Embed Size (px)
Citation preview

10/16/2014
1
Health is Not Measured in Pounds
Arya M Sharma, MD. PhD, FRCPCResearch Chair for Obesity Research &
ManagementUniversity of Alberta
Medical DirectorAlberta Provincial Obesity Program
Edmonton, AB, Canadawww.drsharma.ca

10/16/2014
2
Sharma AM, 1995
Venus of Willendorf ~ 25,000 BC
Museum of Natural History, Vienna, Austria
10/16/2014
3
June 18th, 2013:The AMA recognizes obesity as a diseaserequiring a range of medical interventions to advance obesity treatment and prevention
AMA position statement http://www.ama-assn.org/
A condition characterized by excess body fat that threatens or affects socioeconomic, mental or physical health
Sharma 2007
What is Obesity?

10/16/2014
4
What is Ideal Weight?
Met Life Tower (1911)
“Desirable Weight” introduced in 1943 by the Metropolitan Life Insurance Company (MLIC) in standard height-weight tables for men and women
Metropolitan Life Insurance Company (MLIC) Standard Height-Weight Tables for Women
BMI=19.3 kg/m2 BMI=25.6 kg/m2
10/16/2014
5
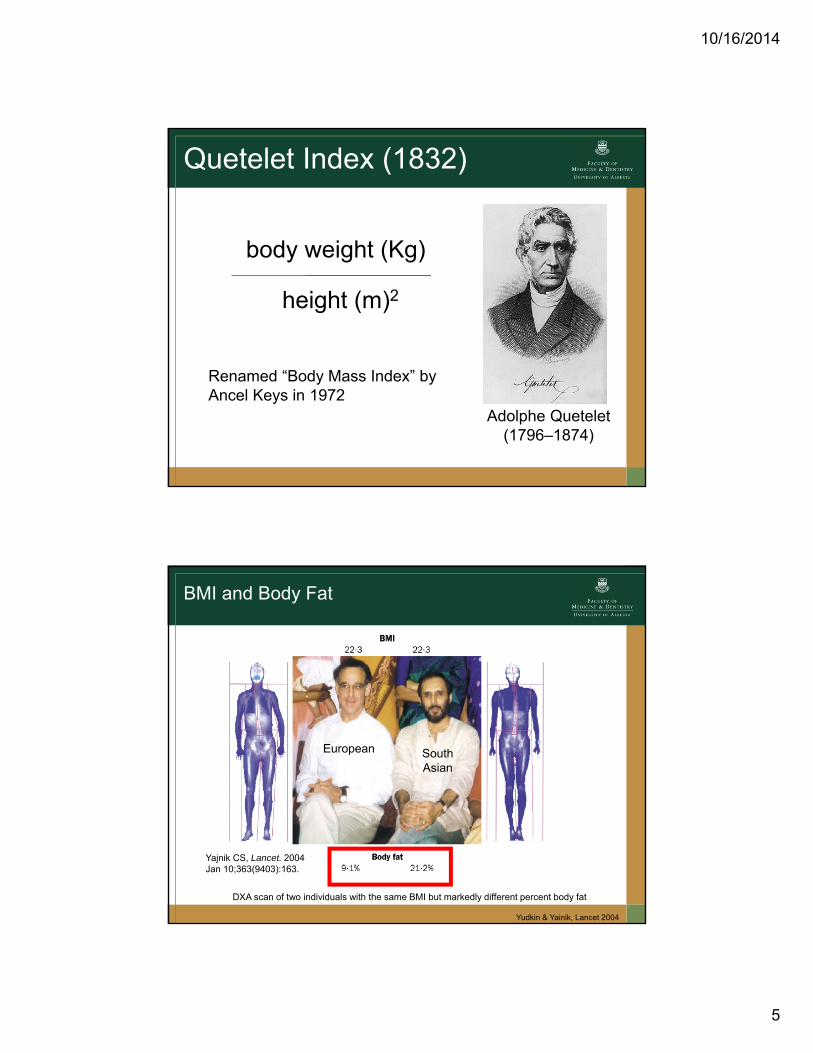
Quetelet Index (1832)
body weight (Kg)
height (m)2
Adolphe Quetelet(1796–1874)
Renamed “Body Mass Index” by Ancel Keys in 1972
BMI and Body Fat
DXA scan of two individuals with the same BMI but markedly different percent body fat
European South Asian
Yajnik CS, Lancet. 2004 Jan 10;363(9403):163.
Yudkin & Yainik, Lancet 2004

10/16/2014
6
Relationship Between BMI and Percent Body Fat in Men and Women
Adapted from: Gallagher et al. Am J Clin Nutr 2000;72:694.
Body
Fat
(%)
Body Mass Index (kg/m2)0 10 30 40 6020 50
Women
Men
0
70
102030405060
BMI and Risk of Cardiovascular Mortality
Calle et al. NEJM 1999

10/16/2014
7
“the surgical treatment benefit with respect to cardiovascularevents was not related to baseline BMI or waist circumference”
“no significant relationships between weight change and cardiovascular events could be demonstrated”
“the surgical treatment benefit with respect to cardiovascularevents was not related to baseline BMI or waist circumference”
“no significant relationships between weight change and cardiovascular events could be demonstrated”
“Although weight loss in general is desirable for obese patients, the overweight condition by itself is not informative. Physicians need to know an individual patient’s risk factor profile before initiating therapy.”
10/16/2014
8
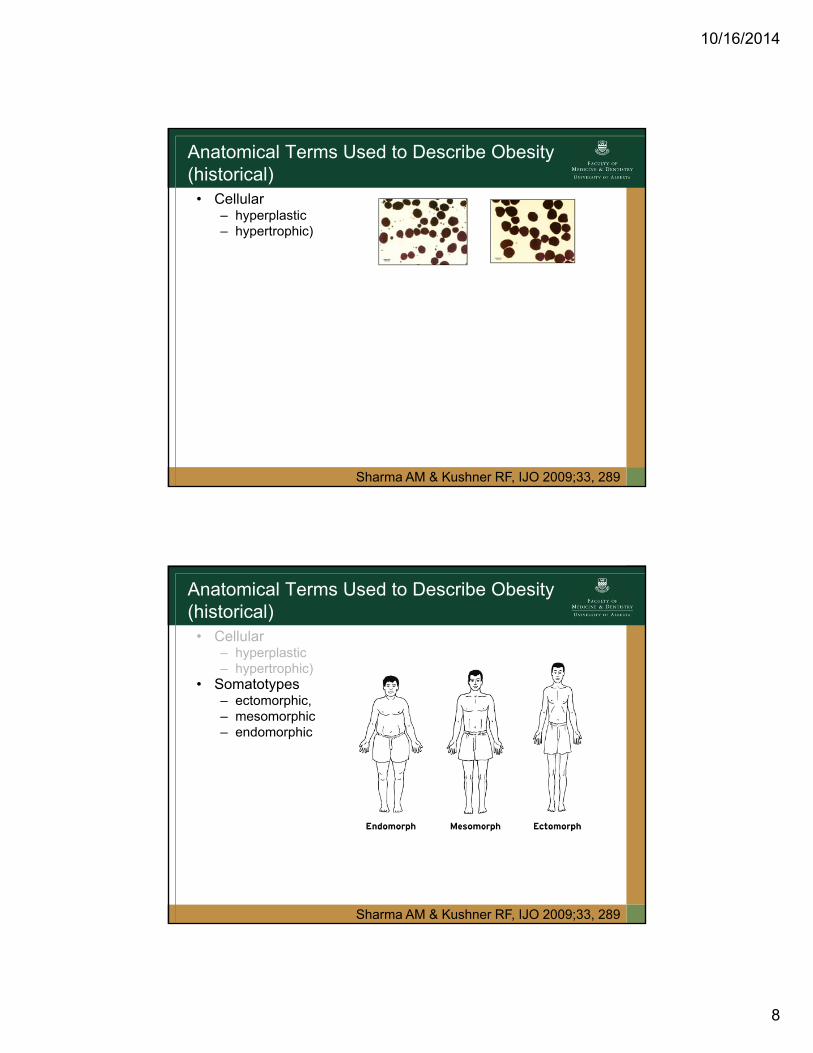
Anatomical Terms Used to Describe Obesity(historical)
• Cellular– hyperplastic– hypertrophic)
Sharma AM & Kushner RF, IJO 2009;33, 289
Anatomical Terms Used to Describe Obesity(historical)
• Cellular– hyperplastic– hypertrophic)
• Somatotypes– ectomorphic,– mesomorphic– endomorphic
Sharma AM & Kushner RF, IJO 2009;33, 289

10/16/2014
9
Anatomical Terms Used to Describe Obesity(historical)
• Cellular– hyperplastic– hypertrophic)
• Somatotypes– ectomorphic,– mesomorphic– endomorphic
• Body segment– central– peripheral
Sharma AM & Kushner RF, IJO 2009;33, 289
Anatomical Terms Used to Describe Obesity(historical)
• Cellular– hyperplastic– hypertrophic)
• Somatotypes– ectomorphic,– mesomorphic– endomorphic
• Body segment– central– peripheral
• Distribution pattern– android (male)– gynoid (female)
Sharma AM & Kushner RF, IJO 2009;33, 289

10/16/2014
10
Anatomical Terms Used to Describe Obesity(historical)
• Cellular– hyperplastic– hypertrophic)
• Somatotypes– ectomorphic,– mesomorphic– endomorphic
• Body segment– central– peripheral
• Distribution pattern– android– gynoid
• Depot– visceral– subcutaneous– ectopic (visceral, subcutaneous, ectopic))
Sharma AM & Kushner RF, IJO 2009;33, 289

10/16/2014
11
Edmonton Obesity Staging System (EOSS)
Stage 0
Sharma AM & Kushner RF, Int J Obes 2009
Stage 1
Stage 2
Stage 3
Stage 4
co-morbidity
moderate
moderate
Obesity

10/16/2014
12
EOSS Predicts Mortality in NHANES III
Padwal R, Sharma AM et al.
EOSS Predicts Mortality at Every Level of BMINHANES III
Padwal R, Sharma AM et al.
Overweight

10/16/2014
13
EOSS Distribution Across BMI CategoriesNHANES III (1988-1994)
Overweight
ClassIII
Padwal R, Sharma AM et al.
50 million
23 million
10 million
6 million

10/16/2014
14

10/16/2014
15
“Excess Weight” is Misleading, Confusing, and Difficult to Communicate
• “You are likely to lose X lbs”
(requires no additional information)
• “You are likely to lose X% of your body weight”
(requires understanding of percentages but can be easily translated into actual weight)
• “You are likely to lose X% of excess weight”
(requires understanding of percentages as well as the terms “excess” and “ideal” weight and cannot be easily translated into actual weight)

10/16/2014
16
“healthy” diet+
physical activity“healthy” weight≠
excess weight‘unhealthy’ diet
+undermoving≠

10/16/2014
17
Assumptions Underlying the Weight-Focused Paradigm of Obesity Management
• Adiposity poses significant mortality risk• Adiposity poses significant morbidity risk• Weight loss will prolong life• Anyone who is determined can lose weight and keep it off
through appropriate diet and exercise• The pursuit of weight loss is a practical and positive goal• The only way for overweight and obese people to improve
health is to lose weight• Obesity-related costs place a large burden on the
economy, and this can be corrected by focused attention to obesity treatment and prevention
Adapted from Bacon & Aphromar, Nutrition J, 2011
Health At Every Size (HAES)Intervention Paradigms
• Focus on health, not weight (“health promotion” not “obesity prevention”)
• Avoid weight-biased stigma• Consider physical, emotional, social, occupational,
intellectual, spiritual, and ecological aspects of health.• Promote self-esteem, body satisfaction, and respect for
body size diversity.• Physical activity and eating advise should use a
compassion-centered approach that encourages self-care rather than prescriptions.
• Weight is not a behavior and therefore not an appropriate target for behavior modification.
Adapted from Bacon & Aphromar, Nutrition J, 2011
DO NOT SET WEIGHT GOALS!

10/16/2014
18
Health At Every Size (HAES): Shifting the Paradigm from Weight to Health
• Encouraging Body Acceptance• Supporting Intuitive Eating• Supporting Active Embodiment
Adapted from Bacon & Aphromar, Nutrition J, 2011
Outcomes of HAES Approach vs. Weight-Centred Interventions
Evidence from six RCTs indicates that a HAES approach is associated with clinically relevant improvements in:• physiological measures (e.g. blood pressure, blood lipids),
health behaviors (e.g. physical activity, eating disorder pathology)
• psychosocial outcomes (e.g, mood, self-esteem, body image)
• self-esteem and eating behaviors.
Adapted from Bacon & Aphromar, Nutrition J, 2011

10/16/2014
19
Targeting Resources to Those Who Will Benefit Most
• A primary focus on ‘weight-loss’ irrespective of health status may not be the best use of limited resources, as long-term success of weight maintenance requires indefinite ongoing support and resources.
• In contrast, limiting weight-loss recommendations and treatments to those individuals most likely to benefit, helps channel limited resources to those patients, who need them most.
• It is likely that these benefits are more likely to be cost-effective in both the short- and long-term.
Best Weight:
Whatever weight someone can achieve and maintain while living the healthiest lifestyle they can truly enjoy.
Freedhoff & Sharma, 2009

10/16/2014
20
“Best Weight” as Treatment Target
• Weight targets (where indicated) should be guided by the concept of ‘Best Weight’, defined as the lowest weight a patient can sustain while still leading a life they enjoy.
• This concept is based on the notion that no one will sustain a lifestyle that is overly restrictive, significantly impairs quality of life or is unrealistic given their psychosocial and biomedical circumstances.
• Individuals will differ widely in what they consider a feasible and enjoyable lifestyle that they can sustain, which is why ‘Best Weight’ will differ between individuals and Program measures focus on quality of life and patient’s perceptions of programming value.
Best Weight

10/16/2014
21
www.DrSharma.ca










![arXiv:1503.05206v1 [astro-ph.GA] 17 Mar 2015for PG1211+143 had a wide angle outflow been directly measured, confirming a high mass-rate and mechanical energy in that case (Pounds](https://img.pdfslide.us/doc/110x75/5e90f5c15df08341ae246731/arxiv150305206v1-astro-phga-17-mar-2015-for-pg1211143-had-a-wide-angle-outiow.jpg)


















