Embed Size (px)
Citation preview

Right shoulder and chest pain
Kate Rubey
November 2013

• Patient is a 70 year old male with PMH of HTN and hyperlipidemia who presents with constant substernal chest pain for 2 weeks and new onset R shoulder pain
• Patient has history of similar substernal chest pain, most recently in February when he had a negative NM cardiac stress test
• Notes cough exacerbates shoulder pain• Patient denied abdominal pain at presentation
Clinical History
2

Vitals
BP: 141/84
Pulse: 80
Temp: 98.1 °F
Resp: 22
SpO2: 98 %
Exam
Unremarkable with exception of RUQ tenderness to palpation
Physical Exam
3

• Concern for pulmonary embolism vs. ACS vs. gallbladder pathology
• Wells PE criteria low risk, so D-dimer indicated before chest CT
• How should we evaluate the gallbladder?
Work-up
4

ACR Appropriateness Criteria
5

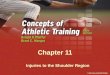
Normal Liver
Ultrasound long

Abdomen - Liver
Ultrasound long
5420719

• Liver ultrasound revealed multiple large hypoechoic, but not cystic, mass lesions seen throughout the liver, measuring up to 7.6-cm., with very little normal intervening liver parenchyma.
• Differential includes:– hepatic hemangiomas: usually hyperechoic lesions– idiopathic noncirrhotic portal hypertension: generally
isoechoic and poorly visualized on ultrasound – hepatocellular carcinoma: usually with poorly-defined
margins and coarse, irregular internal echoes– metastatic disease: variable appearance, almost always
multiple lesions, may be hypoechoic
Differential
8

• Liver metastases are concerning for GI, GU, and lung cancer
• Patient had colonoscopy 4/13 without evidence of GI malignancy
• Patient had CT of the chest, abdomen, and pelvis to look for primary malignancy and characterize liver lesions– For lesions found on US highly suspicious for
malignancy: CT abdomen with contrast is rated an 8 (usually appropriate)
Suspected Liver Metastases
9

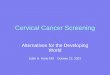
Abdomen
CT – axial, 5 minutes post contrast

Abdomen – Liver hemangioma
Contrast CT – axial

Abdomen – Hepatocellular carcinoma
Contrast CT – axial

Abdomen – Liver metastases
Contrast CT – axial

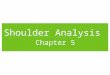
Abdomen
CT - axial
5420893

5420893
Abdomen
CT - axial

Abdomen
CT – axial
5420893

• CT chest showed a R hilar mass associated with subcarinal and paratracheal lymph nodes, concerning for neoplasm
• Patient underwent ultrasound guided biopsy of one of the liver lesions by IR
• Results of the biopsy showed “Poorly differentiated carcinoma. Immunophenotype (CK7+ and TTF-1+) is consistent with lung primary.”
17