-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
1/12
2011
Rosai- Dorfman Disease
(Sinus histiocytosis with massive
lymphadenopathy)
A Case ReportOral Pathology Case Report
A. V. Asanka De Silva D/05/10
F A C U L T Y O F D E N T A L S C I E N C E S - U N I V E R S I
T Y O F P E R A D E N I Y A
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
2/12
2Rosai- Dorfman DiseaseA Case Report
Rosai- Dorfman Disease
(Sinus histiocytosis with
massive lymphadenopathy)
A Case Report
Abstract
Rosai-Dorfman disease (RDD), otherwise
known as sinus histiocytosis with massive
lymphadenopathy is a rare disease ofunknown aetiology. First
described in
1969 with painless cervical lymph node
enlargement in association with fever,
weight loss and sweating. 43% of cases
were reported extra nodally that commonly
involving skin, upper airway, and salivary
glands12
. RDD is usually seen in youngpatients. Cutaneous lesions are
the
common form of extranodal diseases, but
cases of purely cutaneous lesions without
nodal or other extranodal involvement are
rare, Proliferation of large pale or foamy
histiocytes exhibiting enlarged vesicular
nuclei, prominent nucleoli, and distinctivelymphophagocytosis or
emperipolesis is
the basis of the diagnosis. S-100 protein
immunophenotype is useful in confirming
the disease entity.
This case report is about a 52 yrs old male
patient presented with asymptomatic
diffuse swelling on left side pre auricular
area diagnosed as Rosai-Dorfman disease
after histopathological analysis of the
excision biopsy. Currently on follow up
after 3rd month post operatively.
Key words: emperipolesis, Rosai
Dorfman disease, sinus histiocytosis with
massive lymphadenopathy, nodal, head
and neck.
Introduction
Rosai-Dorfman disease (RDD) is a benign
systemic proliferative disorder of
histiocytes resembling the sinus histiocytes
of lymph nodes. The typical clinical
features of this disease include bilateral
painless lymphadenopathy, fever, and
polycolonal hyperglobulinaemia. The
condition with the head and neckinvolvement reported in 22% of
cases,
most commonly the nasal cavity followed
by the parotid gland 10. Extranodal
involvement in 43% (500 pts) of cases,
and cutaneous lesions are the most
common form of extranodal diseases. The
disease is not confined to a particular raceor geographical
area, although African
Negroes are more commonly involved
than whites9. Purely cutaneous RDD occur
rarely, particularly among Orientals10.
Nodal lesions are classified as an
inflammatory/hyperplasic disorder which
usually undergoes spontaneous regression;extranodal lesion
natural history is
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
3/12
3Rosai- Dorfman DiseaseA Case Report
associated with indolent growth and
recurrences along years or decades. It is
often confused with lymphoma.
RDD First described in 1969 with painless
cervical lymph node enlargement in
association with fever, weight loss and
sweating that commonly affects children
and adolescents. The most common sites
affected are the soft tissues of the head and
neck and the paranasal sinuses and nasal
cavity 10-4.
Case report
A 52 year old male presented to the dental
institute Colombo (DIC) with an
asymptomatic swelling on lower left sideof the cheek for 2
months duration (first
noted in November 2010). This lesion had
a sudden onset and the size of the lesion
gradually increased with time. He first got
treatment from general hospital Mathra
where FNAC was done. Microscopically
FNAC smear reveal mixed lymphoid cells
and many macrophages with engulfed
debris and, no oncocytic cells or atypical
cells were seen.The report concluded
giving differential diagnosis as reactive
lymph node and Warthins tumour. Then
he attended to Dental Institute Colombo
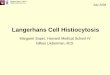
for his convenience. On examination firm,
non tender swelling apprx.34 cm with
demarcated margins on palpation was
noted on the left side angle of the
mandiblular region extending to sub
mandibular region.[figure 1] He had
history of leptospirosis 5years back and no
relevant family history.
Following investigations were
done.WBC/DC and blood picture were
normal, ESR was slightly elevated
(24mm/h), FNAC concluded as
inflammatory lesion and suggested
histology, Ultra sound scan left side neck
suggested Warthins tumourand MRI
suggested biopsy. There were no
radiological abnormalities. Differentialdiagnosis at surgery was
tuberculosis or
lymphoma. The lesion was excised
including level one lymph nodes and sent
for histopathological examination on
27/02/2011. Mantoux test was done later
and the result was negative.
Figure 1
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
4/12
4Rosai- Dorfman DiseaseA Case Report
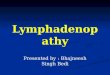
Figure 2 Macroscopic appearance of the lesion
Macroscopically lesions presented as soft
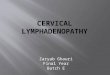
nodule and a lymph node.Microscopic examination of the lymph
node [Figure 3] and the lesion revealed
partial effacement of architecture with
marked capsular fibrosis and sinus
histiocytosis. Emperipolesis of
lymphocytes and plasma cells is marked
immunehistochemically histiocytesshowed nuclear and cytoplasmic
positivity
for S-100 protein [figure 4]. The
histopathological examination confirmed
the diagnosis Rosai- Dorfman Disease
After the surgery patient was on antibiotics
[IV augmentin 1.2g tds] to prevent
infection and analgesics on normalregimes. Patient is currently
on review
appointments without any complaints.
Discussion
Rosai-Dorfman disease (RDD) or Sinus
histiocytosis with massive
lymphadenopathy is a rare benign systemic
proliferative disorder of unknown
aetiology. RDD belongs to broad family of
disorders known as lympho reticular
disorders which consist of 1.Reactivechanges caused by infection
and
inflammation 2.Autoimmune
disorders3.Immunosupression and
4.Neoplasia. Reactive hyperplasia is one of
the disease sub types that belong to
Reactive disorders of lymph nodes which
consist of following categories1.Follicular hyperplasiain a
predominantly humoral response there is a
hyperplasia of the cortical follicles manly
composed of B lymphocytes. With
development of B cell germinal centres.
2.Parafollicular/ paracoticle hyperplasia
- in a predominantly cell mediated
response there is a hyperplasia of the
Figure 4- Immunoreactivity for S-100
Figure 3 Histiocyte cells (H&E, 40)
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
5/12
5Rosai- Dorfman DiseaseA Case Report
paracortical follicles manly composed of T
lymphocytes. 3. Sinus hyperplasia/ sinus
histiocytosis -Certain stimuli evoke
intense phagocytic activity leading to
dilatation of subacapsular and medullary
sinuses with increased numbers and
activity of macrophages and phagocytic
lining cells. This reaction is seen in nodes
draining tissues from which endogenous
particulate matters such as lipid is
released. e.g. Necrotic tumour
It is characterised by overproduction of
histiocytes or tissue macrophages. This
condition was first described by Robb-
Smith in children and was termed as giant
cell sinus reticulosis in 19479. Sinus
histiocytosis with massive
lymphadenopathy (SHML) has beenrecognized as a distinct
clinicopathological
entity, though first given this name by
Rosai and Dorfman in 1969. Incidences
very rare, probably less than 1000 cases
reported in the literature. The disease is
not confined to a particular race or
geographical area, although African
Negroes are more commonly involved
than whites9, 17. Although RDD may occur
in any age group, it is most frequently seen
in children and young adults14. More than
two thirds of registry patients are younger
than 10 years. Patients presenting with
isolated intracranial disease tend to be
older4. The disease is more common in
males16 ranging from 1.4:1 to 3:18, 17.
Although there is no evidence on aetiology
but viruses like Herpes virus 6 (HHV-6)
and Epstein-Barr virus (EBV) have been
suggested as potential causative agents6.
The natural history is that of a regression
and resurgence followed eventually by
complete resolution.
The clinical picture of RDD is hardly
distinguishable from malignant
lymphomas which histopathology usuallycomes as a surprise9. Head
and neck
involvement has been reported in 22% of
cases; most commonly the nasal cavity
followed by the parotid gland14, the
paranasal sinuses, the nasopharynx,
submandibular glands,the larynx, the
temporal bone, the intratemporal fossa, thepterygoid fossa, the
meninges and the orbit
are the other possible sites.Because of
gradual awareness of this disease entity,
more and more extranodal cases with or
without nodal involvement had been
documented. To date, extranodal Rosai-
Dorfman diseases are still on the rise and
accounted for approximately 43% of 600
registry cases, which manifested at least
one site of extranodal involvement12.
Clinical Features in most typical forms are
painless, bilateral, lymph node
enlargement in neck associated with fever,
leukocytosis, elevated erythrocytesedimentation rate in 88.5% of
cases,
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
6/12
6Rosai- Dorfman DiseaseA Case Report
polyclonal hypergammaglobulinaemia.Autoimmune hemolysis can also
occur.
Most common sites involving are eyes and
ocular adnexa (especially orbit), head and
neck region, upper respiratory tract, skin
and subcutaneous tissues, skeletal system
and central nervous system. Other sites are
gastrointestinal tract, salivary glands,
genitourinary tract, thyroid, breast and
uterine cervix.
There are different clinical presentations in
RDD in head and neck region that reported
as Neck mass, facial swelling, Eye
swelling, facial pain, Headache and
Ataxia, difficulty walking and falls.
The differential diagnosis ofextranodal SHML may be a
challenge15.
Comparison of classical clinical case with
this case done in table- 1Imaging (CT and
magnetic resonance imaging) may be used
to assess disease extension. If there is
cervical lymph node enlargement, FNAB
or lymph node biopsies may be useful for
the diagnosis11.The final diagnosis of RDD
usually made on characteristic
histopathological and cytological features.
La Barge et al presented a case series of 13
patients with RDD in head and neck region
in 2008 that was reported within 1997
20075. Table 3 gives the summery.
Classical cases of RDD This case
Clinical features
painless, bilateral, lymph node
enlargement
Painless Unilateral lymph
node enlargement
Fever Fever absent
leukocytosis No leukocytosis
Elevation in ESR ESR slight elevation
Autoimmune haemolysis Autoimmune haemolysis
absent
Classical histopathology In this case
Emperipolesis Emperipolesis marked
Moderately abundant plasmacells and lymphocytes
Moderately abundant plasmacells and lymphocytes
Effacement of involved organ
architecture
Partial effacement of lymph
node architecture
Positivity for CD68, alpha -1
antitrypsin,s-100, cathepsin E
Positivity being checked for
S-100 and positive results
gained.
Table-1
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
7/12
7Rosai- Dorfman DiseaseA Case Report
The cells have histochemical and
phenotypic features of macrophages. Large
amounts of esterases and acid phosphatase
are contained by the cells. Show positivity
for CD 68 and alpha-1 antitrypsin. They
also exhibit some of the phenotypicfeatures of dendritic cells
such as S100,
cathepsin E, fascin and at times CD 1a.6,
71, 8, 13. Skin biopsy non-specific unless
emperipolesis is present but lymph node
pathology is characteristic. emperipolesis
is the presence of an intact cell within the
cytoplasm of another cell.
The characteristic histopathological feature
of RDD is the proliferation of distinctive
histiocytic cells that demonstrate
lymphophagocytosis in the background a
mixed inflammatory infiltrate consisting of
moderately abundant plasma cells and
lymphocytes. As a result effacement of
involved organ architecture leading to
fibrous band formation can be noted19. No
Birbeck granules. Birbeck granules are a
characteristic microscopic finding in
Langerhans cell histiocytosis
(Histiocytosis X), which present as shaped
or "tennis-racket" cytoplasmic organelles
Deferential diagnosis Rosai-Dorfman disease
Hodgkins lymphoma Atypical monocytes, Reed-Sternberg cells
+Langerhans cell histiocytosis Emperipolesis absent, Birbeck
granules
identified by electron microscopy
Inflammatory pseudotumor Emperipolesis absent, positivity for
S-100
protein rare
Malignant histiocytosis and lymphoma with
feature of malignant histiocytosis
Atypia, cellular pleomorphism
Hemophagocytic syndrome associated with T-cell lymphoma and/or
viral infection
Lymphomatous infiltrate, lobularpanniculitis, negativity for
S-100 protein
Eruptive xanthoma Emperipolesis and plasma cells absent
Generalized eruptive histiocytoma
Juvenile xanthogranuloma
Inflammatory malignant fibrous histiocytoma Atypia, cellular
pleomorphism
Lepromatous leprosy Poorly defined infiltrate, plasma cells
rare,
positivity for organisms on Fite stain
Table-2
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
8/12
8Rosai- Dorfman DiseaseA Case Report
Table- 3
with a central linear density and a striated
appearance.
The differential diagnosis is made with
lymphoreticular malignancies such as
lymphomas, Hodgkin's disease, malignant
histiocytosis and monocytic leukaemia, all
of which have similar histopathological
features. Atypias in cytology and the
aggressive clinical course establish the
diagnosis in most cases. Other
histiocytoses, such as rhinoscleromas,
Wegener's granulomatosis, may also be
included in the differential diagnosis
(Table-2).Although in most patients the
extent of SHML does not appear to
determine disease outcome, recent reports
have documented that infiltrates of SHML
can cause death.
Age Sex Clinical presentation Location of the disease
involvament
2.5 M Neck masses, autoimmune
haemolytic Anaemia
Nodal
5 F Neck masses Nodal38 M Neck mass Nodal
30 F Neck mass, elevated ESR Nodal and extranodal
33 M Neck mass, facial swelling Nodal and extranodal
56 M Neck masses Nodal and extranodal
75 M Left parotid and left neck
mass
Nodal and extranodal
12 F Right eye swelling Nodal and extranodal51 M Left-sided
headaches Extranodal without lymphadenopathy
68 M Difficulty walking, ataxia,
falls
Extranodal without lymphadenopathy
20 F Facial pain Extranodal without lymphadenopathy
22 F Right cheek mass, sinus
disease,
no palpable lymph
enlargement
Extranodal without lymphadenopathy
19 F Facial swelling, sinus disease Extranodal without
lymphadenopathy
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
9/12
9Rosai- Dorfman DiseaseA Case Report
Management of the Rosai-Dofman disease
has no ideal protocol, because it is an
uncommon, self-limited disease,
frequently requires no therapy. When
lymph node or extranodal tissue
enlargement causes significant symptoms,
such as airway obstruction or compression
of vital organs treatment is mandatory.
Pulsone at al. reviewed 80 cases published
between 1969 and 2000; 50% of these
cases required no treatment, of which 82%
had full remission18.The role of surgery is
mostly for biopsies and to relieve
obstruction. Local recurrence is frequent
following surgical resection. The role of
radiotherapy is not well understood; some
reports have described full resolution with
this treatment, while others have shown no
response1. Steroids often resolve fever and
reduce lymph node size. Chemotherapy
has yielded controversial results. Further
investigations need to study the possible
efficacy of methotrexate and 6-
mercaptopurine. Use of alpha-interferon
has been limited because of its side effects.
Higher mortality rate is seen in patientswith immunological
abnormalities at or
before presentation.
If a diagnosis of RosaiDorfman disease is
made, the patient can be initially observed
with the hope of spontaneous remission.
For tumours exclusively located in an
anatomic site amenable to surgery,
surgical excision may be considered when:
(i) the lesion persists or recurs; (ii)
cytologic findings are inconclusive; or (iii)
the patient has symptoms or desire for
removal.
References
1. Carpenter RJ III, Banks PM, McDonald TJ, Sanderson DR.
Sinus
histiocytosis with massive
Lynphadenopathy (Rosai-Dorfman
disease): Report of a case with
respiratory tract involvement.
Laryngoscope 1978;88:1963-9.
2. Cheng SP, Jeng KS, Liu CL.Subcutaneous Rosai-Dorfman
disease: is surgical excision
justified? J Eur Acad Dermatol
Venereol. 2005;19:747-50.
3. Chu P, LeBoit PE. Histologicfeatures of cutaneous sinus
histiocytosis (Rosai-Dorfman
disease): study of cases both with
and without systemic involvement.
J Cutan Pathol 1992; 19: 201206.
4. Deodhare SS, Ang LC, and BilbaoJM. Isolated intracranial
involvement in Rosai-Dorfman
disease: a report of two cases and
a review of the literature. Arch
Pathol Lab Med 1998; 122: 161-
165.
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
10/12
10Rosai- Dorfman DiseaseA Case Report
5. Donald V. La Barge III,Karen L.Salzman,H. Ric
HarnsbergerSinus
Histiocytosis with Massive
Lymphadenopathy (Rosai-Dorfman
Disease): Imaging Manifestations
in the Head and Neck AJR:191;
December 2008;299-306.
6. Eiras JC, Schettini APM, de LimaLL. Cutaneous
Rosai-Dorfman
disease ; a case report. An Bras
Dermatol. 2010;85(5):687-690
7. Eisen R N, Buckley PJ, Rosai J:Immunophenotypic
characterization of sinus
histiocytosis with massive
lymphadenopathy (Rosai- Dorfman
disease): Semin Diagn Patho
1990;7:74.
8. Foucar E, Rosai J, Dorfman RF.Sinus histiocytosis with
massive
lymphadenopathy (Rosai-Dorfman
disease): review of the entity.
Semin Diagn Pathol 1990; 7:1973
9. GULL MOHD BHAT, SURENDERKUMAR, ATUL SHARMA, Rosai-
dorfman disease : a case report
with review of literature. Indian
journal of medical & paediatric
oncology 2004 vol. 25 no.4; 39-41.
10.H Y Huang,, C L Yang, W J ChenRosai-Dorfman Disease with
Primary Cutaneous
ManifestationsA Case
Report,Ann Acad Med Singapore
1998; 27:589-93
11.Hazarika P, Nayak DR,Balakrishnan R, Kundaje HG, Rao
PL. Rosai-Dorfman disease of the
subglottis. J Laryngol Otol 2000;
114:970-3.
12.Huang HY, Yang C L, Chen W JRosai-Dorfman Disease with
Primary Cutaneous
ManifestationsA Case Report
Annals Academy of Medicine July
1998, Vol. 27 No. 4: 589-91.
13.Jaffe R,Vaughan De.,LanghoffE:Fascin and differential
diagnosis
of childhood histiocytic lesions.
Pediatrol &Dev Pathol
1998;1:216.
14.Juskevicius R, and Finlay JL.Rosai-Dorfman disease of the
parotid gland, cytologic and
histopathologic findings with
immunohistochemical correlation.
Arch Pathol Lab Med 2001; 125:
1348-1350.
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
11/12
11Rosai- Dorfman DiseaseA Case Report
15.Kroumpouzos G, Demierre M. F.Cutaneous Rosai-Dorfman
Disease: Histopathological
Presentation as Inflammatory
Pseudotumor: A Literature Review.
Acta Derm Venereol 2002; 82:
292296.
16.Lauwers GY, Perez-Atayde A,Dorfman RF, et al. The
digestive
system manifestations of Rosai-
Dorfman disease (sinus
histiocytosis with massive
lymphadenopathy): review of 11
cases. Hum Pathol 2000; 31: 380-
385.
17.McAlister WH, Herman T, DehnerLP. Sinus histiocytosis
with
massive lymphadenopathy (Rosai-
Dorfman disease). Pediatr Radiol
1990; 20:425432
18.Pulsoni A, Anghel G, Falcucci P,Matera, R Pescarmona,
Ribersani
M: Treatment of Sinus
Histiocytosis Whit Massive
Lynfadenopathy (Rosai-Dorfman
Disease): Report of a case and
literature Review. Am J Hematol
2000; 69:61-71.
19.Siriwardena . B.S.M.S.,Tilakaratne W.M., Amaratunga
E.A.P.D, Peiris A.M.O.A case
report of Rosai Dorfman Disease
of the parotid gland Sri Lanka
Journal of Medicine 2004; 13(02)
41-43
AcknowledgementI would be gratefully acknowledging
thecollaboration of Dr. A. M.O Peiris forproviding assistance in
making thisproject a reality and Dr. Amith and Dr.Samadara
Siriwardena for providingvaluable information, photographs for
theproject report.I would give my sincerer gratitude forthe
academic staff of the department oforal pathology Prof. W.M
Thilakarathne,Prof. E. A. P. Amarathunga, Dr.Primalijayasooriya,
and Dr. SamadaraSiriwardena for sharing their pricelessknowledge
and precious experience.Last but not least I thank for all
whocontributed including dental librarystaff, technicians.
-
8/3/2019 Rosai-Dorfman disease (RDD)/ sinus histiocytosis with
massive lymphadenopathy
12/12
12Rosai- Dorfman DiseaseA Case Report