Embed Size (px)
Citation preview

Central JSM Clinical Case Reports
Cite this article: Hardegree EL, Gupta R (2014) Rotational Coronary Angiography: Time to Revisit. JSM Clin Case Rep 2(6): 1058.
*Corresponding authorRajiv Gupta, Division of Cardiology, 1901 Veterans Blvd, Temple, Texas 76502, USA, Tel: 254-743-0912; Email:
Submitted: 29 August 2014
Accepted: 30 September 2014
Published: 02 October 2014
Copyright© 2014 Gupta et al.
OPEN ACCESS
Editorial
Rotational Coronary Angiography: Time to RevisitEvan L. Hardegree1,2 and Rajiv Gupta1*1Department of Medicine, Division of Cardiovascular Disease, Central Texas Veterans Healthcare System, USA 2Department of Medicine, Division of Cardiovascular Disease, Baylor Scott & White Healthcare, USA
BACKGROUNDAlthough coronary angiography is considered the gold
standard for diagnosis of coronary artery disease, it has many limitations. In standard angiography, the operator acquires multiple views of the coronary arteries in 4-6 projections for the left coronary artery and 2-3 for the right coronary artery to find the diseased area for diagnosis and subsequent treatment of coronary artery disease. Multiple projections are necessary to lay out the coronary tree to overcome issues of vessel overlap, tortuosity, foreshortening, and eccentric plaques which may lead to underestimation of the severity of a lesion. Each such projection is associated with increased contrast and radiation use. Even experienced operators may miss eccentric plaques when relying on a limited number of projections. The margin of error may be greater in inexperienced operators. Rotational angiography (RA) is a known but seldom utilized angiographic technique in which the C-arm is programmed to rotate during continuous contrast injection, acquiring a large number of views during a single injection. It can improve assessment of coronary anatomy while minimizing contrast use and radiation exposure.
HISTORY AND EVOLUTIONThe first description of an imaging technique utilizing the
dynamic movement of the C-arm came from Tommasini et al in 1998 [1]. They pioneered a panoramic diagnostic imaging technique of the coronary arteries by manual transverse 180 degree rotation of the C-arm at 25 degree cranial and 25 degree caudal angulations in 129 patients. They reported an improvement in lesion identification in 34 patients with this technique while reducing the contrast dose and total cine time by 50%.
Subsequently the manual gantry movement was automated and has become known as RA. Initially RA was developed for image acquisition in a single angulation plane known as single axis RA. This traditionally went from 55-60 degrees in the left anterior oblique (LAO) position to 55-60 degrees right anterior oblique (RAO). With further evolution of this technique, this arc was further extended to 120 degrees LAO, called extended RA [2]. This permitted more angiographic information to be collected, providing computed tomography-like volumetric
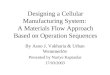
Figure 1 LCA small and medium curve for all patients.
data, but required longer acquisition time, in addition to patient positioning and breath holding issues. The next advancement in RA was the development of simultaneous cranial to caudal and LAO to RAO arcs known as dual axis RA (Xper Swing, Philips Health care, Best, The Netherlands). The system rotates around the patient in pre-programmed trajectories which are optimized for maximal image quality, with dedicated trajectories for the left and right coronary arteries.

Central
Gupta et al. (2014)Email:
JSM Clin Case Rep 2(6): 1058 (2014) 2/3
rate and amount of contrast may need to be increased depending upon the size of the coronary tree.
ADVANTAGES OF RAA number of studies have compared standard angiography
with RA [3-7]. The three major advantages are reduced radiation exposure, reduced contrast use and improved diagnostic accuracy. Akhtar et al described a 40% reduction of contrast utilization in a small sample of patients using a flat panel detector [3]. Kuon et al also demonstrated the value of RA in reducing contrast use in patients with advanced renal insufficiency [4]. Maddux et al showed reduction in contrast use, radiation use and a reduction in the procedural time with RA compared to standard angiography [5]. Klein et al used dual axis RA and showed similar findings [6]. In one study, the number of angiographic runs required for adequate diagnostic yield in conventional angiography was 9.1 per patient, versus only 3.5 runs for dual axis rotational angiography, with no significant difference in total procedure time [7].
Besides reducing overall radiation exposure, the actual benefit to the operator is likely higher. In conventional a ngiography, the operator stands at the bedside during contrast injection and fluoroscopy and may have to pan the table, while in rotational angiography, the operator may stand several feet back from the x-ray tube thereby reducing radiation exposure significantly.
LIMITATIONS OF RAMost cardiac catheterization laboratories in the U.S. do not
have access to systems that can provide RA. Even in catheterization laboratories that do have this technology, it is underutilized due to lack of knowledge and the learning curve associated with its use. It is important that the catheter be well seated for adequate image interpretation. In coronary anatomy where the catheter is not a good fit, RA images will be suboptimal. Also, depending upon the size of the coronary tree, it may be necessary to increase the flow rate and overall volume of the injection.
CONCLUSIONCoronary angiography remains an essential tool in the
diagnosis and treatment of coronary artery disease. Rotational coronary angiography is a known but seldom used technology which has the potential to reduce radiation and contrast use in the cardiac catheterization laboratory, while offering a more comprehensive assessment of coronary anatomy. While there is a brief learning curve associated with its use, the benefits outweigh the limited time and effort invested in learning this technique. It is time to revisit and adopt this technology.
REFERENCES1. Tommasini G, Camerini A, Gatti A, Derchi G, Bruzzone A, Vecchio C.
Panoramic coronary angiography. J Am Coll Cardiol. 1998; 31: 871-877.
2. Klein AJ, Garcia JA. Rotational coronary angiography. Cardiol Clin. 2009; 27: 395-405.
3. Akhtar M, Vakharia KT, Mishell J, Gera A, Ports TA, Yeghiazarians Y, et al. Randomized study of the safety and clinical utility of rotational vs. standard coronary angiography using a flat-panel detector. Catheter Cardiovasc Interv. 2005; 66: 43-49.
TECHNIQUEThe technique consists of two parts: isocentering and
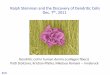
rotational scan set up. The table that the patient rests upon is brought to the neutral position by an automated switch. The heart is then isocentered in the postero-anterior position with the specific magnification determined by the operator. The magnification is generally set at 8-12 inch (22-31 cm) field of view but could also be set up at lower magnification to further reduce radiation. The rotational swing plane is then chosen for the left coronary or right coronary system. There are 2 swing arcs for the left coronary tree: Cranial 30 degrees with a 5.3 sec swing or cranial 35 degrees with a 5.8 sec swing (Figure 1). The swing arcs for right coronary tree are LAO with 3.7 sec swing or AP with 4.0 sec swing time (Figure 2). The gantry is then allowed to swing in the predetermined swing arc to test that there is no obstruction to its movement. Image position may also be confirmed by stepping on fluoroscopy at the end of rotation to ensure that the image is acceptable to the angiographer and is not off the screen. Once this is done the system is ready; stepping on the cine pedal activates the sweeping movement of the gantry. Generally a short 0.5-1 second delay between contrast injection and image acquisition is recommended to allow vessels to fill with contrast. Utilizing a power injector allows for uniform contrast injection and better image acquisition. A rate of 1.5 cc/sec with 460 psi rise and a volume of 8 cc is generally sufficient for the right coronary system while a rate of 1.8-2 cc/sec with a 600 psi rise and a total volume of 14 cc fills the left coronary tree adequately. This flow
Figure 2 RCA standard curves for all patients.

Central
Gupta et al. (2014)Email:
JSM Clin Case Rep 2(6): 1058 (2014) 3/3
4. Kuon E, Niederst PN, Dahm JB. Usefulness of rotational spin for coronary angiography in patients with advanced renal insufficiency. Am J Cardiol. 2002; 90: 369-373.
5. Klein AJ, Garcia JA, Hudson PA, Kim MS, Messenger JC, Casserly IP, et al. Safety and efficacy of dual-axis rotational coronary angiography vs. standard coronary angiography. Catheter Cardiovasc Interv. 2011; 77: 820-827.
6. Maddux JT, Wink O, Messenger JC, Groves BM, Liao R, Strzelczyk J, et al. Randomized study of the safety and clinical utility of rotational angiography versus standard angiography in the diagnosis of coronary artery disease. Catheter Cardiovasc Interv. 2004; 62: 167-174.
7. Horisaki T, Linuma K, Bakker N. Feasibility evaluation of dual axis rotational angiography (XperSwing) in the diagnosis of coronary artery disease. MEDICAMUNDI. 2008; 52: 3-7.
Hardegree EL, Gupta R (2014) Rotational Coronary Angiography: Time to Revisit. JSM Clin Case Rep 2(6): 1058.
Cite this article