Embed Size (px)
Citation preview

Br. J. Surg. 1991, Vol. 78, May. 554557
J. Hill, D. F. Martin* and D. E. F. Tweedle
Departments of Surgery and Radiology*, Gastroenterology Unit, University Hospital of South Manchester, Nell Lane, West Didsbury, Manchester M208LR. UK Correspondence to: Mr D. E. F. Tweedle
Risks of leaving the gallbladder in situ after endoscopic sphincterotomy for bile duct stones
There is controversy concerning the subsequent clinical course ofpatients whose gallbladder is left in situ following successful endoscopic removal of stones from their common bile ducts. A total of 191 patients (median age 76 years) were reviewed between 12 and 100 months (mean 38 months) after endoscopic sphincterotomy. Ten patients (5.2 per cent) had symptoms requiring cholecystectomy which was uneventful, nine in the first year. Cholangitis at presentation or failure to fill the gallbladder by endoscopic retrograde cholangiography were not helpful in identifying these patients. Forty-nine (25.6 per cent) patients died during the review period from non-biliary pathology (usually cardiovascular). Elective cholecystectorny is not required in elderly patients with symptomatic bile duct stones if the common bile duct can be cleared of stones after endoscopic sphincterotomy.
Endoscopic sphincterotomy is a safe and effective method for the management of symptomatic common duct stones in patients with an intact gallbladdeP5, but there are three areas of controversy. What percentage of patients will subsequently require cholecystectomy because of the development of acute cholecystitis and its complications; is there a greater postoperative mortality in these patients .than in those undergoing elective cholecystectomy ; and are there risk factors which can be used to identify patients likely to develop symptoms or complications related to the retained gallbladder?
Patients and methods Between July 1981 and December 1988, a total of 218 patients (89 men and 129 women) with intact gallbladders were seen with symptoms related to the presence of common duct stones. Of these, 81 were the subject of a previous report5; 151 (69.3 per cent) were specifically referred for endoscopic management from other hospitals in the north-west of England and Wales. Their ages ranged from 28 to 94 years (median 76 years), 16 patients (7.3 per cent) being under 60 years and 86 (39.5 per cent) over 80 years.
The main presenting symptoms were jaundice in 131 (60 per cent) patients, cholangitis in 38 (17.4 per cent), pain in 34 (15.6 per cent), and pancreatitis in 15 (6.9 per cent); many patients presented with more than one symptom. No patient exhibited clinical features of gallbladder inflammation at the time of endoscopic sphincterotomy. Intravenous antibiotics, most recently mezlocillin 2 g, were given before endoscopic retrograde cholangiopancreatography (ERCP).
ERCP was performed using Olympus JFIT, JFlTlO and TJFlO duodenoscopes (Olympus Keymed, Southend, UK). Attempts were made not to overfill the biliary tree on cholangiography and no specific attempt was made to opacify the gallbladder. Endoscopic sphincter- otomy was performed using a Classen-Demling sphincterotome or a listulotomy knife when necessary with an Erbotom diathermy unit. Stones were cleared using baskets or balloon catheters where possible. In addition, a combination ofpernasal catheters and duct perfusion with 5 per cent dextrose, stents, extracorporeal shock wave lithotripsy and an Olympus BML-3Q mechanical lithotripter were used to clear the ducts. If duct clearance was not achieved at the first attempt the common duct was drained with either a pernasal catheter or a biliary stent.
Current health status was ascertained directly from the patients and from the general practitioner by questionnaire. Cause of death was established either from hospital records, from the general practitioner or the Registrar of Births, Marriages and Deaths.
Results Endoscopic and radiological features Dilated bile ducts were present in 190 (87.2 per cent) patients
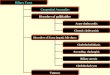
and the gallbladder filled at ERCP in 123 (56-4 per cent) patients. Stones in the gallbladder, identified by a variety of radiological techniques, were present in 150 (68.8 per cent)' patients. Endoscopic sphincterotomy was achieved in 21 1 (96.8 per cent) of 218 patients (Figure I ) and failed in seven (3.2 per cent). Causes of failure were previous Polya- gastrectomy in three patients, duodenal diverticular in two, and there were two patients in whom the papilla could not be found despite more than one attempt to locate it.
Common duct cIearance The common duct was cleared of stones in 193 (88.5 per cent) of the 218 patients and this was confirmed endoscopically in all cases. In 25 (11.5 per cent) patients duct clearance was unsuccessful (Table I). In seven of these 25 patients endoscopic
Endoscopic sphincterotomy attempted
successful
/"B Endoscopic sphincterotorny Endoscopic sphincterotomy
u nsuccessf u I
/'i' 7
Stone extraction Stone extraction u nsuccessfu I successfu I
I Reviewed
Elective cholecystectomy 11 121
Symptomatic cholecystectomy 10 I
Unrelated deaths 49
Figure 1 Clinical outcome of endoscopic sphincterotomy
554 0007-1323/91~050554-04 0 1991 Butterworth-Heinemann Ltd

Leaving the gallbladder in situ after sphincterotomy: J. Hill at al.
sphincterotomy had not been possible. In 14 of the remaining 18 patients the stones were considered too large to be removed by endoscopic sphincterotomy. Two patients refused further ERCP having become asymptomatic. One patient underwent surgery in the hands of the referring clinician while awaiting repeat ERCP and one patient was lost to follow-up. Eighteen of the 25 patients in whom common duct clearance failed underwent cholecystectomy and choledocholithotomy during the same admission without mortality. Of the other seven, four were considered unfit and three discussed above refused ERCP or were lost to follow-up. Two of these seven patients developed recurrent jaundice and required surgery. One is asymptomatic at 12 months and four died of unrelated causes 6,9, 12 and 36 months respectively after endoscopic sphincterotomy.
Complications Immediate complications of endoscopic sphincterotomy occurred in 16 (7.6 per cent) of 211 patients (Table2). Haemorrhage defined as a drop in haemoglobin concentration greater than 2g/dl occurred in seven patients, two requiring blood transfusion only. The other five underwent laparotomy and oversewing of the bleeding point, all five surviving the initial surgery. Two (1.0 per cent) patients died within 30 days of sphincterotomy. One patient, an 85-year-old woman, was transferred back to her referring unit and died 1 week later from recurrent bleeding, her physician deciding that further surgery was not warranted. The other patient who died was a 75-year-old man who presented with acute pancreatitis. The
Table 1
Cause of failure
Causes of failed duct clearance
No. of patients
Failed endoscopic sphincterotomy Stones too large Refused further ERCP
Surgical impatience Lost to follow-up
7 14 2 1 1
ERCP, endoscopic retrograde cholangiopancreatography
Table 2
Complication No. of patients
Complications of endoscopic sphincterotomy in 21 1 patients
Haemorrhage Cholangitis Pancreatitis Retroperitoneal perforation
7 (3-3) 5 (2.4) 2 (1-0) 2 (1-0)
Values in parentheses are percentages
ducts were cleared but he developed a pancreatic abscess during the same admission and died. Five patients developed cholangitis, two pancreatitis and two suffered asymptomatic retroperitoneal perforation, all resolving with conservative treatment. No patient developed clinical features of acute cholecystitis within 30 days of endoscopic sphincterotomy.
Fol lOW-Up All 191 patients with a clear common bile duct following endoscopic sphincterotomy have been reviewed between 12 and 100 months (mean 38 months). Eleven asymptomatic patients had elective cholecystectomy performed by the referring surgeon. Six of these were under 60 years of age. In only one of these 11 patients was exploration of the common duct necessary, a single stone being removed. This duct was clear of stones at ERCP and presumably the stone had passed from the gallbladder. Ten patients required cholecystectomy for symptoms or complications related to the gallbladder calculi. Indications for surgery were acute cholecystitis in five patients, biliary colic in three, jaundice in one and dyspepsia in one. Gallbladder calculi were present in all ten patients when the initial ERCP was performed, but present in only seven at cholecystectomy. The three patients with an empty gallbladder at cholecystectomy were diagnosed as having either biliary colic or dyspepsia. It is possible that cholecystectomy could have been avoided in these three patients if ultrasound scanning had been performed and shown an empty gallbladder. In nine of the ten patients cholecystectomy was necessary in the first year of follow-up. The other cholecystectomy was performed 4 years after endoscopic sphincterotomy, the indication for surgery being dyspepsia. In all, 49 (25.6 per cent) of the 191 patients died during the review period. No death was from biliary disease and no patient suffered symptoms related to the biliary tract. Of the 191 patients, 121 (63.4 per cent) remain alive and well with their gallbladders in situ.
Discussion Endoscopic sphincterotomy compares favourably with cholecystectomy and exploration of the common bile duct in comparable groups of but the subsequent management of the retained gallbladder remains controversial.
Two recent publications have suggested that 18 per cent and 40 per cent of patients undergoing successful endoscopic choledocholithotomy will subsequently require cholecys- tectomy".", but in the present series only ten (5.2 per cent) patients required cholecystectomy for symptoms. The results of ten published series of patients undergoing endoscopic sphincterotomy for removal of symptomatic bile duct stones in patients with intact gallbladders are are shown in Table31A-'0-14. In eight of the ten series with a minimum
Table 3 Results of endoscopic sphincterotomy in patients with gallbladder in situ
Operative No. of Mean age Mean follow-up Cholecystectomies mortality
Author Year patients (years) (months) no. (YO) no. (YO)
Escourrou et 4l.I' 1984 130 79 22 7 (5.4) Nil Davidson et 41.' 1988 105 79 29 9 (8.6) Nil Siege1 et aL4 1987 1272 73 ? 133 (10.5) 4 (3.0) Tanaka et 41. l4 1987 122 69
Hansel1 et 41." 1989 101 80
36 5 (4.1) Not reported
24 18 (17.8) Not reported Worthley and Toouli'' 1988 20 80 9 8 (40) 3 (37.5)
Vaira et al.13 Ingolby et 41.'
1989 265 76 36 1989 186 80 32
24 (9.0) Not reported 18 (9.7) Nil 26 (10.0) Not reported Cotton and Vallon3 1982 260 76 12-72
Present series 1990 191 74 38 10 (5.2) Nil
Total 2656 258 (9.7) 7 (2.7)
Br. J. Surg., Vol. 78, No. 5. May1991 555

Leaving the gallbladder in situ after sphincterotomy: J. Hill et al.
follow-up of 22 months, cholecystectomy for symptoms was necessary in less than 11 per cent of cases and in all ten series the mean rate for cholecystctomy was 9.7 per cent. In this series, nine of the ten patients requiring cholecystectomy did so within 1 year of endoscopic sphincterotomy, a similar finding to that of other ~ e r i e s " . ' ~ . ' ~ . The subsequent development of cholecystitis from gallbladder calculi has been reported at an annual rate of 2-7.5 per cent in patients without duct
Long-term follow-up in our series and other^'^*'^.'* has shown that the incidence of cholecystitis in the first year after endoscopic sphincterotomy is no greater than the predicted rate for all patients with gall stones and significantly less in subsequent years.
In this series the mortality of patients undergoing cholecystectomy for symptoms was nil. Apart from one very small series" with a mortality rate of 3 7 3 per cent, other reported mortality rates (Table 3) are similar to that for elective cholecystectomy in an aged population'9~20, and it is apparent that the mortality and requirement for cholecystectomy reported by Worthley and Toouli" is unrepresentative. In four of the reported series shown in Table 3 there were no details concerning mortality of any subsequent cholecystectomy. In four of the remaining series there were no deaths in these very elderly patients. Overall there were seven deaths in 258 patients (2.7 per cent) undergoing cholecystectomy. In our series 49 (25.6 per cent) patients died during the review period from causes unrelated to the biliary tract, the vast majority from cardiovascular disease. From this and the collected data in Table 3, we believe that routine elective cholecystectomy is not warranted if the common duct can be cleared of stones after endoscopic sphincterotomy.
Attempts have been made to find risk factors that might identify those patients likely to develop complications from their retained gall stones. Cystic duct obstruction in particular3.' and cholangitis at presentat.ion' have been suggested as risk factors. In our series the gallbladder did not fill in 88 (41.7 per cent) patients, a similar percentage to that found in the ten patients who required cholecystectomy for symptoms (Table 4 ) . Non-filling of the gallbladder during biliary excretion scintigraphy in patients who have had endoscopic sphincterotomy has recently been described22 and the authors suggested that stagnant bile may predispose to chronic infective changes or carcinoma in the gallbladder. Our results up to 100 months after endoscopic sphincterotomy d o not suggest that this is likely in the aged population in whom this procedure is usually undertaken. Thirty-eight patients (17.5 per cent) presented with cholangitis. Only two of these required subsequent cholecystectomy. Like others we have not found cystic duct obstruction'.1° or cholangitis at presen- tation" helpful in identifying patients who will require subsequent cholecystectomy. All ten patients undergoing cholecystectomy for symptoms had gallbladder calculi a t presentation but even this was not a positive risk factor for the development of complications from the retained gallbladder.
As in the series of Davidson et al.', none of the 15 patients with acute pancreatitis and an intact gallbladder has had a further attack. After an attack of acute biliary pancreatitis,
Table 4 Impact ofpotential risk faciors on the needfor cholecystectomy
Patients Fisher's at risk Cholecystectomy exact test (n=211) (n=10) P
Non-functioning 88 (41.7) 4 (40) 1.000
Cholangitis at 38 (18.0) 2 (20) 1 .oooo gallbladder
presentation
presentation Gallbladder stones at 150 (71.1) 10 (100) 0.065
Values in parentheses are percentages
556
cholecystectomy is usually Although one patient in our series died of a pancreatic abscess our results would support the view that endoscopic sphincterotomy alone may have a role in elderly patients with acute biliary pancreatitis.
To minimize the risks of biliary sepsis after endoscopy, all patients undergoing endoscopic sphincterotomy for symptomatic common duct stones and an intact gallbladder should have appropriate prophylactic intravenous antibiotics. An attempt should be made to clear the duct immediately, and if this is not possible biliary drainage should be ensured with either a pernasal catheter or a stent.
In conclusion: (1) elective cholecystectomy is not warranted in elderly patients with symptomatic bile duct stones if the common duct can be cleared of stones after endoscopic sphincterotomy, and (2) neither cystic duct obstruction nor cholangitis a t presentation are predictors of further symptoms or complications from the retained gallbladder.
References I .
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Davidson BR, Neoptolemos JP , Carr-Locke DL. Endoscopic sphincterotomy for common bile duct calculi in patients with gallbladders in siru considered unfit for surgery. Gut 1988; 29: 114-20. Ingolby CJH, El-Saadi J , Hall RI, Denyer ME. Late results of endoscopic sphincterotomy for bile duct stones in elderly patients with gallbladders in situ. Gui 1989; 30: 1129-31. Cotton PB, Vallon AG. Duodenoscopic sphincterotomy for removal of bile duct stones in patients with gallbladders. Surgery
Siege1 JH, Safrany L, Ben-Zvi IS, Pullano WE, Cooperman A, Stenzel M, Ramsey WHO. Duodenoscopic sphincterotomy in patients with gallbladders in situ: report of a series of 1272 patients. Am J Gustroenterol 1988; 83: 1255-8. Martin DF, Tweedle DEF. Endoscopic management of common duct stones without cholecystectomy. Br JSurg 1987;74: 209-11. Glenn F , Hays DM. The age factor in the mortality of patients undergoing surgery of the biliary tract. Sury Gynecot Ohstet 1955; 100: 11-18. Wenckert A, Robertson B. The natural course of gall stone disease. Gastroenierology 1966; 50: 376-81. Dixon JM, Armstrong CP, Duffy SW. Davies GC. Factors affecting morbidity and mortality after surgery for obstructive jaundice: a review of 373 patients. Gut 1983; 24: 845-52. Blamey SL, Fearon KCH, Gilmour WHO, Osborne DH, Carter DC. Prediction of risk in biliary surgery. Br J Surg 1983; 70: 535-8. Hansel1 DT, Millar MA, Murray WR, Gray GR, Giliespie G. Endoscopic sphincterotomy for bile duct stones in patients with intact gallbladders. Br J Surg 1989; 76: 8568 . Worthley CS, Toouli J . Gallbladder non-filling: an indication for cholecystectomy after endoscopic sphincterotomy. Br J Surg
Escourrou J, Cordova JA, Lazarthes F. Early and late complications after endoscopic sphincterotomy for biliary lithiasis with and without their gallbladder in situ. Gut 1984; 25:
Vaira D , Ainley CC, Theis B et al. Do patients need cholecystectomy after endoscopic sphincterotomy for bile duct stones? Gut 1989; Abstract W78. Tanaka M, Ikeda S, Yoshimoto H. Matsumoto S. The long-term fate of the gallbladder after endoscopic sphincterotomy : complete follow-up study of 122 patients. Am J Surg 1987; 154: 505-9. Gracie WA, Ronsohoff DF. The natural history of silent gall stones: the innocent stone is not a myth. New Engl J Med 1982;
McSherry CK, Forstenber H, Calhoun F et al. The natural history of diagnosed gall stone disease in symptomatic and asymptomatic patients. Ann Surg 1985; 202: 59-63. Rosseland AR, Solhaug J H . Primary endoscopic papillotomy in patients with stones in the common bile duct and gallbladder in situta5-8yearfollow-upstudy. WorldJSurg 1988; 12: 111-15. Hill J , Martin DF, Tweedle DEF. Endoscopic management of common duct stones without cholecystectomy - a five-year follow-up. Hepato-biliury Surgery 1990; 2: A579. Seitzer M H , Sleiger E, Rosato FE. Mortality following cholecystectomy. Surg Gynecol Ohstel 1970; 130: 64-6.
1982; 91: 628-30.
1988; 75: 796-8.
598-602.
307: 798-800.
Br. J. Surg., Vol. 78, No. 5, May1991

Leaving the gallbladder in situ after sphincterotorny: J. Hill et al.
20. Doyle PJ, Ward-McQuaid JN, McEwan-Smith A. The value of routine per-operative cholangiography - a report of 4000 cholecystectomies. Br J Surg 1982; 69: 617-19. Solhaug JH, Foskuan 0, Rosseland A, Rydberg B. Endoscopic papillotomy in patients with gallbladder in situ. Acta Chir Scand 1984; 150: 475-8. Desa LA, Grace PA, Vipond MN, Henderson B, Thompson JN. Gallbladder function after endoscopic sphincterotomy . Br J Med 1990; 300: 1111 . Elfstrom J. The timing of cholecystectomy in patients with gallstone pancreatitis. Acta Chir Scand 1978; 144: 487-90.
21.
22.
23.
Surgical workshop
24. Osborne D H , Imrie CW, Carter DC. Biliary surgery in the same admission for gall stone associated pancreatitis. Br J Surg 1981;
Ponston GJ , Williamson RCN. Surgical management of acute pancreatitis. Br J Surg 1990; 77: 5-12. Paloyan D, Simonowitz D, Skinner DB. The timing of biliary tract operations in patient with pancreatitis associated gall stones. Surg Gynecol Obstet 1975; 141: 737-9.
68: 758-61. 25.
26.
Paper accepted 14 October 1990
Br. J. Surg. 1991, Vol. 78. May, 557-558
Sheffield cholecystoscope: new instrument for minimally i nvasive ga I I bladder surgery
A. W. Majeed, M. W. R. Reed, D. F. L. Watkin*, J. G. Smart? and A. G. Johnson
Department of Surgery, University of Sheffield, Royal Hallamshire Hospital, Sheffield, UK, *Department of Surgery, L eicester Royal Infirmary, L eicester, UK and ?Department of Urology, Leicester General Hospital, Leicester, UK Correspondence to: Mr A. W. Majeed, Department of Surgery, Royal Hallamshire Hospital, Sheffield S10 2JF, UK
Symptomatic gallbladder stones should be treated electively, preferably before complications occur'. Mortality and morbidity rates increase significantly with emergency oper- ations, especially in the elderly*. Recently introduced alternatives to cholecystectomy include extracorporeal shock wave lithotripsy (ESWL) combined with oral dissolution therapy, ultrasound guided gallbladder puncture with stone dissolution or extraction and laparoscopic cholecystectomy.
Selection criteria for ESWL limit its application to about 15 per cent of patients3. Ultrasound guided puncture of the gallbladder with tract dilatation and gallstone extraction is a lengthy, complicated procedure requiring radiological guidance. Complications include visceral perforation, bile peritonitis and loss of access4. The technique requires general anaesthesia. Contact dissolution with methyl tert-butyl ether, also a complicated procedure, may be associated with duodenal and ' bile duct damage5. Laparoscopic cholecystectomy also requires a general anaesthetic and an extensive pneumo- peritoneum. The procedure is under evaluation to define its indications and complications6.
We report a new instrument which permits gallbladder stones to be removed under direct vision using local or regional anaesthesia by a minimally invasive technique.
Materials and methods The Shefield cholecystoscope (patent pending, application no. GB 2 214 428 A ) is simple in design (Figure 1) . Two concentric tubes with an outer diameter of 2.5 cm and an inner diameter of 2 cm are held apart by perforated spacers. The space between the tubes 1s closed at one end and open at the other. Suction applied to this space has the effect of creating a ring of vacuum which secures the instrument to the
fundus of the gallbladder. The instrument is available in 16 cm and 10 cm lengths depending on the distance of the gallbladder fundus from the skin.
A small (2.5 cm), horizontal, muscle splitting incision is made in the right upper quadrant of the abdomen in the anterior axillary line. A 2 cm incision is made in the peritoneum once this is reached. The scope is then inserted into the peritoneal cavity, ensuring a snug fit into the peritoneal incision. An adapted sigmoidoscopic eyepiece is applied to the working end of the scope and a Higginson's syringe is attached to the vacuum channel. A good view of the liver and gallbladder is obtained and any omentum or viscera may be displaced by pumping a small amount of air (in the same way as performing a sigmoidoscopy). However, a formal pneumoperitoneum is not created. avoiding diaphragmatic splinting. Once the fundus of the gallbladder is seen the scope is approximated to it and a vacuum is created. A minimum vacuum of 0 8 2 mbar for up to 5 min is required for safe fixation to occur and this vacuum is maintained throughout the procedure by continuous suction.
This seal resists distraction of up to 1.2 kg (linear traction). Standard wall suction in most operating theatres is only 0.47 mbar and in practice a Speedivac 2 Vacuum Pump (Edwards High Vacuum, Crawley, U K ) has been used.
Figure 1 gallbiudder fundus by vacuum clamping
Method yffixution of the Sheffield cholecystoscope lo the
-~ ~ _ _ ~ - - 0007-1 323/91/050557-02 ( 1991 Butterworth-Heinemann Ltd 557