Embed Size (px)
Citation preview

Instruments and Techniques
Robotic Retroperitoneal Paraaortic Lymphadenectomy at DonostiaUniversity Hospital
Mikel Gorostidi, MD*, Joana Larreategui, Teresa Bernal, MD, Constance Goiri, MD,Miren Arrue, PhD, Pepe Navarrina, PhD, and Arantxa Lekuona, MDDepartment of Obstetrics and Gynecology, Hospital Donostia, Sebastian, Spain (all authors).
ABSTRACT The purpose of this study was to describe our robotic retroperitoneal para-aortic lymphadenectomy technique and its associ-
The author decla
Corresponding au
Gynecology, Hos
20002, Spain.
E-mail: mgorosti
Submitted Augus
Available at www
1553-4650/$ - see
http://dx.doi.org/1
ated outcomes as well as the advantages and disadvantages. We prospectively collected data on all retroperitoneal aortocavallymphadenectomy procedures performed at Donostia University Hospital from December 2011 to April 2013 using the daVinci S robotic system (Intuitive Surgical, Sunnyvale,CA). A total of 13 of these procedures were performed. The mean pa-tient agewas 60.3 years (SD, 10.18). Most patients were obesewith a mean body mass index of 31.95 kg/m2 (SD, 5), and 9 hadendometrial cancer. Five individuals were restaged: 4 because of lymphovascular space invasion and 1 because of lympho-vascular space invasion with G3 histology. There were 2 cases of F�ed�eration Internationale de Gyn�ecologie et d’Obst�etriquestage IB endometrial cancer: 1 of papillary serous histology and 1 of G3. Two patients had advanced cervical cancer, and 2 hadearly-stage ovarian cancer. The median para-aortic lymph node yield was 12 (range, 4–21). In 3 patients, it was necessary toconvert the procedure to transperitoneal access because of technical difficulties; 1 of these required laparotomy. Themean surgical time was 323 minutes (SD, 58) although this included additional complex procedures. Robotic para-aorticretroperitoneal lymphadenectomy is feasible and offers the advantages of retroperitoneal access. Journal of Minimally Inva-sive Gynecology (2014) 21, 480–485 � 2014 AAGL. All rights reserved.
Keywords: Cervical Cancer; Endometrial Adenocarcinoma; Lymphadenectomy; Retroperitoneal Access; Robotic Surgery
DISCUSS
You can discuss this article with its authors and with other AAGL members athttp://www.AAGL.org/jmig-21-3-JMIG-D-13-00468res no conflict of interest.
thor: Mikel Gorostidi, MD, Department of Obstetrics and
pital Donostia, c/Usandizaga 18-6� Izda, San, Sebastian
t 21, 2013. Accepted for publication October 11, 2013.
.sciencedirect.com and www.jmig.org
front matter � 2014 AAGL. All rights reserved.
0.1016/j.jmig.2013.10.004
Utoadth
se your Smartphonescan this QR code
nd connect to theiscussion forum foris article now*
* Download a free QR Code scanner by searching for ‘‘QRscanner’’ in your smartphone’s app store or app marketplace.
Para-aortic lymphadenectomy is required for surgicalstaging of endometrial and ovarian cancer, aiding in the se-lection of patients whowill benefit from adjuvant treatments.In the case of advanced cervical cancer, the presence oflymph node metastasis in the upper abdomen is an indicationfor the expansion of the radiotherapy field. AlthoughF�ed�eration Internationale de Gyn�ecologie et d’Obst�etriqueclinical staging does not take lymph node status into ac-count, it is an essential part of most treatment protocols.Modern imaging techniques have their limitations; the
false-negative rate of positron emission tomographycomputed tomography has been reported to be as high as22% [1]. Therefore, surgical staging including para-aorticlymphadenectomy is recommended by many prestigious gy-necologic oncology centers.
Retroperitoneal access to para-aortic lymph nodes wasinitially described in the 1970s [2] as an alternative toopen transperitoneal lymphadenectomy. However, it wasabandoned until the end of the 1990s when Dargent et al[3] described their extraperitoneal laparoscopic technique.The objective of this study was to describe our retroperito-neal para-aortic lymphadenectomy technique and its associ-ated outcomes as well as the advantages and disadvantages.
Materials and Methods
We prospectively collected data on patients with en-dometrial, ovarian, and cervical cancer undergoing robotic

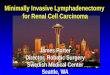
Fig. 1
Robotic trocars disposition. Blue: 12mms trocar por transperitoneal and
retroperitoneal optics. Red: 8 mmss trocar for robotic arms. Green: 10
mms trocar for assistant.
Fig. 2
Robotic trocars disposition.
Gorostidi et al. Robotic Retroperitoneal Para-aortic Lymphadenectomy 481
retroperitoneal para-aortic lymphadenectomies at DonostiaUniversity Hospital, Sebastian, Spain. A single surgeonexperienced in laparoscopic oncologic procedures per-formed a total of 13 retroperitoneal para-aortic lymphade-nectomies between November 2011 and April 2013 usingthe da Vinci S System (Intuitive Surgical, Sunnyvale, CA).
The surgical time was measured from the beginning ofdocking to skin closure, and we did not record the individualtimes for each different procedure. Details of any surgicalcomplications and incidents during surgery were recordedas were the following other data: patient age, height, numberof lymph nodes removed, blood loss, type of cancer andpathological characteristics, F�ed�eration Internationale deGyn�ecologie et d’Obst�etrique stage, and robot position. Af-ter discharge, all patients continued treatment in our hospi-tal’s gynecologic oncology unit with the first follow-upvisit 3 weeks postoperatively. All patients regularly attendedtheir follow-up visits.
Our surgical technique is as follows. The patient is placedwith the left arm extended at an angle as in classic laparos-copy. If a pelvic transperitoneal procedure is planned, theleft arm is tucked at the patient’s side.
The procedure begins with a transperitoneal inspection ofthe abdominal cavity through a 10-mm umbilical trocar torule out peritoneal dissemination. The trocars are placed ina manner similar to that described by Dargent et al [3]. A2-cm incision is made 2 cm medial to the anterior superioriliac spine at the left McBurney point. This will be the opticport. Blunt dissection of the subcutaneous tissue is per-formed as far as the major oblique muscle fascia, which isopened with sharp dissection. The minor oblique and trans-verse muscle fibers are separated without damaging the peri-toneum. The surgeon inserts his/her left index finger toexpand the retroperitoneal space, reaching the psoas majormuscle and the external iliac artery. We determine the trocarplacement points with the objective of spacing the roboticarms as far apart as possible to avoid collisions. The assis-tant’s 10-mm trocar is inserted in the midaxillary line atthe level of the umbilicus or slightly lower guided by the sur-geon’s retroperitoneal finger.
An 8-mm robotic trocar (R2) is placed about 8 cmcaudally to the initial incision medially toward the pubicbone, also under finger guidance. At this point, we beginpassing an insufflation gas via the assistant’s trocar, throughwhich we also insert the camera. The retroperitoneal space isinspected visually, the finger is removed from the initialMcBurney incision, and a balloon trocar is placed. Hence-forth, this will be referred to as the optic trocar. We placethe 8-mm R1 robotic trocar under visual guidance after dis-secting the area with a conventional laparoscopic grasper,approximately 2 fingerbreadths under the last rib, on theanterior axillary line (Figs. 1 and 2). We place the da VinciS system on the right side of the patient.
All procedures are performed using bipolar forceps in R2(left hand) and monopolar scissors in R1. A 0� camera isused for the aortic and left aortic nodes. In the event of dif-
ficulties, a 30� camera can be used for interaortocaval andprecaval dissection.
In all cases, a retroperitoneal infrarenal para-aortic lym-phadenectomy was performed, conserving the inferiormesenteric artery. If transperitoneal access to the pelviswas required after complete para-aortic lymphadenectomyfor more pelvic surgical procedures (hysterectomy, pelviclymphadenectomy, and so on), we repositioned the da Vincisystem for classic pelvic docking. We added a single 8-mm

Fig. 4
Robotic trocar telescoped in 12 mms balloon trocar for transperitoneal
surgery.
482 Journal of Minimally Invasive Gynecology, Vol 21, No 3, May/June 2014
robotic trocar above the right iliac fossa and telescoped theballoon trocar transperitoneally with a robotic trocar, thusworking with just 2 robotic arms (Figs. 3 and 4). The R1trocar and the assistant’s trocar can also be placed transper-itoneally, affording a 10-mm exit port for tissue extraction.
Results
The mean patient age was 60.3 years (SD, 10.18). Mostof the patients in the sample were obese (mean body massindex 5 31.95 kg/m2 [SD, 5]), and 1 was morbidly obese.
A median of 12 para-aortic lymph nodes (range, 4–21)were removed. Therewere no positive lymph nodes. Conver-sion to transperitoneal access was required in 3 cases becauseof peritoneal perforation upon entry. One of these was subse-quently reconverted to laparotomy because of poor visibility.This patient had a body mass index of 32 kg/m2.
The surgical time was 323 minutes (SD, 58 minutes)although in all cases but 1 additional procedures were per-formed including pelvic lymphadenectomy, ovarian transpo-sition, hysterectomy 1 double adnexectomy, omentectomy,appendectomy, and/or biopsies. All these procedures arelisted in Table 1. Individual times for the procedures werenot recorded. In the 1 case in which the procedure consistedexclusively of para-aortic lymphadenectomy, the surgerylasted 180 minutes compared with the 120 to 150 minutesit takes us to perform a conventional laparoscopic aorticlymphadenectomy procedure.
In 10 of the operations, it was necessary to reposition therobot once for pelvic access. In 2 cases, 3 different docking
Fig. 3
Robotic trocars disposition used for transperitoneal approach after
retroperitoneal lymphadenectomy.
procedures were required: lateral for the retroperitoneum,cephalic for the transperitoneal para-aortic lymphadenec-tomy because of peritoneal perforation, and between thelegs for the pelvic procedure. In 2 cases, we began pelviclymphadenectomy retroperitoneally and completed it trans-peritoneally.
We had 1 major intraoperative complication; the inferiormesenteric artery was torn during precaval lymphadenec-tomy because of excessive traction on the peritoneal tentwith the robotic arm. The hemorrhage was managed usingpressure and a FLOSEAL Hemostatic Matrix (Baxter Inter-national Inc., Deerfield, IL) and was contained within 20 mi-nutes. The patient received 2 units of red blood cellsintraoperatively. The blood loss in all other cases was unre-markable; no other patients required transfusion.
The mean hospital stay was 3.4 days. The longest time todischarge was 11 days for a patient who required laparotomyafter developing an ileus. Another patient had a surgicalwound infection, but this did not require hospitalization.The only major postoperative complication in our samplewas a urinoma that developed in 1 patient.
Discussion
Retroperitoneal para-aortic lymphadenectomy offersnumerous advantages including a comfortable operatingfield unencumbered by the bowel loops, which are behindthe peritoneum. It is particularly indicated in cases of morbidobesity, prior surgery, surgical restaging, and retroperitonealrecurrence. It also benefits women with a small mesentericroot or who cannot tolerate the Trendelenburg positionbecause these patients present particular difficulties fortransperitoneal access [4]. An 8% rate of conversion to lap-arotomy has been described for transperitoneal access [5],and this could be reduced with retroperitoneal access.
Research on animal models has shown reduced adhesionformation with retroperitoneal access. It is also worth noting

Table 1
Robotic aortic retroperitoneal lymphadenectomy at Donostia Hospital
Cancer Age BMI
Conversion to
robotic TRANS
Aortic
access
Total
nodes
Pelvic
nodes
Aortic
nodes
Surgical
time LVSI FIGO Complications
Aortic retro 1 pelvic retro 1st, then trans Endometrial adenocarcinoma 47 33 No Retro 21 11 10 330 1 IA
Aortic retro 1 pelvic trans Endometrial adenocarcinoma 59 34 Yes Trans 31 25 6 410 1 IA
Aortic retro 1 pelvic trans Endometrial adenocarcinoma G3 66 36.7 No Retro 29 15 14 360 1 IA Urinoma
Aortic retro 1 pelvic trans 1 TLH-BSO Endometrial adenocarcinoma 78 34 No Retro 10 6 4 360 1 IB
Aortic retro 1 pelvic trans Endometrial adenocarcinoma 59 33.2 No Retro 21 14 7 300 1 IA
Aortic retro 1 pelvic trans 1 TLH-BSO 1
omentectomy
Endometrial serous carcinoma 69 32.05 Yes Trans 30 21 9 360 2 IA Open conversion
Aortic retro 1 pelvic trans Endometrial adenocarcinoma 55 41.5 No Retro 22 8 14 300 1 IA Lymphocele (pigtail)
Aortic trans (1st retro) 1 left ovarian transposition Cervical carcinoma 42 20.07 Yes Trans 10 d 10 280 1 IIIB
Aortic retro 1 pelvic trans 1 omentectomy 1 Bxs Ovarian carcinoma (granulosa) 60 29.19 No Retro 19 7 12 270 2 IA
Aortic retro 1 pelvic trans 1 TLH-BSO Endometrial adenocarcinoma G3 53 24.5 No Retro 24 8 16 300 2 IA IMA injury
Aortic retro Cervical carcinoma 67 32.81 No Retro 19 d 18 180 2 IIB NO
Aortic retro 1 pelvic trans 1 TLH-BSO Endometrial adenocarcinoma* 76 32.34 No Retro 41 20 21 360 2 IA NO
Aortic retro 1 pelvic retro 1st, then trans Low grade Ovarian carcinoma 54 32.03 No Retro 21 6 15 390 2 IA NO
Total 60.3 31.95 24.4* 12.8 12 323
FIGO5 F�ed�eration Internationale de Gyn�ecologie et d’Obst�etrique; BMI5 body mass index; retro5 retroperitoneal; trans5 transperitoneal; TLH5 total laparoscopic hysterectomy; BSO5 bilateral salpingo-oophorectomy; Bxs5biopsies; IMA 5 inferior mesenteric artery.
* We included only paraaortic 1 pelvic nodes.
Gorostid
iet
al.
Robotic
Retro
perito
nealPara-aortic
Lym
phadenectom
y483

Fig. 5
Different trocars dispositions explored in the development of the tech-
nique.
484 Journal of Minimally Invasive Gynecology, Vol 21, No 3, May/June 2014
that any adhesions forming will not affect the bowel loops,unlike those caused by transperitoneal access. To our knowl-edge, there are no studies comparing the morbidity associ-ated with these 2 access sites. A higher lymphocele ratehas been reported with retroperitoneal access [6]. However,it is accepted that there is a lower risk of intraoperative intes-tinal complications with this approach. Furthermore, hypo-thetically, retroperitoneal access could reduce intestinalcomplications in subsequent radiotherapy although this hasnot been shown.
A9% (67%) rate of postradiotherapy intestinal complica-tions has been reportedwith a 5-year follow-up [7]. Similarly,the GOG99 trial (Gynecologic Oncology Group-AdjuvantRadiation for Intermediate Risk Endometrial Cancers) [8]described an 8% rate of postradiotherapy intestinal compli-cations (grade 3 1 4), and at the 2-year follow-up, 8% ofthe patients had severe bowel complications. These figurescontrast with the much lower complication rate (3% intesti-nal complications) of the PORTEC study (Post OperativeRadiation Therapy in Endometrial Carcinoma) [9] in whichlymphadenectomy was not part of the treatment protocol.
Retroperitoneal access improves visualization of the su-perior hypogastric plexus, which affects bladder and bowelfunction as well as orgasm. A new theoretic concept couldbe introduceddthe nerve-sparing para-aortic lymphadenec-tomy, which would allow for preservation of the superior hy-pogastric plexus.
There are publications that report similar lymph nodeyields for the 2 techniques [10]. The ongoing STELLAtrial (Transperitoneal vs. Extraperitoneal Approach forLaparoscopic Staging of Endometrial/Ovarian Cancer,NCT01810874) aims to compare transperitoneal and retro-peritoneal access in endometrial and ovarian cancer; its pri-mary outcome measure is the number of lymph nodesobtained. Its results may help to establish whether retroper-itoneal access improves lymph node yield.
The first robotic para-aortic lymphadenectomy was per-formed on 2 fresh cadavers [4]. Subsequently, Vergoteet al [11] published a series of 5 lymphadenectomies extend-ing to the inferior mesenteric artery, and Narducci et al [12]reported 6 lymphadenectomies extending to the left renalvein. In our series, we performed infra- and supramesentericdissection up to the renal vein following our hospital proto-col.
Dargent et al [3] first described access to the extraperito-neal space using a balloon trocar and finger dissection. Thisis the technique we use. Antonio Gil-Moreno from Barce-lona proposes direct entry without piercing the peritoneum(visualized transperitoneally) as a faster and simpler alterna-tive (unpublished data).
We have not encountered any problems of collision withthe left arm of the patient of the sort described by Vergoteet al [11]. We have experimented with several differenttrocar placements for retroperitoneal para-aortic lymphade-nectomy. The smaller operating field can cause robotic armcollisions. Vergote et al propose placing the balloon trocar
with the camera slightly more medially and higher and asuprapubic assistant trocar. Gil-Moreno proposes tele-scoping R2 and placing an assistant trocar between R2 andthe optic trocar. We have also attempted placing an assistanttrocar under R2 but have found it to be awkward (Fig. 5). Weplace the R1 subcostal trocar 2 fingerbreadths under the lastrib on the anterior axillary line. The higher and more medi-ally the trocar is placed, the better the ergonomics, especiallyin the infrarenal region. However, this position can also in-crease the risk of peritoneal perforation if we do notcorrectly visualize the reflection of the peritoneal sac. Incases in which the peritoneal reflection is not adequatelyvisualized, it may be useful to ascertain correct lateral entryusing a straight needle to avoid tearing the peritoneum,which can greatly encumber surgery. In robotic surgery, con-trary to classic laparoscopy, we can work comfortably evenif this trocar is placed low and laterally.
As for the camera, we place it 2 cm above the left iliacfossa in the balloon trocar. This affords broad visualizationof the entire field, slightly higher than the position used byGil-Moreno, which requires a 30� optic. The only inconve-nience of the position we use is the possibility of a collisionwith R2 during cranial dissection of the aorta. In the event ofany difficulties, this can be quickly repositioned byexchanging camera and assistant positions.
Robotic access requires an additional 10-mm trocar forthe assistant. We use this access during surgery to introducegauze, which we use systematically in all lymphadenecto-mies as a tamponade in the event of hemorrhage as well asfor lymph node collection. The assistant helps to improveexposure of the operating field and provide traction, whichaids in dissection.

Gorostidi et al. Robotic Retroperitoneal Para-aortic Lymphadenectomy 485
Access to interaortocaval nodes can be accomplished bylifting the aorta although this is not a commonly performedprocedure. It can also be achieved robotically without theneed to lift the aorta using a 30� camera and the maneuver-ability of the robotic instruments.
Precaval lymphadenectomy is 1 of the challenges ofretroperitoneal access. The method of bilateral extraperito-neal access described by Dargent et al [3] is time-consuming and risks peritoneal perforation. On the otherhand, the robot’s maneuverability is advantageous in pre-caval dissection.
Benefits related to blood loss, which have been shown forother robotic procedures, are yet to be demonstrated for ro-botic retroperitoneal aortocaval lymphadenectomy. The lackof haptic sensitivity can cause serious complications and is amajor disadvantage of robotic surgery. Our only intraopera-tive surgical complication in which excessive tractioncaused tearing of the inferior mesenteric artery serves asan example (Video 1).
In the near future, robotic systems will become lighterand more agile using smaller ports or single-port entrywith advanced dissection, cut, and sealingmethods. Incorpo-rating tactile feedback would also favor the use of roboticsurgery. Overall, we believe that we should incorporate ro-botic surgery to our range of procedures to favor its develop-ment although we recognize that currently roboticretroperitoneal lymphadenectomy does not offer great ad-vantages over classic laparoscopy.
Conclusions
Robotic retroperitoneal para-aortic lymphadenectomy isfeasible and safe in the hands of experienced surgeons.
Supplementary Data
Supplementary data related to this article can be found athttp://dx.doi.org/10.1016/j.jmig.2013.10.004.
References
1. Gouy S, Morice P, Narducci F, et al. Nodal-staging surgery for locally
advanced cervical cancer in the era of PET. Lancet Oncol. 2012;13:
e212–e220.
2. Berman ML, Lagasse LD, Watring WG, et al. The operative evaluation
of patients with cervical carcinoma by an extraperitoneal approach.
Obstet Gynecol. 1977;50:658–664.
3. Dargent D, Ansquer Y, Mathevet P. Technical development and results
of left extraperitoneal laparoscopic paraaortic lymphadenectomy for
cervical cancer. Gynecol Oncol. 2000;77:87–92.
4. Magrina JF, Kho R,Montero RP,Magtibay PM, PawlinaW. Robotic ex-
traperitoneal aortic lymphadenectomy: development of a technique.
Gynecol Oncol. 2009;113:32–35.
5. Abu-RustumNR, Chi DS, Sonoda Y, et al. Transperitoneal laparoscopic
pelvic and para-aortic lymph node dissection using the argon-beam co-
agulator and monopolar instruments: an 8-year study and description of
technique. Gynecol Oncol. 2003;89:504–513.
6. Occelli B, Narducci F, Lanvin D, et al. De novo adhesions with extrap-
eritoneal endosurgical para-aortic lymphadenectomy versus transperi-
toneal laparoscopic para-aortic lymphadenectomy: a randomized
experimental study. Am J Obstet Gynecol. 2000;183:529–533.
7. Stanic S, Mayadev JS. Tolerance of the small bowel to therapeutic irra-
diation: a focus on late toxicity in patients receiving para-aortic nodal
irradiation for gynecologic malignancies. Int J Gynecol Cancer.
2013;23:592–597.
8. Keys HM, Roberts JA, Brunetto VL, et al. A phase III trial of surgery
with or without adjunctive external pelvic radiation therapy in
intermediate-risk endometrial adenocarcinoma: a gynecologic
oncology group study. Obstet Gynecol Surv. 2004;59:516–518.
9. CreutzbergCL,vanPuttenWL,KoperPC, et al. Surgeryandpostoperative
radiotherapy versus surgery alone for patients with stage-1 endometrial
carcinoma: Multicentre randomised trial. Lancet. 2000;355:1404–1411.
10. Sonoda Y, Leblanc E, Querleu D, et al. Prospective evaluation of surgi-
cal staging of advanced cervical cancer via a laparoscopic extraperito-
neal approach. Gynecol Oncol. 2003;91:326–331.
11. Vergote I, Pouseele B, Van Gorp T, et al. Robotic retroperitoneal lower
para-aortic lymphadenectomy in cervical carcinoma: first report on the
technique used in 5 patients. Acta Obstet Gynecol Scand. 2008;87:
783–787.
12. Narducci F, Lambaudie E, Houvenaeghel G, Collinet P, Leblanc E.
Early experience of robotic-assisted laparoscopy for extraperitoneal
para-aortic lymphadenectomy up to the left renal vein. Gynecol Oncol.
2009;115:172–174.