Embed Size (px)
Citation preview

Risk of Type 2 Diabetes Among U.S. and Foreign Born Asians: Evidence from NHANES 2011-2012.Hannah L. Jackson, PhD, MPH1,2, Dejun Su, PhD1, May C. Wang, DrPH3, Terry T. Huang, PhD, MPH, CPH4
(1) Center for Reducing Health Disparities, University of Nebraska Medical Center.(2) Department of Health Promotion and Social and Behavioral Health, University of Nebraska Medical Center.(3) Community Health Sciences, UCLA Fielding School of Public Health.(4) CUNY School of Public Health.
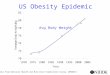
Introduction/ BackgroundNon-Hispanic Asians are the fastest growing demographic group in the U.S. (1) By 2050 Non-Hispanic Asians are projected to make up approximately 8% of the total U.S. population (1). Non-Hispanic Asians have become the largest stream of immigrants to the U.S. comprising 36 % of all new immigrants , surpassing the total number of Hispanic immigrants (2).
Diabetes is the fifth leading cause of death among Non-Hispanic Asians after cancer, heart disease, stroke, and unintentional injuries (3). Diabetes is a debilitating condition that can lead to comorbid health conditions such as heart disease and premature death (4). Metabolic dysfunction associated with type 2 diabetes include high levels of blood glucose and dyslipidemia (5,6).
Non-Hispanic Asians around the world are at increased risk for metabolic symptoms that may contribute to the development of type 2 diabetes (7,8).Nativity to the U.S. has important effects on the development of metabolic dysfunction and type 2 diabetes among Non-Hispanic Asians.
Previous research among Hispanic immigrants demonstrate increased body mass index (BMI), hypertension and high blood pressure after having lived in the U.S. for a period of time (9). Comparable research on Non-Hispanic Asian populations is limited, however there is evidence to show that Asian immigrants are in better health upon arrival to the U.S. (10,11).
Methods
Purpose
Previous studies examining metabolic dysfunction and type 2 diabetes have not utilized a nationally representative sample of Non-Hispanic Asians with objective measures. Using the 2011-2012 NHANES , the purpose of this study was to (1) compare the risk of type 2 diabetes and metabolic dysfunction (2) compare the risk of metabolic dysfunction and type 2 diabetes between U.S. and foreign born Non-Hispanic Asian adults.
Conclusion and Future DirectionsConclusions:The finding of elevated triglycerides and type 2 diabetes, and decreased HDL corroborates with previous literature among Non-Hispanic Asian adults (13). This may due in part to the traditional Asian diet, which is primarily composed of refined grains and simple carbohydrates (14).Plausible theories for our results include, lack of dietary and health knowledge, availability of unhealthy foods in new host environment, diet, chronic stress ,which may be experienced by immigrants through the process of immigration. Another theory, may be that Western culture and lifestyles are not compatible with the metabolic programming of Non-Hispanic Asians born outside rather than within the U.S.
Future Recommendations: Clinical implications include the need for clinicians that serve Non-Hispanic Asian communities to be cognizant of the elevated risk , even if BMI does not reach the overweight/obese threshold. Future surveillance data should consider variations among Non-Hispanic Asian subgroups which may impact health outcomes and disparities.
References1.US Census Bureau. Asians Fastest-Growing Race or Ethnic Group in 2012, US Census Bureau Reports. 2013. 2.US Census Bureau. The Asian Population:2010. 2012.3.US Census Bureau. An Older and More Diverse Nation by MidCentury. 2008.4.Emerging Risk Factors Collaboration, Seshasai SR, Kaptoge S, Thompson A, Di Angelantonio E, Gao P, et al. Diabetesmellitus, fasting glucose, and risk of cause-specific death. N Engl J Med 2011 Mar 3;364(9):829-841.5.American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010 Jan;33 Suppl 1:S62-9. 6.Grundy SM, Brewer HB,Jr, Cleeman JI, Smith SC,Jr, Lenfant C, American Heart Association, et al. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004 Jan 27;109(3):433-438. 7.Shabbir S, Kwan D, Wang MC, Shih M, Simon PA. Asians and Pacific Islanders and the growing childhood obesity epidemic. Ethn Dis 2010;20(2):129-130.8.Ye J, Rust G, Baltrus P, Daniels E. Cardiovascular risk factors among Asian Americans: results from a National Health Survey. Ann Epidemiol 2009;19(10):718-723. 9.Kaplan MS, Huguet N, Newsom JT, McFarland BH. The association between length of residence and obesity among Hispanic immigrants. Am J Prev Med 2004;27(4):323-326.10.Steffen PR, Smith TB, Larson M, Butler L. Acculturation to Western society as a risk factor for high blood pressure: a meta-analytic review. Psychosom Med 2006 May-Jun;68(3):386-397.11.Kim J, Chan MM. Acculturation and dietary habits of Korean Americans. Br J Nutr 2004;91(03):469-478. 12.Centers for Disease Control (CDC) , National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Questionnaire (or Examination Protocol,or Laboratory Protocol). 2013; Available at: http://www.cdc.gov/nchs/nhanes/nhanes2011-2012/current_nhanes_11_12.htm. Accessed March 14, 2014.13.McNeely MJ, Boyko EJ. Type 2 diabetes prevalence in Asian Americans: results of a national health survey. Diabetes Care 2004 Jan;27(1):66-69.14.Dixit AA, Azar KM, Gardner CD, Palaniappan LP. Incorporation of whole, ancient grains into a modern Asian Indian diet to reduce the burden of chronic disease. Nutr Rev 2011;69(8):479-488.
ABSTRACT
The source of this study is the 2011-2012 National Health and Nutrition Examination Survey (NHANES), a cross-sectional nationally representative surveillance system designed to assess the current health status of the non-institutionalized population of residents in the U.S. The 2011-2012 Wave of NHANES over-sampled Non-Hispanic Asians for the first time. Each survey used a complex, stratified, multi-staged probability clustering sample design. NHANES 2011-2012 was approved by the National Center for Health Statistics (NCHS) and Centers for Disease Control (CDC) Institutional Review Board, which included written and informed consent from participants (12). Logistic regression models were used to calculate odds ratios of metabolic dysfunction and type 2 diabetes. Covariates in our model included: age, sex, education, serum cotinine exposure , nativity, marital status and BMI
Results Sample characteristics are presented in Table 1. Relative to Non-Hispanic Whites, Non-Hispanic Asians were slightly older (means SD ± = 50.3 ± 0.4 vs. 44.3 ± 0.5 years, p<0.05) , and had higher BMI ( means ± SD = 28.3 ± 0.15 vs. 24.40 ± 0.15 kg/m2 , p<0.05).
Table 2 shows the odds of metabolic dysfunction among Non-Hispanic Asian adults. Non-Hispanic Asians were at significantly elevated risk for low HDL (OR=1.78, 95% CI: 1.02-3.11), pre-diabetes by HbA1c ≥ 5.6 % (OR= 3.25, 95% CI:1.79-5.90) , and type 2 diabetes by HbA1c ≥ 6.5% (OR= 3.32, 95 % CI:1.58-6.98) relative to Non-Hispanic Whites.
In Table 3, foreign-born Non-Hispanic Asians were at elevated risk for high LDL (OR=1.79, 95% CI: 1.23-2.59), elevated cholesterol (OR=1.77, 95% CI: 1.31-2.39) and type 2 diabetes by HbA1c ≥ 6.5% (OR=1.94, 95% CI: 1.24-3.02) relative to U.S. born Non-Hispanic Asian adults after adjusting for covariates.
Table 1: Sample characteristics of Non-Hispanic Asian and Non-Hispanic white adults (18 years and older)a
Diabetes Risk Odds Ratio 95 % CI
OGTT ≥ 140 mg/dL 2.00 0.48-8.21
OGTT ≥ 200 mg/dL 2.63 0.87-7.95
HbA1c ≥ 5.6 % 3.25* 1.79-5.90
HbA1c ≥ 6.5 % 3.32* 1.58-6.98
IFG ≥ 100 mg/dL 0.97 0.63-1.49
IFG ≥ 126 mg/dL 0.90 0.59-1.37
Metabolic Risk Factors
SBP ≥ 130 mmHg 1.14 0.73-1.79
DBP ≥ 85 mmHg 1.10
1.11-1.33
LDL ≥ 100 mg/dL 0.63
0.33-1.18
Triglycerides ≥ 150 mg/dL 1.42
0.98-2.06
HDL ≤ 40 mg/dL (male) & HDL ≤ 50 mg/dL (female) 1.78*
1.02-3.11
Total Cholesterol ≥ 200 mg/dL 0.78
0.58-1.06
Table 2: Adjusted metabolic risk for Non-Hispanic Asian vs. Non-Hispanic White Adults in the U.S.
Model adjusted for age, sex, education level, marital status, BMI, serum cotinine exposure (for smoking), and nativity. Non-Hispanic Whites serve as the referent. *p<0.05
a National Health and Nutrition Examination and Survey 2011-2012Data are % values unless otherwise indicated as means ± SD. ***p=0.05,.*P<0.05, **P≤ 0.001
Table 3: Adjusted Metabolic Risks for Foreign Born vs. U.S. Born Non-Hispanic Asian Adults in the U.S. Diabetes Risk Odds Ratio 95 % CI
OGTT ≥ 140 mg/dL 1.91 0.55-6.65OGTT ≥ 200 mg/dL 2.53*** 1.00-7.95HbA1c ≥ 5.6 % 0.92 0.52-1.64HbA1c ≥ 6.5 % 1.94* 1.24-3.02IFG ≥100 mg/dL 1.35 0.90-2.02IFG ≥126 mg/dL 1.39 0.89-2.17 Metabolic Risk Factors
SBP ≥ 130 mmHg 0.85 0.57-1.25DBP ≥ 85 mmHg 1.48 0.85-2.57LDL ≥ 100 mg/dL 1.79* 1.23-2.59Triglycerides ≥ 150 mg/dL 1.27 0.91-1.77
HDL ≤ 40 mg/dL (male) ≤ 50 mg/dL (female) 1.37 0.96-1.95
Total Cholesterol ≥ 200 mg/dL 1.77* 1.31-2.39
Odds ratios are adjusted for age, sex, education, marital status, serum cotinine, and BMI. U.S.-born Non-Hispanic Asians serve as the referent group.***=0.05., *p<0.05
Introduction: The purpose of this study was to compare risks for metabolic dysfunction and type 2 diabetes among Non-Hispanic Asian and Non-Hispanic white adults in the U.S. We also examined the impact of nativity on metabolic dysfunction and type 2 diabetes among Non-Hispanic Asian adults. Methods: This study used the NHANES 2011-2012 adult data for Non-Hispanic Asians (n=827) and Non-Hispanic Whites (n=2,108). Standardized risk threshold cutoffs for blood pressure, lipids, and glucose were used to determine metabolic dysfunction. Logistic regression models were used to compare odds of metabolic dysfunction among Non-Hispanic Asians vs. Non-Hispanic Whites, and U.S. - vs. foreign-born Non-Hispanic Asians. Covariates included age, sex, education level, marital status, BMI, serum cotinine exposure (for smoking), and nativity (in model comparing Non-Hispanic Asians and Whites).Results: Non-Hispanic Asians were at increased risk of metabolic dysfunction and type 2 diabetes compared to Non-Hispanic Whites for HDL≤ 40 mg/dL (men) and ≤ 50 mg/dL (women) (OR=1.78, 95% CI=1.02-3.11), HbA1c ≥ 5.6 % (OR=3.23, 95% CI= 1.79-5.90), and HbA1c ≥ 6.5 % (OR=3.32, 95% CI=1.58-6.98). Relative to U.S.-born Non-Hispanic Asians, foreign-born Non-Hispanic Asians had elevated risk for HbA1c ≥ 6.5 % (OR=1.94, 95% CI=1.24-3.02), total cholesterol ≥ 200 mg/dL (OR= 1.77, 95 %CI = 1.31-2.39) and LDL ≥ 100 mg/dL (OR=1.79, 95% CI=1.23-2.59). Conclusions: This is the first analysis of metabolic dysfunction and type 2 diabetes among U.S. vs. foreign -born Non-Hispanic Asians using nationally representative data. Independent of BMI, Non-Hispanic Asians overall are at significantly higher risk for low HDL and type 2 diabetes compared to Non-Hispanic white adults. Non-Hispanic Asian immigrants compared to U.S. born Non-Hispanic Asians appear to be the most at risk.
Total (N=2935)Non-Hispanic Asian (N=827)
Non-Hispanic White (N=2108)
Born in the US % 16.2** 96.6Age xN (years) 44.3* (0.5) 50.3 (0.4)Edu level %Less than HS 8.60% 2.4College Graduate 50.8** 35.9Gender %Female 53.6 51.1Current Marital Status %Married 62.5* 52.2Serum Cotinine % ≥ 1 ng/mL 24.6* 38Metabolic Risk Profile
BMI xN (m/kg2) 24.4* (0.1) 28.3 (0.1)SBP ≥ 130 mmHg 19.3** 28.7DBP ≥ 85 mmHg 9 8.6
HDL ≤ 40 mg/dL (male) & ≤ 50 mg/dL (female) 26.5* 30.8LDL ≥ 100 mg/dL 82.1 83.1Triglycerides ≥ 140 mg/dL 33.8 37.6Total Cholesterol ≥ 200 mg/dL 47.4 46.7Diabetes RiskOGTT ≥ 200 mg/dL 69.2 66.9OGTT ≥ 140 mg/dL 73.9 72.2IFG ≥ 100 mg/dL 64.8 64.4IFG ≥ 126 mg/dL 60.2 58.3HbA1c ≥ 5.6 % 21.2** 15.2HbA1c ≥ 6.5 % 50.7*** 46.7