Embed Size (px)
Citation preview

Risk Stratification ofSudden Cardiac Death
Michael R Gold, MD, PhDMedical University of South Carolina
Charleston, SC USA
Disclosures: None

Sudden Cardiac DeathA Major Public Health Problem
> 1/2 of all cardiac deaths
1/6 of all deaths
> 400,000 SCD annually in US

Sustained Monomorphic VTVFAsystoleSudden Death Can Result From a Variety of Processes

Acute Ischemia Causing Ventricular Fibrillation
Sudden Death Can Result From a Variety of Processes

Complete Heart Block Ventricular Fibrillation
Sudden Death Can Result From a Variety of Processes

Pause – Dependent Torsade de PointesAssociated with Antifungal Drug
Sudden Death Can Result From a Variety of Processes

40 Years of ICD Technology
Engineering Tour de’ Force

ICDs in the Prevention of Death from Tachyarrhythmia Cardiac Arrest
AVID
80% CAD20% other
Secondary Prevention
The AVID Investigators NEJM 1997;337:1576

Secondary Prevention of SCD
AVID/CIDS/CASH Metaanalysis
EVENTS AT2 YEARS ICD
N=934AMIO
N=932H.R.
Deaths 200 255 .73p<0.001
Arrhythmic 61 117 .49p<0.001
Non - Arr 139 138 .93

Survival From Out-of-Hospital Cardiac Arrest
19%Seattle - 1982
30%AED
Seattle - 19880.8% (Blacks)2.6% (Whites) Chicago - 1998
14%Miami - 1974
7%AED
Miami - 2002

HAT Study Primary Endpoint

PAD Trial 993 Units 157 Residential (16%) 836 Public (84%)
Recreational facilities (28%) Shopping centers (28%) Entertainment complexes (10%) Community centers (8%) Large office buildings (8%) Other (hotels, factories, transit centers) (17%)
Hallstrom A, et al. N Engl J Med. 2004;351:637.

PAD Trial
Hallstrom A, et al. N Engl J Med. 2004;351:637.



Septadian Variability of SCD

Subpopulation on Beta Blockers



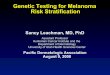
Influence of Race on SCD
Age-adjusted death rates (per 100,000 US population) for sudden cardiac death
Zheng Z. Circulation 2001
Years
Per 1
00,0
00 S
tand
ard
US
Popu
latio
n 600
500
400
300
200
100
0
1989 1990 1991 1992 1993 1994 1995 1996 1997 1998
African-American
White
American IndianAsian

Risk Stratification for SCD
Risk stratification of SCD has been studied for 40 years
The rule of 80 emerged–80% Male–80% VT/VF–80% CAD–80% LV dysfunction
More recent epidemiological studies have questioned these assumptions which are the foundation of preventative strategies

Sudden Cardiac DeathThe Maastricht Prospective Registry
1997-2000: 492 cases
Hx of CHF – 59 pts (12%)
In 54% (224 pts) cardiac arrest was the first manifestation of cardiac disease!
Gorgels et al. European Heart J, 2003; 24:1204

Sudden Cardiac DeathThe Maastricht Prospective Registry
Patients with Cardiac History: n=224
CAD - 171 (77%)
New MI – 10 (6%)
Prior MI – 113 (66%)
Time first MI to SCA – 9.7 ± 7.5 yrs
Prior Ant. MI – 37% Inf. MI – 53%
Gorgels et al. European Heart J, 2003; 24:1204

The Oregon Sudden Unexpected Death Study
2002-2004: 714 cases-Multnomah County, Oregon (pop.: 660,486)
EF measured prior to event in only 121 cases (17%)
Stecker et al. JACC, 2006; 47:1161

LV Ejection Fraction %
≤35% 30
36-54% 22
≥ 55% 48
Sudden Death-The Oregon Sudden Unexpected Death Study
Stecker et al. JACC, 2006; 47:1161
Patients with Known EF (121)

LVEF and SCA Incidence
012345678
0-30% 31-40% 41-50% >50%
deVreede-Swagemakers JJ. J Am Coll Cardiol. 1997;30:1500-1505.
LVEF
% S
CA
Vict
ims
7.5%
5.1%
2.8%
1.4%

Why is there a paradox between SCD and post MI Risk?
Gusto Study (n=2400)Angiographic substudyCardiac Cath 5-7 days post MI
– EF < 30% 4.3%– EF 30-40% 10.1%– EF > 40% 85.6%
Equivalent sudden deaths in EF <30% and EF > 40% groups even if 20-fold greater risk!

Non-Antiarrhythmic Drugs that Reduce Mortality and SCD
Beta BlockersACE InhibitorsARBsStatinsAldosterone AntagonistsASA

Antiarrhythmic Drugs that Reduce Mortality and SCD

MADIT I- Inclusion Criteria
CAD
LVEF < 35%
Nonsustained VT
Inducible VT (+ EPS)

MADIT I - Survival
1.0
0.8
0.6
0.4
0.2
0.00 1 2 3 4 5Year
Prob
abili
ty o
f sur
viva
l
Conventionaltherapy
Defibrillator
Moss AJ. N Engl J Med. 1996;335:1933-1940.
p=.009 at termination2 yr mortality 39% v 16%HR - 0.46

MUSTT Randomized Patient Results Total Mortality
Buxton AE. N Engl J Med. 1999;341:1882-90.
Time after Enrollment (Years)0 1 2 3 4 5
0
0.1
0.2
0.3
0.4
0.5
0.6
Even
t Rat
e
p < 0.001
EP-Guided Rx, No ICD No EP-Guided AA RxEP-Guided Rx, ICD

MADIT II - Eligibility Criteria
LVEF < 30% > 1 prior MI No arrhythmia req.
NYHA Class IV < 1 month from
acute MI CABG or PTCA
< 3 months Patients meeting
MADIT I criteria
Inclusion Exclusion

MADIT-II Survival
Moss AJ. N Engl J Med. 2002;346:877-83.
Defibrillator
Conventional
P = 0.007
1.0
0.9
0.8
0.7
0.6
0.0
Prob
abili
ty o
f Sur
viva
l
0 1 2 3 4
YearNo. At RiskDefibrillator 742 502 (0.91) 274 (0.94) 110 (0.78) 9Conventional 490 329 (0.90) 170 (0.78) 65 (0.69) 3

MADIT II – 8 Year Long Term Follow-up
Number Needed to Treat to save one life (NNT) and Life Years Saved (LYS) for all MADIT II patients (N=1232):
@ month 20 96
NNT 17 6
LYS 0.2 1.2
Death 31% 37%

• 2521 patients with either ischemic or NIDCM• NYHA Class II or III• EF < 35%• Single chamber ICDs – VVI 35/50bpm. Shock only 188 bpm• Amio/placebo drug or ICD/placebo drug

00
0.10.1
0.20.2
0.30.3
0.40.4
00 66 1212 1818 2424 3030 3636 4242 4848 5454 6060
Mor
talit
yM
orta
lity
Months of follow-upMonths of follow-up
AmiodaroneAmiodaroneICD TherapyICD TherapyPlaceboPlacebo
HR 97.5% CI P-ValueAmiodarone vs. Placebo 1.06 0.86, 1.30 0.529ICD Therapy vs. Placebo 0.77 0.62, 0.96 0.007
Mortality by Intention‐to‐treat
Follow-up: 45.5 monthsVital status: 100% known
N = 2,521
Sudden Cardiac Death
SCD-HeFTHeart Failure Trial
36.1%
28.9 %
34.0%
Bardy, NEJM 2005

DINAMIT
Hohnloser, S. et al. N Engl J Med 2004;351:2481-2488
• 674 Patients s/p Acute MI
• Single lead ICD• EF ~ 28%• 70% Q wave MI• Time to ICD
from MI -18 dy

Immediate Risk-Stratification Improves Survival (IRIS) StudyImmediate Risk-Stratification
Improves Survival (IRIS) Study
Steinbeck G, et al. N Engl J Med 2009;361:1427-36.
• Randomized comparison of ICDs vs. OMT 5-31 days after MI • LVEF ≤ 40%, HR > 90 +/- NSVT• No survival benefit with prophylactic ICD therapy
N=902 patients

Incremental Benefits with HF Therapies(Cumulative % Reduction in Odds of Death at 24 Months)
-28% to -49%P<0.0001
-54% to -71%P<0.0001
-68% to -81%P<0.0001
-75% to -86%P<0.0001
-77% to -88%P<0.0001
-72% to -87%P<0.0001
Fonarow GC, Yancy, CW. J Am Heart Assoc 2012;1:16-26.

Primary Prevention ICDs in Nonischemic Cardiomyopathy
• The role of ICDs among patients with ischemic cardiomyopathy was is well established, provided that it is not implanted early post‐MI
• Further expansion of ICD indications for patients with nonischemic cardiomyopathy was evaluated in a series of trials
• This included both narrow and wide QRS patients using conventional ICDs or CRT devices

DEFINITE – NIDCM
ICD – 229 ptsStandard -- 229 pts
P=0.08
HR 0.65 [95% CI, 0.40 to 1.06]
Follow up 29 +/- 14 months
• Age 58• 71% men• 23% DM• 25% AF• QRS 115 ms• LBBB 20%
Kadish A et al NEJM 2004;350:2151
• ACE/ARB 97%• -blockers 85%

DEFINITE
Sudden Death Mortality All-Cause Mortality in NYHA Class III
P=0.006 P=0.02
Kadish A et al NEJM 2004;350:2151

DEFINITE: ICDs in NIDCMNo required “time from HF diagnosis to enrollment”
< 3 mo(150)
Control 17.6%
ICD 7.3%HR = 0.37 (0.14‐0.99)
p =0.05
Kadish et al JACC 200663% RR
Early ICD Implants

00
0.10.1
0.20.2
0.30.3
0.40.4
00 66 1212 1818 2424 3030 3636 4242 4848 5454 6060
Mor
talit
yM
orta
lity
Months of follow-upMonths of follow-up
AmiodaroneAmiodaroneICD TherapyICD TherapyPlaceboPlacebo
HR 97.5% CI P-ValueAmiodarone vs. Placebo 1.06 0.86, 1.30 0.529ICD Therapy vs. Placebo 0.77 0.62, 0.96 0.007
Mortality by Intention‐to‐treat
Follow-up: 45.5 monthsVital status: 100% known
N = 2,521
Sudden Cardiac Death
SCD-HeFTHeart Failure Trial
36.1%
28.9 %
34.0%
Bardy, NEJM 2005

00
0.10.1
0.20.2
0.30.3
0.40.4
0.50.5
00 1212 2424 3636 4848 6060
Mor
talit
yM
orta
lity
Months of follow-upMonths of follow-up
ICD TherapyICD TherapyPlaceboPlacebo
00 1212 2424 3636 4848 6060Months of follow-upMonths of follow-up
Mortality by NYHA Class: ICD vs. Placebo
Class II Class III
HR 97.5% CI0.54 0.40, 0.74
HR 97.5% CI1.16 0.84, 1.61
32%
46%
20%
48%
Sudden Cardiac Death
SCD‐HeFTHeart Failure Trial
NYHA Class II - NNT = 8

Ischemic Etiology Non‐Ischemic Etiology
00
0.10.1
0.20.2
0.30.3
0.40.4
0.50.5
00 1212 2424 3636 4848 6060
Mor
talit
yM
orta
lity
Months of follow-upMonths of follow-up
ICD TherapyICD TherapyPlaceboPlacebo
00 1212 2424 3636 4848 6060Months of follow-upMonths of follow-up
Mortality by CHF Etiology
HR 97.5% CI0.79 0.60, 1.04
HR 97.5% CI0.73 0.50, 1.07
43%
21%
36%
28%
Sudden Cardiac Death
SCD‐HeFTHeart Failure Trial

Mode of Death in SCD‐HeFT: ICD ‐ Placebo
02468
101214
Arrhythmic Heart Failure Other
ICDPlacebo
% D
eaths
37
95
66674.5%
11.2%
7.5%7.9%
p <0.001
Sudden Cardiac Death
SCD‐HeFTHeart Failure Trial
9.6%
78
9.8%
83
Adapted from Packer D, et al HRS 2005
Total Deaths:ICD = 182Placebo = 244
*45.5 mo median f/u

0
100
200
300
400
500
600
II III Isch. N-Isch.
ICD implanted
VT/VF shock
21%25% 21% 24%
# of Pts
Class and etiology of CHF: VT/VF shocks
554
257
420 391
117 65 89 93

From: ACC/AHA/HRS Guideline Committee JACC 2008; 51: 2085-105
Classification of Recommendations for Device-Based Therapy
SIZE OF TREATMENT EFFECT
Class IBenefit > > > RiskProcedure/Treatment SHOULD be performed/administered
Class IIaBenefit > > RiskAdditional studies with focused objectives neededIT IS REASONABLE to perform procedure/administer treatment
Class IIBBenefit > RiskAdditional studies with broad objectives needed; additional registry data would be helpfulProcedure/TreatmentMAY BE CONSIDERED
Class IIIRisk > BenefitProcedure/Treatment should NOT be performed/administered SINCE IT IS NOT HELPFUL AND MAY BE HARMFUL


Danish NIDCM Trial
• NYHA class II or III, or NYHA class IV if CRT• LVEF ≤35%, > 200 pg/ml of NT‐proBNP• GDMT target doses of ACE/ARB and ‐blockers• PM or CRT‐P was not an exclusion• AF with HR resting over 100 bpm excluded• Dialysis excluded

Danish NIDCM Trial
• 1116 patients
• Randomized to ICD or “usual clinical care”
• Mean QRS: 146 ms (ICD); 145 ms (control)
• CRT: 58% (ICD); 58% (control)

Outcomes – All‐Cause Mortality

Outcomes
Cardiovascular Death Sudden Cardiac Death

Comparisons: DEFINITE, SCD‐HeFT, DANISH
DEFINITE SCD‐HeFT DANISH
ACE/ARB 96.7% 89% 97%
‐blockers 85% 78% 92%
Mineralocorticoid ? 30% 58%

Mortality: DEFINITE ‐ DANISH
DEFINITE CONTROL
DEFINITE ICD

Mortality Comparisons
SCD-HeFT CONTROL
SCD-HeFT ICD

COMPARISON OF REPORTED SCD RATES
Blue Dots
PARADIGM
DANISH
DANISH: Unusually low SCD rate:1.5% per year, only 35% of all deaths were sudden

DANISH TRIAL ‐ CONSIDERATIONS
• Selection Bias: Enrolled unusually low risk NIDCM patients– were the more ill already offered ICDs?
• Well – treated on GDMT• Outcome adulterated by CRT–Much higher % of CRT eligible patients enrolled than found in usual outpatient clinics (20‐25% v 60% in DANISH)

CARE-HFCARE-HF
409 383 358 338 209 85404 372 331 298 178 63
CRTMedical therapy
Number at risk
96
CRT
MedicalTherapy
0 400 16000.00
0.25
0.50
0.75
1.00Su
rviv
al
Time (days)800 1200
Hazard Ratio 0.60 (95% CI 0.47 to 0.77; P<0.0001)

COMPANION: All-Cause MortalityCOMPANION: All-Cause Mortality

From: Golwala H et al. Circulation 2017; 135: 201-203
All-cause Mortality in NICM Patients with Primary Prevention ICD or CRT

SUMMARYSCD remains a major cause of mortality in
the US and AsiaTreatment and Prevention of CAD and CHF
are important, including PCI and MedicationsICDs are the most effective therapy to
prevent SCD, but utililaztion remains lowICDs should be considered in ischemic
cardiomyopathy as well as dilated cardiomyopathy which persist with GDMT, despite the recent Danish Trial