Embed Size (px)
Citation preview

INTRODUCTION
wo major factors for a successful complete dentureare superior retention and support. This isachievable once a clinician is able to record an
accurate final impression and replicating the functionaldepth of the sulci and entire denture bearing area1.However; there may be scenarios where the quality ofthe denture bearing tissues is not in a favorable state.Resorbed, displaceable or flabby tissue may be presentwhich may give rise to common complaint of a loosedenture. The prevalence of flabby ridges was found to be5% in edentulous mandibles and 24% in edentulousmaxilla2. It has been reported in the literature that whenmandibular anterior teeth cause trauma in the anteriormaxillary region because of higher occlusal forces, fibroustissue hyperplasia occurs and the mucosa becomes highlymobile and loosely attached to the underlying bone3. Theflabby tissues of residual alveolar ridges could also be aresult of extractions which were uncontrolled andunplanned.
Several techniques for overcoming the problem offlabby ridges have been described in the literature. Atechnique which involves the use of two impression
materials has been described in the literature. It involvesthe use of custom tray with zinc-oxide eugenol overnormal tissues and impression plaster over the flabbytissue areas4. Crawford & Walmsley5 described a techniquewhich involves the use of two trays and the impressionis taken with two different materials. These impressionsare then oriented intra-orally. Osborne6 described thetechnique termed as "window" impression technique inwhich a custom tray made tray is fabricated with a windowover the flabby tissues. Initial impression of the normaltissues is taken using the tray with amuco-compressiveimpression material. When the material is set, theimpression of the flabby tissues is taken through thewindow using low viscosity impression plaster.
There have been recent advancements in materialsciences and newer materials are available in the markethaving different consistencies and methods of dispensing.A practitioner is thus, able to choose the material that ismost suitable for the patient also. The aim of the currentpaper is to review various methods of management offlabby ridges and to describe the classic windowimpression technique.
MANAGEMENT OF FLABBY RIDGES
Crawford & Walmsley5 have described threeapproaches for the management of flabby ridges:a. Surgical RemovalSurgical removal can be done in patients with no medical
JPDA Vol. 24 No. 04 Oct-Dec 2015 210
REVISITING THE "WINDOW TECHNIQUE"
ABSTRACT: Management of mobile and flabby tissues over mandibular and maxillary edentulous ridges duringcomplete denture construction is a challenging task in removable prosthodontics. If not managed effectively, thepresence of flabby ridges may lead to poor denture retention, stability and support. Many techniques and materialshave been used to effectively overcome the difficulty. The current case report sheds light upon a classical andeffective technique termed as the "window technique" for the management of flabby ridges.KEYWORDS: 1. Flabby ridges 2. Impression plaster 3. Conventional prosthodontics 4. Window techniqueHOW TO CITE: Rashid H, Nas A, Ahmed AS, Zuhaib-uddin M. Revisiting the "window technique". J Pak DentAssoc 2015; 24(4):210-214.Received: 24 November 2015, Accepted: 26 December 2015
1. Assistant Professor& Head, Department of Prosthodontics, Ziauddin University,Karachi, Pakistan.2. Assistant Professor and Head, Department of Prosthodontics, Jinnah Medical & DentalCollege, Karachi, Pakistan.3. Research Trainee, Faculty of Dentistry, McGill University, Montreal, Canada.4. Muhammad Zuhaib uddin. Postgraduate trainee, Dow University of Health Sciences,Karachi, PakistanCorresponding author: “Dr. Haroon Rashid ” < [email protected] >
Haroon Rashid 1 BDS, MDScAsma Naz2 BDS, FCPS Ahad Shahid Ahmed3 BDS, MSc
CASE REPORT
T
Muhammad Zuhaib uddin4 BDS

JPDA Vol. 24 No. 04 Oct-Dec 2015211
and dental contraindications and has an advantage thatit produces a firm denture-bearing area. This results infabrication of a prosthesis which is stable and retentivein most cases. However; the procedure should not beperformed here there is reduced height of residual alveolarridges7.
The area from where the tissue is excised/removedusually requires replacement with the denture base materialwhich leads to an increase in the overall bulk of theprosthesis. This could actually result in a prosthesis whichis un-retentive. It could be argued that although presenceof flabby ridge leads to a sub-standard retention of adenture, it may be desirable than having no ridge atall.Ghazali et. al.,8 studied the effects of surgical removalof soft tissues and flabby ridges from edentulous maxillaryalveolar ridges in five subjects. Their results indicatedthat it is beneficial that early surgical removal of theflabby tissues is carried out.b. Implant Retained ProsthesisTreatment of edentulous patients using dental implantsis considered to be the treatment of choice nowadays9.Implant over dentures (IOD) have gained worldwidepopularity, acceptance and significantly improve thequality and standard of life for patients with edentulousridges. The prosthesis retained by dental implants isretentive, stable and often requires good maintenance ofboth the prosthesis and other components10. Continuedresearch related to IODs has resulted in multiple optionsand combinations for IOD attachment systems withvarying success. An IOD, in comparison to fixed implantsupported prosthesis is economical initially and the surgicalprocedure is often easy to perform. However; it is worthmentioning that despite of reduced initial expenses, thecost of maintenance of an IOD could be substantial.As far as time and finances is concerned, the long termmaintenance costs are higher. Other factors that couldhinder implant placement include discomfort andinconvenience, the general health status of the patientand the risk of complications and failure of endosseousimplants. Overdenture abutments, whether it is a retainedroot or an implant, preserves the height of alveolar boneand helps in stabilization of complete dentures particularlyin the lower jaw. The option of retaining roots is a costeffective mean with no invasive therapy. Generalpractitioners should consider retaining the roots as theyserve as a useful platform for over-dentures, especiallyfor those individuals who are old aged.
Maxilla has higher prevalence of flabby ridge as
compared to mandible and implants in maxillaryregions are not as successful as mandibular implants andsuccess rates of about 79% to 82% have beenreported11,12.Decreased success rates could have been dueto placement of short endosseous implants into highvascular bone with poor volume and low-density.c. Conventional ProsthodonticsWhere implant placement and surgical excision is not anoption, conventional prosthodontics techniques areavailable which may be beneficial in overcoming theproblem of flabby ridges. During impression, when mobileflabby tissue is displaced from its resting position, thereis a very high probability that an unfavorable denturebearing area is produced. Literature describes two waysof overcoming this problem conventionally. One methodis to record a muco-displacive impression which aims tocompress the flabby tissues. This will allow functionalsupport from the flabby tissues and by replicating thecontour of the alveolar ridge during function by theocclusal forces. The other way to overcome is by recordinga mucostatic impression that aims to gather support fromother areas of the ridge and maximizes retention, stabilityand support.
Many techniques of overcoming flabby ridges havebeen described in literature. These include the one partimpression technique13, controlled lateral pressuretechnique14, palatal splinting technique and two partimpression technique or the window technique6. Theauthor would like to specifically discuss the two partimpression/ window technique.d. Two Part Impression or Window TechniqueThis classic technique was first described in 1964 byOsborne6 and it ensures that flabby tissues are not distortedduring impression taking as no excessive force is exertedby the tray over mobile tissues. The initial impression isrecorded using impression compound and the displaceabletissue is marked on the recorded impression and istransferred to the study cast. A closed fitting custom madetray is constructed which does not cover the displaceablesoft tissue. This is usually achieved by creating a windowover the flabby tissue area. Border moulding is performedand final impression of the entire supported ridge isrecorded using zinc-oxide eugenol impression paste ormedium bodied silicone impression material. Theimpression of the flabby tissues is then recorded bysyringing impression plaster or by dispensing the lightbodied silicone impression material.
There is a variation in the design of the custom made
Revisiting the "window technique"Rashid H / Nas A / Ahmed AS / Zuhaib-uddin M

JPDA Vol. 24 No. 04 Oct-Dec 2015 212
tray and it could be completely uncovering the sectionof the arch or a window may be created in the areas whereflabby mobile tissue is present. In majority of the custommade tray types, a modification of the placement of thetray handles is necessary. The window type modificationis advantageous since it allows for appropriate bordercorrection before proceeding ahead with the second stageof the impression.
CASE REPORT
A 72 year old male patient reported to the Divisionof Prosthodontics, Ziauddin University Hospital, Karachi,complaining of loose and ill-fitting maxillary andmandibular complete dentures. The patient had beenedentulous for the past 9 years and had worn three setsof complete dentures previously. A thorough clinicalexamination was performed and flabby mobile tissue wasobserved in the anterior region of the upper arch along-with severely resorbed lower mandibular ridge.
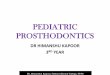
Treatment plan was discussed with the patient and anoption of surgical removal of the upper mobile tissuefollowed by a conventional complete denture andplacement of a lower implant retained over-denture.However; patient could not afford the cost of dentalimplants and was not in a favor of a surgical procedure.It was finally decided that new set of maxillary dentureusing the "Window Technique" would be fabricated anda new set of mandibular dentures were to be fabricatedusing the neutral zone impression technique. Themanagement of maxillary edentulous ridge was carriedout as follows:1. Primary impression of the upper edentulous ridgewas recorded using high viscosity irreversible hydrocolloid(Cavex Holland, BV) (Figure 1). The impression was
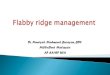
poured in the laboratory and preliminary cast was obtained.2. The flabby mobile tissue was marked on the cast anda custom made tray was fabricated using self-cure acrylicresin. The borders of the custom-made trays were kept2mm short of the vestibules.3. A window was created on the custom made traysusing acrylic trimming burs. The size of the windowopening was determined using the size of the displaceabletissues and two tray handles were constructed (Figure 2).
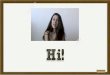
4. Border moulding for the maxillary arch was carriedout using green-stick impression compound (MetroDent)and secondary impression was recorded using zinc-oxideeugenol impression paste (Cavex, Holland, BV). Excessimpression material at the peripheries of the window wastrimmed away carefully using a scalpel (Figure 3).5. The impression was re-inserted in the patient's mouthand thin mixed impression plaster was injected through
the window over the flabby mobile tissues. The tray washeld with light pressure and care was taken to avoid tissue
Figure 1: Maxillary preliminary impression
Figure 2: Custom-made tray with a window in anteriormaxillary region
Figure 3: Final impression of the maxillary denture bearingarea not involving the flabby tissues
Rashid H / Nas A / Ahmed AS / Zuhaib-uddin M Revisiting the "window technique"

JPDA Vol. 24 No. 04 Oct-Dec 2015213
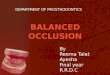
distortion during the procedure.6. The material was allowed to set and the impressionwas removed with care, disinfected and sent to thelaboratory for further processing (Figure 4).7. The usual remaining denture fabrication steps were
carried out, denture was delivered to the patient and post-operative instructions given.
DISCUSSION
Prosthodontic management of flabby ridges can becarried out effectively by various means. The choice ofbest treatment modality is dependent on various factorsincluding the medical health status of the patient andthe degree of displaceability of the flabby tissues.Surgical excision offers promising results but may alsolead to decreased sulci depth. It is worth mentioningthat surgical intervention i.e. the excision of flabbytissues, bone grafting and implant placement may notalways be possible in elderly patients and denturefabrication using the "window technique" may be theonly successful alternative.
Osborne J6 used two different impression materialsi.e. zinc-oxide eugenol and impression plaster for flabbyridge management. In their technique, they used twoseparate trays and impression materials were used torecord the normal and the flabby tissues which wererelated intra-orally. The technique described in thecurrent case report is similar to that of Watson15 whoalso fabricated a custom made tray with a window, usedimpression plaster to record the impression of the mobileflabby tissues and zinc-oxide eugenol to record theimpression of the remaining tissues of the maxillaryridge.
Impression plaster is a mucostatic impressionmaterial with very limited use in clinical dentistrynowadays. It is very effective in scenarios whereminimum displacement of the tissues during impressiontaking is required. The material is difficult to handle,messy and is not well tolerated by patients16. Impressionsrecorded using impression plasters are also difficult topour in the laboratory17. However; the material is cost-effective, offers good dimensional stability and allowsthe clinician to control the setting reaction.
The authors would also like to encourage theclinicians to properly record the orientation of theocclusal plane during recording of the jaw relationships.The use of a suitable face-bow and set up of teeth ona semi-adjustable articulator is highly recommendedas this will help to establish a suitable occlusal schemewith balancing contacts during excursive movements.If this is not achieved, the denture already seating onmobile tissues will be further destabilized.
CONCLUSION
The window technique described in the currentpaper is simple, cost effective and does not require anadditional clinical visit. The materials described in thecurrent case are readily available but authors wouldstill encourage the use of addition cured silicones asthey offer better clinical handling and excellentdimensional stability. Effective communication withthe dental technician is also encouraged for a bettertreatment outcome.
ACKNOWLEDGEMENT
The authors would like to acknowledge Mr. AbdulWaheed, acrylic technician in the dental laboratory ofthe department of prosthodontics, Ziauddin University,for his expertise and help during laboratory stages ofthe denture fabrication.
Author Contribution:HR made the original design of the manuscript, andperformed proof reading, AN wrote section 2 and 3 ofmanuscript and performed proof reading, AS wrotediscussion and MZ took photographs and performedproof reading.Disclosure: None disclosed
Figure 4: Completed final impression
Rashid H / Nas A / Ahmed AS / Zuhaib-uddin M Revisiting the "window technique"

JPDA Vol. 24 No. 04 Oct-Dec 2015 214
REFERENCES
1. Lynch CD, Allen PF.Management of the flabby ridge:using contemporary materials to solve an old problem.Br Dent J. 2006 Mar 11;200:258-61.2. Carlsson G E. Clinical morbidity and sequelae oftreatment with complete dentures. J Prosthet Dent 1998;79: 17-23.3. Kelly E. Changes caused by a mandibular removablepartial denture opposing a maxillary complete denture.J Prosthet Dent; 1972; 27:140-50.4. Magnusson B, Engström H, Kahnberg K. Metaplasticformation of bone and chondroid in flabby ridges. Br JOral Max Surg. 1986; 24: 300-305.5. Crawford R, Walmsley A. A review of prosthodonticmanagement of fibrous ridges. Br Dent J. 2006; 199:715-719.6. Osborne J. Two impression methods for mobilefibrous ridges. Br Dent J. 1964; 117: 392-394.7. Grant A A, Johnson W. Removable dentureprosthodontics. 2nd ed. p 61. Edinburgh: ChurchillLivingstone, 1992.8. Ghazali S, Nilner K, Wallenius K. The functionaldeformation of maxillary complete dentures in patientswith flabby alveolar ridges. Part II: After surgery. SwedDent J. 1991;15(2):63-70.9. Vohra FA, Rashid H. Implant retained overdentureas first choice of care for edentulous mandibles: Apresentation of two cases. J Pak Dent Assoc 2012; 21;
182-187.10. Rashid H, Hanif A, Vohra FA, Sheikh Z. Implantoverdentures: A concise review of the factors influencingthe choice of attachment systems. J Pak Dent Assoc2015; 24: 63-69.11. Goodacre C J, Kan J Y K, Rungcharassaeng K.Clinical complications of osseointegrated implants. JProsthet Dent 1999; 81: 537-552.12. Becker W, Becker BE, Alsuwyed A, Al-Mubarak S.Long-term evaluation of 282 implants in maxillary andmandibular molar positions: a prospective study. JPeriodontol. 1999 Aug; 70 :896-901.13. Lamb D J. Problems and solutions in completedenture prosthodontics. pp 57-60. London: Quintessence,1993.14. Grant A A, Heath J R, McCord J F. Completeprosthodontics: problems, diagnosis and management.pp 90-92. London: Wolfe, 1994.15. Watson RM. Impression technique for maxillaryfibrous ridge. British Dental Journal 1970; 128:552.16. Moonsammy VJ, Owen P, Howes DG. A comparisonof the accuracy of polyether, polyvinyl siloxane, andplaster impressions for long-span implant-supportedprostheses. Int J Prosthodont. 2014 Sep-Oct;27:433-438.17. Thongthammachat S, Moore BK, Barco MT 2nd,Hovijitra S, Brown DT, Andres CJ. Dimensional accuracyof dental casts: influence of tray material, impressionmaterial, and time. J Prosthodont. 2002 Jun;11:98-108.
Rashid H / Nas A / Ahmed AS / Zuhaib-uddin M Revisiting the "window technique"