Embed Size (px)
Citation preview

Risk Factors for Maladjustment in Puerto Rican Children
HECTOR R. BIRD, M.D., MADELY N S. GO ULD , PH.D.. THOMAS YAGER, PH.D.,BEATRIZ STAGHEZZA. M.P.H.. A ND GLORISA CANINO, PH.D.
Abstract. Data are presented on risk factors for childhood psychopathology derived from a stud y of anisland-wide probability sample of children in Puerto Rico aged 4 through 16 years. Analyses estimated the effectsof 12demographic. health. and family variables on the probab ility of being a "case." using two different operationaldefinitions of caseness. as well as on the probabilit y of receiving the diagnoses of oppositional disorder. attentiondeficit disorder. separation anxiety, depression. funct ional enuresis, and adjustment disorder . When compared toother findings. the results from these analyses indicate that the relationship between maladjustment and the riskfactors evaluated does not appear to be culturally specific. J. Am. Acad. Child Adolesc. Psychiatry, 1989. 28,6:847-850. Key Words: epidemiology, risk factors, Hispan ic. crosscultural.
The Puerto Rico child psychiatry epidemiological studyaimed to determine the prevalence of psychiatric disorder inthe island's children. The primary motivating factor that ledto this investigation was a pract ical one . The Office of MentalHealth in the Commonwealth of Puerto Rico lacked persuasive scientific information about the rates of psychiatricdisorders in the population that would convince the legislativebranch ofgovernment of the necessity for increased budgetaryappropriations for mental health . This was particularly relevant to youth, given the paucity of mental health servicesavailable for children and adolescents. Less than 10% of themental health budget was designated for child and adolescentservices, in spite of the fact that approximately 45% of thetotal population of Puerto Rico is under age 20 (U.S. Bureauof the Census, 1980). It was hoped that the argument forincreased resources for child mental health would be strongerif it was backed by descriptive data.
The study, funded by the National Institute of MentalHealth, employed a two-stage procedure for case identification and classification of children aged 4 through 16 years.During the first stage of the survey, the Child BehaviorChecklist (CBCL) (Achenbach and Edelbrock, 1981) was usedas a screening instrument for case identification; clinicalassessments of the children were carried out during the secondstage. The methodology and the measures used were pilotedprior to the field survey (Bird et al., 1987a; Canino et al.,1987). The CBCL behaved as a screen of high sensitivit y inthe Puerto Rican population (Bird et al., 1987a), and theclinicians participating in the stud y were found to agree ondiagnostic assessments with an adequate level of reliability(Canino et al.. 1987). The field survey was conducted in
Accepted November 16. 1988.Dr. Bird is Clin ical Professor ofPsychiatry and Deputy Director of
the Division ofChild Psychiatry. and Dr. Gould is Associate Professor(if Clinical Public Health (Epidemiology) in Psychiatry. both at Columbia University. Dr. Yager and Ms. Staghezza arefrom the DivisionofChild Psychiatry, Nell' York State Psychiatric Institut e. Dr. Caninois Associate Profes sor ofPsychology at the University ofPuerto RicoSchool ofMedicine. San Juan .
This research is supported hy gram MH 3882/ from the NationalInstitute ofMental Health .
Reprint requests to Dr. Bird. Box 78. 722 West /68th Street . Ne\, ·York. NY 10032.
0890-8567/89/2806-0847$02.00/0© 1989 by the American Academy of Child and Adolescent Psychiatry .
847
Puerto Rico during a 6-month period between 1985 and 1986.A more detailed account of the methods and results of thisinvestigation can be found elsewhere (Bird et al., 1988).
Although the primary research question addressed relatedto the nature and extent of the mental health problem in thechildren of Puerto Rico, extensive data were gathered onpossible risk factors of childhood psychopathology, includingprenatal, perinatal, developmental, and psychosocial factors.Of these, a few specific variables were selected for the purposesof the present report, and the selection was done in consultation with other contributors to this section . The authorswanted to define a set of similar variables that had beensystematicall y gathered in all of the investigations and couldbe compared across stud ies carried out in different settings .The results of the Puerto Rico study are of particular interestin this respect because they relate to a population for whichEnglish is not the first language and whose cultural back·ground differs from the others .
Method
The study used a multistage probability sample of 2,064households located in 210 household clusters distributedacross the entire island. Those households containing childrenaged 4 through 16 years constituted 41% (843) of the total.One child was selected at random (Kish, 1965) from amongthe eligible children in each of these households, and thishousehold member became the target of the stud y. The sample is considered to be representative of the children on theisland in the targeted age range.
Screening information was obtained from both the child 'sparent and the child's school teacher during the first stage. Achild was considered to have screened positive if he/she scoredover the published normative cutoff points on the total problem score of either the parent or the teacher CBCL. The firststage screening questionnaires were completed in 777 of the843 target households, a completion rate of 92.2%.
The goal during the second stage was to clinically evaluateall the children who screened positive and who were morelikely to be "cases," as well as a random sample of approximately 20% of those who screened negative. With data on allthe positives and on a proportion of the negatives, prevalencerates could be calculated. adjusting for this sampling procedure. The overall response rate for the second stage was 88%;90.1% of the positive screens and 79% of the targeted nega-

848 BIRD ET AL.
TABLE I. Six-Month Weighted Prevalence ofthe More CommonDiagnostic Categories in Children Aged 4-16 Years
DSM-l11Dx
Regardlessof Severity
(Weighted")
DSM-l11Dx&
CGAS <61"Definite"
(Weighted")Diagnostic Category"(Second Stage Unweighted
N = 386) % SE % SE
below the threshold score of 61 on the CGAS. The effects ofthe same predictor variables on the presence or absence ofthe six most prevalent DSM-I/I diagnoses in the sample wasalso evaluated. The impairment criterion was not consideredin this analysis for various reasons. First, the entire spectrumof children who meet DSM-/II criteria for the disorder wasof interest. Secondly, while the impairment criterion seems todefine the outcome groups more effectively, the marked reduction in numbers leads to problems of predictive powerand the authors were concerned with the possibility of runninginto Type 2 error. The most prevalent diagnoses found in thesurvey appear in Table I.
The predictor variables included age, sex, and social class(using three categories of occupational study), two indicatorsof the child's physical health (whether the child was consideredsickly by his/her parent, and number of hospitalizations), anindicator of the child's school performance (whether the childhad ever repeated a grade), and several family characteristics,including single parenthood, a scaled measure of maritalharmony, a scaled measure of overall family dysfunction (thefamily Apgar [Del Vecchio et aI., 1979]), the number ofstressful life events, using a measure derived from the Coddington scale (Coddington, 1972), and whether the mother orthe father had ever had psychiatric problems.
Analytic Strategy
Using linear regression, the effects of the 12 variables onthe probability of being a "case" were estimated by the twopossible definitions of caseness, as well as on the probabilityof receiving the diagnosis of oppositional disorder, attentiondeficit disorder, adjustment disorder, separation anxiety, functional enuresis, and depression. The effects of each predictorwere estimated individually with age and sex held constant.
Oppositional disorder 9.9 1.6 19.4 2.3Attention deficit disorder 9.5 1.6 16.2 2.0Depression/dysthymia 5.9 l.l 9.1 0.9Separation anxiety disorder 4.7 0.9 12.8 1.9Functional enuresis 4.7 1.0 10.4 1.2Adjustment disorder 4.2 1.1 12.4 2.0
"Weighted by the number of eligible children in the householdand the inverse of the sampling rate of households in the urban andrural areas as well as by the results on the CBCL (corrected fornonresponse).b Disorders are listed without exclusions.
Results
Table 2 shows the relationship between the 12 predictorvariables and the two broad measures of psychopathology:
tives (16% of those who screened negative), were clinicallyevaluated. The second-stage assessments were clinical evaluations carried out by four Board qualified child psychiatrists.Their evaluations, made blind to the screening results, included separate interviews with the child and with one of thechild's parents (usually the mother or mother surrogate). Partof the clinical evaluation involved the administration of theDiagnostic Interview Schedule for Children (DISC) to boththe parents and children. The clinicians were free to addquestions and probes to the structured interview. For thepurposes of this investigation, the DISC was used to providea uniform and consistent interview format that systematicallyinquired about psychiatric diagnostic criteria in children. Aschedule for adjustment disorders developed by PatriciaCohen at Columbia University was appended to the DISC.
The clinicians made independent decisions about the presence or absence of a particular symptom based on the datacollected during the evaluation. Their diagnoses were basedon the symptoms elicited which in their best clinical judgmentmet criteria for the disorders according to the DSM-I/I nosology. The clinicians were free to inquire about any DSM/II diagnosis applicable to children. They were instructed toignore the preemptive or hierarchical criteria of DSM-/lI, somultiple diagnoses were possible. A diagnosis was assignedwhenever the psychiatrist concluded that full criteria for thatclinical entity were satisfied during the previous 6 months.
The psychiatrists also assigned a score on the Children'sGlobal Assessment Scale (CGAS) to each child, based on theinformation obtained during the interviews, as well as on theirclinical observations. The CGAS is a scale of adaptive functioning derived by Shaffer et al. (1983) from the GlobalAssessment Scale for adults devised by Endicott et al. (1976).Scores on the CGAS can range from 0 to 100. Although thescore is assigned on a continuum, each decile on the scale isaccompanied by descriptions and examples of behaviors andfunctional levels in children typical of that decile. The psychometric characteristics of the CGAS published by its authors (Shaffer et aI., 1983), as well as those obtained duringthe pilot phase of our investigation (Bird et aI., 1987b), showit to be an instrument of considerable strength in providing ameasure of impairment. A score of 61 was found to be thebest discriminator, when the CGAS is dichotomized into twogroups, to distinguish between children who exhibit definitemaladjustment and those who do not (Bird et al., 1987b).
The survey (Bird et al., 1988) found a very high proportionof children whose CBCL total score was above thepublished norms for the instrument (Achenbach and Edelbrock, 1983). Similarly, a very high proportion of children(49%) met the psychiatrists' criteria for a DSM-/II diagnosis.This is higher than one would anticipate the rate of maladjusted children to be in the community. A more plausible rateof maladjustment (17.8%) was obtained when the morbiditycriterion was a DSM-/II diagnosis in combination with ascore in the impaired range on the CGAS.
Correlates ofDisorder
The present report examines the effect of 12 factors on twogeneral indicators of clinical status: one is the presence orabsence of a DSM-/II diagnosis: the other identifies thosechildren who not only had a DSM-/II diagnosis but scored
EPIDEMIOLOGY: RISK FACTORS IN PUERTO RICAN CHILDREN 849
TABLE 2. Relationship between Risk Factors and Global MeasuresofPsychopathology
a Age Y = 4-5 yrs., M = 6-11 yrs., A = 12-16 yrs.b SES L = lower, M = middle, U = upper.t p < 0.10, trend; * p < 0.05; ** p < 0.0 I; ***P < 0.00 I.
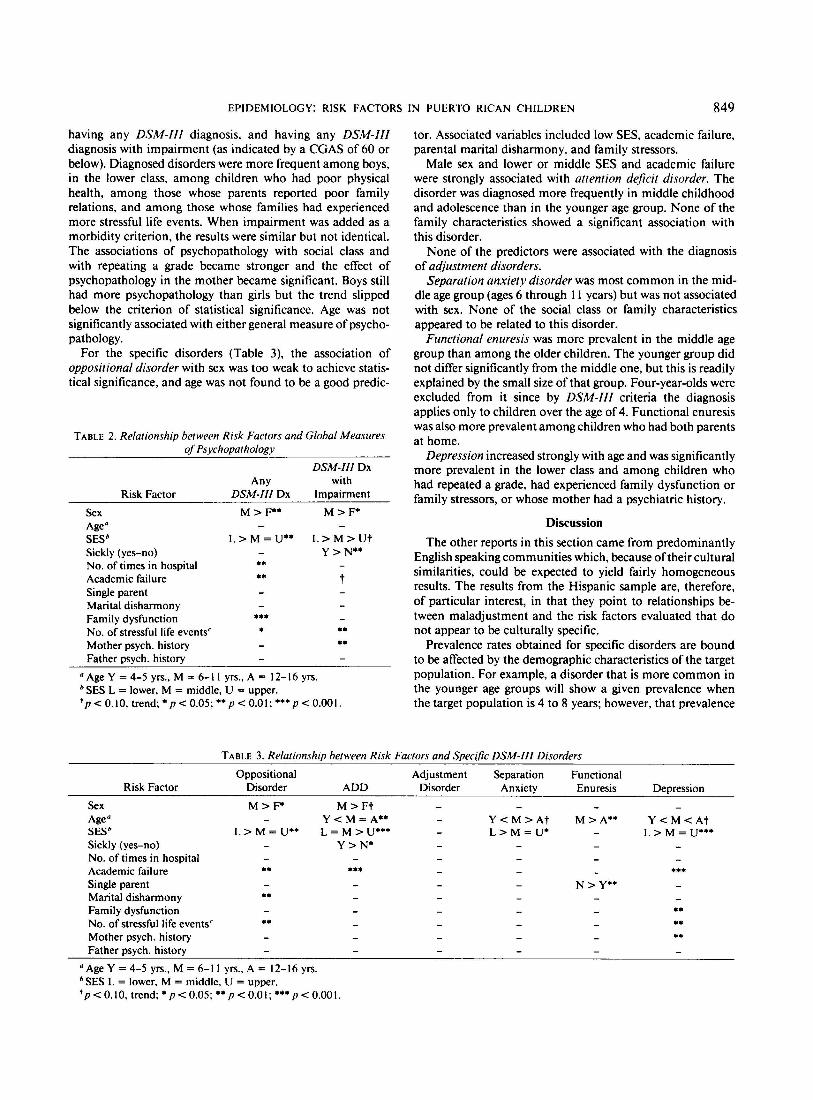
having any DSM-lIl diagnosis, and having any DSM-llIdiagnosis with impairment (as indicated by a CGAS of 60 orbelow). Diagnosed disorders were more frequent among boys,in the lower class, among children who had poor physicalhealth, among those whose parents reported poor familyrelations, and among those whose families had experiencedmore stressful life events. When impairment was added as amorbidity criterion, the results were similar but not identical.The associations of psychopathology with social class andwith repeating a grade became stronger and the effect ofpsychopathology in the mother became significant. Boys stillhad more psychopathology than girls but the trend slippedbelow the criterion of statistical significance. Age was notsignificantly associated with either general measure of psychopathology.
For the specific disorders (Table 3), the association ofoppositional disorder with sex was too weak to achieve statistical significance, and age was not found to be a good predic-
Risk Factor
SexAge"SESb
Sickly (yes-no)No. of times in hospitalAcademic failureSingle parentMarital disharmonyFamily dysfunctionNo. of stressful life events"Mother psych. historyFather psych. history
AnyDSM-Ill Dx
M > p*
L> M = U**
**
***
*
DSM-IIlDxwith
Impairment
M>P
L> M >UtY>N**
t
**
tor. Associated variables included low SES, academic failure,parental marital disharmony, and family stressors.
Male sex and lower or middle SES and academic failurewere strongly associated with attention deficit disorder. Thedisorder was diagnosed more frequently in middle childhoodand adolescence than in the younger age group. None of thefamily characteristics showed a significant association withthis disorder.
None of the predictors were associated with the diagnosisof adjustment disorders.
Separation anxiety disorder was most common in the middle age group (ages 6 through II years) but was not associatedwith sex. None of the social class or family characteristicsappeared to be related to this disorder.
Functional enuresis was more prevalent in the middle agegroup than among the older children. The younger group didnot differ significantly from the middle one, but this is readilyexplained by the small size of that group. Four-year-olds wereexcluded from it since by DSM-lIl criteria the diagnosisapplies only to children over the age of 4. Functional enuresiswasalso more prevalent among children who had both parentsat home.
Depression increased strongly with age and was significantlymore prevalent in the lower class and among children whohad repeated a grade, had experienced family dysfunction orfamily stressors, or whose mother had a psychiatric history.
Discussion
The other reports in this section came from predominantlyEnglish speaking communities which, because of their culturalsimilarities, could be expected to yield fairly homogeneousresults. The results from the Hispanic sample are, therefore,of particular interest, in that they point to relationships between maladjustment and the risk factors evaluated that donot appear to be culturally specific.
Prevalence rates obtained for specific disorders are boundto be affected by the demographic characteristics of the targetpopulation. For example, a disorder that is more common inthe younger age groups will show a given prevalence whenthe target population is 4 to 8 years; however, that prevalence
TABLE 3. Relationship between Risk Factors and Specific DSM-Ill Disorders
Risk FactorOppositional Adjustment Separation Functional
Disorder ADD Disorder Anxiety Enuresis Depression
******
***
Y < M < AtL> M = U***
N >y**
M>A**Y < M > AtL> M = U*
*****
**
**
M > PM> FtY < M = A**L = M > U***
Y>N*L> M = U**
SexAgea
SESb
Sickly (yes-no)No. of times in hospitalAcademic failureSingle parentMarital disharmonyFamily dysfunctionNo. of stressful life events"Mother psych. historyFather psych. history
a Age Y = 4-5 yrs., M = 6-11 yrs., A = 12-16 yrs.b SES L = lower, M = middle, U = upper.t p < 0.10, trend; * p < 0.05; ** p < 0.01; ***p < 0.001.

850 BIRD ET AL.
rate becomes diluted when the age range of the target population is broadened, such as in the present survey, to 4 through16 years. This may account for the low prevalence obtainedin this study for the specific diagnosis of conduct disorder.Since this is a diagnosis that generally does not appear untilprepuberty or early adolescence, and is more commonly seenin males, the rate obtained for both sexes in the age span of 4to 16 years (1.5%) may have been diluted by its absence inthe younger age groups. Based on the data, an approximationof the prevalence rate of conduct disorder in the 13- to 16year-old males would be around 4%; however, the samplesize is not adequate to determine such age/sex specific rateswith accuracy, due to lack of power.
The expected association between psychopathology and sex(M > F) was found, but of the specific disorders evaluated,this association was only significant for ADD, although asimilar trend was apparent for oppositional disorder that didnot reach our threshold of significance. Increasing age was animportant predictor of depression. Age was also important forseparation anxiety and for functional enuresis, possibly reflecting a vulnerability to these disorders during specific developmental periods.
Given that the population of Puerto Rico is predominantlyoflower socioeconomic status, the association of this variableto some of the more prevalent diagnoses, especially whenfunctional impairment was included in the diagnostic criteria,may be part of the reason for the high rates found (Bird et al.,1988). Repeating a grade was associated with these samedependent variables, suggesting an interaction with SES.
The puzzling association between an intact family andfunctional enuresis is not readily explainable and may be achance finding. Contrary to expectations, single parenthoodwas not associated with any of the psychopathology variables.This may be the closest to a culturally specific finding. It maybe that the close family ties, and the importance of theextended family and other support systems that characterizethe Puerto Rican social structure, act as buffers to the development of psychopathology in children of single parents. Inmost other respects, the findings from Puerto Rico are similarto those reported elsewhere in the literature. Longitudinaldata are necessary to test issues of causality.
The present report should serve as an introduction toadditional work on the analysis of risk factors based on thedata generated from this survey. The authors plan to look atthe association between these and other developmental and
psychosocial risk factors, and childhood psychopathology,using hierarchical multiple regression models. The DISC,which was administered and coded by the evaluating psychiatrists for all the children and parents in the second-stagesample, will provide another outcome measure for the evaluation of risk factors. The DISC provides a distinct advantagein this respect in that the outcome can be measured bothcategorically (presence or absence of diagnosis) and dimensionally (symptomatic loadings in specific domains of psychopathology). In general, the employment of continuous variables will afford greater predictive power than the use ofbinary variables.
The authors expect that ongoing research based on theresults of this survey will be of scientific significance to thefield of epidemiology, as well as of practical use since theywill provide empirical data which will inform clinical psychiatry as well as the developers of nosological systems.
ReferencesAchenbach, T. M. & Edelbrock, C. S. (1981), Behavioral problems
and competencies reported by parents of normal and disturbedchildrenaged4 through 16. Monogr. Soc. Res. Child Dev., 46, No.188.
-- -- (1983), Manual for the Child Behavior Checklist andRevised Child Behavior Profile. Queen City, VT: Queen CityPrinters.
Bird, H., Canino,G., Gould, M. S. et al. (l987a), The useof the childbehavior checklist as a screening instrument for epidemiologicresearch: results of a pilot study. J. Am. Acad. Child Adolesc.Psychiatry, 26:207-213.
---- Rubio-Stipec, M. & Ribera, J. (l987b), Further measuresof the psychometric propertiesof the children's global assessmentscale (CGAS). Arch. Gen. Psychiatry, 44:821-824.
---- et al. (in press), Estimates of the prevalence of childhoodmaladjustment in a community surveyin Puerto Rico: the use ofcombined measures. Arch. Gen. Psychiatry.
Canino, G., Bird, H., Rubio-Stipec, M. et al. (1987), Reliability ofchild diagnosis in a Hispanicsample.J. Am. Acad. Child Adolesc.Psychiatry, 26:560-565.
Coddington, R. D. (1972), The significance of lifeeventsas etiologicfactors in the diseases of children. II. A study of a normal population. J. Psychosom. Res., 16:205-213.
Del Vecchio, M. J., Smilkstein, G., Good, B.J., Shaffer, T. & Arons,T. (1979), The family Apgarindex:a study of construct validity. J.Fam. Pract., 8:577-582.
Kish, L. (1965), Survey Sampling. NewYork:Wiley.ShatTer D., Gould, M. S., Brasic, J., Ambrosini, P., Bird, H. R. &
Aluwahlia, S. (1983), A children'sglobal assessment scale(CGAS).Arch. Gen. Psychiatry, 40:1228-1231.
U.S. Bureau of the Census (1980), Decennial Census ojPopulation:1980 Washington, D.C.: U.S.Government PrintingOffice.