Embed Size (px)
Citation preview

Risk factors influencing the outcome of peptic ulcerbleeding in end stage renal diseases after initialendoscopic haemostasis
S.-C. Lin,1 K.-L. Wu,1 K.-W. Chiu,1 C.-T. Lee,2 Y.-C. Chiu,1 Y.-P. Chou,1 M.-L. Hu,1 W.-C. Tai,1
S.-S. Chiou,1 T.-H. Hu,1 C.-S. Changchien,1 S.-K. Chuah1
Introduction
Taiwan is ranked as the top three nations in the
world in terms of the incidence of end-stage renal
disease (ESRD) with the rate of 384 per million pop-
ulations (1). It is definitely not something commend-
able but a threat to the health of the people in the
nation. The prevalence of peptic ulcer (PU) in
patients with ESRD is comparable with those in the
general population (2–5). Nevertheless they are asso-
ciated with more bleeding complications than those
in the general population (6). The major cause of
clinical bleeding among patients with CKD is upper
gastrointestinal bleeding (UGIB) and PU is the most
common cause (7). Patients with CKD are thought
to be associated with higher mortality because of PU
bleeding (8,9). In addition, renal insufficiency is a
predictor of mortality in validated UGIB scoring sys-
tems, such as Rockall score (10). However, improve-
ment in the outcomes of PU bleeding was observed
after the era of interventional endoscopic therapy
and high-dose acid suppression (11).
Reports on outcome studies of PU bleeding in
CKD patients after invasive endoscopic haemostasis
are limited. An interesting study conducted by Che-
ung and colleagues reported that the overall reblee-
ding rates were significantly higher in ESRD patients,
for both high and low-risk ulcers, but had similar in-
hospital mortality compared with those with normal
kidney function (12). However, enquiries regarding
the small sample size and patient selection bias were
made because ESRD patients in the study were
SUMMARY
Background and Aims: Patients suffering from peptic ulcer (PU) bleeding who
have end-stage renal disease (ESRD) may encounter more adverse outcomes. The
primary objective is to investigate the risk factors that influence the outcomes of
ESRD and chronic kidney disease (CKD) patients with PU bleeding after successful
initial endoscopic haemostasis. Methods: A total of 540 patients with PU bleed-
ing after initial endoscopic haemostasis in a tertiary hospital were investigated ret-
rospectively. They were sorted into three groups after randomised age-matched
adjustment: ESRD group (n = 90), CKD group (n = 90) and control group
(n = 360). Main outcome measurements were rebleeding, requirement for blood
transfusion and surgery, length of hospital stay and mortality. Results: The reblee-
ding rates were 43% for the ESRD group vs. 21% for the CKD group vs. 12% for
the control group (overall p = < 0.001). Multivariate analysis showed the predic-
tors of rebleeding were ESRD, time to endoscope, and non-high-dose proton-pump
inhibitors (PPI) users. The risk factors for bleeding-related mortality were presence
of moderate degree of CKD and ESRD group, time to endoscope, and Rockall
score. All-cause mortality was related to presence of moderate degree of CKD and
ESRD group, platelet count, time to endoscope, Rockall score and length of hospi-
tal stay. Conclusions: ESRD patients who suffered from PU bleeding were at risk
of excessive rebleeding and mortality with frequent occurrence of delayed reblee-
ding. This study suggests that early endoscopy for initial haemostasis and high-
dose intravenous PPI are associated with the reduction of rebleeding risk especially
in patients with high Rockall scores.
What’s known• PU bleeding is a major cause of UGI bleeding in
ESRD patients.
What’s new• Age-matched multivariate analysis revealed that
moderate degree of chronic kidney disease,
longer time needed to initiate endoscopic
treatment and non-high-dose PPI users were the
independent risks factor for PU rebleeding in
ESRD patients after initial endoscopic
haemostasis.
• ESRD patients who suffered from peptic ulcer
bleeding were at risk of excessive rebleeding and
mortality with frequent occurrence of delayed
rebleeding even at the earlier stage of the renal
disease. Early endoscope and high-dose
intravenous proton-pump inhibitors are associated
with the reduction of rebleeding risk especially in
the diseased patients with high Rockall score.
1Division of Hepato-
Gastroenterology, Department
of Internal Medicine, Kaohsiung
Chang Gung Memorial Hospital
and Chang Gung University
College of Medicine,
Kaohsiung, Taiwan2Division of Nephrology,
Department of Internal
Medicine, Kaohsiung Chang
Gung Memorial Hospital and
Chang Gung University College
of Medicine, Kaohsiung, Taiwan
Correspondence to:
Seng-Kee Chuah,
Division of
Hepatogastroenterology,
Department of Internal
Medicine, Chang Gang
Memorial Hospital, Kaohsiung
123, Ta-Pei Road, Niaosung,
Hsiang, Kaohsiung Country,
833, Taiwan
Tel.: 886 7 7317123, ext. 8301
Fax: 886 7 7322402
Email: [email protected]
Disclosures
All authors have no disclosure
of any financial involvement in
any organisation with a direct
financial interest in the subject
matter or materials discussed in
the manuscript.
OR IG INAL PAPER
ª 2012 Blackwell Publishing LtdInt J Clin Pract doi: 10.1111/j.1742-1241.2012.02974.x 1

associated with significantly more co-morbidities
which could be misleading in an outcome study.
Therefore, after randomised age-matching patients
with moderate CKD and normal kidney function to
the ESRD patients, we conducted this study to iden-
tify the risk factors that influence the outcomes of
ESRD patients with PU bleeding after initial endo-
scopic haemostasis.
Methods
PatientsFrom January 2008 to December 2010, medical
records of 903 patients with PU bleeding who
received initial successful endoscopic haemostasis
from a university-affiliated tertiary care center were
reviewed. We excluded 77 patients whose bleeding
was not PU-related, 4 patients with unsuccessful
endoscopic haemostasis and 113 patients with
incomplete chart records or insufficient follow-up
period (< 30 days) for reasons other than mortality.
Eventually, a total of 709 patients were entered for
age-matched analysis (Figure 1). Among them,
patients with ESRD were identified and classified as
ESRD group (n = 90). The remaining 239 CKD
patients and 380 normal renal function patients were
randomly age-matched to ESRD patients and subse-
quently sorted to CKD group (n = 90) and control
group (n = 360).
Patient’s baseline characteristics, concomitant co-
morbid diseases (including cardiovascular diseases,
stroke, liver cirrhosis, chronic obstructive pulmonary
disease, diabetes mellitus, and hypertension), present-
ing haemoglobin levels, platelet counts, haemody-
namic status, use of aspirin, non-steroidal anti-
inflammatory drugs (NSAIDs), warfarin ⁄ heparin and
proton-pump inhibitor (PPI) prior to endoscopic
therapy, were recorded using a predetermined
spreadsheet. PU bleeding was defined by endoscop-
ist’s diagnosis combined with no other identifiable
bleeding cause. Endoscopic findings such as ulcer
locations, sizes, difficult treatment sites (lesser curva-
ture of high body; posterior wall of bulb and supe-
rior duodenal angle), Forrest grade, Rockall scores
and treatment methods were also recorded. Patients
who were followed for 30 days after initial endo-
scopic haemostasis were enrolled and analysed. The
end-points were rebleeding within 30 days after ini-
tial endoscopic haemostasis, requirement for surgical
intervention, length of hospital stay and total
amount of blood transfusion required, bleeding–
related mortality and all-cause mortality. This study
was approved in accordance with the principles of
Helsinki, by both the Institutional Review Board and
the Ethics Committee of Chang Gung Memorial
Hospital, Taiwan (IRB 100-2140B).
DefinitionsCKD group referred to non-dialysis dependent
patients with an estimated glomerular filtration rate
< 60 ml ⁄ min for ‡ 3 months calculated using the 4-
variable Modification of Diet in Renal Disease Study
equation (13). ESRD group referred to patients who
were on maintenance haemodialysis or peritoneal
dialysis for more than 6 months (12). Patients on
maintenance haemodialysis received three sessions
per week, and 4 hours for each session. All haemodi-
alyzers contained semisynthetic materials, and hae-
modialysis therapy was performed with a
bicarbonate-based dialysate. It is the policy of our
hospital to use non-heparin haemodialysis protocol
in patients suffering from active gastrointestinal
bleeding (including those who have received endo-
scopic haemostasis). Subjects with normal baseline
kidney function (estimated GFR > 60 ml ⁄ min) were
considered as the control group. The non-high-dose
PPI treatment referred to those patients who received
80 mg PPI bolus and followed by intravenous 80 mg
per day, until alimentation was possible, then 40 mg
per day orally. High-dose PPI treatment patients
received 80 mg PPI intravenous bolus injection, then
8 mg per hour continuous infusion for 3 days, fol-
lowed by intravenous 80 mg PPI per day (11). High-
risk ulcers are defined as Forrest grade higher or
equal to 2b (12).
Rebleeding was defined as new onset of haemate-
mesis, coffee-ground vomitus, or haematochezia,
with an increasing pulse rate more than 110 beats ⁄ -min and decreasing blood pressure below 90 mmHg
Figure 1 Schematic flowchart of the study design and the patient numbers during
follow up
2 Peptic ulcer bleeding in end-stage renal disease
ª 2012 Blackwell Publishing LtdInt J Clin Pract
after a 24 h period of stable vital signs and haemato-
crit following endoscopic treatment (14,15). Delay
rebleeding referred to those patients who rebled only
after 7 days of enrollment. Total amount of blood
transfusion required was defined as units given to
the patients between the time PU bleeding occurred
and the day of discharge. Bleeding-related mortality
was defined as in-hospital death resulted solely from
peptic ulcer bleeding.
Statistical analysisComparisons of continuous variables were conducted
by using one-way analysis of variance (ANOVA) with
multiple comparisons being corrected by using Bon-
ferroni’s method. Categorical variables were com-
pared using the Pearson’s v2 test. A two-tailed
significance value of .05 was used. Logistic regression
analysis was used for analysis of rebleeding and mor-
tality rates including the following covariates: group,
age, shock, use of aspirin, NSAIDs, clopidogrel, war-
farin ⁄ heparin, co-morbidity, multiple ulcers, difficult
site, combination therapy modality vs. monotherapy,
high risk ulcer stigmata (>Forrest 2b), time to endo-
scopic treatment, Rockall score, high-dose and non-
high dose PPI users. The cumulative probability of
no rebleeding was calculated with the Kaplan–Meier
method, and probabilities were compared using the
log-rank test. All statistical analyses were performed
using PASW statistics software, version 18 (IBM Co.,
Somers, NY).
Results
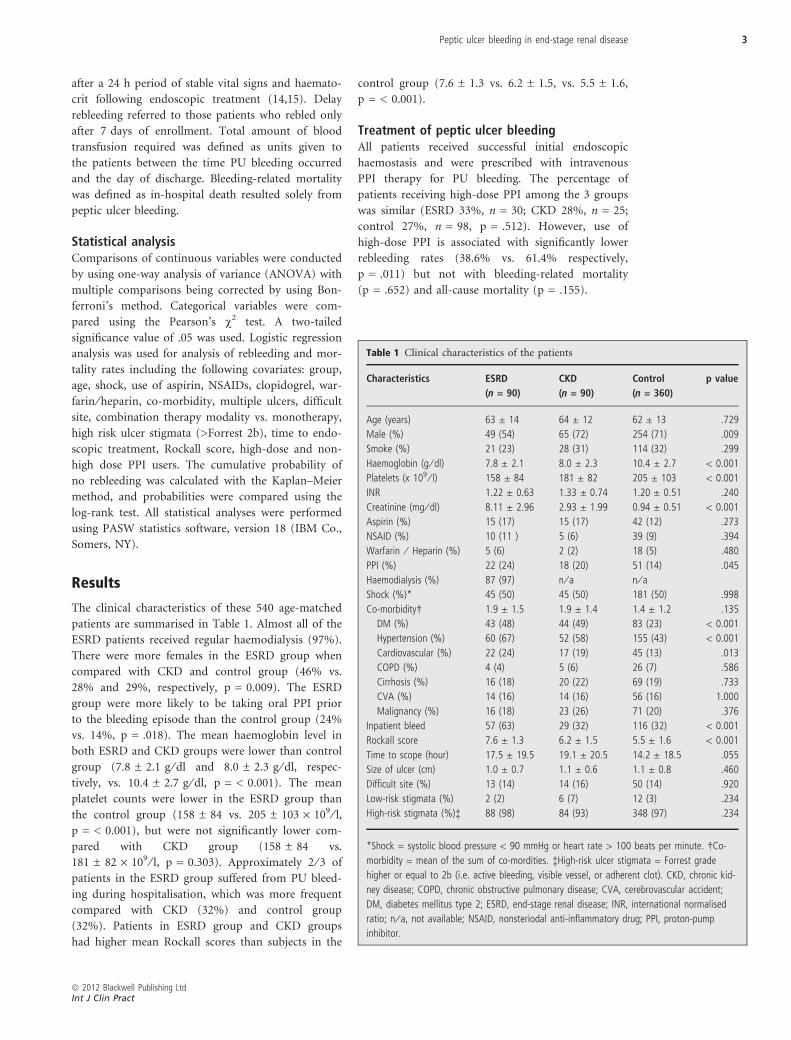
The clinical characteristics of these 540 age-matched
patients are summarised in Table 1. Almost all of the
ESRD patients received regular haemodialysis (97%).
There were more females in the ESRD group when
compared with CKD and control group (46% vs.
28% and 29%, respectively, p = 0.009). The ESRD
group were more likely to be taking oral PPI prior
to the bleeding episode than the control group (24%
vs. 14%, p = .018). The mean haemoglobin level in
both ESRD and CKD groups were lower than control
group (7.8 ± 2.1 g ⁄ dl and 8.0 ± 2.3 g ⁄ dl, respec-
tively, vs. 10.4 ± 2.7 g ⁄ dl, p = < 0.001). The mean
platelet counts were lower in the ESRD group than
the control group (158 ± 84 vs. 205 ± 103 · 109 ⁄ l,p = < 0.001), but were not significantly lower com-
pared with CKD group (158 ± 84 vs.
181 ± 82 · 109 ⁄ l, p = 0.303). Approximately 2 ⁄ 3 of
patients in the ESRD group suffered from PU bleed-
ing during hospitalisation, which was more frequent
compared with CKD (32%) and control group
(32%). Patients in ESRD group and CKD groups
had higher mean Rockall scores than subjects in the
control group (7.6 ± 1.3 vs. 6.2 ± 1.5, vs. 5.5 ± 1.6,
p = < 0.001).
Treatment of peptic ulcer bleedingAll patients received successful initial endoscopic
haemostasis and were prescribed with intravenous
PPI therapy for PU bleeding. The percentage of
patients receiving high-dose PPI among the 3 groups
was similar (ESRD 33%, n = 30; CKD 28%, n = 25;
control 27%, n = 98, p = .512). However, use of
high-dose PPI is associated with significantly lower
rebleeding rates (38.6% vs. 61.4% respectively,
p = .011) but not with bleeding-related mortality
(p = .652) and all-cause mortality (p = .155).
Table 1 Clinical characteristics of the patients
Characteristics ESRD
(n = 90)
CKD
(n = 90)
Control
(n = 360)
p value
Age (years) 63 ± 14 64 ± 12 62 ± 13 .729
Male (%) 49 (54) 65 (72) 254 (71) .009
Smoke (%) 21 (23) 28 (31) 114 (32) .299
Haemoglobin (g ⁄ dl) 7.8 ± 2.1 8.0 ± 2.3 10.4 ± 2.7 < 0.001
Platelets (x 109 ⁄ l) 158 ± 84 181 ± 82 205 ± 103 < 0.001
INR 1.22 ± 0.63 1.33 ± 0.74 1.20 ± 0.51 .240
Creatinine (mg ⁄ dl) 8.11 ± 2.96 2.93 ± 1.99 0.94 ± 0.51 < 0.001
Aspirin (%) 15 (17) 15 (17) 42 (12) .273
NSAID (%) 10 (11 ) 5 (6) 39 (9) .394
Warfarin ⁄ Heparin (%) 5 (6) 2 (2) 18 (5) .480
PPI (%) 22 (24) 18 (20) 51 (14) .045
Haemodialysis (%) 87 (97) n ⁄ a n ⁄ aShock (%)* 45 (50) 45 (50) 181 (50) .998
Co-morbidity� 1.9 ± 1.5 1.9 ± 1.4 1.4 ± 1.2 .135
DM (%) 43 (48) 44 (49) 83 (23) < 0.001
Hypertension (%) 60 (67) 52 (58) 155 (43) < 0.001
Cardiovascular (%) 22 (24) 17 (19) 45 (13) .013
COPD (%) 4 (4) 5 (6) 26 (7) .586
Cirrhosis (%) 16 (18) 20 (22) 69 (19) .733
CVA (%) 14 (16) 14 (16) 56 (16) 1.000
Malignancy (%) 16 (18) 23 (26) 71 (20) .376
Inpatient bleed 57 (63) 29 (32) 116 (32) < 0.001
Rockall score 7.6 ± 1.3 6.2 ± 1.5 5.5 ± 1.6 < 0.001
Time to scope (hour) 17.5 ± 19.5 19.1 ± 20.5 14.2 ± 18.5 .055
Size of ulcer (cm) 1.0 ± 0.7 1.1 ± 0.6 1.1 ± 0.8 .460
Difficult site (%) 13 (14) 14 (16) 50 (14) .920
Low-risk stigmata (%) 2 (2) 6 (7) 12 (3) .234
High-risk stigmata (%)� 88 (98) 84 (93) 348 (97) .234
*Shock = systolic blood pressure < 90 mmHg or heart rate > 100 beats per minute. �Co-
morbidity = mean of the sum of co-mordities. �High-risk ulcer stigmata = Forrest grade
higher or equal to 2b (i.e. active bleeding, visible vessel, or adherent clot). CKD, chronic kid-
ney disease; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident;
DM, diabetes mellitus type 2; ESRD, end-stage renal disease; INR, international normalised
ratio; n ⁄ a, not available; NSAID, nonsteriodal anti-inflammatory drug; PPI, proton-pump
inhibitor.
Peptic ulcer bleeding in end-stage renal disease 3
ª 2012 Blackwell Publishing LtdInt J Clin Pract

Outcomes
RebleedingAfter initial successful endoscopic treatment, a total
of 101 patients (19%) suffered from recurrent bleed-
ing in the current study. The overall rebleeding rates
were 43% (n = 39) for the ESRD group, 21%
(n = 19), for the CKD group, and 12% (n = 43) for
the control group (overall p = < 0.001). Further-
more, more dialysis-dependent ESRD patients rebled
than CKD group (p = .001). Likewise, more patients
in the CKD group encountered recurrent bleeding
compared with the control group (p = .024). Ninety-
seven percent (n = 98) of the rebleeding ulcers
belonged to high-risk ulcers and only 3% were low-
risk ulcers. Among patients with high-risk ulcer stig-
mata, the rebleeding rates were 44% (n = 39) for
ESRD, 21% (n = 18) for CKD and 12% (n = 41) for
control group respectively (overall p < 0.001). Three
of the twenty patients with low risk ulcers rebled.
One was from the CKD group and two were from
the control group. Overall, the cumulative probabil-
ity of rebleeding was significantly greater in the
ESRD group than the CKD group (p = .001) and
control group (p < .001). In addition, the cumulative
probability for rebleeding was also significantly
greater in the CKD group when compared with con-
trol group (p = .028) (Figure 2).
The average time interval from initial haemostasis
to rebleeding was significantly different among the
ESRD, CKD and control groups (5.4 ± 5.6 days vs.
6.0 ± 6.7 days vs.2.9 ± 2.3 days, p = .048). In the
ESRD group, 43.6% (n = 17) of the rebleeding
occurred within 3 days, 35.9% (n = 14) between 4
and 7 days later, and 20.5% (n = 8) between 8 and
30 days. In the CKD group, 42.1% (n = 8) of the
rebleeding occurred within 3 days, 31.6% (n = 6)
between 4 and 7 days later, and 26.3% (n = 5)
between 8 and 30 days. In the control group, 69.8%
(n = 30) of the rebleeding occurred within 3 days of
the first bleed, 27.9% (n = 12) between 4 and 7 days,
and 2.3% (n = 1) between 8 and 30 days. The
delayed rebleeding rates were higher in ESRD and
CKD group compared with the control group (20.5
vs. 2.3%, p = .009 and 26.3 vs. 2.3%, p = .003,
respectively). No difference was observed between
the ESRD and CKD groups in terms of delayed reb-
leeding (p = .619).
On multivariate regression analysis, significant pre-
dictors for rebleeding were ESRD, time to endo-
scopic treatment and non-high-dose PPI users
(Table 2). Patients with ESRD had a higher reblee-
ding rates than CKD group (OR: 2.9, 95% CI, 1.5–
5.5, p = .002) and control group (OR: 5.6, 95% CI,
3.3–9.5, p < 0.001) (Table 3). CKD group rebled
more frequently than control group on univariate
analysis (OR 2.0; 95% CI, 1.1–3.6; p = .026), but it
was not a significant predictor on multivariate
regression analysis (p = .303).
Need for blood transfusions.The total blood transfusion (units of packed RBCs)
requirements were significantly greater in the ESRD
group (9.3 ± 14.7 units) than the control group
(4.8 ± 7.2 units; p < .001) but no difference was
observed between the CKD group and ESRD group
(p = .438) (Figure 3).
Length of hospital stayThe length of hospital stay was significantly longer for
the ESRD group when compared with the CKD group
and with the control group (33.3 ± 56.5 days vs.16.6 ±
21.1 days vs.12.5 ± 15.7 days, p < 0.001) (Figure 3).
Figure 2 Kaplan–Meier estimate of cumulative probability of no rebleeding among
the three groups. The cumulative probability of rebleeding was significantly greater in
the ESRD group when compared with the CKD group (p = .001) and control group
(p < .001). Furthermore, cumulative probability for rebleeding is also significantly
greater in the CKD group compared with control group (p = .028)
Table 2 Predictors of peptic ulcer rebleeding on
multivariate analysis
Predictors Comparison OR 95% CI p value
ESRD Control 5.6 3.3–9.5 < .001
ESRD CKD 2.9 1.5–5.5 .001
Time to scope per 1 hour
increase
1.02 1.002–1.032 .028
Non-high-dose
PPI
High-dose PPI 2.25 1.054–4.797 .036
CI, confidence interval; CKD, chronic kidney disease; ESRD,
end-stage renal disease; OR, odds ratio; PPI, proton pump
inhibitor. Time to scope = time taken to initiate endoscopic
therapy in hours.
4 Peptic ulcer bleeding in end-stage renal disease
ª 2012 Blackwell Publishing LtdInt J Clin Pract

Surgical interventionThe requirement for surgical intervention in the
ESRD group was slightly higher (4.4%, n = 4) than
the CKD group (2.2%, n = 2) and the control group
(2.5%, n = 9) but was not statistically different when
compared with each other (Figure 3).
Bleeding-related mortalityThe mortality rates related to PU bleeding for the
ESRD and CKD group were both higher than the
control group (6.8% vs. 0.9%, p = .001 and 5.1% vs.
0.9%, p = .009). The cumulative probability of
bleeding related mortality was also significantly
greater in the ESRD and CKD group than control
group (p = .028 and p = .024, respectively) (Fig-
ure 4). On multivariate regression analysis, predictors
for bleeding-related mortality were presence of CKD,
including patients from both CKD and ESRD
groups, as defined in current study (OR, 12.63, 95%
CI, 1.080–147.693), Rockall scores (OR, 2.42, 95%
CI, 1.206–4.868), and time to endoscopic treatment
(OR, 1.04, 95% CI, 1.012–1.073) (Table 3).
All-cause mortalityThe all-cause mortality rates for the ESRD and CKD
group were both higher than the control group
(23.3% vs. 6.9%, p < .001 and 16.7% vs. 6.9%,
p = .004). A trend of significant difference was
observed from the cumulative probability of all-cause
mortality in the ESRD and CKD group when com-
pared with control group (p = .071 and p = .080,
respectively) (Figure 5). Multivariate analysis showed
that all-cause mortality was related to presence of
CKD, including both CKD and ESRD groups (OR,
1.99, 95% CI,1.006–3.945), platelet count (OR, 1.01,
Table 3 Predictors of bleeding related mortality and all-cause mortality on multivariate analysis
Predictors Comparison OR 95% CI p value
Bleeding relate mortality
Chronic kidney disease (ESRD + CKD) Normal 12.63 1.080–147.693 .043
Time to scope Per 1 h increase 1.04 1.012–1.073 .006
Rockall score Per score increase 2.42 1.206–4.868 .013
All-cause mortality
Chronic kidney disease (ESRD + CKD) Normal 1.99 1.006–3.945 .048
Platelet Per 1 · 109 ⁄ l decrease 1.01 1.003–1.012 .001
Time to scope Per 1 h increase 1.02 1.006–1.034 .005
Rockall score Per score increase 1.44 1.132–1.834 .003
Length of hospital stay Per 1 day increase 1.04 1.004–1.070 .026
CI, confidence interval; CKD, chronic kidney disease; ESRD, end-stage renal disease; OR, odds ratio. Time to scope = time taken to initiate endoscopic therapy in
hours.
Figure 3 Differences in requirements for surgery
(p = .568), blood transfusion (p < .001 between ESRD and
normal) and lengths of stay (p < .001 between ESRD and
normal) among the three groups
Figure 4 Kaplan–Meier estimate of cumulative probability of no bleeding-related
mortality among the 3 groups. The cumulative probability of bleeding-related
mortality was significantly greater in the ESRD and CKD group when compared with
the control group (p = .028 and p = .024, respectively)
Peptic ulcer bleeding in end-stage renal disease 5
ª 2012 Blackwell Publishing LtdInt J Clin Pract

95% CI, 1.003–1.012), time to endoscope (OR, 1.02,
95% CI, 1.006–1.034), Rockall score (OR, 1.44, 95%
CI, 1.132–1.834) and length of hospital stay (OR,
1.04, 95% CI, 1.004–1.070) (Table 3).
Discussion
After randomised age-matched adjustment, current
study observed that more patients from the ESRD
and CKD group rebled than the control group after
initial endoscopic haemostasis as expected. However,
more delayed rebleeding was also observed in both
of the diseased groups. The predictors of rebleeding
were ESRD, time to endoscope, and non-high-dose
PPI users. The risk factors for bleeding related mor-
tality were presence of CKD, time to endoscope, and
higher Rockall scores. All-cause mortality was related
to presence of CKD, platelet count, time to endo-
scope, Rockall score and length of hospital stay.
In general, the risk of PU bleeding in dialysis
dependent patients is higher than those in the gen-
eral population (6). The mechanism for the excessive
bleeding in patients with ESRD is still unclear but
may be multifactorial (16). Platelet dysfunction in
the form of impaired platelet adhesiveness and
altered platelet-vessel-wall interaction is believed to
have played an important role (17–22). Cheung et al.
found that rebleeding rates were significantly higher
in the ESRD group for patients with both high and
low-risk ulcer stigmata on endoscopy implying that
all dialysis-dependent patients with PU bleeding need
to be managed as high-risk patients. However, exclu-
sion of patients with acute kidney injury (AKI)
requiring dialysis from the control group might arti-
ficially eliminate severe bleeders. Similarly, inclusion
of patients with significantly more existing co-mor-
bidities in the ESRD group than patients in the con-
trol group might contribute to the high rebleeding
rate in the ESRD group. Therefore, current study
randomly aged-matched patients with moderate
CKD and normal kidney function to ESRD patients
as defined earlier, so that patients with AKI were not
excluded from the normal group (n = 16, according
to the AKIN criteria), consequently making the dif-
ference in co-morbidities statistically insignificant
among the groups (p = .135) after the adjustment
process. All of our enrolled patients suffering from
PU bleeding attained initial successful endoscopic
therapy. It is rational that ESRD patients had a sig-
nificantly high rebleeding rate after initial endoscopic
haemostasis for ulcers with high-risk stigmata (44%)
but the difference was not significant with low-risk
ulcers among the three groups in current study
(p = .822). A trend of increase in rebleeding rate was
observed as the renal function deteriorated in current
study which was not observed in Cheung’s study.
(ESRD vs. CKD, p = .001; CKD vs. control,
p = .024).
Frequent occurrence of the delayed rebleeding in
ESRD and CKD patients was observed. Usually, the
fading time of non-bleeding visible vessel is
approximately 3–6 days and it is rational that recur-
rent bleeding occurs within 3 days (23,24). Cheng
and colleagues reported that co-morbidities influence
the rates of recurrent bleeding (25). Recurrent bleed-
ing may be prolonged in those with co-morbidities
(26). The pathogenic cause remains unclear for this
delay in PU bleeding. Some investigators speculate
that it may be a result of poor nutritional status,
ischaemic change of the GI tract and platelet
dysfunction (17,18,27). Therefore, more careful and
prolonged monitoring for patients in this diseased
entity is important in clinical practice. In addition,
the presence of CKD, regardless of dialysis
requirement, as an independent predictor of both
bleeding-related mortality and all-cause mortality in
current study may imply renal function impairment
could be associated with the risk of mortality in
bleeding PU patients even at the earlier stage of the
renal disease.
Delay in time to endoscope was also an important
risk factor of rebleeding, bleeding-related mortality
and all-cause mortality. This is consistent with the
current updated consensus suggesting for early endo-
scopic management of PU bleeding within 24 h of
presentation (11). Rockall scores were higher for the
groups with renal impairment and was a significant
predictor of mortality. The bottom line is that
patients with higher scores should always be treated
more intensively not to mention those with concom-
itant co-morbidities like CKD and ESRD.
Figure 5 Kaplan–Meier estimate of cumulative probability of no all-cause mortality
among the three groups. A trend of significant difference was observed from the
cumulative probability of all-cause mortality in the ESRD and CKD group when
compared with control group (p = .071 and p = .080, respectively)
6 Peptic ulcer bleeding in end-stage renal disease
ª 2012 Blackwell Publishing LtdInt J Clin Pract

Current study also observed that non-high-dose
PPI user was one of the predictors for PU rebleeding
in ESRD. PPIs are mainly metabolised by the path-
way of cytochrome P450 system (CYP) (28). There
are more Caucasians than Asians who belong to
homozygous extensive metabolizer (EM) in the dis-
tribution of genetic polymorphisms of CYP which
may influence the outcome of the effect of PPI
(29,30). Therefore, the effect to maintain intragastric
pH > 6.0 in the EM patients with intravenous pan-
toprazole is inferior to the non-EM patients owing
to the lower plasma concentration (31). Despite con-
troversies on the optimal dosing of PPI in preventing
PU rebleeding, high dose intravenous PPI should be
prescribed for PU bleeding in ESRD (32–34).
This study encounters several limitations. First,
this is a retrospective chart review study. Second, a
significantly higher proportion of ESRD patients
were hospitalised before PU bleeding as compared
with the CKD and control group. We performed
multivariate regression analysis to determine whether
inpatient bleeding was an independent predictor of
adverse outcomes as opposed to severity of the kid-
ney disease but failed to detect any effect. Third,
longer hospital stay in the ESRD group (33 days) as
compared with CKD group (17 days) and control
group (13 days) were probably relevant to the higher
proportion of inpatient bleeding in the ESRD group
enrolled in current study. Fourth, the requirements
for blood transfusion were initially higher for the
patients in the ESRD and CKD groups may be due
partly to the chronic anaemia caused by the kidney
disease itself. Finally, whilst the overall levels of com-
orbidity are apparently the same for the groups in
comparison, diabetes, hypertension and cardiovascu-
lar disease are more common in the renal failure
groups and the presence of these diseases might
adversely affected the outcomes of peptic ulcer bleed-
ing. Given that diabetes and hypertension are the
two most common causes of chronic kidney disease
(making up 33% and 21% of adult CKD, respec-
tively) (13), it could be expected that these diseases
were more common in renal failure groups owing to
disease entity. From the multivariate regression anal-
yses performed, we were unable to demonstrate that
the presence of diabetes, hypertension and cardiovas-
cular diseases were independent predictors of reblee-
ding, bleeding-related mortality and all-cause
mortality.
In conclusion, ESRD patients who suffered from
PUD bleeding were at risk of excessive rebleeding
and mortality with frequent occurrence of delayed
rebleeding. Renal function impairment could be
associated with the risk of rebleeding and mortality
in bleeding PU patients even at the earlier stage of
the renal disease. Despite the debates on the issue of
optimal PPI dosing for patients with bleeding ulcers
among general population, current study suggests
that an early endoscopy for initial haemostasis and
high-dose intravenous PPI are associated with the
reduction of rebleeding risk among ESRD patients
who suffered from PU bleeding especially those with
high Rockall scores.
Acknowledgements
None
Authors’ contributions
S-CL wrote and drafted the article. S-KC is responsible
for the conception and design of the study, critical
revision of the article for important intellectual con-
tent and final approval of the article. K-LW, K-WC,
Y-CC, C-TL, DM-LH, W-CT and T-HH are involved
in the analysis and interpretation of the data.
References
1 United States Renal Data System, Annual Data
Report 2011. Available at http://www.usrds.org/
1adr.htm. Last assessed date May 26th, 2012
2 Milito G, Taccone-Gallucci M, Brancaleone C et al.
The gastrointestinal tract in uremic patients on long-
term hemodialysis. Kidney Int 1985; 28(Suppl. 17):
S157–60.
3 Andrulli A, Malfi B, Recchia S, Ponti F, Triolo G,
Segoloni G. Patients with chronic renal failure are
not at a risk of developing chronic peptic ulcers.
Clin Nephrol 1985; 23: 245–8.
4 Ala-Kaila K. Upper gastrointestinal findings in
chronic renal failure. Scand J Gastroenterol 1987; 22:
372–6.
5 Wee A, Kang JY, Ho MS, Choong HL, Wu AY,
Sutherland IH. Gastroduodenal mucosa in uraemia:
endoscopic and histological correlation and preva-
lence of Helicobacter-like organisms. Gut 1990; 31:
1093–6.
6 Kang JY, Ho KY, Yeoh KG et al. Peptic ulcer and
gastritis in uraemia, with particular reference to the
effect of Helicobacter pylori infection. J Gastroenter-
ol Hepatol 1999; 14: 771–8.
7 Chalasani N, Cotsonis G, Wilcox CM. Upper gas-
trointestinal bleeding in patients with chronic renal
failure: role of vascular ectasia. Am J Gastroentero
1996; 91: 2329–32.
8 Silvertstein FE, Gilbert DA, Tedesco FJ, Buenger
NK, Persing J. The national ASGE survey on
upper gastrointestinal bleeding. II. Clinical
prognostic factors. Gastrointest Endosc 1981; 27:
80–93.
9 Branicki FJ, Boey J, Fok PJ et al. Bleeding duodenal
ulcer. A prospective evaluation of risk factors
for rebleeding and death. Ann Surg 1990; 211: 411–
8.
10 Rockall TA, Logan RF, Devlin HB, Northfield TC.
Risk assessment after acute upper gastrointestinal
haemorrhage. Gut 1996; 38: 316–21.
11 Barkun AN, Bardou M, Kuipers EJ et al. Interna-
tional Consensus Upper Gastrointestinal Bleeding
Conference Group: International consensus recom-
mendations on the management of patients with
nonvariceal upper gastrointestinal bleeding. Ann
Intern Med 2010; 152: 101–3.
12 Cheung J, Yu A, LaBossiere J, Zhu Q, Fedorak RN.
Peptic ulcer bleeding outcomes adversely affected
by end-stage renal disease. Gastrointest Endosc 2010;
71: 44–9.
13 National Kidney Foundation. K ⁄ DOQI Clinical
Practice Guidelines for Chronic Kidney Disease:
Evaluation, Classification and Stratification. Am J
Kidney Dis 2002; 39(2 Suppl 1): S1–266.
14 Xu WH, Wang JH, Tsai MS et al. The effects of ce-
fazolin on cirrhotic patients with acute variceal
Peptic ulcer bleeding in end-stage renal disease 7
ª 2012 Blackwell Publishing LtdInt J Clin Pract

hemorrhage after endoscopic interventions. Surg
Endosc 2011; 25: 2911–8.
15 Hu ML, Wu KL, Chiu KW et al. Predictors of reb-
leeding after initial hemostasis with epinephrine
injection in high-risk ulcers. World J Gastroenterol
2010; 16: 5490–5.
16 Toke AB. GI bleeding risk in patients undergoing
dialysis. Gastrointest Endosc 2010; 71: 50–2.
17 Boccardo P, Remuzzi G, Galbursera M. Platelet dys-
function in renal failure. Semin Thromb Hemost
2004; 30: 579–89.
18 Galbusera M, Remuzzi G, Boccardo P. Treatment
of bleeding in dialysis patients. Semin Dial 2009;
22: 279–86.
19 Sreedhara R, Itagaki I, Lynn B, Hakim RM. Defec-
tive platelet aggregation in uremia is transiently
worsened by hemodialysis. Am J Kidney Dis 1995;
25: 555–63.
20 Remuzzi G, Benigni A, Dodesini P et al. Platelet
function in patients on maintenance hemodialysis:
depressed or enhanced? Clin Nephrol 1982; 17: 60–3.
21 Remuzzi G, Livio E, Marchiaro G. Altered platelet
function in chronic uraemia only partially corrected
by hemodialysis. Nephron 1987; 22: 347–53.
22 Pepper RJ, Gale DP, Wajed J et al. Inadvertent
postdialysis anticoagulation due to heparin line
locks. Hemodial Int 2007; 11: 430–4.
23 Yang CC, Shin JS, Lin XZ, Hsu PI, Chen KW, Lin
CY. The natural history (fading time) of stigmata
of recent hemorrhage in peptic ulcer disease. Gas-
trointest Endosc 1994; 40: 562–6.
24 Lin HJ, Perng CL, Lee YL, Lee CH, Lee SD. Clinical
courses and predictors for rebleeding in patients
with peptic ulcers and non-bleeding visible vessels:
a prospective study. Gut 1994; 35: 1389–93.
25 Cheng HC, Sheu BS. Intravenous proton pump
inhibitors for peptic ulcer bleeding: clinical benefits
and limits. World J Gastrointest Endosc 2011; 3: 49–
56.
26 Cheng HC, Chang WL, Yeh YC, Chen WY, Tsai
YC, Sheu BS. Seven-day intravenous low-dose
omeprazole infusion reduces peptic ulcer rebleeding
for patients with comorbidities. Gastrointest Endosc
2009; 70: 433–9.
27 Tseng GY, Fang CT, Lin HJ, Yang HB, Tseng GC,
Wang PC. Efficacy of an intravenous proton pump
inhibitor after endoscopic therapy with epinephrine
injection for peptic ulcer bleeding in patients with
uraemia: a case-control study. Aliment Pharmacol
Ther 2009; 30: 406–13.
28 Kang JM, Kim N, Lee DH et al. Effect of the
CYP2C19 polymorphism on the eradication rate of
Helicobacter pylori infection by 7-day triple therapy
with regular proton pump inhibitor dosage. J Gas-
troenterol Hepatol 2008; 23: 1287–91.
29 Furuta T, Shirai N, Sugimoto M, Nakamura A,
Hishida A, Ishizaki T. Influence of CYP2C19 phar-
macogenetic polymorphism on proton pump inhib-
itor-based therapies. Drug Metab Pharmacokinet
2005; 20: 153–67.
30 Lim PW, Goh KL, Wong BC. CYP2C19 genotype
and the PPIs – focus on rabeprazole. J Gastroenterol
Hepatol 2005; 20(Suppl): S22–8.
31 Oh JH, Choi MG, Dong MS et al. Low-dose intra-
venous pantoprazole for optimal inhibition of gas-
tric acid in Korean patients. J Gastroenterol Hepatol
2007; 22: 1429–34.
32 Andriulli A, Loperfido S, Focareta R et al. High-
versus low-dose proton pump inhibitors after endo-
scopic hemostasis in patients with peptic ulcer
bleeding: a multicentre, randomized study. Am J
Gastroenterol 2008; 103: 3011–8.
33 Cheng HC, Kao AW, Chuang CH, Sheu BS. The
efficacy of high- and low-dose intravenous omepra-
zole in preventing rebleeding for patients with
bleeding peptic ulcers and comorbid illnesses. Dig
Dis Sci 2005; 50: 1194–201.
34 Simon-Rudler M, Massard J, Bernard-Chabert B
et al. Continuous infusion of high-dose omeprazole
is more effective than standard-dose omeprazole in
patients with high-risk peptic ulcer bleeding: a ret-
rospective study. Aliment Pharmacol Ther 2007; 25:
949–54.
Paper received November 2011, accepted May 2012
8 Peptic ulcer bleeding in end-stage renal disease
ª 2012 Blackwell Publishing LtdInt J Clin Pract