Embed Size (px)
Citation preview
1
Margaret Soper, HMS IVGillian Lieberman, M.D.
Langerhans Cell HistiocytosisMargaret Soper, Harvard Medical School IV
Gillian Lieberman, M.D.
July 2004
2
Margaret Soper, HMS IVGillian Lieberman, M.D.
Outline• What is Langerhans cell histiocytosis?• Radiology of skull and lung lesions
– Patient MK• Different types of common skull lesions
– Patient JS• Involvement of other bones
– Patient TJ• Where else do we see LCH?
3
Margaret Soper, HMS IVGillian Lieberman, M.D.
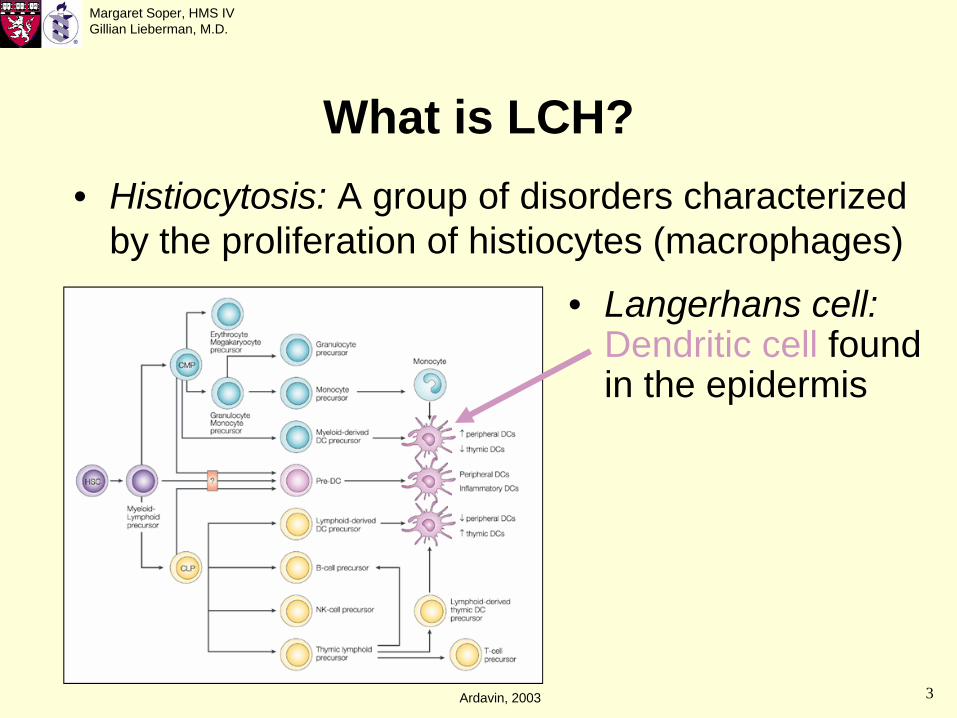
What is LCH?• Histiocytosis: A group of disorders characterized
by the proliferation of histiocytes (macrophages)
• Langerhans cell: Dendritic cell found in the epidermis
Ardavin, 2003

4
Margaret Soper, HMS IVGillian Lieberman, M.D.
What is LCH?• Langerhans cell histiocytosis: Clonal
proliferation of Langerhans cells in one or many organs: Bone, skin, lungs, brain, soft tissues, other organs
• Thought to be caused by abnormal response to infection

5
Margaret Soper, HMS IVGillian Lieberman, M.D.
A disease of many names• Histiocytosis X (Lichtenstein, 1953)
– Eosinophilic granuloma: Localized bone disease– Hand-Schüller-Christian disease: Skull lesions,
proptosis, and diabetes insipidus– Letterer-Siwe disease: Disseminated histiocytosis
• Langerhans cell histiocytosis (1973)
6
Margaret Soper, HMS IVGillian Lieberman, M.D.
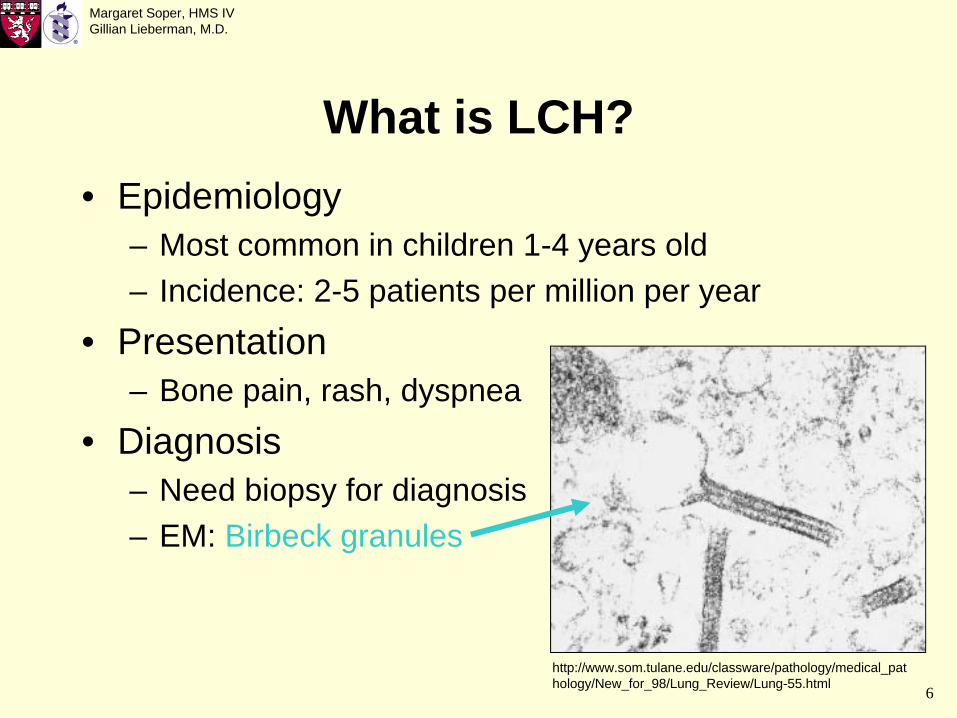
What is LCH?• Epidemiology
– Most common in children 1-4 years old– Incidence: 2-5 patients per million per year
• Presentation– Bone pain, rash, dyspnea
• Diagnosis– Need biopsy for diagnosis– EM: Birbeck granules
http://www.som.tulane.edu/classware/pathology/medical_pat hology/New_for_98/Lung_Review/Lung-55.html

7
Margaret Soper, HMS IVGillian Lieberman, M.D.
Treatment and prognosis• Restricted (no visceral organs involved)
– Treatment: Observation, local radiation, corticosteroid injection, excision
– Prognosis is good• Extensive (visceral organs involved)
– Treatment: Chemotherapy, corticosteroids– Worse prognosis: 50% mortality with disseminated
disease
8
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient MK• Two-year-old girl who presented with a
rapidly-growing bump on her head• Head CT showed parietal bone lesions
http://www.gwc.maricopa.edu/class/bio201/skull/latskul.htm

9
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient MK: CT head w/ contrast• Well-defined lytic
lesions in the R and L parietal bones
• Bone is the most common site of LCH lesions; skull is involved in 30%
• Classic skull lesions: Round, osteolytic, with sharp borders
• Ddx: Mets, venous lakes
Children’s Hospital Boston

10
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient MK: CT head w/ contrast
• What classic feature of LCH skull lesions is seen here?
Children’s Hospital Boston

11
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient MK: CT head w/ contrast
• Classic feature of LCH skull lesions: On tangential views, a beveled edge appearance
Children’s Hospital Boston

12
Margaret Soper, HMS IVGillian Lieberman, M.D.
LCH of skull: Plain skull film
Caldemeyer et al., 2001
• In this similar patient, we see well-defined lytic lesions, one with a beveled edge

13
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient MK• MK was confirmed to have LCH by biopsy• Patients with LCH need a skeletal survey:
– CXR– AP films of all long bones– AP film of pelvis– Lateral spine films
• Bone lesions need CT evaluation to determine treatment
• Look for visceral involvement if the patient has symptoms

14
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient MK• MK’s skeletal survey showed a lesion in her
scapula• A chest CT to evaluate the scapular lesion
also revealed lung involvement

15
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient MK: CT chest w/ contrast• MK’s chest CT
shows multiple nodular opacities in the RML
• Nonspecific, but likely LCH in this patient
• This is evidence of extensive disease, so MK received chemotherapy
Children’s Hospital Boston

16
Margaret Soper, HMS IVGillian Lieberman, M.D.
Pulmonary LCH• Lung is involved in 23-50% of patients• Work up pulmonary symptoms with CXR,
then CT

17
Margaret Soper, HMS IVGillian Lieberman, M.D.
Pulmonary LCH: CXR• Classic CXR
findings: Reticulonodular opacities most prominent in the upper and mid lung fields
• LCH spares the lower lobes
http://www.histio.org/society/LCH/Adult/vassallo1.shtml

18
Margaret Soper, HMS IVGillian Lieberman, M.D.
Pulmonary LCH: CT chest w/ contrast
Schmidt et al., 2004
• Classic chest CT findings in extensive disease: Reticulonodular changes, large cysts, and destruction of lung parenchyma
• Cysts bullaepneumothorax
• Ddx: PCP, TB, LIP
19
Margaret Soper, HMS IVGillian Lieberman, M.D.
LCH of skull• Patient MK had skull and lung findings• Let’s return to the skull, an important site of
involvement for LCH• We’ve seen LCH involving the parietal bones
http://www.gwc.maricopa.edu/class/bio201/skull/latskul.htm

20
Margaret Soper, HMS IVGillian Lieberman, M.D.
LCH of skull• There are three other common sites of LCH
lesions in the skull, each associated with a classic presentation or finding
• The first: Mastoid involvement can spread to
http://www.gwc.maricopa.edu/class/bio201/skull/latskul.htm
the bones of the middle ear deafness
21
Margaret Soper, HMS IVGillian Lieberman, M.D.
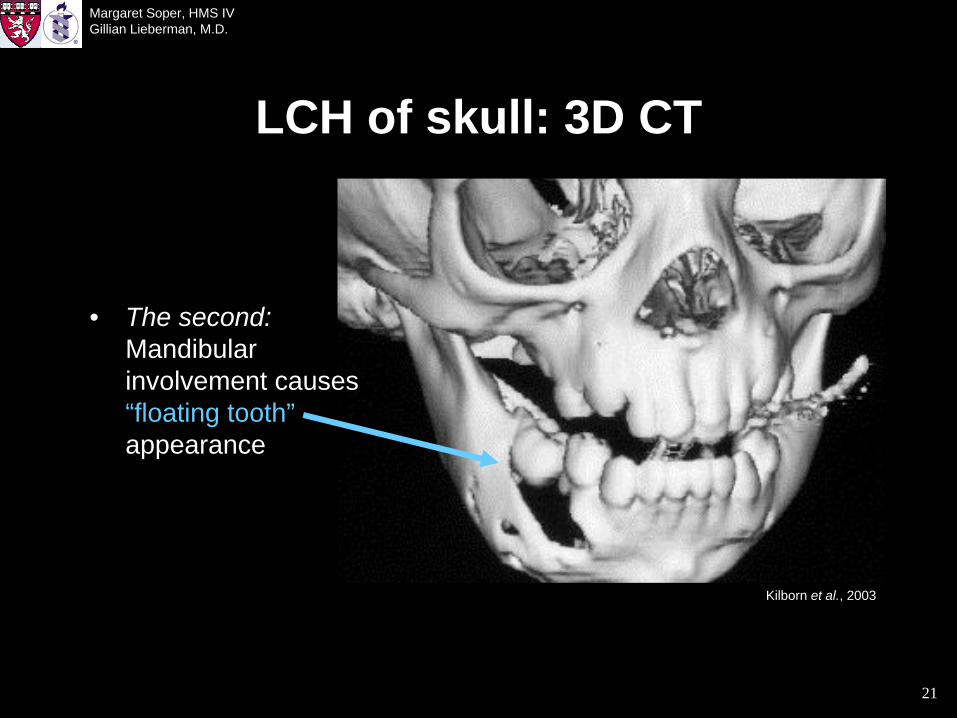
LCH of skull: 3D CT
Kilborn et al., 2003
• The second: Mandibular involvement causes “floating tooth” appearance
22
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient JS• The third: Orbital wall involvement, as
illustrated by patient JS• One-year-old boy who presented with a rash,
which on biopsy showed LCH• Skeletal survey showed L orbital involvement
23
Margaret Soper, HMS IVGillian Lieberman, M.D.
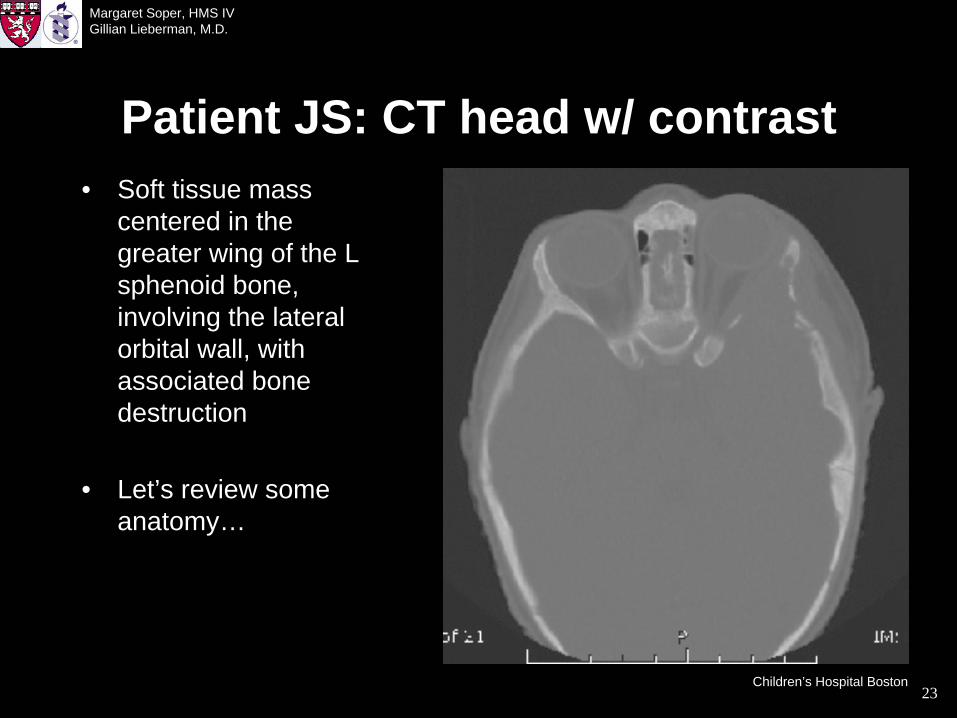
Patient JS: CT head w/ contrast• Soft tissue mass
centered in the greater wing of the L sphenoid bone, involving the lateral orbital wall, with associated bone destruction
• Let’s review some anatomy…
Children’s Hospital Boston

24
Margaret Soper, HMS IVGillian Lieberman, M.D.
Skull anatomy
• JS’s lesion involved the greater wing of the sphenoid on the L
http://www.csuchico.edu/anth/Module/skull.html
Sphenoid bone:

25
Margaret Soper, HMS IVGillian Lieberman, M.D.
• The greater wing of the sphenoid forms part of the lateral orbital wall
Skull anatomy
http://www.oculoplastics.com/topics/tumors_orbit/orbital_tumors_anatomy.htm#volume

26
Margaret Soper, HMS IVGillian Lieberman, M.D.
LCH of skull• The third common skull lesion: Orbital wall
involvement proptosis (downward displacement of orbit)
• Hand-Schüller-Christian disease: Skull lesions, proptosis, and diabetes insipidus
• Summary of common skull lesions:– Mastoid involvement deafness– Mandibular involvement floating tooth– Orbital wall involvement proptosis

27
Margaret Soper, HMS IVGillian Lieberman, M.D.
LCH of bones• What about the rest of the
skeleton?• Radiologically, these
lesions look different than skull lesions
• LCH can occur in any bone except those of hands and feet
• Most common sites of involvement: Skull, ribs, pelvis, femur
Skull
Ribs
FemurPelvis
Howarth et al., 1999

28
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient TJ• Six-year-old boy who presented with pain in
his L arm after falling on it
29
Margaret Soper, HMS IVGillian Lieberman, M.D.
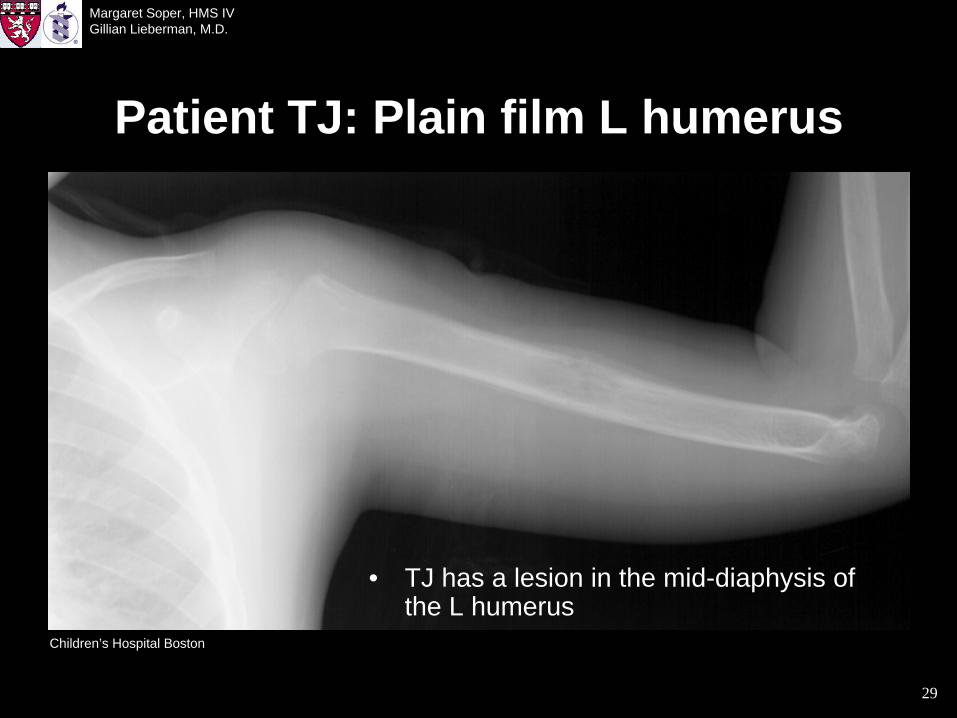
Patient TJ: Plain film L humerus
• TJ has a lesion in the mid-diaphysis of the L humerus
Children’s Hospital Boston
30
Margaret Soper, HMS IVGillian Lieberman, M.D.
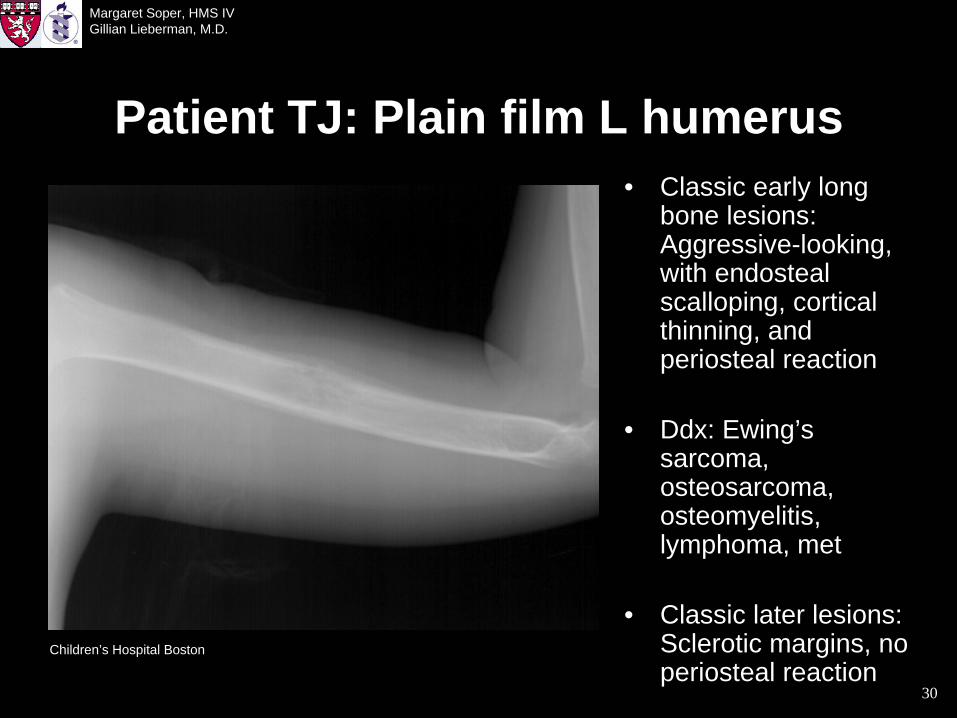
Patient TJ: Plain film L humerus• Classic early long
bone lesions: Aggressive-looking, with endosteal scalloping, cortical thinning, and periosteal reaction
• Ddx: Ewing’s sarcoma, osteosarcoma, osteomyelitis, lymphoma, met
• Classic later lesions: Sclerotic margins, no periosteal reaction
Children’s Hospital Boston

31
Margaret Soper, HMS IVGillian Lieberman, M.D.
Patient TJ: T1 MR L humerus• Ill-defined, hypointense lesion
involving the marrow and cortex of the humerus, with an associated soft tissue mass
• Typical T1 MR appearance for LCH outside the skull
• 30% have an associated soft tissue mass
Children’s Hospital Boston
32
Margaret Soper, HMS IVGillian Lieberman, M.D.
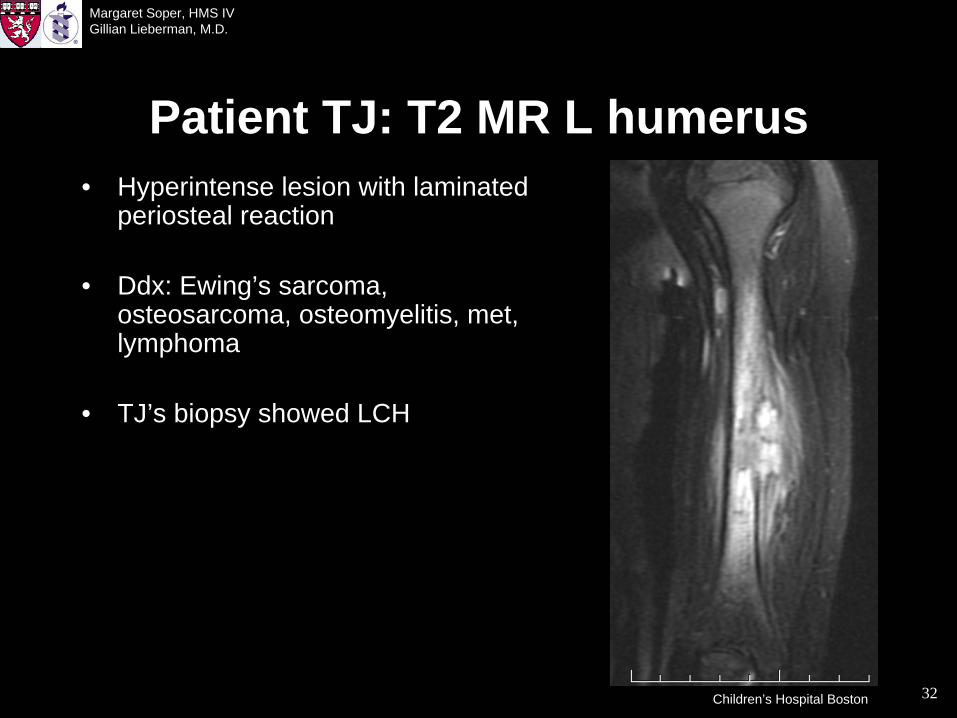
Patient TJ: T2 MR L humerus• Hyperintense lesion with laminated
periosteal reaction
• Ddx: Ewing’s sarcoma, osteosarcoma, osteomyelitis, met, lymphoma
• TJ’s biopsy showed LCH
Children’s Hospital Boston

33
Margaret Soper, HMS IVGillian Lieberman, M.D.
Where else do we see LCH?• We have focused on bone and lung, the most
common sites for radiologically-identifiable LCH lesions
• LCH can be seen radiologically in:– CNS, especially pituitary– Liver, spleen, and biliary system– Lymph nodes– Soft tissues– GI tract
34
Margaret Soper, HMS IVGillian Lieberman, M.D.
Acknowledgements• Gillian Lieberman, M.D.• Pamela Lepkowski• Larry Barbaras• Christine Duncan, M.D.• Matthew Jolley, M.D.• Fabio Komlos, M.D.• Alexander Guimaraes, M.D., Ph.D.

35
Margaret Soper, HMS IVGillian Lieberman, M.D.
References• Ardavin C. Origin, precursors and differentiation of mouse dendritic
cells. Nature Reviews Immunology 2003; 3: 582-590.• Caldemeyer KS, Parks ET, Mirowski GW. Langerhans cell histiocytosis.
Journal of the American Academy of Dermatology 2001; 44: 509-511.• Egeler RM, D’Angio GJ. Langerhans cell histiocytosis. The Journal of
Pediatrics 1995; 127: 1-11.• Howarth, DM, Gilchrist GS, Mullan BP, Wiseman GA, Edmonson JH,
Schomberg PJ. Langerhans cell histiocytosis: Diagnosis, natural history, management, and outcome. Cancer 1999; 85: 2278-2290.
• Kilborn TN, Teh J, Goodman TR. Paediatric manifestations of Langerhans cell histiocytosis: a review of the clinical and radiological findings. Clinical Radiology 2003; 58: 269-278.
• Schmidt S, Eich G, Hanquinet S, Tschäppeler H, Waibel P, Gudinchet F. Extra-osseous involvement of Langerhans cell histiocytosis in children. Pediatric Radiology 2004; 34: 313-321.





























