Embed Size (px)
Citation preview

Review o f Literature

REVIEW OF LITERATURE
HISTORICAL BACKGROUND OF PNEUMONIA
Pneumon~a an anclent d~sease known to Hlppocrates was understood
clearly only after the isolation of Pneumococcus in the year 1880 and
establlshrng Pneumococcr as ~ t s causative agent in humans by
Welchselhaum In 1886 In the year 1889 Townsend and Coolrdge reported
1000 cases of pneumonla treated In the Massachusetts General Hosprtal
wlth a mortalrty rate of 25% Sulfapyr~dlne was prescrrbed for the treatment
of pneumonra In the year 1939 followed by report of the use of serum
therapy Type-specrf~c rabb~t antrserum was used for serum therapy by
Lohman In the year 1939 Trllett et al In 1944 reported the use of 40 000-
100 000 un~ts of pen~crllrn a day for 4 days to cure both bacteremic and
nonbacterem~c pneumococcal pneumonla Th~s amazing discovery had a
remarkable effect In the treatment of cases of pneumonla (Austr~an 1999)
The d~scovery of typ~ng of pneumococcl by uslng raprd techniques
followed - slnce the knowledge of typlng was not necessary In treating cases
of pneumonla, ~t was totally drscarded for few years With the result in the
year 1950 Re~man Mote "Unfortunately slnce the determrnatlon of types of
pneumococcl w t ~ c h cause pneumonla IS no longer of practical necessity for
therapy the procedure has been almost entlrely abandoned It was felt that
among the cases of pneumonla in the age group of 15-60 without any co-
ex~st~ng infectron bacter~olog~c studres were unnecessary This ult~mately
led to the concept of adm~ss~on of very few cases of pneumonia in any
hosp~tal (Austr~an 1999)

Finally, the physicians concluded that prophylaxis IS the only
alternative to those at risk of a fatal outcome from pneumococcal infection.
Thls led to the advent of production of pneumococcal vaccines.
EPIDEMIOLOGY
Pneumonia in industrialised countries with special reference to
Pneumococcal pneumonia:
Acute respiratory infections, particularly pneumonia, are the leading
cause of morbidity and mortality worldwide. The leading cause of bacterial
pneumonia is Spneumoniae in most hospltalised patlents (Ort et al. 1983).
Desplte the avallabllity of effective antibiotics, morbldlty IS still high During
the past 10 years, the overall incidence of bacterernlc pneumococwl
pneumonia has Increased (Plouffe et al, 1996; Breiman et al, 1990. Hedlund
et al, 1995; Foster et al, 1994). Reports from a study conducted at Ohio,
state an Increased Incidence of 1.2 fold between the year 1991 and 1993
(Plouffe et at, 1996) among persons above 65 years of age. In Sweden, the
lncldence of pneumonia among persons 65 years of age and older was 11.7
per 1000 in the year 1995 (Ortqv~st, 1999). Globally, pneurnococcal
pneumonia is responsible for nearly 1.2 mllllon deaths per year and nearly
40% of all pneumonia deaths in children less than 5 years of age
(Mulholland, 1999; WHO, 1994). In the United States, 500,000 cases of
pneumonia are reported annually (Watson, 2000).
Annual mortality rate of 1-5% has been reported worldwide for lower
respiratory tract infections in infants (Tyeryar et al, 1978). Studies conducted
at Scotland reports a mortality rate of 24% (McKenzie et al, 2000). Case
fatality rates with bacteremic pneumococcal pneumonia in adults are 2040%
in the United States. It was reported to be 1 in 10 among all age groups

above 20 years of age (Mufson et al 1999) denoting an Increasing rate w~th
advancing age Case fatality rate was 4 5% In ch~ldren aged 4 years or
younger Reports of case fatality rates from Stockholm and Sweden were 7%
and 11% respectively (Ortqv~st 1993 Ortqvist 1990) Mortality rate of
7 36% due to pneumococcal pneumonia has been reported by Marrie
(1999) In a study conducted by Davis et al (1995) In 3 paediatrlc centres
from Sydney a mortality rate of 6 6% was reported
Pneumonia in developing countries:
Every year, 10 million deaths occur in children less than 5 years of
age in low income countries. Out of this, approximately 3 million deaths are
caused by pneumonia (WHO, 1998). Data on mortality are poorly recorded
~n some developing countries and hence the rates may be even higher. In
countries like Gambia, most of the cases admitted to the paediatric hospitals
are reported to be due to pneumonia (Leowski, 1986; Denny, 1986; de
Francisco et al, 1993). The Incidence of pneumonia in the developing
country is up to 10 times hlgher than that in developed countries like United
States (Mccracken, 2003). The mortality rate goes unnoticed despite being
high ~n developing countries since there IS paucity of infoination describ~ng
the pattern of disease. Annual incidence of pneumonia in children less than
5 years is 3-4 per 100 in industrialised countries but it IS estimated to be 10-
20 per I00 in low income countries (Shann, 1996). Studies from a rural area
of West Africa, reveal a case fatality rate of 1% in children w~th pneumonia.
An annual attack rate of pneumonia In chlldren less than 5 years was 4090
out of 100,000 per year in rural area of West Africa (O'dempsey et al, 1996)
According to a study conducted by Board on Science and Technology for
International Development (BOSTID) in Argentrna, Pakistan, Phillpplnes,
Tharland and Uruguay, intidence ranged from between 12.7 to 16.8 new

ep~sodes of acute respiratory lnfectlon per 100 child-weeks at rlsk. 3ates of
lower respiratory infectlons varied from 0.2 to 3.4 new episodes per 100
child-weeks at risk (Selwyn, 1990).
Mortality rate reported among Israeli adults with pneurnococcal
bacteremla was 27.8% (Raz et al, 1997). In a study undertaken in Argentina,
Braz~l, Chile, Colombia, Mexico and Uruguay in under-fives, out of 3,393
children with systemic pneurnococcal infectlons, 1578 had pneumonia.
Around 63.8% of them were under 2 years of age (Hortal et al, 2000)
Indian scenario:
In India, like the other developing nations acute respiratory tract
Infections continue to be the cause of morbidity and mortality. It is the
second most common cause of mortality In children after acute diarrhoea.
According to a compiled data ~nvolving maliy centres in Indla, a rate of 15-
20% mortality rates in infancy (Registrar General of India, 1987) with acute
lower respiratory tract infections accounting for 20-24% deaths were
recorded (Pocket Book of Health Statist~cs in India, 1980). Datta-Banik et al
(1969) and Gupta et al (1982) reported 5-8 episodes of acute respiratory
tract infections per year in urban children and 3-5 episodes in the rural areas.
Stuciies conducted by the lnvasive Bacterial Infection Surveillance
(IBIS) group which Included 6 hospitals in lndia for a period of 4 years in
3,686 pat~ents with suspected pneumonia, a case fatality rate of 19% was
reported Mortality from invasive pneurnococcal disease in lndia has
exceeded 20% in patients excluding those with underlying illnesses (IBIS
Group, 1999). Roy et al (1991) have reported a case fatality rate of 17.6%
during infancy in children with acute respiratory tract infection who were

admitted to a hospital in Calcutta. Morbidity due to ARI was found to be
12 5% in children under 5 years of age from rural area of Delhi by Chhabra et
al (1993). Sehgal et al (1997) have reported a case fatality rate of 10.45%
Acute respiratory infection is responsible for one million deaths and an attack
rate of 3-7/childlyear has been reported. Of these 10-15% are due to acute
lower respiratory tract infections (Reddiah and Kapoor, 1988).
CONTRIBUTORY FACTORS TO PNEUMOCOCCAL PNEUMONIA
The factors responsible for the high incidence of pneumococcal
disease among young children in developing countries are not fully known.
Factors like age, sex, colonisation, nutritional status and underlying
~nfectrons have been found to have causal relationsh~p wlth the spectrum of
pneumococcal infection.
i .Age:
Information regarding high prevalence of Pneumococcal pneumonia in
certa~n ages suggests that disease IS common at the extremes of life. The
inc~dence of pneumococcal bacteremia is relatively high among infants upto
2 years of age and low among teenagers and young adults; rates increase
steadrly beginning at around 55 years (Musher, 1998). Durlng the flrst year
of Ilfe, pneumonia and bronch~olltrs are most common (Glezen et al, 1973)
In children younger than one year of age the annual incidence of invasive
pneumococcal disease was found to be 5541100,000 and ~t was 2401100,000
in chrldren younger than 5 years according to a report from West Africa
(O'dempsey et al, 1996).
In children less than 2 years old, S.pneumoniae is the leading cause
of death (WHO, 1997). It is responsible for at least 1.2 million deaths

annually (Shann and Steinhoff, 1999). Studies conducted at Soweto. South
Afrlca report that an annual incidence ~n children younger than 5 years of age
increased from 6111 00,000 in 198611 987 to 13011 00,000 in 199611 997
(Karstaedt et al, 2000).
According to a study by Scott et al (1996) different serotypes vaned
with regard to age. Serotype 1 was associated with a progressive decline In
relative risk through adulthood whereas, serotype 3 infection increased in the
7Ih decade of life. Serotype 8 had a relative preference for adults. During the
flrst decade of life, serotype 23 and 18 took over. However, no stat~stically
significant Interactions were noted according to thls study.
2.Sex:
Pneumococcal d~sease has a consistent preference for males and the
reason is largely unexplained One of !?e reasons could be the early
reporting and hospitalization of male chlld In contrast to a female child, In
certain low soclo-economlc communities in developing countries. Some
studies report that male female ratlo varies with serotype. Based on the
study by Scott et al (1906), the proportion of all ~solates that were recovered
from male patients was 0 64 (male.female ratio = 1.8:l) The variation of
males between different serogroups was not marked and the overall
association between sex and serogroup was not statistically significant. A
sllght preference for females were seen In 2 serogroups 14 and 23 (Scott et
al, 1996). The male:female ratio reported from a study in a rural area of
West Afrlca was 1.4:l (O'Dempsey et al, 1996).

3.Nasopharyngeal colonization:
S.pneurnon;ae, the most common causative agent of pneumonia,
colonizes the nasopharynx and can be isolated from 5-10% of healthy adults
and from 20-40% of healthy children. Children are more likely to be carriers
of pneumococci than the adults (Musher, 1998). This colon~zation again has
also shorn to be dependent on factors like age, sex, geographical
predeliction, overcrowding and socioeconom~c status (O'dempsey et al,
1996, Howard et al, 1988). Pneumococcal lnfectlon is usually followed by
colon~zation of the nasopharynx, whrch is an important risk factor for the
development of the disease (Gleblnk, 1989). S.pneumoniae can be ~solated
in 25-60% of nasopharyngeal cultures obtained from healthy carriers
(Ingvarsson et al, 1982 and Anianson et al, 1992). In a study conducted at
Pondicherry, South India, in healthy school children between 5-10 years, a
prevalence rate of 24.3% for S.pneu,non~ae colonization was noted
(Kanungo et al, 2000). In another study of nasopharyngeal colonization
among South Indian infants, prevalence rates of 54%, 64.1% and 70.2% in
Infants by age 2 months, 4 and 6 months respectively were reported thus
(Coles et al, 2004) explalnlng the potential r~sk for pneunonia in these
Infants. Studies from Gambia reported a colon~zat~on rate of 76 1% In healthy
ch~ldren (Lloyd-Evans et al, 1996).
4.Malnutrition:
Malnutrition has been incriminated as one of the factors responsible
for the development of pneumonia in children in low income countries (Wolf
and Fleer, 2000). In malnourished children the biological integrity of the
respiratory tract mucosa may be compromised leading to alteration in the
colonisation rate which is one of the predisposing factors for pneumowccal

disease. Studies have proved that mucosal immunity plays an important role
In inhibiting pneumococcal colon~zat~on (Stenfors and Raisanen, 1993).
Decreased serum retinol concentrations can result in impaired mucosal
immunity decreasing the secretory antibody (IgA) which is a nonspecific
barrier defense (Chandra, 1988; Biesalski and Stom, 1992; Semba, 1998;
Sir~sinha et al, 1980). This clearly suggests that malnourished pat~ents are at
a high risk and this association behveen malnutrition and infection together
with insufficient health care services in the community has been responsible
for the high mortality among chlldren in low income countries (Wolf and
Fleer, 2000). Studies also suggest that reversal of Vitamin A deficiency may
reduce the rate of colonization and ultimately decrease the morbidity rates
associated with the infection (Coles et al, 2001).
5.Underlying infections:
Pneumococcal infections are associated with certain predisposing
illnesses and usually ~t occurs at the extremes of age (Burman et al, 1985).
The usual risk factors associated in an adult include alcoholism, Human
Immunodeficiency Virus (HIV) infection, splenectomy, multiple myeloma,
connective tissue disease, steroid therapy, dlabetes mellltus and intravenous
drug use (Burman et al, 1985; Janoff et al, 1992; Musher, 1992) In children,
Increased incidence has been assoc~ated with sickle cell anaemia (Musher,
1992 Barrett-Conner, 1971; Wong et al, 1992) Increased incidence of
pneumococcal infection can also be due to defects in host defense
mechan~sm like congenital or acquired defects in antibody production,
neutropenia, dysfunction of white blood cells (WBC), complement
deficienc~es or splenic dysfunction (Musher, 1995).

In patients infected with HIV, respiratory tract infections are very
common (Nathoo et al, 1993; Bobat et al, 1998). Studies from rural Zambia
and urban Zimbabwe suggests that HIV infection was a strong predictor of
severe morbidity and mortality from acute lower respiratory tract infection
(Smyth et al, 1997; Nathoo et al, 1993) in part~cular due to S.pneumoniae. A
study conducted to determine the impact of HIV on the epidemiology of
invasive pneumococcal infection in South Africa revealed that the burden of
severe invasive pneumococcal disease was 41.7 fold more In HIV infected
compared with uninfected children (Madhl et al, 2000) Another study
conducted In South Africa reported a high incidence of pneumococcal
bacteremla in children which doubled due to the impact of HIV epidemic
(Karstaedt et al, 2000)
The other underlying conditions predisposing pneumococcal d~sease
Include hospitalization, c~rrhos~s of the liver, renal insuffic~ency, viral
resp~ratory Infections, allergies, cigarette smoking and COPD (Musher,
1998)
ETIOLOGICAL AGENTS OF PNEUMONIA
Identifying the etiologic agent responsible for pneumonia IS
challenging mainly because of diff~culty in acquiring adequate material for
diagnosis of the infection and also due to lack of reliable diagnostic methods
(Isaacs, 1989; Lode et al, 1993; Shann, 1986). Difficulty in identifying the
causative agent in pneumonia is a major drawback In instituting speciflc
treatment and preventive measures.

In a study by Socan et al (1999) on the mlcroblal etlology of
community acqulred pneumonia In hospltalised adult patlents (>I5 years)
S pneumonrae was the bacterium ~solated most frequently (5 7%) 9 5% had
Chlamyd~a pneumonlae 5 7% had Mycoplasma pneumon~ae and 24 1 % had
vlral lnfectlon Bacterial pneumonia was dlagnosed In 39 8% patlents of
bhich 23 had concurrent vlral infection Pneumonia caused only by vlral
agents were dlagnosed In 28 patlents out of the total 211 patlents whlch
formed the study population
Etiology of pneumonia in children:
Pneumonia is a major cause of morbidity and mortality in children in
low income countries. In children, nonbacterial pneumonias are the
frequently seen pulmonary Infections (Correa, 1996) Respiratory syncytial
virus is the commonest agent particularly in infants, followed by
parainfluenza virus, adenovirus and influenza virus. Another leading cause
of pneumonia is Mycoplasma pneumoniae in chlldren (Boyer et al, 1992)
over 5 years of hge. Chlamydia pneumoniae has been reported recently as
an Important cause of community acquired pneumonia among children,
between 5-14 years cf age (Grayson 1994). With respect to the bacterial
pneumonlas, S.pneumoniae appears to be the predominant etiological agent
(Correa, 1996). Incidence of pneumonia due to Haemophilus influenzae has
decreased significantly owing to the success of H.rnfluenzae type b (Hib)
vaccine in the developed nations. However, it is still an important cause of
pneumonias in some developing countries where this vaccine is not yet
~vailable (Klein, 1992). Concurrent viral infection along with bacterial
pneumonia has been reported in 25-75% of children from a children's
hospltal of Northern California, Oakland (Turner et al, 1987). Several studies
have reported S.pneumoniae and H.influenzae as the leading bacterial cause

and RSV, the leading viral cause of pneumonia (Silverman et al, 1977;
Shann, 1986; Avila et al, 1990; Forgie et al, 1991; Greenwood, 1992; Forgie
et al, 1992; Adegbola et al, 1994; Sutmoller et al, 1995; Falade et al, 1997).
Studies from Afr~ca, Asia and Latrn America have reported S.aureus as
another common organism, in children with prior vlral respiratory infection
(Gonzaga et al, 1990). Rarely, Gram negative bac~lli have been incriminated
as a cause ot pneumonia in normal Infants and children in developed
countries (Bang et al, 1993). Moraxella catarrhalis is currently recognised as
the third most common pathogen of respiratory tract after S.pneumoniae and
H.influenzae (Wolf and Fleer, 2000).
Studles from develop~ng countr~es lncludlng lndla have shown that
S pneumoniae and H influenzae are the 2 most predominant bacter~a Isolated
from acute lower respiratory tract ~nfect~ons (Berman 1991) The estimated
case fatallty rate of bacter~al pneumon,a due to Spneumon~ae and
H influenzae In develop~ng countries is 50% more than that due to resplratory
syncyt~al virus and para~nfluenza vlrus (PIV) (Berman 1991) From a report
from Pondlcherry lnd~a 2096 of the ~solates of H ~nfluenzae were non-type b
stralns Prevalence rate of acute lower resplratory tract ~nfectlons was 6 4%
due to Chlamydra pneumoniae (Chaudhry et al 1998) Serological evidence
of pneumonia due to Legionella pneumophila has been reported In 4 out of
45 pat~ents In Bombay Overall incidence of 16 6% of pneumonia associated
w~th Mycoplasma pneumoniae was reported In 1972 by Ayyagarl et al
Detect~on of M pneumoniae has been posltlve by culture In 10 5% of cases
24 samples out of 43 by PCR and 20 out of 43 samples by culture
(Ramamoorth~ et al 1996 N~sar et a1 1998)

Pandey et a1 (1998) reported an incidence of 30% by using a panel of
tests like culture, antigen and antibody detection assays to demonstrate
M.pneumoniae infection in children below 5 years of age. John et a1 (1991)
reported 38% of upper respiratory ~nfect~on (URI) cases and 49% of lower
respiratory infection (LRI) due to vlral agents by conver~tional methods.
Agents associated were RSV (32%) followed by PIV (10.8%), influenza
vlruses (1.5%) and adenovirus (3.6%). Study from Lucknow, India reported
RSV infect~ons in 5%, PIV in 7%, influenza viruses in 4% and adenovirus in
5% (Jain et al, 1991) V~ral etiology was reported in 43.5% of lower
respiratory tract infection where RSV had the maximum association (60%),
followed by influenza v~rus (14.5%), PIV (11.5%) and adenovirus (1.5%)
(Ma~treyi et al, 2000).
In HIV Infected ch~ldren who are at a greater r~sk of develop~ng
pneumonla S pneumoniae IS agaln one bf the most frequently Isolated
agents (Madh~ et al 2000) Reports from Southern Afr~ca suggests that
pneumonla due to H influenzae S aureus Klebaella sps, E COB and
Salmonella sps are also seen In HIV Infected ch~ldren (Nathoo et al 1993)
Clinical features:
The signs and symptoms of bacterial pneumonia vary with bacterial
pathogen, the age of the patient and the severity of the disease (Klein, 1998).
Infants: In infants, it is characterized by a mild upper respiratory tract
~nfect~on wth stuffy nose, fretfulness and diminished appetite. This mild
~llness of several days duration ends with abrupt onset of fever of 3g°C or
higher, restlessness and respiratory distress. The patient appears ill with
moderate-to-severe air hunger often with cyanosis. The respiratory distress

is man~fested by grunting, flaring of the alaenasi, retractions of the
supraclavicular, intercostal and subcostal areas, tachypnea and lachycard~a
(Behrman et al, 1992). This is reflected by the proliferation of bacteria and
the inflammatory response In the alveol~.
Children: The signs and symptoms are similar to those of adults.
Symptoms and signs of pneumonla in children may be classified for
convenience into five categories: nonspecific manifestations of Infection and
toxic~ty; general signs of lower respiratory tract disease; signs of pneumonia;
signs of pleural fluid and signs of extrapulmonary disease (Klein, 1998).
Respiratory rates are correlated inversely w th age dur~ng the I* 3
years of l~ fe and vary between a medlan of 47 breathslm~n ~n the l d month of
llfe to 381m1n at the end of 1' year to 28Im1n by 3 years of age In case of
older ch~ldren the respiratory rate varies between 15 and 25im1n Based on
these flndlngs, to dlagnose ALRl tachypnea IS deflned as 50 breathslm~n In
Infants I-; 1 months of age 401m1n In ch~ldren 1-4 years of age and 30lm1n In
children 5 years of age or older (Korpp~ 1995)
Radiographic findings:
Failure to recognize various rad~ological presentations by the
physicians is a problem often compl~cat~ng the diagnosis of pneumococcal
pneumonia. Pneumococcal pneumonla can appear with a variety of
radiological patterns leading to difficulty in making a specific bacteriologic
diagnosis ~n patients with bacterial bronchopneumonia (Kantor, 1981)
However, in pat~ents wth a classic lobar presentation, the clinical symptoms
and roentgenographic findings are often characteristic, and an etiological
diagnosis can be made, based on these findings (Davies et al, 1996).

The radiographic diagnosis of pneumonia is made on the basis of
pulmonary perihilar linear opacities or infiltrates (airways disease) andlor
consolidatlon (airspace disease) (Friis et al, 1990; Swischuk et at, 1986;
Khamapirad et al, 1987).
In most cases of pneumococcal pneumonia, the chest X-ray reveals
an area of infiltration involving less than a full segment. Whereas, In young
adults, true consolidation with an alr bronchogram is seen. A moth-eaten,
less homogenous appearance IS seen In pneumonia superimposed on
severe chronic lung disease. In half of the cases, segmental or lobar
consolidatlon is apparent (Musher, 1992)
General laboratory findings:
In majority of the patlents wth pneun~ococcal pneumonia, white blood
cell count (WBC) is >12,000 cellslpl. However, the count can be as low as
~ 6 0 0 0 cellslpl in 5-10% of persons hospitalized for pneumococcal
pneumonia. This decreased count is often not because of bone marrow
suppression and tbe outcome of thls findlng may be fatal (Musher, 1998) A
study by Korppi et al (1993)reports elevation of C-reactive protein
concentrations (CRP), erythrocyte sedimentation rate (ESR) levels and WBC
counts by 25%, 40% and 36% respectively in patients with pneumonia. This
f~ndlng of elevated WBC counts are independent of age. C-reactive protein is
more often elevated in patients wth bacterial infection alone than in those
patlents with viral or mixed viral-bacterial infections. However, correlation of
pneumococcal etiology with nonspecific indicators of a bacterial infection like
elevated WBC, CRP amd ESR is poor (Korppi et al, 1993).

Microbiological diagnosis:
Optimum treatment of any infection requires definition of the etiologic
agent. For the diagnosis, efforts should be made to obtain adequate and
appropriate clinical materials. Viral and bacterial pathogens responsible for
lower respiratory tract infections produces a variety of cllnical spectrum
ranging from mild illness to life threatening pneumonias. Using various
clinical specimens, isolation of that particular pathogen is possible.
Alternative technique for conventional tube cultures to culture virus, which
take several days to weeks for isolation and identification, is the
centrifugation enhanced culture combined with indirect immunofluorescence
stalning on direct smears as described by Gleaves et al (1984) for isolation
of RSV.
Apart from culture, other rapid methods include antigen detection
assays These assays are simple and rap~d techniques where the antigens
of the pathogen is detected from the clinical specimens like serum, urine,
sputum, pleural fluid etc. Antigen can be detected by various techniques llke
Co-agglutination, Counter-immunoelectrophores~s, Latex agglutination,
lmmunofluorescenca tests and Enzyme immunoassay (Coonrod and Rytel
1973; Chattopadhya et al, 1992. Whitby et al 1985; Chaudhry et a l 1998)
lrnmunofluorescent stainlng with monoclonal antibodies is also a preferred
method (Broor et al, 1999).
Detection of antibodies to various antigens has been demonstrated by
enzyme immunoassays, complement fixation test and micro-
immunofluorescence test. The other methods employed for the diagnosis
include antigen capture enzyme immunoassay and monoclonal immunoblot
assay (Kok et al, 1988; Madsen et al, 1988, Hirschberg and Holme, 1991).

Molecular techniques available include detect~on by nucleic acid
probes or PCR, DNA probe hybridization uslng specific primers and probes
which help in the rapid detect~on of respiratory viruses (Sullender and Wertz,
1991; Paton et al, 1992; Class et al, 1992; Gilbert et at, 1996; Maitreyi et al,
2000) Multiplex quantitative reverse transcription PCR enzyme hybridization
is another molecular technique which has been descr~bed for rapid and
s~multaneous detection of multiple viruses.
PNEUMOCOCCUS
In the year 1880, George Miller Sternberg isolated pneumowccus for
the f~rst time. It was also isolated by Louis Pasteur in the same year. In the
year 1882, Friedlander identified a bacterium from the lungs section which
was s~milar to pneumococci by Grem's technique. Initially, this bacterium
was named as Diplococcus pneumoniae (1926) based on its appearance in
Gram-stained sputum. In the year 1974, the organism was renamed
Streptococcus jneumoniae since it grew in chains in a liquid medium
(Austrian, 1999).
Typing of pneumococcl based on the nature of the capsular
polysaccharide was discovered helping in the serum therapy of
pneumococcal pneumonia Followng this, pneumococcal vaccine was
introduced in 1927 based on the d~scovery of the immunogenicity of
pneumococcal capsular polysaccharides by Schieman and Casper (Austrian,
1999).

Some of the major contributions of molecular biology and medic~ne
resulted from studies of pneumococcus. Studies with S.pneumoniae has !ed
to the identification of the first polysaccharide antlgen, genetic recombination
mechanisms, identification of DNA as the genetic matertal, m~crob~al
hormone inducing and controlling the physiological state of competence and
identification of the first bacterial autolysin (Tomasz, 1999). Apart from all
these findings, S.pneumoniae has played an important role in the history of
antimicrobtal therapy.
Finally, the history of pneumococci can be concluded with a quotation
from Benjamin White's Monograph (1937), "opportunities for enquiries into
the ways of pneumococcus are by no means exhausted. The prosecution of
future studies on the life, activities of pneumococcus cannot fail to bring new
gold to the abundant store of bullion already accumulated" (Austrian, 1999).
General properties:
S.pneumoniae is a Gram positive coccus that replicates in chains in
liquid medium. They usually occur in pairs or In short chains. The coccus is
nearly 1 pm in diameter. The diplococcus is ovoid or lanceolate shaped, with
their distal ends narrowed. They are nonmotile and nonsporing (Duguid and
Ross,1 989).
Pneumococcus is an aerobtc and facultative anaerobe. It requlres alr
or hydrogen with 5-10% COz with an optimum temperature of 37% for its
growth. When pneumococci grows on media containing glucose vhich
stimulates growth (energy source) there is the formation of acid which leads
to cessation of growth. This could be prevented by addition of blood and

serum which was shown to protect them from hydrogen peroxide formed
durlng ~ t s growth (Colrnan, 1990).
Pneumococc~ produce alpha haemolysin which breaks down Hb
producing a green colour and as a result pneumococcal colonles are
surrounded by a green zone durlng growth on blood agar plates Colonies
on blood agar are small transparent and glittering that tend to d ~ p down in
the centre and resemble a doughnut or draughtsrnan form Colonles of type
3 are usually larger and have a mucold appearance After anaerobic
lncubatlon on blood agar and a subsequent period at 6°C zones of a-
haernolysls appear around the colonles especially for the colonies close to
the dlscs contaln~ng antlblotlcs which act on the cell wall of the bacterium
Pneumococci tends to die in cultures within 24-48 hours. Once the
bacterium dies, it gets autolysed. The blle or other detergents activate the N-
acetylmuramyl-L-alan~ne amidase wtlch IS responsible for the lysis of
cultures of pneumococci.
Important tests used routinely in a laboratory to identify pneumococci
Include (1) Alpha haemolysls on blood agar, (2) Catalase negativity, (3)
Solubility in bile salts, (4) Susceptibility to ethyl hydrocupreine (Optoch~n)
hydrochloride, (5) lnulin fermentation.
More than 98% of pneumococcal isolates are susceptible to optoch~n
Reports of optochln resistant pneumococcl have been described (Kontlalnen
and Slvonen, 1987, Munoz et al, 1990) Alternative methods have been
evaluated to ldentlfy pneumococcl such as the pneumosllde test (BD

Diagnostics, Cockeysville, MD) and Accuprobe S.pneumoniae culture
identiflation test which is a DNA-based test (Geneprobe, Sandiego).
Animal pathogenicity:
Pneumococci isolated from infective conditions are mostly virulent for
the mouse except serotype 14 which is avirulent (Duguid and Ross, 1989).
Peritonitis, septicemia and death of the mouse results on intraperitoneal
inoculation of pneumococci. Because of this fact, mouse serves as a
selective animal model facilitating the isolation of scanty pneumococci from
clinical specimens. Currently, much of the molecular work such as studies on
mutations In the various genes of pneumococci are carr~ed out using mouse
as the animal model (Berry et at, 1999). Studies on virulence of d~fferent
mutants of S.pneumoniae are also carried out in mice after intranasal or
intraper~toneal challenge (Berry et at, 1989) Rabbits are also hlghly
susceptible to pneumococci and are predomnantly used to ralse ant~bodies
against various antigens of pneumococci like pneumolys~n and capsular
polysaccharides (Cima Cabal, 1999; Lund, 1978).
Structure:
Cell wall:
The outermost structure on the surface of the non-encapsulated
pneumococcus, is composed of an electron-dense outer and inner band, and
enclosing a less electron dense band, represents the pneumococcal cell wall.
Whereas in an encapsulated pneumococci, this trilaminated structure is
covered fram outside with a less structured layer of polysacchar~de capsule
(Tomasz, 2000).

Pneurnococcal replication:
Pneumococc~ divide in a single plane in the central equatorial region
of the cell and the site of incipient septum is marked by a morphological
alteration at the cell wall, which appears as a "hump" of the cell wall located
at the middle of the cell surface. The equatorial ring is made of cell wall
material and the next event involves the division of the eqyatorial ring into
two which may be due to the action of autolysin. This splitting event
coincides with the formation of septum. The cell wall enveloping the dividing
bacterium between the equatorial ring and the septa1 tip is one generation
younger in biosynthetic age than the cell wall between the equatorial rings
and the left or right poles of the bacterium (Tomasz, 2000). It is known that
pneumococcus may engage in a new cycle of cell division before the physical
separation from the daughter cell is accomplished. This leads to the
appearance of a cham of cells in cultures
Pneumococcal cell organisation:
Plasma membrane:
Plasma membrane represents the five osn~iophylic bands ~nslde the
cell wall which stain with different intens~ty It IS a unit membrane, with band 1
representing the inner leaflet, band number 3 the outer leaflet, band number
5, the inner surface of the cell wall and band number 4, represents the
structural or functional analogue of periplasmic space found In Gram
negative bacteria. A number of bridges or invaginations connect the plasma
membrane and the cell wall representing a close anatomical andlor functional
interd~gitation of the plasma membrane and the cell wall in pneumococcl

Cytoplasm:
Pneumococci has a cytoplasm containing an evenly distributed, large
number of electron dense particles wth the dlameter of approximately 150A.
representing the ribosomes and polysomes (Tomasz, 2000).
Membranous organelles:
These organelles are usually referred to as "mesosomes" or
"chondrioids". However, the function of these organelles are not known. It is
simply referred as intracellular membranes. It is reported that due to
peculiarity of these intracellular membranes In their assocratron \nth septa
and alignment of pairs of these intracellular membranes with the dividing
chromosome, it may be involved with the equatorial biosynthesis of cell wall
or rn the separation of chromosomes during cell div~sion (Tomasz, 2000).
Nuclear region:
It is represented by the centrally located low electron densrty region
which is filled with packed fibrils of uniform 25-30 A width. These fibrils
represent the appearance of bacterial chromosome.'
Morphology of S.pneumonrae was made possible with the help ot high
resolution electron microscopic study of a laboratory strain R6 which is a
derrvative of R36A. This strain represents the prototype of the
pneumococcus and has been extensively used for the characterization of the
complete genome of S.pneumoniae. The clinical isolate, serotype 2 was the
parent strain of R36A (Tomasz, 2000)

Chromosome structure:
By fragmentation of genomic DNA of S.pneumoniae with low-
frequency-cleadage restriction endonucleases and separation of the
fragments by field-inversion gel electrophoresis (FIGE) it is possible to get a
DNA-finger-print of a strain. This process helps in constructing a physical
and genetic map of the R6 laboratory strain The ability to separate large
fragments of DNA by pulsed-field gel electrophoresis has provided the
technology to map bacter~al chromosomes. Genetrc markers are located on
the map of chromosome of S.pneumon1ae Th~s method IS being used to
compare the profiles of several strains and also for typing S.pneumoniae
strains (Lefevre et al, 1993). Genes in S pneumoniae were identified by DNA
sequence sampling and gene disruption system was developed to identrfy
several potential lethal targets for antibiotic intervention (Baltz et al, 2000).
VIRULENCE FACTORS
The subcapsular surface components ,i.e, the cell wali and
Iipopolysaccharide) of bacteria are the rmportant determinants of
inflammat~on apart from the other components like pili and polysaccharide
capsule. Evidences are available, indicating the role of pneumococcal
proteins in the pathogenesis of disease, either as mediators of inflammation
or by directly attacking host tissues (Paton et al, 1993). The three major
proteins contributing to the virulence of the organism include the toxin
pneumolysin, the major pneumococcal autolysin and pneumococcal surface
protein A) Other enzymes contributing to the virulence of S pneumoniae are
neuraminidase, hyaluronidase and lgAl protease

Surface components of pneumococci:
Capsule:
The presence of capsule was first reported as type-specific soluble
substance in filtrates of pneumococcal cultures and in the sera and urine of
infected person. Later on, this specific-soluble substance was k n o w as type
specific capsular polysaccharide (CPS). Discovery of the antigenicity of CPS
led to the development of pneumococcal vaccines. This was the flrst non-
protein substance discovered to be antigenic in humans (Kamerling, 2000).
Based on the nature of its capsular polysacchar~de. Spneumonrae
has been divided into several serotypes Two different systems of
nomenclature exlst for the pneumococcal serotypes viz, the Danish system
and the American System. Danish system is based on the cross-reactions
between d~fferent types and the cross-reactive types are included under a
common serogroup, with individual serotypes within each group distinguished
by the trailing letter Whereas, according to the American system, numbering
of serotypes are based on the order at which they are discovered and it does
n ~ t recognize antigenic cross-reactivity among types (Kamerling, 2000)
There are 90 serotypes to date, which are distinguished by chemical
differences in their capsular polysacchar~des and also by the ability of the
immune system of rabbits to recognize these structural differences and to
respond with specific antibodies against the antigens of each different type
(Shapiro, 1991) Typing methods include Capsular reaction test, Latex
agglutination, Co-agglutination and Capillary precipitation. Newer methods
include the use of DNA probes and DNA sequence-based subtyping
(Henrichsen, 1999).

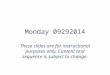
PATHWAY OF BIOSYNTHESIS OF CAPSULAR POLYSACCHARIDES
TC;: phog lucomut ase
UTP ~~ i~o~I~Pho~pha le Uridylyl transferare
UDP-Glc + Ppi ""4 UD-Glc dehydrogenase
NaDH
UDP-GI Type 3 capsular polysacchande synthase
Biosynthetic pathway for type 3 CPS
Fig.1. Proposed biosynthetic pathway for type 3 CPS (Dillard et al, 1995)
Using the traditonal methods of structural analysis, the structure of
CPS was analysed in the year 1964 and was re-examined by Larm and
Lindberg in the year 1976 (Kamerling, 2000).
As a virulence factor:
Capsular polysaccharide is one of the component of S.pneumoniae responsible for the virulence of the bacterium. The function of capsular

polysaccharide (CPS) is to protect the pneumococci from phagocytosis by
polymorphonuclear leukocytes.
As early as 1928, Griffith reported that unencapsulated pneumococcal
variants were avirulent (Garcia et al, 2000). Loss of the capsule is
accompanied by a 100,000-fold reduction of the virulence of S.pneumoniae
and it was found that nonencapsulated pneumococci were readily
phagocytized M e n added to a suspension of leukocytes In normal serum,
whereas mucoid, capsulated organisms were resistant to phagocytosis and
multipl~ed rapidly. Although the chemical composition of the capsule plays
an ~mportant role in the virulence, a quantitative relationship between the
amount of type-specific polysaccharide and v~rulence has been reported
(Garcia et al, 2000).
Host defense mechanism agalnst S.pneumoniae IS based on humoral
immun~ty, that IS, antibodies directed to the CPS can protect humans to
infections with viable pneumococci (Kamerling, 2000). Function of CPS in
preventing ingestion and Killing by phagocytic cells is due to hidlng the FC of
IgG that reacts with cell wall and the C3b that is fixed during that reaction or
by the alternative complement pathway (Musher et al, 2000).
Virulence of pneumococci is determined by the chemical composition
of the capsule and to a lesser extent, its size (Knecht et al, 1970).
CPS, which is purified, does not elicit any inflammation when it is
~nstilled directly into the lung in contrast to unencapsulated pneumowcci,
vhich have inflammatory properties (Tuomanen et at, 1987). However, CPS
is not required for inflammation but favour the progression of the infection

due to its property of inhibiting phagocytosis. Owing to its antigenic nature, it
is able to elicit the production of serotype-specific, protective antibody.
Currently, a total of 90 serotypes of S.pneumoniae has been recognized
which includes 21 serogroups.
Pneumococcal capsular types vary significantly in their virulence.
Type 3 is highly virulent because of formation of a larger capsule ~ 4 t h the
requirement of only one colony forming unit to produce a lethal infection in a
mouse. Also, the case fatality rate 1s 50% for a penicillin treated type 3
bacteremlc pneumococcal pneumonia (Austrian, 2000) whereas type 37
which also has the same capsular slze as that of type 3 is a rare cause of
any lnfectlon and a larger dose 1s required to produce an infection in mouse.
Serotypes 3, 4 14 and 19 predominate in ~ t s isolation from the blood
stream or they are more vlrulent In case of infants and chlldren lnfectlon
can occur no matter what the type colonized - serotypes 6, 14, 19F and 23F
are seen to be common (Gray et al, 1980) Whereas in adults thls does not
hold true Stud~es have been conducted to determ~ne the virulence of each
serotype and ~t has been found that the serotypes 1,2 3,5,8 and 12F appear
to be most vlrulent (Heffron 1979 Austra~n 1981)
Genetic analysis:
Capsular polysaccharide of S.pneumon~ae has an Important role in the
development of molecular genetla. Genetic exchange of DNA among
S.pneumoniae strains seems to have an important role in the generation of
new strains and in the evolution of capsular serotypes (Henrichsen, 1995;
dan Dam et al, 1990).

Genetic evidence indicated that the genes responsible for capsular
polysaccharide biosynthesis were closely linked in the pneumococcal
chromosome and could be transferred as a unit during transformation (Garcia
et al, 2000). Inter-type transformation takes place when the donor DNA
displaces the resident capsular genome and it was assumed that this
interchange was mediated by homologous sequences flanking the type-
specific gene cluster.
Role of capsular polysaccharide in diagnosis:
Soluble pneumococcal capsular polysaccharide was f~rst shown in the
circulation of patients wth pneumococcal pneumonia more than 50 years ago
(Coonrod and Drennan, 1976). Due to the insensitivity of the tests available
for detecting circulating polysaccharide, efforts to evaluate the balance
between antigen and antibody in the serum in pneurnococcal pneumonia
were hindered.
Capsular polysaccharide antigen has been detected from various
clln~cal samples like urine, transtracheal secretion, serum, CSF and sputum
by techniques like Co-agglut~nation, Latex agglutination and Counter
~mrnunoelectrophoresis (Coonrod and Rytel, 1973; Kronvall, 1973; Burman et
al, 1991; Singhal et al, 1996).
Studies on measurement of anticapsular antibodies have been
reported by various workers by enzyme-linked immunosorbent assay (ELISA)
(Barett et al, 1980; Shyarnala et al, 1988, Korppi et al, 1992; Korppi et al.
1993 and Musher et al, 2000). ELISA has been used to measure IgM, IgG
and IgA antibody concentrations.

Immune complexes containing type specific CPS has been studied in
the sera of children with lower respiratory tract infection by Korppi et al
(1998). Holloway et al (1993) has also developed ELlSA for the
demonstration of circulating pneumococcal IgG immune complexes in
patients with community acquired pneumonia. From the dissociated
circulating Immune complexes pneumococcal capsular antigen was
demonstrated by latex agglutinat~on.
Role of capsular polysaccharide in prevention:
Pneumococcal polysaccharide vaccines
Although llcensed vaccines against invasive pneumococcal disease
are available in the United States, Europe and other countries, their use IS
l~m~ted (Poland, 1999). Currently available pneumococcal vaccines,
manufactured by Merck and Company (Pneumovax 23; Nest Po~nt
Pennsylvania), Lederle Laboratories (Pnu-Immune 23; Wayne, New Jersey)
,and Pasteur Merieux (Pneumo 23, Lyon, France) contain 25 ~g of each of 23
purlfled capsular polysaccharide antigens of S pneumoniae (Serotypes 1. 2,
3, 4, 5, 6B. 7F, 8, 9N, 9V, IOA, I l A , 12F, 14, 158, 17F, 18C, 19A, 19F, 20,
22F, 23F and 33F). According to the data from surveillance conducted by
the Centres for Disease Control and Prevention (CDC), these 23 capsular
types represent atleast 85-90% of the pneumococcal serotypes causing
invasive infections among children and adults in the United States.
Pneurnococcal capsular polysaccharide antigens induce serotype-
specific antibodies that enhance opsonlzation, complementdependent
phagocytosis and killing of pneumococci by leukocytes and other phagocytic
cells. Concentration of antibodies to pneumowccal polysaccharides begin to
increase within 1 week afler vaccination and remain elevated for over 5 years

In healthy adults (Mufson et al, 1983; Mufson et al, 1987; Musher et al,
1993). The overall efficacy against lnvasive pneumococcal disease among
immunocompetent persons greater than 65 years of age is 75% (Butler et al,
1993).
Recently, prevention of pneumococcal infection by vacc~nation has
become Important In light of the emergence and spread of drug-res~stant
strains of pneumococci (Hoffman et al, 1995, Butler et al, 1996). Innovative
strategies to improve the protectlon prov~ded by the pneumococcal
polysaccharide vacclne are under evaluation.
Limitations of Pneumococcal polysaccharide vaccines:
Though the pneumococcal polysaccharide vaccine is effective against
pneumococcal invasive Infections in adult patients, immunization has not
been protective ~n infants and young children as these vaccines are not
sufficiently immunogenic in these age groups (Fedson et al, 1999; Makela et
al, 1980; Karma et al, 1985; Riley et al, 1986). Therefore, this vaccine is not
recommended for children <2 years of age (Eskola, 2000). It is known to
c ~ n f e r only limited protectlon to patients with certain underlying illnesses
Conjugate Pne~mococcal vaccines:
Development of pneumococcal conjugate vacclnes offers the potentla1
beneflts of prevent~on of pneumococcal d~sease In populations that are
unable to generate an adequate Immune response to polysacchar~de
vacclnes (Bruyn and Van Furth, 1991) By conjugating a capsular
polysaccharlde wlth an lmmunogenlc proteln the Immune response changes
from a T-cell Independent response, wh~ch IS poorly developed In ch~ldren <2
years of age, to a T-cell dependent response enhanc~ng protective antlbody

formation and ~mmunologic memory in infants and young children (Watson,
2000). Common protein carriers include diphtheria toxoid, tetanus toxoid, the
CRM 197 nontoxic cross-reactive variant of diphtheria toxin (Pnc CRM) and
men~ngococcal outer membrane protein complex (Pnc-OMPC).
Measurement of serum antibody concentrations help in the evaluation of the
immunogenicity of pneumococcal conjugate vaccines.
Pneumococcal conjugate vaccines have proven to b e safe in clinical
trials. Two separate efficacy field trials of pneumococcal conjugate vaccines
were initiated in 1995 at Northern Kalser Permanente and in Finland.
Efficacy of 2, 7-valent conjugate vaccines against otitis media were evaluated
in Flnland (Eskola et al, 1998). A surveillance trial was conducted in
Northern California, vhich evaluated the efficacy of pneumococcal CRM
conjugate vaccine against the primary endpoint of invasive pneumococcal
infections caused by serotypes included in the vaccine in -38,000 ~nfarts
from a multiethnic population. The efficacy of Pnc CRM vaccine aga~nst
pneumonia and otitis media evaluation produced a significant (p < 0.01)
reduction in ali episode of otitis media among fully vaccinated children
(Shinefield and Black, 2000). Based on a study on the evaluation of
irnmunogenicity and reactogenicity of a pneumococcal conjugate vaccine
adm~n~stered comb~ned with a H.inf/uenzae type b conjugate found well-
tolerated, safe and immunogenic when adm~nistered as a separate or as a
comblned 7V PncIHbOC lnjection (Choo et al, 2000)
LlPOTElCHOlC AND TElCHOlC ACID
Lipoteichoic acids (LTAs) and teichoic acids (TAs) are the polymers of
+he cell wall membrane complex in a Gram positive bacteria. LTAs and TAS
of pneumococci are unique because they possess identical repeat and chain

structures unlike other Gram positive bacteria vhich are structurally and
biosynthetically distinct entities (Fischer, 2000).
Previously, pneumococcal TA was described as C-polysaccharide by
Tillet et al in the year 1930. After 13 years, pneumococcal LTA was isolated
by Goebel et al and named as lipocarbohydrate or pneumococcal F-antigen
because of its fatty acid content and immunological properties (Fischer,
2000). The two polymers differ immunologically, as Forssman antigenicity is
associated with LTA (Briles et al, 1973; Behr et al, 1992). By
~mmunoelectron microscopy, it was proved that C-polysaccharide is uniformly
distributed on both inside and outside of the cell walls and LTA on the
surface of the cytoplasmic membrane (Sorensen et al, 1988). N-acetyl
galactosamine and choline are the components of C-polysaccharide
(Tomasz, 1967; Kilpper-Balz et al, 1985; Garcia et al, 1986). However, it is
known that choline is an essential growth factor of pneumococci.
As a virulence factor:
Cell wall has the highest ability to cause inflammation than the
capsule or cytoplasm. Signs and symptoms of infection induced by cell wall
mlmlc that of livlng bacteria in animal models of invasive pneumococca!
infections (Tuomanen et al, 1985; Tuomanen et al, 1987, Ripley-Petzoldt et
a1 1988)
The TAs and LTAs are strongly associated with acute inflammation by
activating the alternative pathway of the complement cascade and also binds
the acute phase reactant C-reactive protein. It also activates the
procoagulant activity on the surface of endothelial cells, promotes cytokine
release initiating the influx of leukocytes (Winkelstein et al, 1978; Riesenfeld-

Orn et al, 1989; Geelen et al, 1993). Recently, it has been reported that IL-2,
an important component inducing cell mediated immunity, is induced by
pneumococcal cell wall (Cleveland et al, 1996).
Tha peptidoglycan portion of the pneumococcal cell wall 1s a potent
stimulus of blood brain barrier permeability. It is also cytotoxic to cil~ated
cells of the choroid plexus, neurons and can induce sleep (Spellerberg et al,
1995)
AUTOLYSIN
Autolysins are enzymes that degrade different bonds in the
peptidoglycan and eventually cause the lysis and death of the cell. Substrate
and bond specificities are exhibited by these enzymes. Most of the
organisms contain lytic enzymes.
S.pneumoniae contalns a powerful autolytic enzyme, an amidase,
which is the best characterized autolysin described so far (Lopez et al, 2000).
The major pneumococcal autolysin is a 36-KDa N-acetyl muramic and L-
alanine amidase located in the cell envelope (Paton et al, 1993) The
enzyme is bound to choline residues of lipoteichoic acid (Forssman antigen)
which in turn is anchored to the cell membrane. Cells growing in
ethanolarnine-containing medium, contain an inactive form of the amidase
which can be activated by incubating at low temperature with choline-
containing cell walls (Tomasz, 1981).
Attempts to isolate autolysin-defective mutants were tried which
helped in cloning and sequencing a gene (lyt A) coding for a bacterial
autolysin (Garcia et al, 1985). Cloning of lyt A also helped in the isolation of

genes encoding the cell wall lytic enzymes from pneumococcal
bacteriophages (Garcia et at, 1986; Garcia et al, 1987; Garcia et al, 1988).
Possible role as a virulence factor:
Activity of the autolytic enzyme or its regulation can give rise to
remarkable changes affecting the phenotypic properties of a clinical isolate of
pneumococcus It can also influence the pathogenic role of such strains
resulting in hlgher morbidity and mortality from this type of Infection
(Tuomanen et al, 1988). Such atyp~cal stralns of pneumococci are clinically
important as they are often associated wth more invasive types of infections
like meningitis (Salyers and Whitt, 1994).
Autolysin-induced lysis of a proportion of the Invading pneumococcl
can injure the host by releasing increased concentrations of potent toxins
and hydrolytic enzymes locally (Paton et al, 1993).
lmmun~zation of mice with purified autolysin resulted in the production
of antibodies capable of inhibiting autolysis of both rough and encapsulated
pneumococcal cultures (Berry et al, 1989). Autolysin can indirectly act as a
virulence factor by releasing the cytoplasmic protein, pneumolysin into the
external medium which happens when pneumococci undergo autolysis. But
when autolysis is inhibited by growth of pneumococci in the presence of anti-
autolysin antibody, pneumolysin activity stays cell-associated.
NEURAMINIDASES
Most of the fresh clinical isolates of pneumococci have the ability to
synthesize one or more neuraminidases. Camara et al (1994) have cloned
and sequenced a neuraminidase encoding gene (nan-A) from S.pneumoniae.

Molecular weight of nanA was determined to be 107 KDa. It is assumed that
neuraminidase can be released from the cells either by proteolytic cleavage
or after cellular autolysis. It was found later that S.pneumoniae produced
more than one neuraminidase enzyme. The gene responsible for this was
identified and designated as nan-8, which is located on the pneumococcal
chromosome. The molecular weight of nan-B was found to be 74.5 KDa.
Role as a virulence factor:
Neuraminidase cleaves terminal salicyltc acid residues present in
glycolipids, glycoproteins and oligosaccharide on cell surfaces or in body
fluids. This activity results in great damage to the host (Paton et al, 1993). It
can also unmask potential cell surface receptors for putative pneumococcal
adhesins (Krlvan et al, 1988). It is also noted that both coma and bacterem~a
can occur significantly more often in patients with pneumococcal mentngitis
when the concentration of N-acetylneuraminlc acid in the cerebrosptnal fluid
is elevated (O'Toole et al, 1971).
HYALURONIDASE
Hyaluronidase enzyme is produced by almost all strains of
S.pneumoniae. Substrate of thls enzyme is hyaluronic acid which is found
associated with connective tissue and extracellular matrix. This enzyme is
secreted by 99% of clinical isolates of S.pneumoniae during log-phase
growth in vitro. Characterization of hyaluronidase gene has been done from
a type 23 pneumococcus (Berry et al, 1994). Hyaluronidase enzyme has
been produced from recombinant E.coli carrying this gene. Molecular weight
of the purified hyaluronidase enzyme was 89 KDa. Western blot analysis
using antiserum raised against the purified 89 KDa hyaluronidase indicated
that the E.coli clone also expressed the 107-KDa form of the enzyme and this

antiserum labeled a 107 KDa protein in partially-purified hyaluronidase
preparations from S.pneumoniae (Paton et al, 2000). The enzyme act~vity is
cell-associated, which is consistent with the presence of the Gram-positive
cell surface anchorage domain (LPXTGE) near its C-terminus
As a virulence factor:
Role of hyaluronidase enzyme in the pathogenesis of pneumococcal
Infection remains unclear. Role of hyaluronidase in a nasal colonization
model is currently being assessed. Hyaluronic acid being the substrate of
thls enzyme might have a role in pathogenesis facilitating the spread of
infection, providing a greater microbial access to host tissue for colonization.
It can also help in the migration of the organism like translocation from the
lung to the vascular system, between tissues. However, it has not been able
to demonstrate any protection in a mouse immunization I challenge model
(Paton et al, 2000).
IgA I PROTEASE
S.pneumoniae colonizing the mucosal surfaces produces a protease
enzyme which has the ability to cleave human IgA I at a specific point w~thin
the hinge region, providing intact Fab and Fc fragments (Paton et al, 1993).
S.pneumon~ae gene encoding IgA I protease has been cloned. But
due to instability its further characterization has not been possible. Further
analysis of a more stable clone is needed M i c h was isolated (Camara,
19921. .

As a virulence factor:
Till now, no definite evidence is available to prove the involvement of
any of these proteases in pathogenesis of the disease. This is mainly
because the enzymes are highly specific and do not cleave IgA from any
animal species commonly used as models for disease (Paton et al, 1993).
PNEUMOCOCCAL SURFACE PROTEIN A (PspA)
Pneumococcal surface protein A is a pneumococcal virulence protein
(Yother et al, 1991). It is antigenic in nature and can elicit the production of
antibodies which is being explored currently in the production of vaccines It
serves as a good protein candidate for the preparation of pneumococcal
vaccines. It is also known that PspA is serologically variable (Mc Daniel et
al, 1987; Crain et al, 1990). Because of this property, a PspA based vaccine
may need to contain PspAs of more than one pneumococcus to be able to
protect against all pneumococci.
As a virulence factor:
According to a study it was observed that an encapsulated mutant
strain lacking PspA expression fixed more complement than the isogenic
parent strain expressing PspA even though they were found to have identical
levels of capsular polysaccharide (de Velasco et al, 1995). It was also
observed that infections of nonimmune mice with PspA' capsular type 3
pneurnococci caused greater early activation of serum complement than did
infections with a ~ s p A ' isogenic parent. These findings suggest that PspA is
able to decrease the consumption of complement by pneumococci, ultimately
reducing complement mediated clearance and phagocytosis of pneumococcl
(Briles et al, 2000).

PNEUMOCOCCAL SURFACE ADHESIN A (PsaA)
PsaA has a molecular weight of 37KDa and was detected for the 1'
time by Russell et a1 (1990) using monoclonal antibodies. Experiments have
proved that immunization with purified PsaA protected mice from challenge
with virulent S.pneumoniae (Talkington et al, 1996). Sequence analysis of
the clonal PsaA gene has been determined and it was found that there exists
a homology with putative lipoprotein adhesins of S.sanguis and
S.parasanguis (Sampson et al, 1994). Location of PsaA on S.pneumoniae is
not clear. Since it is able to elicit a protective antibody in humans, it is being
tried as a candidate for non-serotype-dependent vaccine antigen.
PNEUMOLYSIN
Production of haemolysin by pneumococci was first reported 9
decades ago (Paton et al, 1993). It is a pore-forming, thiol-activated toxin
produced by S.pneumoniae. Pneumolysin belongs to the family of sulphydryl
(SH)-activated t~aemolysins (Kanclerski and Mollby, 1987). These thiol-
activated toxins are produced by 4 genera of Gram positive bacteria,
Streptococcus, Listeria, Clostridium and Bacillus.
General properties:
Although an intracellular prote~n, rt IS always detected extracellularly in
broth cultivation and released only when the bacterium undergoes autolys~s
due to autolysin or lyt~c agent. Pneumolysin is oxygen-labrle whlch is only
apparent in crude preparations (Andrew et al, 2000). When pure, the toxlns
are not oxygen-labile and no longer activated by thiol-reduc~ng agents since
they are fully active. It is antigenic and irreversibly inactivated by treatment
with cholesterol (Paton et al, 1993).

Mode of action:
All the thiol-activated cytolysins are known to have a common mode of
action which involves an interaction with cholesterol in the target cell-
membrane leading to insertion of the toxin into the lipid bilayer and lateral
diffus~on and oligomerization of 20-80 toxin molecules ending up in the
format~on of arc and ring structures which are assumed to be transmembrane
pores (Bhakdi et al, 1986). Presence of transmembrane pores results in cell
lysis or modulation in cell activity, thereby leading to leakage of solutes from
erythrocytes, nucleated cells and liposomes (Andrew et al, 2000)
The binding of pneumolysin is independent of temperature, whereas
oltgomer~zation is dependent on it. The mechanism of binding of
pneumolysin to mammalian cells is not clear. Cholesterol may be the cell
receptor (Alouf and Geoffroy, 1991) based on the evidence that cells which
do not contain cholesterol In their cell membranes are insensitive to lys~s. A
recent report by Jacobs et a1 (1998) suggests that the role of cholesterol is
more involved mth pore formation than mth binding.
Regarding the mode of action, it is unclear whether insertion of
pneumolysin into the target membrane precedes oligomer~zation or
oligomerization occurs on the membrane surface before insertion (Andrew et
al 2000)
Structure:
Pneumolysin is 53 KDa polypeptide of 471 ammoacids and is
produced by almost all strains of pneumococci (Paton et al, 1993; Wheeler et
al, 1999). Complete nucleotide sequence of the pneumolysin gene has been

carr~ed out. The N-terminal aminoacid sequence of purified pneumolys~n was
observed to be NH2-A-N-K-A-V-N-D-F-I-L-A-M-N-Y-D-K as demonstrated by
Walker et al (1987). Cloning of pneumolysin gene has been useful in
carrylng out a number of ~nvest~gations of the structure-function relationships
of the thiol-act~vated toxins. These toxins are called hydrophilic channel
form~ng proteins.
Predicted aminoacid sequence of pneumolysin reveals that the protein
contalns a single cysteine residue at position 428. Substitution of cysteine
with serlne or glyc~ne resulted in reduced cytolytic activity. It has been
demonstrated that 4th doma~n mediates b~nd~ng and self-association of toxin.
So, cysterne region is Important in the orrentation of pneumolysrn, for the
functioning of the channels and cell bind~ng. Pneumolysin contains 8
histidine residues wh~ch are Important In ant~celluiar activity and pore
formatron (Andrew et al, 2000).
Biological properties:
The role of haemolysln In the pathogenes~s of pneumococcal infection
wab reported for the first time by Shumway who observed an Increased
erythrocytic osmotic fragility and hemoglobinemia in rabbits on intravenous
injections of the purified hemolysin (Shumway and Klebanoff, 1971).
Pneumolysin has a variety of toxic effects on different cell types.
It is known that pneumolysin causes lysis of all eukaryotic cells that
have cholesterol in their membrane. Pneumolysin can also injure bronchial
epithelial cells, alveolar epithelial cells and pulmonary arterial endothelial
cells. It is known that these cells are involved in lung-capillary barrier,
destruction by the toxin may lead to the histopathological conditions of early

pneumococcal pneumonia like alveolar flooding and hemorrhage (Mitchell
and Andrew, 2000).
Pneumolysin, at low doses is known to inhibit the respiratory burst of
human polymorphonuclear leukocytes (PMNL) (Paton and Ferrante, 1983).
This is also assoc~ated with reduced ability to take up and kill opsonized
pneumococci. Other properties of pneumolysin included the inhibition of
chernotaxis, random migration of PMNL, respiratory burst, degranulation,
bactericidal activity and phospholipid methylation of human monocytes. All
these effects of pneurnolysin could be blocked when pneumolysin
preparation was pretreated with cholesterol. Inflammatory cytokines TNF-a
and ILI-P was produced when human monocytes were stimulated by very low
doses of pneumolysin Pneumolysin is a potent activator of phospholipase A
In pulmonary artery endothel~al cells. Same phenomenon within the host
during an infection can contribute to direct lung injury and to inflammatory
response. Activation of PMNL and release of toxic molecules can injure
pulmonary tissue (Mitchell and Andrew, 2000). Pneurnolysin has detrimental
effects on ciliated epithelium. The toxln has been found to inhibit the
beatings of cilia on human respiratory epithelial cells and disrupt the
monolayers of cultured epithelial cells from the upper respiratory tract and
alveoli. Breaching of the endothelial barr~er facilitates the development of
pneumococcal bacteremia which is associated with high fatality rate.
Pneurnolysin Increases the alveolar permeability in isolated perfused rat
lungs. Alveolar epithelium acts as a limiting membrane providing a barrier to
tissue invasion by bacteria. Damage to alveolar epithelium can also be one
of the factor contributing for pathogenesis of pneumococcal ~nfection
(Mitchell and Andrew, 2000). Ventricular surface of the brain and cerebral
aqueducts are lined by ciliated ependymal cells which acts as a barrier

between the CSF which is infected during meningitis and neuronal tissue.
These cilia may protect the neuronal tissue from damage during infection by
allowing continual movement of the CSF and preventing margination of
bacteria durlng meningitis. Perturbation of cilia1 function can play a role in
the pathophysiology of pneumococcal meningitis and pneumolysin has
effects on host tissue that could compromise nonspecific host defence
mechanisms (Mitchell and Andrew, 2000).
It is indicated that pneurnolysin plays an important role in
sensorineural hearlng loss, a complication of pneumococcal meningitis This
is studied in guineapig model. Electrophysiological and histological damage
occurred when pneumolysin was perfused through the Scala tympani (Comis
et al, 1993).
Pneumolysin when added to human serum activates the classical
complement pathway in the absence of specific antibody resulting in
decreased serum opsonic activity. This activatton is due to the nonspecific
binding of IgG Fc by the toxin (Mitchell et al, 1991). Function of pneumolysin
to dctivate the complement pathway cannot be blocked by incubation with
cholesterol (Paton et al, 1984). All these studies demonstrate that
pneumolysin can interfere with opsonization, phagocytos~s and killing of
pneumococci and also block the establishment of humoral immune response
to the infection (Paton et al, 1993).
It is also known that significant antipneumolysin antibody titres or
circulating pneumolysin immune complexes are found in sera from the
majority of patients with pneumococcal pneumonia. Antibody levels against
pneumolysin evaluated by neutralrsation test revealed a titer of more than 4-

fold In patients with invasive pneumocoml infections than controls (Bhaskar
et al, 1999). Antipneumolysin levels were lowest in children under 1 year of
age and adults over 70 years of age in whom the risk of pneumocoml
pneumonia is high. Patients with pneumonia had low levels of
antipneumolysin in acute phase sera than in age-matched healthy controls,
indicating that individuals with lower pneumolysin antibody levels may be at
greater risk of contracting pneumococcal pneumonia (Paton et al, 1993).
Genetic analys~s of pneumolysin virulence factor:
Studies with cloned pneumolysin gene has enabled the construction of
a defined pneumolysin-negative derivative of S.pneumoniae type 2 by
insertion-dupl~cation mutagenesis. Virulence of pneumolysin-negative
derivative was compared with its isogenic parental type in a mouse intranasal
and intraperitoneal challenge model. Intravenous challenge with the w~ld
type straln resulted in an ovelwhelrn~ng bacteremia (IO~-IO~ organ~srnslml of
blood) and the animal died within 24 hours. Whereas the mutant
pneumococci had a bacteremia (105-10~rganismslml) that persisted for a
week In several cases wthout any detrimental effect (Paton et al, 1993).
lntratracheal challenge wth pneumolysin negative mutant resulted in
lobar pneumonia in mice rather than the bronchopneumonia seen with
intranasal inoculation. Pneumolysin-negative mutant had decreased ability
to grow and multiply within the lungs and invade the blood stream. Infection
with the wild type pneumococci led to the leakage of serum albumin into the
alveolar air space increasing the permeability of the alveolar capillary barrier
and induced separation of the tight junctions of the epithelial cells and
aaherence of pneumococci. This mechanism may be important In the
invasion process. But infection with pneurnolysin-negative mutant did not

induce the same separation of tight junctions or adherence of pneumococci
(Mitchell and Andrew, 2000).
Association of pneumolysln to meningitis-associated sensorineurai
deafness has been studied using pneumolysin-negative mutant. When
purifled pneumolysin was perfused through the guinea pig cochlea,
substantial electrophysiological and ultrastructural damage occurred (Comis
et al, 1993). Also there was pneumococcal invasion of the scala tympani and
ultrastructural damage to the organ of corti when meningitis was established
experimentally in a guinea pig model by subarachnoid inoculation (Winter et
al, 1996). Pneumolysin negative mutant in this model induced an
inflammatory response in the CSF which was similar to the wild type.
Infection with the wild type also caused a progressive hearing loss at all
frequencies tested. Studies proved that pneumolysin mediated the local
cochlear damage.
In another study by Berry et al (1999), a comparattve virulence of the
type 2 S.pneumoniae strain D39 and derivatives containing insertion-
duplication, deletion or point mutations in the ply gene was examined. Based
on the survival time after i.p. challenge and the numbers of pneumococci in
blood, lungs, brain, llver or spleen at various times after challenge, virulence
of the strain was assessed. A derivative of the type 2 S.pneumoniae strain
D39 in which the portion of the pneumolysin gene encodlng aminoacids 55 to
437 was deleted in-frame was constructed. The virulence of this strain (A
ply) was compared with those of wild type D39, a pneumolysin insertion-
duplicat~on mutant (PLN-A), and a derivative (PdT) carrying a toxin gene with
three point mutations known to abolish both cytolytic activity and complement
activation. PdT was intermediate in virulence between D39 and either PLN-A

or A ply in a niouse, intraperitoneal challenge model. This study provided
unequivocal evidence that pneumolysin has an additional property that is not
abolished by point mutations which reduce cytotoxicity and complement
activation to virtually undetectable levels. This property contributes
significantly to the pathogenesis of disease.
Though pneumolysin clearly plays a role In the pathogenes~s of
pulmonary, ocular and systemic infections by the pneumococcus, its role in
other infections is not very clear. It is known that although pneumolysin does
not have a role in the generation of inflammation in meningitis, it does have
role In the hearing loss associated with the ~nfection (Winter et al, 1996).
All these studies confirm the involvement of pneumolysin in the
pathogenesis of pneumococcal infections. However, the finding that, the
nactivation of the pneumolysin gene s~gnificantly reduced, but did not totally
inhibit, the ability of pneumococci to kill their host indicates that other
pneumococcal products are also involved (Paton et al, 1993).
Role of pneurnolysin i n diagnosis of pneurnococcal infections:
Pneumolysin, has an advantage over CPS as an antigen. It is
common in most or all strains and capable of eliciting an antibody response
and hence an ideal target for diagnosing pneumococcal disease. It occurs in
99% of clinical isolates of S.pneumoniae. Less than 5% cross reaction
between streptolysin and pneumolysin is seen (Kalin et al, 1987).
Systematic study of pneumolysin began with the work on examining
extracts obtained from frozen and ground pneumococci as well as from the
cells dissolved in sodium cholate. Antigenicity of pneumolysin was

demonstrated It was found that haernolyt~c extracts could be ~nact~vated by
ox~dat~on and react~vated by reduction Haemolys~n has been synthestzed
from pneumococcl (Stratn Dl39lR) (M~tchell and Andrew 2000)
Pneumolysln was extracted and pur~fred by Shumway and Klebanoff (1971)
whch Included sonlcat~on, ac~d preclpltatton, ammonrum sulphate
prec~p~tat~on, adsorb~ng on to d~ethyl amno ethyl cellulose concentratlon by
ultraf~ltrat~orl fract~onat~on wth Sephadex G-100 and concentratlon
Kanclersk~ and Mollby (1987) have produced and purtf~ed pneumolys~n
They demonstrated that pneumolys~n was produced by 112 of 113 cl~n~cal
~solates of S pneumonlae In the study The culture of S pneumon~ae was
concentrated by f~ltrat~on 10 t~rnes before centr~fugat~on followed by
pur~f~cat~on of the cellular content by on-exchange chromatography covalent
th~opropyl gel chromatography and gel flitratton Y~eld of 66% and a speclflc
act~vrty of 1 400 000 haemolyt~c unlts per mg of prote~n was reported
Pur~f~cat~on of pneumolys~n helped In further studtes on th~s haemolys~n
A pneumolysin-based agglutination test has been developed by Cima-
Cabal et a1 (1999) to differentiate pneumococcl from other related human and
a, .~mal pathogenic bacter~al strams.
Pneumolys~n has been detected from sputum samples by Western blot
which was reported to be almost as sens~tive as PCR for the non-cultural
detection of pneumococci in S.pneumoniae culture positive sputa from
patients with chest infections (Wheeler et al, 1999). According to a study
(Kearns et al, 2000), pneumolysin detection has led to the identification of
atypical isolates of S.pneumoniae. The atypical ~solates w r e examined by
real-time PCR method for the pneumolysin gene. Using the first defined 559-
bp and 649-bp regions of the pneumolysin gene as nested primers, the ability

of PCR to detect S.pneumoniae in blood was tested by Rudolph et a1 (1993)
which seemed to be a promising alternative for definitive diagnosis.
Polymerase chain reaction assay based on the amplification of
pneumolysin gene fragments in patient sera was developed for the diagnosis
of acute pneumococcal pneumonia by Salo et al (1995) reporting a high
specificity and sensitivity.
Frasen and Tunewall (1969) have detected antibodies against crude
preparations of pneumolysin. The sensitivity and reproducibility of this assay
were not sat~sfactory.
Detection of antibod~es to pneumolysin by a neutralization test using
crude pneumolysin has been done by Bhaskar et al (1999) in invasive
childhood infections. Enzyme linked ~mmunosorbent assay (ELISA) has
been used for measurement of antibodies against highly purifled
pneumolysin by various workers (Kalin et al, 1987; Kanclerski et al, 1988;
Korppi et al, 1992). Detect~on of IgG response to pneumolysln by ELISA
hdve proved to be an aid in the laboratory diagnosis of pneumococcal
pneumonia.
For quantlficatlon of c~rculating Immune complexes (IC) containing
specific antipneumococcal immunoglobulins, ELISA has been developed by
Korppl et al (1998) for the diagnosis of pneumococcal infections. These ICs
containing antibodies to pneumolysin, a protein antigen detected by ELISA
has proved to be more sensitive than other serological methods for the
diagnosis of pneumococcal lower respiratory infection (Korppi et al, 1998).
Based on a study by Toikka et al (1999), it was concluded that a combination

of several methods are needed for the detection of invasive pneumococcal
infection.
Role of pneumolysin in prevention of pneumococcal infection
Future pneumococcal vaccine formulation using pneumolysin:
Studies on the immunogenicity of genetically obtained pneumolysin
toxoids and their conjugation to S.pneumoniae type 19F polysaccharide
conducted by Paton et al (1991) revealed that significant anti-pneumolysoid
titers could be obtained and the immunogenicity of the 19F polysaccharide
moiety was markedly enhanced compared to that of unconjugated
polysaccharide. Conjugation resulted in conversion of 19F polysaccharide
Into an antigen capable of inducing a booster effect. Studies have proved
that pneumolysin toxoids can be a su~table candidate for development of
pneumococcal vaccine as it was able to confer significant degree of
protection in mice (Alexander et at, 1994).
HOST DEFENSE MECHANISMS
Specific or nonspecific ~mmunolog~cal mechanism can be exhibited in
a host. Usually pneumococcal infection does not occur without prior
nasopharyngeal colonization. This colonization is influenzed by various
factors like age, exposure, overcrowding, the season, etc. To colonize,
pneumococcal cells have to get attached to the nasopharyngeal epithelial
cells with the help of adhesin M i c h mediate adherence. Chlldren are more
likely to be carriers of pneumococci than the adults (Gray et al, 1980). A
patient may carry upto four different serotypes of pneumococci. Once
colonized, pneumowccus has the potential to become invasive M e n it
migrates out of the nasopharynx (Musher et al, 2000), to the middle ear of the
paranasal sinuses, bronchial tree, or the blood stream too. The nonspecific

mechanisms which inhibit the pneumococci to invade include, laminar airflow
across mucous layers that filter the inspired air, the glotteal reflex, laryngeal
closure, the cough reflex and ciliary mechanisms. If the normal clearance
mechanism fail to remove pneumococci that have been migrated beyond the
nasopharynx, next comes the secondary defense line consisting of
professional phagocytes which will ingest the bacteria. Again the
pneumococci is w l l protected from this act because of the presence of a
polysaccharide capsule which inhibits phagocytosis. Anticapsular antibody
produced by the host provides serotype-specific protection against
pneumococcal infection. Antibodies appear either afler colonization or
infection following immunization. In persons who have diminished lower
airway clearance, there is a risk of developing pneumonia before antibody is
produced. The incidence of invasive pneumococcal infection is greatly
increased in patients with decreased antibody synthesis or decreased activity
of polymorphonuclear cells and macrophages. In an adult, it is related to
immunocompromised conditions like HIV infection. This increased incidence
is seen in developing countries. Other conditions underlying serious
pneumococcal infections include malnutr~t~on, alcoholism, diabetes and those
wi:h hepatic or renal insufficiency, myeloma and lymphoma. Absence of
spleen further predisposes the infection to a fulminant state resulting in
pneumococcal sepsis.
Antibiotic resistance in S.pneurnoniae:
S.pneurnoniae is a major cause of pneumonia, meningitis, acute otitis
media and acute sinusitis (Austrian, 1994; Musher, 1995). Before the
introduction of penicillin, mortality and morbidity rates of pneumococcal
infect~ons were very high. The only antimicrobial agent used to treat
pneumococcal infections then was sulphonamides. Resistance to

sulphonamides were reported as early as 1943 There was a dramatic
reduction in the death rates once penicillin was introduced. Benzyl penicill~n
soon became the drug of choice for treating pneumococcal infections (Barry,
1 999).
Slowly, reports stating the development of resistance to tetracycline,
chloramphenicol and erythromycin came up. During 1980s and 1990s,
resistance to the alternative drugs became more prevalent As these drugs
had limited use in the treatment of pneumococcal infections, there was little
selective pressure on the normal susceptible population of pneumococci
Penicillin resistance was first reported from the natives of New Gu~nea in the
year 1967 (Jacobs et al, 1978). In 1980s penicillin-resistant pneumococci
emerged in many countries. Currently, the prevalence of resistant
pneumococci to penicillin and other antibiotics IS increasing globally
(Pallares et al, 2000). Antimicrobial consumption is a major factor
contributing to the development of resistance to penicillin and other
antibiotics (Arason et al, 1996; Baquero, 1996; Kanungo et al, 2001).
Mechanism of resistance
Penicillin:
Minimum inhibitory concentrations (MIC) of penicillin of penicillin-
susceptible S.pneumoniae are 5 0.06 pglml. Strains with MlCs from 0.1-1.0
pglml are termed as intermediately susceptible and isolates with MIC > 2.0
pglml are considered as truly resistant to penicillin. Penicillin-intermediate
p~eumococci are not truly resistant to penicillin in all clinical settings; at the
same time, they are not susceptible when used to treat meningitis or other
infections for which low concentrations may be achieved at the site of

infection. The truly reslstant isolates of S.pneumoniae has to be treated wth
alternat~ve drugs (Barry, 1999).
Development of peniclllln reslstance ~n clinical lsolates of
Spneumoniae IS due to the alterat~on of penlclllin blndlng protelns (PBPs)
PBPs from penlclllin-resistant Spneumonfae have reduced affinities for the
antlblotlc molecule (Z~ghelbolm and Tomasz 1980) PEPS catalyze
Important steps in the assembly of peptldoglycan wth the transpept~dat~on
between 2 pept~de s~de chams of the mucln subunlts It Interacts wth p- lactams enzymatically by formlng a covalent complex vla the active site
serlne Alterations In PBPs of reslstant stralns result In decreased afflnlty to
the antrblotlc so that hlgher penlclllln concentrations are requlred for blndlng
and rnhib~tlon of the enzyme (Hakenbeck et al 2000) It was also found that
hlgh-level reslstance to peniclllln lnvolved gradual remodeling of several (3-
4) of the h~gh molecular weight PBFs In parallel wlth the stepwse increase In
the resistance level This was demonstrated by genei~c transformat~on of
reslstance using the cllnical isolates as DNA donors (Zlghelbo~m and
Tornasz 1980, Clonlng and sequencing of these reslstant PBP genes
id~n t~ f ied mosarc sequences In each one of these lndlcatlng a heterologous
recombination (Dowson et al 1989) Development of reslstance to penlclllln
among pneumococci have occurred ~ndependently at several times glvlng
rlse to unique penlcillin-res~stant clones or genetlc lineages (Munoz et al
1992) The beglnnrng of a reslstance clone IS marked by the lncorporatlon of
one of such altered low-affln~ty PBP genes Through cell dlvislon this llneage
wlth low level reslstance expands which agaln gets lnvolved In a znd recornblnat~onal event resulting In the modlflcat~on of another of the high
molecular welght PBP genes In the recipient pneumococcus Th~s process
further continues resulting ~n a stra~n with full blown reslstance to penlclllln

and an increased MIC. But the genetic background of the bacterium remalns
unaltered.
Five PBPs have been described: IA , 18, 2A, 28 and 2X (Musher et al,
2000) Changes in PBP 1A and 2A may explain low level (intermediate)
penlclllln decreased susceptibility; higher levels of reslstance to penicillin
requlres alterations of PBPs I A , 2X and 28 In contrast, high level
reslstance to th~rd generation cephalosporins may result from altered PBPs
1A and 2X Alternat~ve mechanisms leading to res~stance not ~nvolving
PBPs, IS the mutat~ons In genes llke CiaH and CiaR (Musher et al, 2000)
Macrolldes and related antlblotlcs.
Development of reslstance to erythromycln IS by 2 mechanisms
Pneumococc~ that are resistant by vlrtue of an efflux system show low-level
res~stance to erythromycln and are suscept~ble to the llncosamlde
cllndamycln Hlgh level reslstance occurs due to altered target sltes and
those stralns are resistant to cl~ndamycln as well as erythromycln (Leclercq
and Courvalln 1993 Sutcliffe et al 1996) When the lnvitro actlvity of
d~ffxent antlb~ot~cs were compared against 3 phenotypes of pneumococcl
the macrol~des such as clarithromycln dlrlthromyc~n and roxithromyc~n
showed complete cross-res~stance Whereas the streptogramln
qulnuprlstin-dalfoprlstln and the ketolide telithromycln did not show such
cross resistance However both can be used in areas where erythromycln-
resistant stralns are prevalent (Barry 1999)
Quinolones:
Quinolone-resistance in pneumococci has been reported among
patient isolates (Janolr et al, 1996; Tankovic et al, 1996) To develop a hlgh

level resistance atleast 2 mutations are requ~red. The f~rst, Par C, mutation
results in low level resistance to ciprofloxacin (MIC 4 or 8 pglml). These
mutants undergo the 2& mutation, Mhlich involves DNA gyrase (gyr A)
resulting in high level resistance to ciprofloxacin (MIC 16-64 pglml) (Barry,
1999) Resistance to qu~nolones can arise through point mutations in any
subunit of DNA gyrase. The isolate that has undergone the 2" mutatlon
usually are relatively resistant to all other fluoroquinolones except some of
the newer agents llke trovafloxacln and moxafloxacin may have MlCs below
achtevable levels. H~gh level reslstance to ciprofloxacin and related
quinolones are extremely rare
Rifampicin:
Rifampicin reslstance has risen in several different species of bacterla
due to alterations in 1 or more regions in the target of the antib~ot~c, the p- suburiit of RNA polymerase encoded by rpoB. Resistance to rifampicln has
been shorn to evolve by polnt mutatlon In a number of nontransformable
specles (Enr~ght et al, 2C00) R~fampic~n-resistant pneumococci is very rare
Tetracycline:
Tetracycline belng a broad spectrum antib~ot~c, is used in the
treatment of both Gram posltlve and Gram negative infections (Chopra et 31,
1981). Its wdespread use has resulted tn development of resistance in
pneumococci and other bacteria (Widdowson and Klugman, 2000).
Tetracycline reststance gene In pneumococci tet(M), was 1' described
~n Spneumon~ae by Burdett, lnamine and Rajagopalan (1982) Later on,
tet(0) was also described from South Africa The tet(0) and tet(M) genes are

closely related, sharing -76% nucleotide sequence homology and 77%
aminoacid homology (Widdowson and Klugman, 2000).
Trimethoprim:
Trimethoorim, usually in combination with sulfamethoxazole is one of
the most commonly used antibiotics globally
Tr~methoprim inhibits dlhydrofolate reductase (DHFR), thus blocking
the reduction of dihydrofolate to tetrahydrofolate, an important precursor for
the synthesis of purines, thymidylate and certain aminoac~ds and v~tam~ns
Cloning and sequencing of the trimethoprim resistance determinant from
these pneumococcal stralns lndlcated that an altered chromosome-encoded
DHFR was responsible for the observed resistance. Comparison of DHFR
sequences from pneumococcal strains wth various suscept~bilities to
trimethoprim, together with slte-directed mutagenesis, showed that
substitut~on of so leu cine-100 with a leucine residue resulted in trimethoprim
resistance (Pikis et al, 1998).
Sulphonamide resistance in S.pneumoniae can arise by alterations to
the chromosomally encoded dihydropterate synthase (sulA) (Enright et al.
2000).
Clones of antibiotic resistant pneumococci:
Pneumococcal genetic lineages that have achieved massive
gecgraphic spread across continental boundaries have been described. The
most w~dely spread of these is the SpanishlUSA serotype 23F clone.
Spanish serotype 23F strains are resistant to penicillin, tetracycline,
chloramphenicol and variably resistant to erythromycin and trlmethoprim-

sulfamethoxazole (Tomasz, 1999) Th~s clone has spread to numerous
countr~es In Europe the Un~ted K~ngdom Un~ted States South Afrlca South
Amer~ca and some reglons In the Far East (Mc Gee et a1 2000)
Pneumococc~ belong~ng to th~s clone are not only wdespread but also
represents a very large proportion of pen~c~ll~n-res~stant pneumococcl In a
glven epldemlolog~c sett~ng Isolates belong~ng lo th~s clone have been
recovered from all normally sterlle s~tes In lnvaslve paedlatrlc as well as adult
dlsease from different countr~es (Tomasz, 1999)
The second pneumococcal clone is the FrenchlSpanish clone,
resistant to penicillin and trimethopr~m-sulfamethoxazole and expresses
either serotype 14 or 9 also has widely spread all over the world.
A third clone of S.pneumon~ae expressing capsular serotype 6B
carries multidrug res~stant genes. It was identifled in Spain, the UK and
particularly in Iceland (Soares et al, 1993).
Reports of antimicrobial resistance among S.pneumoniae:
Clinical resistance to penic~ll~n in S pneumoniae was l* reported In
Boston In the year 1965. Resistance was later reported from Australla in
1967 and especially In South Afr~ca In 1977 where stralns with both a hlgh
level of penicillin resistance and multiple antibiotic resistance were reported
(Jacobs et al, 1978).

Table 1.Penicillin Resistance of S.pneumoniae from Europe
Country Resistance Year Reference
Poland Germany Switzerland Northern Ireland Belglum Iceland England Spain Romanla France Hungary Finland
Jeljaszewicz et al Milatovlc et al Wust et al Lafong et al Verhaegen et a1 Kristinsson et al Ridgway et al Fenoll et al Millar et al Geslin et al Marton Nissinen and Leinonen
In Portugal, penicillin resistance increased fron~ 4.6% in 1989 to
17.9% In 1993 (Pato et al, 1995) in France it increased from 3.2% in 1987 to
20% in 1992 (Bedos et al, 1996) and In the Unlted States it Increased from
around 5% in the 1980s to 33 5% In 1996 (Thornsberry et al, 1997). But the
incidence of panic~llin-resistant pneumococci remained stable at very low
levels in other areas of Europe Denmark (<2%) Germany (1 8%), Belgium
(2-4%), Sweden (1 7%), Finland (1.7%), Great Britain (1 53.9%) and Italy
(5 5%) (Hedlund et al, 1995; Johnson et al, 1996; Marchese et al, 1995.
Nielsen and Henrichsen, 1996; Nissinen et a l 1995; Re~nert et al, 1995;
Verhaegen et al, 1995). Mult~res~stance to antib~ot~cs has been prominent ln
Brita~n from 1985 onwards (Colman et al, 1998).

Studies from Edinburgh C~ty Hospital, UK, In the year 1995, reported a
very low prevalence rates of penicillin (2:3%) and erythromycin (2.5%)
resistance than those reported elsewhere in the UK (Kalima et al, 1999)
Studles from North America reports a prevalence rate of 68% for
sensitive, 15% for intermediate and 17% for resistance to pencillin among
S.pneumoniae isolates (Barry et al. 1999) during the period of 1996-1997.
Indian scenario:
Epidemiologic character~stics of lnvaslve pneumococcal infections In 6
hospitals In lndla were studled for a perlod of 4 years by the lnvasive
Bacterial lnfectlon Surveillance Group (IBIS) The antlmlcroblal suscept~bil~ty
pattern of 307 lsolates of Spneumon~ae were tested 56 3% were
nonsuscept~ble to co-trlmoxazole 16 6% to chloramphen~col 4 2% to
erythromyc~n 1 3% to oxacllhn and none of the lsolates were resistant to
cefotaxlme (IBIS Study 1999)
The antlbiotlc susceptibilities of 94 isolates of S.pneumoniae obtalned
fr0.n outpatients with respiratory tract lnfectlons were determined by disk
dlffuslon and E-test In the Union Territory of Pondicherry in South India. 6%
of the pneumococcal isolates showed reduced suscept~bility to penicillin (MIC
2 0.125 pglml) and 3% showed reduced susceptibility to cefotaxime (MIC z 0 25 pglml). Resistance to tetracycline (MIC z 4 pglml) and chloramphenicol
(MIC 2 16 pglml) was found in 37% and 4% of the isolates respectively.
Resistance to erythromycin was not found in any of the isolates. 15% of the
pneumococcal isolates showed reduced susceptibility to TMP-SMZ (MIC = 32
[1.6 i 30.4) pglml) and 52% were resistant (MIC 2 64 [3.2 i 60.81 vglml)
(Larsson et al, 1999; Kanungo et al, 2001).

SEROTYPES AND ANTIBIOTIC RESISTANCE
Rates of antibiotic resistance are increasing continuously in the
following years. In the present decade, reslstance to penicillrn has spread
throughout the world This causes concern and knowledge of its evolution
could be of interest for those countries Were lncreaslng resistance is being
observed
A study from Spain, revealed that penicillin resistance was present in
strains of all serogroupslserotypes, the h~ghest rate being found in serogroup
19 and 23 strains Erythromycin resistant rate (48.4%) appeared to be
associated wlth serotype 19 (17.7%) Two rnultiresistant isolates, one
serotype 19 and one nontypeable were resistant to rifarnplcin (,Lopez et al,
1999).
Studles on the impact of human ~mmunodef~c~ency vlrus type 1 on the
disease spectrum of S pneumoniae in South African chlldren revealed that
there was no d~fference in pen~clllln reslstance between HIV-infected and
HIV unlnfected chlldren among the paedlatrlc sero groups (6, 9 14 19 or 23)
64 of 115 (55 6%) vs 99 of 44 (43 2%) respectively, or among other of
serogroups 2 of 27 (7 4%) vs 3 of 33 (9 1 %) (Madhl et al 2000)
Out of 768 (14%) isolates which were rnsusceptlble to 1 or more
antlblotic, 591 of these belonged to serotypes 6, 9, 14, 9 or 23 from a study
by Colman et a1 (1998) in Brltaln Representatives of type 14 resistant to
erythromyc~n were prominent from 1986 onwards Also there was an
Increase In the number of multl-res~stant pneurnococci from 1985 Type 23
was found non-suscept~ble to penlclllln, chlorarnphen~col and tetracycline

Table 2. Predominant Penicillin Resistant Serotypes from Different Countries
Country Predominant Penicillin Reference, year
Ta~wan Europe Thailand Spain Israel Asia Gaza Bangladesh
resistant serotypes 23F,l9F,6B 6,9,14,19,23 23F,9V 19,23 23,19,9,4,6 23,19,6 6,14,19,23 14
Hsueh et al (1999) Priviteria (1994) Dejsirilert et al (1999) Lopez et al(1999) Raz et al(1997) Song et a1 (1999) El-Astal et al (1997) Saha et a1 (1 999)
LABORATORY DIAGNOSIS OF PNEUMOCOCCAL PNEUMONIA
The causes of pneumonia, are st111 ~ncompletely def~ned, pr~mar~ly
because of the d~fficulty In obtaln~ng adequate and appropr~ate samples for
testlng and the lack of rellable diagnostic methods Th~s serves as the maln
drawback because knowledge of causat~ve agents In d~fferent patlent
populations and settlngs IS cruclal for the emplr~cal treatment of the lnfect~on
Recent development of newer d~agnost~c methods, such as serology and
PCR testing have complemented the use of blood and pleural fluid cultures to
assess the etiology of pneumonia.
Sputum examination and culture:
An etiologic role for the pneumococcus in pneumonia is strongly
suggested by the demonstration of large numbers of polymorphonuclear
leukocytes and slightly elongated Gram positive cocci in pairs and chains in
tbr? sputum. Diagnosis can be confirmed by the identification of
S.pneumoniae in sputum culture. But sputum is rarely used as a diagnostic
specimen in children as they do not produce it. In older children and

adolescent, the diagnosis is complicated by lndlgenous flora of the mouth
and pharynx. Correlation between the results of sputum culture, smear and
blood culture in pneumococcal pneumonia IS poor (Parkinson et al, 1992,
Weissenbacher et al, 1990). Some physlclans completely reject sputum
culture and rely on a characteristic sputum Gram's staln or more invasive
procedures. A study by Ort et a1 (1983), suggested a correlation between
Gram's stain and culture data with radiographic findings. However, diagnosis
by sputum culture relies on the quality of the specimen provided, the care
with which the relevant purulent component is sampled (Musher, 1998).
Throat swabs and nasopharyngeal swabs have limited use as
diagnostic procedure, as both sample the normal flora of the upper
respiratory tract.
Blood culture
Fewer than 5% of children wth pneumonia have cu!ture positive
bacteremia (Anonymous 1988) Blood culture is speciflc but the sensittvity is
very low It IS posltlve only In 20-25% of cases (Austrian 1981 Mac Farlane
et al 1982 Kalin and Llndberg 1983) In ambulatory patlents wth
pneumonia the range IS between 3-10% (Parkinson et al 1992 Mason and
Jacobs 1994) Blood cultures are often negatlve from pattents who have
received prior anttmicrobral therapy It has been shorn that drugs can be
transferred along wth blood into the culture broth and suppress the growth of
bacterla (Pazln et al 1982) In patrents wth pleural effusron proport~ons of
posltive blood culture IS found to be hlgh as reported by Hortal et al (1990)
Modern automated systems often y~eld pos~trve blood cultures wthln 12
hours after the sample IS obtatned (Musher 1998)

lnvasive diagnostic techniques:
For dlagnoslng bacterlal pneumonia, isolation of bacter~a from
consolidated lung parenchyma IS a speclflc method (Adegbola et al 1994
Falade et al, 1997) These techniques are usually performed In patlents wth
clln~cal deterloratron or In whom non-rnvaslve methods fall to provlde a
dlagnosls (Parkinson et al, 1992)
In developing countries 50-70% of lung asplrates from those who have
not recelved prior antlb~otlcs are posltlve for bacterla (Funkhouser et al
1991) A range of 46-50% IS reported by other workers (Kalra et al, 1981)
Thls technique, ~f not undertaken wth due care IS often associated wlth
compl~cat~ons of pneumothorax Although, the results of lung puncture
obtalned provlde a deflnltlve dlagnosls of bacterlal pneumonla, ~t IS not
performed routinely as ~t IS lnvaslve and IS regarded as unethical In most
cases (Wolf and Fleer 2000)
Other methods to determine the bacterlal cause of pneumonla In
chrldren Include specimens taken by deep tracheal suctlon and broncho-
alve~lar lavage. Both these methods cannot be employed as routine
methods but can be considered in children requiring endotracheal lntubatlon
(Wolf and Fleer, 2000). Broncheoalveolar lavage and flexlble bronchoscopy
are relatively safe, effective and its diagnostic yield ranges from 27-75% in
children with various underlying diseases (Winthrop et al, 1990).
Antigen detection assays:
A number of rapid diagnostic methods have been developed based
mainly on antigen detection from various clirtical specimens. The various

antigens of S.pneumoniae which has been detected from varlous clinical
specimens include pneumolysln and capsular polysaccharide
Antigen detection assays have several advantages over bacterial
culture Samples for ant~gen detection usually do not need any special
transport media and the tests are simple and can be performed directly aftar
sampling These assays are less influenced by concomitant use of
antimicrobial drugs (Lankinen et al, 1997)
Pneumolysin, a protein antlgen, found in all stra~ns of S pneumoniae is
an Ideal target for antigen detection Studies have proved ~ t s presence in
large amounts in pneumococcus-induced inflammatory processes, in which it
may be an important virulence factor (Walker et al, 1987).
The routlne presumptlve ldentificatlon of pneumococcal colonies relies
primarily on thelr sensitivity to optochin and secondarily on their bile
solub~lity But there are reports where pneumococcl has shown res~stance to
optochin Such misinterpretations can be avoided by performing the
pneumolys~n-based agglutination test It was found to be easy, rapld, cost-
effective and accurate (100% speciflc and 95% sensitive) in identify~ng
pneumococci from other related human and anlmal pathogenic bacteria
(Clma-Cabal et a1 1999) Kearns et al (2000) reported that pneumolysin-
mediated agglut~nation w l l be a rapld and reliable new method for the
identification of S pneumon~ae including atypical stralns
Demonstration of pneunococcal capsular polysaccharide antlgens in
blood, urine or sputum has decreased the time for diagnosis and increased
the diagnostic sensitivity Counter immunoelectrophores~s, Co-agglutination,

Latex agglutination have been employed to detect capsular polysaccharide
antigen and positive results with these methods have indicated a
pneumococcal etiology inspite of negative cultures.
Capsular polysaccharide is a type-specific antigen of pneumowccl
detected by utilizing 'Omniserum' (Statens Serum Institut, Copenhagen,
Denmark), a mixture of rabblt polyclonal antibodies to all known capsular
serotypes The drawback is the cross reaction between Omniserum and the
antlgens of viridans Streptococci (Holmberg et al, 1985). Pneumococcal
polysacchar~des have been detected from urine by Counter
~mrnunoelectropnoresis by Coonrod and Rytel (1973) The test was found to
be less sensitive for the detection of polysaccharide types 7 and 14 than for
other types. Rates of antigen detection varies in different studies. 46% of
sputa revealed the presence of antigen by latex agglutination (Holloway et al,
1991) Singhal et al (1996) has reported a sens~tivity of 100% and a
specificity of 97.1% for detection of pneumococcal antlgens dlrectly In
untreated CSF by modifled latex agglutination test. Pneumococcal capsular
antigen was detected by latex agglutination tests by Boersma et al (1993).
reprtlng a sensitivity of 89% A sensitivity of 78% 100% and 71% was
reported from Baltimore, Sao Paulo and Calro sltes for the diagnosis of
lnvaslve pneumococcal Infection by monovalent latex agglutination tests
using alkalinized, unconcentrated urine samples (Harrison et al, 1996)
Coagglutination for the detection of capsular antigen using sputum and
concentrated urine had a sensitivity of 79% and 12% respectively (Burman et
al, 1991). Whitby et al (1985) reported 74% sensitivity and 98% specificity
by CoA, 71% and 99% by LA and 67% and 98% by Counter
~mmunoelectrophoresis for pneumococcal antigen detection.

Molecular methods:
Molecular based techniques provides rap~d detection of Infectious
dlseases (Cartwight, 1992) lnvitro DNA amplification by the polymerase
chain reaction (PCR) has gained considerable importance in the field of
diagnostic microbiology for its exquisite sensitivity and speclfic~ty (Saiki et al,
1988) According to a study by Toikka et al (1999) blood-based pneumolystn
PCR was compared to blood culture and detection of pneumolysin Immune
complexes, as well as to detection of antibodies to pneumolysin and to C-
polysaccharide, for the diagnosis of pneumococcal infection In febr~le
children. In vitro sens~tivity of the PCR was found to be 10 CFU and 1 CFU
after southern hybridization of the PCR product. It was concluded that
pneumolysin PCR was the most sensitive assay, but its clinical value is
reduced by the fact that 3 blood fractions were needed. Rudolph et al (1993)
studied 16 adults with culture-proven pneumococcal pneumonia using nested
PCR, with primers designed from pneumolyin and autolysin genes. He
reported a invitro sensitivity of 10 fg or 200 CFU for whole bacteria and 20
CFU for buffy coat samples. The sensit~vity of the assay was 37.5% for the
vhole blood and 75% for the buffy coat. 25 adults from Gambia wth
suspcted pneumonia were examined by PCR with primers detecting the
autolysin gene sequence, lnvitro sensitlvity was 50 fg or 3 CFU (Hassan-
King et al, 1994). Salo et al (1995) studied 20 serum samples from adult
patlents with blood culture positive acute pneumococcal pneumonia by using
nested PCR method. In vitro sensitivity was found to be 24 fg. All 20
samples were posltive by PCR with a specificity of 94%. Using whole-blood
PCR, 36 paediatric patients were studied wth suspected bacterem~a, using
the prlmers and probes derlved from penicillin-binding proteln 28 gene The
lnvitro sensitivity was 100 fg or 1 CFU (Zhang et al, 1995). Based on a
prospective study to evaluate the accuracy of pneumolysin PCR of serum, for

the detect~on of pneumococcal infections In ch~ldren, the lnvltro senslt~v~ty of
the pneumolys~n PCR assay was found to be 10 CFU whereas the cllnlcal
sensrtlvlty of blood and CSF culture pos~t~ve samples from 13 pat~ents was
100% It was noted that although pneumolysln PCR was sensltlve ~t was not
very useful for the detect~on of deep-seated pneumococcal lnfect~ons
because a h~gh rate of pos~tlv~ty was seen In the controls (Dagan et a1 1998)
Also, it was proved that pneumolysin PCR IS currently not a feasible
method for routlne d~agnos~s of lnvasive pneumococcal infection in children
Garc~a et al (1999) reported a sensitivity of 911.3% and specificity of 96.5%
for PCR with samples obta~ned by thorac~c needle asp~ratlon (TNA) for
d~agnosis of pneumococcal pneumonia. It was noted that PCR assay was
more sensitive than TNA culture. part~cularly In patlents who had recelved
prior ant~biotic therapy Though PCR was considered as a sensitive and
speclflc techn~que, ~t has not proved to be cost-effect~ve. Western blot
detection of pneumolysin was shown to be almost as sensitive as PCR In 27
sputum samples whlch were culture positive for S.pneurnoniae obtained from
pat~ents having chest infections Western blot and PCR was found to be
mois sensitlve than Counter current ~mmunoelectrophores~s (CIE) for
pneumococcal capsular polysacchar~de ant~gens on the same specimens
The sensitivities noted were loo%, 85% and 67% for PCR, pneumolysln-
immunoblotting and capsular polysacchar~de-CIE respectively. Pneumolysin
detection seems to be a promising technique for the noncultural diagnosis of
pneurnococcal chest infection (Wheeler et al, 1999).
Serological diagnosis of pneumococcal pneumonia:
W ~ t h the development of vaccines to pneumococcl, estimation of
antibodies in the vaccines to determine the level of protection has become

essential. Antibodies against various type of antigens of S.pneumon~ae have
been detected in children and adults Serologic assays for diagnosing
pneumococcal pneumonia have been used less than other methods.
Antlbodles against type-specif~c capsular polysacchar~de (IgG), C-
polysaccharide (IgG, IgM), pneumolysln (IgG) and phosphoryl chollne (IgG,
IgM) have been detected by Burman et al (1991). Significant increase in
antibodies against all pneumococcal antigens were noted.
Serum IgM and IgG antlbodles agalnst pneumococcal polysaccharlde
antlgens have been detected by enzyme-l~nked ~mmunosorbent assay
(ELISA) (Barrett et al 1980) Shyamala et al (1988) has descr~bed an
enzyme-~mmunoassay (EIA) for ant~bodles to pneumococcal
polysacchar~des Assay uses the 14-valent vacclne (Pneumovax) as the
source of antlgen EIA was developed to allow the quant~tat~on of the human
response to ~mmun~zatlon wth pneumococcal polysacchar~de All
nonlmmunlzed subjects tested had IgG ant~bod~es In serum and lmmun~zed
subjects hsd IgG In the~r serum wlth a rlse In IgM and IgA spec~flc ant~body
~o~icentrat~ons at a mean of 6 weeks post-~mmun~zatlon
Modification of a direct ELISA for the detection of IgG and M
antibodies to pneumococcal capsular polysaccharide was reported by
Messina et al (1985) Antlbody responses to serotypes 1, 3, 9N and 23F
were measured Direct ELISA was also performed for the determination of
ant~body responses In ind~viduals immun~zed with 14-valent pneumococcai
vacclne. It was noted that direct ELISA was a sens~t~ve and specific assay.

A sensitivity of 83% was noted in patients with blood culture posltive
pneumococcal pneumonia by ELlSA in paired samples for the detection of
antibodies to pur~fied pneumolysin. Significant rise in ELlSA titre was found
in 17% of the patients (Kanclerski et al, 1988). Kalin et al (1987) reported a
sensitivity of 95% by ELlSA to detect antibodies to pneurnolysin. A two-fold
rise in antibody titres were noted in bacteremic pneumococcal pneumonia
cases.
Ant~body response to CPS, pneumolysin and C-polysacchar~de
antigens of S.pneumoniae were measured by Korppi et al (1992). Findings
of this study suggested that each serologlcal test for pneumococcal etiology
was insensitive and to get an optimal result, a large panel of pneumococcal
antigen and antibody must be used Another study reported a 3-fold rise of
antibody titre to CPS, 3-fold rise of antibodies to C-polysacchar~de and a 2-
fold rise in IgG antibody titre for pneumolysin antigen (Korppi et al, 1993).
Circulatlng pneurnococcal IgG immune complexes in patients wth
comrnun~ty acquired pneumonia were demonstrated by Holloway et al (1993).
E L J A was developed for quantitat~on of circulat~ng immune complexes (ICs)
contaming specific antipneumococcal immunoglobulin G. According to thls
study, no correlation was found between ICs and serum IgG antibody levels.
In the year 1998, Korppi et al evaluated the usefulness of ICs in the
diagnosis of pneumococcal lower respiratory infection in children.
Pneumococcal immune complexes containing antibodies to species-specific
C-polysaccharide, type-specific capsular polysaccharide and pneumolysin
were studied. Measurement of ICs were more sensitive than other
serologlcal methods except in infants to diagnose pneumococcal IOWW
respiratory infections.