Embed Size (px)
Citation preview

Rheumatoid arthritis for finals
By Paula Roberts
FY1

Definition Epidemiology Pathophysiology Signs and symptoms Investigations Management Case study
Objectives

Rheumatoid arthritis is an Inflammatory condition. Characterised by a symmetrical deforming polyarticular arthritis with extra-articular manifestations. It is a chronic disease which can result in significant disability.
Definition – What is Rheumatoid arthritis?

Affects 1% of population More prevalent in females (3:1) Peak incidence between 45-75 y/o Incidence
- Males: 0.1-0.2/1000 - Females: 0.2- 0.4/1000
Epidemiology

Family history Other autoimmune conditions Female HLA DR1 or DR4 Smoking
Risk factors

Inflammatory cells infiltrate the synvoium and they proliferate Macrophages and osteoclasts create chronically inflamed tissue (pannus) This extends from the joint margins and erodes the articular cartilage, by:
- blocking the normal route for nutrition - direct effect of cytokines on the chrondrocytes
Extensive erosion of cartilage and inflammation of ligament insertions Bone is exposed and deformity ensues There is marked vascular proliferation and increased permeability to
blood vessels and the synovial layer leads to effusions
Rheumatoid factor can predict prognosis: high titres is associated with progressive disease
Anti-cyclic citrullinated peptide antibodies (anti-CCP) are much more specific
Pathophysiology

Signs & symptoms

Symptoms Pain Stiffness Swelling Reduced movement/functional loss Occurs in the morning Improves during the day Fatigued Unwell Weight loss
Signs Warm and tender joints Redness Swollen joints Small joints Symmetrical deformity Ulnar deviation of the fingers
Radial deviation of the wrist Swan neck deformity Boutonniere’s deformity Z deformity of the thumb Trigger finger Wasting of the small muscles of the hand Palmar erythema Carpel tunnel syndrome Fixed flexion contracture of the elbow Rheumatoid tenosynovitis Rotator cuff tendonitis + tears Hammer Toes Knee effusion + synovitis Atlanto- Axial subluxation
Signs & Symptoms

FACEBOOKS Felty’s syndrome Atlanto-axial subluxation Caplans syndrome and pulmonary nodules Effusions (pleural exudates) Blood – normochromic normocytic anaemia Olecronon bursitis Oral dryness (sicca syndrome)Kidneys (amyloid, gold and penicilliame)Sensory neuropathy and scleromalacia
Extra-articular manifestations

Extra-articular manifestations

Palindromic Transient Remitting Chronic, persistent – Typical form Rapidly progressive
Presentations

Rheumatoid arthritis Psoratic arthropathy Systemic lupus OA with an inflammatory component Gout Septic arthritis
Differential diagnosis

Target population (Who should be tested?): Patients who: have at least 1 joint with definite clinical synovitis (swelling) with the synovitis not better explained by another disease Score >6/10 = RA (collectively in criteria A-D)A- Joint involvement
1 large joint (0) 2-10 large joints (1) 1-3 small joints (2) 4-10 small joints (3) >10 small joints (5)
B- Serology -ve RF and –ve anti-CCP (0) Low +ve RF or low +ve anti CCP (2) High +ve RF or high +ve anti-CCP (3)
C – Acute phase reactants Normal CRP and ESR (0) Abnormal CRP or ESR (1)
D – Duration of symtpoms <6 weeks (0) >6 weeks (1)
American college of Rheumatology:
2010 Rheumatoid arthritis classification

Bedside - Peak flow - ECG - Urine dip – nephrotic syndrome
Bloods - FBC- UEs - LFTs- ESR - CRP- Anti- CCP- RF (70%)- ANA (30%)
Imaging - X-ray - (MRI if knee/ C-spine involvement/ persistant symptoms and X-ray NAD)
Special tests - Joint aspiration
Investigations

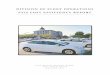
Peri-articular osteoporosis
Reduced joint space
Erosion
Soft tissue swelling

SPADES: Soft tissue swellingPeri-articular osteoporosis Absent osteophytes Deformity Erosions Subluxation
Radiological changes

Conservative Weight loss Smoking CessationMedical NSAIDs DMARDs (methotrexate, sulfasalazine) Steroids – low dose until DMARDs start working Biological agents (adalimumab, etanercept and infliximab) Surgical Synovecotomy, arthrodesis, arthroplasty, tendon repair, joint replacement Psychological Screen for depression Social Support groups Patient edcucation
Management
KEY WORDS - MDT - Biopsychosoc
ial


Rheumatologist Specialist nurse – Education, DMARD
monitoring Orthopaedic surgeon Physiotherapist Occupational therapist Podiatrist
MDT

Case scenario: 34 year old woman comes to see you. She has a 8 week history of pain affecting the small joint of her hand. The pain is worse first thing in the morning and is associated with stiffness. It takes about 1 hour for the stiffness to improve. She has felt generally unwell over the period too.She has noticed her hands and slightly swollen. She is otherwise well and only takes the OCP. She smokes 10 cigarettes a day and drinks <14 units of alcohol per week. She works as a secretary. She is concerned that she has been late to work recently because of the disruption to her morning routine. ON examination her hands are slightly swollen over the MCP and PIP joints of both hands and are tender to palpation over these joints. There is no obvious deformity to them. She has a temp of 37.5 but has no skin changes to her elbows or scalp. Her right eye is slighty red around the cornea, but not painful.
Case

What are your differentials for this lady? What investigations would you do? What Xray changes would you expect in RA? Name the typical hand changes you would see in an exam
patient with RA What are the extra-articular manifestations of RA? How would you manage this patient? Name some DMARDs, give a side effect for each of them? What is the mechanism of action of the biologic agents used to
treat RA? What test should be done before starting biolgics? What are the diagnostic criteria for RA?


Ask doctor Clarke. Medicine for finals 2013-2014 Sam, AH & Theo JTH (2010). Rapid Medicine, 2nd
edition, West Sussex: Wiley-Blackwell. Shipley, M, Rahman, A, O’Gradaigh, D & Compston
JE. 2009. Rheumatology and bone disease. In: Kumar, P & Clarke, M eds. Kumar and Clarke’s clinical medicine. Edinburgh: Elsevier LTD pp. 499 – 569.
NICE (2007). Adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis.
References