Embed Size (px)
Citation preview

Endo-urology
Robotic Laparoendoscopic Single-Site Surgery Using GelPort as the
Access Platform
Robert J. Stein, Wesley M. White, Raj K. Goel, Brian H. Irwin, George Pascal Haber,Jihad H. Kaouk *
Glickman Urologic and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 1 3 2 – 1 3 7
avai lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Article info
Article history:
Accepted March 23, 2009Published online ahead ofprint on March 31, 2009
Keywords:
Da Vinci
Laparoscopic
Laparoscopy
LESS
Nephrectomy
NOTES
Partial nephrectomy
Pyeloplasty
Reconstructive
Robot
Robotic
Single access
Single port
Abstract
Background: Laparoendoscopic single-site surgery (LESS) allows for the perfor-
mance of major urologic procedures with a single small incision and minimal
scarring. The da Vinci Surgical System provides advantages of easy articulation and
improved ergonomics; however, an ideal platform for these procedures has not
been identified.
Objective: To evaluate the GelPort laparoscopic system as an access platform for
robotic LESS (R-LESS) procedures.
Design, setting, and participants: Since April 2008, 11 R-LESS procedures have
been completed successfully in a single institutional referral center. For the last
four consecutive cases, the GelPort has been used as an access platform through a
2.5–5-cm umbilical incision.
Intervention: R-LESS cases performed with the GelPort included pyeloplasty
(n = 2), radical nephrectomy (n = 1), and partial nephrectomy (n = 1).
Measurements: Perioperative data were obtained for all patients including demo-
graphic data, operative indications, operative records, length of stay, complica-
tions, and pathologic analysis.
Results and limitations: Forbothpyeloplastycases,averageoperativetime(OR time)
was 235 min and estimated blood loss (EBL) was 38 cm3. For the patient undergoing
radical nephrectomy for a 5.1-cm renal tumor, OR time was 200 min and EBL was
250 cm3. The final patient underwent partial nephrectomy without renal hilar
clamping for an 11-cm angiomyolipoma with OR time of 180 min and EBL of
600 cm3. All R-LESS procedures attempted with the GelPort were completed success-
fullyandwithoutcomplication.Averagelengthofhospitalstaywas1.75d(range:1–2).
The partial nephrectomy patient required transfusion of 1 U of packed red blood cells.
Conclusions: Use of the GelPort as an access platform for R-LESS procedures
provides adequate spacing and flexibility of port placement and acceptable access
to the surgical field for the assistant, especially during procedures that require a
specimen extraction incision. Additional platform and instrumentation develop-
ment will likely simplify R-LESS procedures further as experience grows.
# 2009 Published by Elsevier B.V. on behalf of European Association of Urology.
* Corresponding author. Glickman Urological and Kidney Institute, Cleveland Clinic, 9500 EuclidAvenue/Q-10, Cleveland, Ohio 44195, United States. Tel: +1 216 444 2976; Fax: +1 216 445 7031.
E-mail address: [email protected] (J.H. Kaouk).0302-2838/$ – see back matter # 2009 Published by Elsevier B.V. on behalf of European Association of Urology. doi:10.1016/j.eururo.2009.03.054

1. Introduction
Laparoendoscopic single-site surgery (LESS) provides the
ability to perform major surgery with minimal incisions and
nearly scar-free results. Use of a single incision within the
umbilicus conceals much, if not all, of the wound while
allowing access to the abdomen during transabdominal
procedures.
Several difficulties are immediately apparent with this
approach. The two greatest challenges include clashing of
the laparoscope with instruments and the loss of triangula-
tion with limitation of instrument maneuverability. To
overcome these obstacles, articulating instruments for
greater spacing have been developed. Nevertheless, current
articulating, laparoscopic equipment can be bulky and
difficult to master, thus reducing ergonomics and efficiency
for the surgeon.
The primary advantage of the da Vinci Surgical System
(Intuitive Surgical, Sunnyvale, CA, USA) for LESS includes
easier articulation using EndoWrist instruments. Other
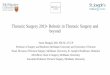
Fig. 1 – Port placement prior to attaching the GelSeal cap to the woundprotector.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 1 3 2 – 1 3 7 133
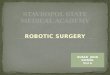
Fig. 2 – Intraoperative image of the da Vinci S Surgical System docked intothe GelPort platform.
benefits include three-dimensional visualization, motion
scaling, and tremor filtration. We reported our initial
experience with robotic LESS (R-LESS) using a multichannel
single port (Triport, Advanced Surgical Concepts, Dublin,
Ireland), next to which one additional robotic port was
placed through the same umbilical incision [1]. This
platform arrangement is usable, but limitations include
less flexibility for customized placement of ports and
interference with placement of ports in tandem through the
single incision, as the multichannel port has a rigid outer
ring. The GelPort system (Applied Medical, Rancho Santa
Margarita, CA, USA) provides a larger working platform that
can be useful in all cases but especially for patients
requiring a 3–5-cm specimen extraction incision.
To this point, our experience includes 11 R-LESS
procedures: radical prostatectomy (n = 1), partial nephrec-
tomy (n = 2), ureteroneocystostomy (n = 1), radical
nephrectomy (n = 2), and dismembered pyeloplasty
(n = 5). We report our robotic single-site technique using
the GelPort as a surgical platform.
2. Materials and methods
Since April 2008, we have performed 11 R-LESS cases for patients
otherwise considered to be candidates for LESS surgery. Exclusion criteria
included body mass index >35 kg/m2, significant prior abdominal
operations, and evidence of systemic malignancy. For the four most
recent R-LESS procedures, the GelPort was used as the surgical platform
due to the subjective ease of use noted during the first such procedure.
2.1. Access
Access for renal procedures involves placement of the patient in modified
flank position. A 2–5-cm transumbilical incision (depending on the size of
the specimen for extraction) is created either directly through the middle
of the umbilicus or using a semicircle incision concealed within the
umbilicus. Access to the peritoneum is then obtained, and the wound
retractor is introduced and positioned. At this point, the GelSeal cap is
marked with a pen for ideal trocar positioning. For upper tract procedures,
a 12-mm trocar for the camera is placed in the most medial position. Eight
millimeter robotic trocars are then placed more laterally and near the
edges of the cap (Fig. 1). An assistant 5- or 12-mm port is positioned
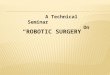
between the camera and robotic ports, as needed. The GelSeal cap is then
latched to the wound retractor, and the robot is docked (Figs. 2 and 3). For
upper-tract procedures, a 308 robotic scope is positioned viewing
downward. Great care is used to visualize the initial positioning of robotic
instruments. A helpful maneuver to place the robotic instruments is to
introduce an atraumatic grasper through the robotic port to align the port
under vision, followed by positioning of the robotic instrument.
For all cases, standard 8-mm robotic instruments were used. A
standard three-arm robotic system or a da Vinci S system was used,
depending on availability for the procedure. The da Vinci S is preferred
due to the improved range of motion provided by the newer system.
2.2. Surgical procedure
Standard techniques for renal and ureteral dissection were used,
depending on the specifics of the surgery being performed. Table 1
provides data for each case. Partial nephrectomy was carried out for an
11-cm right renal angiomyolipoma not amenable to angioembolization.

Fig. 3 – Intraoperative image of the da Vinci standard system docked intothe GelPort platform.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 1 3 2 – 1 3 7134
The renal mass was exposed, and the tumor was excised robotically with
a harmonic scalpel (Ethicon, Cincinnati, OH, USA) and Hem-o-lok clips
(Weck, Research Triangle Park, NC, USA), without hilar clamping.
Surgical assistance was possible through a port placed through the
GelPort. Hemostasis was achieved using the argon-beam coagulator and
Floseal (Baxter, Deerfield, IL, USA). The specimen was placed in a large
specimen bag for removal through the 5-cm umbilical skin incision.
Radical nephrectomy was performed for a 5-cm left lower pole renal
mass not amenable to nephron-sparing techniques. After R-LESS
dissection of the lower pole and renal hilum, the renal artery and vein
were controlled and transected separately with an endoscopic stapler.
Monopolar cautery with a robotic hook was used for upper-pole and
lateral dissection, and the kidney was placed in a large specimen bag for
removal through the 4-cm single incision.
Dismembered pyeloplasty was performed for ureteropelvic junction
(UPJ) obstruction in two patients. Neither patient had a lower-pole
crossing vessel. Ureteral spatulation and the running UPJ anastomoses
using 4-O Vicryl sutures were aided by robotic articulation.
3. Results
All data were retrospectively collected and entered into our
institutional review board–approved database. All four
R-LESS procedures attempted with the GelPort were
completed successfully without need for placement of
additional ports. Median operative time was 200 min, and
Table 1 – Perioperative data following robotic single-site surgery thro
Patient No. Age, yr Gender BMI (kg/m2) Procedure Side
1 55 M 31 Pyeloplastya Left
2 88 F 35 Partial nephrectomyb Righ
3 42 M 25 Radical nephrectomyc Left
4 24 F 25 Pyeloplastyd Righ
BMI = body mass index; F = female; M = male; NA = not available; OR = operativea Postoperative symptomatic and radiographic improvement.b Final pathology: angiomyolipoma.c Final pathology: Fuhrman grade III clear cell renal cell carcinoma, margin negad Awaiting follow-up imaging.
hospital stay was 1–2 days in all cases. The patient
undergoing partial nephrectomy had 600 cm3 of estimated
blood loss, as the lesion was excised using a harmonic
scalpel without hilar clamping, and was transfused 1 U of
packed red blood cells. Pathology revealed angiomyolipoma
with negative margins. Differential right renal function as
determined by radionuclide renal scanning remained stable
at 41% postoperatively compared with 41.2% preoperatively
Pathology after radical nephrectomy revealed a 4.9-cm
Fuhrman grade III clear cell renal cell cancer with negative
margins. The initial patient who underwent pyeloplasty had
resolution of flank pain postoperatively. Differential renal
function was maintained at 33%, and drainage as deter-
mined by diuretic radionuclide scanning was improved. The
final patient who also underwent pyeloplasty has not had
postoperative imaging, given the brevity of follow-up from
surgery. There were no operative or wound complications in
any case.
4. Discussion
The evolution of urologic surgery involves an increasingly
brisk progression toward scar-less technique. Natural
orifice translumenal endoscopic surgery (NOTES), in its
purest form, involves only visceral incisions to perform
surgical procedures. Severe challenges for NOTES currently
include deficient instrumentation and platforms, issues of
securely closing hollow viscera, and societal taboos
regarding access points. To date, largely hybrid techniques
involving visceral as well as transcutaneous access have
been used, especially for major procedures [2].
With the ability to perform laparoscopic surgery through
single-incision access, along with the ability to conceal such
an incision within the umbilicus, LESS has garnered
increasing interest in multiple specialties [3–5]. In urology,
LESS has been used to carry out several procedures that can
be performed laparoscopically, including nephrectomy,
partial nephrectomy, donor nephrectomy, adrenalectomy,
renal cryoablation, pyeloplasty, ileal interposition, ureter-
oneocystostomy, varicocelectomy, radical prostatectomy,
simple prostatectomy, and radical cystoprostatectomy [4–
13]. Early data from our donor nephrectomy and pyelo-
plasty experience suggest a modest advantage for LESS
when compared with standard laparoscopy in terms of
convalescence and postoperative pain (unpublished data).
ugh a GelPort
Tumor size, cm OR time, min EBL, cm3 LOS, d Transfusion, RBC
NA 270 50 2 0
t 11 180 600 2 1 U
5.1 200 250 2 0
t NA 200 25 1 0
; EBL = estimated blood loss; LOS = length of stay; RBC = red blood cells.
tive.

E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 1 3 2 – 1 3 7 135
The major challenges of LESS, including clashing of
instruments and lack of triangulation, can be addressed in
part by the use of articulating instruments. Nevertheless, at
present, laparoscopic articulating instruments can be
difficult to use, bulky, and generally nonergonomic. A
logical consideration is the use of the da Vinci Surgical
System to provide intuitive articulation with EndoWrist
technology and greater surgeon comfort. The authors’ initial
report using this approach used the R-port with one robotic
port in tandem through the single incision. R-LESS was
possible using this approach but was challenging at times,
with careful port placement being of the utmost impor-
tance. It must be mentioned that, thus far, the nomenclature
for these procedures has not been standardized; we have
used the term R-LESS as a close modification of the now
accepted term of LESS for single-incision surgeries.
For radical nephrectomy, we previously used several
robotic ports through a single incision without a specific
platform but found that assistant access is severely limited.
Ponsky and colleagues have described using the GelPort as a
platform for LESS radical nephrectomy [14]. Benefits of the
GelPort include a larger extracorporeal profile for greater
spacing of ports, flexibility of port placement anywhere on
the GelCap, easy replacement of ports if another config-
uration is desired, durability of the gel platform, and easy
specimen extraction without the need for removal of the
entire port. Disadvantages include the need to create a
slightly larger incision for positioning of the inner ring (at
least 2–2.5 cm) and bulging of the GelCap with insufflation.
Furthermore, a built-in central defect in the gel of the
GelCap should be sutured closed at the beginning of the
procedure, as this can lead to loss of pneumoperitoneum
during the surgery.
It is noted that the larger incision required to place the
GelPort can be efficiently used to extract specimens for
extirpative procedures; however, for purely reconstructive
procedures, the extended incision may provide the benefit
of improved range of motion for instruments for suturing
and tissue handling. Moreover, the extended incision can be
partially concealed within the umbilicus. The smaller
external profile of the da Vinci S system is preferred, as it
provides the greatest range of movement through the
smallest incision. Additionally, the da Vinci S system allows
the surgeon to use digital zoom and to maintain distance
from the operative area. Operative times in the present
series are longer than those usually required for corre-
sponding cases using conventional laparoscopic technique.
This is probably due to a requisite learning curve for
understanding robot and port positioning, which is likely to
improve with experience.
A comparison of R-LESS techniques to LESS and
conventional laparoscopic procedures is needed. As yet,
experience is still limited for R-LESS and consists of several
different procedures. With more experience, a comparison
of several of these minimally invasive techniques will be
more meaningful [15,16]. It is our purpose in this report to
convey a modification in technique that may facilitate the
early experience with R-LESS for other surgeons.
One patient in our series did require a transfusion of 1 U
of packed red blood cells. The patient was elderly and
underwent unclamped resection of a large angiomyoli-
poma. Use of an R-LESS technique for such a procedure
should be considered carefully and probably should be
performed by only a very experienced laparoscopic/robotic
surgeon.
Thus far, the GelPort has facilitated our R-LESS
procedures, largely due to greater spacing and flexibility
of port placement and easier access to the surgical field for
the assistant. Since using the GelPort for all R-LESS
procedures, we have not had to convert to a standard
robotic or laparoscopic approach or place any additional
ports. Use of the robot for LESS procedures has dramatically
improved surgeon ergonomics and made delicate recon-
structive suturing possible without additional port place-
ment.
Nevertheless, R-LESS still can be challenging, and the
surgeon must become accustomed to a variable amount of
restricted movement as well as clashing of robotic
instruments and the scope. In the future, robotic technology
with even less extracorporeal profile and greater flexibility
may simplify the R-LESS approach and make it a more
universal option for urologic procedures.
5. Conclusions
Use of the GelPort as a platform for single-site access has
provided advantages for performing R-LESS urologic
surgery, largely by allowing greater spacing of robotic
ports and easier assistant access. The GelPort requires a
slightly larger skin incision compared with available
multichannel single ports and may be especially attractive
for surgeries that involve eventual specimen extraction.
Currently, the existing robotic system and available ports
are not specifically designed for R-LESS procedures. Further
developments in robotic and access platform designs are
needed.
Author contributions: Jihad H. Kaouk had full access to all the data in the
study and takes responsibility for the integrity of the data and the accuracy
of the data analysis.
Study concept and design: Stein, Kaouk.
Acquisition of data: White, Goel, Irwin, Haber.
Analysis and interpretation of data: Stein, White, Kaouk.
Drafting of the manuscript: Stein, Kaouk.
Critical revision of the manuscript for important intellectual content: Kaouk,
Stein, Goel.
Statistical analysis: White.
Obtaining funding: None.
Administrative, technical, or material support: Kaouk, Haber, White.
Supervision: Kaouk.
Other (specify): None.
Financial disclosures: I certify that all conflicts of interest, including specific
financial interests and relationships and affiliations relevant to the subject
matter or materials discussed in the manuscript (eg, employment/affilia-
tion, grants or funding, consultancies, honoraria, stock ownership or

E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 1 3 2 – 1 3 7136
options, expert testimony, royalties, or patents filed, received, or pending),
are the following: Jihad Kaouk is affiliated with Intuitive Surgical.
Funding/Support and role of the sponsor: None.
References
[1] Kaouk JH, Goel RK, Haber GP, Crouzet S, Stein RJ. Robotic single-port
transumbilical surgery in humans: initial report. BJU Int
2009;103:366–9.
[2] Branco AW, Branco Filho AJ, Kondo W, et al. Hybrid transvaginal
nephrectomy. Eur Urol 2008;53:1290–4.
[3] Canes D, Desai MM, Aron M, et al. Transumbilical single-port
surgery: evolution and current status. Eur Urol 2008;54:1020–30.
[4] Raman JD, Bensalah K, Bagrodia A, Stern JM, Cadeddu JA. Laboratory
and clinical development of single keyhole umbilical nephrectomy.
Urology 2007;70:1039–42.
[5] Kaouk JH, Haber GP, Goel RK, et al. Single-port laparoscopic surgery
in urology: initial experience. Urology 2008;71:3–6.
[6] Desai MM, Rao PP, Aron M, et al. Scarless single port transumbilical
nephrectomy and pyeloplasty: first clinical report. BJU Int
2008;101:83–8.
[7] Kaouk JH, Palmer JS. Single-port laparoscopic surgery: initial
experience in children for varicocelectomy. BJU Int 2008;102:97–9.
Editorial Comment on: Robotic Laparoendoscopic
Single-Site Surgery Using GelPort as the Access Platform
Alexander Bachmann, Stephen Wyler
Department of Urology, University Hospital Basel,
Spitalstr. 21, 4031 Basel, Switzerland
More than 15 yr ago, duplicating standard open surgical
procedures with minimally invasive laparoscopic techni-
ques was considered to be very sophisticated, technically
demanding, or even sensational [1]. Over time, many
experienced centers have successfully established laparo-
scopy in their standard repertoires [2].
Focusing on radical prostatectomy, numerous papers
are being published in 2009 that deal with the comparison
of standard open retropubic radical prostatectomy
(RRP), conventional laparoscopic radical prostatectomy
(LRP), extraperitoneal endoscopic radical prostatectomy
(EERP), and robotic-assisted laparoscopic radical prosta-
tectomy (RALP) [3,4]. LRP has never shown an overall
advantage over RRP, except for less blood loss and
sometimes lower overall complication rates. Although
the surgical steps are comparable with LRP, RALP surges
ahead as the standard prostatectomy procedure in the
United States and in Europe. As medical equipment is
constantly being improved, the standard of care in
robotics in 2009 seems to be a four-arm HDTV system,
and older systems are replaced or are not recommended
any more.
The question arises of whether we can generally expect
better results with newer techniques. It seems that not
only clinical results can influence trends in minimally
[8] Goel RK, Kaouk JH. Single port access renal cryoablation (SPARC):
a new approach. Eur Urol 2008;53:1204–9.
[9] Rane A, Rao P, Rao P. Single-port-access nephrectomy and other
laparoscopic urologic procedures using a novel laparoscopic port
(R-port). Urology 2008;72:260–3, discussion 263–4.
[10] Gill IS, Canes D, Aron M, et al. Single port transumbilical (E-NOTES)
donor nephrectomy. J Urol 2008;180:637–41, discussion 641.
[11] Castellucci SA, Curcillo PG, Ginsberg PC, Saba SC, Jaffe JS,
Harmon JD. Single port access adrenalectomy. J Endourol 2008;
22:1573–6.
[12] Raman JD, Bagrodia A, Cadeddu JA. Single-incision, umbilical
laparoscopic versus conventional laparoscopic nephrectomy: a
comparison of perioperative outcomes and short-term measures
of convalescence. Eur Urol 2009;55:1198–206.
[13] Aron M, Canes D, Desai MM, Haber GP, Kaouk JH, Gill IS. Trans-
umbilical single-port laparoscopic partial nephrectomy. BJU Int
2009;103:516–21.
[14] Ponsky LE, Cherullo EE, Sawyer M, Hartke D. Single access site
laparoscopic radical nephrectomy: initial clinical experience.
J Endourol 2008;22:663–6.
[15] Rassweiler J. Editorial comment on: transumbilical single-port
surgery: evolution and current status. Eur Urol 2008;54:1030.
[16] Zigeuner R. Editorial comment on: transumbilical single-port sur-
gery: evolution and current status. Eur Urol 2008;54:1029.
invasive surgery: The financial interests of the industry
supporting novel techniques must be considered.
The paper published by Stein et al [5] demonstrates
that radical prostatectomy can be performed through one
single access. But the most important question is whether
patients are concerned about scars when having an
oncologic procedure performed. This advantage could
not be demonstrated for LRP in comparison with RRP
during the last 10 yr.
For cT1 renal tumors, the laparoscopic approach is
increasingly considered to be the standard technique [6].
The clinical rationale for laparoscopic renal surgery is the
smaller scar, minimally invasive access, less pain during
early and longer follow-up, and comparable oncologic
results to the open procedure. Therefore, further devel-
opments of minimal access techniques are obvious. The
manuscript of Stein et al [5] has to be seen in this context.
The next era of minimally invasive and virtually
invisible surgical procedures has already started with
natural orifice transluminal endoscopic surgery (NOTES)
and laparoendoscopic single-site surgery (LESS). Stein et al
[5] demonstrate the feasibility of robotic-assisted LESS
(R-LESS) procedures only, but the final importance and
benefit for the patient of LESS procedures has to be
clarified with consecutive comparative studies.
The undisputable advantage of LESS and NOTES is
surely the smaller or invisible scar and possibly less pain
compared with standard laparoscopy. As shown by
Stein et al [5], it will take many years to demonstrate
an advantage to performing radical prostatectomy, donor
nephrectomy, or tumor nephrectomy in large renal tumors
using LESS or NOTES. LESS, however, could become a

Editorial Comment on: Robotic Laparoendoscopic
Single-Site Surgery Using GelPort as the Access Platform
Andrea Cestari, Giorgio Guazzoni
Department of Urology, Vita-Salute University,
San Raffaele Turro Hospital, Milan, Italy
Single-port surgery is still in its infancy, although
interest in this evolution of minimally invasive surgery is
progressively growing in the urological community.
Embryonic natural orifice transluminal endoscopic sur-
gery (E-NOTES) and single-port access could represent the
evolution of laparoscopy toward a new form of minimally
invasive surgery if proper indications were defined.
We are feeling the same enthusiasm that we experi-
enced in the early 1990s after the pioneering experiences
in laparoscopic nephrectomy [1], when laparoscopy
seemed likely to replace conventional open surgery.
Laparoscopy evolved over the years, thanks to the
experience of the leading groups and the technological
innovations that offered high-definition vision and opti-
mal instrumentation and tools for hemostatic control.
Similarly, a wide range of surgical procedures have used
single-port surgery, including complex and challenging
procedures such as radical nephrectomy, pyeloplasty, and
even living donor nephrectomy [2].
Nevertheless, actual instrumentation for single-port
surgery, although directly derived from laparoscopic
instrumentation, is still not adequate to allow proper
diffusion of this technique. The major problems concern-
ing the closeness of the optics and the working instru-
ments must be solved. Industry is directly involved in the
evolution and diffusion of this technique, with the creation
of a proper optical system, possibly with a steerable tip,
and instruments with moveable tips and moldable shafts
inside the body. Finally, even being able to slightly modify
the trocars could have pivotal importance. The authors
should be congratulated for the idea of using a GelPort for
the site of entry for the optical and surgical instruments in
single-port surgery [3]. GelPort is a valid device for the
entry site in the abdomen and offers the possibility of
modifying the relationship between the ports during the
procedure as well as a nice degree of angulation between
the instruments compared with the commercially avail-
able device.
References
[1] Clayman RV, Kavoussi LR, Soper NJ, et al. Laparoscopic nephrec-
tomy: initial case report. J Urol 1991;146:278–82.
[2] Canes D, Desai MM, Aron M, et al. Transumbilical single-port
surgery: evolution and current status. Eur Urol 2008;54:1020–30.
[3] Stein RJ, White WM, Goel RK, Irwin BH, Haber PG, Kaouk JH.
Robotic laparoendoscopic single-site surgery using GelPort as the
access platform. Eur Urol 2010;57:132–7.
DOI: 10.1016/j.eururo.2009.03.056
DOI of original article: 10.1016/j.eururo.2009.03.054
standard procedure in reconstructive urologic surgery
(eg, pyeloplasty, ureterocystoneostomy) within the next
few years.
References
[1] Schuessler WW, Schulam PG, Clayman RV, Kavoussi LR. Laparo-
scopic radical prostatectomy: initial short-term experience. Urol-
ogy 1997;50:854–7.
[2] Imkamp F, Herrmann TR, Rassweiler J, et al. Laparoscopy in
German urology: changing acceptance among urologists. Eur Urol
2009;56:1074–81.
[3] Berryhill Jr R, Jhaveri J, Yadav R, et al. Robotic prostatectomy:
a review of outcomes compared with laparoscopic and open
approaches. Urology 2008;72:15–23.
[4] Ficarra V, Novara G, Artibani W, et al. Retropubic, laparoscopic, and
robot-assisted radical prostatectomy: a systematic review and
cumulative analysis of comparative studies. Eur Urol 2009;55:
1037–63.
[5] Stein RJ, White WM, Goel RK, Irwin BH, Haber GP, Kaouk JH.
Robotic laparoendoscopic single-site surgery using GelPort as the
access platform. Eur Urol 2010;57:132–7.
[6] Ljungberg B, Hanbury DC, Kuczyk MA, et al. Renal cell carcinoma
guideline. Eur Urol 2007;51:1502–10.
DOI: 10.1016/j.eururo.2009.03.055
DOI of original article: 10.1016/j.eururo.2009.03.054
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 1 3 2 – 1 3 7 137