Embed Size (px)
Citation preview

Gut, 1992, 33, 460-465
Role of duplex Doppler ultrasound in the assessmentof patients with postprandial abdominal pain
A F Muller
AbstractIn 10 patients with postprandial abdominalpain thought likely to be the result ofmesentericischaemia Doppler ultrasound examinations ofthe superior mesenteric and coeliac arterieswere performed both after fasting and astandard meal of 800 kcal. Compared withcontrol values Doppler waveform analysis sug-gested seven abnormal vessels. Two patientshad abnormal fasting superior mesentericartery waveforms manifested by very high peaksystolic velocities together with spectralbroadening (one also had evidence of coeliacartery stenosis), and one patient had normalvelocities but an abnormal signal and evidenceof proximal superior mesenteric stenosis wassupported by colour Doppler imaging andconfirmed by angiography. Postprandialiy, twopatients showed very high peak systolic andend diastolic velocities in the superior mesen-teric artery (one had had a normal fastingwaveform signal) and one in the coeliac artery,suggestive of vascular stenosis, while onepatient showed a fall in peak systolic velocity.The diagnosis of mesenteric ischaemia in twoof these patients was supported by digitalsubtraction angiography and abdominal com-puted tomography. Doppler ultrasound maybe a useful non-invasive investigation forpatients with postprandial abdominal pain thathelps to select patients for angiography.Patients with tight vascular stenosis may haveabnormal fasting Doppler waveform patternsbut in symptomatic patients further informa-tion may be obtained after the haemodynamicstress of feeding. Additional information toenhance the diagnostic sensitivity of the testmay be obtained by colour Doppler imaging.
vascular disease.' Similarly, symptoms may arisefrom reduced blood flow - the so called non-occlusive mesenteric ischaemia - usually as aconsequence of massive blood loss but also inthose with very poor cardiac reserve.
Doppler ultrasound has become increasinglyimportant in investigating abdominal vasculardisease. Both the coeliac and superior mesentericvessels have been studied in detail in response tophysiological stimuli such as feeding andexercise."'2 Dubbins'3 has reported its use indiagnosing renal artery stenosis, and a fewanecdotal reports have discussed the potentialrole of ultrasound in investigating both superiormesenteric artery and coeliac artery stenosis.' "These papers found abnormal velocity profilesacross stenosed vessels, and the non-uniformvelocities within the sample volume which mayoccur in areas of turbulence or stenosis'7 havebeen termed 'spectral broadening,' an additionalindicator of high grade stenoses.'3-'5This study aimed to assess the likelihood of
mesenteric ischaemia (used collectively todescribe stenosis of either the superior mesen-teric and coeliac arteries and assuming stenosisor occlusion of the inferior mesenteric artery) in agroup of patients with postprandial abdominalpain in whom previous investigations had provedunhelpful. From a knowledge of the velocitywaveform changes seen postprandially in normalsubjects,"7'" it might be expected that diges-tion would accentuate the velocity waveformchanges seen in vascular stenosis. While a numberof authors have commented that a meal would bea useful circulatory stress test of the gut, this isthe first paper to describe the effects of a meal inpatients with a high possibility of actually havingmesenteric ischaemia using duplex Dopplerultrasound.
Atherosclerosis of the coeliac, superior, andinferior mesenteric arteries is claimed to affectup to 50% ofpeople over the age of45 years and iseven more frequent when there is coexistentvascular disease elsewhere.A4 Despite the factthat chronic abdominal pain is a common com-plaint, 'intestinal angina' is diagnosed only in-frequently. It is generally accepted that at leasttwo of the three splanchnic vessels need to showhaemodynamically significant stenoses or com-plete occlusion2 for symptoms to occur, andultrasound, which is being used increasingly inthe investigation of abdominal disease, may havea role in selecting patients for more invasiveinvestigations such as angiography.While splanchnic ischaemia is usually caused
by progressive atherosclerosis of proximalarteries, the same symptoms may result fromexternal compression, fibromuscular hyper-plasia, or small vessel disease typified by collagen
Patients and methodsSubjects were drawn from both hospital in-patients and outpatients. Ten patients of mean(SEM) age 67 (2) years (three women, 64-77years) were studied. All complained of post-prandial epigastric pain occurring between 30and 60 minutes after a meal, with seven patientscommenting that symptoms were related to thesize of the meal. Two had lost weight and one hadcomplained of a change in bowel habit (thispatient had had a normal barium enema save forthe presence of scattered diverticulae). All hadevidence of some form of cardiovascular disease:hypertension (2), ischaemic heart disease (5),cardiac failure (2), the presence of carotid bruits/or peripheral vascular disease or both (2), andone patient had a 4 cm abdominal aorticaneurysm. Eight ofthe 10 patients had undergoneupper gastrointestinal endoscopy as part of their
Department of Medicine,University Hospital,Nottingham NG7 2UHA F MullerAccepted for publication2 July 1991
460

Role ofduplex Doppler ultrasound in the assessment ofpatients with postprandial abdominal pain
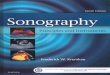
Pulsatility index =
Peak to peak amplitude (AB)
Peak systolic Meanvelocity (Vmax)
- --------------------------- Mean
End diastolic- B velocity (Vmin)
Figure 1: Doppler waveform parameters measured in both the superior mesenteric and coeliacarteries (time averaged velocity not shown).
diagnostic assessment and in each case this wasnormal. Haematochemical parameters in allpatients were also normal. In view of theassociated cardiovascular diseases, mesentericischaemia was considered a distinct possibility toexplain their symptoms. Although formal angio-
cm/s
12o01
100L-
80k60 .
401.-
201-
0
cm/s
200 1
180 1
160
140
120
100
80
60
40
20 _
0
graphy was not performed routinely, the diag-nosis of mesenteric ischaemia in three patientswas supported by additional investigations, andthese included: a digital subtraction angiographystudy; abdominal computed tomography to lookfor evidence of pancreatic disease, which showeda very narrow superior mesenteric artery withpancreatic ischaemia, and angiography, at thesame time as coronary angiography was per-formed.Twenty volunteers aged 26-68 years (mean
(SEM) age 46 (3) years; 20 superior mesentericand 10 coeliac arteries) were similarly studied toestablish normal values. Previous studies haveshown that there is no relation between para-meters of superior mesenteric artery blood flowand age. 16
All subjects were asked to fast overnight andthe following morning abdominal ultrasono-graphy was performed after 30 minutes' supinerest on an examination couch. Superior mesen-teric and coeliac arteries were identified by duplex
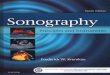
Figure 2: Pre- (above) and postprandial (below) Doppler wavejorn patternsfJr the superior mesenteric arterv in a volunteer.Systolic and diastolic velocities can be seen to increase postprandially.
461

Muller
TABLE I Mean (SEM) valuesfor Doppler waveform parameters ofthe superior mesenteric (n=20) and coeliac (n= 10) arteriesin control subjects before and after an 800 kcal meal with the respective changes seen in the patients thought to have abnormalwaveforms. Exceptfor pulsatility index (PI), units are cm/second
Superior mesentenc arteryPre-meal Post meal
Vmax Vmin TAMV PI Vmax Vmin TAMV PI100-5(4-2) 16(0 9) 35(1*1) 3-6(0 2) 154(7-8) 46(2 5) 59(5-2) 1*8(0 3)
97 24 33 2-7 95 30 40 1-2162 22 36 3-7 (No postprandial signals)145 47 50 1-7 310 131 116 1-396 14 25 3-2 63 26 22 1-9108 20 28 3-1 312 78 70 2-4Coeliac artery
Normal subjects 120 (7)Patient no,
age/sex:(2) 73/M 156(6) 68/F 127
30 (3-3) 30 (3 3) 1-5 (0-2) 130 (2 2) 40(48) 41(33) 15(01)
53 66 1-5 (No postprandial signals - pt 2 above)36 40 1-5 225 70 69
Vmax=peak systolic velocity; Vmin=end diastolic velocity; TAMV=time averaged mean velocity; PI=pulsatility index.
ultrasound of the upper abdomen, either longi-tudinally or transversely. Both a 5 MHz curvi-linear probe or sector scanner were used, eachwith 2 MHz offset Doppler, keeping the angle ofinsonation ofthe Doppler beam as low as possibleand constant for repeated measurements. Theproximal portion of each vessel was scannedinitially, having adjusted the sample volume sizeto the diameter of the vessel. After this, thevessels were scanned along their visible length.Fasting measurements were made on threeoccasions. The inferior mesenteric artery wasinconsistently visualised. Figure 1 shows theparameters of blood flow that were measured byDoppler (Doptek Ltd). These included peaksystolic and end diastolic velocities, meanvelocity, and pulsatility index, a measurement ofdistal vascular impedance.9'19 To enhance thediagnostic assessment, two patients withabnormal waveforms were also studied using aultrasound machine with integral colour flowimaging facilities (Diasonics, SonotronVingmed).18
All subjects then received a standard 800 kcalmeal containing 90 g carbohydrate and 35 g eachof fat and protein. Serial Doppler measurementswere made over the next hour with peak changesbeing accepted.
Doppler ultrasound examinations were per-formed by a single operator. In the light ofprevious reported changes in superior mesenteric
and coeliac artery blood flow postprandially itwas not possible for the operator to be blinded asto whether subjects had been fed or not.
ResultsThe coefficients of variation for repeated fastingparameters were all less than 10%.
CONTROL SUBJECTSFigure 2 shows the pre- and postprandial Dopplerwaveform patterns for the superior mesentericartery in a control subject. Mean results for thegroup are shown in Table I. The meal caused anincrease in both systolic and diastolic velocities,mean velocity, and a fall in the pulsatility index,indicative of a fall in distal mesenteric vascularimpedance. As can be seen in Table I,the changes in these parameters in the coeliacartery were less noticeable confirming that thebulk of coeliac artery blood flow is not to thegut.
PATIENTS
Fasting waveform parametersOf the 10 patients studied, seven vessels (fivesuperior mesenteric and two coeliac arteries)were deemed abnormal by Doppler criteria either
TABLE II Author's assessment ofpre- and postprandial superior mesenteric and coeliac artery Doppler waveforms. Only thosepatients thought to have abnormal vessels are quoted. Patient numbers correspond with those described in Table I
Superior mesenteric artery Coeliac artery
Patient no Fasting Post meal Fasting Post meal Comments
(1) Abnormal Abnormal Normnal Normal Colour Doppler showed proximal stenosis confirmedwaveform by angiography. (See Figs 3 and 4)
(2) Abnormal No signal Abnormal No signal Suggestive of tight proximal stenoses. DSA scanwaveform confirmed 80% SMA and 50% coeliac stenosis
(3) Abnormal Abnormal, Normal Normal Suggestive of tight proximal stenosis. CT scanwaveform spectral showed stenosed SMA with pancreatic ischaemiawith spectral broadeningbroadening
(4) Normal Abnormal, Normal Normal ? Tight stenosis ? Non-occlusive ischaemia. (Pt withfall in Vmax low output cardiac failure)and Vmin
(5) Normal Abnormal, Normal Normal Suggestive of moderate SMA stenosisspectralbroadening
(6) Normal Normal Normal Abnormal, Suggestive of moderate coeliac stenosis. (Pt withhigh abdominal aneurysm)velocities
DSA=digital subtraction angiography; SMA=superior mesenteric artery; CT=computed tomography.
462
Normal subjectsPatient no,
age (yrs)/sex:(1) 68/F(2) 73/M(3) 74/M(4) 77/F(5) 65/M
1-4

Role ofduplex Doppler ultrasound in the assessment ofpatients with postprandial abdominal pain
cm / s
120 -
100
80
60 .
40 .
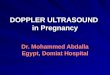
Figure 3: The abnormalfasting Doppler waveformpattern in patient I whichchanged littlepostprandially. Stenosis wasconfirmed by colour Doppler(Fig 4) and angiography.
20 k
0
pre- or postprandially, or both (Table I). TableII shows the author's assessment of the pre- andpostprandial waveforms for each of the vesselsfor the patients numbered in Table I.Two patients were found to have abnormal
fasting superior mesenteric artery waveformsmanifested by high peak systolic velocities, withone of these patients showing a high diastolicvelocity with spectral broadening. These changeswere thought to represent moderate to severesuperior mesenteric artery stenosis. One of thesepatients (patient 2) was also shown to haveresting coeliac waveform parameters consider-ably higher than those of any of the controlsubjects, suggesting coeliac artery stenosis aswell. This patient was investigated further bydigital subtraction angiography and shown tohave proximal stenosis of both vessels (superiormesenteric artery 80%, coeliac >50%).The other three patients had normal fasting
parameters for the superior mesenteric arterybut the waveform pattern was deemed abnormalin patient 1 (Fig 3). This patient was studiedagain using colour Doppler and was shown tohave proximal superior mesenteric artery stenosiswith appreciable turbulence in comparison withthe expected colour picture in a control subject(Fig 4). This patient suffered from ischaemicheart disease, aortic stenosis, peripheral vascularand carotid vascular disease for which she hadhad both femoral angioplasties and carotidendarterectomies on two occasions. The failureto alter significantly parameters of postprandialsuperior mesenteric artery blood flow was takento suggest a severe stenosis which was confirmedby an angiogram at the time ofcardiac catheterisa-tion.
Postprandial waveform changesBecause all subjects showed a postprandial fall inthe pulsatility index of an order similar to thatseen in the controls, this was not found to be auseful measurement in defining abdominalvascular stenosis. Satisfactory postprandialsignals could not be obtained in one patient butthe fasting parameters for both coeliac andsuperior mesenteric arteries were abnormal
(Table I). In two subjects there was a noticeableincrease in both systolic and diastolic velocities,far in excess of that seen in the controls. One ofthese subjects had been identified from fastingtraces as being likely to have mesenteric stenosis(Fig 5) but in the other the fasting traces werethought to be normal. One patient was thoughtto have shown an abnormal response post-prandially in the coeliac artery suggestingstenosis but at present has not undergone furtherinvestigation to confirm the diagnosis. Patient 1showed little change in peak systolic velocitypostprandially but was thought to have anabnormal waveform, and a colour ultrasoundexamination that was highly suggestive ofsuperior mesenteric artery stenosis. In patient 4,systolic velocity together with mean velocity fellpostprandially. This lady had complained ofweight loss and postprandial abdominal pain formore than two years without obvious cause andhad troublesome cardiac failure. It was thoughtthat this result was suggestive of either severestenosis or non-occlusive mesenteric ischaemiafrom a low output cardiac failure. Abdominalultrasound, chest x ray, and haematochemicalparameters were normal but further invasiveinvestigation was not performed because of hermedical problems.
DiscussionThese results suggest that for patients withsymptoms of postprandial abdominal pain inwhich other (often extensive) investigations haveproved unhelpful, Doppler ultrasound may havean important role in confirming the possibility ofmesenteric ischaemia and enable a more appro-priate selection of patients for angiography.Fasting Doppler signals may be abnormal but insubjects with apparently normal fasting signals,the use of a meal as a circulatory stress test to thegut will provide additional information.
For symptoms of mesenteric ischaemia tooccur, at least two ofthe three splanchnic arteriesneed to be stenosed or occluded.) Because theinferior mesenteric artery is frequently asympto-matically occluded and in most patients is adifficult vessel to visualise satisfactorily using
11
463

464 Muller
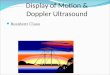
Figure 4: Fasting colourDoppler pictures ofthe superiormesenteric and coeliac arteries (arrowed) in (A) a controlsubject, and (B) a patient with mesenteric stenosis. Flowtowards the ultrasound probe is showvn in red. The whitecoloration seen resultsfrom turbulence around a proximal.superior mesenteric artery stenosis (arrowed).
ultrasound, the coeliac and superior mesentericarteries, which can be more easily examined,should be analysed carefully for evidence ofproximal stenosis. The results presented forabnormal fasting Doppler signals agree withthose of others'14 16: patients with ischaemia mayshow abnormal waveforms, manifested by highpeak systolic velocities, and spectral broadeningand these two features have been taken torepresent high grade stenoses. Jager'14 confirmedthis impression in one patient by digital sub-traction angiography. Nicholls'16 examined anumber of different Doppler waveformparameters in both normal subjects and fourpatients with symptoms thought to be caused bymesenteric ischaemia that was subsequently con-firmed by angiography. In his subjects, whowere studied in the fasting state, a loss of reversediastolic flow in stenotic superior mesentericarteries compared with controls and consider-ably higher values for systolic and diastolicvelocities were observed.
Previous reports have established an ultra-sound diagnosis in the fasting state and none havereported the effects of a meal in such a group of
pains h ddtoa nomainpoieby thisworkillustrates how a test meal may~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
proidevdece f plnchicvasulr sensievni ujcsta ae'oml atn wv-formparameters. It is possible that such a~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~findingrpresents less sevre stenoss but thiremains peculatve as tis grou of patents di
not have confirmation by angiography, unlikeNicholls' patients. Additionally, even if fastingwaveform patterns are normal or abnormal,there may be no change in postprandial Dopplerparameters and they may actually fall. Thesefindings may represent a tight vascular stenosisor possibly non-occlusive mesenteric ischaemia.The use of colour Doppler imaging may help inthe investigation of these patients and it may bepossible to quantify the degree of vascularstenosis without the need for Doppler spectralanalysis.20Buchardt Hansen, et all' have previously
shown that patients with angiographicallydemonstrated severe stenoses affecting the threesplanchnic arteries had normal fasting splanchnicblood flow when compared with control subjectsin whom angiograms measured by hepatic veincatheterisation using indocyanine green werenormal. These patients, however, failed toincrease their splanchnic blood flow post-prandially but were shown to do so aftersplanchnic vascular reconstruction. In patientswith less severe arterial lesions, flow did increasepostprandially but the authors could not deter-mine whether these patients had intestinalischaemia as the cause of their pain. While this isopen to question, Poole, et al,22 using tonometryas an indirect measurement of intramural pH,showed that when greyhounds were subjected topartial occlusion ofthe superior mesenteric arterythere was a precipitous decrease in tissue pH as aconsequence ofa decrease in oxygen delivery andthe addition of a meal into the stomach resultedin a more severe acidosis. They proposed this asthe mechanism for the symptom of pain thatpatients experience. Ifthis is true, even moderatestenoses may, under certain circumstances, resultin symptoms.
Patients with tight vascular stenosis of thesplanchnic arteries may have abnormal fastingDoppler waveform signals. More moderatedegrees of stenosis may be found in symptomaticpatients after the haemodynamic stress of feed-ing. Doppler ultrasound is a useful tool inassessing the evidence for mesenteric ischaemiaand newer technology such as the use of colourflow imaging may make this easier. The avail-ability of a non-invasive screening test will helpto select those patients that need to be consideredfor angiography. For patients that have under-gone either surgery or transluminal angioplasty23for this condition, Doppler ultrasound may alsobe expected to be of value in predicting furtherstenosis.
Preliminary results from this study were presented at the autumnmeeting of the British Society of Gastroenterology, Southampton1990.The author thanks Dr C J Hawkey for his helpful comments on
reviewing the manuscript.
1 Anonymous. Chronic intestinal ischaemia. [Editorial]. Lancet1977; ii: 1332-3.
2 Derrick JR, Pollard HS, Moore RM. The pattern of athero-sclerotic narrowing of the celiac and superior mesentericarteries. Ann Surg 1959; 149: 684-9.
3 Marston A. Vascular disease of the gut. London: EdwardArnold, 1986.
4 Croft RJ, Menon GP, Marston A. Does intestinal angina exist?A critical study of obstructed visceral arteries. Br J Surg1981; 68: 316-8.
5 Hunter GC, Guernsey JM. Mesenteric ischaemia. Med ClinNorth Am 1988; 72: 1091-1 15.

Role ofduplex Doppler ultrasound in the assessment ofpatients with postprandial abdominal pain 465
Figure 5: Pre- (A) andpostprandial (B) Dopplerwaveform patterns in apatient with superiormesenteric artery stenosis.The abnormalfastingwaveform shows a high peaksystolic velocity. This isaccentuated in thepostprandial signal andaccompanied by very highpeak systolic and diastolicvelocities.
cm/s180 _
160 _
140
120
100
80
60
40
20
0 B
cm/s
220
200
180
160
140
120
I0080
40
20
0 - _________________-
6 Qamar MI, Read AE. Effects of ingestion of carbohydrate, fat,protein and water on the mesenteric blood flow in man.Scandj Gastroenterol 1988; 23: 26-30.
7 Qamar MI, Read AE, Mountford R. Increased superiormesenteric artery blood flow after glucose but not lactuloseingestion. QJ3 Med 1986; 60: 893-6.
8 Qamar MI, Read AE, Skidmore R, Evans JM, WilliamsonRCN. Transcutaneous Doppler ultrasound measurement ofcoeliac axis blood flow in man. Brj Surg 1985; 72: 391-3.
9 Qamar MI, Read AE. Intestinal blood flow. QJrMed 1985; 56:417-9.
10 Moneta GL, Taylor DC, Helton WS, Mulholland MW,Strandness DE. Duplex ultrasound measurement of post-prandial intestinal blood flow: effect of meal composition.Gastroenterology 1988; 95: 1294-301.
11 Muller AF, Stainer K, Fullwood L, Hawkins M, Cowley AJ.The regional haemodynamic effects of food in normalvolunteers [Abstract]. J Physiol (Lond) 1990; 427: 35P.
12 Qamar MI, Read AE. Effects of exercise on mesenteric bloodflow in man. Gut 1987; 28: 583-7.
13 Dubbins PA. Renal artery stenosis: duplex Dopplerevaluation.BrJ Radial 1986; 59: 225-9.
14 Jager KA, Fortner GS, Thiele BL, Strandness DC. Non-invasive diagnosis of intestinal angina. 7 Clin Ultrasound1984; 12: 588-91.
15 Jager K, Bollinger A, Valli C, Ammann R. Measurement ofmesenteric blood flow by duplex scanning. J Vasc Surg 1986;3: 462-9.
16 Nicholls SC, Kohler TR, Martin RL, Strandness DE. Use ofhemodynamic parameters in the diagnosis of mesentericinsufficiency. J Vasc Surg 1986; 3: 507-10.
17 Qamar MI, Read AE, Skidmore R, Evans JM, Wells PNT.Transcutaneous Doppler ultrasound measurement ofsuperior mesenteric artery blood flow in man. Gut 1986; 27:100-5.
18 Mitchell DG. Color Doppler imaging: principles, limitationsand artefacts. Radiology 1990; 177: 1-10.
19 Qamar MI, Read AE, Skidmore R, Evans JM, Wells PNT.Pulsatility index of superior mesenteric artery blood velocitVwaveforms. Ultrasound Med Biol 1986; 12: 773-6.
20 Landwehr P, Schindler R, Heinrich U, Dolken W, Krahe T,Lackner K. Quantification of vascular stenosis with colorDoppler flow imaging: in vitro investigations. Radiology1991; 178:701-4.
21 Buchardt Hansen HJ, Engell HC, Ring-Larsen H, Ranek L.Splanchnic blood flow in patients with abdominal anginabefore and after arterial reconstruction: a proposal for adiagnostic test. Ann Surg 1977; 186: 216-20.
22 Poole JW, Sammartano RJ, Boley SJ. Hemodynamic basis ofthe pain of chronic mesenteric ischemia. Am]7 Su,g' 1987;153:171-6.
23 Roberts L, Wertman DA, Mills SR, Moore AV, Heaston DK.Transluminal angioplastv of the superior mesenteric artery:an alternative to surgical revascularisation. Amnj7 Roenrtnclol1983; 141: 1039-42.