Embed Size (px)
Citation preview

Role of incretins inthe treatment of type 2 diabetes
Jens Juul HolstDepartment of Medical PhysiologyPanum InstituteUniversity of CopenhagenDenmark
Diabetes & ObesitySpanish Society of Internal MedicinePalma de Mallorca, February 2007

Incretin function in type 2 diabetes
• Secretion of GLP-1 impaired• Beta-cell sensitivity to GLP-1 decreased• Secretion of GIP slightly impaired• Effect of GIP abolished or grossly impaired

• If the impaired incretin responsecontributes significantly to the defectiveinsulin secretion in type 2 diabetes, willrestoration of incretin action improve metabolism?
00
22
44
66
88
1010
1212
1414
1616
00:0000:00 04:0004:00 08:0008:00 12:0012:00 16:0016:00
SnackSnackLunchLunchBreakfastBreakfast
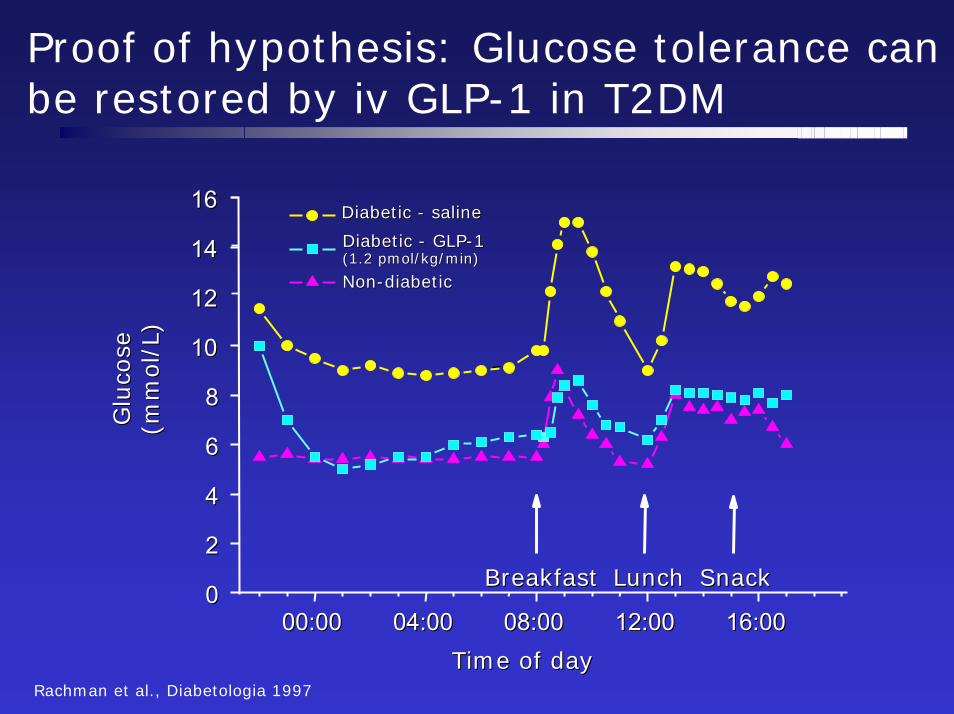
Diabetic Diabetic -- salinesaline
NonNon--diabeticdiabetic
Glu
cose
Glu
cose
(mm
ol/
L)(m
mol/
L)
Time of day Time of day Rachman et al., Diabetologia 1997
Proof of hypothesis: Glucose tolerance canbe restored by iv GLP-1 in T2DM
Diabetic Diabetic -- GLPGLP--11(1.2 (1.2 pmolpmol/kg/min)/kg/min)

Actions of GLP-1
• Insulin secretion:– Potentiates glucose-induced insulin secretion– Enhances all steps of insulin biosynthesis– Upregulates insulin gene expression– Upregulates expression of genes essential for beta-cell function
(glucokinase, Glut 2, etc.)– Mitotic for beta-cells– Promotes differentiation of duct progenitor cells– Inhibits apoptosis
• Inhibits glucagon secretion• Inhibits gastrointestinal secretion and motility• Inhibits appetite and food intake• Expedient cardiovascular effects

Native GLP-1 is rapidly degraded by DPP-IV
DPP-IV
7
37
9
T½ = 1–2 min (i.v.)MCR = 5–10 l/min
Vilsboll et al. J Clin Endocrinol Metab 2003
How can we exploit the therapeutical potential of GLP-1?
• Continuous administration of GLP-1

Effects of six weeks’ continuous subcutaneousinfusion of GLP-1 in patients with type 2diabetes
Zander et al, Lancet 2002

Main findings: Zander et al. Lancet 2002
• Continuous subcutanous infusion of GLP-1 for 6 weeks in type 2 diabetes patients:– Reduced fasting and mean plasma glucose by
4.3 and 5.5 mmol/l, respectively– Reduced HbA1c by 1.3% and normalised
fructosamine– Resulted in a weight loss of 2 kg, presumably
because of significantly reduced appetite– Improved insulin sensitivity and enhanced
beta-cell secretion– Had no significant side effects

ResultsWeek 0
Beta-cell function (C-peptide levels) Week 14000Week 6
2000
3000
pmol
/l
Saline NS1000
00 10 20 30 40 50 60 70 80 90
0
1000
2000
3000
4000
5000
6000
7000
0 10 20 30 40 50 60 70 80 90
pmol
/l
Incremental AUC:(0–90 min): p = 0.001
∆ values: p = 0.0002
GLP-1
Time (min)

How can we exploit the therapeuticalpotential of GLP-1?
• Continuous administration of GLP-1• Resistant analogues of GLP-1 (receptor activators, incretin mimetics)
GLP-1 receptor agonists
• Exendin 4, from saliva of the GilaMonster, 53%homologous withGLP-1 and fullagonist on the GLP-1 receptor
• Insensitive to DPP-IV
Gila Monster

0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.50
100
200
300
400
500
600
700
800 0.1 µg/kg0.2 µg/kg0.3 µg/kg0.4 µg/kg
Pla
sma
AC
2993
(pg/
mL)
Kinetics of s.c. AC2993 in type 2 diabetes patients
Time (hours after dose)Kolterman et al 2005

Placebo-ControlledTrials
Exenatide reduces HbA1c after 2 years
Add-on to existing OHA
Exenatide 10µg bid
Duration of treatment (years)
Open-Label UncontrolledExtension studies
∆A
1C (%
)
-1.2 ± 0.1%
0.0
-0.5
-1.5
-1.0
0.0 0.5 1.0 1.5 2.0
Baseline A1c8.2%
2 yr data for 82-wk cohort N = 146 Mean ± SE
Ratner et al, ADA 2005

Exenatide reduces body weight after 2 years
Add-on to existing OHA
Exenatide 10µg bid
-15.0
-12.5
-10.0
-7.5
-5.0
-2.5
0.0
2.5I II III IV
+1.9 kg
-2.5 kg
-5.9 kg
-12.2 kg
Meanbaseline weight: 104 kg 100 kg 97 kg 98 kg
Ch
ang
e in
bo
dy
wei
ght (
kg)
0 10 20 30 40 50 60 70 80 90 100 110-7
-6
-5
-4
-3
-2
-1
0
1
Time (wk)
Placebo-ControlledTrials
Open-Label UncontrolledExtension Studies
Baseline Weight100 kg
-4.7 ± 0.3 kg
∆ B
ody
Wei
ght (
kg)
N = 283; Mean (SE).
Henry et al. ADA 2006: 485-P
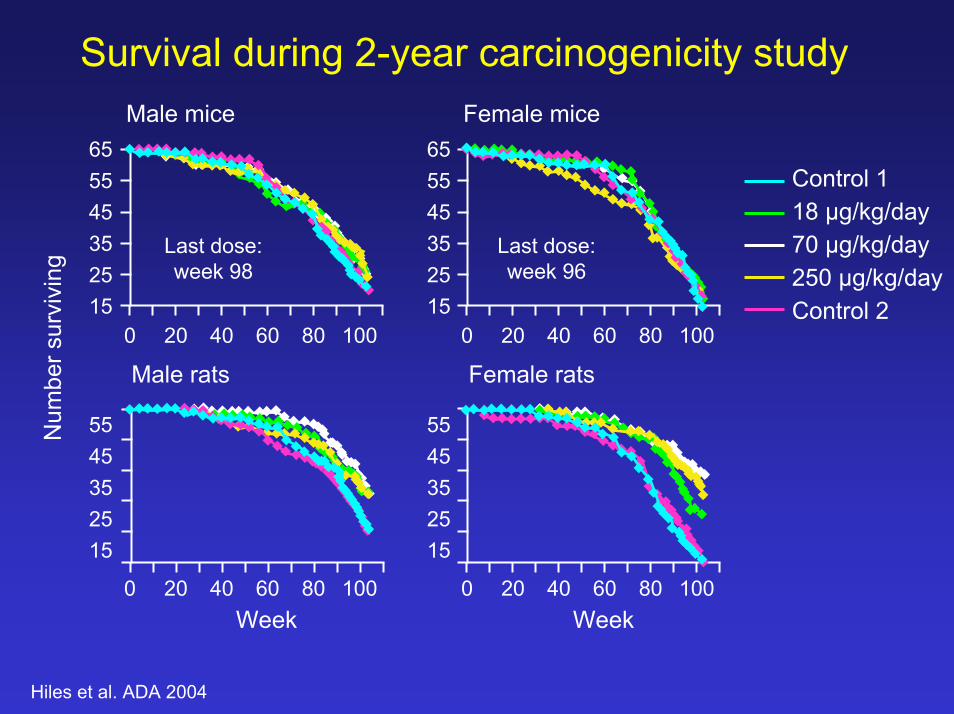
Survival during 2-year carcinogenicity studyMale mice Female mice
65
Hiles et al. ADA 2004
Num
ber s
urvi
ving
15
4555
0
3525
65
15
4555
3525
15
4555
3525
15
4555
3525
20 40 60 80 100 0 20 40 60 80 100
0 20 40 60 80 100 0 20 40 60 80 100Week Week
Male rats Female rats
Last dose:week 98
Last dose:week 96
Control 118 µg/kg/day70 µg/kg/day250 µg/kg/dayControl 2

Exenatide has been on the marketin the US since June 1 2005 under thename ”Byetta” and launch in Europeis expected in May 2007

Liraglutide is a long-acting GLP-1 derivative
Improved pharmacokinetics by:• Self association• Albumin binding
• Slow absorption from subcutis• Metabolic stability• Long plasma half-life • Stability against DPP-IV
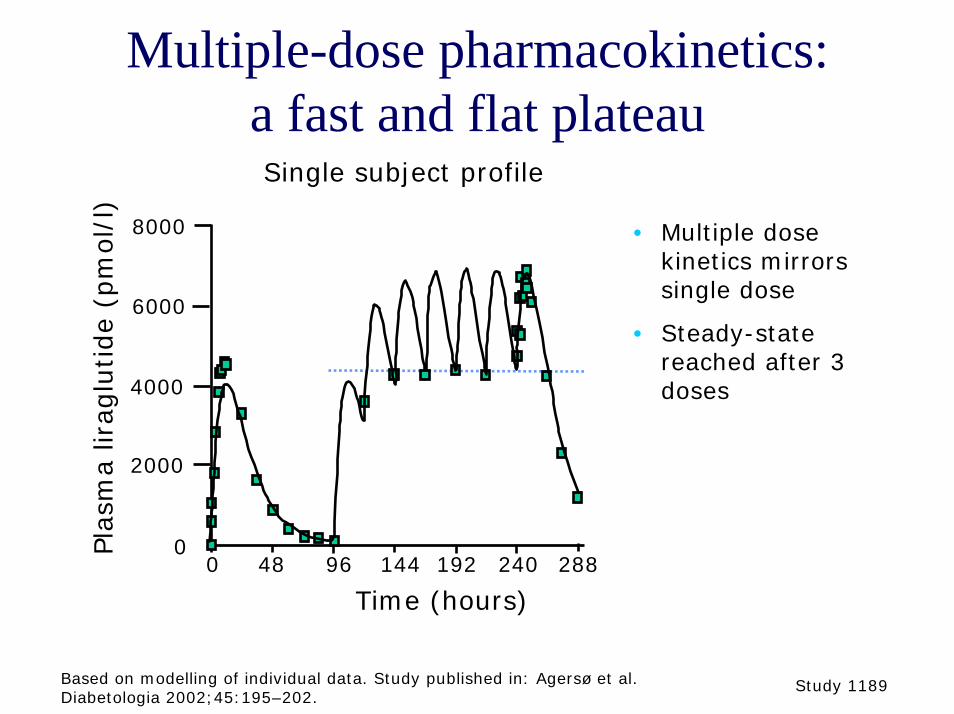
Multiple-dose pharmacokinetics: a fast and flat plateau
Pla
sma
lirag
lutide
(pm
ol/
l)
Time (hours)0 48 288144 192 24096
6000
4000
2000
0
8000 • Multiple dose kinetics mirrors single dose
• Steady-state reached after 3 doses
Single subject profile
Based on modelling of individual data. Study published in: Agersø et al. Diabetologia 2002;45:195–202.
Study 1189

Liraglutide, Phase 2b-studies (June 2006):
•165 patients with type 2 diabetes previously treated with OAA,HbA1c 8.5 %
•Double-blind, placebo-controlled, randomised trial•Liraglutide was given for 14 weeks in monotherapy
•HbA1c decreased 1.5-2 %, 45 % had < 7% (vs < 8 % in Placebo)•Fasting BG reduced by > 3 mmol/L•Body weight decreased by 3 kg from 90 kg.
•Nausea in 5-10 % initially, decreasing markedly with time.•No hypoglycaemia
• Vilsboll et al: ADA 2006

Liraglutide, japanese study (August 2006):
•200 subjects previously treated withdiet/exercise and/or single oral agentwere given liraglutide once daily•HbA1c down 2.0 % after 15 weeks•75 % below 7 %•No hypoglycemia

How can we exploit the therapeuticalpotential of GLP-1?
• Continuous administration of GLP-1• Inhibition of GLP-1 degradation• Resistant analogues of GLP
(receptor activators, incretin mimetics)

Survival of s.c. GLP-1 in type 2 diabetes
0 30 60 90 120 150 180 210 240
Time (min)
0
100
200
300
400
GLP
-1 (p
mol
/l)
**
** ** ** ** ** *
Intact GLP-1 + metabolite
Intact GLP-1
Deacon et al. 1995
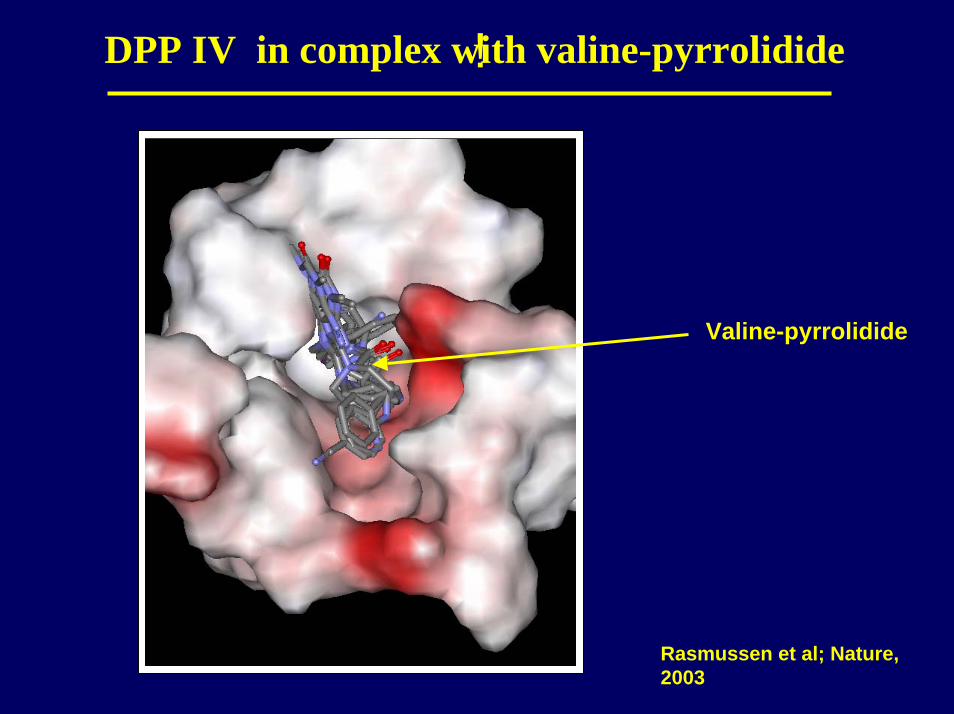
!DPP IV in complex w valine-pyrrolidideith
Valine-pyrrolidide
Rasmussen et al; Nature, 2003
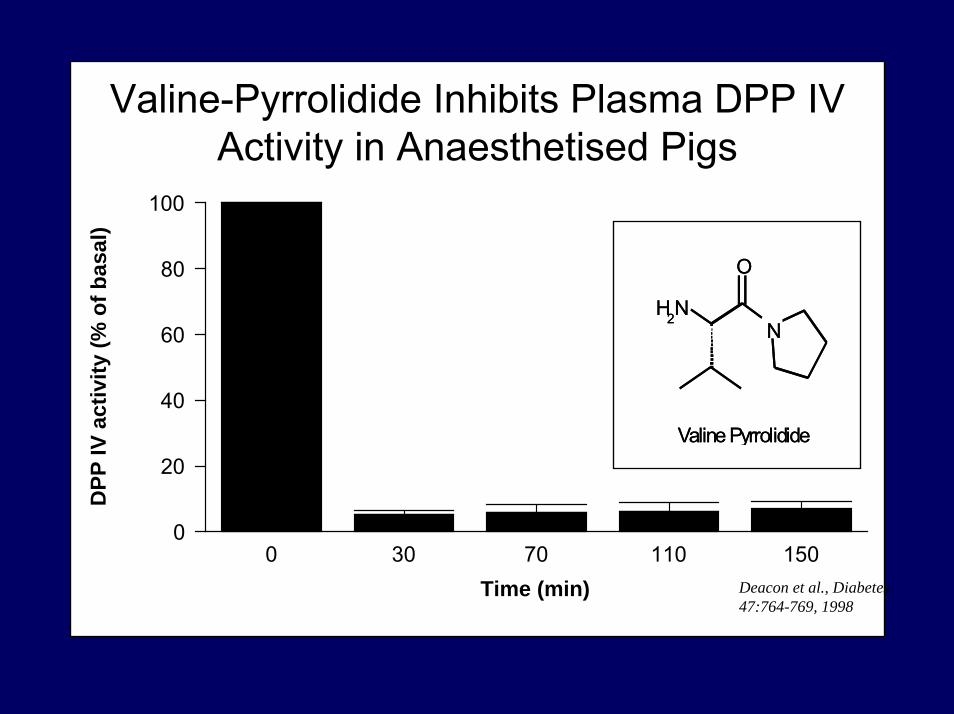
Valine-Pyrrolidide Inhibits Plasma DPP IV Activity in Anaesthetised Pigs
0 30 70 110 150Time (min)
0
20
40
60
80
100
DPP
IV a
ctiv
ity (%
of b
asa l
)
N
O
NH2
Valine Pyrrolidide
N
O
NH2
Valine Pyrrolidide
Deacon et al., Diabetes 47:764-769, 1998
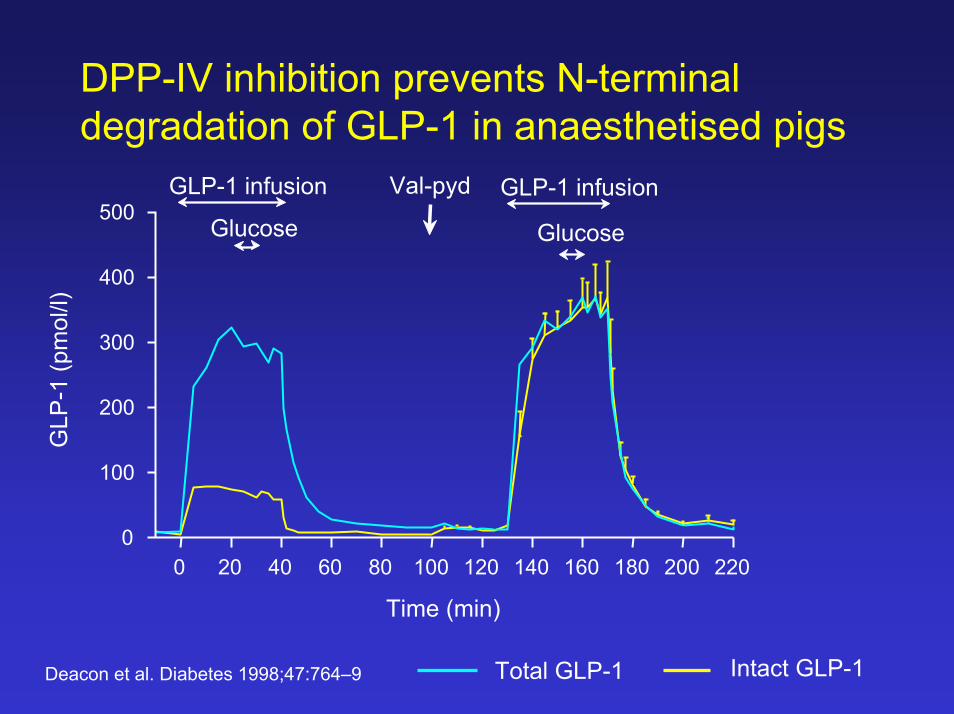
DPP-IV inhibition prevents N-terminal degradation of GLP-1 in anaesthetised pigs
Deacon et al. Diabetes 1998;47:764–9
0 20 40 60 80 100 120 140 160 180 200 220
GLP-1 infusion
Glucose
GLP-1 infusion
Glucose
Val-pyd500
GLP
-1 (p
mol
/l)
400
300
200
100
0
Time (min)
Intact GLP-1Total GLP-1

DPP-IV inhibition enhances GLP-1 induced insulin secretin in pigs
0 10 20 30 40 50 60 70 80 90–10–20–300
100
200
300
400
500
600
Insu
lin (p
mol
/l)
GLP-1 infusion
Glucose
Val-pyr
Time (min)+ Val-pyr - Val-pyr

More than 30 companies start to develop DPP-IV inhibitors
Leading compounds:
Novartis: LAF 237 (Vildagliptin, Galvus)
Merck: MK-0431 (Sitagliptin, Januvia)

Diabetes Care 2004
–4 0 4 8 12 16 20 24 28 32 36 40 44 48 526.8
7.2
7.6
8.0
8.4
LAF/MET(core, ITT, n = 56)
PBO/MET(core, ITT, n = 51)
LAF/MET(extension, ITT, n = 42)
PBO/MET(extension, ITT, n = 29)
Time (weeks)MET, metformin; PBO, placebo
Ahrén et al. LAF 237 for 12 and 52 weeks
HbA
1c(%
)

Meal-related beta-cell function and insulin sensitivity by LAF 237 (vildagliptin) in metformin-treated patients with type 2 diabetes
0.050
0.045
0.040
0.035
0.030
0.0250 12 24 52
300
Insu
lin s
ensi
tivity
275
250
225
200
14
12
10
8
60 12 24 52 0 12 24 52
Ada
ptat
ion
inde
x
Time (weeks) Time (weeks) Time (weeks)
* * * * * * * **
Insu
lin s
ecre
tion
LAF 237 + Metformin Metformin alone
Ahrén et al. Diabetes Care 2005;28:1936–40
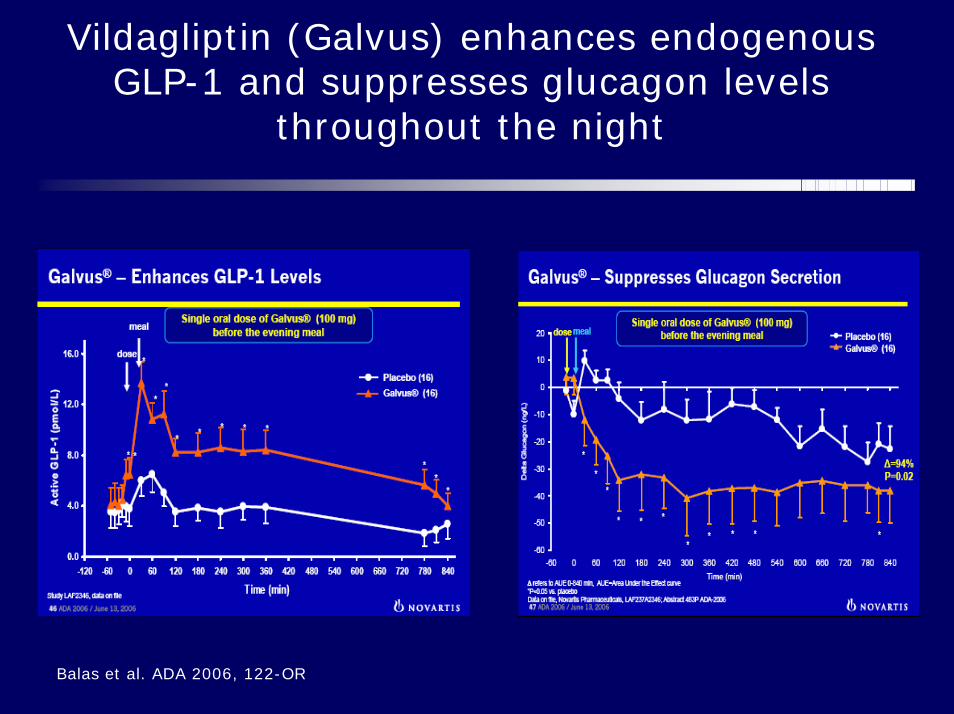
Vildagliptin (Galvus) enhances endogenousGLP-1 and suppresses glucagon levels
throughout the night
Balas et al. ADA 2006, 122-OR

Vildagliptin (Galvus) suppresses endogenousglucose production throughout the night
Balas et al. ADA 2006, 122-OR
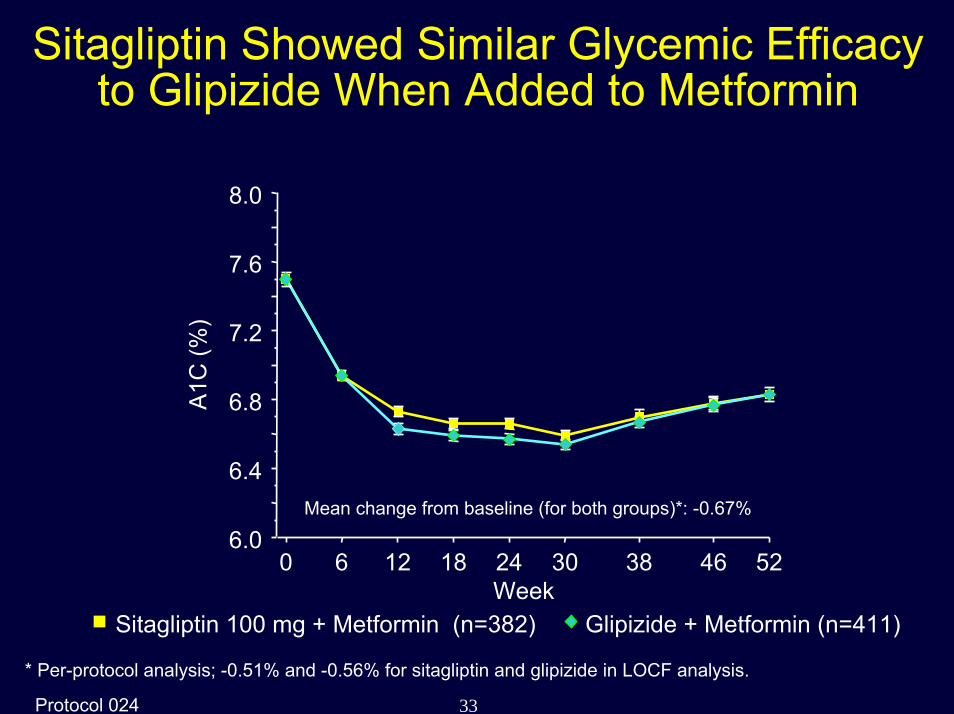
33Protocol 024
Sitagliptin Showed Similar Glycemic Efficacy to Glipizide When Added to Metformin
Week0 6 12 18 24 30 38 46 52
A1C
(%)
6.0
6.4
6.8
7.2
7.6
8.0
Mean change from baseline (for both groups)*: -0.67%
Sitagliptin 100 mg + Metformin (n=382) Glipizide + Metformin (n=411)
* Per-protocol analysis; -0.51% and -0.56% for sitagliptin and glipizide in LOCF analysis.

34Protocol 024
Progressively Greater Reductions in A1C as Baseline A1C Rises
Per Protocol Population
Study inclusion criteria 6.5-10%.
∆ A
1C (%
)
-2.4
-2.0
-1.6
-1.2
-0.8
-0.4
0.0
Baseline A1C Category<7% 7 - <8% 8 - <9% ≥9%
Sitagliptin 100 mg qd Glipizide
-1.68 -1.76
-1.13 -1.11
-.53 -.59
-.27 -.13

35Protocol 024
Sitagliptin Once Daily Showed Decreased Body Weight Compared to Glipizide (52 Weeks)
∆ between groups = –2.5 kg (p<0.001)
86
88
90
92
94
0 12 24 38 52Time (weeks)
Bod
y W
eigh
t (kg
)
Sitagliptin 100 mg + Metformin (n=382)Glipizide + metformin (n=411)
Hypoglycaemia: Sitagl. 4.9 %, Glipizide 32 %
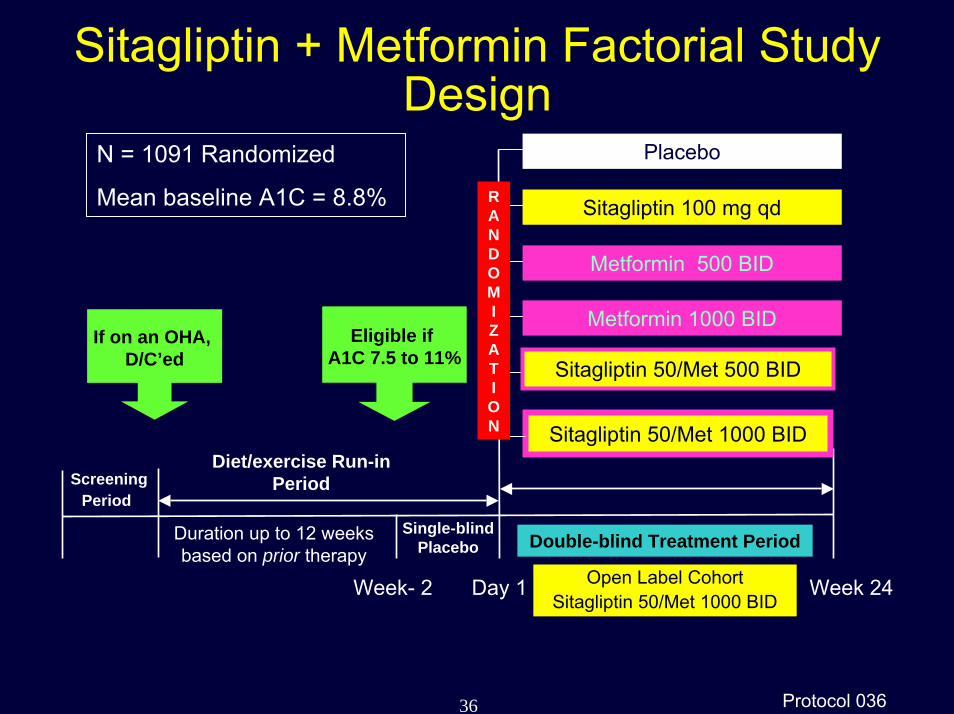
36 Protocol 036
Sitagliptin + Metformin Factorial Study Design
N = 1091 Randomized
Mean baseline A1C = 8.8%
ScreeningPeriod
Single-blindPlacebo Double-blind Treatment Period
Diet/exercise Run-in Period
Eligible if A1C 7.5 to 11%
If on an OHA, D/C’ed
Week- 2 Day 1
Sitagliptin 50/Met 1000 BID
Placebo
Sitagliptin 100 mg qd
Metformin 500 BID
Metformin 1000 BID
Sitagliptin 50/Met 500 BID
Week 24
Duration up to 12 weeks based on prior therapy
Open Label Cohort Sitagliptin 50/Met 1000 BID
RANDOMIZATION

37 Protocol 036
Initial Combination of Sitagliptin and MetforminProduced a Marked Improvement in A1C
A1C
(%)
Sita 50 mg b.i.d+ Met 1000 mg b.i.d.
Sita 50 mg b.i.d+ Met 500 mg b.i.d.
Met 1000 mg b.i.d.
Met 500 mg b.i.d.
Sita 100 mg q.d.
Placebo
0 6 12 18 246.5
7.0
7.5
8.0
8.5
9.0
9.5
Week

Clinical experience with DPP-IV inhibitors:
• There is experience from up to 104 weeks treatment inthousands of patients
• The inhibitors are comparable to existing OADs in monotherapy
• They show additional efficacy when used in combination bothwith SU, glitazones, metformin and insulin.
• Their effect on HbA1C is maintained for 104 weeks
• Effect on HbA1c depends on starting level (up to 3 %)

DPP-IV inhibition:
•Inhibitors (Januvia) for once daily oral administrationare already on the market in the US and in Mexico
•Recommended for Approval in Europe, Jan. 2007
•So far no class related adverse effects
•Effective in experimental and clinical diabetes
•Potential for diabetes prevention
•Neutral with respect to body weight

Conclusions
• GLP-1 based therapy of type 2 diabetes mellitus canbe expected to:
– reduce hyperglycaemia andHbA1C levels– Reduce appetite and lower body weight
(agonists) or be weight neutral (inhibitors)– Improve blood lipids– Improve insulin sensitivity– Enhance beta-cell secretion– Be efficacious without side effects
• Will the therapy prevent progression of disease?
![Combination Use of Insulin and Incretins in Type 2 ... Update - Incretins- Insulin v… · Combination Use of Insulin and Incretins in Type 2 Diabetes [DRAFT] 1 1 BACKGROUND Type](https://img.pdfslide.us/doc/110x75/5f2de9130649e313ed28bd46/combination-use-of-insulin-and-incretins-in-type-2-update-incretins-insulin.jpg)