Embed Size (px)
Citation preview

Rome, 9 -11 October 2013
Università Cattolica del Sacro CuoreSala Italia - Centro Congressi Europa
Honorary President:Rocco Bellantone
Presidents:John WatkinsonPresident, British Association of Thyroid & Endocrine Surgeons
Celestino P. Lombardi
Local Organizer: Marco Raffaelli
U.O. Chirurgia Endocrina e Metabolica(Head R. Bellantone)
U.O. Chirurgia Endocrina CIC (Head C.P. Lombardi)
Gruppo SC Studio Congressi Servizi per la Comunicazione
Bhavnita Borkhatria Patel
BAETS Administrator35 - 43 Lincoln’s Inn FieldsLondonWC2A 3PEWebsite: www.baets.org.ukDirect dial: +44.20.7304.4771Email: [email protected]: +44.20.74309235
OrgAnIzEr SECrETArIAT
Via n. Colajanni, 4 - 00191 romaTel. +39.06.3290250 - Fax [email protected] - www.grupposc.com
British Association of
Endocrine and Thyroid Surgeons (BAETS)
EXECUTIVE COMMITTEE President
Mr John Watkinson (Birmingham)
President Elect
Mr David Scott Coombes (Cardiff)
Secretary
Mr Ashu Gandhi (Manchester)
Treasurer
Mr Jeremy Davis (Medway, Kent)
Director of Audit
Mr David Chadwick (Chesterfield)
Members of Executive
Mr Fausto Palazzo (Hammersmith, London)
Mr Anthony Skene (Bournemouth)
Mr Radu Mihai (Oxford)
Ms Alison Waghorn (Liverpool)
General Information
VENUE Sala Italia – Centro Congressi Europa Università Cattolica del Sacro Cuore, Policlinico ‘A. Gemelli’, Largo Francesco Vito 1, 00168 Roma (entrance to the Europe Congress Centre – Sala Italia) How to reach the Centro Congressi Europa – Sala Italia: Arrival by Public Transport: From Termini Station: underground (Line A – destination Battistini) to Valle Aurelia then Local Train FM3 (destination "Roma-Viterbo") and descend at "Gemelli" station (three stops) in Via Pineta Sacchetti. Walk then for about 500 mt. until Largo Francesco Vito entrance (after Largo Gemelli entrance where is also located the TAXI POINT) From Tiburtina Station: take FR1 train to Ostiense station then change for the FM3 train (direction Trastevere - S. Pietro-Viterbo), getting off at Gemelli stop in Via Pineta Sacchetti. Walk then for about 500 mt. until Largo Francesco Vito entrance (after Largo Gemelli entrance where is also located the TAXI POINT) Underground: from Valle Aurelia, Cornelia or Battistini resurface and take one of the following buses that stop outside the Gemelli Hospital in Via Pineta Sacchetti (walk then for about 200 mt. until Largo Francesco Vito entrance (after Largo Gemelli entrance where is also located the TAXI POINT ) LINE 994: (Valle Aurelia - Pineta Sacchetti - Gemelli Hospital - San Filippo Neri) LINE 446: (Circonvallazione Cornelia - Pineta Sacchetti - Gemelli Hospital - Cortina d'Ampezzo - Piazza Mancini) LINE 146: (Battistini - Pineta Sacchetti - Gemelli Hospital) By motorway From Naples take the G.R.A. – exit Via Aurelia (city centre); from L’Aquila/Florence take the G.R.A. – exit Via Flaminia – Via Cortina d’Ampezzo – Via Trionfale Arrival by Taxi: From: Rome/Leonardo Da Vinci-Fiumicino Airport - FCO Estimated taxi fare: 55.00 EUR (one way) From: Rome/Ciampino Airport - CIA Estimated taxi fare: 60.00 EUR (one way) From Fiumicino airport By car: From Rome’s main airport take on the G.R.A. Via Aurelia exit 1 and continue until Piazza Irnerio towards C. Cornelia – Piazza dei Giureconsulti until Via della Pineta Sacchetti. By train: Fiumicino Station: take FR1 train to Trastevere station then change for the FM3 train (direction Cesano or Bracciano or Viterbo), getting off at Gemelli stop in Via Pineta Sacchetti. Walk then for about 500 mt. until Largo Francesco Vito entrance (after Largo Gemelli entrance)
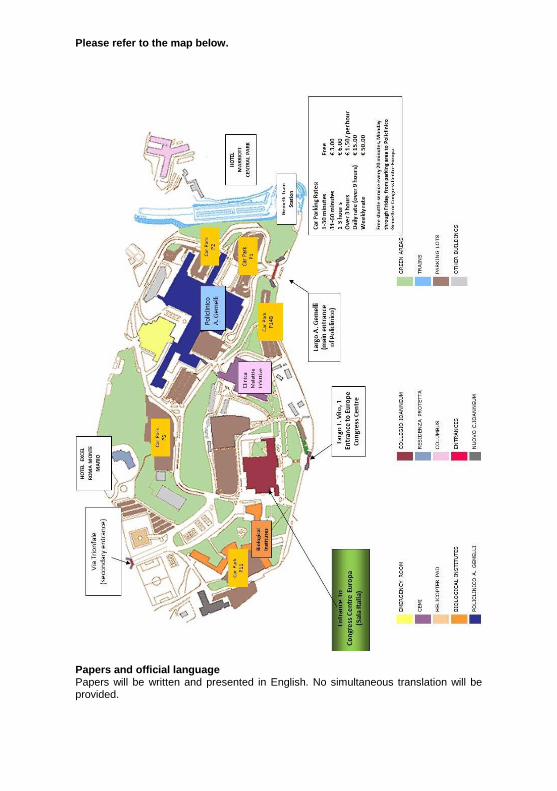
Please refer to the map below.
Papers and official language Papers will be written and presented in English. No simultaneous translation will be provided.
Registration
Early Bird until 9th
October 2013
On site
BAETS Full Member £220 £230
BAETS Affiliate
Member
£150 £170
Nurses £120 £140
Non BAETS Member £220 £240
*Please note BAETS members will receive a £10 discount upon check out. Nurses have a discount factored into the fee.
Continuing Professional Development
A Certificate of Attendance will be included in your Registration Pack and can be used to claim your CPD points as follows:
New Technologies & Ultrasound procedures for Endocrine &
Thyroid Surgeons
3 Points
BAETS Annual Scientific Meeting 10 Points
IONM in thyroid and parathyroid surgery: reality, myths and
pitfalls
5 Points
BAETS Annual Dinner
Thursday 10th
October 2013 Venue: Palazzo Colonna Dress Code: Lounge suits Price: £70
Wednesday 9 October 2013 Pre-meeting course
15.00 – 15.10 Welcome 15.10 – 17.00 US and US-guided operative procedures for endocrine
and thyroid surgeons: Chairmen: S. Aspinall, A. Pontecorvi, L. Rosato
Ultrasound Imaging: new technologies in tissue characterization P. Maceroni
Ultrasound-guided aspiration cytology - When to perform cytological examination:
How to do it E. Traini
- Cytological classification. Immunohistochemical and molecular markers G. Fadda
Controversies in US-interventional techniques - Percutaneous Ethanol Injection (PEI)
E. Papini - Percutaneous Laser Ablation (PLA)
G. Stecconi Bortolani - Percutaneous Radiofrequency Ablation (RFA)
P. Limone
Critical comments S.M. Corsello
Endocrinological perspectives: M.L. Appetecchia, M. Cappa, C. Durante, A. Giaccari,
A. Grossi, C. Panunzi, G. Reda, D. Van Doorne
17.00 - 18.30 New technologies in Endocrine Surgery Chairmen: F. Palazzo, A. Barbarisi
Haemostatic agents M. Testini
Vessel sealing devices: - US technology - Bipolar technology
G. Docimo
Video-assisted and endoscopic procedures C. De Crea
Robotic procedures L. Brunaud
Panel discussion L. Revelli, M. Boscherini
Thursday 10 October 2013
08.00 - 09.00 Registration 09.00 - 09.10 Welcome 09.10 – 11.40 Video-Symposium on surgical techniques
Minimally invasive, video-assisted, endoscopic and
robotic procedures Chairmen: R. Bellantone, D. Scott-Coombes
Mini-incision parathyroidectomy G. Sadler Endoscopic Parathyroidectomy by the lateral approach F. Sebag IEO minimally invasive approach to differentiated thyroid carcinoma G. Giugliano Video-assisted thyroidectomy C.A. Ambrosini Video-assisted central compartment neck dissection M. Raffaelli Robotic thyroidectomy M. Piccoli The “ways” towards the adrenal glands B. Harrison Transperitoneal laparoscopic adrenalectomy A. Valeri Retroperitoneoscopic and bilateral adrenalectomy C.P. Lombardi Robotic adrenalectomy L. Brunaud
11.40 - 12.00 Coffee break 12.00 - 13.00 Audit session 13.00 - 14.00 Lunch and poster viewing 14.00 - 16.30 Free paper session 1 (BJS papers) Chairmen: G. De Toma, R. Mihai
O1. Thyroid lobectomy for treatment of well differentiated intrathyroid malignancy. I.J. Nixon, I. Ganly, S.G. Patel, F.L. Palmer, M.M. Whitcher, R.M. Tuttle, A. Shaha, J.P. Shah
O2. Temporary post-thyroidectomy hypocalcaemia: not only due to loss of parathyroid function I. Christakis, V.A. Constantinides, K. Nastos, N. Tolley, F. Palazzo
O3. Parafibromin, galectin-3, PGP9.5, Ki67 and cyclin D1: using an immunohistochemical panel to aid in the diagnosis of parathyroid cancer P. Truran, S. Johnson, R. Bliss, T.W.J. Lennard, S. Aspinall
O4. Variations in single/two stage thyroidectomies for cancer may be due to differences in thyroid fine needle cytology provision
B. Ranganathan, S. Thiryayi, R. Swindell, B. Yap, A. Gandhi
O5. Using cumulative summation curve versus funnel plot as an alert for hypocalcaemia rates following total thyroidectomy Z. Awad, A. Yao, F. Palazzo, N.S. Tolley
O6. Near infrared fluorescence imaging of rabbit thyroid and parathyroid glands R. Antakia, P. Gayet, S. Guillermet, T.J. Stephenson, B. Harrison, N.J. Brown, S.P. Balasubramanian
O7. Increasing incidence and survival of thyroid cancer in the West of Scotland – a 20 year experience N.B. Oozeer, G. Konstantinidis, A. Nagatani-Rose, K. Hugh, R.B. Townsley, N. Amiraraghi, D. McLellan, A. Shaukat, N. Reed, L.J. Clark
O8. Exome sequencing of familial non-RET medullary thyroid cancer (MTC) identifies a novel potential disease susceptibility gene. J.A. Smith, N. Wake, C. McCabe, M. Read, J.C. Watkinson, E.R. Maher, E.R. Woodward
O9. Parathyroidectomies in patients with renal failure: the Hull experience R. Srivastava, A. Lamplugh, V. Allgar, C. Snowden, S. Bhandari, S. Atkin, J. England
O10. Clinical outcomes of genotype-directed prophylactic total thyroidectomy in children with germline RET mutation in the UK F. Prete, T. Ezzat, C. Morkane, J. Watkinson, N. Shaw, S. Alvi, R. Squire, B. Harrison, J. Wales, P.
Clayton, F. Eatock,
P. Morrison, D. Carson, C. Brain, P. Hindmarsh, M. Dattani, H. Spoudeas, C. Buchanan, A. Albanese, R. Amin, A. Piero, P. De Coppi, T.R. Kurzawinski
16.30 – 17.00 Coffee Break and poster viewing 17.00 - 18.00 BAETS AGM 2013 20.00 BAETS Annual Dinner and BJS Prize
Friday 11 October 2013
08.30 - 10.30 Free papers session 2 Chairmen: G. Gasparri, A. Waghorn
O11. The value of continuous neuromonitoring in thyroid surgery for prediction of postoperative vocal cord function in surgeries with intraoperative recovery of loss of signal R. Schneider, K. Lorenz, C. Sekulla, P.N. Thanh, A. Machens, H. Dralle
O12. Observation of clinically negative central compartment lymph nodes in papillary thyroid carcinoma I.J. Nixon, I. Ganly, S.G. Patel, L.G. Morris, F.L. Palmer, D. Thomas, R.M. Tuttle, J.P. Shah, A.R. Shaha
O13. Does post-operative parathyroid hormone predict early hypocalcaemia following parathyroidectomy and total thyroidectomy? K. Hiew, R. Trivedi, R. Hardy
O14. A randomized clinical trial comparing open superficial cervical plexus block versus standard incisional anaesthesia in thyroid and parathyroid surgery. R.J. Egan, J.C. Hopkins, A.J. Beamish, R. Shah, A.G. Edwards, J.D.T. Morgan
O15. Recurrent laryngeal nerve monitoring via continuous vagal nerve stimulation during thyroid surgery S. Ifeacho, R. Nash, G. Mochloulis
O16. The evidence base for a randomised controlled trial in the management of differentiated thyroid cancer: lessons from a systematic review W. Craig, S. Fielding, C. Ramsay, Z. Krukowski
O17. Intraoperative nerve monitoring is used by a small (but slowly increasing) minority of members of British Association of Endocrine and Thyroid Surgeons (BAETS) R. Mihai, D. Chadwick
O18. Reoperative parathyroid surgery in the era of focused primary procedures A.C. Walker, J.G.H. Hubbard, J.J. Fraile
O19. Minimally invasive video-assisted thyroidectomy (MIVAT) and thyroiditis: retrospective analysis of 391 cases. New inclusion criteria? B. De Simone, P. Del Rio, M. Sianesi
O20. Incidence and predictors of post-thyroidectomy hypocalcaemia in a tertiary endocrine surgical unit O. Edafe, P. Prasad, B.J. Harrison, S.P. Balasubramanian
O21. Normocalcemic primary hiperparathyroidism: could we use intraoperative PTH measure? J. Jimeno, A. Walker, J. Hubbard
O22. Ipsilateral central neck dissection plus frozen section examination Vs prophylactic bilateral central neck dissection in cN0 papillary thyroid carcinoma A. D’Amore, M. Raffaelli, C. De Crea, L. Sessa, S.E. Tempera, C. Bellantone, C.P. Lombardi
10.30 – 11.00 Coffee break and poster viewing
11.00 - 11.15 Best Poster prize 11.15 - 12.15 BJS lecture:
Prevention and management of iatrogenic hypoparathyroidism
A. Sitges-Serra Chairman: J. Watkinson 12.15 - 13.15 Lunch 13.15 - 14.15 Free-paper session 3 Chairmen: S. Filetti, J. Hubbard
O23. Evaluation of Salford Royal Foundation Trust’s management of adrenal incidentaloma – is the duration of radiological follow up necessary? R. Brindle, A. Thomson, A. Mukherjee, T. Kearney, I. Anderson, H. Doran
O24. Binding of Helix Pomatia agglutinin glycoproteins is a predictor of poor survival in adrenal cancers. M. Heetun, G.P. Sadler, R. Mihai, S. Brooks, P. Rajeev
O25. Variations in the post-op management of primary hyperparathyroidism in the UK J. Barnes, A. Midgley-Hunt, S. Thrush
O26. FNA versus Rotex biopsy in thyroid nodules; effect on Bethesda 1 scores. A. Huibers, T. Klooker, K. Hof, S. van Eeden, P.H. Bisschop, E.J.M. Nieveen van Dijkum.
O27. Quantification of lymph nodes in the central compartment of the neck: an anatomical cadaveric study. E. Ofo, S. Thavaraj, P.D. Cope, J.P. Jeannon, R. Oakley , K. Kapoor, E. Odell, C. Lock, R. Simo
O28. Papillary thyroid microcarcinoma - therapeutic/follow up trends in UK N. Charaklias, T. Mazhar, S. Atkin, J. England
14.15 Close of the 33
rd Annual Meeting of the BAETS
Post-meeting Symposium
14.15 - 18.00 IONM in thyroid and parathyroid surgery: reality, myths and pitfalls Chairmen: G.W. Randolph, H. Dralle, R. Bellantone IONM 2013 State of The Art: G.W. Randolph Different IONM devices: - Medtronic: G.W. Randolph - Langer: S. Van Slycke - Inomed: M. Kirkup IONM study group report: H. Dralle Is there still a role for neurostimulation with laryngeal palpation in the era of vagal nerve continuous stimulation? O. Piccin
Superior laryngeal nerve monitoring: M. Barczynski Staged thyroidectomy: is it justified? A. Sitges-Serra Final remarks - Technical perspectives: G. Dionigi - Medico-legal implications: C.P. Lombardi Panel discussion: G. Ardito, N. Avenia, M. Boniardi, C. Bellotti, A. Biondi, P.G. Calò, A. Camaioni, M.A. Cannizzaro, A. Catania, M.G. Chiofalo, G. Conzo, L. D’Alatri, M. De Palma, P. Del Rio, P. Gentileschi, L. Giacomelli, E. Leopaldi, M.R. Marchese, P. Marini, A. Pezzolla, L. Pezzullo, S. Sorrenti, F. Tartaglia, M. Piemonte, A. Zaccaroni
18.00 End of symposium
Oral Presentations
O1. Thyroid lobectomy for treatment of well differentiated intrathyroid malignancy. I.J. Nixon1, I. Ganly1, S.G. Patel1, F.L. Palmer1, M.M. Whitcher1, R.M. Tuttle2, A. Shaha1, J.P. Shah1 1Department of Head and Neck Surgery/2Department of Endocrinology, Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York, NY, 10065, USA Background. There remains controversy over the type of surgery appropriate for T1T2N0 well differentiated thyroid cancers (WDTC). Current guidelines recommend total thyroidectomy for all but the smallest lesions, despite previous evidence from large institutions suggesting that lobectomy provides similar excellent results. The objective of this study was to report our experience of T1T2N0 WDTC managed by either thyroid lobectomy or total thyroidectomy. Methods. Eight hundred and eighty nine patients with pT1T2 intrathyroid cancers treated surgically between 1986 and 2005 were identified from a database of 1810 patients with WDTC. Total thyroidectomy was carried out in 528 (59%) and thyroid lobectomy in 361 (41%) patients. Overall survival (OS), disease specific survival (DSS) and recurrence free survival (RFS) were determined by the Kaplan Meier method. Factors predictive of outcome by univariate and multivariate analysis were determined using the log rank test and Cox proportional hazards method respectively. Results. With a median follow up of 99 months the 10 year OS, DSS and RFS for all patients were 92%, 99% and 98% respectively. Univariate analysis showed no significant difference in OS by extent of surgical resection. Multivariate analysis showed that age over 45y and male gender were independent predictors for poorer OS, whereas T stage and type of surgery were not. Comparison of the thyroid lobectomy group and the total thyroidectomy group showed no difference in local recurrence (0% for both) or regional recurrence (0% versus 0.8%, p=0.96). Conclusion. Patients with pT1T2 N0 WDTC can be safely managed by thyroid lobectomy alone.

O2. Temporary post-thyroidectomy hypocalcaemia: not only due to loss of
parathyroid function I. Christakis, V.A. Constantinides, K. Nastos, N. Tolley, F. Palazzo Department of Endocrine and Thyroid Surgery, Imperial College NHS Trust, Hammersmith Hospital, Du Cane Road, London, W12 0HS Background. Post-operative hypocalcaemia is common after thyroid surgery and is attributed to the loss of parathyroid function. The high rate of temporary hypocalcaemia on departmental audit was ascribed to the higher BAETS definition of hypocalcaemia at 2.1mmol/l and the liberal use of parathyroid autotransplantation. Whilst permanent hypoparathyroidism is a universally accepted quality measure in thyroid surgery temporary hypocalcaemia is still perceived as a measure of technical proficiency. The goal of this study is to establish whether post-operative hypocalcaemia relates exclusively to parathyroid function after thyroid surgery. Methods. Data on patients undergoing total thyroidectomy between 2008 and 2012 were retrospectively reviewed. Patients having reoperative surgery, those requiring a sternotomy or patients with concurrent hyperparathyroidism were excluded. Variables analyzed included demographics, pre-operative calcium, PTH, phosphate, Vitamin D levels. Chi-square test was performed to compare PTH and corrected calcium values. Hypocalcaemia was set at <2.1mmol/l and Hypoparathyroidism at <1.2pmol/l. Routine postoperative calcium was not administered. Results. During the study period, 166 patients satisfied the inclusion criteria: The mean age was 50.83 years and 132 were female (79.5%). Indications for thyroidectomy were multinodular goitre (41.6%), Graves’ disease (31.3%), papillary carcinoma (22.3%), medullary carcinoma (3%) and follicular carcinoma (0.6%) and other (1.2%). Lymphadenectomy was performed in 15% of cases. Hypoparathyroidism and hypocalcaemia at 12-24 hours occurred in 29% and 56.7% of patients respectively (p-value=0.018). Permanent hypoparathyroidism with PTH<1.2 pmol/L and/or requirement for calcium and active vitamin D supplements at 6 months was present in 3.6% of patients . Conclusion. Post-operative serum calcium is a blunt quality measure in thyroid surgery. True temporary hypoparathyroidism is a better measure of parathyroid preservation and whilst common is significantly less common than hypocalcaemia.
O3. Parafibromin, galectin-3, PGP9.5, Ki67 and cyclin D1: using an
immunohistochemical panel to aid in the diagnosis of parathyroid cancer P. Truran, S. Johnson, R. Bliss, T.W.J. Lennard, S. Aspinall Royal Victoria Infirmary, Newcastle, England This research was funded in part by a £5000 grant from BAETS awarded in March 2012. Background. Parathyroid cancer is rare. Differentiating parathyroid carcinoma from degenerative changes at histopathology can be difficult and studies investigating the value of single immunohistochemical markers have had variable results. In this study we aimed to investigate whether a panel of immunohistochemistry markers could aid the diagnosis of parathyroid cancer. Methods. All cases of parathyroid cancer at our institution from 2000 to 2012 were identified retrospectively. Controls with benign parathyroid disease were included for comparison. Immunohistochemistry for Parafibromin, Galectin-3, PGP 9.5, Ki67 and Cyclin D1 were performed by an experienced endocrine pathologist. Results. There were 24 patients with parathyroid cancer and 14 controls. Median pre operative calcium in the cases was 3.02 mmol/L and PTH 260 nmol/L. 16/24 had further surgery with ipslateral thyroid lobectomy and 15 also had a prophylactic level VI lymph node dissection. Apart from one patient with distant metastases at presentation none developed recurrence at follow up (median 28 months). Immunohistochemistry results associated with parathyroid cancer were seen in 14/24 parafibromin, 14/22 Galectin-3, 8/24 PGP9.5, 5/23 Ki67 and 2/21 Cyclin D1. None of the controls had immunohistochemical staining suggestive of cancer. 23/24 patients had at least one immunohistochemical result associated with parathyroid cancer (sensitivity 97%, specificity 100%). Parafibromin or galectin-3 immunohistochemistry suggested cancer in 21/23 cases making these the most useful markers. Cyclin D1 did not suggest malignancy in any case that did not already have another abnormal marker, and so did not add value to the panel in this study. Conclusion. A panel of immunohistochemistry is better than any single marker and can be used to supplement classical histopathology in diagnosing this difficult disease.

O4. Variations in single/two stage thyroidectomies for cancer may be due
to differences in thyroid fine needle cytology provision B. Ranganathan1, S. Thiryayi2, R. Swindell3, B. Yap4, A. Gandhi5 1LAT ENT Surgeon, Pennine Acute Trust, Manchester 2Consultant Cytopathologist, Manchester Cytology Centre, Manchester Royal Infirmary 3Medical Statistics, Christie Hospital, Manchester 4Consultant Oncologist, Christie Hospital, Manchester 5University of Manchester, Manchester Academic Health Sciences Centre, University Hospital of South Manchester Background. Recommended surgical treatment for most thyroid cancers is total thyroidectomy preferably as a single stage procedure (SST). However, cancers diagnosed subsequent to diagnostic lobectomy may need completion thyroidectomy resulting in second operations for patients and subsequent delays in adjuvant treatment. We have noticed significant variation in numbers of SST and two stage thyroidectomies (TST) between hospitals within our cancer network. We explored reasons for this variation using a prospectively collected database containing all cases referred to a regional Thyroid Cancer MDT from 2004-2011 (n=1030) and by conducting a survey of thyroid cytology provision across the network during 2010-2011. Methods. A central university hospital with the highest rate of SST for thyroid cancer (51%) was chosen as “baseline”. Of 14 remaining hospitals within the network 3 were excluded from analysis due to low numbers of thyroid operations and the remaining compared with baseline. We used individual chi-squared tests with Bonferroni correction to explore variation in expected and observed numbers of SST/TST. Analysis of variance (ANOVA) was used to examine reasons for any observed differences. Results. A significant variance in SST/TST was seen between hospitals (p<0.00001). Three hospitals had observed frequencies of SST statistically similar to the reference hospital. The remaining 8 had statistically lower rates of SST with the 2 lowest performing hospitals having rates of 12% (p=0.0004) and 13% (p<0.0001). ANOVA showed that differences were unrelated to patient age, gender, tumour histology or stage. Only the reference hospital had specialist thyroid cytopathologists. The 3 hospitals with similar observed frequencies of SST to baseline hospital each reported 201-300 thyroid cytology cases during the period of the survey. The remaining 8 hospitals reported fewer than 200 cases each which were shared amongst 4-7 pathologists per site. Conclusion. Variation in thyroid cytology provision results in increased TST for patients. Thyroid cytology should be concentrated in high volume centers or those with specialist thyroid cytopathologists. Using cumulative summation curve versus funnel plot as an alert for hypocalcaemia rates following total thyroidectomy

O5. Using cumulative summation curve versus funnel plot as an alert for
hypocalcaemia rates following total thyroidectomy Z. Awad, A. Yao, F. Palazzo, N.S. Tolley Imperial College Healthcare NHS Trust, London Background. Hypocalcaemia is a well-recognised complication of total thyroidectomy irrespective of the indication. The 4th National audit report of The British Association of Endocrine and Thyroid Surgeons (BAETS) used funnel plot to create alert lines and quoted a mean of 27.4% transient and 12.1% permanent hypocalcaemia. We aim to compare funnel plot with cumulative summation (Cusum) curve as means to describe outcomes alert lines. Methods. A retrospective analysis of hypocalcaemia rates after total thyroidectomy for all cases performed at our unit between September 2008–June 2012 using BAETS definitions. The outcomes were incorporated into the BAETS funnel plot and into a Cusum curve to assess the applicability and sensitivity of the two methods. Cases with neck dissection and re-do’s were excluded. Results. 201 total thyroidectomies were performed, 127 by surgeon-1 and 74 by surgeon-2. Overall transient hypocalcaemia rate was 39%(45% for surgeon-1 and 28% for surgeon-2). Permanent hypocalcaemia rate was 5%(3% for surgeon-1 and 7% for surgeon-2). Using funnel plot; these rates fall under the 99% transient hypocalcaemia alert line for surgeon-2 but not surgeon-1. Both were under the 99% alert line for permanent hypocalcaemia. Cusum curve, using the BAETS database mean, showed an “upward curve” (crossing alert lines) for surgeon-1 transient hypocalcaemia rates but a flat one for surgeon two. Both surgeons’ permanent hypocalcaemia Cusum curves were “downward curves” Conclusion. Although both tools showed similar findings, funnel plot shows overall performance compared to a cohort as a snapshot. Cusum curves have a sequential value and can detect change as early as few cases, irrespective of previous performance, which can affect the position on the funnel plot. We will present an amalgamation of the two methods to show performance of an individual surgeon over time, yet compared with a large cohort, this is potentially useful in assessment and revalidation.

O6. Near infrared fluorescence imaging of rabbit thyroid and parathyroid
glands R. Antakia, P. Gayet, S. Guillermet, T.J. Stephenson, B. Harrison, N.J. Brown, S.P. Balasubramanian Department of Oncology and the School of Health and Related Research, University of Sheffield1 Fluoptics, Grenoble, FRANCE2 Background. Near infrared fluorescence (NIR) from intravenous Methylene Blue (MB) is a novel technique to aid parathyroid localisation during thyroid and parathyroid surgery. The aim of this study was to examine MB fluorescence from soft tissues in the rabbit neck and determine the relationship between dose, time and fluorescence from thyroid and parathyroid glands. Methods. Thyroid and external parathyroid glands were exposed in 6 New Zealand White (NZW) rabbits under anaesthesia using a standard protocol. Varying doses of intravenous MB were injected through the marginal ear vein. NIR fluorescence from exposed tissues was recorded at varying time intervals using Fluobeam®700 technology. Specimens of identified glands were taken at the end of procedure for histology. Results. Histology confirmed accurate identification of all excised thyroid and parathyroid tissues. Thyroid and parathyroid glands were the only neck structures to fluoresce; with lower intensities observed in the latter. The parathyroids had shorter peak and quicker washout times at all doses. 0.1 mg/kg of IV MB was adequate to observe fluorescence. MB fluorescence also outlined the parathyroid blood supply. Conclusion. Fluobeam®700 is able to detect fluorescence in thyroid and parathyroid glands at doses as low as 0.1 mg/kg of intravenous MB. These results will guide the development of a protocol for use of IV low-dose MB with Fluobeam®700 in human thyroid and parathyroid surgery. This has the potential to avoid side effects of MB (associated with currently used doses of 3-7mg/kg) and improve outcomes in thyroid and parathyroid surgery.
O7. Increasing incidence and survival of thyroid cancer in the West of
Scotland – a 20 year experience N.B. Oozeer1, G. Konstantinidis1, A. Nagatani-Rose2, K. Hugh1, R.B. Townsley3, N. Amiraraghi1, D. McLellan4, A. Shaukat5, N. Reed5, L.J. Clark1 1Department of Otolaryngology-Head and Neck Surgery, NHS Greater Glasgow and Clyde, Southern General Hospital, 1345 Govan Road, Glasgow, UK 2University of Glasgow, Wolfson Medical School Building, University Avenue, Glasgow, UK 3Department of Otolaryngology-Head and Neck Surgery, NHS Greater Glasgow and Clyde, Glasgow Royal Infirmary, 84 Castle Street, Glasgow, UK 4Department of Pathology, NHS Greater Glasgow and Clyde, Southern General Hospital, 1345 Govan Road, Glasgow, UK 5Beatson Oncology Centre, 1053 Great Western Road, Glasgow, UK Background. Official figures have shown a doubling of the incidence of thyroid cancer in Scotland rising from 1.8 in 1986 to 3.1 per 100 000 in 2010. We aim to audit the incidence and survival of thyroid cancer in the West of Scotland (WoS) and surmise on the possible causes for the observed change. Methods. A prospectively held database of all thyroid cancers treated in the West of Scotland between 1990 and 2011 was retrospectively reviewed. The overall incidence, survival and the disease free survival of 1063 patients with full data was calculated using the Kaplan-Meier method for all histological types. Results. There has been an increase in incidence of thyroid cancer in the WoS by 30% over the last 22 years, which mirrors the trend in Scotland. Other Healthboards did not show a similar pattern of increase. The average age at presentation for papillary cancer (n=669, 63% of sample size) was 47.1±17.0 years (range 8-91), follicular cancer (n=208, 20%) 51.9±18.4 years (range 11-92), medullary cancer (n=68, 6.4%) 54.3±17.6 years (range 3-87), anaplastic cancer (n=63, 6%) 70.5±11.8 years (range 32-94), lymphoma (n=30, 3%) 67.4±15.1 years (range 19-87) and Hurtle cell cancer (n=28. 2.6%) 58.8±21.0 years (range 21-90). Papillary cancer was the predominant histological type and found more commonly amongst the younger age group. Together with an increased incidence of thyroid cancer, there has been a trend of improved overall and disease-free survival especially in the well differentiated thyroid malignancy at 1, 5 and 10 years. Two thirds of the 415 patients where full pathological data was available showed early tumours (pT1 and pT2). Conclusion. Evolution in clinical practice may have been a major factor responsible for the increased thyroid cancer incidence. It is controversial whether a recognized environmental risk factor in Scotland, such as Chernobyl radiation fallouts, can explain the increase.
O8. Exome sequencing of familial non-RET medullary thyroid cancer (MTC)
identifies a novel potential disease susceptibility gene. J.A. Smith, N. Wake, C. McCabe, M. Read, J.C. Watkinson, E.R. Maher, E.R. Woodward School of Clinical and Experimental Medicine. The University of Birmingham. Mindelsohn Way. Edgbaston. Birmingham Background. Between 85% and 98% of familial MTC is caused by a germline mutations of the RET proto-oncogene. There are however, rare families and individuals with predisposition to MTC in whom no RET mutation has been identified (non-RET MTC). The British Thyroid Association (BTA) recommends the investigation of such families as identification of novel candidate genes may inform the molecular behaviour of more common, sporadic disease. Whole exome sequencing (WES) technology enables all protein coding regions of the genome to be sequenced; a novel technique in searching for predisposing genes in MTC. We present our experience and preliminary data using this novel approach. Methods. Patients with non-RET familial and sporadic MTC were recruited through national and internationally developed collaborations. Germline and tumour DNA from three families with non-RET MTC and 63 cases of non-RET sporadic MTC were analysed. WES of affected family members was completed in three generations of the index family. Functional analysis to confirm the biological pathways underlying identified mutations is currently underway. Results. WES identified over 20,000 mutations that were screened using an established protocol. A frameshift mutation has been identified in familial non-RET MTC within a single gene (MTC2) with familial segregation confirmed by Sanger sequencing. Further mutations have been identified in germline DNA from a patient with young onset sporadic disease and in tumour DNA extracted from a patient with sporadic MTC. Preliminary in-vitro studies suggest RET up-regulation in MCF-7 cells transfected with the MTC2 mutant establishing a possible tumorigenic pathway for MTC development. Conclusion. We have established a method of using WES in the context of MTC. Identification of a novel susceptibility gene represents a significant breakthrough in our understanding of MTC. As well as the potential for a genetic test, and as a prognostic biomarker, the on-going functional work may elucidate targets for novel therapies.

O9. Parathyroidectomies in patients with renal failure: the Hull experience
R. Srivastava1, A. Lamplugh2, V. Allgar3, C. Snowden4, S. Bhandari2, S. Atkin5, J. England1 1Department of Otolaryngology, Hull Royal Infirmary 2Department of Renal Medicine, Hull Royal Infirmary 3Department of Health Sciences, University of York 4Department of Anaesthesia, Hull Royal Infirmary 5Department of Endocrinology and Metabolic Medicine, Hull Royal Infirmary Background. Most patients with chronic renal failure will have secondary or tertiary hyperparathyroidism. If they meet the criteria, they are referred to the ENT department for a parathyroidectomy. We present our parathyroidectomy series and compared mortality rates and survival times with non-parathyroidectomised patients. Methods. The renal database at Hull Royal Infirmary was retrospectively analysed. Our parathyroidectomy series covers an 8 year period (2004 to 2011 inclusive). Patients with chronic renal failure who had not received a parathyroidectomy and were on the database during this time period were included for comparison. Results. 112 cases of parathyroidectomy and 1442 non surgical cases were identified. In the surgical group, there were 69 males and 43 females. The mean age was 51.6 years and the number of deaths in our series was 24 (21.4%). In the non-surgical group, there were 925 males and 517 females. The mean age was 64.1 years and the number of deaths was 678 (47.0%). Survival function estimates based on the Kaplan Meier curve showed the cumulative survival is greater in the surgical group as compared with the non-surgical group. Patients were followed up from the date of surgery or first dialysis (in the non surgical group) to the date of death or censorship. The log-rank test showed a significant difference (0.019) between those who had surgery and those who hadn’t. When adjusted for age and sex, a Cox regression analysis was used and found there was no significant difference between the groups. Conclusions. In our series, we found the mortality rates were lower and survival times higher as compared to the non surgical group in the same time period. The literature on the influence of parathyroidectomy on survival times in chronic renal failure patients is scarce. Various studies have suggested that this could be related to the number and severity of associated co-morbidities.
O10. Clinical outcomes of genotype-directed prophylactic total
thyroidectomy in children with germline ret mutation in the UK F. Prete1, T. Ezzat1, C. Morkane1, J. Watkinson2, N. Shaw2, S. Alvi3, R. Squire3, B. Harrison4, J. Wales4, P. Clayton5, F. Eatock6, P. Morrison6, D. Carson6, C. Brain1, P. Hindmarsh1, M. Dattani1, H. Spoudeas1, C. Buchanan7, A. Albanese8, R. Amin9, A. Piero1, P. De Coppi1, T.R. Kurzawinski1. 1Centre for Endocrine Surgery, University College London Hospital and Great Ormond Street Hospital. 2Birmingham Children’s Hospital, Birmingham 3Leeds General Infirmary, Leeds 4Sheffield Children’s Hospital, Sheffield 5Royal Manchester Children’s Hospital, Manchester 6Royal Belfast Hospital for Sick Children, Belfast 7King’s College Hospital, London 8S. George’s Hospital, London 9S. Bartholomew’s Hospital, London Background. Identification of MEN2/FMTC gene carriers by genetic testing allows affected children to access total thyroidectomy(TT)at the earliest stages of C-cell disease(CCH).Little information is available on the outcome of prophylactic TT(pTT) for hereditary medullary thyroid cancer(hMTC). Methods. All UK centers performing pTT were invited to participate in this study.Children within 16 years of age(YOA),operated or awaiting TT for hMTC and all tested for RET codon preoperatively were included.Data were obtained from notes and hospitals electronic databases.TT was performed by endocrine paediatric surgeons on the basis of DNA test.Outcome measures included in-hospital and long-term complications. Results. 71 patients were collected and stratified into ATA risk classes A(FMTC-moderate,14 patients),B(FMTC/MEN2A-high,19 patients),C (MEN2A-higher,34 patients) and D(MEN2B-highest, 4 patients). DNA was tested at a mean age of 5.9 years(0.3-15.18),and TT performed 9.7 months(median)after DNA test(2.13-159). 69 patients underwent TT(2 awaiting surgery),with lymph node dissection(LND) in 15 cases.35.7% patients in class A had TT beyond 10 YOA;52.6% in class B and 58.8% in class C had TT after 5 YOA,while 75%patients in class D had TT beyond 1 YOA.Histology revealed 26 MTC,29 CCH,8 normal thyroids. 19 patients(27.5%)developed postoperative complications:22% hypocalcaemia(14 patients,of which 12(19.6%)required calcium for >2months);24.5%(15pts)had Vit.D prescribed for >2months.Respiratory events and minor transient hoarseness accounted for 4.3%.Complications were relatively more frequent in patients undergoing LND(57.1% vs 23.9% non-LND,p=0.046).LND correlated with risk of excision of intact parathyroids(p=0.001),and inversely to parathyroid preservation(p=0.003).LND correlated to risk of low postoperative calcium (p=0.002),or Vit D administration(p=0.0001).At pathology,lymph nodes were negative in all cases but one(MEN 2B). Conclusion. DNA-directed total thyroidectomy in hMTC confirms a safe procedure in tertiary Centers.When an index case is identified,children may already be beyond the age window for pTT,some may already show raised basal calcitonin.LND in these cases may be of uncertain benefit.Every effort in counselling should be made to take patients to true pTT,avoiding any unnecessary dissection to limit complications.

O11. The value of continuous neuromonitoring in thyroid surgery for
prediction of postoperative vocal cord function in surgeries with intraoperative recovery of loss of signal R. Schneider, K. Lorenz, C. Sekulla, P.N. Thanh, A. Machens, H. Dralle Department of General, Visceral, and Vascular Surgery, Martin Luther University Halle-Wittenberg, Halle (Saale), Germany Background. There is a debate about the potential of intraoperative recovery in thyroid surgeries with loss of signal (LOS) despite anatomical preservation of the recurrent laryngeal nerve (RLN). Continuous recording of amplitude and latency during surgery continuous (CIONM) instead of intermittent nerve monitoring might help (a) to differentiate LOS type 1 (“localised”) from LOS type 2 (global) lesions, and (b) to prognosticate postoperative vocal cord (VC) function according to the extent of amplitude decrease during LOS. Methods. CIONM was performed during 345 thyroidectomies with 557 nerves at risk (NAR). Decrease of amplitude in LOS type 1 and type 2 lesions were calculated and correlated with postoperative VC function examined by videolaryngoscopy in all patients. Results. LOS was registered in 26 of 557 NAR (4.7%), 11 NAR (42.3%) with LOS type 1 lesion, and 15 (57.7%) with LOS type 2. EMG wave forms revealed different patterns in both types suggesting different pathophysiologic mechanisms of functional defects. 12(46.2%) of the 26 NAR with LOS functionally recovered during surgery. 8 out of 12 (66.7%) with intraoperative recovery showed recovery to <50% of baseline amplitude, while 4 (33.3%) had recovery of >50%. 6 (75.0%) of 8 NAR with incomplete compared to 0 of 4 NAR with >50% amplitude recovery had postoperative VC palsy. There was no permanent RLN palsy. Conclusion. CIONM reliably predicted the type of LOS. Incomplete (<50%) amplitude recovery after LOS was consistent with a high risk of postoperative VC palsy. In such cases staged thyroidectomy should be considered when observed at the first side and bilateral surgery was intended.
O12. Observation of clinically negative central compartment lymph nodes in
papillary thyroid carcinoma I.J. Nixon1, I. Ganly1, S.G. Patel1, L.G. Morris1, F.L. Palmer1, D. Thomas1, R.M. Tuttle2, J.P. Shah1, A.R. Shaha1 Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York, NY, USA, 10021 1Head and Neck Service, 2Department of Endocrinology Background. The role of propyhlactic central neck dissection (CND) in the management of papillary thyroid cancer (PTC) is controversial. We report our experience of an observational approach to the cN0 neck in PTC. Methods. 1129 patients with PTC, who had total thyroidectomy between 1986-2005 were reviewed. 470 patients were pN1, 384 had benign nodes removed (pN0) and the remaining 275 had no nodes removed (pNx). The pNx group formed the cohort for this study. Results. With a median follow-up of 70 months the 10year disease specific survival was 100%. Four patients had evidence of radioactive iodine (RAI) uptake on scans performed during follow-up without diagnostic cytology. All subsequently received RAI and are considered disease-free. Three patients had biopsy proven lateral-neck recurrence and underwent neck dissection. 1 patient developed a low-level thyroglobulin suspicious for recurrence. 1 patient has a sub-centimeter level-VI node suspicious for recurrence which has been observed. Therefore, the rate of structural recurrence in the central neck was 0.4% (1/275) and the rate of reoperation on the central neck was 0%. Conclusion. Our results suggest that properly selected patients can safely be managed with observation of the central neck rather than prophylactic CND, which has a higher complication rate.

O13. Does post-operative parathyroid hormone predict early hypocalcaemia
following parathyroidectomy and total thyroidectomy? K. Hiew, R. Trivedi, R. Hardy Department of Endocrine Surgery, Aintree University Hospital NHS Foundation Trust, Aintree University Hospital, Longmoor Lane, Liverpool, L9 7AL Background. Hypocalcemia is a serious complication following parathyroidectomy or total thyroidectomy. It is the commonest factor that impedes discharge until the calcium levels are stable post-operatively. The aims of this study were to assess whether post-operative PTH levels predict hypocalcaemia following parathyroidectomy or total thyroidectomy, and whether its use reduces length of stay for these procedures. Methods. We conducted a prospective study of 153 patients who underwent parathyroidectomy (n=92) or total thyroidectomy (n=61) between 2010 and 2012 at Aintree University Hospital NHS Foundation Trust. Serum adjusted Calcium levels, fall in adjusted Calcium levels, and parathyroid hormone (PTH) levels were measured preoperatively, and at 1-hour, 24-hours, and 12-months postoperatively. Microsoft EXCEL was used for data analysis. Results. Out of 153 patients, 12 patients were excluded due to incomplete records. There was a significant correlation between post-operative PTH levels and fall in adjusted calcium levels 24 hrs (p<0.001) and 12 months (p<0.001) following total thyroidectomy. Post-operative PTH levels and fall in adjusted Calcium levels 24-hours (p<0.001) and 12-months (p<0.001) following parathyroidectomy were not correlated. 19 patients who underwent total thyroidectomy had low 24-hour postoperative PTH levels of < 0.03pmol/L, 78.95% (n=15) of these patients were found to have hypocalcemia 24-hour post-surgery; 63.16% (n=12) of these patients have recorded hypocalcemia 12-months following surgery. 30 patients who underwent total thyroidectomy with borderline low PTH levels of 0.4 – 2pmol/L were also recorded. 40% (n=12) of these patients had hypocalcemia 24-hour post-operative; 33.33% (n=10) of these patients had hypocalcemia 12-months post-operatively. The average hospital stay shortened from 4 to 2 days due to this change of practice. Conclusion. The post-operative PTH level was found to be a reliable predictive of post-operative hypocalcemia in patients who underwent total thyroidectomy in our study, and adoption of its measurement reduced our length of stay.

O14. A Randomized clinical trial comparing open superficial cervical plexus
block versus standard incisional anaesthesia in thyroid and parathyroid surgery. R.J. Egan1,3, J.C. Hopkins2,3, A.J. Beamish1, R. Shah2,3, A.G. Edwards3, J.D.T. Morgan3 1Higher Surgical Trainee, Wales Deanery 2Higher Surgical Trainee, Severn Deanery 3Department of Endocrine & General Surgery, Southmead Hospital, Bristol. BS10 5NB Background. Moderate incisional pain following thyroid and related neck surgery is well documented. The aim of this randomized controlled trial was to investigate whether open superficial cervical plexus block would lead to a reduction in post-operative pain and analgesia use in the post-operative period, following thyroid and parathyroid surgery. Methods. Fifty eight patients (29 in each group) were randomized to receive either incisional anaesthesia alone (control group) or open superficial cervical plexus block (SCPB) combined with incisional local anaesthesia. The primary outcome measure was pain, assessed using a visual analogue scale, during the four hours following surgery, and on the first post-operative day. Secondary outcome measures were analgesia use, respiratory rate, and sedation score. Results. Pain scores were significantly lower in the open SCPB group at time points 30 (p=0.017), 90 (p=0.002), 150 (p<0.0001), and 210 (p<0.0001) minutes post-operatively, and also at 07:00 on post-operative day 1 (p=0.003). Significantly fewer patients required strong opiate medications in the open SCPB group (p=0.003). This was reflected as significantly fewer patients using tramadol (p=0.005) or oramorph (p=0.021). Significantly less patients in the intervention group required rescue opiate analgesia for breakthrough pain than in the control group (p<0.0001) Conclusion. Open SCPB can significantly reduce pain scores in the 24 hours following thyroid and parathyroid surgery, whilst reducing the need for strong or rescue opiate medications. This trial supports the conclusion that pain following thyroid and parathyroid surgery can be effectively managed with open SCPB and simple analgesia in the majority of patients.

O15. Recurrent laryngeal nerve monitoring via continuous vagal nerve
stimulation during thyroid surgery S. Ifeacho1, R. Nash2, G. Mochloulis3 1,2Specialist Registrar – Otolaryngology/ENT 3Consultant Head & Neck Surgeon Ear, Nose & Throat Department, Lister Hospital, East & North Hertfordshire NHS Trust, Corey Mills Lane, Stevenage SG1 4AB Background. Continuous recurrent nerve monitoring is an emerging technique proving valuable in reducing the incidence of post-operative temporary and permanent recurrent laryngeal nerve palsy . Methods. Automatic periodic vagal nerve stimulation was used to continuously monitor the recurrent laryngeal nerve during thyroid surgery. Prior to dissection of the thyroid gland, lateral dissection of the neck was performed for identification and placement of an electrode probe on the vagus nerve. 1mA currents stimulated the vagus nerve at 2ms intervals. Continuous audible and colour-coded visual feedback were displayed and recorded on an attached monitor. Results. Data was recorded for 50 recurrent laryngeal nerves. All were female, within the age range 30-82 years. Warning signals of impending recurrent laryngeal irritation were recorded for more than 30% of cases. There were no cases of temporary or permanent recurrent laryngeal nerve injury. Conclusion. Our study demonstrates that recurrent laryngeal nerve monitoring via continuous vagal nerve stimulation is a beneficial adjunct during thyroid surgery and serves as a useful indicator of impending nerve damage. The use of continuous intra-operative nerve monitoring during thyroid surgery not only serves as a warning of irritation of the nerve, but also provides insight into the exact mechanism of intra-operative injury to the recurrent laryngeal nerve, for example traction injury, thermal damage or compression injury. This provides an immediate opportunity to adjust surgical technique intra-operatively and therefore reduce the rate of temporary or permanent nerve damage.
O16. The evidence base for a randomised controlled trial in the
management of differentiated thyroid cancer: lessons from a systematic review W. Craig, S. Fielding, C. Ramsay, Z. Krukowski Health Services Research Unit, University of Aberdeen and Aberdeen Royal Infirmary Background. The lack of evidence supporting the management of differentiated thyroid cancer is underpinned by disease-specific and health service related barriers to undertaking randomised controlled trials(RCTs). Significant variation in practice continues. A systematic review of two objectively defined management strategies was conducted: risk-stratified (RS) where management is tailored by individual risk and non risk-stratified (NRS). This review highlighted the problems establishing high level evidence, with the current aim to describe problems and possible solutions. Methods. Literature search included English language datasets (MEDLINE, EMBASE 1970-2012), identifying cohorts undergoing primary interventions, described adequately for allocation to RS/NRS. A validated, case series specific Risk of Bias tool was applied. Data were extracted on: patient, tumour, intervention and outcomes (operative morbidity, disease control, survival). Pooled outcomes were compared via weighted mean effects. Sensitivity analysis was carried out around disease, intervention, timescale, and follow up. Results. 73 cohorts were identified; no RCTs nor prospective comparative series. Significant practice variation was confirmed. No differences in outcomes were identified by management approach across 20 pooled measures, only one (10 year disease specific survival) time-specific; 20/73 included time-specific measures. Diverse definitions of recurrence were noted: risk stratification is also relevant to follow. Adverse events occurred up to 20 years post diagnosis. Only 21/73 cohorts had mean follow-up >10years. On sensitivity analysis, lower risk cohorts had significantly improved rates of distant recurrence (-4.5%, 95% CIs -8.5-0.5, p=0.03) by RS approach; no other differences were found. An intermediate risk group is increasingly defined; these patients have higher rates of adverse events with apparent consensus around clinical equipoise. Only 1/73 cohorts included patient preference/quality of life measures. Conclusion. The importance of long-term, time specific data, with individual risk described is confirmed. The possible over-treatment of low risk cohort continues. Patient preferences require investigation. A pragmatic RCT of surgical approach in intermediate risk patients is proposed.
O17. Intraoperative nerve monitoring is used by a small (but slowly
increasing) minority of members of British Association Of Endocrine And Thyroid Surgeons (BAETS) R. Mihai1, D. Chadwick2 / on behalf of BAETS 1John Radcliffe Hospital, Oxford, UK; 2Chesterfield Royal Hospital, Chesterfield, UK; Director of BAETS Audit Background. Intraoperative nerve monitoring (IONM) has been adopted as a valuable adjunct to thyroid surgery in many countries. The aim was to estimate patterns of IONM use by BAETS members. Methods. Analysis of data recorded between 2000-2012 in the prospective national BAETS audit. Results. Out of a total of 26365 thyroid operations recorded, IONM was used in 1902 operations (7%) and not used in 13655 (missing data on 10808 cases), with a progressive increase from 59 cases in 2008 (4%) to 294 cases in 2010 and 672 cases in 2012 (22%). IONM use was similar in patients <16 years (22/174,13%) and >16 years (1857/14718,13%) and in those with malignant disease (381/2482,15%) and benign disease (1498/12410,12%). There was a trend to use IONM more commonly in reoperative surgery (248/1531,16% vs. 1596/13182 first-time cases,12%)(Chi-square p<0.00001), mainly on same-side re-operations (94/404,23% vs. 154/965 not-same-side re-operations,16%) (Chi-square p=0.0014). Reporting of post-op vocal cord function (VCF) was more accurate when IONM was used (745/1879 cases, 40%) than when IONM was not used (1352/13013,10%)(Chi-square p<0.0001). Differing policies between surgeons for routine/selective post-op VCF checks and the high rate of missing data for VCF, make it impossible to discern if the apparent difference in palsy rates between the IONM groups (3.1% in IONM+ vs. 1.3% in IONM-) is significant. Majority of BAETS members remained non-users (60%), many (20%) used it seldom (<5% of cases) and only 10% used it for >50% of cases. There was a small number of “converts” (i.e. previously non-users who have become routine users). During 2010-2012, the number of IONM consumables sold by Medtronic in UK was at least five times higher than the number of cases reported on the BAETS audit. This suggests that many IONM users are not members of BAETS. Conclusion. BAETS members are reluctant to accept IONM. Lack of level I evidence of IONM impact on the incidence of postoperative vocal cord palsy and financial concerns are unlikely to be sufficient to explain the contrasting attitude of surgeons from different countries towards (not) using IONM.
O18. Reoperative parathyroid surgery in the era of focused primary
procedures A.C. Walker, J.G.H. Hubbard, J.J. Fraile St Thomas’ Hospital, London UK Background. Parathyroid surgery has evolved with imaging localisation techniques which allow, where possible, a focussed operation. Reoperative surgery is therefore also evolving with the legacy of this approach. There are now three populations of reoperative patients: traditional four gland explorations; focussed procedures; or bilateral neck explorations converted from a focussed procedure. Our study seeks to characterise our experience of reoperative surgery in the era of focussed parathyroidectomy. Methods. Patients undergoing reoperation for primary hyperparathyroidism between 2003-12 at a tertiary referral centre were identified. Data was collected retrospectively. Results. 407 parathyroidectomies were performed at our centre between 2003-12. 33 patients with persistent PHPT were identified, undergoing a total of 41 reoperations. 5 patients required more than one reoperation at our centre. 20 patients were referred from external sources, while 13 were internal reoperations. 79% presented with a first operation of BNE, and 21% with a focussed or unilateral approach. A summary of perioperative imaging and workup is presented in Table 1:
% of procedures where test was utilized
% yielding useful results
Ultrasonography 54 22
99c-technetium 90 57
CT/MRI 54 27
PET 22 33
PTH venous sampling 27 73
Intraoperative PTH sampling
66 100
At curative or final procedure, a focussed approach was used 15 times (45%) including three focussed mediastinal explorations. Histopathology of final procedures revealed 55% adenomas, 27% hyperplastic glands, 3% parathyroid cancers. Conclusion. In our experience, reoperative parathyroidectomy is still largely carried out in patients who have previously undergone BNE. Single adenomas represented the greatest disease burden at reoperation, and multigland disease was responsible for only a minority of cases. Reoperation can be successfully carried out via focussed approach in nearly half of all patients. Pre-operative imaging yields homogenous results, and work up for reoperative procedure requires an accurate record of previous approaches to exploration of the neck.
O19. Minimally invasive video-assisted thyroidectomy (MIVAT) and
thyroiditis: retrospective analysis of 391 cases. New inclusion criteria? B. De Simone, P. Del Rio, M. Sianesi University Of Parma; Unit Of General Surgery And Organ Trasplantation, Department Of Surgical Sciences Background. The indications to MIVAT, applied only to carefully selected patients at the beginning, with the spread of the procedure and the increasing experience of the endocrine surgeons, have been progressively extended. The aim of our study is to verify what are today the most appropriate inclusion criteria for this videoassisted technique and which remain the absolute and relative contraindications to be respected to avoid the increasing of the risk of postoperative complications. Methods. We have statistically analyzed data related to 2072 patients underwent thyroidectomy in our operative unit, from july 2005 to december 2012; 391of these cases were treated with MIVAT (18.9%). We have divided the MIVAT patients into two subgroup: MIVAT-first period (MIVAT-fp), (0-211 patients treated), and MIVAT-second period (M-sp), (212-391 cases). MIVAT-sp was characterized by the esclusion of the patients affected by thyroiditis. All the patients operated were followed up at day 7 (surgical consultation fixed on discharge) and at day 30 and 180 (ambulatory visit or telephone contact) after intervention. The data of MIVAT and Conventional Thyroidectomy (CT) group were matched. Results. There are no statistically significant differences in postoperative pain, nerve palsy and transitory hypoparathyroidism between MIVAT group and CT group. Postoperative pain at 24 hours is lower in MIVAT group. There is a different percentage of transitory nerve palsy in the MIVAT-fp and MIVAT-sp. Conclusion. MIVAT is safe and reproducible and it has excellent cosmetic results. Our data confirm the validity of the eligibility criteria for MIVAT; we can extend these indications to those patients with an associated thyroiditis (often the detection of thyroiditis is intraoperative) but there is a variable risk of conversion to CT. MIVAT is feasible in selected cases of hyperthyroidism but it is safer if the endocrine surgeon excludes from this surgical procedure patients affected by preoperative thyroiditis.

O20. Incidence and predictors of post-thyroidectomy hypocalcaemia in a
tertiary endocrine surgical unit O. Edafe, P. Prasad, B.J. Harrison, S.P. Balasubramanian Department of Oncology, University of Sheffield and Endocrine Surgical Unit, Sheffield Teaching Hospitals NHS Foundation Trust Background. The incidence of post-thyroidectomy hypocalcaemia varies across centres. Independent estimation of the incidence and factors associated with post thyroidectomy hypocalcaema in the local unit have not been studied before. The aim of this study was to determine the incidence and predictors of post-thyroidectomy hypocalcaemia (as defined by a corrected calcium < 2.1 mmol/L). Methods. A total of 242 consecutive patients who underwent completion or bilateral thyroid surgery between 2008 and 2011 were included in this retrospective study. Clinical and biochemical data were obtained from electronic and hard copy medical records. Biochemical data was validated by a second observer. Results. The incidence of transient hypocalcaemia on post-op day one and hypocalcaemia at six months were 28.9% and 5.4% respectively. However, the transient rate increased to 35.1% when all calcium levels until 6 months after surgery were included. The long term rate increased to 8.4% when hypocalcaemic patients not on supplements were included. Factors associated with transient hypocalcaemia in univariate analysis were lower preoperative corrected calcium (P=0.005), central neck dissection (P=0.03), parathyroid gland auto-transplant (P=0.001) and inadvertent parathyroid excision (P=0.039). However, only low preoperative corrected calcium (P=0.001) and parathyroid gland auto-transplant (P=0.015) were significant in multivariate analysis. Other clinical factors such as ethnicity, preoperative diagnosis, preoperative thyroid function, thiazide diuretics, hypertension, preoperative calcium/vitamin D supplements, Lugol’s iodine and weight of excised gland were not associated with post thyroidectomy hypocalcaemia. Conclusion. Incidence of hypocalcaemia was underestimated by 6% when only the first post-op day measurements were considered. The need for auto-transplantation and lower preoperative calcium levels are independent predictors of transient hypocalcaemia; the latter may reflect pre-existing vitamin D deficiency.
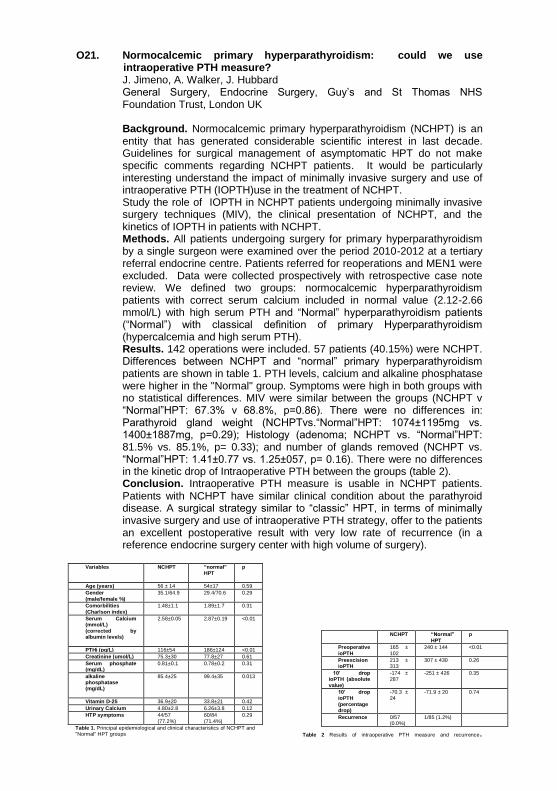
O21. Normocalcemic primary hyperparathyroidism: could we use
intraoperative PTH measure? J. Jimeno, A. Walker, J. Hubbard General Surgery, Endocrine Surgery, Guy’s and St Thomas NHS Foundation Trust, London UK Background. Normocalcemic primary hyperparathyroidism (NCHPT) is an entity that has generated considerable scientific interest in last decade. Guidelines for surgical management of asymptomatic HPT do not make specific comments regarding NCHPT patients. It would be particularly interesting understand the impact of minimally invasive surgery and use of intraoperative PTH (IOPTH)use in the treatment of NCHPT. Study the role of IOPTH in NCHPT patients undergoing minimally invasive surgery techniques (MIV), the clinical presentation of NCHPT, and the kinetics of IOPTH in patients with NCHPT. Methods. All patients undergoing surgery for primary hyperparathyroidism by a single surgeon were examined over the period 2010-2012 at a tertiary referral endocrine centre. Patients referred for reoperations and MEN1 were excluded. Data were collected prospectively with retrospective case note review. We defined two groups: normocalcemic hyperparathyroidism patients with correct serum calcium included in normal value (2.12-2.66 mmol/L) with high serum PTH and “Normal” hyperparathyroidism patients (“Normal”) with classical definition of primary Hyperparathyroidism (hypercalcemia and high serum PTH). Results. 142 operations were included. 57 patients (40.15%) were NCHPT. Differences between NCHPT and “normal” primary hyperparathyroidism patients are shown in table 1. PTH levels, calcium and alkaline phosphatase were higher in the "Normal" group. Symptoms were high in both groups with no statistical differences. MIV were similar between the groups (NCHPT v “Normal”HPT: 67.3% v 68.8%, p=0.86). There were no differences in: Parathyroid gland weight (NCHPTvs.“Normal”HPT: 1074±1195mg vs. 1400±1887mg, p=0.29); Histology (adenoma; NCHPT vs. “Normal”HPT: 81.5% vs. 85.1%, p= 0.33); and number of glands removed (NCHPT vs. “Normal”HPT: 1.41±0.77 vs. 1.25±057, p= 0.16). There were no differences in the kinetic drop of Intraoperative PTH between the groups (table 2). Conclusion. Intraoperative PTH measure is usable in NCHPT patients. Patients with NCHPT have similar clinical condition about the parathyroid disease. A surgical strategy similar to “classic” HPT, in terms of minimally invasive surgery and use of intraoperative PTH strategy, offer to the patients an excellent postoperative result with very low rate of recurrence (in a reference endocrine surgery center with high volume of surgery).
Variables NCHPT “normal”
HPT
p
Age (years) 56 ± 14 54±17 0.59
Gender
(male/female %)
35.1/64.9 29.4/70.6 0.29
Comorbilities
(Charlson index)
1.48±1.1 1.89±1.7 0.31
Serum Calcium (mmol/L)
(corrected by albumin levels)
2.58±0.05 2.87±0.19 <0.01
PTHi (pg/L) 116±54 186±124 <0.01
Creatinine (umol/L) 75.3±30 77.8±27 0.61
Serum phosphate (mg/dL)
0.81±0.1 0.78±0.2 0.31
alkaline phosphatase (mg/dL)
85.4±25 99.4±35 0.013
Vitamin D-25 36.9±20 33.8±21 0.42
Urinary Calcium 4.80±2.8 6.26±3.8 0.12
HTP symptoms 44/57
(77.2%)
60/84
(71.4%)
0.29
Table 1. Principal epidemiological and clinical characteristics of NCHPT and "Normal" HPT groups
NCHPT “Normal”
HPT
p
Preoperative
ioPTH
165 ±
102
240 ± 144 <0.01
Preexcision ioPTH
213 ± 313
307 ± 430 0.26
10’ drop ioPTH (absolute
value)
-174 ± 287
-251 ± 426 0.35
10’ drop ioPTH
(percentage drop)
-70.3 ± 24
-71.9 ± 20 0.74
Recurrence 0/57 (0.0%)
1/85 (1.2%)
Table 2 Results of intraoperative PTH measure and recurrence.

O22. Ipsilateral central neck dissection plus frozen section examination vs
prophylactic bilateral central neck dissection in cN0 papillary thyroid carcinoma A. D’Amore, M. Raffaelli, C. De Crea, L. Sessa, S.E. Tempera, C. Bellantone, C.P. Lombardi Division of Endocrine and Metabolic Surgery – Università Cattolica del Sacro Cuore – Rome - Italy Background. Ipsilateral central compartment node dissection (IpsiCCD) can reduce the morbidity of prophylactic bilateral central compartment node dissection (BilCCD) in papillary thyroid carcinoma (PTC), but it carries the risk of contralateral metastases being overlooked. Frozen section examination (FSE) of removed ipsilateral nodes has been proposed to intraoperatively assess the nodal status. We compared IpsiCCD plus FSE and BilCCD in clinically unifocal and node negative (cN0) PTC. Methods. One hundred patients with clinically unifocal and cN0 PTC who underwent surgery between September 2010 and February 2013 were prospectively assigned to 1 of the 2 following surgical procedures: total thyroidectomy (TT) plus BilCCD (TT-BilCCD) and TT plus IpsiCCD (TT-IpsiCCD). In the TT-IpsiCCD group removed nodes were sent for FSE. If FSE was positive for metastases, a BilCCD was accomplished. Results. The 2 groups included 50 patients each. No significant difference was found among them concerning age, sex, operative time, tumor size, pT and microscopic multifocal disease (P=NS). Overall occult nodal metastases were found in 41 patients: 20 in TT-IpsiCCD and 21 in TT-BilCCD group. FSE identified occult node metastases in 13/20 pN1a patients of TT-IpsiCCD group (overall accuracy 86%). Seven node metastases were not detected at FSE: 5 were micrometastases (≤2mm). 6/13 (46%) of TT-IpsiCCD patients who underwent BilCCD and 6/21 TT-BilCCD (28%) pN1a patients had bilateral metastases. More patients in the TT-BilCCD group showed transient hypocalcemia than in the TT-IpsiCCD group (27/50Vs18/50, respectively) (P=NS). At a mean follow-up of 15 months, no patients experienced recurrent disease. Conclusion. Occult central neck metastases are frequent in cN0 PTC and are bilateral in at least one fourth of the patients with clinically unifocal tumors. FSE of ipsilateral nodes allows to reliably modulate the extension of the central neck clearance and provides an accurate staging in most of clinically unifocal cN0 PTC patients.

O23. Evaluation of Salford Royal Foundation Trust’s management of adrenal
incidentaloma – is the duration of radiological follow up necessary? R. Brindle, A. Thomson, A. Mukherjee, T. Kearney, I. Anderson, H. Doran
Salford Royal NHS Foundation Trust, Salford, M6 8HD
Background. Adrenal incidentalomas are observed in 5% CT scans. When non- functional, determination of clinical significance is often reliant on interval change, with consensus on duration lacking. At our institution interval radiological re-evaluation typically occurs at 6 and 18 months. We evaluated this with specific reference to the later scan’s value Methods. Patients with adrenal lesions detected between 2007 - 2009 were identified from radiology’s database. Reports were reviewed for number, frequency, duration of scanning, plus nodule(s) characterization and size change. Scans were categorized to presentation (PS), early (EFUS) and late follow up scans (LFUS). Biochemical evaluation and outcome was retrieved from clinical records. Results. 143 patients (187 nodules) were identified (59% adenoma, 22% indeterminate, 6% functional, 4% malignancy, 9% other). Nine patients with functional nodules were excluded. 134 patients received variable radiological re-evaluation, 97 (120 nodules) beyond 3 months with subsequent EFUS and / or LFUS. Patients received up to 6 scans, twelve% > 2 FUS, typically over 15 months but 30% had LFUS at > 18 months. Three-quarters (138 / 187) nodules were diagnosed at PS and /or EFUS. Sixty-five % of radiologically benign lesions were followed up beyond 6 months. The LFUS altered outcome in 2 cases, and provided diagnostic clarification in 3 cases. Seventy-two % of those undergoing LFUS (46 patients, 59 nodules) remained under clinical follow up. Nodule size range was 0.6 – 18.1cm, 80% < 4cm and all malignant lesions > 6cm. 40% (48/120 nodules) increased in size over median 15 months, but only 2% nodules increased > 1cm , with 71% of those increasing by < 1cm size detected by EFUS. Twenty-two / 23 indeterminate nodules remained stable size at LFUS. Conclusion. Patients with benign and clinically insignificant diagnoses are enduring lengthy and costly (economically and patient anxiety) surveillance with potentially unnecessary radiation exposure.

O24. Binding of Helix Pomatia agglutinin glycoproteins is a predictor of
poor survival in adrenal cancers. M. Heetun1, G. P Sadler1, R. Mihai1, S. Brooks2, P. Rajeev1 1Department of Endocrine Surgery, Oxford Radcliffe Hospitals 2Department of Cellular Biology, Oxford Brookes University Background. Adrenocortical cancers are rare endocrine cancers with poor prognosis if untreated. Binding of the lectin Helix pomatia agglutinin (HPA) has been shown to be associated with poor prognosis in many human cancers but has not been shown in adrenal cancers. Methods. Lectin histochemistry was performed on archival paraffin wax embedded specimens of adrenocortical tumours excised between the years 2000 – 2012 at a tertiary referral centre. Demographic data, histological data, recurrence of disease, local invasion and mortality data were recorded. The aims of the study were to assess alteration in cellular glycosylation, detected by HPA binding in adrenal cancers and to determine if such altered glycosylation carries any prognostic significance. Results. The sample group consisted of 53 patients with cancers (n=36; 21F:16M), metastasis into adrenals (n=9; 6F:3M) and benign (adenoma and normal) (n=8) (5F:3M). Histological blocks were not available on 14 patients with adrenal cancers. In the cancer group where blocks were available (n=22) 10 were functional cancers (9 Cushing’s and 1 Conn’s). Normal and benign adrenal tumours showed no binding with the lectin HPA. In the cancer group, although there was no difference seen in the incidence of local recurrence, local invasion or metastatic disease between HPA-positive and negative tumours, HPA binding was associated with an advanced stage of disease and greater mortality. Patients with positive HPA binding (n=11) survived a mean of 21 months (range 2-55 months) whilst those patients with negative HPA binding (n=11) survived (range 36-108 months follow up) with the exception of one patient (p=0.0015). Conclusion. This is the first study showing that HPA-binding glycoproteins are synthesised by adrenal cancers. Positive HPA binding in adrenal cancer is a predictor of both aggressive disease and poor prognosis.

O25. Variations in the post-op management of primary hyperparathyroidism
in the UK J. Barnes, A. Midgley-Hunt, S. Thrush Department of General Surgery, Worcester Royal Hospital Background. The post operative management of patients with primary hyperparathyroidism usually involves monitoring serum calcium and parathyroid hormone levels. The intention is to both confirm curative surgery and monitor hypocalcaemia in the short term, but also assess patients for evidence of recurrent disease in the longer term. There are no definitive guidelines for either the short term management or longer term surveillance of these patients and therefore practice in the UK seems to be variable. The aim of this study was to assess the variations in practice in the post-operative management of primary hyperparathyroidism in the UK. Methods. British endocrine surgeons performing parathyroid surgery were identified from the BAETS National Database. A survey tool was developed to assess individual practice regarding the post-operative management of primary hyperparathyroidism. The survey was disseminated in June 2013 with both paper and electronic versions available for completion. Results. 91 surgeons were identified through the BAETS database. Serum calcium was checked by 95% of surgeons after hospital discharge following surgery. This was most commonly done within 2 weeks (50%) and at 3 months (32%). Annual calcium levels were checked by 16% of surgeons. Post-op serum PTH was checked by 32% of surgeons, most commonly within 2 weeks (14%) and 3 months (13%). 68% of surgeons reviewed patients within 6 weeks of surgery whereas 32% reviewed at 2-3 months instead. 89% of surgeons discharged their patients back to GP care within 3 months of surgery. 32% of surgeons ask GPs to check calcium levels annually. 58% of surgeons felt that the lifetime risk of recurrent disease was between 1-5%. Conclusion. The post-operative management of patients with primary hyperparathyroidism varies considerably between endocrine surgeons in the UK. The majority of surgeons do not routinely request long term calcium surveillance to detect recurrent disease.
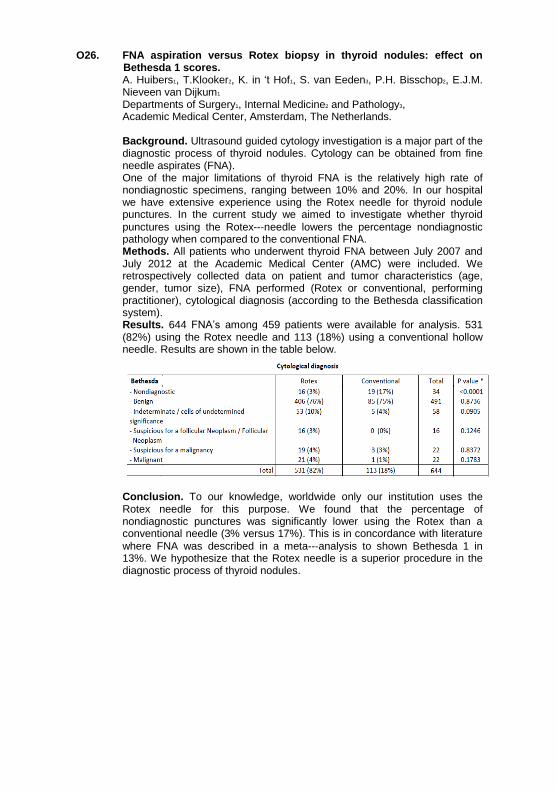
O26. FNA aspiration versus Rotex biopsy in thyroid nodules: effect on
Bethesda 1 scores. A. Huibers1, T.Klooker2, K. in ‘t Hof1, S. van Eeden3, P.H. Bisschop2, E.J.M. Nieveen van Dijkum1 Departments of Surgery1, Internal Medicine2 and Pathology3, Academic Medical Center, Amsterdam, The Netherlands. Background. Ultrasound guided cytology investigation is a major part of the diagnostic process of thyroid nodules. Cytology can be obtained from fine needle aspirates (FNA). One of the major limitations of thyroid FNA is the relatively high rate of nondiagnostic specimens, ranging between 10% and 20%. In our hospital we have extensive experience using the Rotex needle for thyroid nodule punctures. In the current study we aimed to investigate whether thyroid
punctures using the Rotex--‐needle lowers the percentage nondiagnostic pathology when compared to the conventional FNA. Methods. All patients who underwent thyroid FNA between July 2007 and July 2012 at the Academic Medical Center (AMC) were included. We retrospectively collected data on patient and tumor characteristics (age, gender, tumor size), FNA performed (Rotex or conventional, performing practitioner), cytological diagnosis (according to the Bethesda classification system). Results. 644 FNA’s among 459 patients were available for analysis. 531 (82%) using the Rotex needle and 113 (18%) using a conventional hollow needle. Results are shown in the table below.
Conclusion. To our knowledge, worldwide only our institution uses the Rotex needle for this purpose. We found that the percentage of nondiagnostic punctures was significantly lower using the Rotex than a conventional needle (3% versus 17%). This is in concordance with literature
where FNA was described in a meta--‐analysis to shown Bethesda 1 in 13%. We hypothesize that the Rotex needle is a superior procedure in the diagnostic process of thyroid nodules.

O27. Quantification of lymph nodes in the central compartment of the neck:
an anatomical cadaveric study E. Ofo1, S. Thavaraj2, D. Cope1, J.P. Jeannon1, R. Oakley1, K. Kapoor1, E. Odell2, C. Lock2, R. Simo1
1Department of Otolaryngology, Head & Neck Surgery. Guy’s & St Thomas’ NHS Foundation Trust. Great Maze Pond, London, SE1 9RT 2Head and Neck/Oral Pathology. King’s College London and Guy’s & St Thomas’ NHS Foundation Trust. Great Maze Pond, London, United Kingdom SE1 9RT Background. Differentiated thyroid cancer (DTC) accounts for over 90% of thyroid malignancies. Despite a 15-30% risk of nodal metastasis, elective central compartment neck dissection (CCND) for DTC remains controversial. Current knowledge on the expected lymph node yield from a CCND is limited, compared to the lateral neck. Where CCND is indicated, the surgeon and pathologist must be confident on the adequacy of oncological clearance, for the benefits to outweigh the risks of surgery. This study’s aim was to accurately quantify the number of lymph nodes present in the cadaveric central neck compartment. Methods. Twenty-nine cadaveric necks were dissected; one case was excluded due to widespread nodal metastasis by carcinoma. Level VI was subdivided into four compartments for the dissection i.e. pre-cricoid (delphian), pre-tracheal, right and left para-tracheal regions. Each para-tracheal compartment contained thyroid gland, which was removed prior to histological analysis. All other tissue in each compartment was routinely processed and stained with haematoxylin and eosin. Only lymphoid tissue with a defined microscopic fibrous capsule and subcapsular sinus was included in the nodal count. Data analysis was performed using Microsoft Excel (Office) 2008. Results. The median total nodal count per cadaver was four (range: 1-16), with a median of one node present in each para-tracheal and pre-tracheal region (range: 0-7 and 0-8, respectively). The median delphian node count was 0 (range 0-2). The average size of lymph nodes across all compartments was 2.9mm. Conclusion. This is the first study to assess cadaveric level VI neck lymph nodes and establish baseline counts for lymph node yield. Elective CCND for differentiated thyroid cancer remains controversial. Should elective CCND be performed, those involved in the management of DTC need to recognise the wide range but low median yield of level VI neck lymph nodes.
O28. Papillary thyroid microcarcinoma - therapeutic/follow up trends in UK
N. Charaklias, T. Mazhar, S. Atkin, J. England Department of Otolaryngology and Department of Endocrinology Castle Hill Hospital, UK Background. Papillary thyroid carcinoma (PTC) is the most common histological type of thyroid malignancy. In most patients, PTC is characterized by an indolent course, and the overall 10-year survival rate exceeds 90%. An increase in the use of ultrasonography has led to an increase in the detection of papillary thyroid microcarcinoma (PTMCs) (less than or equal to 1 cm in size) in the absence of nodal metastases. Our study would like to find out the current follow up practice in the UK in a hypothetical patient post lobectomy with a histological diagnosis of PTMC. Methods. A questionnaire survey sent to all members of the British Association of Endocrine and Thyroid Surgeons (BAETS) regarding a hypothetical post lobectomy patient with a histological diagnosis of PTMC. Results. From 51 responds received a big variety of therapeutic /follow up practice was noticed. 53% of correspondents reassure and discharge a patient with confirmed unifocal area of PTMC less than 5mm. 45% will suppress TSH and 6% will proceed to near/total thyroidectomy and RAI ablation. In the above scenario 31% will follow up patients for more than 5 years, 41% will reassure and discharge them. In the case of unifocal PTMC of more than 5mm and less than 1cm the discharge rate has fallen to 21%, TSH suppression has risen to 59% and completion surgery with ablation is practiced in 22%. The follow up trend in the above scenario was 47% for more than 5 years, 33% for 2-5 years and only 18% will discharge the patient. 80% of correspondents mentioned that unilateral multifocality was the most important factor that would influence their treatment choice. Conclusion. From the results of the survey there is a big variety of treatment and follow up trends in the UK. Maybe there is a need for a national guideline.
Posters
P1. Minimally Invasive Parathyroidectomy aided by Intraoperative PTH
monitoring in patients with discordant imaging T. Ezzat, P. Wignarah, F. Prete, J. Honour, I. Phillips, J. Smart, T.R. Kurzawinski Centre for Endocrine Surgery, University College London Hospital and Great Ormond Street Hospital
P2. Intraoperative Parathyroid Hormone measurement during
Parathyroidectomy is cost effective T. Ezzat, I. Philips, J. Honour, F. Prete, J. Smart, T.R. Kurzawinski Centre for Endocrine Surgery, University College London Hospital and Great Ormond Street Hospital
P3. Clinical outcomes of thyroid surgery in children F. Prete, T. Ezzat. C.K. Sinha, P. De Coppi, T.R. Kurzawinski Centre for Endocrine Surgery, University College London Hospital and Great Ormond Street Hospital
P4. An audit of two-week-wait referrals for thyroid and head and neck cancer T. Dessouki1, J.D.T. Morgan2 1University of Bristol; 2Southmead Hospital
P5. Increasing incidence of Thyroid cancer in the Teesside area E. Ward, H. Freeman, W.M. Elsaify Department of Endocrine Surgery, James Cook University Hospital
P6. Prophylactic antibiotics and risk of Surgical site infections (SSI) in thyroid and parathyroid surgery H. Freeman, E. Ward, W.M. Elsaify Department of Endocrine Surgery, James Cook University Hospital
P7. Recurrence of phaeochromocytoma and paraganglioma after initial surgical intervention: a retrospective comparative study P.C. Johnston1, F.C. Eatock2, KR Mullan1, P Martin2, M. Gray3, S.J. Hunter1 1Regional Centre for Endocrinology and Diabetes, 2Department of Endocrine Surgery, 3Department of Pathology, Royal Victoria Hospital, Belfast, UK
P8. Thromboembolic Prophylaxis in Thyroid Surgery. Do the Benefits outweigh the Risks? B. Morris, R.B. Townsley, O. J. Hilmi Glasgow Royal Infirmary, Glasgow, Scotland
P9. Safe day case thyroid surgery is possible N. Allen, S. Mui, T. Hakim, M. Lamb, M.A. Tomlinson University Hospitals of Morecambe Bay NHS Trust, UK
P10. Thyroid Surgery in West Africa: Experience of 134 Cases Onboard Mercy Ships J. van Gangelen1, A.J. Collins2
1Wollongong Hospital, Australia; 2Bega Hospital, Australia
P11. Thyroid incidentalomas on nuclear imaging – Evaluation of management and clinical outcomes S. Elzein, A. Abdulkhaled, E. Lorenz, S.P. Balasubramanian Sheffield Teaching Hospitals NHS Foundation Trust, UK
P12. Outcomes of Surgery for Patients with Retrosternal Multinodular Goitre Requiring Midline Sternotomy R. Simo1, I. Nixon1, E. Ofo1, J.P. Jeannon1, T. Routledge2, K. Harrison-Phipps2 Otorhinolaryngology, Head and Neck Surgery1 and Thoracic Surgery2 Units, Guy’s and St Thomas NHS Foundation Trust, London UK
P13. Does elective parathyroidectomy for pHPT affect renal function? A prospective study R.J. Egan, R. Arkell, J. Ansel, S. Zouwail, D.M. Scott-Coombes, M.J. Stechman Department of Endocrine and General Surgery, University Hospital of Wales, Cardiff, CF14 4XW
P14. Role of routine MIBG scintigraphy in the pre-operative localisation of phaeochromocytoma R. Arsalani-Zadeh, M. Kumar, S. Ghattamaneni, T. Kearney, I. Anderson, H. Doran Salford Royal Hospital, Manchester, UK
P15. A comparative study of the use of LigaSure vessel sealing system and conventional techniques in thyroid surgery K.K. Varadhan, N. Pattni, C.S. Ubhi Department of Surgery, Nottingham University Hospitals, City Hospitals Campus, Nottingham, U.K
P16. A phase I feasibility study of intra-operative near infra-red fluorescent imaging in parathyroid surgery S.P. Balasubramanian1, D. Lee1, B.J. Harrison1, E. Wallis1, S. Guillermet2, P. Rizo2 1Department of General Surgery and 2Research and Development Unit, Sheffield Teaching Hospitals NHS Foundation Trust; 2Fluoptics, Grenoble, France
P17. Impact of plasma total homocysteine on cardiovascular and anesthesiological risk in patients with thyroid disease: a single centre study P. Princi1, R.S. Auriemma2, R. Corona2, I. Mariano2, B. Zappacosta3, C. Cavicchioni1, M. Gasperi2 1Division of Surgical Oncology, Department of Oncology, Università Cattolica del Sacro Cuore, Fondazione “Giovanni Paolo II”, Campobasso; 2Endocrinology, Università del Molise, Campobasso; 3 Department of Laboratories and Service, Fondazione Giovanni Paolo II, Campobasso
P18. An analysis of surgical outcomes based on current systems of data collection using post-operative haemorrhage in thyroid surgery as an illustrative example J.A. Smith, J.H. Hardman, N. Sharma, P. Nankivell, J. Douglas, J.C. Watkinson Department of Head and Neck Surgery, University Hospital Birmingham, UK
P19. Persistent elevation of parathyroid hormone following parathyroidectomy – the effect of Vitamin D replacement N Chand1, G Weston-Petrides2, P Antonas1, J Begley2, T Richardson1, A Evans3, AI Skene1 1Endocrine Surgery Unit, Royal Bournemouth Hospital, Castle Lane East, Bournemouth BH7 7DW, United Kingdom; 2Bournemouth University Fern Barrow, Poole, Dorset BH12 5BB, United Kingdom; 3Endocrine Surgery Unit, Poole General Hospital, Longfleet Road, Poole, Dorset BH15 2JB, United Kingdom
P20. Incidence and Management of Tracheomalacia in Patients with Long-standing Thyroid Goitres J. Jimeno, I. Nixon, E. Ofo, K. Kappor, R. Simo Otorhinolaryngology, Head and Neck Surgery Guy’s and St Thomas NHS Foundation Trust, London UK
P21. Persistently elevated parathyroid hormones in normocalcaemic patients following successful parathyroidectomy A. Razif, J. Vance-Daniel, D. Goulding, M.J. Stechman, D.M. Scott-Coombes Department of Endocrine Surgery, University Hospital of Wales, Cardiff UK
P22. Intra-operative nerve monitoring during thyroid surgery: a waste of time? N.B. Oozeer1, S.Y. Hey1, N. O’Donnell2, O.J. Hilmi1 1Department of Otolaryngology-Head and Neck Surgery, NHS Greater Glasgow and Clyde, Glasgow Royal Infirmary, United Kingdom; 2Department of Anaesthesia, NHS Greater Glasgow and Clyde, Gartnavel General Hospital, United Kingdom
P23. Screening carotid Doppler US in patients undergoing lateral neck dissection: is it worthwhile? L. Revelli, A. Santoliquido, C. De Crea, P. Kateta Tshibamba, E. Traini, A. D’Amore, P. Tondi, M. Raffaelli, C.P. Lombardi Division of Endocrine and Metabolic Surgery – Università Cattolica del Sacro Cuore – Rome – Italy
P24. Can the relationship between the location of the primary tumor and the pattern of lateral neck metastases justify limited lateral neck dissection in papillary thyroid carcinoma? L. Sessa, C.P. Lombardi, M. Raffaelli, C. De Crea, E. Traini, S. Ronti, V. Milano, P. Gallucci, M.D., R. Bellantone Division of Endocrine and Metabolic Surgery – Università Cattolica del Sacro Cuore – Rome – Italy
P25. Patient preference in exploratory Parathyroidectomy versus Minimally Invasive Surgery – Interim Analysis T. Zahoor, A. Rafferty, S.L. Atkin, R.J. England Castle Hill Hospital, Cottingham, East Yorkshire. United Kingdom
P26. Bone turnover markers (PINP and CTX) in primary hyperparathyroidism as a predictor of increased bone turn over in primary hyperparathyroidism D. Von-Hagt, J. Lynch, M. Al-Mryat, V. Lawrence, A. Baharani, P. Rajeev Department of Endocrine & General Surgery, St Mary’s Hospital, Newport, Isle of Wight UK
P27. Ambulatory same day discharge thyroid surgery: our experience at the Basildon and Thurrock University Trust R. Boulton, S. Nanda, B. Wong, N. Makwana, P. Gogalniceanu, T. Jeddy Basildon and Thurrock University Hospitals NHS Foundation Trust, Basildon, United Kingdom
P28. Is a previous cancer a risk factor for papillary thyroid cancer? M. Poussier1, S. Jambet1, J.M. Petit2, H. Lecomte1, L. Osmak-Tizon1 1Department of Endocrine Surgery, Dijon University Hospital, France 2Department of Endocrinology, Dijon University Hospital, France
P29. Non-biochemical predictors of post-thyroidectomy hypocalcaemia – a systematic review O. Edafe, N. Laskar, R. Antakia, L. Uttley, S.P. Balasubramanian Department of Oncology and the School of Health and Related Research, University of Sheffield
P30. Ethnicity, young age and Vitamin D deficiency do not predict multiple gland disease in primary hyperparathyroidism V. Constantinides, I. Christakis, C. Halkias, N. Tolley, F. Palazzo Department of Endocrine and Thyroid Surgery, Imperial College NHS Trust, Hammersmith Hospital, London, UK
P31. Does the Sestamibi scan outcome affect the decision to refer to an endocrine surgeon for primary hyperparathyrodisim K. Bowling, S. Baker, C. Radcliffe, J. Mottram, A. Skingle, U. Kirkpatrick Endocrine surgery department, Wrexham Maelor Hospital, Wales, United Kingdom
P32. Spontaneous pneumothorax as an initial presentation of Neurofibromatosis Type 1 (NF1) may herald an increased risk of phaeochromocytoma P. Martin1, K. Cornelius2, D.M. Scott-Coombes2, F. Eatock1 1Department of Endocrine Surgery, Royal Victoria Hospital, Belfast; 2Department of Endocrine Surgery, University Hospital of Wales, Cardiff
P33. The Role of Sesta-mibi scanning in the pre-operative diagnosis of parathyroid adenoma R. French, V. Kurup University Hospital North Tees
P34. Diagnostic role of CD56, HBME-1 and cyclin D1 in the differential diagnosis of thyroid cancer A. Ozolins1, I. Strumfa2, D. Gailis2, G. Volanska2 , Z. Narbuts1, J. Gardovskis1 1Department of Surgery, Pauls Stradins Clinical University Hospital, Riga, Latvia; 2Department of Pathology, Riga Stradins University
P35. Thyroidectomy Neck Scars and Cosmesis – A Systematic Review M. Dordea, S. Aspinall Department of Surgery, Northumbria Healthcare NHS Foundation Trust, UK
P36. The Changing Face of Thyroid Surgery in Scotland R.B. Townsley, B. Morris, O.J. Hilmi Department of Otolaryngology, Glasgow Royal Infirmary, Glasgow UK
P37. A Prospective Comparison of Complications in Re-Operative Thyroid Surgery between Local and National Data J.C. Hardman, J.A. Smith, J.C. Watkinson Department of Otolaryngology Head and Neck Surgery, Queen Elizabeth Hospital, Birmingham UK
P38. Vitamin D deficiency and severity of symptoms in primary hyperparathyroidism A.C. Walker, J.G.H. Hubbard, J.J. Fraile St Thomas’ Hospital, London UK
P39. Textural analysis of echo-planar diffusion-weighted imaging improves preoperative characterisation of suspected thyroid tumours S. Nagala1, A.M. Brown2,3, D. Scoffings4, M.A. McLean2, A.N. Priest5; P. Jani1, J.R. Griffiths2 1Department of Otolaryngology, Addenbrooke’s Hospital, University of Cambridge, UK, 2Cancer Research UK Cambridge Institute, Li Ka Shing Centre, University of Cambridge, UK, 3Duke University School of Medicine, Durham, NC, USA, 4Department of Radiology, Addenbrooke’s Hospital, Cambridge, UK, 5Department of Radiology, Addenbrooke’s Hospital, University of Cambridge, UK
P40. Radical adrenalectomy and IVC replacement after downstaging of adrenocortical cancer despite subtherapeutic levels of Mitotane R. Mihai1, Z. Soonawalla1, A. Weaver2, M. Petrou3 Department of Surgery1, Oncology2 and Cardiac Surgery3, Oxford University Hospitals NHS Trust
P41. Day Case Thyroid Surgery: on or off? J. Torres-Grau, J. Mason, J. Morgan, G. Kirby Southmead Hospital, Bristol, UK
P42. Should Thyroid Surgery be performed in an Airway Centre when there is a significant Airway Risk? A Literature Review of bilateral Vocal Paralysis with 2 Case Reports J.A. Joseph, P. Touska, N.S. Tolley Department of Endocrine and Thyroid Surgery, Hammersmith Hospital, Imperial College NHS Healthcare Trust
P43. Selective Radioiodine in intermediate group Papillary Thyroid Cancer I.J. Nixon1, S.G. Patel1, F.L. Palmer1, M.M. Di Lorenzo1, R.M. Tuttle2, A. Shaha1, J.P. Shah1, I. Ganly1 1Department of Head and Neck Surgery/2Department of Endocrinology, Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York, NY, 10065, USA
P44. Simulation-based learning improves the accuracy of thyroid fine needle aspiration cytology J. Ansell1, R.J. Egan2, M. Varma3 1Royal College of Surgeons of England Clinical Research Fellow, Welsh Institute for Minimal Access Therapy (WIMAT), Cardiff CF14 4UJ; 2Department of Endocrine and General Surgery, University Hospital of Wales, UK; 3Department of Histopathology, University Hospital of Wales, UK

The BAETS gratefully acknowledges the support of the following companies:
PLATINUM SPONSOR
GOLDEN SPONSORS
SILVER SPONSORS





























