Embed Size (px)
Citation preview
CHAPTER -VI
ROLE OF INDIAN NATIONAL MOVEMENT (INM),
MISSIONARIES, PRESS AND INDIAN RESPONSES TO PUBLIC
HEALTH POLICIES
CHAPTER –VI
ROLE OF INDIAN NATIONAL MOVEMENT (INM), MISSIONARIES, PRESS AND INDIAN RESPONSES TO PUBLIC HEALTH POLICIES
In the previous chapter we have explained the aspects and expansion of
British Health Policy. Various historians have put their views regarding the
British health policies. They have looked into the effects of these policies on
Indian minds, their responses towards Western Health and Medicine System.
Mark Harrison has put the most liberal view by arguing that there was
suspicion, fear and hatred among the common poor towards the aim of
Government and therefore Imperial Government could not win the trust of the
indigenous population. He further argues that the community leaders played a
vital role towards satisfying the poor.1 He is very much true in his statement.
When we focus on 19th Century and early 20th century, a time at momentous
change in the history of medical science, technology and Indian society also,
we see the Indian elite class welcomes the technological and developmental
changes and contributes a lot by seeking employments in the Indian Civil
Services, legal services, and medical services.2 They come forward for the
1 Mark Harrison, ‘Public Health in British India: Anglo- Indian Preventive Medicine
1914, Cambridge; Cambridge University Press’ p.232. See also F.E. Udwadia (Editor) Man and Medicine: A History, Published in India, Oxford University Press, New Delhi, 2000, p.344.
2 In 1835 Indian Natives were selected in IMS, to serve as assistant civil surgeons. In the same year Calcutta Sanskrit College and Calcutta Madrasa started giving instructions in Ayurvedic and Unani systems, and professor Madhusudan Gupta provided the indigenous knowledge of the works of Charaka and Sushrauta along
134
transformation of the society. Leaders like Raja Ram Mohan Roy, Akshay
Kumar Dutta, Keshub Chandra Sen, Ishwar Chandra Vidhya Sagar propagated
and supported scientific developments and opposed social barriers as Sati and
child marriage and so 19th century India is regarded as a period of Renaissance.
(I)
Indian National Congress:-
As being the single largest political party, Indian National Congress
made a platform to bring out the problems of Indian people in front of the
imperial Government; it showed its concern for science and education. In the
9th resolution of INC, it was said:
‘We argue on government the desirability of encouraging
all branches of education, general as well as technical’. 3
It also showed its concern towards the growing poverty, and poor
industrial conditions in the Indian subcontinent. In the second resolution of
Indian National Congress, it was said:
‘That this Congress regards with the deepest sympathy
and views with grave apprehension, the increasing
poverty, desires to record its fixed conviction that the
with western medicine. Similarly Professor Sulfer Khan Ali taught Unani Tibb including the works of Unani physician Avicena at Calcutta Madrasa.
3 9th resolution presented in the report of four day proceedings of the fourth session of INC, (29th December 1888).
135
introduction of representative institutions will prove one
of the most important practical steps towards the
amelioration of the conditions of people’. 4
In the 3rd resolution passed at the 5th session of Indian National
Congress (1889) at Bombay, it was said:
‘There is an extreme importance of the appointment of
the mixed commission to enquire into the present
industrial conditions of the country, that this Congress
regards with the deepest sympathy and views with grave
apprehension, the increasing poverty, desires to record
its fixed conviction that the introduction of representative
institutions will prove one of the most important practical
steps towards the amelioration of the conditions of
people’.5
Indian National Congress opposed the government whenever it
witnessed the inadequate progress in these fields even after beseeching at the
different sessions of Indian National Congress.
Though Congress was aware of the poor hygienic conditions of the
industrial workers but it was not until the First World War when it showed its
interest in the field of Health & Medicine. After seeing the miserable condition
4 Second Resolution passed at the Second session of Indian National Congress held
in Calcutta (27th – 29th Dec., 1886). 5 Third Resolution passed at the fifth session of Indian National Congress held at
Bombay (1889)
136
that had been created by the First World War (1914) Indian National Congress
considered about the promotion of indigenous systems of medicine.6
And thus we see that M.K Gandhi7 ran a systematic programme of
village sanitation after 1914 and focused on personal cleanliness. Conversely
there were many orthodox people also who were divergent to science and
technology. They almost opposed every step of the Colonial Government.
There were influential individuals and reformists also who took up some
strategies to reform the society nevertheless it was not according to the
standard of the West, it was delicately according to the Indian culture.8
(II)
Efforts of Indian Elite for Women’s Emancipation:-
During the 19th Century (The age of renaissance) the educated
Indians came up to reform the public and private spheres of women life.
These reforms may be understood in the context of social reforms done by
British Government in India. The reformers supported the government
whole heartedly to improve the condition of women. They laid their
concern on issues like sati (widow burning), widow remarriage, and female 6 In the later year 1918, Congress took up the case of indigenous system of
medicine – Ayurveda and Unani and argued the government to give proper status to them.
7 Under the leadership of M.K.Gandhi, Congress gave prime importance to cottage industries which involved low level of technical skills. Health, hygiene and sanitation together with indigenous systems of medicine were promoted by M.K.Gandhi.
8 Muslim critiques as Nazir Ahmad and Maulana Hali strongly favored Purdah but were against the system that deprives the women from their basic liberties
137
infanticide child marriage. It was the sustain of Indian elite that the
Government was able to pass Sati Abolition Act (1829 & 1856), Widow
remarriage Act (1856) Female Infanticide Act (1870), Bill for the prohibition
of child marriage (1891).
A number of works were produced in the last quarter of 19th Century
aiming to remove the tribulations of female society and to uplift their moral
standards. These works were produced in vernacular language (Urdu) and
(Hindi). These journals and newspapers not only aimed at social and moral
training of women but they contained articles and information regarding
female diseases and the measures of prevention. Traditional Unani and
Ayurvedic medicines were suggested to the women for their motherhood
period. Medical aid to women was extended by generous individuals along
with the government’s efforts.
In 1878 Sir Salar Jung of Hyderabad opened a Zenana Dispensary. In the
same year a separate clinic for Zenana treatment was opened in Afzal Jung
Hospital Hyderabad. The foundation of Cama Hospital in 1886 at Bombay by a
Parsi lady Bhikaji Cama is most noteworthy; as she was the first women and
children’s hospital in India to be staffed exclusively by medically trained
women. In 1909 efforts to improve Traditional Midwifery were made by
Hakim Ajmal Khan who founded a training Centre for Dais (midwives) at Delhi.
Christian missionaries were the pioneers in starting the first training classes
for Dais (midwives) in 1866 at Amritsar.
138
The reformist Ulamas of Darul-Ulum-Deoband privileged the education
of Muslim women in the favor of patronizing purity of body, mind, and soul.
Maulana Ashraf Ali Thanevi wrote his celebrated work Bahishti Zewar9 for
women in which he described about two types of diseases among women-
general and female.10 He described the measures about the childcare and has
also prescribed preventive medicines for child as well as mothers also.
Maulana Ashraf Ali Thanewi said in the introduction of 9th Section of his book
Bahishti Zevar:-
‘Some methods should be adopted by women for the
maintenance of their health as well as their children the
women who do not know about all these cannot prove
themselves as good wives. Such problems can be resolved
easily by adopting the method of health care and
medicine as it was also appreciated by our Prophet
(PBUH)’.
Apart from suggesting medicine A.Thanevi suggested various Quranic
words and verses which could be used either through written amulets or
incantation. This sort of treatment according to A.Thanewi, could be very
effective in cases of stomachache, Cholera, plague, fever and small pox. The 9 It was a comprehensive handbook of fiqh especially for the education of girls &
women. It was first published in 1335 A.H., in 8 volumes. 10 Among females, diseases regarding menstruation, according to him accrued due
to some psychological stress and frustration among the young widows and unmarried girls at a general stage.
139
Indian elite turned their attention to the issues related to women’s health.
Macho Khan, Publisher of Mufidul Madaris, a monthly journal launched in
1872 from Agra, emphasized modern and scientific methods for midwifery.11
As said earlier in 19th century India ,condition of women was very
feeble in the sense that they were not allowed to discuss their health
problems even with their husbands, and their treatments during the mother
hood period was done by midwives who were not medical trainers.
A number of books were written by the eminent doctors of the time on
midwifery in the vernacular language There were another books published in
the last decades of 19th century they are:
Table-6.1: Books on Midwifery:
1. Dhatrividya (1886), two volumes - Khirodaprasad Chattopadhyay
2. Dhatrividya (1887) - Alok Chandra Das Gupta
3. Dhatrividya (1888) - Rajendra Nath Mitra
4. Nari Chikitsa (1888) - Shekhar Kumar Basu
5. Dhatri Sanchar (1893) - R.G. Kar & S.C. Basu
11 There were other journals also as Tehzib-e-Niswan founded by Syed Mumtaz Ali
(1898) and monthly/weekly Chashma-e-Khirad by Abdul Rahim Khan (1876) that played a vital role to aware the women section of the society.
140
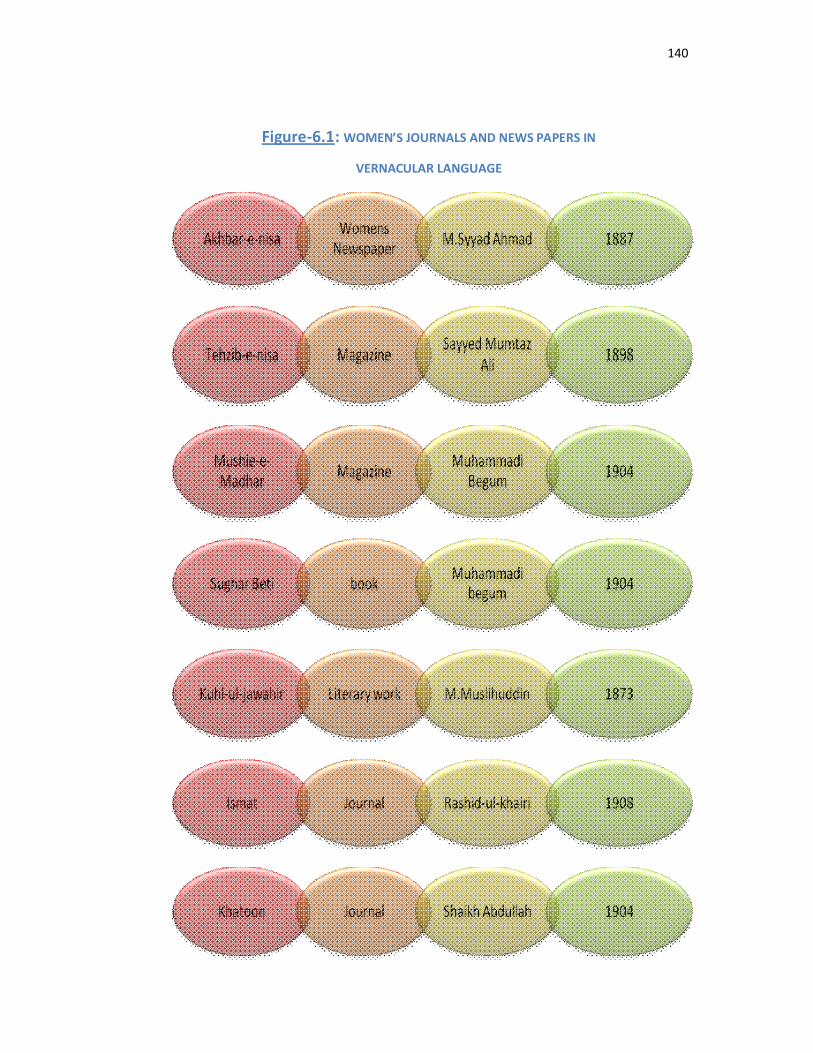
Figure-6.1: WOMEN’S JOURNALS AND NEWS PAPERS IN
VERNACULAR LANGUAGE
141
Many other quarterly journals and magazines were published at various
places.Shibchandra Sen published mother and child care manual-ShishuPalan
in1875 at Bengal. A journal Calcutta journal of medicine was published in
1868-69, regarding midwifery, childcare and mothers care. Similarly Dr.
Jadunath Mukhopadhyaya wrote Dhatrishiksha and Prasutishiksha in1891.It
was a progressive effort of the elite Indians to create awareness among them.
Christian missionaries took the first step in this regard to start training
classes for dais from 186612 Medical aid for women was also given by
generous individuals in 1878. Sir Salam Jung of Hyderabad opened a Zenana
dispensary also. Local Hindus and Muslims of high respect donated for the
establishment of charitable hospitals and dispensaries for the care of poor
people. The Ulamas of Darul- Ulum also patronized Unani Tibb which was
considered to be superior or equivalent to western medicine system. There
established three types of hospitals in India. 13
(i) Funded by provincial revenues
(ii) Financed by municipal & Local boards
(iii) By private subscribers among the private subscribers
12 Nursing services in Bombay also were provided by All saints sisters (missionaries)
from 1884-1902. Dr. Annette who served at Cama Hospital from 1894-1918 recommended the training of nurses.
13 Mridula Ramanna ‘Gauging Indian Responses to Western Medicine, Hospitals and Dispensaries’, Bombay Presidency, 1900-20. In Deepak Kumar, Disease and Medicine, in India, op.cit., p.236.
142
We also observe the direct state involvement whenever the diseases
became epidemic and covered the large area including the Native, Industrial,
Military and European settlements. Free distribution of some medicines as
malaria quinine,14 black pills15 and potassium permanganate16attracted the
people to come to the dispensaries and its effectiveness led the Indian people
realize the importance of its treatment.
(III)
Works of Missionaries: Canadian Baptists and Anglican missionaries in Southern Regions:-
The missionaries believed that the prevalence of superstitions and
ruthless belief among the indigenous communities led to heavy loss of lives.
As a result, India was perceived by the missionaries as a strange land of
irrational beliefs. However, by the last years of the nineteenth century,
western medical missionaries in India realized the implications of health care
systems along with the multifarious process of Christianization. In this context,
as late as the 1920s, a European medical missionary observed:
14 It was prepared from Alkaloid found especially in Cincona bark and used as
Febrifuge tonic and anti periodic. However, it was not fully effective it could have unpleasant side effects; also it was not every time available still it was a reliable remedy for malarial fever. From - NAI, GOI, ‘Report of the Director of Government, Cincona Plantations, Madras’, in Home Department Proceedings, Medical Branch, Nos. 38-39, Oct. 1887,
15 It proved to be slight effective medicine for plague and was distributed by the Government during the outbreak of plague in 1896 in Bombay.
16 Potassium per magnate was used to protect water supply from bacterias.
143
‘For the continued preservation of Christianity to Hindus
and Muslims, there is no more potent agency than the
work of Medical Mission. The successful evangelization of
a block of 320,000,000 may be regarded as the dream of
an enthusiast. But the idea of let us say 320 medical
missionaries, each ministering and witnessing to
1,000,000, no longer seems wildly impracticable’.17
By the end of the 19th Century, In Telgu region the involvement of the
medical missionaries with the treatment of diseases like tuberculosis and
leprosy became very prominent; the Canadian medical missionaries
constructed a big tubercular sanatorium at Rajahmundry to improve the
health standards of the rural laboring classes, who were particularly from
depressed-class background. The medical missionaries also renovated the
Ramachandrapuram and Vizianagaram leper homes to protect the diseased
from all forms of social discrimination.18
Nursing services in Bombay city were being provided by the Anglican
missionaries, since 1884. It was pointed out that modern methods of
treatment required constant skilled attention of doctors and trained nurses to
assist them in the hospitals. At the same time, the indifference of Indians in
contributing to the G.T. Hospital Nursing Association was also noted.
17 Basu R.S,’Medical Missionaries At Work: Canadian Baptist Missionaries in Telegu
Country, 1870-1952’, in Kumar Deepak, (edited) Disease and Medicine in India: A Historical Overview, op.cit., p.181.
18 Ibid., p.189
144
The statistics of attendance at hospitals and dispensaries had shown a
little change in Indian attitudes towards medical institutions. In his paper
presented at the Bombay Medical congress in 1909, Turner attributed the
repugnance to hospitals to the plague epidemic, and the unpopular measures
of segregation and isolation.19
Cholera and smallpox were not unknown to the Indians, but the great
mortality of plague was an unknown experience, and they ascribed this to
doctors and hospitals and not to the disease. This led to protests against the
infectious Diseases and hospitals in Bombay in 1897 and 1899. Turner
regretted that though thousands of patients left the hospitals cured, they did
not advise their caste men to resort to them. He believed that sanitary
knowledge should be provided to the inhibitions. Yet Indian financial support
of these institutions continued.
On occasion, the paucity of funds postponed the establishment of
dispensaries till Indian donors came forward, as in Khed district. Endowing
public welfare was in keeping with the Indian tradition. Thus the Ranchodlal
home medical relief institution was set up at Ahmedabad to provide relief to
those who were unable to attend hospitals and dispensaries. Thus the
19 Turner, J.A., ‘Sanitation in India’ in Transactions of the Bombay Medical Congress
1909, Bombay Printed and published by Benett Coleman, The Times Press, pp.462-63.
145
Ranchodlal home medical relief institution was set up at Ahmedabad to
provide relief to those who were unable to attend hospitals and dispensaries.
Indigenous responses: Positive and Negative:-
The indigenous section showed no particular response towards
government’s initiative. Since there had been no effective remedy for some of
the deadly diseases in the previous Indian system, the western medicine was
adopted by the Indians as in the case of Kala-azar, Surgery and Malaria. We
also see the poor people used to gather around the Missionaries in the hope
of getting free medicines for their ailments. We also see that the diseases,
which were treated by local practitioners in earlier decads of 19th Century,
were also being treated in the hospitals of the government. Slowly and
gradually many government hospitals were being opened:
1. Calcutta Medical College – 1835 2. Bombay Medical College – 1845 3. Calcutta University – 1857 4. Madras Medical College – 1875 5. Indian Medical Research Fund Association – 1911
Many researches were conducted in these hospitals. We have
evidences which suggest that people slowly and gradually were turning
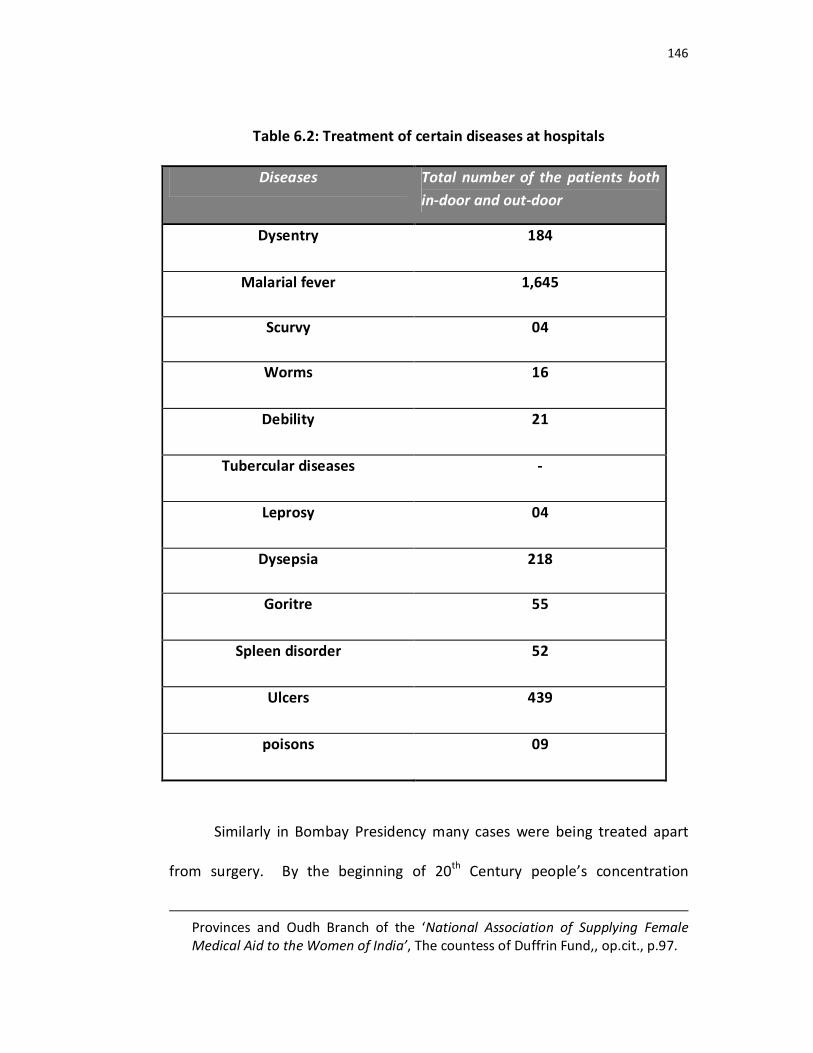
towards the western medicine. The following diseases were consulted by the
doctors of the hospitals established by countess of Dufferin fund.20
20 A letter from H. Fraser, the Chairman to the Honorary Secretary of the countess
of Dufferin’s Fund, Provincial Branch North Western Provinces & Oudh Branch Allahabad, 1st Dec., 1893 in Seventh Annual Report of the North Western
146
Table 6.2: Treatment of certain diseases at hospitals
Diseases Total number of the patients both in-door and out-door
Dysentry 184
Malarial fever 1,645
Scurvy 04
Worms 16
Debility 21
Tubercular diseases -
Leprosy 04
Dysepsia 218
Goritre 55
Spleen disorder 52
Ulcers 439
poisons 09
Similarly in Bombay Presidency many cases were being treated apart
from surgery. By the beginning of 20th Century people’s concentration
Provinces and Oudh Branch of the ‘National Association of Supplying Female Medical Aid to the Women of India’, The countess of Duffrin Fund,, op.cit., p.97.
147
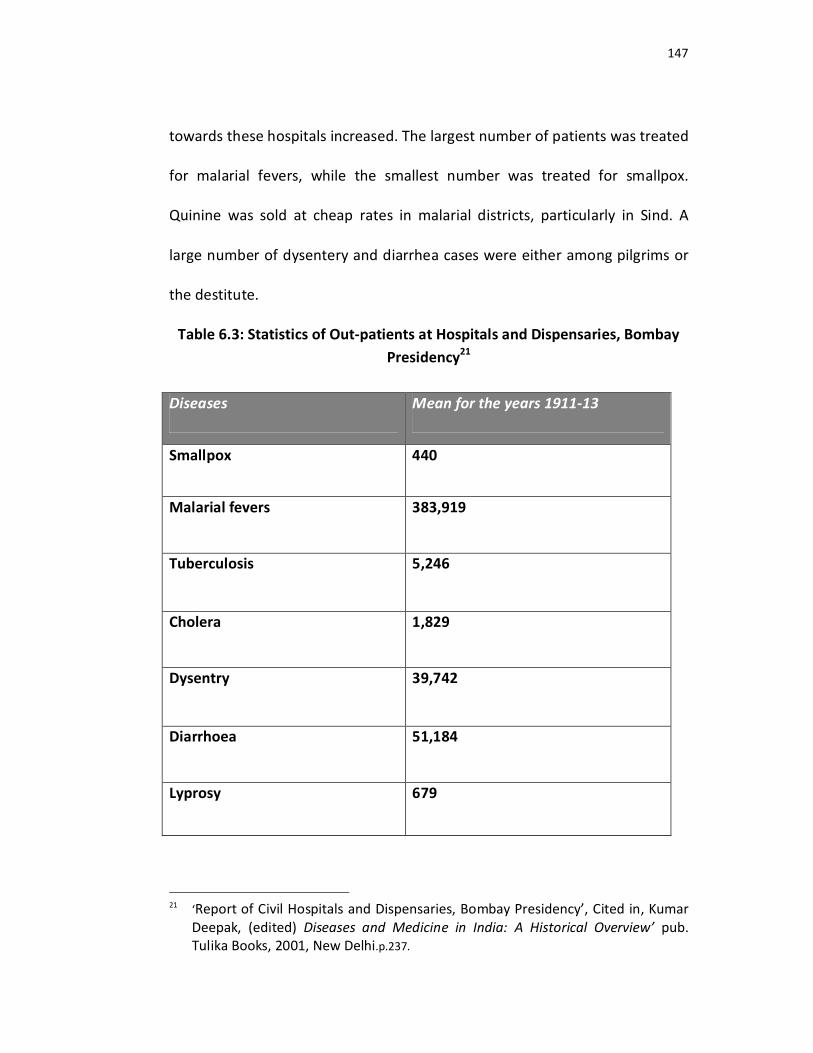
towards these hospitals increased. The largest number of patients was treated
for malarial fevers, while the smallest number was treated for smallpox.
Quinine was sold at cheap rates in malarial districts, particularly in Sind. A
large number of dysentery and diarrhea cases were either among pilgrims or
the destitute.
Table 6.3: Statistics of Out-patients at Hospitals and Dispensaries, Bombay Presidency21
Diseases Mean for the years 1911-13
Smallpox 440
Malarial fevers 383,919
Tuberculosis 5,246
Cholera 1,829
Dysentry 39,742
Diarrhoea 51,184
Lyprosy 679
21 ‘Report of Civil Hospitals and Dispensaries, Bombay Presidency’, Cited in, Kumar
Deepak, (edited) Diseases and Medicine in India: A Historical Overview’ pub. Tulika Books, 2001, New Delhi.p.237.
148
Though the indigenous section of society showed no clear response
towards the western health measures, but it is also evident that they did not stop
to go to those medical trainers who could provide them the cheapest medicine or
could suggest them the cheapest measures. That’s why the poor unaware class
always tried to seek shelter and protection in the worship of deities and in
performing rituals as suggested by Ojhas and Tantriks.
Let’s now consider the reasons why indigenous section was showing its
indifference towards some health care measures done by the government. Some
native people did not adopt vaccination because it could not match with their old
practice (inoculation). 22 Its secular nature was not accepted by some orthodox
people. Hindu community was not ready to have vaccination as it was prepared
with calf Lymph. The Brahmins thought it impurity if the lymph was taken from
the child of untouchables23 and the Muslims believed that the English were
searching for Mehdi (the Savior)24 in the veil of vaccination.25
There was also a problem of quick infection after vaccination on the
children. People fled away from the areas where vaccination was to be done, and
22 There was a problem of quick infection also just after the infection and the
researches suggested that diseases like syphilis and lyprosy were often transmitted through vaccination. From, Report on Vaccination, Bombay Presidency and Sind: 1873-74 XXIV, O.P.R. cited in Harrison Mark and Sanjoy Bhattacharya (edited), Fractured States: Small Pox, Public Health and Vaccination Policy in British India, 1800-1947, op.cit., p.58-59.
23 Satya Laxaman, Medicine, Disease and Ecology in Colonial India, p.248 24 According to Muslim belief (Mehdi) will be the person who will drove away the
evil from the world. 25 David Arnold, ‘Smallpox and Colonial Medicine in 19th Century India’, in Arnold
David edited, Imperial medicine and indigenous societies, op.cit. pp.45-65.
149
the British government made it compulsory for every one to be vaccinated.26 And
this step was welcomed by Indian elites.
Sir Syed Ahmad Khan the Indian member of Legislative Council also
favored the step.27 Sir Syed Ahmad Khan showed his courage and pointed out the
government’s negligence and indifference while imposing compulsory
vaccination and establishing Relief Camps. He suggested the government to
consider and understand the communities’ sentiments and to take lenient steps
to start such programs. Thus he delivered a speech in the legislative council and
convinced the government that Indian Community evils readily accept any step
taken by the government only if their sentiments are respected. This is an extract
of the introductory speech which he delivered on 30th September 1879 in the
Viceroy’s Legislative Council while introducing the vaccination Bill:28
‘My Lord there was a time when the people of this country
had prejudices, to which superstition and ignorance had
given birth, against the practice of vaccination. But the time
has now arrived when such nations no longer find the minds
of the gentry of India; Compulsory vaccination is thus a
26 Compulsory vaccination Acts in the various provinces were all first introduced in
selected urban centres. 27 Indian Press welcomed the steps taken by the government towards public health.
But they also apprised the interference of European in the affairs of local government by saying – ‘Any step to force sanitary measures an unwilling people must lead to failure’
28 Vaccination Bill introduced by Sir Syed Ahmad Khan in Viceroy’s Legislative Council, cited in Mohammad Shan, Writings and speeches of Sir Syed Ahmad Khan, Nachiketa Publication Limited, Bombay, 1972, pp.139-142.
150
measure for the protection of the lives of innocent children
from the results of the folly of their parents…..
My Lord, so far as my experience extends, I have no
hesitation in saying that compulsory vaccination would meet
the approval of the gentry of India. Indeed one of my Hindu
friends – a gentleman of good birth and good influence at
Benaras, the source of Hindu law and religion – asked me to
induce the government for making vaccination compulsory. I
have also received communication from respectable
Mohammadan gentle men of Punjab to impose compulsory
vaccination in Punjab region also…. Sir a law having for its
object the security of the future generations of India from a
calamity so universal and severe would, if properly put into
operation, for from being unpopular, be welcomed by the
people of this country.
Vaccination was favored by the Bengali News paper Hindu Patriot.29 The
doctors and surgeons of Indian origin in IMS also played a vital role in
propagating the vaccination programme. Some times the local members as
Hakims and Vaidyas were also appointed in vaccination camps to bring the
people and to convince them.30
29 Hindu Patriot, (News paper), ‘6 May 1878. 30 Mark Harrison, ‘Social History
151
E.A. Balfaur, Indian Medical Department has stated that these Vaids and
Hakeems also practiced as physicians in Madras Presidency and their number
was for greater than educated government servants. He noted that out of 8,000
practitioners in the territories under the government of Madras were 7,550 Vaids
and Hakeems and only 450 were educated doctors.31
The subordinate staffs who were generally, head constables, Chaukidards,
native vaccinators and even coolies were often employed by the government at
the time of fairs, epidemics, and at pilgrimage sites to communicate with the
people and to detect the sickness among the people. They also played a vital role
in informing the government about indigenous sentiments.32
However, the secular nature of the Government in establishing relief
camps & poor houses was also unacceptable because it interfered into the
religious and cultural practices of the community. Regarding the causes of the
unpopularity of the poor houses established by the government in the North
Western Provinces and Oudh, during the Famine of 1878, Sir Syed Ahmad Khan
said that the character of the management of the poor houses was not justified
as it did not respect the religions sentiments of the countrymen where as, the
poor house, managed by Sir Syed Ahmad Khan at Moradabad, during the time
when John Strachey was the Magistrate and Collector of Moradabad, gained
popularity, as it had following characteristics.33
31 NAI, Government of India, Home Department Proceedings, Medical Branch, NOS,
41-87, August, 1877. 32 Ibid. pp.45-70. 33 Report of the Indian Famine Commission, 1880-1885, pp.250-255.
152
1. Poor house was divided into different enclosures and separate areas were
assigned to different classes and castes.
2. A committee was formed which consisted of respectable Hindu and
Mohammadan members who would select persons fit for working.
3. Separate Chaukas were provided for each class.
4. Various kinds of works were performed as spinning, trusting of ropes,
weaving to support the poor etc.
As Plague had been an endemic disease in the Himalyan foot hills and the
regions of Kumayun and Garhwal, it occurred for many times in these regions.
The British government did not take serious steps until the International Sanitary
Conference held at Venice, blamed British government for existing cholera
tensions in India and then the plague.34 This international pressure and threats to
its overseas trade compelled GOI to take quick preventive measures to combat
plagues which were not acceptable for the indigenous section.
The municipal commissioner under the municipal board of 1888
authorized the municipal health officers to segregate the infected buildings.
Further Epidemic Disease Act was passed in 1897, and it authorized the officials
to inspect any ship, or passenger, to search to disinfect, to demolish any dwelling
or to stop any pilgrimage or religious fair.
The treatment of the officials with the indigenous section was really
painful. The passengers complained about the treatment of white doctors while
inspecting the sensitive body organs of male and female was intolerable. Even 34 The French attacked the British as ‘rulers of home of cholera and now one of the
epicenters of plague’.
153
the people preferred to die, rather than to be inspected or treated by the
doctors.35
The news of sexual harassment by the colonial officials became common
and the rumour was spread that the government made a deliberately crude
attempt to punish the people who had been involved in anti-colonial activities.36
These hasty steps taken by the government spread the wild rumors that
the sahibs had taken the poison from cobra and put it into the Bombay Water
Supply to spread plague.37As a result there occurred there occurred a number of
Anti plague riots.38
When GOI saw its failure, it started appointing the Vaids and Hakeems for
the treatment in camps and hospitals. Though some changes were done by
British Government and the values of India society were taken into consideration,
but even thereafter British Government could not win the trust of the indigenous
society. People did not show their positive response towards the village
sanitation programme because it levied more tax (sanitary tax) upon them. Due
to the unawareness also positive response was not seen from poor people
sanitary Commissioner of Assam reported:-
35 National Archives of India, Home, Medical, 2 February 1896, No.40. 36 Majumdar, R.C. History of the Freedom Movement in India, Vol.-I, Calcutta, 1971
pp.390-403. 37 Anil Kumar, ‘Medicine And The Raj:British Medical Policy in India 1835-1911,’
p.198. 38 Anti Plague riot occurred in Kanpur in 1900, Poona in & the people burnt the
segregation camps armed with lathis. R.C. Majumdar , p.400.
154
‘Much attention has given to rural sanitation but the Chief
Commissioner points out that title can be done until the
people have been educated to appreciate its benefits’.39
We have several other incidents which may tell us the indifferent attitude
response and resistance of the poor people. It was a particular poor and down
trodden section of the society who had a fear of imposing new tax among their
minds and therefore they used to flee here and there to escape from the
Government. However we do not notice any strong resistance or rebellion
against the Government. Regarding enumeration also there was fear amongst
the people but no special obstacles were encountered by the people as observed
by the district officials, when they were asked about it.40
The statistics collected by the hospitals and dispensaries show the
increase in the number of patients who used to come for cure especially for
surgery. The largest numbers of surgeries were for the removal of stone and
extraction of the lens for cataract. Other surgeries included abdominal
operations, operations for hernia, abuses of the liver etc.41
39 Report of the Sanitary Commissioner with the government of India (Assam) 1894,
p.259, 40 Census of India. N.W.P. 1872, Vol.-I, General, Report, Statements and tables-
Allahabad – 1873. Appendix-C, p.112. 41 Report of the Civil Hospitals and Dispensaries, Bombay Presidency, Bombay, 1909,
p.3.
155
(IV)
Role of Press:-
However there is another interesting aspect which can not be ignored
while talking about the responses, that is the role of press. The news papers,
magazines, journals did their work quite honestly in order to let the people
aware for their health problems. We find many opinions expressed through
press which were sometimes in favor and sometimes against the Western
Medical measures. Vernacular press also published some books in medicine
M. Kempson, Director of Public Instructions N.W.P. informed that the total
No. of registered publications in North Western Provinces during 1871 were
317 out of which 12 books (6 Urdu, 2 Hindi and 4 Persian) were published in
Medicine.42 We also find its dominant role in advertising the Indian traditional
products, healthy food etc. Many English newspapers and Medical journals
advertised for suppliers of western medicine and surgical instruments.
The news paper Abhyudya43 advertised a number of indigenous
medical products in its columns. The medical product Pran Sanjeevani was
42 M. Kempson, Director of Public Instruction N.W.P. to C.A. Elliotty Secretary to the
Government N.W.P. (No.3089) Date 20th Feb., 1872 in Selections From the Records of Government N.W.P. Vol.-VI, Allahabad Government Press, N.W.P., 1874, p.254.
43 It was the first Hindi weekly established by Madan Mohan Malviya in 1907.
156
advertised by using words like Ramban and Sulaimani.44 It also published the
book Hanuman Chalisa 45 for the advertisement of Pustraj Vatika. Arogyata Ki
Devi was printed for the advertisement of Amrit Dhara.46 The Medicine Piyush
Ratnakar, the remedy for 80 types of diseases was advertised by the news
paper Abhyudya.47 Often these newspapers /magazines published the articles
and opinion of various leaders in their columns. As compulsory vaccination
favored by Sir Syed Ahmad Khan was in the news lines in the Madras Times.48
To conclude, we can say that there was a consistent awareness among the
people. One cannot say that there was an absolute indifference towards
health care among the people.
44 ‘Abhyudya’ 18 February, 1912, p.8. 45 ‘ Abhyudya’, 18 Feb., 1912, p.7. 46 Abhyudya, 22 Feb., 1912. 47 Abhyudya; 18 Feb., 1912, p.8. 48 Madras Times, 3 July 1880, pp.2-3.