Embed Size (px)
DESCRIPTION
Peptic ulcer disease
Citation preview

Peptic ulcer disease
VyshyvanyukVyshyvanyukVira YuriivnaVira Yuriivna
Chair of internal medicine #1 with course Chair of internal medicine #1 with course of clinical immunology and allergologyof clinical immunology and allergology
Ivano-Frankivsk national medical university
Peptic ulcer disease is chronic poliethiologic disease of the stomach or duodenum, the main sign of which is an chronic excoriated segment (ulcer defect) on gastro-intestinal mucosa
About 10% of the population in different countries are suffered this disease
DefinitionDefinition
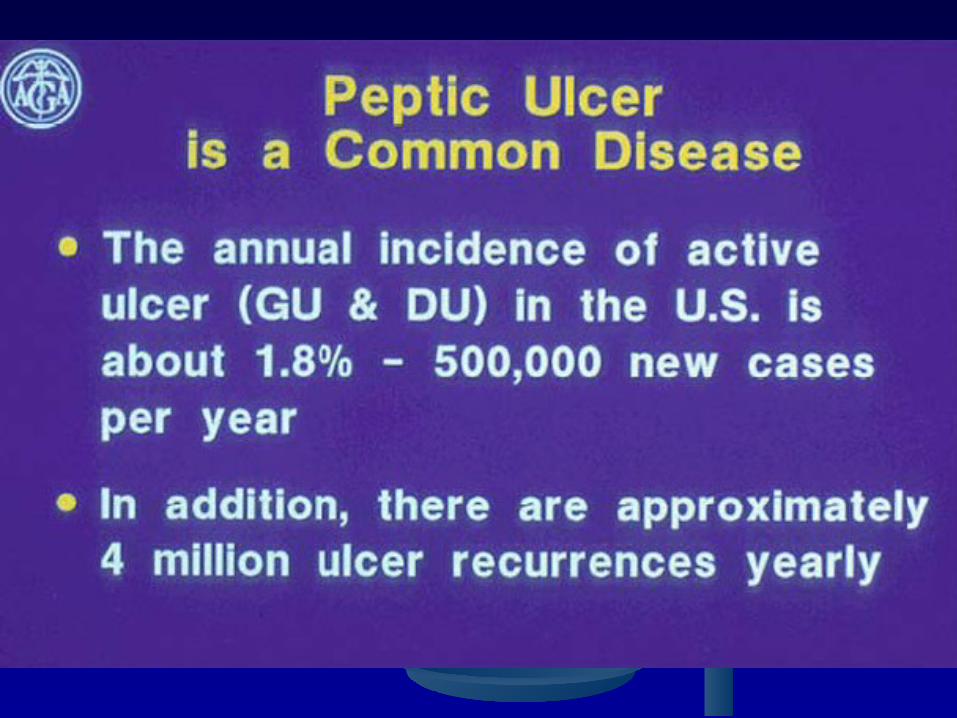
. Prevalence and Incidence of Peptic Ulcer
DU most common in Europe, GU in Japan
Incidence of DU declining, GU stable
Probably most common chronic disease of humans. Human populations throughout the world affected. Incidence increases with age and occurs earlier and at increased rates in the developing world and lower socioeconomic groups. Up to 90% of some populations affected.
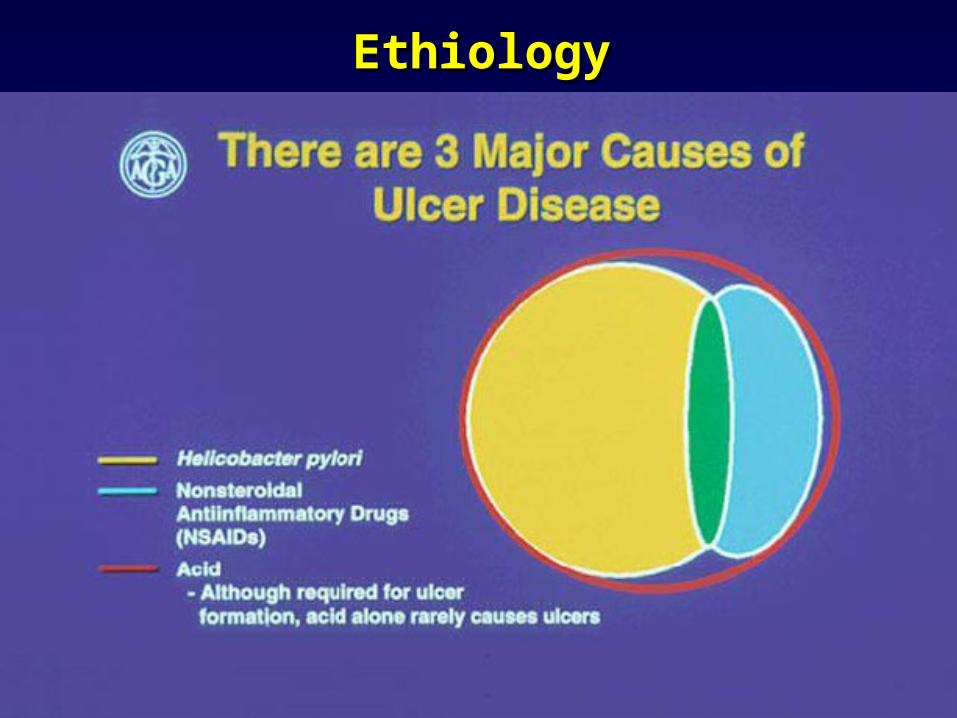
EthiologyEthiology
Predisposing factors:Predisposing factors:
1. Modifying factors1. Modifying factors
- Alimentary factors- Alimentary factors (sharp, spice diet, (sharp, spice diet, nonregulatory diet)nonregulatory diet)
- Smoking, alcohol, coffee abuse- Smoking, alcohol, coffee abuse(chronic ischemia of mucosa)(chronic ischemia of mucosa)
- Stress, psychogenic overexertion- Stress, psychogenic overexertion (hypersecretion)(hypersecretion)
- Professional factors- Professional factors (bussines trip)(bussines trip)
- Scull and brain trauma - Scull and brain trauma
- Other GI diseases- Other GI diseases (gastritis, duodenitis)(gastritis, duodenitis)
----
Predisposing factors:Predisposing factors:
2. Nonmodifying factors2. Nonmodifying factorsa) age and sexa) age and sex
b) hereditary predisposition b) hereditary predisposition - High quantity of parietal cells - High quantity of parietal cells - 0 (I) blood group- 0 (I) blood group- Fucoglycoprotein deficiency- Fucoglycoprotein deficiency- Intensified response of parietal cells - Intensified response of parietal cells
for food stimulation and gastrinfor food stimulation and gastrin- Factors of local immunity- Factors of local immunity
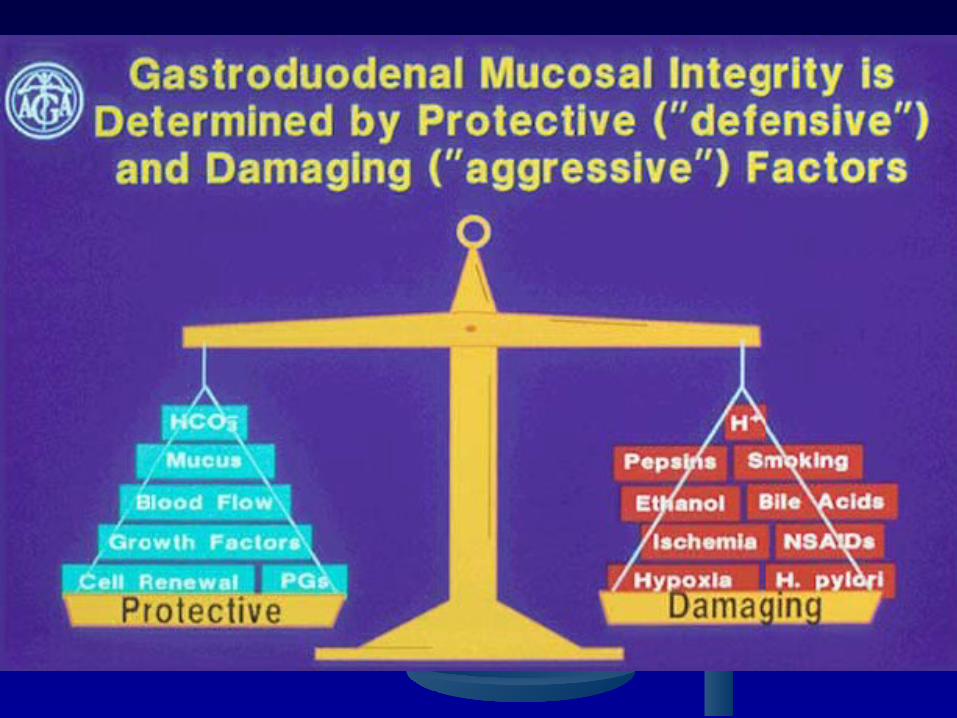
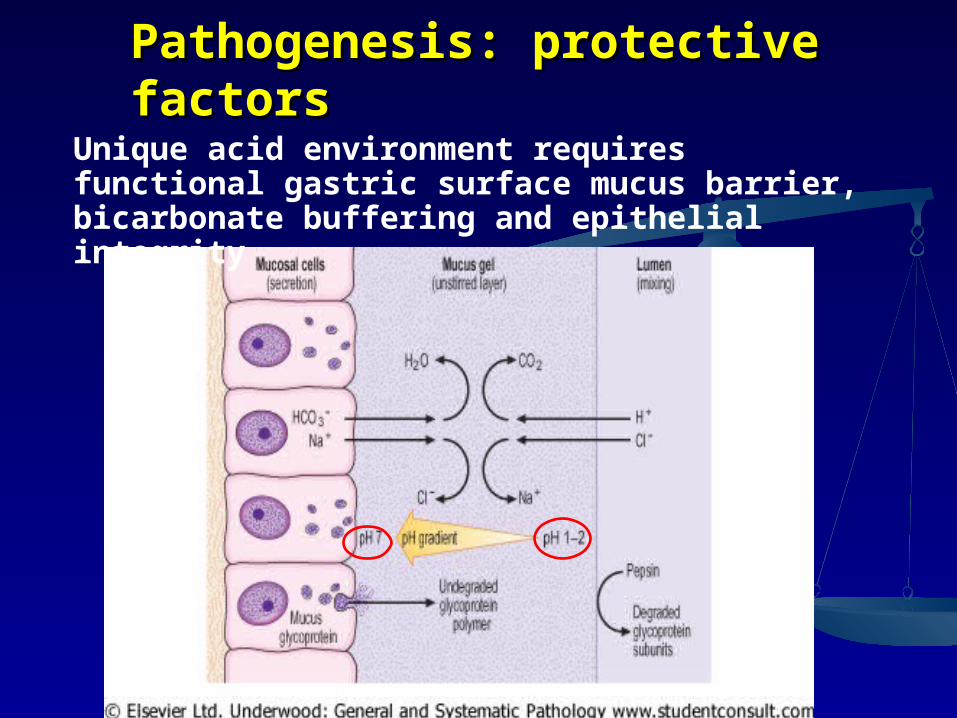
Pathogenesis: protective Pathogenesis: protective factorsfactors
Unique acid environment requires functional gastric surface mucus barrier, bicarbonate buffering and epithelial integrity
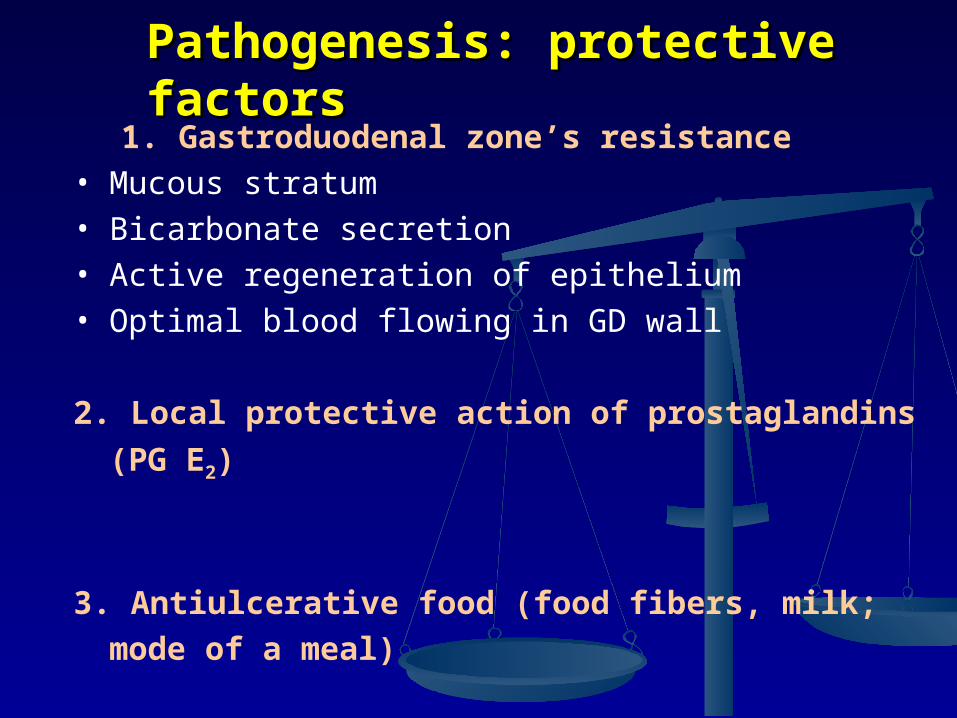
1. Gastroduodenal zone’s resistance• Mucous stratum• Bicarbonate secretion• Active regeneration of epithelium• Optimal blood flowing in GD wall
2. Local protective action of prostaglandins (PG
E2)
3. Antiulcerative food (food fibers, milk; mode of a meal)
Pathogenesis: protective Pathogenesis: protective factorsfactors

Pathogenesis: aggressive Pathogenesis: aggressive factorsfactors
1.Acid-peptic factor (hyperproduction of HCl and pepsin) - Hyperplasia of the major and parietal (parietal) cells - Vagotony - Increase sensitivity of the gastric glands to the nervous and humoral regulation 2. Gastroduodenal dismotility 3. Contact difusion H+ ions 4. Proulcerative nutritional factors (hot, spice food, irregular diet) 5. Autoimmune factors 6. Helicobacter pylori infection


Pathogenesis
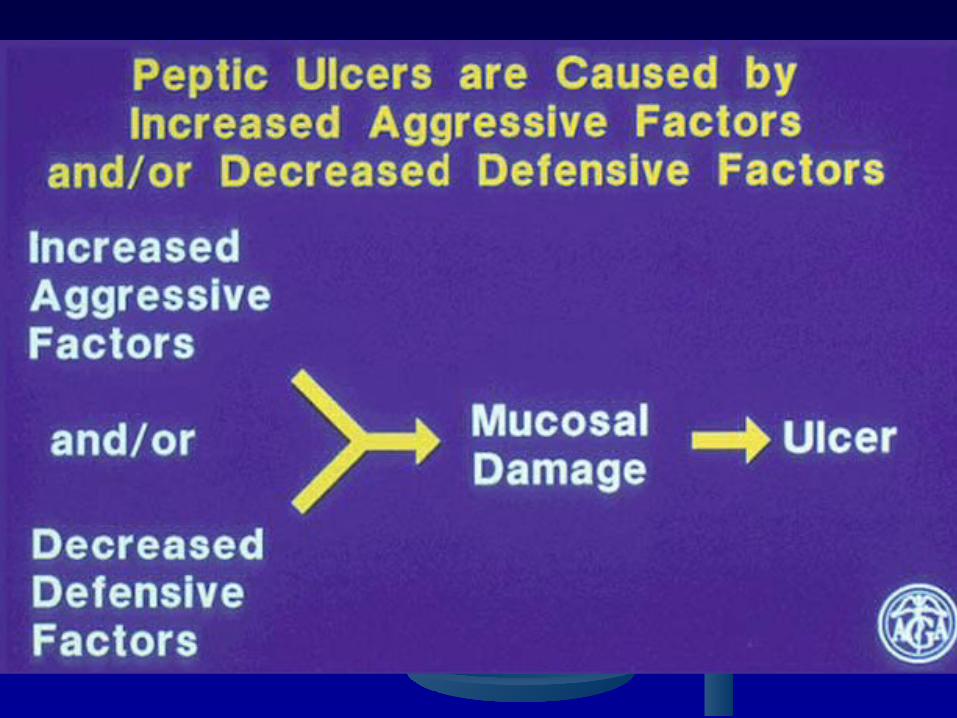
The traditional theory regarding pathogenesis of peptic ulcer focus on pepsin action and acid hypersecretion.
According to this theory, hydrochloric acid and pepsin is the main reason of damage gastrointestinal mucosa, in situation, when local defense factors are decreased. These findings are not universal and it is now known that hypersecretion is not the primary exclusive mechanism ulcerogenesis.
Pathogenesis
Infectious theory now is very important. According to this theory, the main cause of
ulcerogenesis is Helicobacter pylori, which produce enzyme – urease, mucinase, phospholipase, which may erode the mucous barrier, leading to epithelial damage.
Mucolitic enzymes (eg bacterial proteases, lipase) appear to be involved in degradation of the mucous layer, making the epithelium more susceptible to acid damage.
Warren J. R. (1983) Unidentified curved bacilli on gastric epithelium in active chronic gastritis Lancet (i): 1273
Marshall B. J. & Warren J. R. (1984) Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration Lancet (i): 1311-1314

The Nobel Prize in Physiology or Medicine 2005
"for their discovery of the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease"
Barry J. Marshall Australia
J. Robin Warren Australia
b. 1937b. 1951
« I preferred to believe my eyes, not the medical
textbooks of the medical fraternity »
R. Warren (2002)

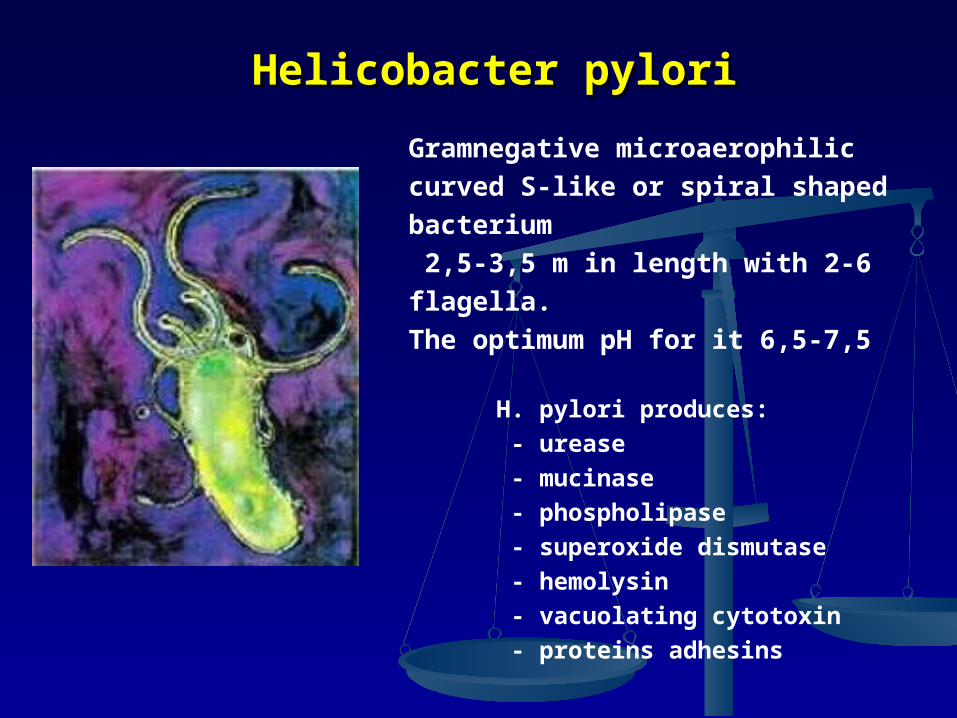
Helicobacter pyloriHelicobacter pylori
Gramnegative microaerophilic curved S-like or spiral shaped bacterium 2,5-3,5 m in length with 2-6 flagella. The optimum pH for it 6,5-7,5
H. pylori produces: - urease - mucinase - phospholipase - superoxide dismutase - hemolysin - vacuolating cytotoxin - proteins adhesins
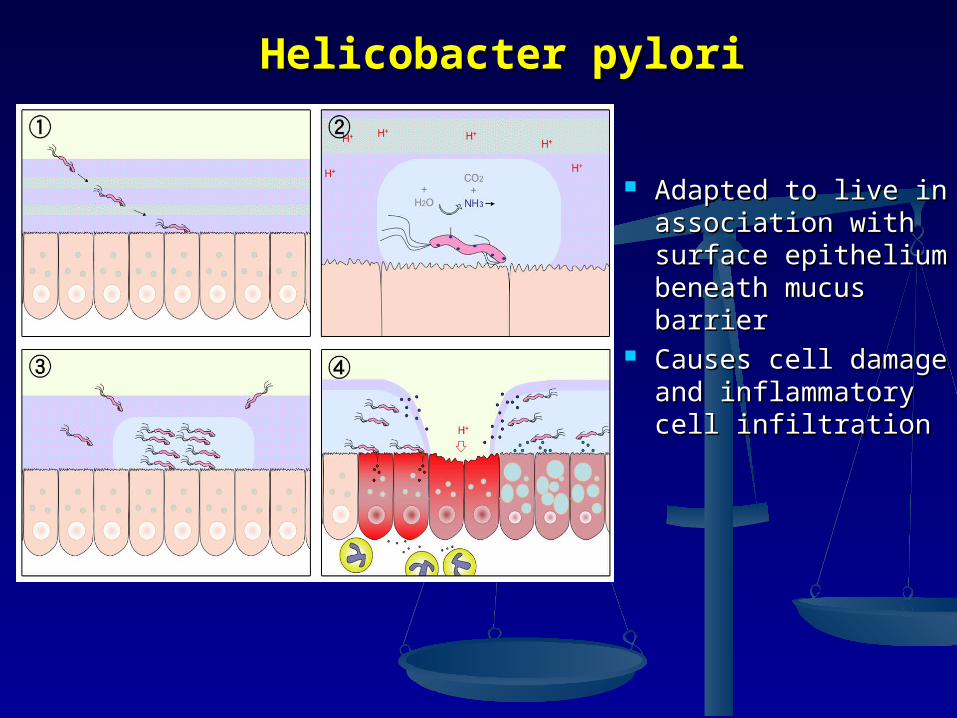
Helicobacter pyloriHelicobacter pylori
Adapted to live in Adapted to live in association with association with surface epithelium surface epithelium beneath mucus beneath mucus barrierbarrier
Causes cell damage Causes cell damage and inflammatory and inflammatory cell infiltrationcell infiltration

H. pylori H. pylori is a causal factor in mostis a causal factor in mostcases of peptic ulcer diseasecases of peptic ulcer disease
Marshall 1994
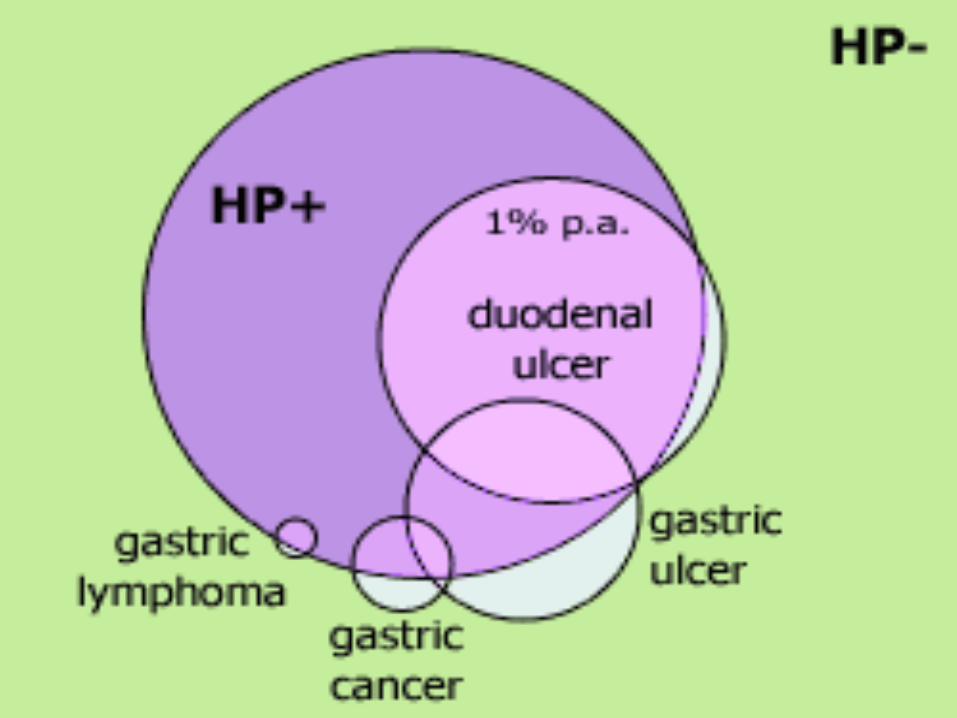
Duodenal ulcerDuodenal ulcer Gastric ulcerGastric ulcer
H. pyloriNSAID
Cancer (Zollinger Ellison)Other
92%92% 70%70%
5% 1%2%
25%
3%
2%

Helicobacter pyloriHelicobacter pylori Source H. pylori - the patient or bacillicarriers
Natural environment habitat of H. pylori are fossa gastric epithelium, intercellular connections, gastric mucus
Transmission - oral-oral or fecal-oral (including at fibrogastroduodenoscopy, pH-metry, probing for poor sterilization processing equipment)
In 1983, Warren (a biologist) and Marshall (a clinician)
described Helicobacter pylori (HP). At first, they named the bacterium
Campylobacter pyloridis. Later, it was named Campylobacter pylori.
Since then, a large number of reports have been produced on HP and
its pathogenetic potential.

Pathogenesis: the role of Pathogenesis: the role of neuroendocrine factorsneuroendocrine factors
1. Dysfunction of the parasympathetic NA
2. Dysfunction of the sympathetic NA
3. Dysfunction of the hypothalamus- pituitary-endocrine gland
4. Gastrointestinal endocrine dysfunction

In normal acid/pepsin In normal acid/pepsin attack is balanced by attack is balanced by mucosal defencesmucosal defences
Increased attack by Increased attack by hyperacidityhyperacidity
Weakened mucosal Weakened mucosal defence – the major defence – the major factor (factor (H. pylori H. pylori related)related)
PathogenesisPathogenesis

PathomorphologyPathomorphology
stomach
ulcer
Sites:Duodenum (DU)Stomach (GU)OesophagusGastro-enterostomy stomaRelated to ectopic gastric mucosa (e.g. in Meckel’s diverticulum)
ulcer
ulcer
Peptic ulcer

ClassificationClassification I. By association with H. pylori
- H. Pylori-assosiated - Nonassosiated
II. By the number of ulcers: - Single ulcer - Multiple
III. The size of the defect - Small - large - gigantic
IV. Localization of ulcers - gastric ulcer
- duodenal - combined gastric and duodenal - ulcer of gastrojejunoanastomosis
пищевод
Малая кривизна
Луковица ДПК
Большая кривизна
Привратник

Complications of peptic ulcerComplications of peptic ulcer
HaemorrhageHaemorrhage by erosion of vessel in base by erosion of vessel in base PerforationPerforation leading to peritonitis leading to peritonitis PenetrationPenetration of surrounding organ of surrounding organ
(liver/pancreas)(liver/pancreas) ObstructionObstruction (by scarring) – pyloric stenosis (by scarring) – pyloric stenosis (Cancer – rare event in true peptic ulcer)(Cancer – rare event in true peptic ulcer)
- Attack of epigastric - Attack of epigastric painpain, which arise , which arise after food from 30-60 min (ulcer after food from 30-60 min (ulcer stomach) or 1,5-2 hours and fasting stomach) or 1,5-2 hours and fasting or in the night (ulcer duodenum) and or in the night (ulcer duodenum) and relieved by vomiting, alkali food and relieved by vomiting, alkali food and medicines. Pain may be near the medicines. Pain may be near the xiphoid process or in the epigastrium xiphoid process or in the epigastrium to the left of the midle line and may to the left of the midle line and may radiation to the back near the angle radiation to the back near the angle of the left scapulaof the left scapula
Complains of patientComplains of patient
Clinical findingsClinical findings
HHeartburneartburn
NauseaNausea VomitingVomiting on height of the pain and on height of the pain and
is afferent reliefis afferent relief
ConstipationConstipation
Clinical findingsClinical findings
On examination:On examination: Usually low weight, tongue is furredUsually low weight, tongue is furred Tenderness and cutaneous hyperalgesia in Tenderness and cutaneous hyperalgesia in
the epigastriumthe epigastrium Mendel symptom’s positive (tenderness in Mendel symptom’s positive (tenderness in
one point on middle line due to percussion)one point on middle line due to percussion) Muscular rigidity of the upper rectus Muscular rigidity of the upper rectus
musclemuscle
due to free perforation due to free perforation

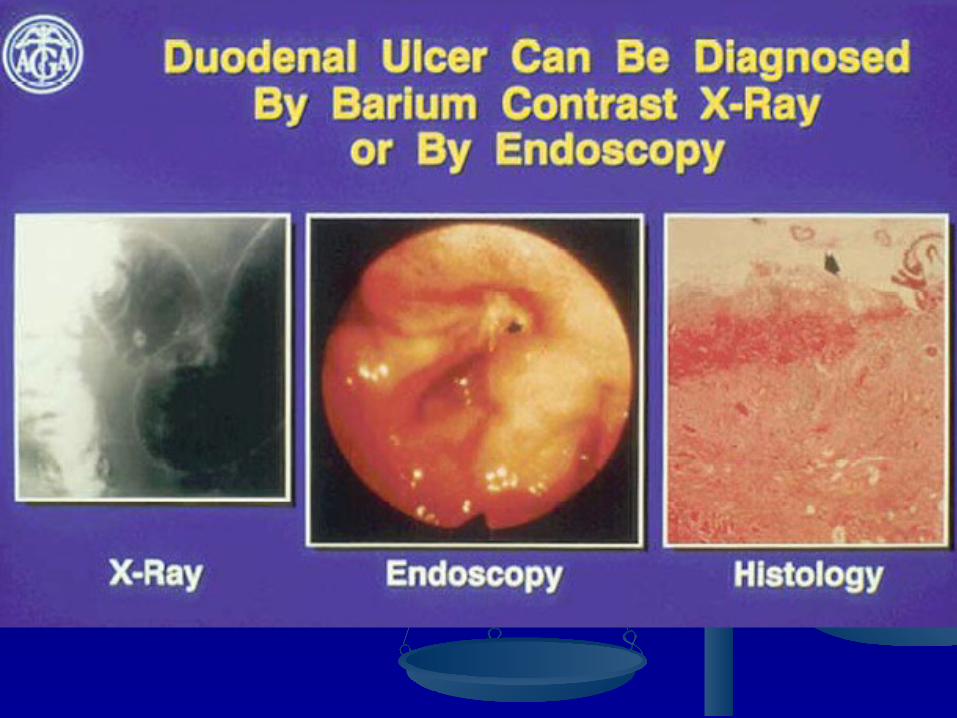
Diagnosis
• Complaints, anamnesis• Gastroscopy• Roentgenoscopy (a barium meal test)• Endoscopic biopsy and histologic evaluation• pH-metry of stomach• Tests for Helicobacter infection
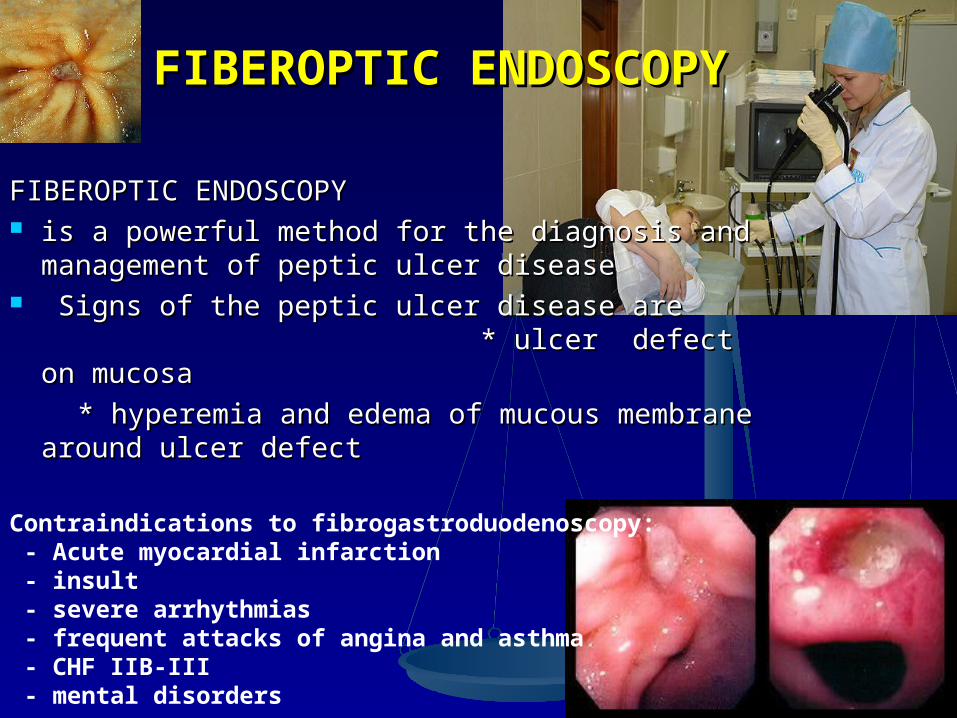
FIBEROPTIC FIBEROPTIC ENDOSCOPYENDOSCOPY
Contraindications to fibrogastroduodenoscopy: - Acute myocardial infarction - insult - severe arrhythmias - frequent attacks of angina and asthma - CHF ІІB-III - mental disorders
FIBEROPTIC ENDOSCOPY FIBEROPTIC ENDOSCOPY is a powerful method for the diagnosis and is a powerful method for the diagnosis and
management of peptic ulcer diseasemanagement of peptic ulcer disease Signs of the peptic ulcer disease are Signs of the peptic ulcer disease are
* ulcer defect on mucosa * ulcer defect on mucosa
* hyperemia and edema of mucous * hyperemia and edema of mucous membrane around ulcer defectmembrane around ulcer defect


Double-contrast barium X-rayDouble-contrast barium X-ray
Direct symptom of ulcer disease:Direct symptom of ulcer disease: * * nicheniche - symptom or permanent filling defect in the - symptom or permanent filling defect in the stomach wallstomach wall
Nondirect symptoms of ulcer:Nondirect symptoms of ulcer: * pyloric spasm* pyloric spasm * Forefinger – symptom of de Kerven* Forefinger – symptom of de Kerven ** gastric gastric foldfold’s convergence convergence ** Local changes of gastric movingLocal changes of gastric moving * Duodenal deformation* Duodenal deformation
Views demonstrate projection of crater away from the lumen

Intragastral Intragastral рН-рН-metrymetry
Hyperacidity
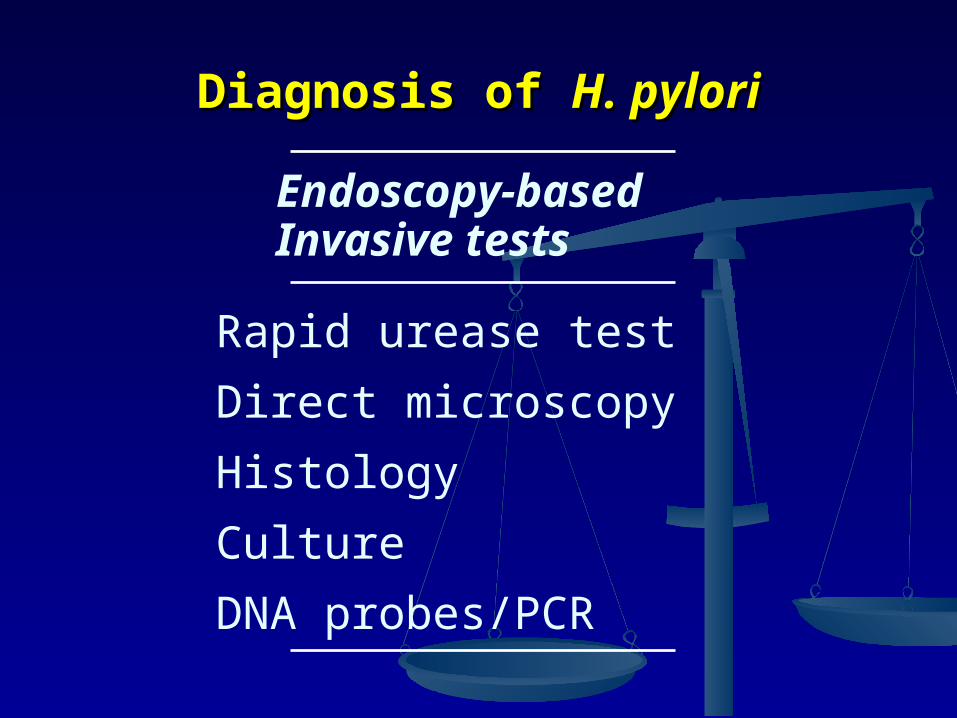
Rapid urease test
Direct microscopy
Histology
Culture
DNA probes/PCR
Endoscopy-basedInvasive tests
Diagnosis of Diagnosis of H. pyloriH. pylori

Non-invasive tests
13/14C-urea breath test (UBT)
Serology (lgG, lgA)
PCR in saliva and faeces
Diagnosis of Diagnosis of H. pyloriH. pylori
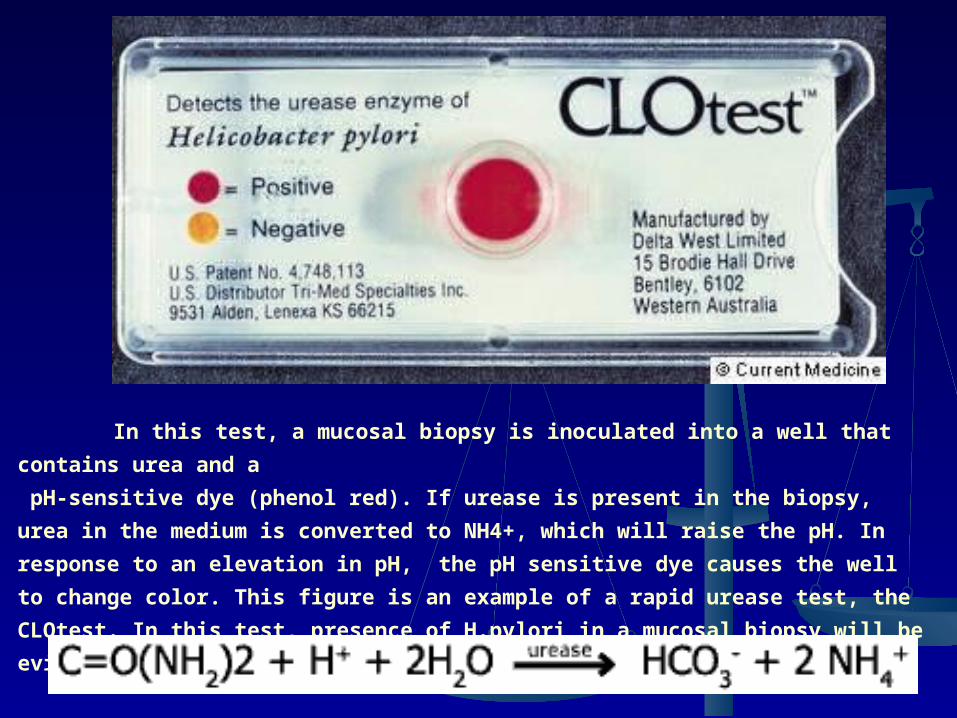
In this test, a mucosal biopsy is inoculated into a well that contains urea and a
pH-sensitive dye (phenol red). If urease is present in the biopsy, urea in the medium is
converted to NH4+, which will raise the pH. In response to an elevation in pH, the pH
sensitive dye causes the well to change color. This figure is an example of a rapid urease
test, the CLOtest. In this test, presence of H.pylori in a mucosal biopsy will be evidenced
by a color change from yellow to red.
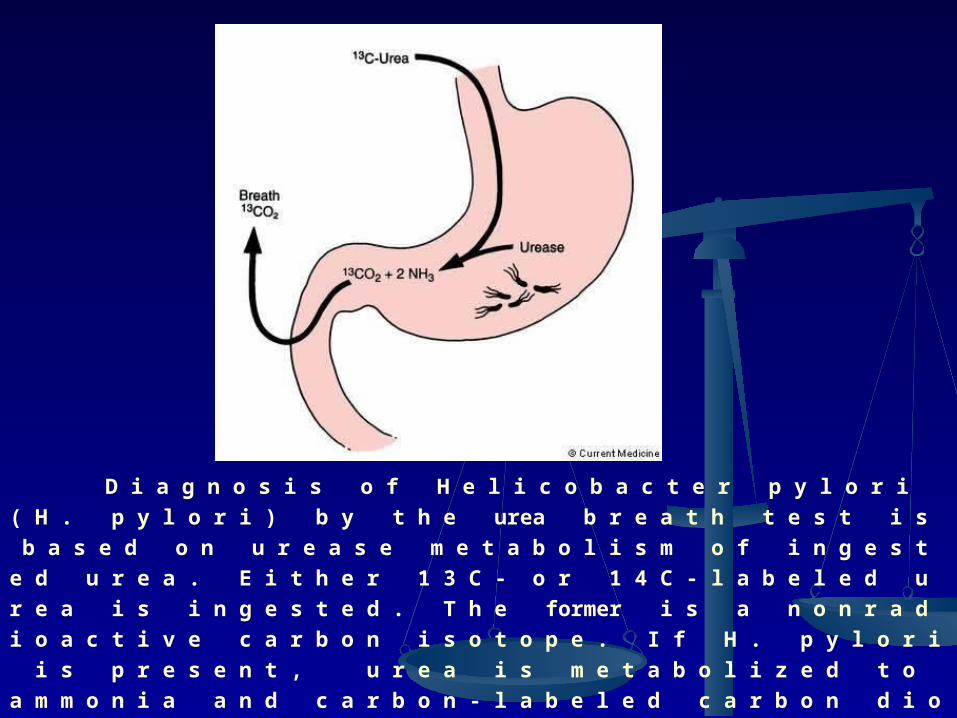
D i a g n o s i s o f H e l i c o b a c t e r p y l o r i ( H . p y l o r i ) b y t h e
urea b r e a t h t e s t i s b a s e d o n u r e a s e m e t a b o l i s m o f i n g e s t e d
u r e a . E i t h e r 1 3 C - o r 1 4 C - l a b e l e d u r e a i s i n g e s t e d . T h e former
i s a n o n r a d i o a c t i v e c a r b o n i s o t o p e . I f H . p y l o r i i s p r e s e n t ,
u r e a i s m e t a b o l i z e d t o a m m o n i a a n d c a r b o n - l a b e l e d c a r b o
n d i o x i d e . T h e l a b e l l e d c a r b o n d i o x i d e i s t h e n e x c r e t e d i n
b r e a t h a s l a b e l e d c a r b o n d i o x i d e , w h i c h i s t h e n c o l l e c t e d
and q u a n t i f i e d .

Breathtest

Infra-red spectroscope IRIS
(Germany)
Bags with exhaled air

TreatmentTreatment
Non-pharmacological therapy 1. Elimination of harmful factors (ulcerogenic drugs, smoking, alcohol) 2. Rational diet - mechanically, thermally, chemically bland food
3. Curative treatment - bed rest lax 7-10 days + light phisical activity
Drug therapy 1. Antisecretory tools 2. Antacids 3. Gastrocytoprotection 4. Reparants 5. Means, normalizes motility 6. Centrally acting drugs 7. Eradication of Helicobacter pylori infection
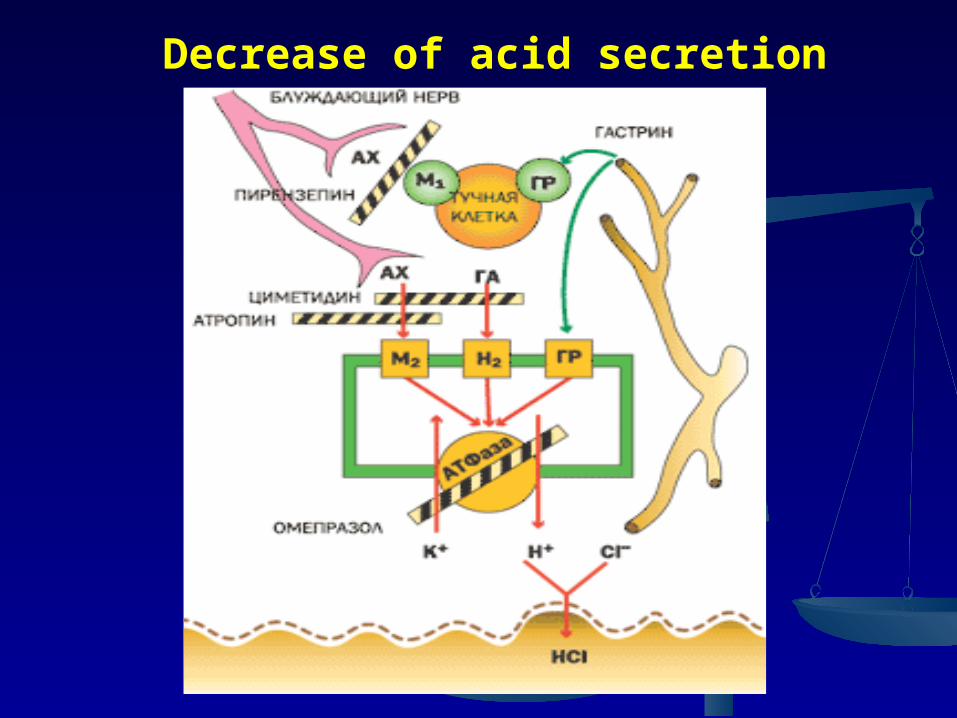
Decrease of acid secretion
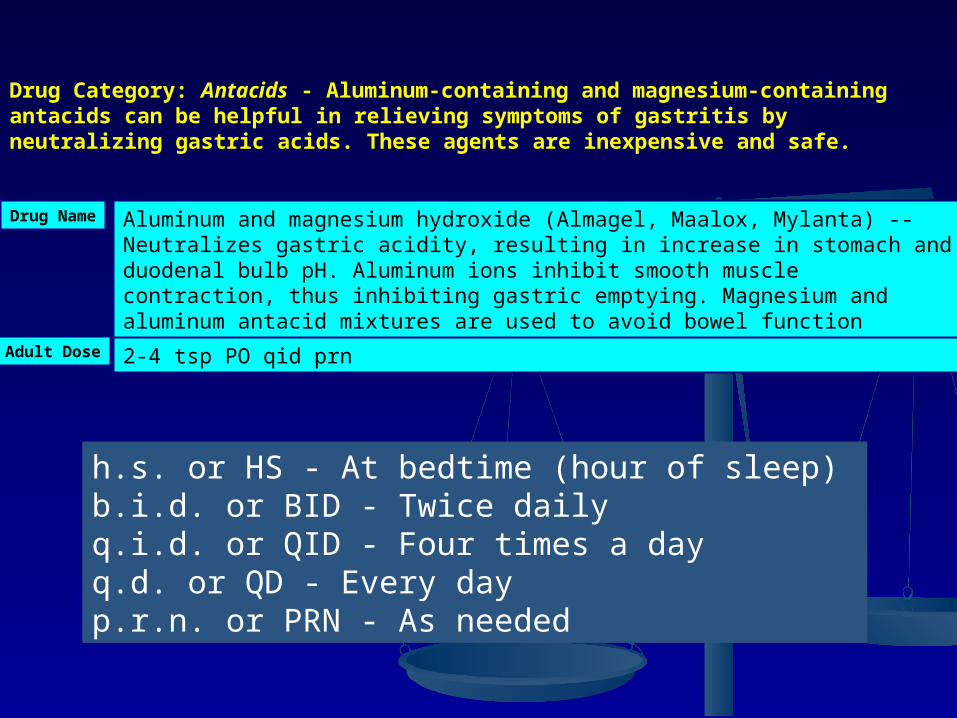
Drug Category: Antacids - Aluminum-containing and magnesium-containing antacids can be helpful in relieving symptoms of gastritis by neutralizing gastric acids. These agents are inexpensive and safe.
Drug Name
Adult Dose
Aluminum and magnesium hydroxide (Almagel, Maalox, Mylanta) -- Neutralizes gastric acidity, resulting in increase in stomach and duodenal bulb pH. Aluminum ions inhibit smooth muscle contraction, thus inhibiting gastric emptying. Magnesium and aluminum antacid mixtures are used to avoid bowel function changes.
2-4 tsp PO qid prn
h.s. or HS - At bedtime (hour of sleep) b.i.d. or BID - Twice dailyq.i.d. or QID - Four times a day q.d. or QD - Every day p.r.n. or PRN - As needed
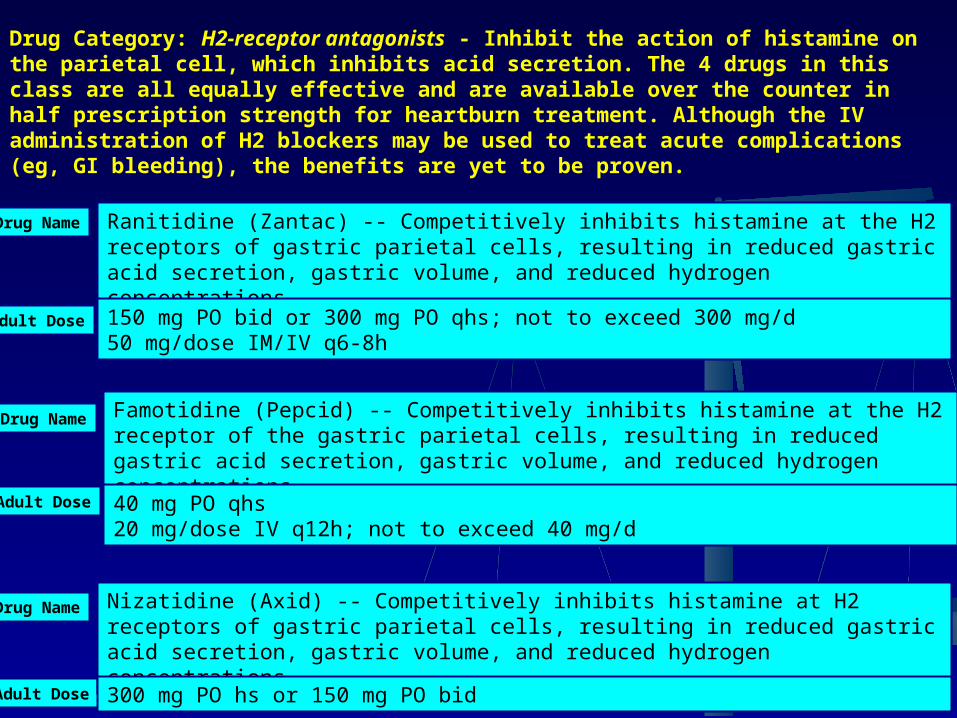
Drug Category: H2-receptor antagonists - Inhibit the action of histamine on the parietal cell, which inhibits acid secretion. The 4 drugs in this class are all equally effective and are available over the counter in half prescription strength for heartburn treatment. Although the IV administration of H2 blockers may be used to treat acute complications (eg, GI bleeding), the benefits are yet to be proven.
Drug Name
Adult Dose
Famotidine (Pepcid) -- Competitively inhibits histamine at the H2 receptor of the gastric parietal cells, resulting in reduced gastric acid secretion, gastric volume, and reduced hydrogen concentrations.
40 mg PO qhs20 mg/dose IV q12h; not to exceed 40 mg/d
Drug Name
Adult Dose
Nizatidine (Axid) -- Competitively inhibits histamine at H2 receptors of gastric parietal cells, resulting in reduced gastric acid secretion, gastric volume, and reduced hydrogen concentrations.
300 mg PO hs or 150 mg PO bid
Drug Name
Adult Dose
Ranitidine (Zantac) -- Competitively inhibits histamine at the H2 receptors of gastric parietal cells, resulting in reduced gastric acid secretion, gastric volume, and reduced hydrogen concentrations.
150 mg PO bid or 300 mg PO qhs; not to exceed 300 mg/d50 mg/dose IM/IV q6-8h

Drug Category: Proton pump inhibitors -- Bind to the proton pump of parietal cell, inhibiting secretion of hydrogen ions into gastric lumen. Proton pump inhibitors relieve pain and heal peptic ulcers more rapidly than H2 antagonists do. Drugs in this class are equally effective. They all decrease serum concentrations of drugs that require gastric acidity for absorption, such as ketoconazole or itraconazole.
Drug Name
Adult Dose
Lansoprazole (Prevacid) -- Decreases gastric acid secretion by inhibiting the parietal cell H+/K+ ATP pump.Used for up to 4 wk to treat and relieve symptoms of active duodenal ulcers. Physicians may prescribe for up to 8 wk to treat all grades of erosive esophagitis.
30 mg PO qd for 4-8 wk
Drug Name
Adult Dose
Omeprazole (Prilosec) -- Decreases gastric acid secretion by inhibiting the parietal cell H+/K+ ATP pump.Used for up to 4 wk to treat and relieve symptoms of active duodenal ulcers. Physicians may prescribe for up to 8 wk to treat all grades of erosive esophagitis.
20 mg PO qd for 4-8 wk
Drug Name
Adult Dose
Esomeprazole (Nexium) -- S-isomer of omeprazole. Decreases gastric acid secretion by inhibiting the parietal cell H+/K+ ATP pump.Used for up to 4 wk to treat and relieve symptoms of active duodenal ulcers. Physicians may prescribe for up to 8 wk to treat all grades of erosive esophagitis.
20-40 mg PO qd
Drug Name
Adult Dose
Rabeprazole (Aciphex) -- Decreases gastric acid secretion by inhibiting the parietal cell H+/K+ ATP pump. For short-term (4-8 wk) treatment and symptomatic relief of gastritis.Used for up to 4 wk to treat and relieve symptoms of active duodenal ulcers. Physicians may prescribe for up to 8 wk to treat all grades of erosive esophagitis.
20 mg tab PO qd 4-8 wk
Drug Name
Adult Dose
Pantoprazole (Protonix) -- Decreases gastric acid secretion by inhibiting the parietal cell H+/K+ ATP pump. For short-term (4-8 wk) treatment and symptomatic relief of gastritis.Used for up to 4 wk to treat and relieve symptoms of active duodenal ulcers. Physicians may prescribe for up to 8 wk to treat all grades of erosive esophagitis.
40 mg PO qd
Drug Category: Antidiarrheals
The approved antidiarrheal for this infection is bismuth subsalicylate. It has both antisecretory and antimicrobial activity.
Drug Name
Adult Dose
Bismuth subsalicylate (Bismatrol, Pepto-Bismol)Has cytoprotective effect on GI mucosa, probably due to stimulation of prostaglandin production and modulation of immune response. In addition, has been demonstrated that some deposits (probably bismuth salts) appear on both surfaces of the cell wall of HP after <1 h. Such deposits induce distortion and vacuolization of the bacterial cell and loss of adherence of HP from antral epithelium.
120 mg PO qid; not to exceed 4.2 g/d

Drug Category: Gastrointestinal agents - Are effective in the treatment of peptic ulcers and in preventing relapse. Their mechanism of action is not clear. Multiple doses are required, and they are not as effective as the other options.
Drug Name
Adult Dose
Sucralfate (Carafate) -- Binds with positively charged proteins in exudates and forms a viscous adhesive substance that protects the GI lining against pepsin, peptic acid, and bile salts. Used for short-term management of ulcers.
1 g PO qid
Drug Category: Prostaglandins - Can prevent peptic ulcers in patients taking NSAIDs and may be used with NSAIDs in patients at a high risk of complications.
Drug Name
Adult Dose
Misoprostol (Cytotec) -- A prostaglandin analog that protects the lining of the GI tract by replacing depleted prostaglandin E1 in prostaglandin inhibiting therapies.
200 mcg PO qid with food; if not tolerated, decrease to 100 mcg qid or 200 mcg bid with food

The Maastricht European The Maastricht European Consensus GuidelinesConsensus Guidelines
Indications strongly recommended Indications strongly recommended forforH. pyloriH. pylori eradication therapy: eradication therapy:
peptic ulcer disease (active or inactive)peptic ulcer disease (active or inactive)
bleeding peptic ulcerbleeding peptic ulcer
low-grade gastric MALT lymphomalow-grade gastric MALT lymphoma
gastritis with severe abnormalitiesgastritis with severe abnormalities
following early resection for gastric cancerfollowing early resection for gastric cancer

H. pyloriH. pylori eradication regimens eradication regimens supported by the Maastricht supported by the Maastricht
Consensus ReportConsensus Report
PPI standard dosePPI standard doseamoxicillin 1000 mgamoxicillin 1000 mgclarithromycin 500 mgclarithromycin 500 mg
PPI PPI standard dosestandard dose
metronidazole metronidazole 400 mg400 mg
clarithromycin clarithromycin 250 mg250 mg
PPI standard dosePPI standard dose
amoxicillin 1000 mgamoxicillin 1000 mg
metronidazole 400 mgmetronidazole 400 mg
twice daily for 1 weektwice daily for 1 week
twice daily for 1 weektwice daily for 1 week
3 times daily for 1 week3 times daily for 1 week
twice daily for 1 weektwice daily for 1 week

Resistance of Resistance of H. pyloriH. pylori to to metronidazole is common, but shows metronidazole is common, but shows
geographic variationgeographic variation
60
100
Primary resistance%
2727 2626
41.241.2
27.527.5
6.46.4
24241717
10.810.8
84847777
Belgium
Finland
France
Ireland
The Netherlands
USA
Australia
Malaysia
Zaire
Burkina Faso0
20
80
40
Mégraud 1994

Drug Category: AntibioticsUse agents known to be effective against HP.
Drug Name
Adult Dose
Metronidazole (Flagyl)Reduced to its active form intracellularly only by anaerobic organisms, then disrupts helical structure of DNA and inhibits bacterial nucleic acid synthesis.
250-500 mg PO qid
Drug Name
Adult Dose
Tetracycline (Sumycin)Inhibits bacterial protein synthesis by binding with 30S and possibly 50S ribosomal subunit(s).
500 mg PO qid
Drug Name
Adult Dose
Clarithromycin (Biaxin)Inhibits bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes, causing RNA-dependent protein synthesis to arrest.
500 mg PO q12h
Drug Name
Adult Dose
Amoxicillin (Amoxil, Trimox)Inhibits final stage of bacterial cell wall synthesis due to binding to specific PBPs on inner part of bacterial wall, leading to bacterial lysis.
1 g PO bid

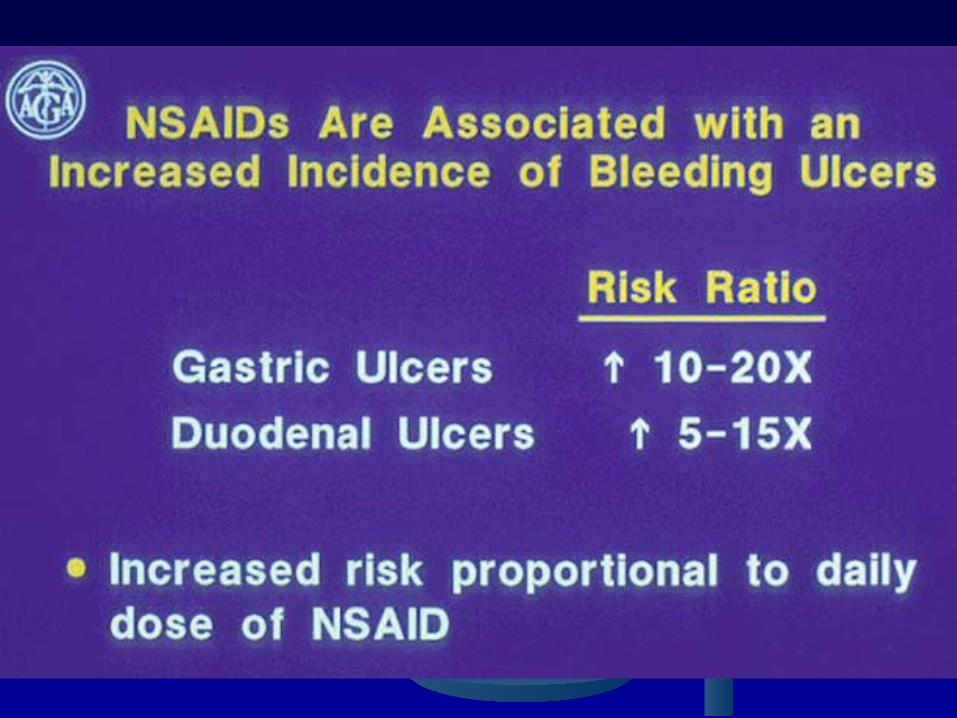
Prevention
• Primary prevention of NSAID-induced ulcers includes the following:
- Avoid unnecessary use of NSAIDs.
- Use acetaminophen or nonacetylated salicylates when possible.
- Use the lowest effective dose of an NSAID and switch to less toxic NSAIDs, such as
the newer NSAIDs or cyclooxygenase-2 (COX-2) inhibitors, in high-risk patients
without cardiovascular disease.
• Consider prophylactic or preventive therapy for the following patients:
- Patients with NSAID-induced ulcers who require chronic, daily NSAID therapy
- Patients older than 60 years
- Patients with a history of PUD or a complication such as gastrointestinal bleeding
- Patients taking concomitant steroids or anticoagulants or patients with significant
comorbid medical illnesses
• Prophylactic regimens that have been shown to dramatically reduce (prevent) the risk of
NSAID-induced gastric and duodenal ulcers include the use of a prostaglandin analogue or
a PPI.
- Misoprostol 100-200 mcg PO 4 times per day
- Omeprazole 20-40 mg PO every day
- Lansoprazole 15-30 mg PO every day

Thank you for attention!