Embed Size (px)
Citation preview

Med J Malaysia Vol 67 No 5 October 2012 549
INTRODUCTIONUltrasonography (US) is the imaging modality of choice forevaluating scrotal abnormalities. Scrotal swellings arefrequently seen in children and adolescents and narrowingdifferential diagnosis is important in assisting the referringclinicians and enhancing their efficiency in coming to adiagnosis. The spectrum ranges from incidental topathological findings and can be divided into chronic (or atleast subacute) and acute; painless and painful.
Familiarity with US is essential for establishing the correctdiagnosis. The objective of this pictorial review is to providecurrent information on common and unusual scrotalabnormalities.
Most common causes of painless scrotal swelling in childrenand adolescents include hydrocele and non-incarceratedinguinal hernia. Less common causes are varicocele,spermatocele, localized edema, and testicular tumors. Painfulscrotal swelling in children are usually require urgentdiagnosis and intervention and include but not limited toabscess, testicular torsion, torsed appendix ofepididymis/testis, and epidydmitis/orchitis.
KEY WORDS:ultrasound, pediatric, testes, swelling
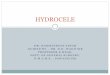
PAINFUL SCROTAL MASSESAbscessScrotal abscess can be a complication of epididymo-orchitis,trauma, or surgery. The clinical history and physicalexamination of a painful hyperemic scrotum is essential inmaking the diagnosis. On US, this lesion can have a varietyof appearances such as a heterogenous hypoechoic mass,thickened wall, and internal debris (Fig. 1). Areas of infectionare generally hyperemic and heterogeneous in echotexture. Iforganized, an abscess may have a well-defined hyperemicwall. If there is gas within the collection, hyperechoic fociwith “dirty” shadowing are seen.
Testicular torsionTesticular torsion leads to ischemia and possibly death of thetestis. There are two peak incidences for testicular torsion –one is during puberty and the other is during the neonatalperiod. There are two types of testicular torsion: extra andintra vaginal. Extra vaginal testicular torsion occurs inneonates, due to the loose attachment of testes and thespermatic cord to the scrotum thus the entire cord above thelevel of the scrotum can undergo torsion. Intra vaginal
testicular torsion occurs more frequently in boys undergoingpuberty. This is due to the abnormal development of thetunica vaginalis, where the tunica vaginalis completelycovers the epididymis and testis, thus the testis is not fixed tothe scrotal walls and is allowed to rotate freely. This deformityis usually seen on both sides, and would require surgicalfixation 1.
Usually, these children present with acute onset of severetesticular pain. The ischemia can lead to testicular necrosis ifnot corrected within 5-6 hours of the onset of pain 2. Torsioncan be intermittent and can undergo spontaneous de-torsion.US is the modality of choice and shows an enlargedhypoechoic testes, showing minimal or no internalvascularity (Figs. 2 and 3).
Torsion of testicular appendixThe appendix epididymis and appendix testis areembryologic remnants of the mesonephric (wolffian) ductand paramesonephric (müllerian) duct, respectively. Torsionof these appendages causes acute scrotal pain and a focalbluish discoloration beneath the skin (so-called “blue-dot”sign) in about one third of the cases; as well as a tendernodule is commonly palpated on physical examination 3. UStypically shows a nonvascular hyperechoic small oval massadjacent to the testis or epididymis, which may be associatedwith epididymal inflammation and hydrocele (Fig. 4).
In a child with an acute scrotum, torsion of testicularappendices represents the more common cause of scrotalpain rather than testicular torsion. Typically, torsion oftesticular appendices has a more gradual onset thantesticular torsion and patients may endure pain for severaldays before seeking medical attention.
Epididymitis and orchitisEpididymitis is the most common inflammatory processinvolving the scrotum and more common in adults but canoccur in children. Children usually present with fever, dysuriaand a painful scrotum. With the acute and sometimesexcruciating scrotal pain presentation associated with asevere orchitis, the clinicians do often encounter difficulties indifferentiating an orchitis with a testicular torsion or torsionof the testicular appendix. On conventional ultrasound bothorchitis and torsion may result in an enlarged diffusely orheterogeneously hypoechoic testes. US doppler is useful insuch a setting, as orchitis usually demonstrates an increasedvascular flow in the testicular parenchyma; while the torsedtestes will show decreased or absent vascularity withincreased flow at the testicular capsule.
Role of Ultrasound in Management of Scrotal Abnormalitiesin ChildrenHenry Oscar, FRCR (UK), Jeevesh Kapur, FRCR (UK)
National University Hospital, Department of Diagnostic Imaging, 5 Lower Kent Ridge Road, Singapore, 119074
CONTINUING MEDICAL EDUCATION
This article was accepted: 27 July 2012Corresponding Author: Jeevesh Kapur, National University Hospital, Department of Diagnostic Imaging, 5 Lower Kent Ridge Road, Singapore, 119074Email: [email protected]

Continuing Medical Education
550 Med J Malaysia Vol 67 No 5 October 2012
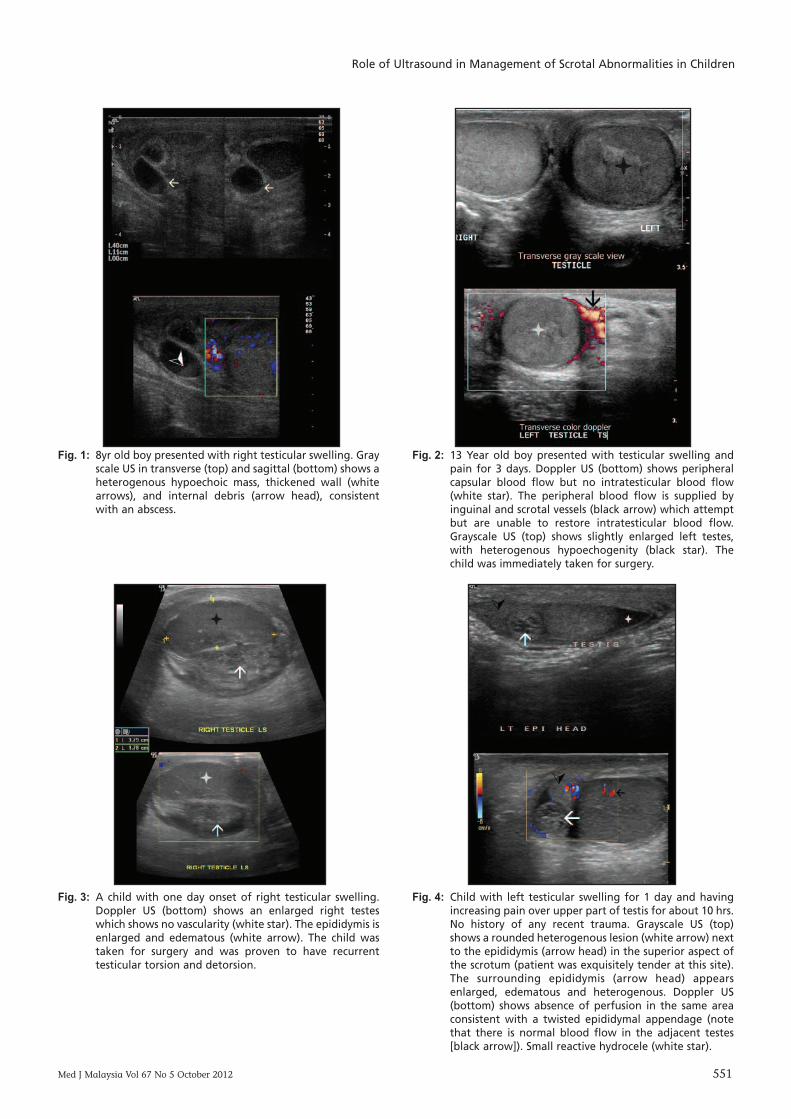
Orchitis is characterized by focal, peripheral, hypoechoiclesions that is poorly defined (Fig. 5). Orchitis may alsoexhibits testicular hyperemia on color Doppler US images,and is usually follows an underlying epididymitis 4 (Fig. 6). Areactive hydrocele may also be associated with epididymo-orchitis. Focal testicular infarction can also occur as acomplication of epididymitis when swelling of the epididymisis severe enough to constrict the testicular blood supply. Thisappears as a hypoechoic intratesticular mass devoid of bloodflow.
PAINLESS SCROTAL MASSESHydrocele, encysted hydrocele of the spermatic cord A hydrocele is a collection of fluid in the scrotal sac betweenthe layers of the tunica vaginalis; and is usually painless. Areactive hydrocele occurs when there is an underlyingpathology of the testes or its epididymis for example reactivehydrocele can occur in trauma, infection, torsion and tumors.Encysted hydrocele of the spermatic cord is a fluid along thespermatic cord, separated from and located above the testicleand the epididymis. This is due to abnormal closure of theprocessus vaginalis. There are two types of hydrocele ofspermatic cord - encysted hydrocele of the cord, and funicularhydrocele. Encysted hydrocele of the spermatic cord is whenthe fluid does not communicate with the peritoneum or thetunica vaginalis and the latter is where fluid is seencommunicating with the peritoneum at the internal ring. USshows well demarcated anechoic lesion in the inguinalregion, with no color flow on the Doppler (Fig. 7). Mostimportantly, the underlying testes and epididymis are normal5, 6.
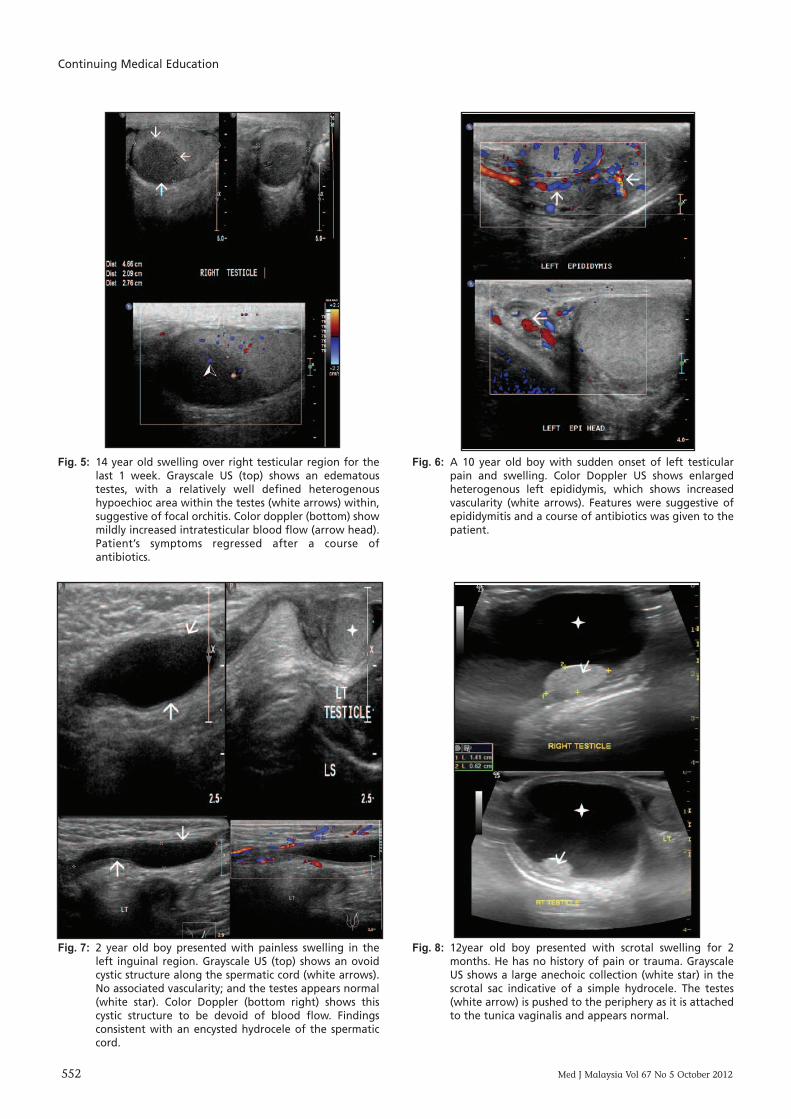
US features of a simple hydrocele include anechoiec welldemarcated fluid collection outlining the testis, with posterioracoustic enhancement. Presence of internal echoes/septaemay suggest a complex hydrocele, which could be secondaryto trauma or infection (Figs. 8 and 9).
MicrolithiasisTesticular microlithiasis appear as tiny nonshadowinghyperechoic foci ranging in diameter from 1-2 mm. They areusually intraparenchyma but can be seen distributedperipherally or segmentally; and maybe unilateral orbilateral (Fig. 10). Common consensus for the number ofmicroliths required to define testicular microlithiasis is five 7.
Several associations have been reported with testicularmicrolithiasis including Klinefelter's syndrome,cryptorchidism, Down's syndrome, malepseudohermaphroditism, pulmonary alveolar microlithiasis,previous radiotherapy, and subfertility states 8. The mostimportant association is with testicular neoplasms. These are,however, only associations, and no cause-and-effectrelationship has been established. Associations aside, theincreased risk appears to be real, as there are now severalcase reports documenting the interval development of germcell tumors of the testis in patients with previously identifiedisolated microlithiasis 8, 9, 10. As these patients withmicrolithiasis are usually found on incidental USinvestigation for other scrotal abnormality and are mostlyasymptomatic, the current recommendation in managementof microlithiasis is for annual US follow-up and patienteducation about self-examination 11.
Testicular tumorPediatric testicular tumors are uncommon occurrences.Teratomas and yolk sac tumors are most commonly testiculartumors before puberty and after puberty, embryonalcarcinoma occurs more frequently.
A painless testicular mass is the most common finding in achild with a testicular tumor. There are no sonographicfeatures that can reliably distinguish benign and malignanttumors. Size of the lesion is not a factor in determining if thelesion maybe benign or malignant. US features of testicularmalignancy may include enlarged testis, with ill-definedheterogenous hypoechoic areas (Figs. 11, 12, and 13). ColorDoppler US has also been reported to be more effective thangray-scale sonography in detecting intratesticular neoplasmsin the pediatric population 12.
If surgery is warranted, US can also assess whether there isenough normal testis parenchyma remaining for testissparing surgery 13, 14, 15. US can also be used to aid in imageguided biopsies.
Testicular tumor markers are important tools in theevaluation of testicular tumors in children. Alpha fetalprotein (AFP) is more reliable because it is secreted by 90% ofyolk sac tumors in children. Pointer in using AFP in thesepatients is to remember that serum AFP level is normally veryhigh in infancy. It measures in the tens of thousands innewborns and does not decrease to normal adult levels untilnearly 1 year of age 16. Therefore, although elevated AFP in achild older than 1 year with a testicular tumor almost alwaysreflects the presence of a yolk sac tumor, an "elevated" levelin infants can also occur in the case of benign tumors.
Scrotal wall edemaEdema of the scrotum can be due to a multitude of reasons,such as ascites, nephrotic syndrome, or even insect bites. It issometimes clinically difficult to assess the underlying testesdue to the overt overlying swelling, and thus US can providedvaluable tool in assessing the testes in such conditions. OnUS, features include marked thickening of the scrotal wallwith normal appearing testis and epidydmis (Fig. 14).Normal to slightly increased flow to the scrotal wall ondoppler is sometimes seen.
Inguinal herniaHernias in children are more common in premature infants.If the hernia is filled with bowel, it is usually easier to detect,but sometimes the hernia maybe filled with soft tissue such asomental fat. On US, the testis and epididymis are normal.Fluid or air containing loops in the scrotum or echogenicareas representing herniated omentum are seen (Fig. 15).Clinical examination of the inguinal canal to distinguishfrom primary scrotal pathology is essential.
HematomaUS plays a vital role in patients with penetrating or blunttrauma. Blunt trauma to the scrotum can lead to damage ofthe testicle and adjacent structures. Injuries to scrotuminclude laceration, hemorrhage, or contusion of the testicle.The goal of scrotal US in patients with acute trauma to thescrotum is to evaluate injury to the testicle. Acute intra-testicular hematomas appear hyperechoic at US and may
Role of Ultrasound in Management of Scrotal Abnormalities in Children
Fig. 1: 8yr old boy presented with right testicular swelling. Grayscale US in transverse (top) and sagittal (bottom) shows aheterogenous hypoechoic mass, thickened wall (whitearrows), and internal debris (arrow head), consistentwith an abscess.
Fig. 2: 13 Year old boy presented with testicular swelling andpain for 3 days. Doppler US (bottom) shows peripheralcapsular blood flow but no intratesticular blood flow(white star). The peripheral blood flow is supplied byinguinal and scrotal vessels (black arrow) which attemptbut are unable to restore intratesticular blood flow.Grayscale US (top) shows slightly enlarged left testes,with heterogenous hypoechogenity (black star). Thechild was immediately taken for surgery.
Fig. 3: A child with one day onset of right testicular swelling.Doppler US (bottom) shows an enlarged right testeswhich shows no vascularity (white star). The epididymis isenlarged and edematous (white arrow). The child wastaken for surgery and was proven to have recurrenttesticular torsion and detorsion.
Fig. 4: Child with left testicular swelling for 1 day and havingincreasing pain over upper part of testis for about 10 hrs.No history of any recent trauma. Grayscale US (top)shows a rounded heterogenous lesion (white arrow) nextto the epididymis (arrow head) in the superior aspect ofthe scrotum (patient was exquisitely tender at this site).The surrounding epididymis (arrow head) appearsenlarged, edematous and heterogenous. Doppler US(bottom) shows absence of perfusion in the same areaconsistent with a twisted epididymal appendage (notethat there is normal blood flow in the adjacent testes[black arrow]). Small reactive hydrocele (white star).
Med J Malaysia Vol 67 No 5 October 2012 551
Continuing Medical Education
552 Med J Malaysia Vol 67 No 5 October 2012
Fig. 7: 2 year old boy presented with painless swelling in theleft inguinal region. Grayscale US (top) shows an ovoidcystic structure along the spermatic cord (white arrows).No associated vascularity; and the testes appears normal(white star). Color Doppler (bottom right) shows thiscystic structure to be devoid of blood flow. Findingsconsistent with an encysted hydrocele of the spermaticcord.
Fig. 8: 12year old boy presented with scrotal swelling for 2months. He has no history of pain or trauma. GrayscaleUS shows a large anechoic collection (white star) in thescrotal sac indicative of a simple hydrocele. The testes(white arrow) is pushed to the periphery as it is attachedto the tunica vaginalis and appears normal.
Fig. 5: 14 year old swelling over right testicular region for thelast 1 week. Grayscale US (top) shows an edematoustestes, with a relatively well defined heterogenoushypoechioc area within the testes (white arrows) within,suggestive of focal orchitis. Color doppler (bottom) showmildly increased intratesticular blood flow (arrow head).Patient’s symptoms regressed after a course ofantibiotics.
Fig. 6: A 10 year old boy with sudden onset of left testicularpain and swelling. Color Doppler US shows enlargedheterogenous left epididymis, which shows increasedvascularity (white arrows). Features were suggestive ofepididymitis and a course of antibiotics was given to thepatient.
Role of Ultrasound in Management of Scrotal Abnormalities in Children
Med J Malaysia Vol 67 No 5 October 2012 553
Fig. 9: A 13 yr old boy with painless scrotal swelling of 1 monthduration. Grayscale US shows a large complex hydrocelewith multiple septations (white arrows) and internaldebris (black arrow). It was likely secondary to resolvinginfection.
Fig. 10: 7 year old boy, with history of cryptorchidism presentedwith possible swelling of his right testes. Grayscale USshowed numerous tiny nonshadowing hyperechoic foci(black arrows) scattered in the testes consistent withtesticular microlithiasis.
Fig. 11: 14 year old with known B cell lymphoma presentedwith progressive increasing painless scrotal swelling for2 months. No history of pain nor trauma. Grayscale US(top) shows heterogeneously ill defined hypoechoicintratesticular mass (black arrows). Color doppler(bottom) shows the mass to be extremely vascular(white arrows). Histologically proven to belymphomatous involvement.
Fig. 12: A 15 year old boy presented with painless righttesticular swelling for 4 months. Grayscale US (top)shows a nearly well-defined hypoechoic solid lesion inthe right testes (black arrow). Color Doppler (bottom)shows with increased peripheral vascularity (whitearrows). The lesion was biopsy proven to be aseminoma and an orchidectomy was performed.
Continuing Medical Education
554 Med J Malaysia Vol 67 No 5 October 2012
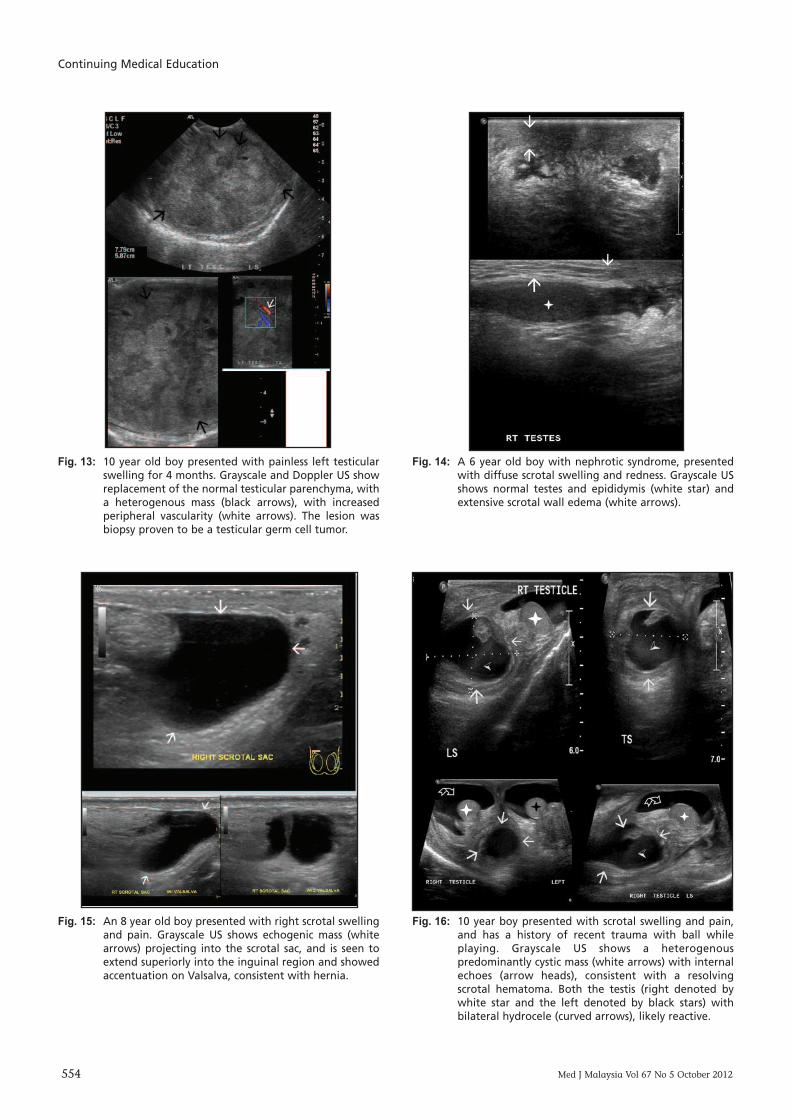
Fig. 13: 10 year old boy presented with painless left testicularswelling for 4 months. Grayscale and Doppler US showreplacement of the normal testicular parenchyma, witha heterogenous mass (black arrows), with increasedperipheral vascularity (white arrows). The lesion wasbiopsy proven to be a testicular germ cell tumor.
Fig. 14: A 6 year old boy with nephrotic syndrome, presentedwith diffuse scrotal swelling and redness. Grayscale USshows normal testes and epididymis (white star) andextensive scrotal wall edema (white arrows).
Fig. 15: An 8 year old boy presented with right scrotal swellingand pain. Grayscale US shows echogenic mass (whitearrows) projecting into the scrotal sac, and is seen toextend superiorly into the inguinal region and showedaccentuation on Valsalva, consistent with hernia.
Fig. 16: 10 year boy presented with scrotal swelling and pain,and has a history of recent trauma with ball whileplaying. Grayscale US shows a heterogenouspredominantly cystic mass (white arrows) with internalechoes (arrow heads), consistent with a resolvingscrotal hematoma. Both the testis (right denoted bywhite star and the left denoted by black stars) withbilateral hydrocele (curved arrows), likely reactive.

Role of Ultrasound in Management of Scrotal Abnormalities in Children
Med J Malaysia Vol 67 No 5 October 2012 555
simulate a focal mass. After 1–2 weeks, the hematomaundergoes liquefaction and may appear cystic. Thesonographic appearance can vary depending on the age ofthe hematoma, and at times it may be difficult todifferentiate between this entity and neoplastic lesions 17.
US usually shows an avascular mass, variable echogenicity(with age of hematoma) (Fig. 16). Associated findings ofscrotal hemaotma, hematocele and wall thickeningsometimes may give a clue.
VaricoceleVaricocele is abnormal dilatation of the pampiniform plexus.Varicocele is mass of painless enlarged testicular veins like abag of worms and usually occurs on the left due to the leftspermatic vein entering the left renal vein at a perpendicularangle (where else on the right, it enters the inferior vena cavaobliquely which may have protective element). Retrogradeflow into the spermatic vein causes dilatation and tortuouspampinifrom plexus. There are other more sinister causes ofvaricocele, such as mass effect or thrombosis of the renalveins, or the internal vena cava. As such, if an asymmetricright sided varicocele is found it is necessary to exclude othercauses of abdominal compression secondary effects 18.
On US, serpentine, anechoic structures greater than 2mm areseen with flow on the Doppler imaging; and shows venouswaveform on the pulsed Doppler imaging (Fig. 17).Augmentation of Doppler flow on valsalva and uprightposition are usually seen.
CONCLUSIONUS plays a major role in the diagnosis, follow up andmanagement of scrotal abnormality in pediatric age group.It is readily available, and usually the first and usually onlyinvestigation required for assessment of the scrotum andprovides an accurate insight into the underlying process. It isable to easily distinguish causes of acute scrotal swelling such
as testicular torsion and epidiymo-orchitis from not so acuteones such as hematomas, hydrocele and testicular tumors.
The authors declared no conflicts of interest.
APPENDIX: SONOGRAPHIC TERMS1. Echogenicity: refers to ‘brightness’ directly related to the
type and density of the tissue- echogenic/hyperechoic = bright- hypoechoic = dark- anechoic = black
2. Characteristics: refers to tissue composition- cystic = no internal echos, smooth borders good through
transmission, posterior enhancement- complex = cystic with solid components, septae- solid = no cystic areas
3. Pattern: refers to tissue uniformity- homogenous = uniform echos throughout- heterogenous = echo levels variable
4. Planes: sagittal and transverse- sagittal = divides into vertical plane (right half, left half)- transverse = divides into horizontal plane (top half,
bottom half)
REFERENCES1. Pavlica P, Barozzi L. Imaging of the acute scrotum. Eur Radiol 2001; 11:
220-228.2. Waldert M, Klatte T, Schmidbauer J, Remzi M, Lackner J, Marberger M.
Color doppler sonography reliably identifies testicular torsion in boys.Urology 2010; 75: 1170-4.
3. Frush DP, Sheldon CA. Diagnostic imaging for pediatric scrotal disorders.Radiographics 1998; 18: 969-85.
4. Cook J, Bewbury K. The changes seen on high resolution ultrasound inorchitis. Clinical Radiology 2000; 55: 13-8.
5. Martin LC, Share JC, Peters C, Atala A. Hydrocele of the spermatic cord:embryology and ultrasonographic appearance. Pediatr Radiol 1996; 126:528-30.
6. Kogan SJ. Acute and chronic scrotal swellings. In: Gillenwater JY,Grayhack JT, Howards SS, Duckett JW, ed. Adult and pediatric urology.Chicago, London, Boca Raton: Year Book Medical Publishers, 1987; 1948-1950.
7. Janze DL, Mathieson JR, Marsh Jl, et al. Testicular microlithiasis:sonographic and clinical features. AJR 1992; 158: 1057-60.
8. Frush DP, Kliewer MA, Madden JF. Testicular microlithiasis and subsequentdevelopment of metastatic germ cell tumor. AJR 1996; 167:889-90.
9. Doherty FL, Mullins TL, Sant GR, Drinkwater MA, Ucci AA Jr. Testicularmicrolithiasis: a unique sonographic appearance. J US Med 1987; 6:389-392.
10. Winter TC, III, Zunkel DE, Mack LA. Testicular carcinoma in a patient withpreviously demonstrated testicular microlithiasis. J Urol 1996; 155: 648.
11. Cast JE, Nelson WM, Early AS et al. Testicular microlithiasis: prevalenceand tumor risk in a population referred for scrotal sonography. AJR 2000;175: 1703-6.
12. Luker GD, Siegel MJ. Pediatric testicular tumors: Evaluation with gray-scale and color Doppler US. Radiology 1994; 191: 561-4.
13. Rushton HG, Belman AB, Sesterhenn I, Patterson K, Mostofi FK. Testicularsparing surgery for prepubertal teratoma of the testis: A clinical andpathological study. Urology 1990; 144: 726-30.
14. Grunert RT, Van Every MJ, Uehling DT. Bilateral epidermoid cysts of thetesticle. J Urology 1992; 147: 1599-601.
15. Valla JS for the Group D'Etude en Urologie Pediatrique. Testis-sparingsurgery for benign testicular tumors in children. Journal of Urology June2001; 165: 2280-3.
16. Wu JT, Book L, Sudar K. Serum alpha fetoprotein (AFP) levels in normalinfants. Pediatric Research 1981; 15:50-52.
17. LangerJE. US of the scrotum. Semin Roentgenology.1993; 28:5-18.18. Beddy P, et al. Testicular varicocele. Clinical Radiology. 2005; 60:1248-
1255.
Fig. 17: A 14 year old boy with pain and heaviness in the leftscrotum. Color Doppler US shows normal testes, withdilated pampiniform plexus (white arrows). The plexusshows accentuation on Valsalva (black arrows),appearing consistent with a varicocele.











![Idiopathic Infected Hydrocele in a Toddler: A Case Report ... · Hydrocele, the most common cause of scrotal swelling[1], is a fluid collection within the tunica vaginalis of the](https://img.pdfslide.us/doc/110x75/60bd41f77450a90b774b35f1/idiopathic-infected-hydrocele-in-a-toddler-a-case-report-hydrocele-the-most.jpg)