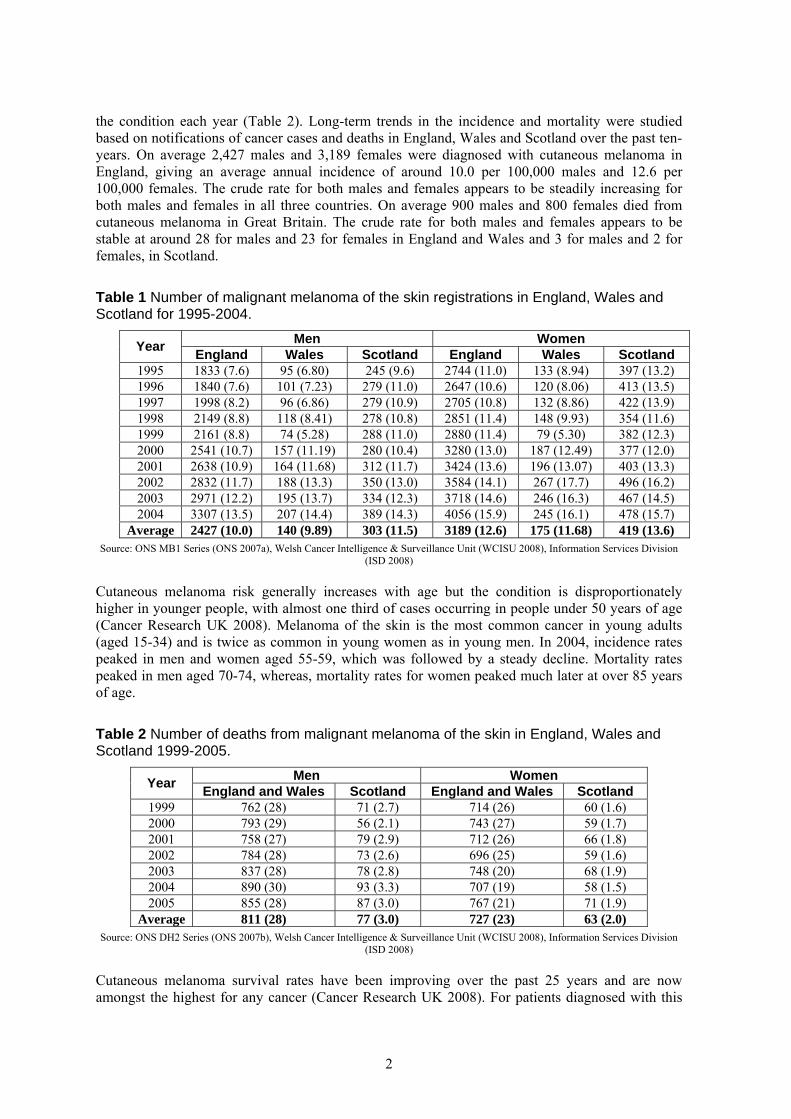
the condition each year (Table 2). Long-term trends in the incidence and mortality were studied based on notifications of cancer cases and deaths in England, Wales and Scotland over the past ten-years. On average 2,427 males and 3,189 females were diagnosed with cutaneous melanoma in England, giving an average annual incidence of around 10.0 per 100,000 males and 12.6 per 100,000 females. The crude rate for both males and females appears to be steadily increasing for both males and females in all three countries. On average 900 males and 800 females died from cutaneous melanoma in Great Britain. The crude rate for both males and females appears to be stable at around 28 for males and 23 for females in England and Wales and 3 for males and 2 for females, in Scotland.
Table 1 Number of malignant melanoma of the skin registrations in England, Wales and Scotland for 1995-2004.
Men Women Year England Wales Scotland England Wales Scotland 1995 1833 (7.6) 95 (6.80) 245 (9.6) 2744 (11.0) 133 (8.94) 397 (13.2) 1996 1840 (7.6) 101 (7.23) 279 (11.0) 2647 (10.6) 120 (8.06) 413 (13.5) 1997 1998 (8.2) 96 (6.86) 279 (10.9) 2705 (10.8) 132 (8.86) 422 (13.9) 1998 2149 (8.8) 118 (8.41) 278 (10.8) 2851 (11.4) 148 (9.93) 354 (11.6) 1999 2161 (8.8) 74 (5.28) 288 (11.0) 2880 (11.4) 79 (5.30) 382 (12.3) 2000 2541 (10.7) 157 (11.19) 280 (10.4) 3280 (13.0) 187 (12.49) 377 (12.0) 2001 2638 (10.9) 164 (11.68) 312 (11.7) 3424 (13.6) 196 (13.07) 403 (13.3) 2002 2832 (11.7) 188 (13.3) 350 (13.0) 3584 (14.1) 267 (17.7) 496 (16.2) 2003 2971 (12.2) 195 (13.7) 334 (12.3) 3718 (14.6) 246 (16.3) 467 (14.5) 2004 3307 (13.5) 207 (14.4) 389 (14.3) 4056 (15.9) 245 (16.1) 478 (15.7)
Average 2427 (10.0) 140 (9.89) 303 (11.5) 3189 (12.6) 175 (11.68) 419 (13.6) Source: ONS MB1 Series (ONS 2007a), Welsh Cancer Intelligence & Surveillance Unit (WCISU 2008), Information Services Division
(ISD 2008)
Cutaneous melanoma risk generally increases with age but the condition is disproportionately higher in younger people, with almost one third of cases occurring in people under 50 years of age (Cancer Research UK 2008). Melanoma of the skin is the most common cancer in young adults (aged 15-34) and is twice as common in young women as in young men. In 2004, incidence rates peaked in men and women aged 55-59, which was followed by a steady decline. Mortality rates peaked in men aged 70-74, whereas, mortality rates for women peaked much later at over 85 years of age.
Table 2 Number of deaths from malignant melanoma of the skin in England, Wales and Scotland 1999-2005.
Men Women Year England and Wales Scotland England and Wales Scotland 1999 762 (28) 71 (2.7) 714 (26) 60 (1.6) 2000 793 (29) 56 (2.1) 743 (27) 59 (1.7) 2001 758 (27) 79 (2.9) 712 (26) 66 (1.8) 2002 784 (28) 73 (2.6) 696 (25) 59 (1.6) 2003 837 (28) 78 (2.8) 748 (20) 68 (1.9) 2004 890 (30) 93 (3.3) 707 (19) 58 (1.5) 2005 855 (28) 87 (3.0) 767 (21) 71 (1.9)
Average 811 (28) 77 (3.0) 727 (23) 63 (2.0) Source: ONS DH2 Series (ONS 2007b), Welsh Cancer Intelligence & Surveillance Unit (WCISU 2008), Information Services Division
(ISD 2008)
Cutaneous melanoma survival rates have been improving over the past 25 years and are now amongst the highest for any cancer (Cancer Research UK 2008). For patients diagnosed with this
2
cancer in 2000-2001 in England and Wales, the population-based five-year relative survival rate is very high for both males (78%) and females (91%), with rates being consistently higher in females. Generally, the five-year relative survival rate varies between 20% and 90% depending on the stage of disease, thickness of the tumour and age at diagnosis. Patients with advanced stage cutaneous melanoma have a significantly lower five-year survival rate than patients diagnosed in the early stages (Stage 1: 90%, Stage 2: 80%, Stage 3: 40-50% and Stage 4: 20-30%). Survival rates decline slightly both with tumour thickness and age. The five-year survival rate decreases from around 90% for the thinnest tumours (<1.5mm) to around 50% for the thickest (>3.5mm). Patients diagnosed who are under 40 years of age have a five-year survival rate of about 76% for men and 90% for women but for patients aged over 80 years this decreases to 44% in men and 61% in women. In 2004, cancer mortality to incidence ratios for melanoma of the skin (C43) were 0.25 for men and 0.16 for women (ONS 2006). 1.2 MELANOMA OF THE EYE
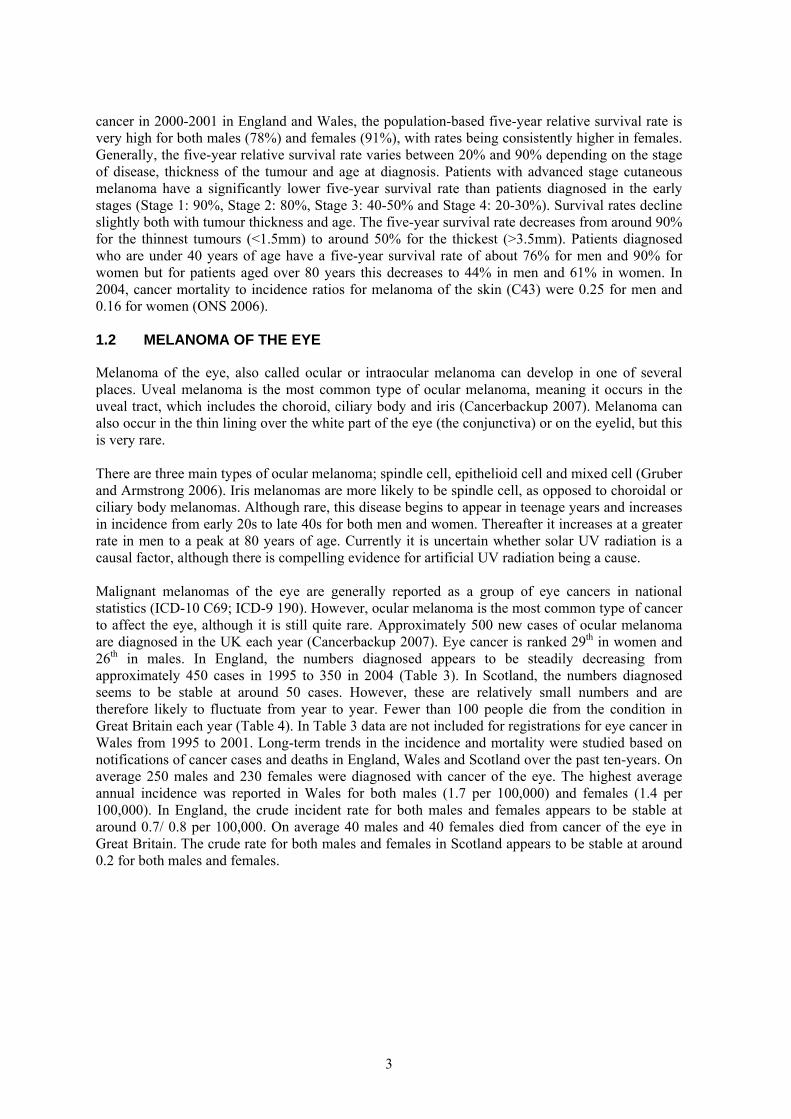
Melanoma of the eye, also called ocular or intraocular melanoma can develop in one of several places. Uveal melanoma is the most common type of ocular melanoma, meaning it occurs in the uveal tract, which includes the choroid, ciliary body and iris (Cancerbackup 2007). Melanoma can also occur in the thin lining over the white part of the eye (the conjunctiva) or on the eyelid, but this is very rare. There are three main types of ocular melanoma; spindle cell, epithelioid cell and mixed cell (Gruber and Armstrong 2006). Iris melanomas are more likely to be spindle cell, as opposed to choroidal or ciliary body melanomas. Although rare, this disease begins to appear in teenage years and increases in incidence from early 20s to late 40s for both men and women. Thereafter it increases at a greater rate in men to a peak at 80 years of age. Currently it is uncertain whether solar UV radiation is a causal factor, although there is compelling evidence for artificial UV radiation being a cause. Malignant melanomas of the eye are generally reported as a group of eye cancers in national statistics (ICD-10 C69; ICD-9 190). However, ocular melanoma is the most common type of cancer to affect the eye, although it is still quite rare. Approximately 500 new cases of ocular melanoma are diagnosed in the UK each year (Cancerbackup 2007). Eye cancer is ranked 29th in women and 26th in males. In England, the numbers diagnosed appears to be steadily decreasing from approximately 450 cases in 1995 to 350 in 2004 (Table 3). In Scotland, the numbers diagnosed seems to be stable at around 50 cases. However, these are relatively small numbers and are therefore likely to fluctuate from year to year. Fewer than 100 people die from the condition in Great Britain each year (Table 4). In Table 3 data are not included for registrations for eye cancer in Wales from 1995 to 2001. Long-term trends in the incidence and mortality were studied based on notifications of cancer cases and deaths in England, Wales and Scotland over the past ten-years. On average 250 males and 230 females were diagnosed with cancer of the eye. The highest average annual incidence was reported in Wales for both males (1.7 per 100,000) and females (1.4 per 100,000). In England, the crude incident rate for both males and females appears to be stable at around 0.7/ 0.8 per 100,000. On average 40 males and 40 females died from cancer of the eye in Great Britain. The crude rate for both males and females in Scotland appears to be stable at around 0.2 for both males and females.
3
Table 3 Number of cancer of the eye registrations in England, Wales and Scotland for 1995-2004.
Men Women Year England Wales Scotland England Wales Scotland 1995 217 (0.9) 24 (1.0) 221 (0.9) 29 (0.9) 1996 169 (0.7) 33 (1.4) 175 (0.7) 30 (0.9) 1997 205 (0.8) 35 (1.4) 173 (0.7) 33 (1.0) 1998 169 (0.7) 29 (1.1) 144 (0.6) 36 (1.2) 1999 154 (0.6) 22 (0.9) 146 (0.6) 26 (0.9) 2000 192 (0.8) 28 (1.1) 181 (0.7) 39 (1.3) 2001 186 (0.8) 24 (0.9) 158 (0.6) 29 (0.9) 2002 189 (0.8) 19 (1.3) 27 (1.0) 151 (0.6) 21 (1.4) 23 (0.8) 2003 203 (0.8) 29 (2.0) 23 (0.9) 166 (0.7) 22 (1.5) 26 (0.8) 2004 169 (0.7) 26 (1.8) 23 (0.9) 179 (0.7) 19 (1.3) 24 (0.6)
Average 195 (0.8) 25 (1.7) 27 (1.1) 179 (0.7) 21 (1.4) 30 (0.9) Source: ONS MB1 Series (ONS 2007a), Welsh Cancer Intelligence & Surveillance Unit (WCISU 2008), Information Services Division
(ISD 2008)
Table 4 Number of deaths from cancer of the eye in England and Wales 1999-2005. Men Women Year England and Wales Scotland England and Wales Scotland
1999 39 3 (0.1) 45 5 (0.2) 2000 43 9 (0.3) 30 7 (0.2) 2001 34 2 (0.1) 34 9 (0.3) 2002 42 5 (0.2) 33 4 (0.1) 2003 24 3 (0.1) 45 3 (0.1) 2004 33 4 (0.1) 37 8 (0.2) 2005 35 4 (0.2) 38 6 (0.1)
Average 36 4 (0.2) 37 6 (0.2) Source: ONS DH2 Series (ONS 2007b), Welsh Cancer Intelligence & Surveillance Unit (WCISU 2008), Information Services Division
(ISD 2008)
The five-year relative survival rate for ocular melanoma generally varies between 50% and 90% depending on how advanced the cancer is and which parts of the eye are affected by the condition (Cancer Research UK 2008). For an early stage small eye melanoma (<2.5mm thick and <5mm wide), the five-year rate is approximately 90%. For medium stage eye melanomas (<10mm thick and <16mm wide), this rate reduces to approximately 75% and for people with large eye melanomas (>10mm thick or 16mm wide), which have spread beyond the eyeball; survival reduces further to around 50%. In 2004, cancer mortality to incidence ratios for malignant neoplasm of eye and adnexa (C69) were 0.34 for men and 0.68 for women (ONS 2006).
4
2 OVERVIEW OF AETIOLOGY
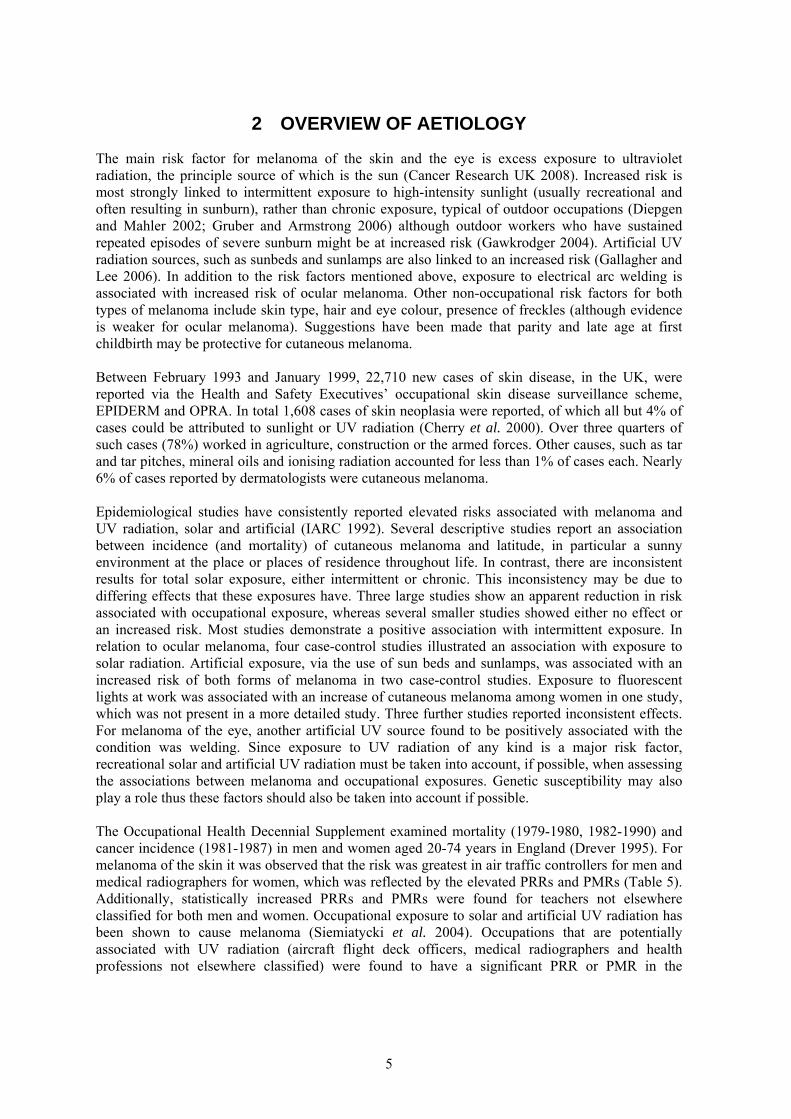
The main risk factor for melanoma of the skin and the eye is excess exposure to ultraviolet radiation, the principle source of which is the sun (Cancer Research UK 2008). Increased risk is most strongly linked to intermittent exposure to high-intensity sunlight (usually recreational and often resulting in sunburn), rather than chronic exposure, typical of outdoor occupations (Diepgen and Mahler 2002; Gruber and Armstrong 2006) although outdoor workers who have sustained repeated episodes of severe sunburn might be at increased risk (Gawkrodger 2004). Artificial UV radiation sources, such as sunbeds and sunlamps are also linked to an increased risk (Gallagher and Lee 2006). In addition to the risk factors mentioned above, exposure to electrical arc welding is associated with increased risk of ocular melanoma. Other non-occupational risk factors for both types of melanoma include skin type, hair and eye colour, presence of freckles (although evidence is weaker for ocular melanoma). Suggestions have been made that parity and late age at first childbirth may be protective for cutaneous melanoma. Between February 1993 and January 1999, 22,710 new cases of skin disease, in the UK, were reported via the Health and Safety Executives’ occupational skin disease surveillance scheme, EPIDERM and OPRA. In total 1,608 cases of skin neoplasia were reported, of which all but 4% of cases could be attributed to sunlight or UV radiation (Cherry et al. 2000). Over three quarters of such cases (78%) worked in agriculture, construction or the armed forces. Other causes, such as tar and tar pitches, mineral oils and ionising radiation accounted for less than 1% of cases each. Nearly 6% of cases reported by dermatologists were cutaneous melanoma. Epidemiological studies have consistently reported elevated risks associated with melanoma and UV radiation, solar and artificial (IARC 1992). Several descriptive studies report an association between incidence (and mortality) of cutaneous melanoma and latitude, in particular a sunny environment at the place or places of residence throughout life. In contrast, there are inconsistent results for total solar exposure, either intermittent or chronic. This inconsistency may be due to differing effects that these exposures have. Three large studies show an apparent reduction in risk associated with occupational exposure, whereas several smaller studies showed either no effect or an increased risk. Most studies demonstrate a positive association with intermittent exposure. In relation to ocular melanoma, four case-control studies illustrated an association with exposure to solar radiation. Artificial exposure, via the use of sun beds and sunlamps, was associated with an increased risk of both forms of melanoma in two case-control studies. Exposure to fluorescent lights at work was associated with an increase of cutaneous melanoma among women in one study, which was not present in a more detailed study. Three further studies reported inconsistent effects. For melanoma of the eye, another artificial UV source found to be positively associated with the condition was welding. Since exposure to UV radiation of any kind is a major risk factor, recreational solar and artificial UV radiation must be taken into account, if possible, when assessing the associations between melanoma and occupational exposures. Genetic susceptibility may also play a role thus these factors should also be taken into account if possible. The Occupational Health Decennial Supplement examined mortality (1979-1980, 1982-1990) and cancer incidence (1981-1987) in men and women aged 20-74 years in England (Drever 1995). For melanoma of the skin it was observed that the risk was greatest in air traffic controllers for men and medical radiographers for women, which was reflected by the elevated PRRs and PMRs (Table 5). Additionally, statistically increased PRRs and PMRs were found for teachers not elsewhere classified for both men and women. Occupational exposure to solar and artificial UV radiation has been shown to cause melanoma (Siemiatycki et al. 2004). Occupations that are potentially associated with UV radiation (aircraft flight deck officers, medical radiographers and health professions not elsewhere classified) were found to have a significant PRR or PMR in the
5
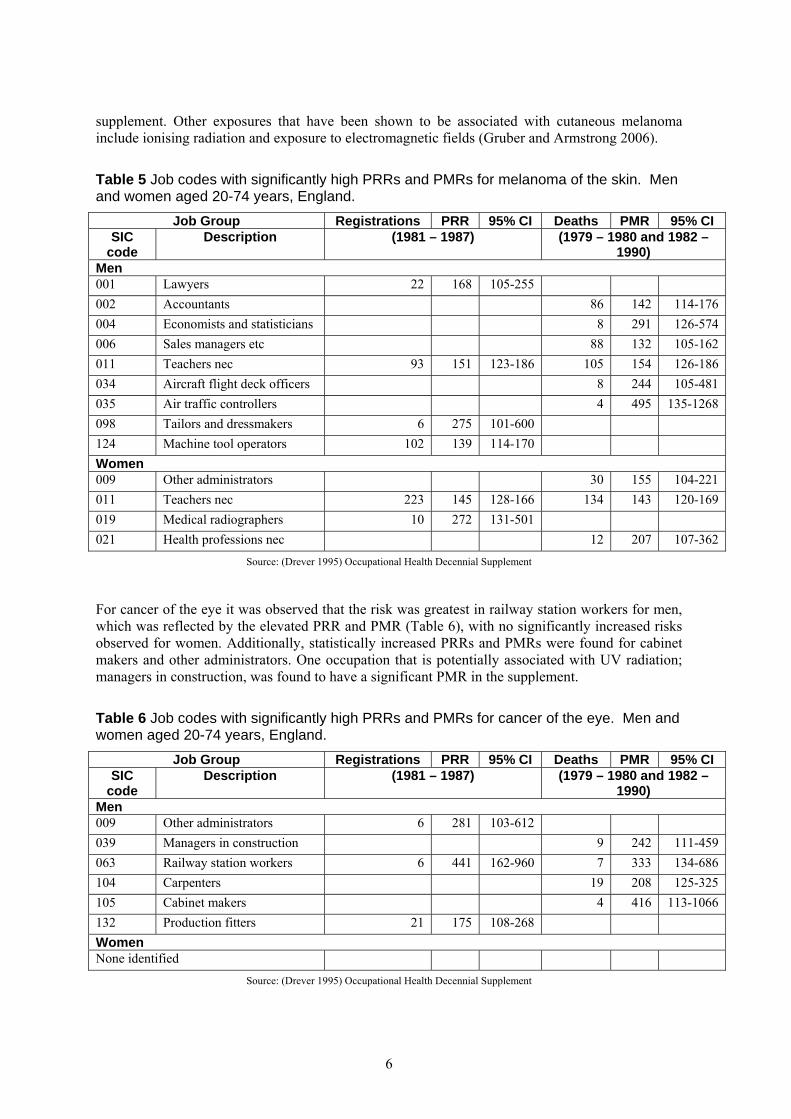
supplement. Other exposures that have been shown to be associated with cutaneous melanoma include ionising radiation and exposure to electromagnetic fields (Gruber and Armstrong 2006).
Table 5 Job codes with significantly high PRRs and PMRs for melanoma of the skin. Men and women aged 20-74 years, England.
Job Group Registrations PRR 95% CI Deaths PMR 95% CI SIC
code Description (1981 – 1987) (1979 – 1980 and 1982 –
1990) Men 001 Lawyers 22 168 105-255 002 Accountants 86 142 114-176 004 Economists and statisticians 8 291 126-574 006 Sales managers etc 88 132 105-162 011 Teachers nec 93 151 123-186 105 154 126-186 034 Aircraft flight deck officers 8 244 105-481 035 Air traffic controllers 4 495 135-1268 098 Tailors and dressmakers 6 275 101-600 124 Machine tool operators 102 139 114-170 Women 009 Other administrators 30 155 104-221 011 Teachers nec 223 145 128-166 134 143 120-169 019 Medical radiographers 10 272 131-501 021 Health professions nec 12 207 107-362
Source: (Drever 1995) Occupational Health Decennial Supplement
For cancer of the eye it was observed that the risk was greatest in railway station workers for men, which was reflected by the elevated PRR and PMR (Table 6), with no significantly increased risks observed for women. Additionally, statistically increased PRRs and PMRs were found for cabinet makers and other administrators. One occupation that is potentially associated with UV radiation; managers in construction, was found to have a significant PMR in the supplement.
Table 6 Job codes with significantly high PRRs and PMRs for cancer of the eye. Men and women aged 20-74 years, England.
Job Group Registrations PRR 95% CI Deaths PMR 95% CI SIC
code Description (1981 – 1987) (1979 – 1980 and 1982 –
1990) Men 009 Other administrators 6 281 103-612 039 Managers in construction 9 242 111-459 063 Railway station workers 6 441 162-960 7 333 134-686 104 Carpenters 19 208 125-325 105 Cabinet makers 4 416 113-1066 132 Production fitters 21 175 108-268 Women None identified
Source: (Drever 1995) Occupational Health Decennial Supplement
6
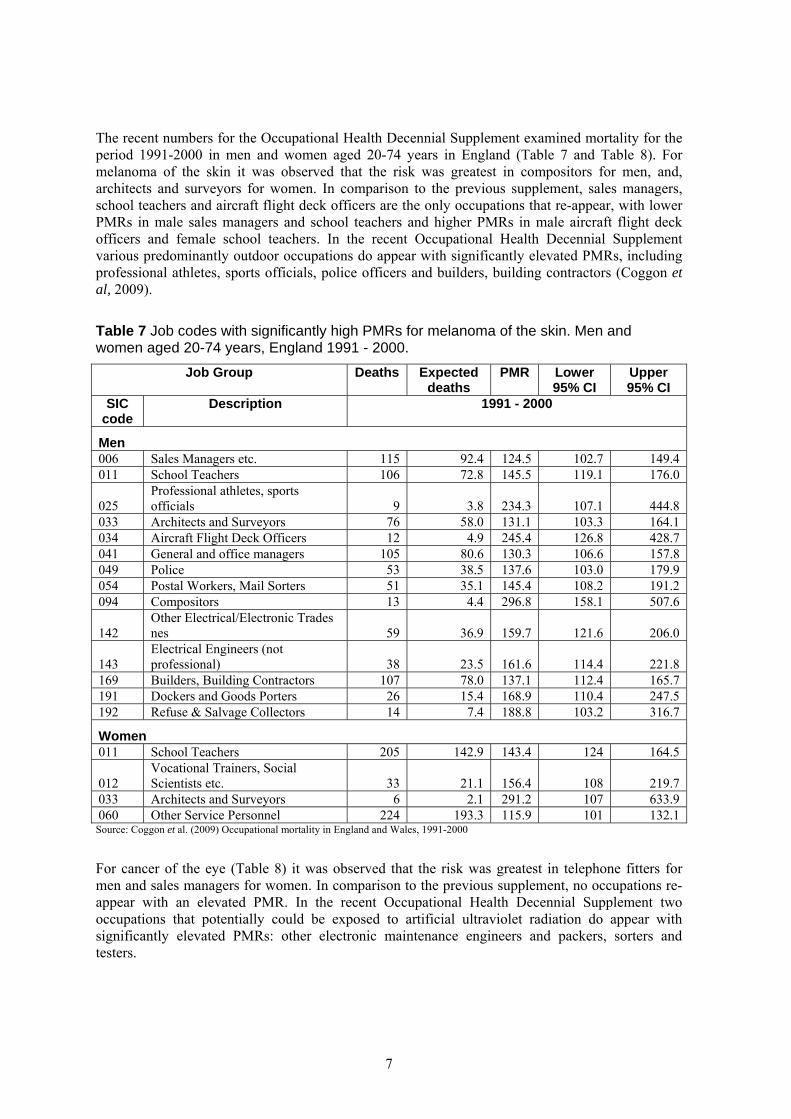
The recent numbers for the Occupational Health Decennial Supplement examined mortality for the period 1991-2000 in men and women aged 20-74 years in England (Table 7 and Table 8). For melanoma of the skin it was observed that the risk was greatest in compositors for men, and, architects and surveyors for women. In comparison to the previous supplement, sales managers, school teachers and aircraft flight deck officers are the only occupations that re-appear, with lower PMRs in male sales managers and school teachers and higher PMRs in male aircraft flight deck officers and female school teachers. In the recent Occupational Health Decennial Supplement various predominantly outdoor occupations do appear with significantly elevated PMRs, including professional athletes, sports officials, police officers and builders, building contractors (Coggon et al, 2009).
Table 7 Job codes with significantly high PMRs for melanoma of the skin. Men and women aged 20-74 years, England 1991 - 2000.
Job Group Deaths Expected deaths
PMR Lower 95% CI
Upper 95% CI
SIC code
Description 1991 - 2000
Men 006 Sales Managers etc. 115 92.4 124.5 102.7 149.4 011 School Teachers 106 72.8 145.5 119.1 176.0
025 Professional athletes, sports officials 9 3.8 234.3 107.1 444.8
033 Architects and Surveyors 76 58.0 131.1 103.3 164.1 034 Aircraft Flight Deck Officers 12 4.9 245.4 126.8 428.7 041 General and office managers 105 80.6 130.3 106.6 157.8 049 Police 53 38.5 137.6 103.0 179.9 054 Postal Workers, Mail Sorters 51 35.1 145.4 108.2 191.2 094 Compositors 13 4.4 296.8 158.1 507.6
142 Other Electrical/Electronic Trades nes 59 36.9 159.7 121.6 206.0
143 Electrical Engineers (not professional) 38 23.5 161.6 114.4 221.8
169 Builders, Building Contractors 107 78.0 137.1 112.4 165.7 191 Dockers and Goods Porters 26 15.4 168.9 110.4 247.5 192 Refuse & Salvage Collectors 14 7.4 188.8 103.2 316.7
Women 011 School Teachers 205 142.9 143.4 124 164.5
012 Vocational Trainers, Social Scientists etc. 33 21.1 156.4 108 219.7
033 Architects and Surveyors 6 2.1 291.2 107 633.9 060 Other Service Personnel 224 193.3 115.9 101 132.1
Source: Coggon et al. (2009) Occupational mortality in England and Wales, 1991-2000
For cancer of the eye (Table 8) it was observed that the risk was greatest in telephone fitters for men and sales managers for women. In comparison to the previous supplement, no occupations re-appear with an elevated PMR. In the recent Occupational Health Decennial Supplement two occupations that potentially could be exposed to artificial ultraviolet radiation do appear with significantly elevated PMRs: other electronic maintenance engineers and packers, sorters and testers.
7
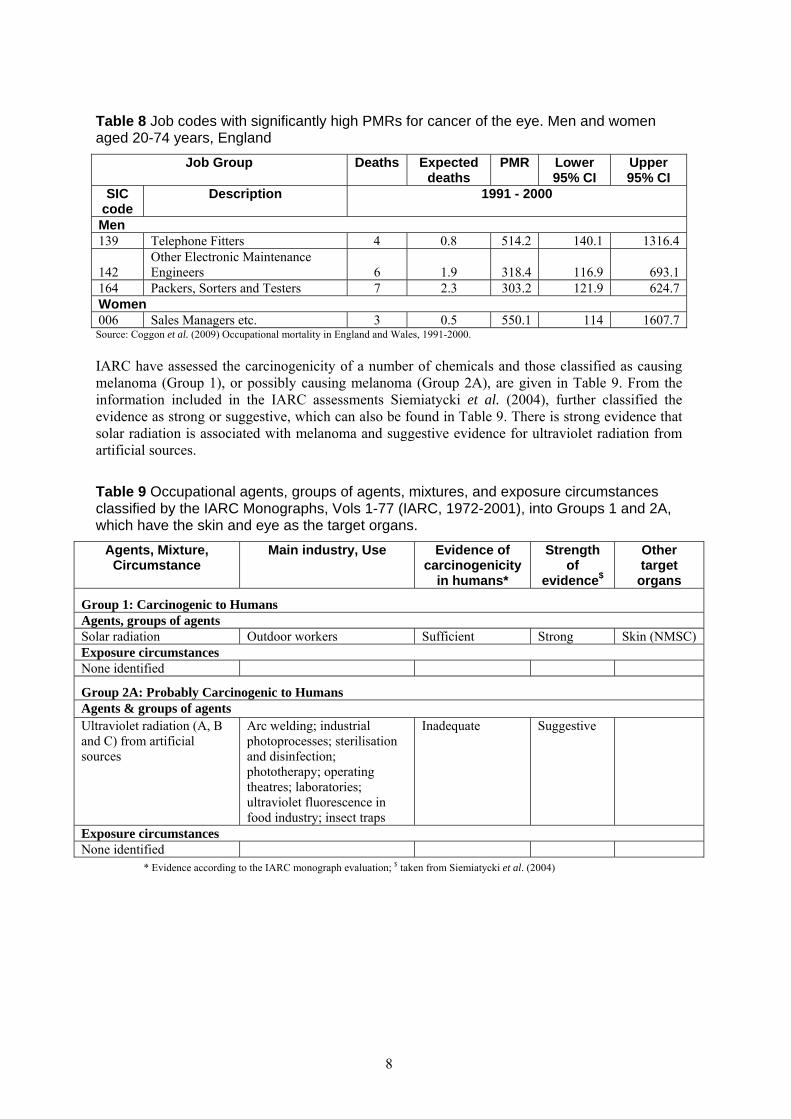
Table 8 Job codes with significantly high PMRs for cancer of the eye. Men and women aged 20-74 years, England
Job Group Deaths Expected deaths
PMR Lower 95% CI
Upper 95% CI
SIC code
Description 1991 - 2000
Men 139 Telephone Fitters 4 0.8 514.2 140.1 1316.4
142 Other Electronic Maintenance Engineers 6 1.9 318.4 116.9 693.1
164 Packers, Sorters and Testers 7 2.3 303.2 121.9 624.7 Women 006 Sales Managers etc. 3 0.5 550.1 114 1607.7
Source: Coggon et al. (2009) Occupational mortality in England and Wales, 1991-2000. IARC have assessed the carcinogenicity of a number of chemicals and those classified as causing melanoma (Group 1), or possibly causing melanoma (Group 2A), are given in Table 9. From the information included in the IARC assessments Siemiatycki et al. (2004), further classified the evidence as strong or suggestive, which can also be found in Table 9. There is strong evidence that solar radiation is associated with melanoma and suggestive evidence for ultraviolet radiation from artificial sources.
Table 9 Occupational agents, groups of agents, mixtures, and exposure circumstances classified by the IARC Monographs, Vols 1-77 (IARC, 1972-2001), into Groups 1 and 2A, which have the skin and eye as the target organs.
Agents, Mixture, Circumstance
Main industry, Use Evidence of carcinogenicity
in humans*
Strength of
evidence$
Other target
organs
Group 1: Carcinogenic to Humans Agents, groups of agents Solar radiation Outdoor workers Sufficient Strong Skin (NMSC) Exposure circumstances None identified
Group 2A: Probably Carcinogenic to Humans Agents & groups of agents Ultraviolet radiation (A, B and C) from artificial sources
Arc welding; industrial photoprocesses; sterilisation and disinfection; phototherapy; operating theatres; laboratories; ultraviolet fluorescence in food industry; insect traps
Inadequate Suggestive
Exposure circumstances None identified
* Evidence according to the IARC monograph evaluation; $ taken from Siemiatycki et al. (2004)
8
2.1 EXPOSURES FOR MELANOMA OF THE SKIN
2.1.1 Solar Radiation
Sunlight is visible light from the sun. Solar radiation is the combination of UV radiation and visible light that manages to reach the earths’ surface (wavelengths greater than 295nm). UV radiation that is less than 295nm does not reach the surface of the earth because the atmosphere absorbs it. UVB (280 to 315nm) is much more effective at producing cancer in animals, sunburn in humans, and DNA damage, than UVA (315 to 400nm). De Fabo et al. (2004) concluded that UVB was responsible for the induction of mammalian cutaneous malignant melanoma and UVA was ineffective. In epidemiological studies it is difficult to separate out the effects of UVB, UVA and visible light therefore it is typically treated as a whole. No consistent evidence that solar radiation causes melanoma of the eye could be found (English et al. 1997). For cutaneous melanoma, the distributions by atomic site, ethnic origin, place of residence and the effects of migration implicate solar radiation as a cause. Evidence that the condition is related to occupational exposure to the sun is lacking; however, the risk appears to increase with increasing exposure. The patterns emerging may be due to differences in characteristics between indoor and outdoor workers, for example, more genetically susceptible individuals choose to work in an indoor occupation (Diepgen and Mahler 2002). Any individual working outside regularly may be at increased risk; this includes farmers, construction workers, roadwork labourers, policemen and fishermen/sailors. Pilots and flight deck crews also come into contact with cosmic radiation, which includes solar UV radiation, and an increased risk has been observed (Gruber and Armstrong 2006). Vågerö et al. (1986) conducted an analysis based on cases diagnosed as malignant melanoma in Sweden between 1961 and 1979. The cancer cases were obtained from the extended Swedish Cancer Environment Registry and included all men and women who were born in the period 1896-1940 and were economically active at the Population Census of 1960. The population under study consisted of 2,630,458 individuals who were classified into three exposure groups: office workers, other indoor workers and outdoor workers, based on their occupation code and description. There were 4,706 cases of malignant melanoma. The entire working population was used for reference. Overall the morbidity ratios, standardised for age and county of residence (in 1960), showed a negative association between melanoma and outdoor workers (SMR=86, 95% CI=81-92) and indoor non-office workers (SMR=94, 95% CI=90-98). A significantly elevated risk was discovered for office workers (SMR=131, 95% CI=124-138). This trend remained present when the analysis considered only melanomas on covered parts of the body (trunk, upper limb and lower limb). However, when melanomas on uncovered parts of the body (eyelids, ear/auricular canal, face and scalp/neck) were investigated there was an elevated risk for all outdoor workers (SMR=107, 95% CI=92-123). After adjusting for social class the risk of melanoma on uncovered parts of the body remained elevated (SMR=109, 95% CI=94-126), and the risk for covered parts slightly increased (SMR=90, 95%CI=83-97). The authors note that there is a possibility that within each social class the patterns of sunlight exposure are different for the three groups and this cannot be entirely ruled out. Garland et al. (1990) conducted a study investigating the association between occupational sunlight exposure and melanoma in the US Navy. A total of 176 cases of cutaneous melanoma were identified in active-duty white males enlisted as Navy personnel in the period 1974 to 1984. Based on a review of job descriptions, individuals were categorised as indoor, outdoor or indoor and outdoor workers. The US civilian population was used for reference. The SEER (Surveillance Epidemiology and End Results) average annual age-adjusted incident rate was 9.2 per 100,000. Outdoor workers had a slightly higher rate of 9.4 per 100,000 (indoor workers were higher at 10.6 per 100,000). For all workers combined, melanoma occurred most frequently on the trunk, this rate
9
was significantly elevated for outdoor workers (3.9 per 100,000, p-value<0.05). In particular, two occupations yielded statistically significant increases in risk for melanoma; these were aircrew survival equipment men (SIR=6.8, 95% CI=2.5-14.7) and enginemen (SIR=2.8, 95% CI=1.3-5.1); however, these two occupations are carried out primarily indoors. Potential confounding genetic factors and recreational sun exposure were not taken into account in this study. The authors note that: “if persons genetically at higher risk of melanoma migrate into indoor occupations, then this for this reason alone indoor occupations may appear to be at higher risk of melanoma than outdoor occupations”. A case-control analysis was conducted using data recorded by the Los Angeles County Cancer Surveillance program (Goodman et al. 1995). Records were collected for all cancer cases among adult white males without Spanish surnames who were aged between 20 and 65 years in the period 1972 to 1990. In total there were 3,527 cutaneous melanoma cases and 53,129 other cancer cases used for reference. Among other aspects, exposure to sunlight during work was examined. Job titles were blindly categorised into three categories: mainly indoor (reference category), indoor/outdoor or mainly outdoor. For the two non-reference exposure categories, the age adjusted proportionate incidence odds ratios were close to that expected (OR=0.97 for indoor/outdoor and OR=0.78 for mainly outdoor). However, when the estimates were further adjusted to take into account birthplace (as a substitute for sun exposure in childhood and adolescence) and education, there were elevated risks for melanoma, 1.16 (95%CI=1.07-1.27) and 1.15 (95%CI=0.94-1.40) for indoor/outdoor and mainly outdoor respectively. On investigating anatomical location of the cases, there were slightly elevated ORs for face/head/neck and trunk for outdoor workers (OR=1.26, 95% CI=0.78-2.05 and OR=1.28, 95% CI=0.99-1.67). In terms of occupations for the non-reference groups, many had significantly elevated OR estimates, some of which include sign painter/letterer, surveyor and chemical engineer. The authors suggest that lifestyle factors associated with higher education levels may be more important than work environment on melanoma risk. Miller and Beaumont (1995) conducted a proportionate mortality study of various causes of deaths among California veterinarians from January 1960 through December 1992. Deceased veterinarians were identified from archived files from the California State Board of Examiners in Veterinary Medicine and a computerised list from the American Veterinary Medical Association. The study consisted of 450 veterinarians (430 white males, 6 non-white males and 14 white females). Mortality from malignant melanoma was significantly higher than expected (SPMR=3.25, 95%CI=1.62-6.52, n=7). The one observed death of cancer of the eye was also melanoma, which yielded a significant estimate (SPMR=12.41, 95%CI=2.70-56.96). All the deaths due to malignant melanoma were in white males. Analyses by race and sex gave similar estimates (white males: SPMR=3.47, 95%CI=1.74-6.94; white total: SPMR=2.23, 95% CI=1.61-6.49 and males total: SPMR=3.46, 95%CI=1.73-6.92). Self-employed and employee veterinarians had significantly elevated mortality from malignant melanoma: SPMR=2.68 (95%CI=1.05-6.85, n=4) and SPMR=6.05 (95%CI=1.81-20.27, n=2) respectively. Deaths from malignant melanoma were significantly elevated in individuals who had been employed in the profession between 20-29 years (SPMR=4.48, 95%CI=1.27-15.78, n=2) and 30 or more years (SPMR=3.86, 95%CI=1.35-11.00, n=3). Elwood and Jopson (1997) conducted a systematic review of all published case-control studies that had assessed melanoma and sun exposure. Studies were identified via many sources including the IARC review up to 1992, MEDLINE and other referenced studies. Results from the studies were classified as relating to intermittent, occupational or total sun exposure and the highest reported exposure category was compared to the lowest exposure category. Where possible, estimates that were adjusted for demographic factors, such as age and sex, and susceptibility characteristics, such as ethnic origin and skin pigmentation, were used. Studies were excluded if there was no OR or 95% CI reported and they could not be calculated from the information provided. Overall, 29 studies contributed data on sun exposure yielding a significant positive risk (OR=1.71,
10
95%CI=1.54-1.90, 6,934 cases, 23 studies) for intermittent exposure and a significantly reduced risk (OR=0.86, 95%CI=0.77-0.96, 6,517 cases, 20 studies) for heavy occupational exposure. Of the studies used in evaluating occupational exposure, eight showed increased risk (4 of which were significant) and twelve showed reduced risk (again 4 were significant). The four studies giving the highest risks contributed to heterogeneity, removing these gave a significantly reduced risk estimate (OR=0.76, 95%CI=0.68-0.86, 16 studies). Fourteen of the studies collected information on both intermittent and occupational exposure; therefore, a comparison could be made. A significantly elevated OR for intermittent exposure and a significantly decreased OR for occupational exposure prevailed even after the five studies contributing to heterogeneity were removed. The authors state that a more detailed analysis of some of the large studies suggests that the relationship between melanoma and occupational sun exposure may be non-linear. With an increased risk related to small amounts of exposure, possibly due to intermittent outdoor work, and a decrease in risk for continued long heavy exposure, possibly due to constant solar radiation exposure resulting in an adequate protection mechanism. However, protection mechanisms such as tanning and skin thickening may not be the total explanation. All deaths from melanoma between 1984 and 1991 in 24 states in the US were analysed by Freedman et al. (1997). Cases were from a 24 state mortality database, aged 20 and over and identified as either white or African American. Two controls were selected from non-cancer deaths in the database and matched by sex, race and age. Potential sunlight exposure was assessed by state of residence and usual occupation recorded on the death certificate. Mean residential sunlight exposure was collected from the United States Weather Bureau and each state was characterised as low sun, moderate sun or high sun exposure. Occupations were classified by an industrial hygienist into four categories: indoor work, combined indoor and outdoor work, outdoor work by non-farmers and farming. For non-farming occupational sunlight exposure, the risk of melanoma was close to that expected (OR=0.99, 95%CI=0.87-1.12), whereas farmers were at significantly increased risk compared to indoor workers (OR=1.31, 95%CI=1.14-1.52). The risk of melanoma was found to be elevated among outdoor workers with low and moderate residential exposure (OR=1.22, 95%CI=0.99-1.50 and OR=1.05, 95%CI=0.86-1.29 respectively). The estimates were adjusted for age, sex, race, residential sunlight exposure and socioeconomic status. There was no clear pattern of risk associated with occupational exposure across sex, race or age groups. Cerhan et al. (1998) conducted a cancer mortality study on white male Iowa farmers aged over 20 years in 1987 to 1993. The final cohort consisted of 88,090 white male farmers, using a reference group of all deaths of Iowa decedents who were white male non-farmers. Overall farmers had an excess of deaths due to melanoma of the skin (PMR=1.17, 85%CI=0.94-1.45). However, the excess was only significantly elevated for younger farmers, aged 20-64 years (PMR=1.60, 95% CI=1.07-2.38). All estimates were adjusted for age. The authors state that this excess was consistent with occupational exposure to ultraviolet light. A meta-analysis of 37 studies to assess whether farmers had an elevated cancer incidence rate was conducted in 1998 (Acquavella et al. 1998). The studies used were identified from references of a previous meta-analysis conducted by Blair and colleagues in 1992 and a MEDLINE search through 1994. Blair and colleagues reported an elevated rate for malignant melanoma amongst farmers (RR=1.15, 95%CI=1.04-1.28). One study from Blair et al. could not be obtained. Other studies that did not report findings for three or more diseases were excluded to reduce publication bias, along with additional studies that did not provide adequate information to enable calculation of standard errors (another study from Blair et al. was excluded for this reason). In total, there were twenty-one studies analysed for malignant melanoma in white male farmers resulting in a pooled random effects estimate of 0.95 (95% CI=0.82-1.09). However, there was evidence of heterogeneity. Reanalysis of the original studies, apart from two, gave a pooled estimate for the ten relevant studies as 1.12 (95% CI=0.96-1.29) and no evidence for heterogeneity. Pooled rates varied depending on study design; RR=0.87 (95%CI=0.69-1.10), RR=0.94 (95%CI=0.84-1.04) and
11
RR=1.14 (95%CI=0.74-1.47) for follow-up studies, PMR studies and case-control studies respectively. Unfortunately, there was no detail available to enable a specific exposure analysis. In addition, there were no clear conclusions from the results, due to variations in the reported RRs both above and below the null hypothesis. A hospital based case-control study was conducted in five Italian rural areas to examine the association between cancer and farming among women (Settimi et al. 1999). Altogether 1,044 newly diagnosed cancer cases, aged 20-75 years were ascertained from hospital records from March 1990 to September 1992, of which 26 were skin melanoma cases. The reference group was drawn from other cancer cases, excluding lung and non-melanoma skin cancer cases. All estimates were adjusted for age. Ever being employed as a farmer or farm labourer was associated with a statistically significant increased risk (OR=2.7, 95%CI=1.2-6.0, n=26), as did being engaged in agricultural jobs for 10-19 years (OR=6.6, 95%CI=2.2-19.0, n=5). Vine growing was non-significantly associated with an OR of 2.5 (95%CI= 0.4-14.8, n=8). Non-significant increases in risk were observed for length of employment of 1-9 years (OR=1.1, 95% CI=0.1-8.9) and over 20 years (OR=2.1, 95%CI=0.8-5.8). An excess risk was also found for growing vegetables (OR=1.4, 95%CI= 0.3-5.9, n=3). No associations were found for growing wheat or fruit-trees, 0.9 (95%CI= 0.2-5.4, n=7) and 0.7 (95%CI=0.1-5.2, n=1) respectively. A case-control study in Ontario, Canada found that chronic exposure to solar UV radiation was associated with a significantly reduced risk of malignant melanoma (Walter et al. 1999). Eligible cases were individuals who had been newly diagnosed with cutaneous melanoma, were 20-69 years of age at diagnosis, lived in one of six counties in southern Ontario and were diagnosed through one of the hospitals or a private pathology laboratory between 1984 and 1986. Controls were randomly selected from property tax assessment rolls and were matched to cases based on age, sex and residence. Non-whites and non-English speaking individuals were excluded from the study. Chronic exposure was indicated either by days of outdoor activity during adolescence (non-vacation and non-beach) or occupational outdoor hours in recent adult life. For recent occupational exposure the adjusted odds ratio was 0.78 (95%CI= 0.61-0.99). Investigating body location of the tumour gave similar results, 0.82 (95%CI=0.60-1.12) and 0.74 (95%CI=0.56-0.99) for trunk and non-trunk respectively. For the four tumour subtypes (superficial spreading/on situ, nodular, lentigo maligna and other/unclassifiable) the estimates varied from 0.49 to 0.86. The estimates were adjusted for age, sex and initial reaction to summer sun (burning or not burning). The authors conclude that their results provide qualified support that intermittent UV exposure may carry an elevation in melanoma risk and, conversely, that chronic exposure may provide some protection. Lee et al. (2002) conducted a proportionate mortality analysis on 267,479 farmers from 26 states in the US who worked in the crop (n=222,549) or livestock (n=44,930) industry. Death certificate information was collected from the National Occupational Mortality Surveillance database for the years 1984-1993. The reference group was all deaths among decedents in the database. All estimates were age adjusted. For melanoma of the skin estimates were produced for white male farmers only which gave PMR=95 (95%CI= 87-105, n=459) and PMR=110 (95%CI=92-132) for crop and livestock farmers respectively. Investigating age revealed a significant increase in young (aged 15-64 years) livestock farmers with PMR=150 (95%CI=110-200, n=47). Young crop farmers also had an excess risk but this was non-significant (PMR=106, 95% CI=88-125, n=131). Older (over 65 years) farmers in both groups had non-significant decreased risks of 92 (95%CI=82-103, n=328) for crop farmers and 95 (95% CI=75-119, n=76) for livestock farmers. No combined estimates were given for all white male farmers or for all farmers (white male, non-white male, white female and non-white female). Travier et al. (2003) used the nationwide, Swedish Cancer Environment Registry III to compare cancer incidence among male veterinarians to that of the remaining active population (excluding other occupational groups that have extensive contact with animals, such as breeders, hunters and
12
butchers). Individuals were followed for cancer incidence and mortality from January 1971 to December 1989, focusing on males who were employed as veterinarians or in veterinary medicine in either the 1960 or the 1970 census. A total of 1,178 male veterinarians were identified. Within the group individuals were categorised into one of three sub groups: veterinarians in the veterinary industry, veterinarians in other industries, workers other than veterinarians in the veterinary industry. However, when these three subgroups were analysed separately, any workers employed as a veterinarian in one census and as a non-veterinarian in the veterinarian industry in the other were excluded. For males identified as veterinarians or other workers of the veterinary industry a significant increase in risk was observed for melanoma of the skin (SIR=2.86, 95%CI=1.43-5.13, n=11) compared to the remaining active male population. For the subgroups an increased risk was observed in all three, veterinarians in the veterinary industry RR=2.77 (95% CI=1.24-6.17, n=6); which mainly arose on the trunk (RR=4.80, 95%CI=1.99-11.55, n=5), veterinarians in other industries RR=1.84 (95%CI=0.26-13.08, n=1) and other workers in the veterinary industry RR=3.12 (95%CI=1.01-9.67, n=3). A significant increase was also found just for veterinarians employed at the 1960 or 1970 censuses (RR=2.33, 95%CI=1.16-4.67, n=8) when compared to the rest of the male employed population with the highest income and education. RRs were adjusted for age, calendar period, geographic region and urban setting. The authors conclude that the excesses observed for melanoma could not be explained by the high socio-economic status of veterinarians, as the excess remained when comparisons were made with other high socio-economic groups. They also note that the results may reflect the carcinogenicity of occupational exposures including solar radiation. Ramirez et al. (2005) conducted a review on occupational skin cancer and ultraviolet and other forms of radiation from available published papers. They found an increased risk of skin cancer (including melanoma) amongst outdoor workers. In particular, deaths from melanoma were increased for non-white farmers (PMR=2.3, OR=6, n=6), police officers (SIR=1.37, 90%CI=1.08-1.72), physical education teachers (SIR=2.01) and pilots and cabin attendants (SIR varies between studies from 1.8 to 10.20). The authors noted a lack of available information on other professionals who spend time outside as part of their job, such as professional cyclists. A meta-analysis investigating sun exposure and cutaneous melanoma found a positive association for intermittent sun exposure, and, an inverse association with a high continuous pattern of sun exposure (Gandini et al. 2005). Relative risks for sun exposure were extracted from fifty-seven studies published prior to September 2002, based on subjects aged over 20 years, of which forty-one were eligible for investigation of chronic (occupational) sun exposure. The majority of studies were carried out in European countries, with others being conducted in North America, Australia, New Zealand, Argentina, Brazil and Israel. There were several studies that presented risk estimates lower than one indicating an inverse association, the majority being non-significant. The pooled estimate showed a slight inverse association but was again non-significant (RR=0.95, 95%CI=0.87-1.04). On further investigation it was found that the variability between studies could be explained by “inclusion of controls with dermatological diseases” and “latitude”. The pooled RR of the twenty-six studies that did not include dermatological diseased controls was 0.87 (95% CI=0.74-1.02), whereas the studies that did include them resulted in a significantly higher RR of 1.29 (95%CI=1.06-1.57). It was shown that living at higher latitudes gave a greater association between chronic sun exposure and melanoma. For the thirty-two studies that latitude was calculated, the pooled estimate was RR=0.98 (95%CI=0.85-1.12). Cancer incidence among indoor and outdoor working longshoremen in Genoa was retrospectively studied (Puntoni et al. 2005). In total 4,993 longshoremen that were ever employed at the dock of Genoa between 1933 and 1980 were included in the study. They were employed at one of two dockyard trading companies: the “Stefano Canzio” and “San Giorgio”. Cancer incidence was obtained from the Genova Cancer Registry for 1986-1996. According to their prevalent pattern of occupational sunlight exposure, eligible individuals were categorised as an indoor (n=2,451) or
13

outdoor (n=2,101) worker. The male population of the City of Genova was used for reference and estimates were adjusted for age. A statistically significant excess risk of cutaneous melanoma was observed for outdoor workers (SIR=288, 95%CI=125-568, n=8). No excess was observed among indoor workers (SIR=97, 95% CI=20-284). When outdoor workers were compared to indoor workers, a higher incidence for melanoma was observed (RR=2.97, 95%CI=0.71-17.41) although this was non-significant. The authors note that the non-significance is due to similar exposures being shared by the two subgroups, and the lower statistical power obtained by using an internal rather than external reference group. The threefold increased risk detected only among outdoor workers supports the causal role of exposure to sunlight. 2.1.2 Ultraviolet Radiation from Artificial Sources
Occupational exposure to artificial UV radiation occurs in many medical and industrial processes. Electric welding arcs are the main occupational exposure to UV radiation; they emit radiation within a radius of several meters, thus people working nearby not just welders themselves can suffer from overexposure. Gas welding and cutting torches also produce UV radiation but at a much lower level as this process mainly consists of exposure to infrared radiation. Arc lamps are commonly used in film/movie projection and as a source of light in large spotlights and floodlights. They can also be used in the printing industry. However, more often, curing lamps are used, particularly for hardening resins and for drying paints and other substances. Germicidal lamps are commonly used for sterilisation of workspaces and tools, particularly in biology laboratories and medical facilities. Germicidal lamps can also be used for sterilisation of hot tubs and aquariums, for industrial water treatment to kill microorganisms and by geologists to aid identification of particular minerals. They emit strong UVB and UVC radiation thus tend to be placed where direct exposure cannot occur. Ultraviolet lasers are also used in medical and industrial processes; however, they do not emit visible light and thus exposure can be unexpected and intense. Therapeutic lamps used in physiotherapy and dermatology for treatment of skin conditions emit either UVA or UVB radiation, phototherapy is typically exposure to UVB and tends to last for a short amount of time (under 1 minute) due to the possibility of skin damage. “Black lights” are UVA lamps mainly used for non-destructive testing, such as authentication of antiques and banknotes, detection of substances not visible to the naked eye (forensic examination) and for medical diagnosis. Other uses of “black lights” include insect control in food preparation areas and in the entertainment industry. Typically, “black lights” are low exposure risk unless exposure to the eye occurs at close range. People may also be exposed to fluorescent lighting which is commonly used on the workplace, these may emit UV radiation but the levels are generally low; IARC (1992) classified fluorescent lighting as a group 3 carcinogen. A retrospective cohort study conducted on biomedical research laboratory personnel in Swedish Universities found elevated incidence for malignant melanoma among female scientists in laboratories and male scientists in non-laboratory departments (Wennborg et al. 1999). The study included all individuals who had been employed at least 1 year and 1 day for more than 50% of full time between January 1970 and December 1989. Laboratory departments with biological or biomedical research as their main activity were identified from four institutions. Departments were eligible if they had existed as an independent research institution for at least 10 years before 1989. A non-laboratory group working in departments of law, economics, social sciences and sciences (such as mathematics and statistics) at the same four institutions were used as an internal reference group. Swedish national mortality rates were used for comparison. In total, 7,958 individuals (5,035 laboratory and 2,923 non-laboratory) were followed for mortality and cancer incidence until December 1992. Deaths were identified using the Swedish register of causes of death at Statistics Sweden and cancer cases were identified from the National Swedish Cancer Registry. For women in laboratory departments and men in non-laboratory departments there was an increased SIR for malignant melanoma of 1.46 (95%CI=0.54-3.18, n=6) and 2.62 (95%CI=0.96-5.70, n=6) respectively. In contrast for men in laboratory departments and women in non-laboratory
14

departments there was a reduced risk with SIR=0.79 (95% CI=0.16-2.30, n=3) and SIR=0.96 (95%CI=0.02-5.36, n=1) respectively. In terms of occupations within the laboratory group, elevated risks of melanoma were observed for female scientists (SIR=3.51, 95% CI=0.96-8.98, n=4) and male technical staff (SIR=1.32, 95% CI=0.03-7.33, n=1). Male scientists, female laboratory technicians and secretaries were found to have a reduced risk (SIR=0.69, 95% CI=0.08-2.51, n=2 and SIR=0.86, 95%CI=0.10-3.11, n=2 and SIR=0.99, 95%CI=0.03-5.52, n=1 respectively). Estimates were adjusted for age and calendar time. Unfortunately no combined estimate for males and females was given. The authors note that the numbers in the study are low and there are few cases due to the young cohort, affecting the precision of the study and resulting in broad confidence intervals for estimates. They also state that the follow-up may not be long enough to detect certain cancer types. Shaham et al. (2003b) conducted a cohort study on 4,300 laboratory workers in Israel (3,272 female and 1,028 male). All the workers were either employees or retirees from hospital laboratories, peripheral clinic laboratories, research institute laboratories or industrial research and development laboratories during 1960-1997. Individuals were classified in terms of job type (routine, researcher, maintenance and administration) and further in terms of the type of laboratory (i.e. research, bacteriology, general analysis and pathology), corresponding to if they had ever worked in that job or particular laboratory type. The follow-up period was from 1960 to 1997 and cancer cases were identified via the Israeli Central Cancer Register. Israel cancer rates from the Central Cancer Registry were used for comparison. Estimates were adjusted for age, sex, origin and periods of calendar time. A total of 19 cases of melanoma of the skin were observed resulting in a non-significant SIR of 1.47 (95%CI=0.89-2.30). The elevated risk was seen in both men (SIR=2.14, 95% CI=0.78-4.65, n=6) and women (SIR=1.29, 95% CI=0.69-2.20, n=13). In terms of job classes, significant excesses were observed for all male workers, all researchers and all workers (the whole cohort) after a 20 year latency period was introduced, SIR=3.96 (95%CI=1.08-10.2, n=4), SIR=5.77 (95%CI=1.19-16.9, n=3) and SIR=2.39 (95%CI=1.15-4.39, n=10) respectively. In terms of laboratory type, elevated risks were found for laboratory type 2 (bacteriology, virology, animal, parasitology and plants) and laboratory type 3 (routine/general analysis – chemistry, urine, endocrine, haematology and endocrinology) workers, with respective SIRs of 2.48 (95% CI=0.91-5.40) and 1.54 (95% CI=0.70-2.92). In order to investigate further the cancer pattern in this cohort and associations with particular occupational exposures and personal risk factors, the authors performed a nested case-control study and published the results separately (Shaham et al. 2003a). In total there were 163 cases of cancer diagnosed in individuals who has worked for at least 1 year in the laboratory. The two control groups comprised of healthy workers who had no diagnosis of cancer; the first group (internal controls) were laboratory workers (n=311) who were original members of the cohort and matched to cases by type of laboratory in the same workplace, age, gender and origin, and the second group (external controls) were 448 individuals selected from the general population who were matched to cases by age, gender, origin, year of immigration to Israel and residential area. A reference age was chosen for each set of cases and controls based on the age of the case at diagnosis; the duration of exposure to particular agents for both the case and relevant controls was calculated up to the reference age. Overall, there were 16 cases of melanoma skin cancer used in the analysis. All laboratory cases and controls were categorised into four exposure groups; group 1: exposed to known human carcinogens (further divided into subgroups relative to the carcinogen), group 2: exposed to suspected human carcinogens, group 3: exposed to substances that are not known to be human carcinogens and group 4: exposures due to handling laboratory animals. The analysis concentrated on laboratory types 1 and 2 since these were where the majority of excess cancer incidents were found. Of the 16 melanoma cases, 2 were exposed to solar radiation and 13 were exposed to suspected carcinogens. The authors conclude that there is a possible association between risk of melanoma and working in a laboratory, that cannot be explained by chance or personal risk
15
factors. However, laboratory workers are exposed to a variety of carcinogens, thus the excess risk observed in the cohort study (Shaham et al. 2003b) could not be attributed to a specific exposure. A cohort consisting of all male and female nurses registered with the professional regulatory body in British Columbia for at least a year between 1974 and 2000 was studied for cancer incidence and mortality (Dimich-Ward et al. 2007). The Canadian Mortality Database and the Canadian Cancer Registry were used to ascertain individual status. The British Columbia population was used for reference. The follow-up for mortality was from 1974 to 2000; the follow-up for cancer incidence was from 1974 to 1999. In total there were 58,125 registered nurses in the cohort., However, due to the low numbers of male deaths and cancer incidence, the study was conducted on 56,213 female registered nurses. There was an increased, although non-significant, mortality risk for malignant melanoma (SMR=1.27, 95%CI=0.84-1.85, n=27). The only significantly increased cancer incidence risk was observed for malignant melanoma (SIR=1.27, 95%CI=1.10-1.46, n=206). There was also a significantly elevated risk for 15-25 years of employment (with a 10 year lag), and a statistically significant trend (RR=1.37, 95%CI=0.92-2.06 for 5-15 years, RR=2.05, 95%CI=1.22-3.45 for 15-25 years and RR=1.89, 95%CI=0.9-3.98 for over 25 years). Since melanoma is known to be highly associated with sun exposure, the authors note that the relationship found may be attributable to non-occupational factors such as sun exposure. One study on occupational ultraviolet radiation exposure was investigated and reported in the IARC monograph (1992). No association between arc welding fumes or ultraviolet radiation was found in the study. Associations between melanoma of the skin and use of sunbeds or sunlamps and exposure to fluorescent lighting at work were found. There is little evidence that the exposure induces occupational cutaneous melanoma. As mentioned previously, there is also inadequate evidence that fluorescent lighting at work is associated with the disease and IARC classified the exposure as group 3. 2.2 EXPOSURES FOR MELANOMA OF THE EYE
2.2.1 Solar Radiation
A case-control study in France examined the role of occupational exposure to ultraviolet radiation on the occurrence of ocular melanoma (Guenel et al. 2001). This study used the French cohort from the European study by Lutz et al. (2005). Cases (n=50) were from ten French administrative areas, diagnosed with uveal melanoma in 1995-1996 and aged 35-70 years. Controls (n=479) were selected at random from electoral rolls, matched on age, gender and area. Estimates of occupational exposure to solar and artificial UV light were made using a job exposure matrix. All estimates were adjusted for age and gender. Exposure was assessed relative to the median cumulative exposure estimated among exposed controls (scores of 220 and 70 for Solar and Ultraviolet Radiation respectively). A risk similar to that expected was observed with exposure to solar ultraviolet radiation. The odds ratios were 1.2 (95%CI=0.5-2.8) and 0.9 (95%CI=0.4-2.3) for exposure less than and greater than the median respectively. No excess risk was observed in the agricultural workers, forestry workers or fishermen group (Men: OR=0.5, 95%CI=0.2-1.6; Women: OR=1.6, 95%CI=0.5-5.5). Unfortunately, information on recreational exposures to UV radiation was not collected, so this could not be taken into account in the analysis. The authors note that indoor and outdoor workers may have similar total sunlight exposure, which would lead to no detection of an elevated risk due to sunlight exposure from occupation, and may explain the non-significant association observed. Also noted was the possibility that a continuous pattern of exposure to sunlight of outdoor workers may not increase ocular melanoma risk. A meta-analysis to examine the association between ultraviolet light exposure and uveal melanoma was carried out on twelve studies that provided sufficient information to calculate odds ratios and standard errors (Shah et al. 2005). The published data was categorised as either intermittent
16

ultraviolet exposure (including welding) or chronic ultraviolet exposure (including occupational sunlight exposure). Of the twelve studies, nine relate to artificial UV exposure from welding or occupational solar radiation (five of the studies are discussed independently in this report (Ajani et al. 1992; Monarrez-Espino et al. 2002; Guenel et al. 2001; Holly et al. 1996; Vajdic et al. 2004)). Regarding occupational sunlight, based on exposure scores comparing the most extreme to the lowest exposure, the meta-analysis identified 572 cases of uveal melanoma from four studies, resulting in an elevated but non-significant summary OR of 1.37 (95%CI=0.96-1.96). Between the studies there was no significant evidence of heterogeneity. The authors concluded that occupational sunlight exposure was a non-significant risk factor for the development of uveal melanoma. Due to the relatively small number of studies available that potentially under-power the analysis the results should be interpreted with caution. Lutz et al. (2005) conducted a case-control study in nine European countries (Denmark, France, Germany, Italy, Latvia, Portugal, Spain, Sweden and the UK), to study potential occupational risk factors for uveal melanoma, in particular occupational exposure to sunlight and artificial UV radiation. Cases were incidents of uveal melanoma in patients aged 35-69 years diagnosed or possibly diagnosed within a two-year period (mainly January 1995 to December 1996, with last recruitment in August 1997). Controls were frequency matched with cases by region, gender and five-year birth cohorts. In the UK one control per case was selected from the cases’ General Practitioners’ list. Otherwise, two types of controls were used in the European rare cancer study; population based cancer controls (from population registers in Denmark, Germany, Italy and Sweden, and from electoral rolls in France), and colon cancer controls (from incidence cases in Denmark and Latvia and from hospital patients in Spain and Portugal). However, when colon cancer controls were used in the analysis, confounding could not be excluded, thus estimates given below are for population-based controls only. The dataset from the UK was relatively small (17 cases) and was subsequently merged with the German dataset. Information was collected on demographics, personal characteristics, medical history, tobacco and alcohol use, as well as occupational exposures and occupational history of jobs of at least six months (implying that individuals can contribute to more than one occupation). Occupational exposure to sunlight and artificial UV radiation was assessed from a job exposure matrix. Each job was assigned a probability for proportion of workers exposed, frequency of exposure and intensity of exposure, resulting in a cumulative dose for each individual. Estimates were adjusted for country, gender and five-year birth cohort. Additionally, estimates were adjusted to control for eye colour, this gave similar results and therefore are not presented. In total there were 226 cases and 2,049 population controls used in the analysis. Exposure to occupational sunlight was associated with an elevated, but non-significant, risk of uveal melanoma (RR=1.24, 95% CI=0.88-1.74, n=63). This elevated risk was higher in women (RR=1.83, 95%CI=0.94-3.54, n=14) than men (RR=1.09 95% CI=0.74-1.62, n=49). Relative to cumulative dose, exposure below the median gave a risk of 1.34 (95% CI=0.90-1.99, n=40) and exposure above the median gave a risk of 1.10 (95% CI=0.68-1.79, n=23). In terms of country, risks were elevated for all but one, but again results did not reach statistical significance (Denmark: RR=1.96, 95%CI=0.97-3.94, n=21, France: RR=1.11, 95%CI=0.56-2.20, n=14, Germany and UK: RR=1.28, 95%CI=0.64-2.56, n=14, Italy: RR=1.16, 95%CI=0.35-3.83, n=4 and Sweden: RR=0.78, 95%CI=0.35-1.77, n=10). With respect to particular occupations, seamen and fishermen had an elevated risk (RR=2.46, 95%CI=0.94-6.41, n=6), as did bricklayers and other construction workers (RR=1.29, 95%CI=0.69-2.41, n=13), forestry workers, hunters and related workers NOS (RR=1.28, 95%CI=0.47-3.47, n=5) and farmers (RR=1.09, 95%CI=0.72-1.66, n=33). In particular, female farmers were at increased risk (RR=1.84, 95%CI=0.91-3.74, n=12) and male farmers appeared to have a reduced risk (RR=0.87, 95%CI=0.52-1.45, n=21). The authors conclude that occupational exposure to sunlight was overall not associated with a significantly increased risk of uveal melanoma. Occupational exposure to solar radiation was reported in the IARC monograph (1992) as exposure of farmers. The study results were inconsistent, with two studies reporting an increased risk of
17
death, two studies reporting a decreased risk and a further study reporting no elevated risk for incidence. Two of the five studies were conducted in Great Britain; both these studies report no elevated risk for incidence or mortality. The overall IARC evaluation was that solar radiation causes cutaneous malignant melanoma and non-melanocytic skin cancer. Hence, this report will not investigate occupational exposure to solar radiation and the occurrence of melanoma of the eye. 2.2.2 Ultraviolet Radiation from Artificial Sources
Holly et al. (1990) conducted a case-control study in the United States to investigate the relationship between uveal melanoma and potential risk factors. Cases were patients that were diagnosed with uveal melanoma between January 1978 and February 1987 at the Ocular Oncology Unit at the University of California, San Francisco. In total 407 white patients, who were aged between 20 and 74 years of age and resided in one of the eleven Western United States (Washington, Oregon, California, Idaho, Nevada, Utah, Arizona, Montana, Wyoming, Colorado and New Mexico), were interviewed. Random-digit dial telephone methods were used to select a sample of 870 white control subjects from the eleven Western States where the patients resided. A larger proportion of patients (4%) than controls (1%) had been exposed to UV (excluding sunlight exposure) or black lights, which resulted in significant excesses being observed. The unadjusted estimate was RR=3.52 (95% CI=1.49-8.41, n=16) and the adjusted estimate was RR=3.69 (95% CI=1.57-8.70). The estimate was adjusted for eye colour, number of cups of coffee per day, effect of half and hour sun exposure, leisure time spent indoors or outdoors, occurrence of snow blindness/eye burns and age. Investigation of the number of years exposed to UV or black lights supported an association with uveal melanoma with corresponding risk estimates of 2.9 and 3.8 for 1-5 years exposure and for 6 or more years exposure respectively. Ever suffering from welding burn to the eye, sunburn to the eye or snow blindness was also positively associated with ocular melanoma (RR=7.54, 95% CI=2.60-23.52 unadjusted and RR=7.17, 95% CI=2.50-20.57 adjusted). The French study described previously by Guenel et al. (2001) found that there was a significantly increased risk of ocular melanoma in individuals exposed to artificial UV radiation, with a significant dose-response relationship. The odds ratios were 2.6 (95%CI=0.5-12.4) and 5.5 (95%CI=1.8-17.2) for exposure less than and greater than the median respectively. In particular the increased risk was observed for welders and sheet-metal workers (OR=7.3, 95%CI=2.6-20.1); this risk was unchanged after adjustment for eye and skin colour. To further examine this risk, duration of employment was considered, in which there was a strong trend. Being employed as a welder or a sheet-metal worker for less than 20 years gave an OR of 5.7 (95%CI=1.6-19.8, n=4), whereas being employed for over 20 years increased this to 11.5 (95%CI=2.4-55.5, n=3). Unfortunately, information on recreational exposures to UV radiation was not collected, so this could not be taken into account in the analysis. However, the authors note that confounding from recreational exposure to UV radiation cannot fully explain these findings. They also suggested that the pattern of the disease among welders (electronic arc and gas) indicates that ultraviolet radiation may not be the sole occupational risk factor for ocular melanoma. Vajdic et al. (2004) examined the risk of ocular melanoma with exposure to artificial sources of ultraviolet radiation (UVR). Cases were Australian residents aged 18 to 79 years with histopathologically or clinically diagnosed melanoma originating in the choroids, ciliary body, iris or conjunctiva. For each case, three controls matched by age, gender and residence were randomly selected from the Australian electoral rolls. Overall, interviews were completed for 290 cases (138 male, 108 female). In terms of exposure assessment, information was collected on use of sun-protective wear, exposure to welding either at work or home (including a 5 metre radius), and the use of sunbeds/sunlamps/tanning booths. Odds ratios are presented for both males and females combined and were adjusted for age, gender, place of birth, measures of ocular sensitivity to the sun (eye colour, ability to tan and squinting as a child), and total personal sun exposure at 10, 20, 30 and 40 years of age. For choroidal and ciliary body melanoma, there were 246 cases and 893
18
controls used in the analysis. Of the 73 cases and 239 controls that had ever welded, exposure was shown to be weakly associated (OR=1.2, 95%CI=0.8-1.7). This excess was only present in males (OR=1.4, 95%CI=0.9-2.1). A trend with duration was evident with corresponding estimates of 0.8 (95%CI=0.4-1.4, n=15), 1.2 (95%CI=0.7-2.2, n=23) and 1.7 (95% CI=1.0-2.7, n=35) for up to 4 years, between 4 and 22 years and over 22 years respectively. Use of both arc and oxy-acetylene welding equipment was significantly associated, OR=1.6 (95%CI=1.0-2.4, n=46). Among the individuals that had ever welded, risk was non-significantly higher in subjects who did not always wear protective equipment (OR=1.7, 95%CI=0.5-5.4, n=6) and in subjects who had suffered from more than five eye burns (OR=1.6, 95%CI=0.7-3.6, n=14). Other welding exposure measures including usual daily exposure and estimated lifetime exposure, showed little evidence of being positively associated with choroids and ciliary body melanoma. Iris and conjunctival melanoma was not found to be significantly associated with welding (no results given). The authors conclude that the above results, taken together with results of other epidemiologic studies, suggest that welding does increase risk of ocular melanoma. However, they also note that while UVR is the likely causal exposure in welding, there are other possible causes including visible light and particulate or gaseous metallic fumes, but these causes are implausible for melanomas of the eye. Vajdic et al. suggest that the reason welding was not more strongly related to risk of ocular melanoma could be due to the regular use of protective eyewear. A meta-analysis previously described (Shah et al. 2005) gave results regarding ever having occupational exposure to welding. There were 1137 cases of uveal melanoma identified from five studies resulting in a significant summary OR of 2.05 (95%CI=1.20-3.51). Between the studies there was significant heterogeneity. This was found to be due to two studies that included iris melanomas as well as choroids and ciliary body melanomas, reporting higher ORs. The authors concluded that welding was a significant risk factor for the development of uveal melanoma, but due to the relatively small number of studies available, potentially under-powering the analysis, the results should be interpreted with caution. However, they note that welding could be confounded by other exposures, including asbestos and arc-welding fumes. The European rare cancer study by Lutz et al. (2005) also published results relating to occupational exposure to artificial UV radiation. It was found that exposure was associated with an elevated, but non-significant, risk of uveal melanoma (RR=1.56, 95%CI=0.91-2.66, n=19). This elevated risk was higher in women (RR=3.09, 95% CI=0.50-19.02, n=2) than men (RR=1.47 95% CI=0.84-2.58, n=17). Relative to cumulative dose, exposure below the median gave a risk of 1.52 (95% CI=0.74-3.12, n=10) and exposure above the median gave a risk of 1.60 (95% CI=0.76-3.38, n=9). In terms of country, risks were elevated for all but one, but only reached statistical significance in France (Denmark: RR=1.88, 95%CI=0.62-5.63, n=5, France: RR=4.45, 95%CI=1.17-11.58, n=7, Germany and UK: RR=0.62, 95% CI=0.18-2.10, n=3 and Sweden: RR=1.71, 95%CI=0.49-5.92, n=4). Regarding occupation, significant excesses were observed among cooks (RR=2.40, 95% CI=1.35-4.28, n=18), and, welders and sheet metal workers (RR=1.95, 95%CI=1.08-3.52, n=16). Male welders and sheet metal workers had a significantly increased risk (RR=2.18, 95% CI=1.18-4.04, n=15), whereas female welders and sheet metal workers had a reduced risk (RR=0.75, 95% CI=0.09-6.33, n=1). However, the association with male welders was no longer significant once the data from France was excluded (RR=1.22, 95%CI=0.54-2.73, n=8); France was excluded, as this was where an association was previously observed (Guenel et al. 2001). Ever working with welding resulted in a non-significant reduced risk (RR=0.94, 95%CI=0.62-1.46, n=30). The authors conclude that occupational exposure to artificial UV radiation was associated with a non-significantly increased risk of uveal melanoma. 2.3 OCCUPATION AS AN EXPOSURE
Exposure to solar radiation and artificial ultraviolet radiation can be difficult to determine and can be subject to both recall bias and problems with personal/recreational exposure. To overcome recall
19

bias the majority of studies investigate occupation as a risk factor rather than specific exposures. The following section describes study results relating to occupations that are likely to be exposed to either solar or UV radiation, including farmers, welders and medical workers. This section is included in the report for completeness and further confirms industries that are likely to be at high risk. Vågerö et al. (1990) conducted a study based on cases of malignant melanoma from the cancer registries of England and Wales and Sweden. In England and Wales registered cases of malignant melanoma occurring in subjects aged 15-64 during the period 1971-1978 were included. In total there were 3991 cases of malignant melanoma and 662 cases of ocular melanoma eligible for study. In Sweden the cases of malignant cutaneous melanoma were obtained from the Swedish Cancer Environment Registry for the period 1961-1979, and subjects born between 1896 and 1940. In total there were 5003 cases eligible for study. For the England and Wales data, age-adjusted proportional registration ratios (PRR) were calculated. For the Swedish data, standardised registration ratios (SRR) were calculated. For England and Wales, various occupations appeared to be at increased risk of cutaneous and ocular melanoma (Table 10). For Sweden, various occupations appeared to have an elevated risk of cutaneous melanoma. Combining the data from England, Wales and Sweden and for both males and females produced significantly elevated risks (Obs/Exp) for several occupations. The authors note that although ultraviolet levels external to an aircraft would be expected to be higher than at ground level, it is unlikely that airline pilots are exposed due to the shielding of the window glass. However, frequent flights abroad may give opportunities for intense recreational sun bathing, which may contribute to the elevated risks observed in this occupational group. Overall they conclude that lifestyle factors may be responsible for the consistent excess risks found, although the possibility of an occupational induced excess on small occupational groups cannot be ruled out.
20
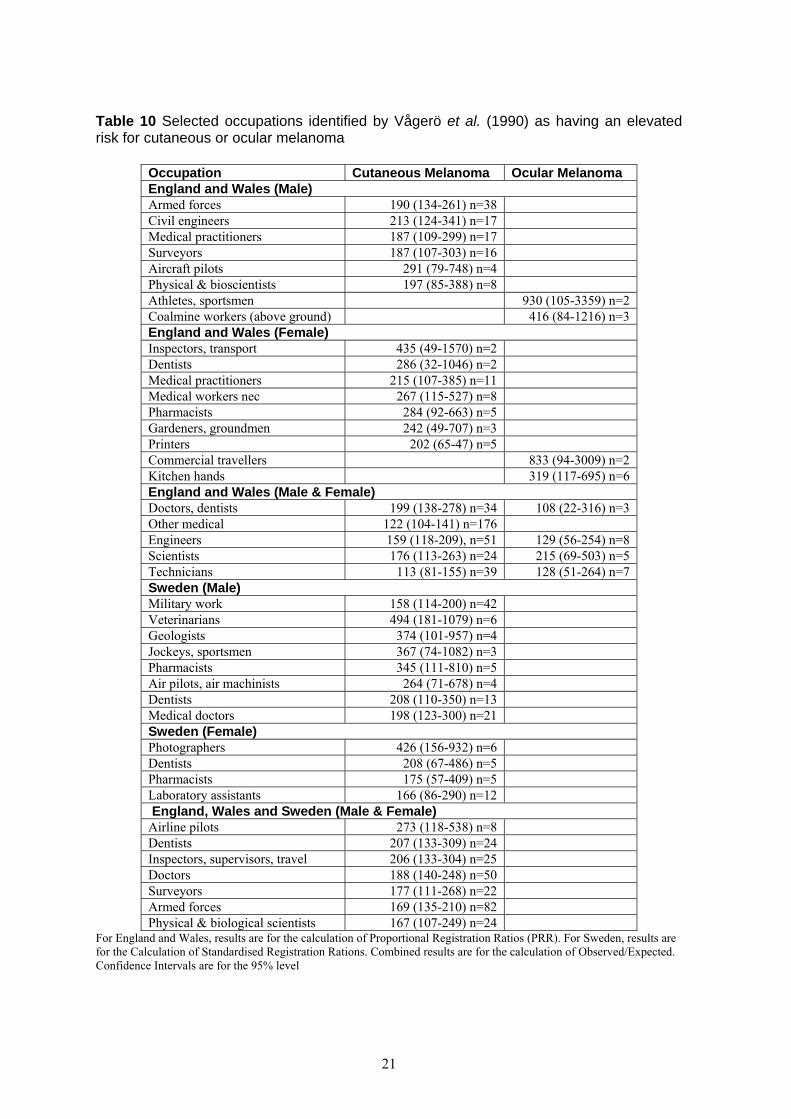
Table 10 Selected occupations identified by Vågerö et al. (1990) as having an elevated risk for cutaneous or ocular melanoma
Occupation Cutaneous Melanoma Ocular Melanoma England and Wales (Male) Armed forces 190 (134-261) n=38 Civil engineers 213 (124-341) n=17 Medical practitioners 187 (109-299) n=17 Surveyors 187 (107-303) n=16 Aircraft pilots 291 (79-748) n=4 Physical & bioscientists 197 (85-388) n=8 Athletes, sportsmen 930 (105-3359) n=2 Coalmine workers (above ground) 416 (84-1216) n=3 England and Wales (Female) Inspectors, transport 435 (49-1570) n=2 Dentists 286 (32-1046) n=2 Medical practitioners 215 (107-385) n=11 Medical workers nec 267 (115-527) n=8 Pharmacists 284 (92-663) n=5 Gardeners, groundmen 242 (49-707) n=3 Printers 202 (65-47) n=5 Commercial travellers 833 (94-3009) n=2 Kitchen hands 319 (117-695) n=6 England and Wales (Male & Female) Doctors, dentists 199 (138-278) n=34 108 (22-316) n=3 Other medical 122 (104-141) n=176 Engineers 159 (118-209), n=51 129 (56-254) n=8 Scientists 176 (113-263) n=24 215 (69-503) n=5 Technicians 113 (81-155) n=39 128 (51-264) n=7 Sweden (Male) Military work 158 (114-200) n=42 Veterinarians 494 (181-1079) n=6 Geologists 374 (101-957) n=4 Jockeys, sportsmen 367 (74-1082) n=3 Pharmacists 345 (111-810) n=5 Air pilots, air machinists 264 (71-678) n=4 Dentists 208 (110-350) n=13 Medical doctors 198 (123-300) n=21 Sweden (Female) Photographers 426 (156-932) n=6 Dentists 208 (67-486) n=5 Pharmacists 175 (57-409) n=5 Laboratory assistants 166 (86-290) n=12 England, Wales and Sweden (Male & Female) Airline pilots 273 (118-538) n=8 Dentists 207 (133-309) n=24 Inspectors, supervisors, travel 206 (133-304) n=25 Doctors 188 (140-248) n=50 Surveyors 177 (111-268) n=22 Armed forces 169 (135-210) n=82 Physical & biological scientists 167 (107-249) n=24
For England and Wales, results are for the calculation of Proportional Registration Ratios (PRR). For Sweden, results are for the Calculation of Standardised Registration Rations. Combined results are for the calculation of Observed/Expected. Confidence Intervals are for the 95% level
21
An exploratory study into occupation and risk of uveal melanoma was conducted in 1992 using population-based case-control methods (Ajani et al. 1992). Cases were drawn from the United States residents who had been diagnosed with melanoma of the choroids and/or ciliary body. Due to the histopathological differences between these two melanomas and melanoma of the iris, the latter cases were excluded from the study. Since the condition is rare among non-whites, the study was further limited to including only white individuals. Patients were enrolled between January 1984 and June 1987. However, to minimise potential recall bias and behavioural changes that may have occurred due to disease diagnosis, only those patients diagnosed in the previous year were recruited. Overall, there were 197 cases that participated in the analysis. Random-digit dialling, using telephone numbers with the same area code and first five digits as the cases, was used to select controls. Information was collected regarding ocular/medical histories, ultraviolet exposure, occupational history and work related exposure occurring up to 15 years previously. The data were coded for industries and occupations according to two different systems; the Occupation-exposure cross linkage system (OEC) and the Bureau of census classification system (BOC). OEC has three components, an occupational code, an agent list and a link between occupation and agent. BOC consists of 231 industry categories arranged into 13 major groups and 503 occupational categories arranged into 6 summary and 23 major groups. Patients and controls were compared in terms of industry and occupation by using both systems, but only the OEC system was used to study specific exposures. Odds ratios were calculated for each industry or occupation by treating all other industries/occupations as unexposed. Estimates were adjusted for age, ancestry, skin colour, moles, use of sunlamps and past income level. Non-occupational exposure to ultraviolet light was not adjusted for since this could not be separated from occupational exposures. Using the OEC system, no significantly elevated risks were observed. However, elevated risks were found in the agriculture, forestry and fishing industry (OR=2.02, 95% CI=0.61-6.73, n=6) and the metal industry (OR=4.42, 95% CI=0.71-27.40, n=6), with reduced risks in the construction industry (OR=0.49, 95% CI=0.22-1.12, n=9) and the medicine and science industry (OR=0.73, 95% CI=0.26-2.05, n=7). Similarly using the BOC system revealed no significantly elevated results. An increase in risk was observed for agriculture, forestry and fisheries (OR=1.52, 95% CI=0.38-6.06, n=4) and a decreased risk for construction (OR=0.53, 95% CI=0.21-1.31, n=8). In terms of occupation, agricultural, fishery, forestry and related occupations were elevated using both classification systems (OR=2.18, 95% CI=0.63-7.55, n=6 and OR=1.82, 95% CI=0.42-7.87, n=4, OEC and BOC respectively). Adjusted OR estimates were also calculated for self-reported exposures, including welding arc, this gave an estimate close to expected (OR=0.99, 95% CI=0.48-2.05, n=18). The authors note that exposure to ultraviolet radiation may be a plausible cause for this elevated risk associated with farming, fishing and forestry; but this cannot be confirmed using the current dataset. A population-based linked-registry was used to evaluate incidence of malignant melanoma of the skin among Swedish men by industry and occupation (Linet et al. 1995). Cancer cases were obtained from the Swedish Cancer Environment Registry for the period 1961-1979 with occupational information from the 1960 census. The Swedish male population for 1961 to 1979 was used as the reference group in the analysis. Melanoma incidence was evaluated for overall occurrence and separately for four anatomic sites (face, neck & scalp, trunk, arms and legs). Only occupations with a minimum of 500 subjects with more than three cases were analysed. In the 1960 census, the numbers of employed women was relatively small with very small incidence numbers, thus women were not included in this study. In total there were 3850 cutaneous melanoma cases identified in the 19-year follow-up. Standardised cumulative incidence ratios (SIR) were calculated for all major, general and specific industrial and occupational categories. Estimates were adjusted for age and region. In terms of major industrial categories, the only significantly elevated risks were in the manufacturing 1 industry (SIR=1.1, n=549, p<0.05) and the service industry (SIR=1.5, n=604, p<0.01). Reduced risks were observed in the farming, forestry, hunting and fishing industry (SIR=0.8, n=513, p<0.05) and the construction industry (SIR=0.9, n=390). However, the risk of
22

cutaneous melanoma on the face, neck & scalp was significantly increased among the farming, forestry, hunting and fishing industry (SIR=1.2, n=143, p<0.05); this pattern was repeated for occupation in farming, fishing, hunting and related work (All sites: SIR=0.8, n=491, p<0.05, face, neck & scalp: SIR=1.2, n=143, p<0.05). Occupation in service, sports and recreational work was significantly elevated for all sites combined (SIR=1.3, n=217, p>0.01) and elevated for each site (face, neck & scalp: SIR=1.1, n=28, trunk: SIR=1.3, n=109, p<0.01, arms: SIR=1.4, n=23, legs: SIR=1.6, n=35, p<0.05). For general and specific industries there were several significantly increased risks observed, including in graphics and publishing (SIR=1.4, n=91, p<0.01), in particularly, newspaper printing shops (SIR=1.9, n=39, p<0.01) and newspaper publishers (SIR=3.1, n=7, p<0.05). In addition, significant excesses were observed for research and scientific institutes (SIR=2.3, n=9, p<0.05), military work (SIR=1.6, n=43, p<0.01), veterinary work (SIR=4.8, n=6, p<0.01), medical and related work (SIR=2.1, n=36, p<0.01 corresponding to physician work: SIR=2.0, n=22, p<0.01 and dentistry: SIR=2.2, n=14, p<0.05) and secretarial, stenographic and typing work (SIR=2.2, n=12, p>0.05). Recreational sun exposure is given as a part explanation for the increased risk among Swedish military workers. Also noted is the significant excess of melanoma of the face, neck & scalp but no overall increase among Swedish farmers, this could suggest a possible causal role of sun exposure. A record linkage cancer incidence study was conducted on 1,577 female and 187 male cabin attendants who had worked for a Finnish airline company (Pukkala et al. 1995). Recruitment for the study started in the late 1940s with the cancer follow-up being from 1967 until 1992. Length of employment was recorded from the files of the Finnair Flight Company. A unique personal identification number given to all residents in Finland since 1967 was used to ascertain cancer incidence from the Finnish cancer registry. Standardised incidence ratios were calculated, using national cancer incidences as reference. A non-significant excess was obtained for skin melanoma (SIR=2.11, 95% CI=0.43-6.15, n=3). All of the melanoma cases were among subjects with at least two years in exposed work, and two subjects were aged 27 and 29. The authors note that the origin of these cancers was probably in the youth of these women before they started cabin crew work. Holly et al. (1996) conducted a case-control study in the Western United States to determine the relationship between occupations (or chemical exposures) and the risk of uveal melanoma. In total there were 221 white male cases and 447 white male controls, obtained as described in the earlier study (Holly et al. 1990). Occupations were coded according to the Alphabetical Index of Industries and Occupations for the six jobs each individual held the longest, thus individuals could appear in more than one occupational group. In the analysis an unadjusted estimate and an estimate adjusted for age, number of large nevi, eye colour and tanning/burning response to 30-minute summer noonday sun exposure was calculated. Significantly elevated risks were found for four main occupation groups (Table 11). Other occupational groups were also found to be at increased risk. Risk estimates were elevated for each stratum for duration of work in years and latency (length of employment until diagnosis), adjusted for age only. However, significance was only reached in the highest strata. The authors conclude that intense UV light exposure to the eye is associated with an increased risk of uveal melanoma. They state that welders and sailors are exposed to intense UV light, sailors particularly since strong UV light is reflected off the surface of the water. Referral bias is offered as an explanation why health occupations have an elevated risk, since few of the subjects in this group were employed in jobs involving unusual sources of UV light exposure (germicidal and photochemical lamps). However, the authors did not collect specific information on the use of intense lighting in laboratories or clinical settings. In addition, the authors point out that both cases and controls were of similar educational background; therefore, it is unlikely that education was a confounder of the noted associations with occupational groups.
23
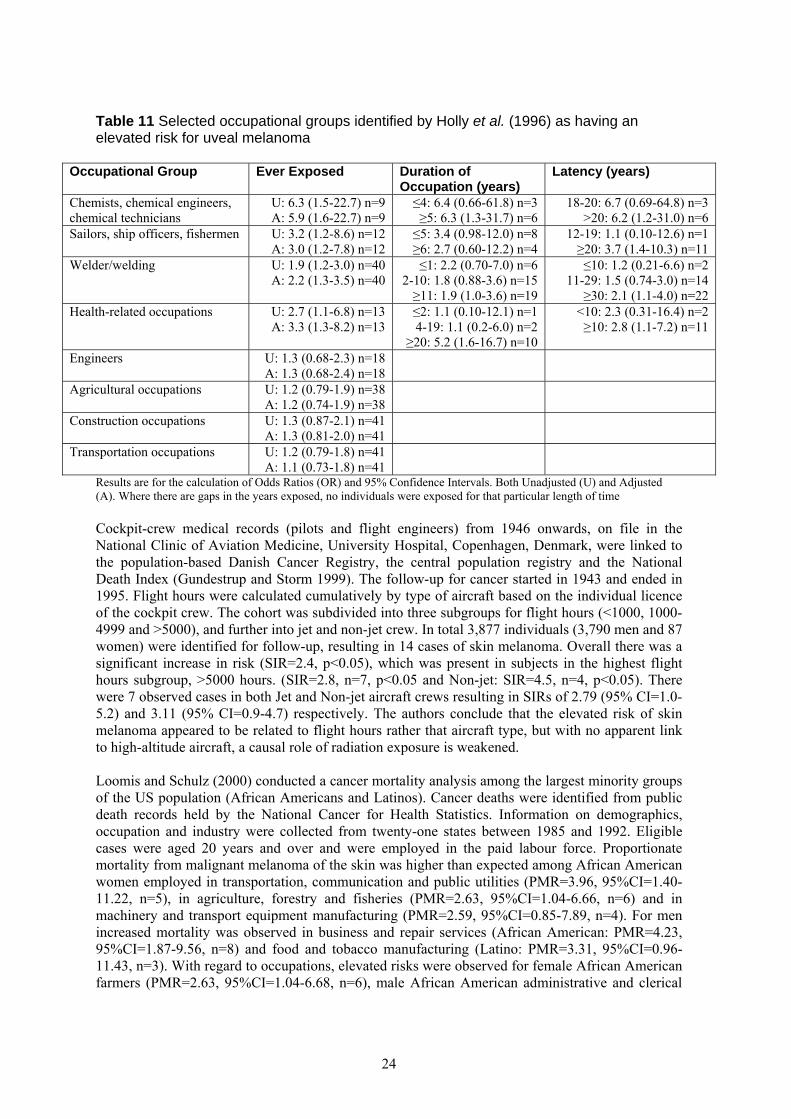
Table 11 Selected occupational groups identified by Holly et al. (1996) as having an elevated risk for uveal melanoma
Occupational Group Ever Exposed Duration of Occupation (years)
Latency (years)
Chemists, chemical engineers, chemical technicians
U: 6.3 (1.5-22.7) n=9 A: 5.9 (1.6-22.7) n=9
≤4: 6.4 (0.66-61.8) n=3 ≥5: 6.3 (1.3-31.7) n=6
18-20: 6.7 (0.69-64.8) n=3 >20: 6.2 (1.2-31.0) n=6
Sailors, ship officers, fishermen U: 3.2 (1.2-8.6) n=12 A: 3.0 (1.2-7.8) n=12
≤5: 3.4 (0.98-12.0) n=8 ≥6: 2.7 (0.60-12.2) n=4
12-19: 1.1 (0.10-12.6) n=1 ≥20: 3.7 (1.4-10.3) n=11
Welder/welding U: 1.9 (1.2-3.0) n=40 A: 2.2 (1.3-3.5) n=40
≤1: 2.2 (0.70-7.0) n=6 2-10: 1.8 (0.88-3.6) n=15 ≥11: 1.9 (1.0-3.6) n=19
≤10: 1.2 (0.21-6.6) n=2 11-29: 1.5 (0.74-3.0) n=14
≥30: 2.1 (1.1-4.0) n=22 Health-related occupations U: 2.7 (1.1-6.8) n=13
A: 3.3 (1.3-8.2) n=13 ≤2: 1.1 (0.10-12.1) n=1 4-19: 1.1 (0.2-6.0) n=2
≥20: 5.2 (1.6-16.7) n=10
<10: 2.3 (0.31-16.4) n=2 ≥10: 2.8 (1.1-7.2) n=11
Engineers U: 1.3 (0.68-2.3) n=18 A: 1.3 (0.68-2.4) n=18
Agricultural occupations U: 1.2 (0.79-1.9) n=38 A: 1.2 (0.74-1.9) n=38
Construction occupations U: 1.3 (0.87-2.1) n=41 A: 1.3 (0.81-2.0) n=41
Transportation occupations U: 1.2 (0.79-1.8) n=41 A: 1.1 (0.73-1.8) n=41
Results are for the calculation of Odds Ratios (OR) and 95% Confidence Intervals. Both Unadjusted (U) and Adjusted (A). Where there are gaps in the years exposed, no individuals were exposed for that particular length of time Cockpit-crew medical records (pilots and flight engineers) from 1946 onwards, on file in the National Clinic of Aviation Medicine, University Hospital, Copenhagen, Denmark, were linked to the population-based Danish Cancer Registry, the central population registry and the National Death Index (Gundestrup and Storm 1999). The follow-up for cancer started in 1943 and ended in 1995. Flight hours were calculated cumulatively by type of aircraft based on the individual licence of the cockpit crew. The cohort was subdivided into three subgroups for flight hours (<1000, 1000-4999 and >5000), and further into jet and non-jet crew. In total 3,877 individuals (3,790 men and 87 women) were identified for follow-up, resulting in 14 cases of skin melanoma. Overall there was a significant increase in risk (SIR=2.4, p<0.05), which was present in subjects in the highest flight hours subgroup, >5000 hours. (SIR=2.8, n=7, p<0.05 and Non-jet: SIR=4.5, n=4, p<0.05). There were 7 observed cases in both Jet and Non-jet aircraft crews resulting in SIRs of 2.79 (95% CI=1.0-5.2) and 3.11 (95% CI=0.9-4.7) respectively. The authors conclude that the elevated risk of skin melanoma appeared to be related to flight hours rather that aircraft type, but with no apparent link to high-altitude aircraft, a causal role of radiation exposure is weakened. Loomis and Schulz (2000) conducted a cancer mortality analysis among the largest minority groups of the US population (African Americans and Latinos). Cancer deaths were identified from public death records held by the National Cancer for Health Statistics. Information on demographics, occupation and industry were collected from twenty-one states between 1985 and 1992. Eligible cases were aged 20 years and over and were employed in the paid labour force. Proportionate mortality from malignant melanoma of the skin was higher than expected among African American women employed in transportation, communication and public utilities (PMR=3.96, 95%CI=1.40-11.22, n=5), in agriculture, forestry and fisheries (PMR=2.63, 95%CI=1.04-6.66, n=6) and in machinery and transport equipment manufacturing (PMR=2.59, 95%CI=0.85-7.89, n=4). For men increased mortality was observed in business and repair services (African American: PMR=4.23, 95%CI=1.87-9.56, n=8) and food and tobacco manufacturing (Latino: PMR=3.31, 95%CI=0.96-11.43, n=3). With regard to occupations, elevated risks were observed for female African American farmers (PMR=2.63, 95%CI=1.04-6.68, n=6), male African American administrative and clerical
24
workers (PMR=2.76, 95%CI=1.11-6.86, n=6), Latino women employed in sales (PMR=2.26, 95%CI=0.60-8.51, n=3) and Latino males in the construction trade (PMR=2.05, 95%CI=0.77-5.43, n=5). Estimates were adjusted for age using all industries/ occupations within the same ethnic origin as the referent. A retrospective cohort study was conducted in order to describe the cancer pattern of commercial pilots using follow-up through the Icelandic Cancer Registry (Rafnsson et al. 2000). The cohort comprised of 458 men who were all licensed commercial pilots in Iceland according to the computerised files from the Icelandic Aviation Authority. Of these, 265 pilots had ever been employed by Icelandair, the study is primarily restricted to these individuals. For all employees after 1985 there was information on the type of aeroplane and number of block hours flown each year. The personal identification number of each individual was used for linkage to the National Registry and the Icelandic Cancer Registry. Follow-up started in 1955 and ended in 1997 with a time lag of 5 years. The reference group used was the male population of Iceland. The cohort was divided into three subgroups according to accumulated block hours (<5000, 5000-9999 and 10000+). Among the whole cohort (458 pilots) there were 5 observed cases of malignant melanoma of the skin resulting in a significantly increased SIR estimate of 10.20 (95%CI=3.29-23.81) and 1 case of eye cancer, which was also subsequently found to be malignant melanoma (SIR=10.00, 95%CI=0.13-55.64). These six cases all occurred in the smaller sub-cohort (malignant melanoma of the skin: SIR=15.63, 95% CI=5.04-36.46 and eye cancer: SIR=14.29, 95%CI=0.19-79.48). According to accumulated dose in the Icelandair pilots, there was significantly increased risk at 5000-9999 hours (SIR=40.00, 95%CI=4.49-144.42, n=2) and over 10000 hours (SIR=13.04, 95%CI=2.62-38.11, n=3). The same cohort was also at significant risk for exposure to cosmic radiation of 3-9.9mSv (SIR66.67, 95%CI=7.49-240.70, n=2) and over 20mSv (SIR=28.57, 95%CI=3.21-103.16, n=2), as well as having an elevated risk for 10-19.9mSv (SIR=33.33, 95%CI=0.44-185.46, n=1). The authors note that the risks found in this study are remarkably high compared to other studies and no conclusions can be drawn with respect to the role of cosmic radiation, number of bloc-hours flown and lifestyle factors (such as recreational sun exposure). Pukkala et al. (2002) studied the incidence of cancer among Nordic airline pilots, specifically focusing on the relation to cosmic radiation. National cohorts of airline pilots were identified from registers in Denmark, Finland, Iceland, Norway and Sweden. In Denmark all members of commercial cockpit crews on file since 1946 in the National Clinic of Aviation Medicine were enrolled (3,790 men), along with 793 male pilots from Finland flying for Finnair up to 1996, 239 men who were commercial pilots in Iceland. In Norway there were 3,752 male commercial pilots who held a valid licence between January 1946 and February 1994, in Sweden there were 1,478 male aircraft pilots of the Scandinavian Airline System employed between 1957 and 1994. This cohort overlaps with the cohorts of Gundestrup et al. (1999) and Rafnsson et al. (2000). The cohorts were linked to the national population registers and cancer registries. The cancer follow-up period varied for each country (Denmark: 1943-1996, Finland: 1953-1997, Iceland: 1984-1997, Norway: 1962-1996 and Sweden: 1961-1996). The flight histories of the pilots before the cancer follow-up period were also taken into account when evaluating exposure to radiation. National cancer rates were used for reference. In total there were 10,032 men followed up, from which 56 cases of skin melanoma (7 head and neck, 32 trunk and 14 limbs) were observed. There was significant excess for malignant melanoma (SIR=2.29, 95% CI=1.73-2.98), which was evident in all three anatomic sites (head and neck: SIR=2.49, 95%CI=1.00-5.14, trunk: SIR=2.33, 95% CI=1.60-3.30 and limbs: SIR=2.29, 95%CI=1.25-3.84). The risk increased significantly with increasing estimated exposure to radiation during flight (p=0.008) with SIRs of 1.37 for 1-2999μSv (95%CI=0.75-2.30, n=14), 3.00 for 3000-9999μSv (95%CI=1.37-5.69, n=9), 3.02 for 10000-19999μSv (95%CI=1.61-5.14, n=13) and 3.47 for 20000+μSv (95%CI=2.02-5.55, n=17). This trend was also significant in the trunk (p=0.02) and limbs (p=0.04). Using an internal reference (exposure of 1-2999μSv) and adjusting for age and calendar period gave a significant trend (p=0.007). The resulting SIRs were 2.10 (95%CI=0.91-4.87), 2.20 (95%CI=1.03-4.72) and 2.78
25

(95%CI=1.30-5.93) for 3000-9999μSv, 10000-19999μSv and 20000+μSv respectively. The authors found that the risk of melanoma decreased with recent calendar periods suggesting that sunbathing is a major determinant of risk. However, they conclude that some influence on the observed excess of melanoma from cosmic (and ultraviolet) radiation cannot be entirely excluded. A project evaluating the cancer incidence among Association of Flight Attendants members residing in California was published in 2002 (Reynolds et al. 2002). Data from over 49,000 members at 27 airlines were linked to the California Cancer Registry in the period 1988 through 1995. California statewide incidence rates were used to calculate SIRs for two reference groups; all races combined and non-Hispanic whites. Estimates were adjusted for age and presented separately by gender. For both men and women the second most common cancer was found to be malignant melanoma of the skin (n=3 and 12), resulting in elevated estimates for all four subgroups. Males had the highest risk for both reference groups (SIR=3.93, 95% CI=0.74-11.62 using all males as reference and SIR=2.74, 95% CI=0.52-8.12 using non-Hispanic whites as reference); in contrast females were at lower risk (SIR=2.50, 95%CI=1.28-4.38 and SIR=1.83, 95%CI=0.94-3.21 for the two reference groups respectively). A race-adjusted PIR of 3.16 (95% CI=0.60-9.35) was observed. The risk of cutaneous melanoma was significantly elevated for women flying domestic routes (n=11) using non-Hispanic white females (SIR=2.55, 95%CI=1.27-4.58) and all white females (SIR=3.53, 95%CI=1.75-6.34) as reference. Results were significantly increased for males but these were based on only three cases, the SIR compared to non-Hispanic white males was 6.99 (95%CI=1.32-20.70) and compared to all males was 10.28 (95%CI=1.94-30.42). The authors conclude that flight attendants experience higher rates of malignant melanoma of the skin although no direct exposure data was available and lifestyle differences could be a contributory factor. A pooled analysis based on two case-referent studies, (one hospital-based the other population-based), was conducted in Germany between 1995 and 1998, to explore occupational risks and their link to uveal melanoma (Monarrez-Espino et al. 2002). The population-based case-referent study was the German cohort from the European study by Lutz et al. (2005). Cases (n=37) were patients diagnosed with uveal melanoma (located in the choroids or ciliary body) between July 1995 and December 1997, aged between 35 and 69 years and residing in one of five geographic regions (Hamburg, Bremen, Essen, Saarbrücken and Saarland). Referents (n=327) were randomly selected from mandatory lists of residence and matched to cases by gender and region of residence. For the hospital-based case referent study, cases (n=81) were patients diagnosed with uveal melanoma between December 1996 and March 1998, aged between 35 and 74 years and were residents of North Rhine-Westphalia. Referents (n=148) were patients with newly diagnosed benign disease of the posterior eye segment visiting the eye clinic during the same period as the cases. All referents had not suffered from occupational accidents involving the eye, and were matched to cases by age, gender and region of residency. Both studies included the city of Essen, therefore, for the overlapping period (December 1996 to December 1997) cases from the hospital-based case-referent study were used. Lifetime occupation history was used to evaluate exposure. All jobs that were held by an individual for at least 6 months were chronologically recorded along with a “main task”. This “main task” was classified into 34 ‘job groups’ according to the International Standard Classification of Occupations (ISCO) and also into 36 “industrial branches” according to the General Industrial Classification of Economic Activities within the European Communities (NACE). Further to these two classification systems, a job specific questionnaire classification (JSQ) was determined based on occupational category. For all three classifications, an unadjusted estimate and an estimate adjusted for age and region of residence was calculated (Table 12). The occupational groups that included welders did not show positive associations with uveal melanoma. However, an elevated risk was observed for “ever having welded” (OR=1.3, 95%CI=0.6-2.5). The authors note that the study is limited since occupation title was used as a surrogate for exposure, and the small numbers of cases and pooling of occupation may be responsible for the lack of statistical significance.
26
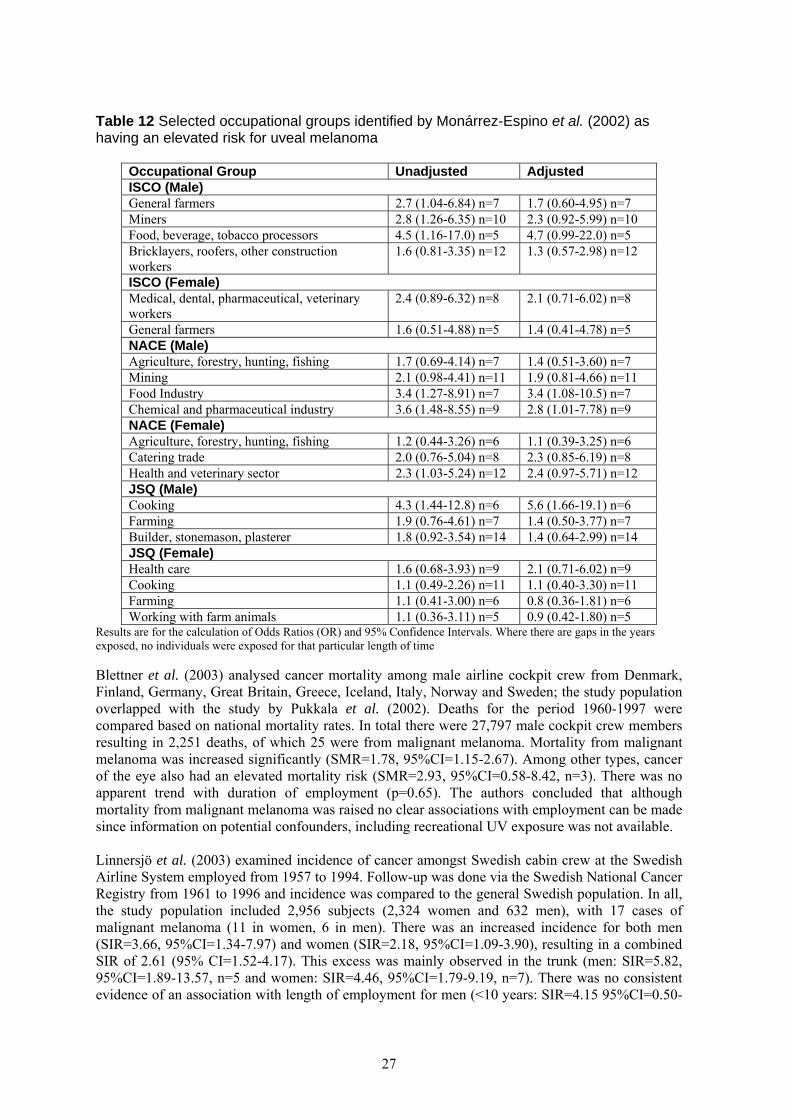
Table 12 Selected occupational groups identified by Monárrez-Espino et al. (2002) as having an elevated risk for uveal melanoma
Occupational Group Unadjusted Adjusted ISCO (Male) General farmers 2.7 (1.04-6.84) n=7 1.7 (0.60-4.95) n=7 Miners 2.8 (1.26-6.35) n=10 2.3 (0.92-5.99) n=10 Food, beverage, tobacco processors 4.5 (1.16-17.0) n=5 4.7 (0.99-22.0) n=5 Bricklayers, roofers, other construction workers
1.6 (0.81-3.35) n=12 1.3 (0.57-2.98) n=12
ISCO (Female) Medical, dental, pharmaceutical, veterinary workers
2.4 (0.89-6.32) n=8 2.1 (0.71-6.02) n=8
General farmers 1.6 (0.51-4.88) n=5 1.4 (0.41-4.78) n=5 NACE (Male) Agriculture, forestry, hunting, fishing 1.7 (0.69-4.14) n=7 1.4 (0.51-3.60) n=7 Mining 2.1 (0.98-4.41) n=11 1.9 (0.81-4.66) n=11 Food Industry 3.4 (1.27-8.91) n=7 3.4 (1.08-10.5) n=7 Chemical and pharmaceutical industry 3.6 (1.48-8.55) n=9 2.8 (1.01-7.78) n=9 NACE (Female) Agriculture, forestry, hunting, fishing 1.2 (0.44-3.26) n=6 1.1 (0.39-3.25) n=6 Catering trade 2.0 (0.76-5.04) n=8 2.3 (0.85-6.19) n=8 Health and veterinary sector 2.3 (1.03-5.24) n=12 2.4 (0.97-5.71) n=12 JSQ (Male) Cooking 4.3 (1.44-12.8) n=6 5.6 (1.66-19.1) n=6 Farming 1.9 (0.76-4.61) n=7 1.4 (0.50-3.77) n=7 Builder, stonemason, plasterer 1.8 (0.92-3.54) n=14 1.4 (0.64-2.99) n=14 JSQ (Female) Health care 1.6 (0.68-3.93) n=9 2.1 (0.71-6.02) n=9 Cooking 1.1 (0.49-2.26) n=11 1.1 (0.40-3.30) n=11 Farming 1.1 (0.41-3.00) n=6 0.8 (0.36-1.81) n=6 Working with farm animals 1.1 (0.36-3.11) n=5 0.9 (0.42-1.80) n=5
Results are for the calculation of Odds Ratios (OR) and 95% Confidence Intervals. Where there are gaps in the years exposed, no individuals were exposed for that particular length of time Blettner et al. (2003) analysed cancer mortality among male airline cockpit crew from Denmark, Finland, Germany, Great Britain, Greece, Iceland, Italy, Norway and Sweden; the study population overlapped with the study by Pukkala et al. (2002). Deaths for the period 1960-1997 were compared based on national mortality rates. In total there were 27,797 male cockpit crew members resulting in 2,251 deaths, of which 25 were from malignant melanoma. Mortality from malignant melanoma was increased significantly (SMR=1.78, 95%CI=1.15-2.67). Among other types, cancer of the eye also had an elevated mortality risk (SMR=2.93, 95%CI=0.58-8.42, n=3). There was no apparent trend with duration of employment (p=0.65). The authors concluded that although mortality from malignant melanoma was raised no clear associations with employment can be made since information on potential confounders, including recreational UV exposure was not available. Linnersjö et al. (2003) examined incidence of cancer amongst Swedish cabin crew at the Swedish Airline System employed from 1957 to 1994. Follow-up was done via the Swedish National Cancer Registry from 1961 to 1996 and incidence was compared to the general Swedish population. In all, the study population included 2,956 subjects (2,324 women and 632 men), with 17 cases of malignant melanoma (11 in women, 6 in men). There was an increased incidence for both men (SIR=3.66, 95%CI=1.34-7.97) and women (SIR=2.18, 95%CI=1.09-3.90), resulting in a combined SIR of 2.61 (95% CI=1.52-4.17). This excess was mainly observed in the trunk (men: SIR=5.82, 95%CI=1.89-13.57, n=5 and women: SIR=4.46, 95%CI=1.79-9.19, n=7). There was no consistent evidence of an association with length of employment for men (<10 years: SIR=4.15 95%CI=0.50-
27
14.98, n=2, 10-19 years: SIR=6.59, 95%CI=1.36-19.25, n=3 and >20 years: SIR=1.59, 95%CI=0.04-8.86, n=1) or women (<10 years: SIR=2.45, 95%CI=0.90-5.33, n=6, 10-19 years: SIR=1.08, 95% CI=0.13-3.89, n=2 and >20 years: SIR=4.60, 95%CI=0.95-13.44, n=3). In relation to flight hours over 10000, a risk specifically for men could not be calculated since there were no exposed controls. However, for women and all cabin crew combined, elevated risks were found (OR=2.67, 95%CI=0.20-35.14, n=2 and OR=4.67, 95%CI=0.45-49.14, n=5 respectively). The study concluded that there was a real increased risk of malignant melanoma among Swedish cabin crew, both men and women, but the causes remain unclear and could be due to occupational and non-occupational causes. The authors note that the windshields of aircraft give good protection against UV radiation thus cabin attendants should not have an increase in exposure. Male workers employed in 1970 and living in Sweden in 1960 were followed for cutaneous melanoma from 1971 to 1989 using the Swedish Registers of Death and Cancer (Perez-Gomez et al. 2004). Subjects were aged between 25 and 64 years at the beginning of the follow-up. In total there were 1,890,497 men included in the study. Of these, a sub-cohort of 755,728 men, who had the same occupation in both the 1960 and 1970 censuses, were analysed separately. SIR estimates were age adjusted and RR estimates were adjusted for age, period, town size and geographical area, using the whole male cohort for reference. Each occupation was compared only with other occupations within the same occupational sector. Only occupations with a minimum of five cases and an RR>1.5 (RR>2 for site specific using the whole cohort) were reported. In the whole cohort a total of 6,187 cases of cutaneous melanoma were found with 2,816 occurring in the sub-cohort. In the cohort as a whole, significant risks were observed in several occupations, including, dentists (SIR=197, RR=1.50, 95%CI=1.02-2.21, n=26), well drillers and diamond drillers (SIR=154, RR=3.64, 95%CI=1.35-9.82, n=6) and typographers and lithographers (SIR=129, RR=1.40, 95%CI=1.10-1.78, n=69). Dentists and typographers continued to be at elevated risk in the sub-cohort (SIR=222, RR=1.55, 95%CI=1.01-2.37, n=22 and SIR=136, RR=1.37, 95%CI=1.03-1.81, n=52, respectively), as well as physiotherapists & occupational therapists (SIR=571, RR=4.21, 95% CI=1.58-11.26, n=4). Chemists had an increased risk of melanoma occurring on the head and neck (SIR=460, RR=4.21, 95%CI=1.72-10.27, n=5), whereas veterinarians, dentists and well/diamond drillers had an increased risk at the thorax site (SIR=472, RR=3.87, 95%CI=1.73-8.64, n=6, SIR=251, RR=1.95, 95%CI=1.20-3.15, n=17 and SIR=199, RR=5.13, 95%CI=1.42-18.54, n=4, respectively). Significantly elevated risk of melanoma on the lower limbs was observed for forestry managers and supervisors (SIR=195, RR=3.07, 95%CI=1.16-8.15, n=5) and aircraft pilots, navigators and flight engineers (SIR=749, RR=7.45, 95%CI=2.28-24.27, n=3). Typographers and lithographers had significantly increased risks for two sites: the thorax (SIR=136, RR=1.45, 95%CI=1.04-2.02, n=37) and upper limbs (SIR=193, RR=2.35, 95%CI=1.34-4.15, n=13). The authors note that holiday travel and leisure time activities cannot account for the variation in risk between occupations and sites. The study concludes that the high incidence observed in some occupations, particularly dentists, printers/lithographers, supports the aetiological role of occupational artificial sources of UV radiation of their effect is presumed not to be restricted to exposed sites. Pérez-Gómez et al. (2005) also conducted a study on Swedish women, using the same inclusion criteria as that used for Swedish men (Perez-Gomez et al. 2004). The cohort included 1,101,669 women, of which 245,921 had the same occupation recorded in the 1960 and 1970 censuses. RR estimates were adjusted for age, period, town size and geographical area, using the whole female cohort for reference. Each occupation was compared firstly with the whole female working population then with other occupations within the same occupational sector. Only occupations with a minimum of three cases and an RR>1.5 (RR>2 for site specific) were reported. In the whole cohort a total of 3,598 cases of cutaneous melanoma were discovered, with 875 occurring in the sub-cohort. There was a consistent increase in risk found among horticultural workers in the complete cohort (all females: RR=1.60, 95%CI=1.11-2.29; within sector: RR=1.73, 95%CI=1.10-2.74, n=30), which was mainly observed in the thorax (all females: RR=2.03, 95%CI=1.01-4.09;
28

within sector: RR=1.98, 95%CI=0.78-5.02, n=8) and lower limbs (all females: RR=1.79, 95%CI=1.01-3.16; within sector: RR=2.78, 95%CI=1.36-5.65, n=12). Significantly elevated risks were also observed for dental nurses (all females: RR=1.71, 95%CI=1.21-2.42; within sector: RR=1.57, 95%CI=1.10-2.23, n=32), particularly in the lower limbs (all females: RR=2.60, 95% CI=1.65-4.09; within sector: RR=2.40, 95%CI=1.51-3.82, n=19). In the sub-cohort excesses were observed among hatmakers and milliners, packers and nursemaids. The authors note that a result of interest is that of an increased risk among bank tellers (all females: RR=1.84, 95%CI=1.19-2.86; within sector: RR=1.68, 95%CI=1.08-2.63, n=20), which reflects an excess risk in the upper limbs (all females: RR=3.23, 95%CI=1.45-7.22; within sector: RR=2.68, 95%CI=1.18-6.10, n=6). This may be due to the use of ultraviolet A to verify signatures and the result could suggest a local effect of such radiation, however, in male bank tellers the excess was mainly due to thorax cases.
29
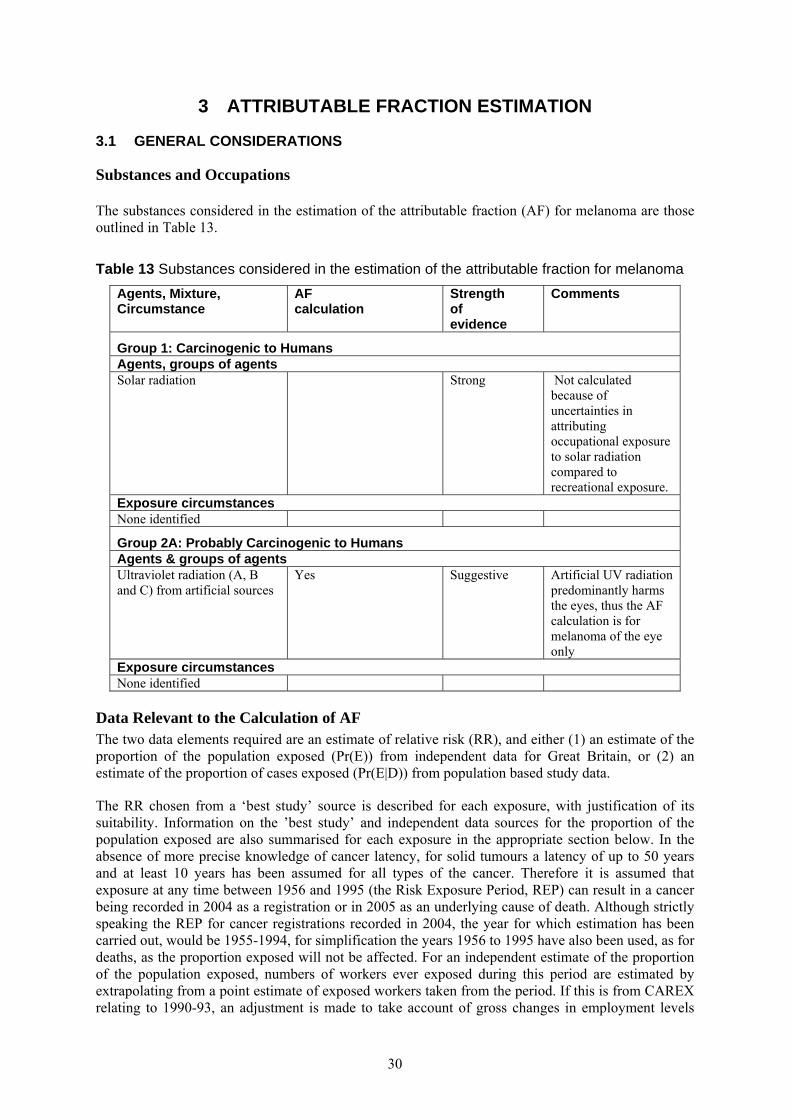
3 ATTRIBUTABLE FRACTION ESTIMATION
3.1 GENERAL CONSIDERATIONS
Substances and Occupations The substances considered in the estimation of the attributable fraction (AF) for melanoma are those outlined in Table 13.
Table 13 Substances considered in the estimation of the attributable fraction for melanoma Agents, Mixture, Circumstance
AF calculation
Strength of evidence
Comments
Group 1: Carcinogenic to Humans Agents, groups of agents Solar radiation Strong Not calculated
because of uncertainties in attributing occupational exposure to solar radiation compared to recreational exposure.
Exposure circumstances None identified
Group 2A: Probably Carcinogenic to Humans Agents & groups of agents Ultraviolet radiation (A, B and C) from artificial sources
Yes Suggestive Artificial UV radiation predominantly harms the eyes, thus the AF calculation is for melanoma of the eye only
Exposure circumstances None identified
Data Relevant to the Calculation of AF The two data elements required are an estimate of relative risk (RR), and either (1) an estimate of the proportion of the population exposed (Pr(E)) from independent data for Great Britain, or (2) an estimate of the proportion of cases exposed (Pr(E|D)) from population based study data.
The RR chosen from a ‘best study’ source is described for each exposure, with justification of its suitability. Information on the ’best study’ and independent data sources for the proportion of the population exposed are also summarised for each exposure in the appropriate section below. In the absence of more precise knowledge of cancer latency, for solid tumours a latency of up to 50 years and at least 10 years has been assumed for all types of the cancer. Therefore it is assumed that exposure at any time between 1956 and 1995 (the Risk Exposure Period, REP) can result in a cancer being recorded in 2004 as a registration or in 2005 as an underlying cause of death. Although strictly speaking the REP for cancer registrations recorded in 2004, the year for which estimation has been carried out, would be 1955-1994, for simplification the years 1956 to 1995 have also been used, as for deaths, as the proportion exposed will not be affected. For an independent estimate of the proportion of the population exposed, numbers of workers ever exposed during this period are estimated by extrapolating from a point estimate of exposed workers taken from the period. If this is from CAREX relating to 1990-93, an adjustment is made to take account of gross changes in employment levels
30
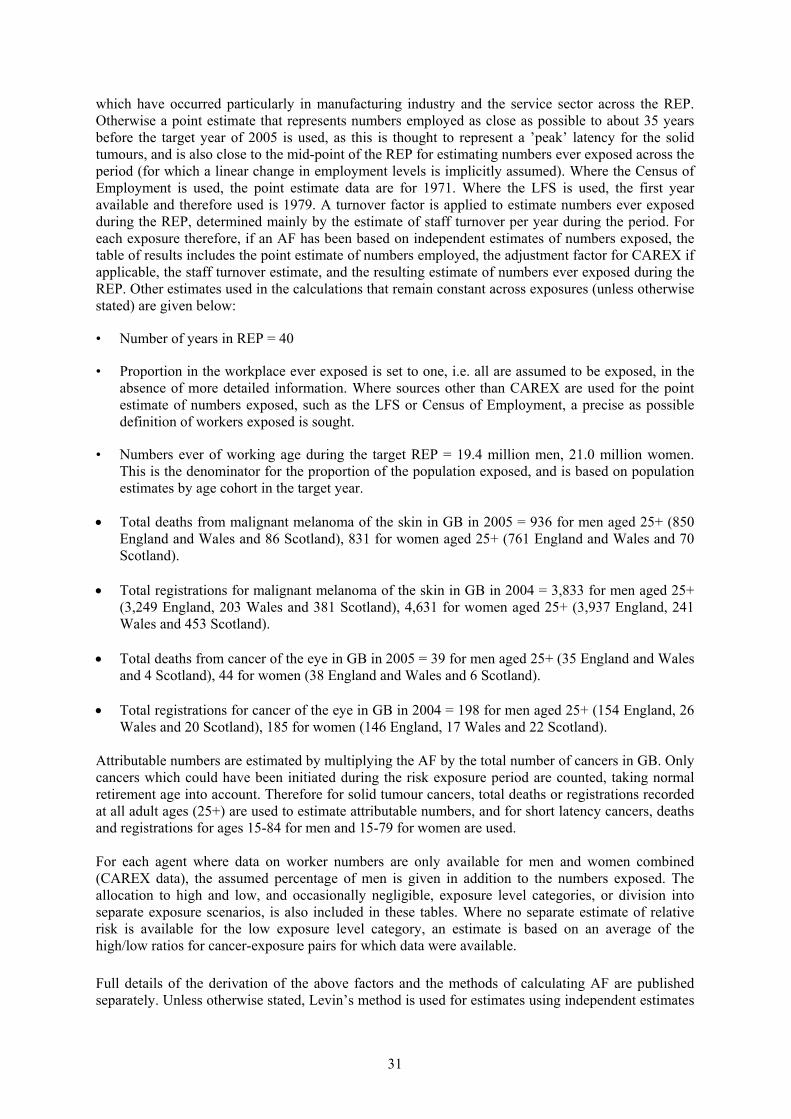
which have occurred particularly in manufacturing industry and the service sector across the REP. Otherwise a point estimate that represents numbers employed as close as possible to about 35 years before the target year of 2005 is used, as this is thought to represent a ’peak’ latency for the solid tumours, and is also close to the mid-point of the REP for estimating numbers ever exposed across the period (for which a linear change in employment levels is implicitly assumed). Where the Census of Employment is used, the point estimate data are for 1971. Where the LFS is used, the first year available and therefore used is 1979. A turnover factor is applied to estimate numbers ever exposed during the REP, determined mainly by the estimate of staff turnover per year during the period. For each exposure therefore, if an AF has been based on independent estimates of numbers exposed, the table of results includes the point estimate of numbers employed, the adjustment factor for CAREX if applicable, the staff turnover estimate, and the resulting estimate of numbers ever exposed during the REP. Other estimates used in the calculations that remain constant across exposures (unless otherwise stated) are given below:
• Number of years in REP = 40
• Proportion in the workplace ever exposed is set to one, i.e. all are assumed to be exposed, in the absence of more detailed information. Where sources other than CAREX are used for the point estimate of numbers exposed, such as the LFS or Census of Employment, a precise as possible definition of workers exposed is sought.
• Numbers ever of working age during the target REP = 19.4 million men, 21.0 million women. This is the denominator for the proportion of the population exposed, and is based on population estimates by age cohort in the target year.
• Total deaths from malignant melanoma of the skin in GB in 2005 = 936 for men aged 25+ (850 England and Wales and 86 Scotland), 831 for women aged 25+ (761 England and Wales and 70 Scotland).
• Total registrations for malignant melanoma of the skin in GB in 2004 = 3,833 for men aged 25+
(3,249 England, 203 Wales and 381 Scotland), 4,631 for women aged 25+ (3,937 England, 241 Wales and 453 Scotland).
• Total deaths from cancer of the eye in GB in 2005 = 39 for men aged 25+ (35 England and Wales
and 4 Scotland), 44 for women (38 England and Wales and 6 Scotland). • Total registrations for cancer of the eye in GB in 2004 = 198 for men aged 25+ (154 England, 26
Wales and 20 Scotland), 185 for women (146 England, 17 Wales and 22 Scotland). Attributable numbers are estimated by multiplying the AF by the total number of cancers in GB. Only cancers which could have been initiated during the risk exposure period are counted, taking normal retirement age into account. Therefore for solid tumour cancers, total deaths or registrations recorded at all adult ages (25+) are used to estimate attributable numbers, and for short latency cancers, deaths and registrations for ages 15-84 for men and 15-79 for women are used. For each agent where data on worker numbers are only available for men and women combined (CAREX data), the assumed percentage of men is given in addition to the numbers exposed. The allocation to high and low, and occasionally negligible, exposure level categories, or division into separate exposure scenarios, is also included in these tables. Where no separate estimate of relative risk is available for the low exposure level category, an estimate is based on an average of the high/low ratios for cancer-exposure pairs for which data were available. Full details of the derivation of the above factors and the methods of calculating AF are published separately. Unless otherwise stated, Levin’s method is used for estimates using independent estimates
31

of numbers exposed, and Miettinen’s method is used for study based estimates. A summary of the methodology is given in the Statistical Appendix.
3.2 SOLAR RADIATION
(a) Risk Estimate: The risk for malignant melanoma caused by occupational exposure to solar radiation is difficult to estimate because everyone at some time in their life is exposed to sunlight at a greater or lesser degree depending on residential location and leisure time activities. Epidemiological studies have used various methods, if any at all, to adjust risk estimated for non-occupational solar exposure. Typically, residential location is used as a surrogate for recreational sunlight exposure. There is uncertainty regarding the nature of how malignant melanoma develops regarding type of solar exposure (frequent or intermittent) and the relationship with potential co-factors such as age, gender and social class. Occupational exposure to solar radiation is usually measured via exposure categorisation (recreational or occupational) or job categorisation (indoor or outdoor). Outdoor work has been associated with an elevated risk of malignant melanoma (Goodman et al. 1995; Puntoni et al. 2005; Garland et al. 1990). However, due to difficulties in classifying solar exposure as occupational or recreational, and thus being treated as a single exposure, there have been negative associations found (Elwood and Jopson 1997; Gandini et al. 2005; Vagero et al. 1986). A consistently elevated risk has been observed for farmers (Cerhan et al. 1998; Settimi et al. 1999; Freedman et al. 1997) and veterinarians (Miller and, Beaumont 1995; Travier et al. 2003). The risk of melanoma of the skin is uncertain because of the difficulty in separating occupational exposure from recreational exposure. The Northern European studies summarised in Table 14 show studies reporting positive and negative associations. Consequently no estimate of occupational melanoma attributable to solar radiation was carried out.
32
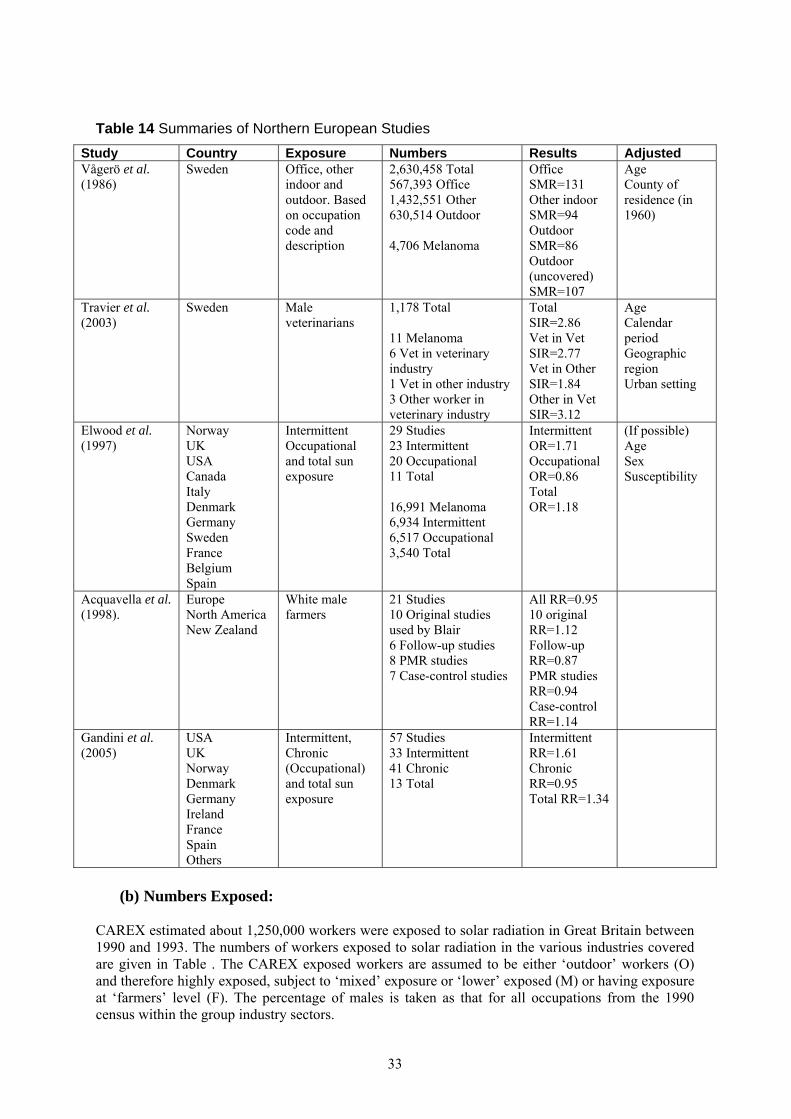
Table 14 Summaries of Northern European Studies Study Country Exposure Numbers Results Adjusted Vågerö et al. (1986)
Sweden Office, other indoor and outdoor. Based on occupation code and description
2,630,458 Total 567,393 Office 1,432,551 Other 630,514 Outdoor 4,706 Melanoma
Office SMR=131 Other indoor SMR=94 Outdoor SMR=86 Outdoor (uncovered) SMR=107
Age County of residence (in 1960)
Travier et al. (2003)
Sweden Male veterinarians
1,178 Total 11 Melanoma 6 Vet in veterinary industry 1 Vet in other industry 3 Other worker in veterinary industry
Total SIR=2.86 Vet in Vet SIR=2.77 Vet in Other SIR=1.84 Other in Vet SIR=3.12
Age Calendar period Geographic region Urban setting
Elwood et al. (1997)
Norway UK USA Canada Italy Denmark Germany Sweden France Belgium Spain
Intermittent Occupational and total sun exposure
29 Studies 23 Intermittent 20 Occupational 11 Total 16,991 Melanoma 6,934 Intermittent 6,517 Occupational 3,540 Total
Intermittent OR=1.71 Occupational OR=0.86 Total OR=1.18
(If possible) Age Sex Susceptibility
Acquavella et al. (1998).
Europe North America New Zealand
White male farmers
21 Studies 10 Original studies used by Blair 6 Follow-up studies 8 PMR studies 7 Case-control studies
All RR=0.95 10 original RR=1.12 Follow-up RR=0.87 PMR studies RR=0.94 Case-control RR=1.14
Gandini et al. (2005)
USA UK Norway Denmark Germany Ireland France Spain Others
Intermittent, Chronic (Occupational) and total sun exposure
57 Studies 33 Intermittent 41 Chronic 13 Total
Intermittent RR=1.61 Chronic RR=0.95 Total RR=1.34
(b) Numbers Exposed:
CAREX estimated about 1,250,000 workers were exposed to solar radiation in Great Britain between 1990 and 1993. The numbers of workers exposed to solar radiation in the various industries covered are given in Table . The CAREX exposed workers are assumed to be either ‘outdoor’ workers (O) and therefore highly exposed, subject to ‘mixed’ exposure or ‘lower’ exposed (M) or having exposure at ‘farmers’ level (F). The percentage of males is taken as that for all occupations from the 1990 census within the group industry sectors.
33
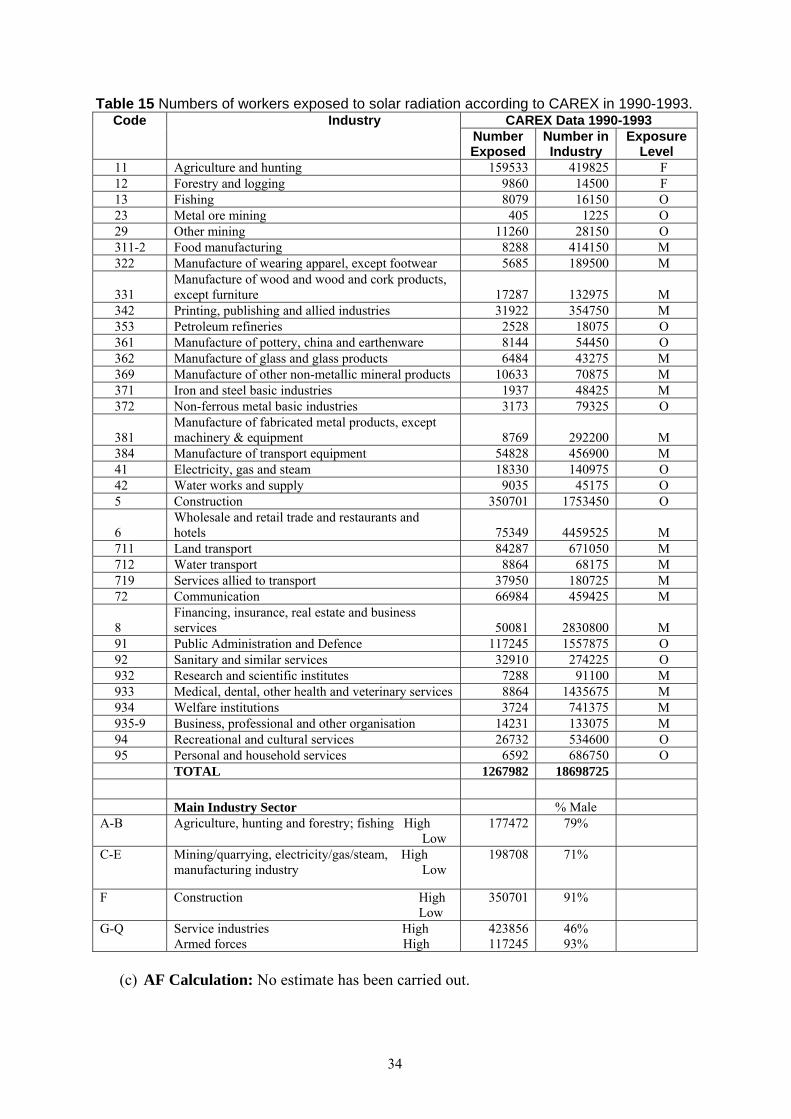
Table 15 Numbers of workers exposed to solar radiation according to CAREX in 1990-1993. Code Industry CAREX Data 1990-1993
Number Exposed
Number in Industry
Exposure Level
11 Agriculture and hunting 159533 419825 F 12 Forestry and logging 9860 14500 F 13 Fishing 8079 16150 O 23 Metal ore mining 405 1225 O 29 Other mining 11260 28150 O 311-2 Food manufacturing 8288 414150 M 322 Manufacture of wearing apparel, except footwear 5685 189500 M
331 Manufacture of wood and wood and cork products, except furniture 17287 132975 M
342 Printing, publishing and allied industries 31922 354750 M 353 Petroleum refineries 2528 18075 O 361 Manufacture of pottery, china and earthenware 8144 54450 O 362 Manufacture of glass and glass products 6484 43275 M 369 Manufacture of other non-metallic mineral products 10633 70875 M 371 Iron and steel basic industries 1937 48425 M 372 Non-ferrous metal basic industries 3173 79325 O
381 Manufacture of fabricated metal products, except machinery & equipment 8769 292200 M
384 Manufacture of transport equipment 54828 456900 M 41 Electricity, gas and steam 18330 140975 O 42 Water works and supply 9035 45175 O 5 Construction 350701 1753450 O
6 Wholesale and retail trade and restaurants and hotels 75349 4459525 M
711 Land transport 84287 671050 M 712 Water transport 8864 68175 M 719 Services allied to transport 37950 180725 M 72 Communication 66984 459425 M
8 Financing, insurance, real estate and business services 50081 2830800 M
91 Public Administration and Defence 117245 1557875 O 92 Sanitary and similar services 32910 274225 O 932 Research and scientific institutes 7288 91100 M 933 Medical, dental, other health and veterinary services 8864 1435675 M 934 Welfare institutions 3724 741375 M 935-9 Business, professional and other organisation 14231 133075 M 94 Recreational and cultural services 26732 534600 O 95 Personal and household services 6592 686750 O
TOTAL 1267982 18698725
Main Industry Sector % Male A-B Agriculture, hunting and forestry; fishing High
Low 177472 79%
C-E Mining/quarrying, electricity/gas/steam, High manufacturing industry Low
198708 71%
F Construction High Low
350701 91%
G-Q Service industries High Armed forces High
423856 117245
46% 93%
(c) AF Calculation: No estimate has been carried out.
34
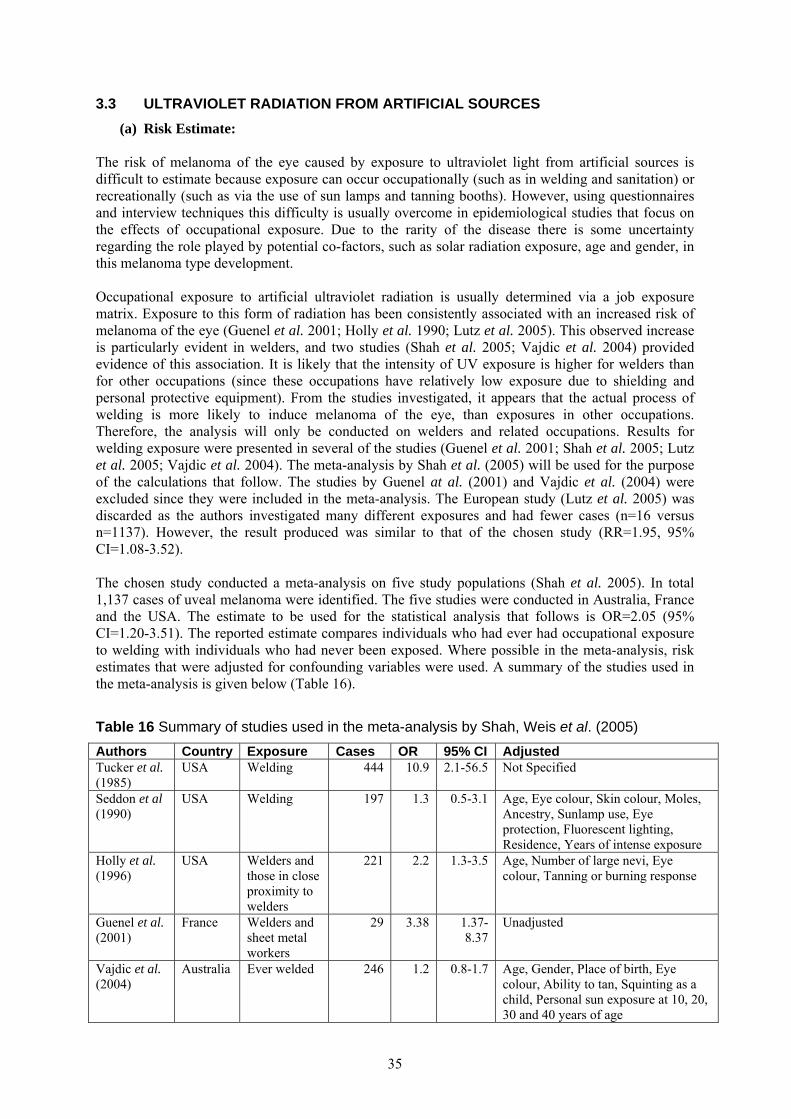
3.3 ULTRAVIOLET RADIATION FROM ARTIFICIAL SOURCES (a) Risk Estimate:
The risk of melanoma of the eye caused by exposure to ultraviolet light from artificial sources is difficult to estimate because exposure can occur occupationally (such as in welding and sanitation) or recreationally (such as via the use of sun lamps and tanning booths). However, using questionnaires and interview techniques this difficulty is usually overcome in epidemiological studies that focus on the effects of occupational exposure. Due to the rarity of the disease there is some uncertainty regarding the role played by potential co-factors, such as solar radiation exposure, age and gender, in this melanoma type development. Occupational exposure to artificial ultraviolet radiation is usually determined via a job exposure matrix. Exposure to this form of radiation has been consistently associated with an increased risk of melanoma of the eye (Guenel et al. 2001; Holly et al. 1990; Lutz et al. 2005). This observed increase is particularly evident in welders, and two studies (Shah et al. 2005; Vajdic et al. 2004) provided evidence of this association. It is likely that the intensity of UV exposure is higher for welders than for other occupations (since these occupations have relatively low exposure due to shielding and personal protective equipment). From the studies investigated, it appears that the actual process of welding is more likely to induce melanoma of the eye, than exposures in other occupations. Therefore, the analysis will only be conducted on welders and related occupations. Results for welding exposure were presented in several of the studies (Guenel et al. 2001; Shah et al. 2005; Lutz et al. 2005; Vajdic et al. 2004). The meta-analysis by Shah et al. (2005) will be used for the purpose of the calculations that follow. The studies by Guenel at al. (2001) and Vajdic et al. (2004) were excluded since they were included in the meta-analysis. The European study (Lutz et al. 2005) was discarded as the authors investigated many different exposures and had fewer cases (n=16 versus n=1137). However, the result produced was similar to that of the chosen study (RR=1.95, 95% CI=1.08-3.52). The chosen study conducted a meta-analysis on five study populations (Shah et al. 2005). In total 1,137 cases of uveal melanoma were identified. The five studies were conducted in Australia, France and the USA. The estimate to be used for the statistical analysis that follows is OR=2.05 (95% CI=1.20-3.51). The reported estimate compares individuals who had ever had occupational exposure to welding with individuals who had never been exposed. Where possible in the meta-analysis, risk estimates that were adjusted for confounding variables were used. A summary of the studies used in the meta-analysis is given below (Table 16). Table 16 Summary of studies used in the meta-analysis by Shah, Weis et al. (2005) Authors Country Exposure Cases OR 95% CI Adjusted Tucker et al. (1985)
USA Welding 444 10.9 2.1-56.5 Not Specified
Seddon et al (1990)
USA Welding 197 1.3 0.5-3.1 Age, Eye colour, Skin colour, Moles, Ancestry, Sunlamp use, Eye protection, Fluorescent lighting, Residence, Years of intense exposure
Holly et al. (1996)
USA Welders and those in close proximity to welders
221 2.2 1.3-3.5 Age, Number of large nevi, Eye colour, Tanning or burning response
Guenel et al. (2001)
France Welders and sheet metal workers
29 3.38 1.37-8.37
Unadjusted
Vajdic et al. (2004)
Australia Ever welded
246 1.2 0.8-1.7 Age, Gender, Place of birth, Eye colour, Ability to tan, Squinting as a child, Personal sun exposure at 10, 20, 30 and 40 years of age
35
(b) Numbers Exposed: To determine the number of workers exposed to ultraviolet radiation from artificial sources, the Labour Force Survey was used, as no estimate is provided by CAREX (Tables 17 and 18). According to the Labour Force Survey there were 1,773,338 workers (1,704,761 Males and 68,577 females) employed as a welder or in a related occupation in 1979 (Table 17).
Table 17 Numbers of workers employed as a welder, in an occupation involving welding or an occupation in close proximity to welding, according to LFS in 1979
SIC code Description Male Female Total124.6 Foremen of Welders 4663 4663 128.0 Welders 153235 14520 167755 TOTAL 157898 14520 172418
Table 18 Numbers of workers employed as a welder, in an occupation involving welding or an occupation in close proximity to welding, according to LFS in 2005
SOC code Description Male Female Total5215 Welding Trades 75448 882 76330 TOTAL 75448 882 76330
(c) AF Calculation:
The estimated total (male and female) attributable fraction for melanoma of the eye is 1.56% (95%Confidence Interval (CI)=0.30-3.62), which equates to 1 (95%CI=0-3) death and 6 (95%CI=1-15) registrations, all of which were attributable to occupational exposure to ultraviolet radiation from welding. The estimated AF for men is 2.87% (95CI=0.56-6.61) resulting in 1 (95%CI=0-3) and 6 (95%CI=1-13) attributable registrations and deaths respectively; and for women the estimated AF is 0.41% (95%CI=0.07-0.96) resulting in 0 (95%CI=0-0) attributable deaths and 1 (95%CI=0-2) attributable registration (Table 19).
36
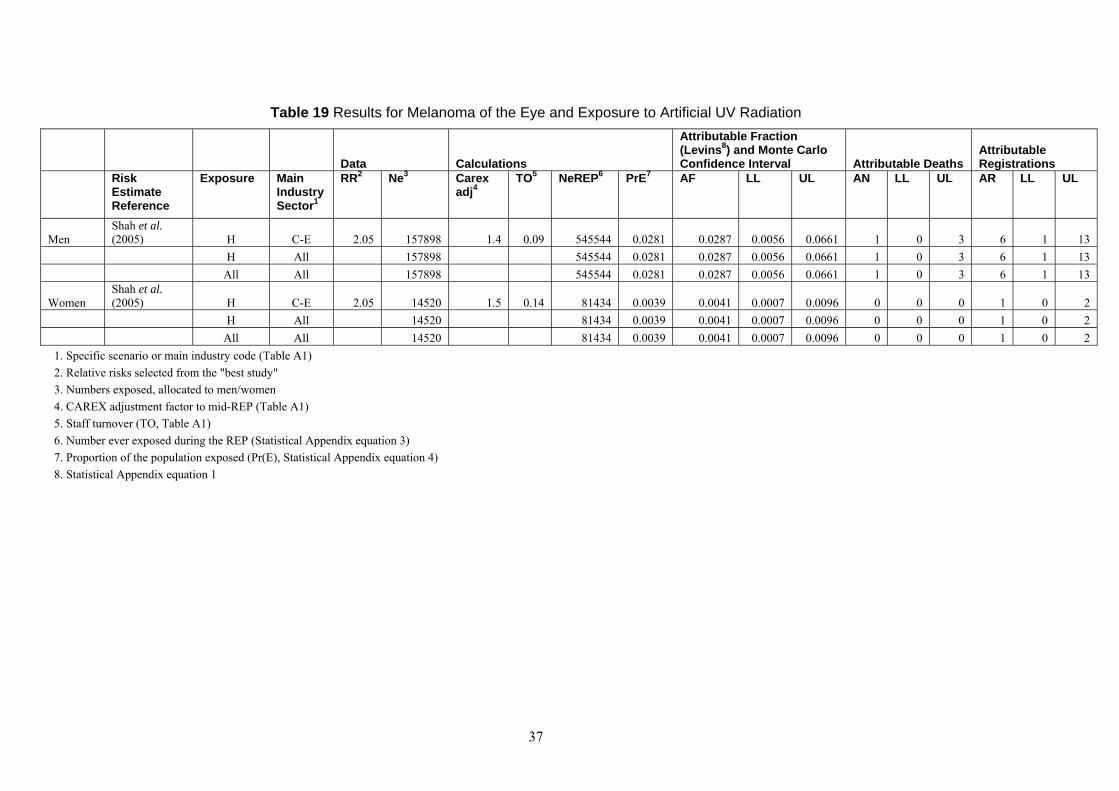
Table 19 Results for Melanoma of the Eye and Exposure to Artificial UV Radiation
Data Calculations
Attributable Fraction (Levins8) and Monte Carlo Confidence Interval Attributable Deaths
Attributable Registrations
Risk Estimate Reference
Exposure Main Industry Sector1
RR2 Ne3 Carex adj4
TO5 NeREP6 PrE7 AF LL UL AN LL UL AR LL UL
Men Shah et al. (2005) H C-E 2.05 157898 1.4 0.09 545544 0.0281 0.0287 0.0056 0.0661 1 0 3 6 1 13
H All 157898 545544 0.0281 0.0287 0.0056 0.0661 1 0 3 6 1 13 All All 157898 545544 0.0281 0.0287 0.0056 0.0661 1 0 3 6 1 13
Women Shah et al. (2005) H C-E 2.05 14520 1.5 0.14 81434 0.0039 0.0041 0.0007 0.0096 0 0 0 1 0 2
H All 14520 81434 0.0039 0.0041 0.0007 0.0096 0 0 0 1 0 2 All All 14520 81434 0.0039 0.0041 0.0007 0.0096 0 0 0 1 0 2
1. Specific scenario or main industry code (Table A1) 2. Relative risks selected from the "best study" 3. Numbers exposed, allocated to men/women 4. CAREX adjustment factor to mid-REP (Table A1) 5. Staff turnover (TO, Table A1) 6. Number ever exposed during the REP (Statistical Appendix equation 3) 7. Proportion of the population exposed (Pr(E), Statistical Appendix equation 4) 8. Statistical Appendix equation 1
37
4 OVERALL ATTRIBUTABLE FRACTION
4.1 EXPOSURE MAP
No exposure map is given since the two exposures, solar radiation and artificial UV radiation, do not overlap with regard to the melanoma type. 4.2 SUMMARY OF RESULTS
The results are summarised in Table 20 and Table 21.
Table 20 Summary of RR used to calculate AF
Agent Exposure RR LL UL UV H 2.05 1.2 3.51
38
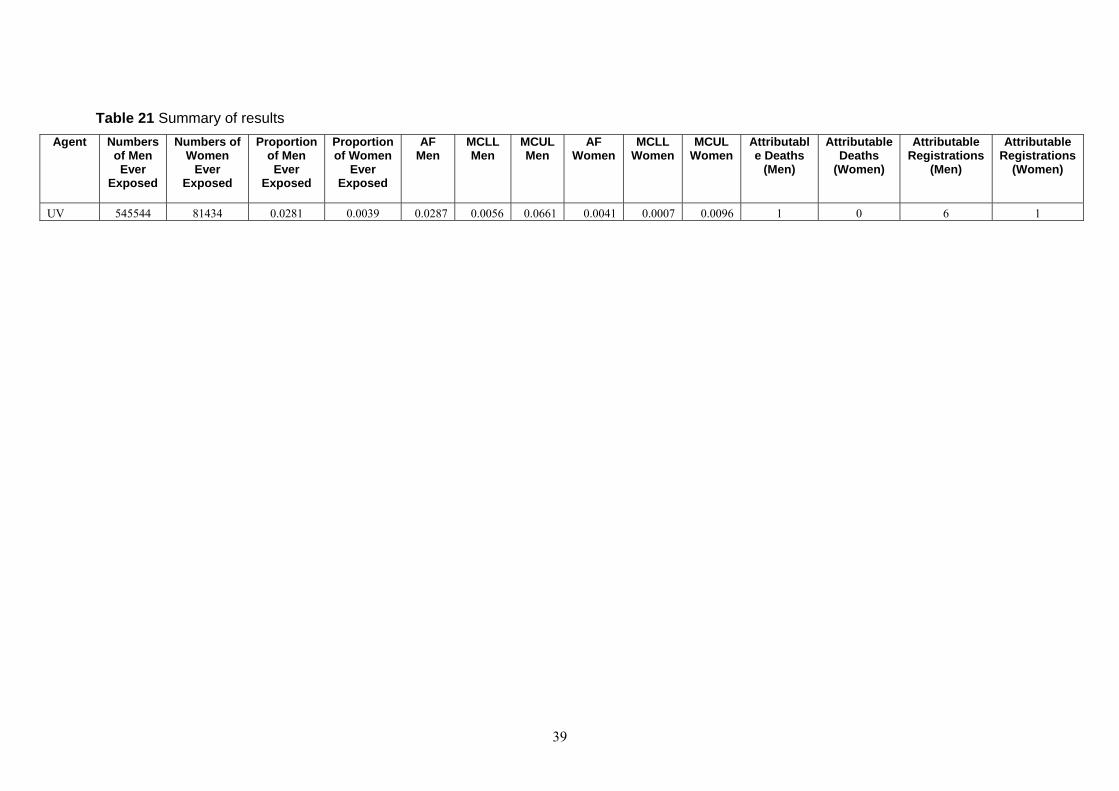
Table 21 Summary of results Agent Numbers
of Men Ever
Exposed
Numbers of Women
Ever Exposed
Proportion of Men Ever
Exposed
Proportion of Women
Ever Exposed
AF Men
MCLL Men
MCUL Men
AF Women
MCLL Women
MCUL Women
Attributable Deaths
(Men)
Attributable Deaths
(Women)
Attributable Registrations
(Men)
Attributable Registrations
(Women)
UV 545544 81434 0.0281 0.0039 0.0287 0.0056 0.0661 0.0041 0.0007 0.0096 1 0 6 1
39
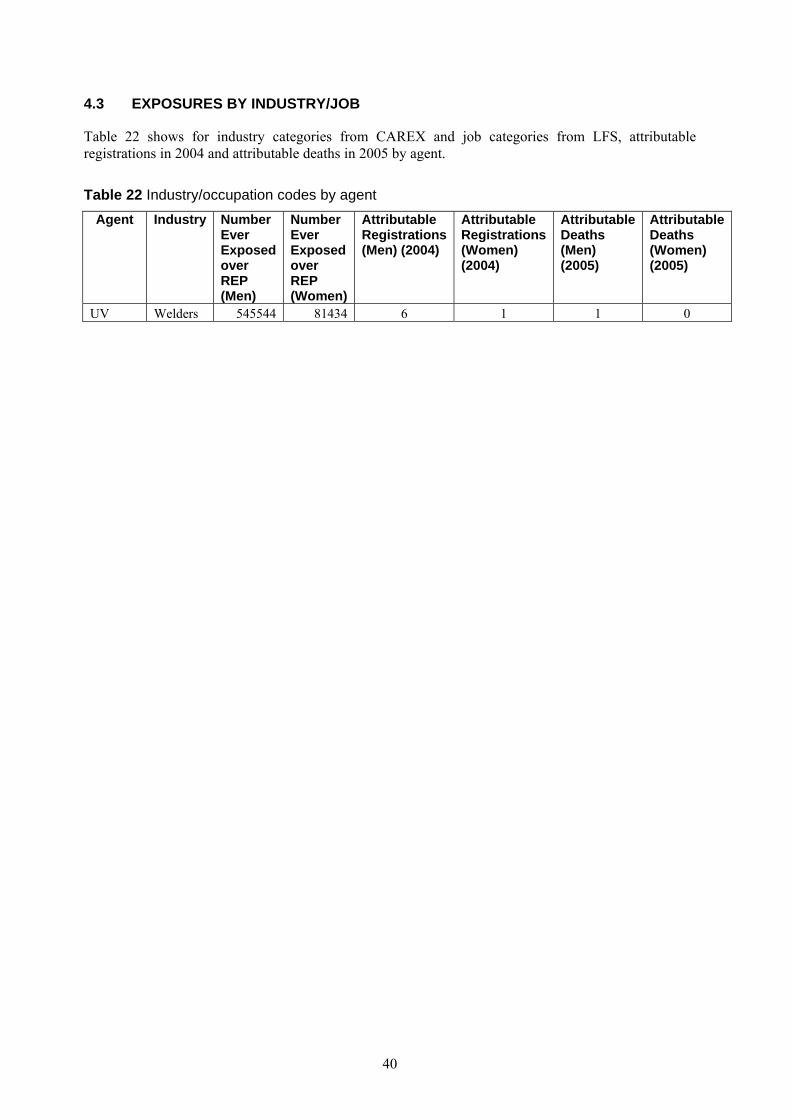
4.3 EXPOSURES BY INDUSTRY/JOB
Table 22 shows for industry categories from CAREX and job categories from LFS, attributable registrations in 2004 and attributable deaths in 2005 by agent.
Table 22 Industry/occupation codes by agent Agent Industry Number
Ever Exposed over REP (Men)
Number Ever Exposed over REP (Women)
Attributable Registrations (Men) (2004)
Attributable Registrations (Women) (2004)
Attributable Deaths (Men) (2005)
Attributable Deaths (Women) (2005)
UV Welders 545544 81434 6 1 1 0
40
5 BIBLIOGRAPHY
Acquavella JF, Olsen G, Cole P, Ireland B, Kaneene J, Schuman S, Holden L (1998) Cancer among farmers: a meta-analysis. Annals of Epidemiology 8(1): 64-74
Ajani UA, Seddon JM, Hsieh CC, Egan KM, Albert DM, Gragoudas ES (1992) Occupation and risk of uveal melanoma. An exploratory study. Cancer 70(12): 2891-2900
Blettner M, Zeeb H, Auvinen A, Ballard TJ, Caldora M, Elliasch H, Gundestrup M, Haldorsen T, Hammar N, Hammer GP, Irvine D, Langner I, Paridou A, Pukkala E, Rafnsson V, Storm H, Tulinius H, Tveten U and Tzonou A (2003) Mortality from cancer and other causes among male airline cockpit crew in Europe. Int .J. Cancer 106(6): 946-95
Cancer Research UK, 2008-last update, UK skin cancer statistics. Available: http://info.cancerresearchuk.org/cancerstats/types/skin/?a=5441 [February, 2008].
Cancerbackup, 22 August 2007, 2007-last update, melanoma of the eye (ocular melanoma). Available: http://www.cancerbackup.org.uk/Cancertype/Eye/Melanomaoftheeye [February, 2008].
Cerhan JR, Cantor KP, Williamson K, Lynch CF, Torner JC, Burmeister LF (1998) Cancer mortality among Iowa farmers: recent results, time trends, and lifestyle factors (United States). Cancer Causes & Control 9(3): 311-319
Cherry N M, Meyer JD, Adisesh A, Brooke R, Owen-Smith V, Swales C, Beck MH (2000) Surveillance of occupational skin disease: EPIDERM and OPRA. British Journal of Dermatology 142: 1128-1134
Coggon D, Harris EC, Brown T, Rice T, Palmer KT (2009) Occupational mortality in England and Wales, 1991-2000. Office of Public Sector Information, London
De Fabo E C, Noonan FP, Feras T, Merlino G (2004) Ultraviolet B but not ultraviolet A radiation initiates melanoma. Cancer Research 64(18): 6372-6376
Diepgen TL, Mahler V (2002) The epidemiology of skin cancer. British Journal of Dermatology 146(Supplement 6): 1-6
Dimich-Ward H, Lorenzi M, Teschke K, Spinelli JJ, Ratner PA, Lee ND, Chow Y, Shu D, Gallagher RP (2007). Mortality and cancer incidence in a cohort of registered nurses from British Columbia, Canada. American Journal of Industrial Medicine 50(12): 892-900
Drever F (1995) Occupational Health Decennial Supplement. London: HMSO.
Elwood JM and Jopson J (1997) Melanoma and sun exposure: an overview of published studies.
English DR, Armstrong BK, Kricker A, Fleming C (1997) Sunlight and cancer. Cancer Causes and Control 8(3): 271-283
Freedman DM, Zahm SH, Dosemeci M (1997) Residential and occupational exposure to sunlight and mortality from non-Hodgkin's lymphoma: composite (threefold) case-control study. BMJ 314(7092): 1451-1455
Gallagher RP, Lee TK (2006) Adverse effects of ultraviolet radiation: a brief review. Progress in Biophysics and Molecular Biology 92: 119-131
Gandini S, Sera F, Cattaruzza MS, Pasquini P, Picconi O, Boyle P, Melchi CF (2005) Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. European journal of cancer 41(1): 45-60
Garland FC, White MR, Garland CF, Shaw E, Gorham ED (1990) Occupational sunlight exposure and melanoma in the U.S. Navy. Archives of Environmental Health 45(5): 261-267
Gavin A, Walsh P (2005) Melanoma of skin. In: Quinn M, Wood H, Cooper N and Rowan S, M. eds, Cancer Atlas of the United Kingdom and Ireland 1991-2000.
41
Studies on Medical and Population Subjects No. 68. London: Office for National Statistics, pp. 151-161.
Gawkrodger DJ (2004) Occupational skin cancers. Occupational Medicine 54: 458-463
Goodman KJ, Bible ML, London S, Mack TM (1995). Proportional melanoma incidence and occupation among white males in Los Angeles County (California, United States). Cancer Causes & control 6(5): 451-459
Gruber SB, Armstrong BK (2006) Cutaneous and Ocular Melanoma. In: Schottenfeld D and Fraumeni J F. eds, Cancer Epidemiology and Prevention. 3rd edn. Oxford University Press, Oxford, pp. 1196-1229
Guenel P, Laforest L, Cyr D, Fevotte J, Sabroe S, Dufour C, Lutz JM, Lynge E (2001) Occupational risk factors, ultraviolet radiation, and ocular melanoma: a case-control study in France. Cancer Causes & Control 12(5): 451-459
Gundestrup M, Storm HH (1999) Radiation-induced acute myeloid leukaemia and other cancers in commercial jet cockpit crew: a population-based cohort study. Lancet 354(9195): 2029-2031
Holly EA, Aston DA, Ahn DK, Smith AH (1996) Intraocular melanoma linked to occupations and chemical exposures. Epidemiology 7(1); 55-61
Holly EA, Aston DA, Char DH, Kristiansen JJ, Ahn D K (1990) Uveal melanoma in relation to ultraviolet light exposure and host factors. Cancer Research 50(18): 5773-5777
IARC (1992): Solar and Ultraviolet Radiation: Volume 55. Lyon: International Agency for Research on Cancer, Lyon.
ISD, 2008. ISD Cancer Information Programme. Available at http://www.isdscotland.org.
Lee E, Burnett CA, Lalich N, Cameron LL, Sestito JP (2002) Proportionate mortality of crop and livestock farmers in the United States, 1984-1993. American Journal of Industrial Medicine 42(5): 410-420
Linet MS, Malker HS, Chow WH, Mclaughlin JK, Weiner JA, Stone BJ, Ericsson JL, Fraumeni JF (1995) Occupational risks for cutaneous melanoma among men in Sweden. Journal of Occupational and Environmental Medicine 37(9): 1127-1135
Linnersjo A, Hammar N, Dammstom BG, Johansson M, Elliasch H (2003) Cancer incidence in airline cabin crew: experience from Sweden. Occupational and Environmental Medicine 60(11): 810-814
Loomis D, Schulz M (2000) Mortality from six work-related cancers among African Americans and Latinos. American Journal of Industrial Medicine 38(5): 565-575
Lutz JM, Cree I, Sabroe S, Kvist TK, Clausen LB, Afonso N, Ahrens W, Ballard TJ, Bell J, Cyr D, Eriksson M, Fevotte J, Guenel P, Hardell l, Jockel KH, Miranda AA, Merletti F, Morales-Suarez-Varela MM, Stengrevics A, Lynge E (2005) Occupational risks for uveal melanoma results from a case-control study in nine European countries. Cancer Causes and Control 16(4): 437-447
Miller JM, Beaumont JJ (1995) Suicide, cancer, and other causes of death among California veterinarians, 1960-1992. American Journal of Industrial Medicine 27(1): 37-49
Monarrez-Espino J, Stang A, Bromen K, Merzenich H, Anastassiou G, Jockel KH (2002) Occupation as a risk factor for uveal melanoma in Germany. Scandinavian Journal of Work, Environment and Health 28(4): 270-277
ONS, 2007a. Cancer Statistics: Registrations. No. 25-35. Available at http://www.statistics.gov.uk/statbase/Product.asp?vlnk=8843.
ONS, 2007b. Mortality statistics: Cause. No. 26-32. Available at http://www.statistics.gov.uk/statbase/Product.asp?vlnk=618.
42
ONS, 2006. Cancer Statistics, Registrations. Registrations of Cancer Diagnosed in 2004, England. No. 35. London: Office for National Statistics. Available at http://www.statistics.gov.uk/statbase/Product.asp?vlnk=8843
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global Cancer Statistics, 2002.Cancer Journal for Clinicians 55(2): 74-108
Perez-Gomez B, Aragones N, Gustavsson P, Plato N, Lopez-Abente G, Pollan M (2005) Cutaneous melanoma in Swedish women: Occupational risks by anatomic site. American Journal of Industrial Medicine 48(4): 270-281
Perez-Gomez B, Pollan M, Gustavsson P, Plato N, Aragones N, Lopez-Abente G (2004) Cutaneous melanoma: hints from occupational risks by anatomic site in Swedish men. Occupational and Environmental Medicine 61(2): 117-126
Pukkala E, Aspholm R, Auvinen A, Ellasch H, Gundestrup M, Haldorsen T, Hammar N, Hrafnkelsson J, Kyyronen P, Linnersjo A, Rafnsson V, Storm H, Tveten U (2002) Incidence of cancer among Nordic airline pilots over five decades: occupational cohort study. BMJ 325(7364):. 567
Pukkala E, Auvinen A, Wahlberg G (1995) Incidence of cancer among Finnish airline cabin attendants, 1967-92. BMJ 311(7006): 649-652
Puntoni R, Ceppi M, Casella C, Ugolini, Gennaro V, Puntoni M, Vercelli M, Merlo DF (2005) Increased incidence of cutaneous malignant melanoma among longshoremen in Genoa, Italy: the role of sunlight and occupational exposure. Occupational and Environmental Medicine 62(4): 270-271
Rafnsson V, Hrafnkelsson J, Tulinius H (2000). Incidence of cancer among commercial airline pilots. Occupational and Environmental Medicine 57(3): 175-179
Ramirez CC, Federman DG, Kirsner RS (2005) Skin cancer as an occupational disease: the effect of ultraviolet and other forms of radiation. International Journal of Dermatology 44(1): 95-100
Reynolds P, Cone J, Layefsky M, Goldberg DE, Hurley F (2002) Cancer incidence in California flight attendants (United States). Cancer Causes & Control 13(4): 317-324
Settimi L, Comba P, Carrier P, Boffetta P, Magnani C, Terracinin B, Andrion A, Bosia S, Ciapini C, De Santis M, Desideri E, Fedi A, Luccoli L, Maiozzi P, Masina A, Perazzo PL, Axelson O (1999) Cancer risk among female agricultural workers: a multi-center case-control study. American Journal of Industrial Medicine 36(1): 135-141
Shah CP, Weis E, Lajous M, Shields JA, Shields CL (2005) Intermittent and chronic ultraviolet light exposure and uveal melanoma: a meta-analysis. Ophthalmology 112(9): 1599-1607
Shaham J, Gurvich R, Kneshet Y (2003a) Cancer incidence among laboratory workers in biomedical research and routine laboratories in Israel: Part II-nested case-control study. American Journal of Industrial Medicine 44(6): 611-626
Shaham J, Gurvich R, Kneshet Y (2003b) Cancer incidence among laboratory workers in biomedical research and routine laboratories in Israel: Part I-the cohort study. American Journal of Industrial Medicine 44(6): 600-610
Siemiatycki J, Richardson L, Striaf K, Letreille B, Lakhani R, Campbell S, Rousseau M, Boffetta P (2004) Listing occupational carcinogens. Environmental Health Perspectives 112: 1447-1459
Travier N, Gridley G, Blair A, Dosemeci M,d Boffetta AP (2003) Cancer incidence among male Swedish veterinarians and other workers of the veterinary industry: a record-linkage study. Cancer Causes & Control 14(6): 587-593
Vagero D, Ringback G, Kiviranta H (1986) Melanoma and other tumours of the skin among office, other indoor and outdoor workers in Sweden 1961-1979. British Journal of Cancer 53(4): 507-512
43
Vagero D, Swerdlow AJ, Beral V (1990) Occupation and malignant melanoma: a study based on cancer registration data in England and Wales and in Sweden. British Journal of Industrial Medicine 47(5) 317-324
Vajdic CM, Kricker A, Giblin M, McKenzie J, Aitken JF, Giles GG, Armstrong BK (2004) Artificial ultraviolet radiation and ocular melanoma in Australia. International Journal of Cancer 112(5): 896-900
Walter SD, King WD, Marrett LD (1999) Association of cutaneous malignant melanoma with intermittent exposure to ultraviolet radiation: results of a case-control study in Ontario, Canada. International Journal of Epidemiology 28(3): 418-427
WCISU, 2008. Cancer Incidence in Wales. Available at http://www.wales.nhs.uk.
Wennborg H, Yuen J, Axelsson G, Ahlbom A, Gustavsson P,and Sasco AJ (1999) Mortality and cancer incidence in biomedical laboratory personnel in Sweden. American Journal of Industrial Medicine 35(4): 382-389
44
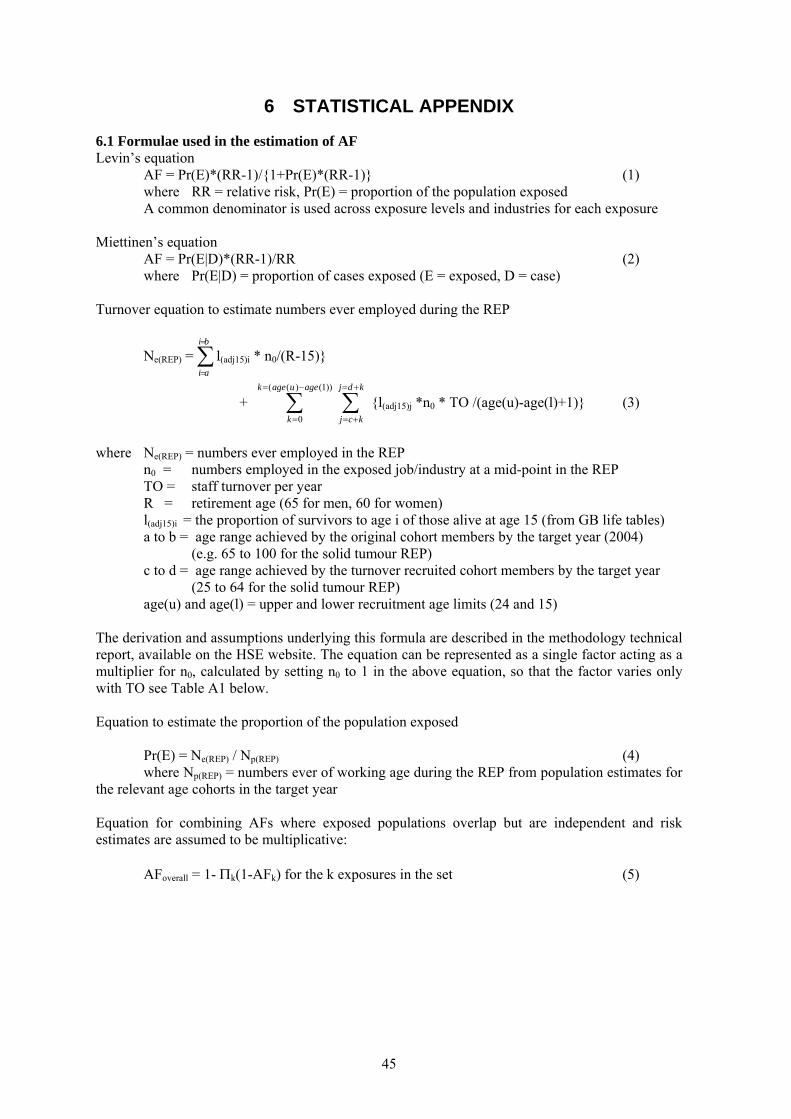
6 STATISTICAL APPENDIX
6.1 Formulae used in the estimation of AF Levin’s equation AF = Pr(E)*(RR-1)/{1+Pr(E)*(RR-1)} (1) where RR = relative risk, Pr(E) = proportion of the population exposed A common denominator is used across exposure levels and industries for each exposure Miettinen’s equation AF = Pr(E|D)*(RR-1)/RR (2) where Pr(E|D) = proportion of cases exposed (E = exposed, D = case) Turnover equation to estimate numbers ever employed during the REP
Ne(REP) = ∑ l(adj15)i * n0/(R-15)} =
=
bi
ai
+ ∑ {l(adj15)j *n0 * TO /(age(u)-age(l)+1)} (3) −=
=
))1()((
0
ageuagek
k∑
+=
+=
kdj
kcj
where Ne(REP) = numbers ever employed in the REP n0 = numbers employed in the exposed job/industry at a mid-point in the REP TO = staff turnover per year R = retirement age (65 for men, 60 for women) l(adj15)i = the proportion of survivors to age i of those alive at age 15 (from GB life tables) a to b = age range achieved by the original cohort members by the target year (2004) (e.g. 65 to 100 for the solid tumour REP) c to d = age range achieved by the turnover recruited cohort members by the target year (25 to 64 for the solid tumour REP) age(u) and age(l) = upper and lower recruitment age limits (24 and 15) The derivation and assumptions underlying this formula are described in the methodology technical report, available on the HSE website. The equation can be represented as a single factor acting as a multiplier for n0, calculated by setting n0 to 1 in the above equation, so that the factor varies only with TO see Table A1 below. Equation to estimate the proportion of the population exposed Pr(E) = Ne(REP) / Np(REP) (4) where Np(REP) = numbers ever of working age during the REP from population estimates for the relevant age cohorts in the target year Equation for combining AFs where exposed populations overlap but are independent and risk estimates are assumed to be multiplicative: AFoverall = 1- Πk(1-AFk) for the k exposures in the set (5)
45
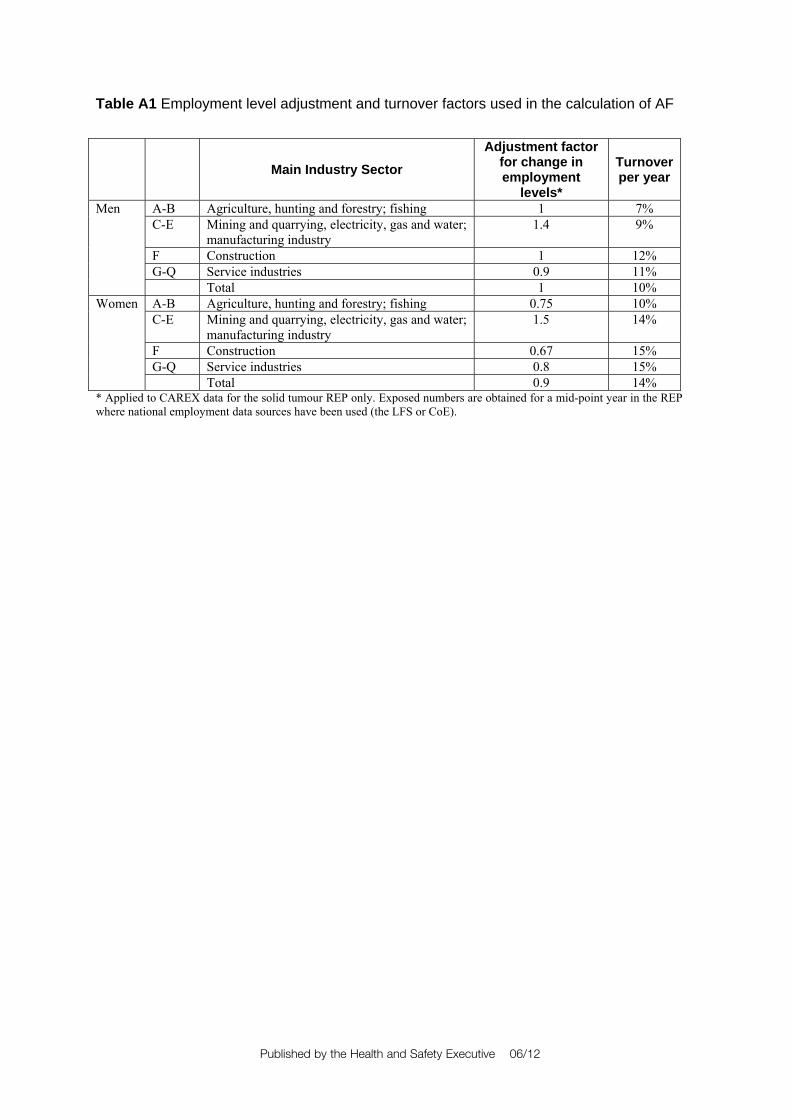
Table A1 Employment level adjustment and turnover factors used in the calculation of AF
Main Industry Sector Adjustment factor
for change in employment
levels*
Turnover per year
A-B Agriculture, hunting and forestry; fishing 1 7% C-E Mining and quarrying, electricity, gas and water;
manufacturing industry 1.4 9%
F Construction 1 12% G-Q Service industries 0.9 11%
Men
Total 1 10% A-B Agriculture, hunting and forestry; fishing 0.75 10% C-E Mining and quarrying, electricity, gas and water;
manufacturing industry 1.5 14%
F Construction 0.67 15% G-Q Service industries 0.8 15%
Women
Total 0.9 14% * Applied to CAREX data for the solid tumour REP only. Exposed numbers are obtained for a mid-point year in the REP where national employment data sources have been used (the LFS or CoE).
Published by the Health and Safety Executive 06/12
The burden of occupational cancer in Great BritainMelanoma
Health and Safety Executive
RR860
www.hse.gov.uk
The aim of this project was to produce an updated estimate of the current burden of cancer for Great Britain resulting from occupational exposure to carcinogenic agents or exposure circumstances. The primary measure of the burden of cancer was the attributable fraction (AF) being the proportion of cases that would not have occurred in the absence of exposure; and the AF was used to estimate the number of attributable deaths and registrations. The study involved obtaining data on the risk of the cancer due to the exposure of interest, taking into account confounding factors and overlapping exposures, as well as the proportion of the target population exposed over the relevant exposure period. Only carcinogenic agents, or exposure circumstances, classified by the International Agency for Research on Cancer (IARC) as definite (Group 1) or probable (Group 2A) human carcinogens were considered. Here, we present estimates for melanoma that have been derived using incidence data for calendar year 2004, and mortality data for calendar year 2005.
The estimated total (male and female) AF for melanoma of the eye related to overall occupational exposure is 1.56% (95%Confidence Interval (CI)= 0.30-3.62), which equates to 1 (95%CI= 0-3) death and 6 (95%CI= 1-15) registrations, all of which were attributable to occupational exposure to ultraviolet radiation from welding.
This report and the work it describes were funded by the Health and Safety Executive (HSE). Its contents, including any opinions and/or conclusions expressed, are those of the authors alone and do not necessarily reflect HSE policy.