Embed Size (px)
Citation preview
MinistryofHealthGhana
IndependentReviewHealthSectorProgrammeofWork2009
Ghana(Draft)
April2010

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 i
IndependentReviewHealthSectorProgrammeofWork2009
Ghana
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 ii
TableofContents
Acknowledgement.................................................................................................................................iv
Listofabbreviationsandacronyms.......................................................................................................v
Executivesummary................................................................................................................................ix
1. Introduction...................................................................................................................................1
2. SectorPerformance.......................................................................................................................2
2.1 HolisticAssessmentofthesectorperformancein2009........................................................2
2.2 MidTermDeskReviewPOW2007-2011...............................................................................6
3. Governanceandhealthsectororganisation..................................................................................7
3.1 Ahealthsectorevolvingoverthepastdecadesfromfragmentationtointegrationandagaintofragmentation......................................................................................................................7
3.1.1 Fragmentationandpoorcoordinationofessentialgovernancefunctions....................8
3.1.2 Whiletheresourceenvelopeforhealthcontinuestoincrease,fundingshiftstowardsclinicalcareandlessflexiblefunding...........................................................................................10
3.1.3 Giventhedynamicchangesinthesector,arewelosingfocus?Anddowekeepprioritiesright?............................................................................................................................12
3.2 Asectorfacingincreaseddemandbutconstrainedbyimportantinefficienciesandweaknesses......................................................................................................................................13
3.2.1 Increasingcoverageofhealthinsuranceleadstoincreaseddemandforservices......13
3.2.2 Delaysinreleaseoffundingandinreimbursementsconstraineffectiveimplementationandservicedelivery..........................................................................................14
3.2.3 TheaveragepriceofmedicinesinGhanaisonaveragethreetimesthemedianinternationalreferenceprice.......................................................................................................15
3.2.4 TheNHIAmanagesalargepartofthehealthsectorresourcesbutisconstrainedbyanumberofinefficienciesorweaknesses......................................................................................16
3.2.5 Humanresourcesforbetterhealth.............................................................................19
3.2.6 Managinganduseofinformationfordecision-making...............................................21
3.2.7 CapitalinvestmentsinsupportofreachingtheMDGs................................................23
3.2.8 Publicfinancemanagement.........................................................................................23
3.3 Whatarethechallengesthatdistrictfaceinordertodeliver?...........................................24
3.4 Andwhathasbeendeliveredintermsofthemain2009servicerelatedpriorities?..........26
4. Howcanannualindependentreviewsbestcontribute?.............................................................31
5. Mainconclusionsandrecommendations....................................................................................32
ANNEXES................................................................................................................................................1
Annex1.TermsofReference.................................................................................................................1
Annex2.HolisticAssessmentofperformanceinthehealthsector2009...........................................10
Annex3.MidTermDeskReviewPOW2007-2011..............................................................................44
Annex4.NoteonInter-AgencyLeadershipCommittee......................................................................56
Annex5.Noteonhumanresources....................................................................................................59
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 iii
Annex6.Noteoninformationsystems...............................................................................................66
Annex7.Noteoncapitalinvestment..................................................................................................72
Annex8.Noteonhealthfinancingandhealthinsurance....................................................................78
Annex9.NoteonCHPS........................................................................................................................91
Annex10.Listofkeyinformants.........................................................................................................93
Annex10.Listofkeyinformants.........................................................................................................93
Annex11.Referencesanddocumentsconsulted................................................................................95
Listoftables
Table1:Sectorscore..............................................................................................................................2Table2.Annualsector-wideindicatorsfortheperiod2006to2009....................................................3Table3.ComparisonofInternationalreferenceprices,medianpricesinmission,publicanprivatesectorswithNHIAreimbursementprices(2007/2008).......................................................................15Table4.Selectedhealthserviceindicatorsasperholisticassessment2009......................................28Table5.Summaryofmainrecommendations.....................................................................................33
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 iv
Acknowledgement
Theindependentreviewofthehealthsector2009ProgrammeofWorkwasconductedonbehalfoftheMinistryofHealth (MoH)anddevelopmentpartnersbya teamof international andGhanaianexperts. International members of the review team were Andreas Bjerrum, Chet Chaulagai, LeoDeville,EdjoMartins,P.K.MensahandMiriamVisser.
Ghanaianmembersoftheteam,drawnfromtheMinistryofHealth,GhanaHealthServices,teachinghospitalsandacademia,were:Koku Awoonor-Williams, JanBorg,GeorgDakpallah, JanetKwansah,SallyLakeandFrankNyonator.
Theteamwouldliketothankthemanyindividualswhocontributedtothisreview.ParticularthanksareduetoJanetKwansahwhohasfacilitatedthedifferentmeetings,fieldvisitsanddatacollection.
The Review Teamwould like to express its gratitude to all officials and individualswho providedinformationandwhograciouslygavetheirtimeandsupporttothereviewprocess.
TheReviewTeam
Accra,April2010
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 v
Listofabbreviationsandacronyms
ADHA AdditionalDutyHoursAllowance
ARI AcuteRespiratoryInfection
ART AntiretroviralTherapy
ATF AccountingTreasuryandFinancial
BCC BehaviourChangeCommunication
BMC BudgetManagementCentre
CHAG ChristianHealthAssociationofGhana
CHIM CentreforHealthInformationManagement
CHN CommunityHealthNurse
CHO CommunityHealthOfficer
CHPS CommunityHealthPlanningandService
CIP CapitalInvestmentPlan
CMA CommonManagementArrangement
CMR ChildMortalityRate
CMS CentralMedicalStores
CYP CoupleYearsProtection
DA DistrictAssembly
DANIDA DanishInternationalDevelopmentAssistance
DCE DistrictChiefExecutive
DFID UKDepartmentforInternationalDevelopment
DHA DistrictHealthAdministration
DHIMS DistrictHealthInformationManagementSystem
DHMT DistrictHealthManagementTeam
DMHIS DistrictMutualHealthInsuranceScheme
DP DevelopmentPartner
EC EuropeanCommission
EOC EmergencyObstetricCare
EPI ExpandedProgrammeonImmunisation
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 vi
FC FinancialController
FP FamilyPlanning
GH¢ NewGhanacedis
GAS GhanaAmbulanceServices
GBS GeneralBudgetSupport
GDHS GhanaDemographicandHealthSurvey
GHS GhanaHealthServices
GOG GovernmentofGhana
GMA GhanaMedicalAssociation
GPRS GhanaPovertyReductionStrategy
GSS GhanaStatisticalServices
GWEP GuineaWormEradicationProgramme
HA HolisticAssessment
HF HealthFund
HIPC HighlyIndebtedPoorCountries
HIRD HighImpactRapidDelivery
HMIS HealthManagementInformationSystem
HR HumanResources
HRD HumanResourceDirectorate
IALC Inter-AgencyLeadershipCommittee
ICB InternationalCompetitiveBidding
ICT Information&ComputerTechnology
IEC Information,EducationandCommunication
IGF InternallyGeneratedFunds
ILO InternationalLabourOrganisation
IMR InfantMortalityRate
IRP InternationalReferencePrice
IRT IndependentReviewTeam
ITN InsecticideTreatedNet
JICA JapanInternationalCooperationAgency
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 vii
KATH KomfoAnokyeTeachingHospital
KBTH Korle-BuTeachingHospital
MDG MillenniumDevelopmentGoal
M&E MonitoringandEvaluation
MA MedicalAssistant
MCH MaternalandChildHealth
MDBS MultiDonorBudgetSupport
MDG MillenniumDevelopmentGoal
MICS MultipleIndicatorClusterSurvey
MMR MaternalMortalityRatio
MoH MinistryofHealth
MOFED MinistryofFinanceandEconomicDevelopment
MOLGRD MinistryofLocalGovernmentandRuralDevelopment
MOU MemorandumofUnderstanding
MTEF MediumTermExpenditureFramework
NAS NationalAmbulanceServices
NBTS NationalBloodTransfusionServices
NCD Non-CommunicableDisease
NDPC NationalDevelopmentPlanningCommission
NHI NationalHealthInsurance
NHIA NationalHealthInsuranceAuthority
NHIF NationalHealthInsuranceFund
NHIS NationalHealthInsuranceSystem
OPD Out-PatientDepartment
PE PersonalEmoluments
PFM PublicFinancialManagement
PNC PostNatalCare
POW ProgrammeofWork
PPM PlannedPreventiveMaintenance
PPME Policy,Planning,MonitoringandEvaluation
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 viii
PPP Public-PrivatePartnership
RCH ReproductiveandChildHealth
RDHS RegionalDirectorofHealthServices
RH ReproductiveHealth
RHA RegionalHealthAdministration
RHMT RegionalHealthManagementTeam
RHNP RegenerativeHealthandNutritionProgramme
RSIMD ResearchStatisticsandInformationManagementDirectorate
SBS SectorBudgetSupport
SD SupervisedDelivery
SWAp Sector-WideApproach
TA TechnicalAssistance
TBA TraditionalBirthAttendant
TH TeachingHospital
TTH TamaleTeachingHospital
TWG TechnicalWorkingGroup
U5MR Under-FiveMortalityRate
UNAIDS JointUnitedNationsProgrammeonHIV/AIDS
UNFPA UnitedNationsFundforPopulationActivities
UNICEF UnitedNationsChildren’sFund
USAID UnitedStatesAgencyforInternationalDevelopment
WHO WorldHealthOrganisation
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 ix
Executivesummary
Briefsummaryofthereportwillbeaddedtothefinaldraft.

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 1
1. Introduction
Theindependenthealthsectorreview2009wascarriedoutfromMarch15thtoApril2nd2010.Itispart of a broader annual review including Budget Management Centre (BMC) reviews andperformance hearings (involving districts, regions and heath related agencies); the inter-agencyreview;thehealthpartner’sreview;andthein-depthreviewofsomeagreedkeyareas.TheMinistryofHealth(MoH)anditsagenciesbrieftheParliamentarySelectCommitteeonHealthonthesectorperformance,progressandchallenges.Finally, findingsandrecommendationsarediscussedat theHealthSummitandthewayforwardmappedout.
The independent sector review has been carried out annually for many years by a mixedinternational and national expert team. Some ‘fatigue’ has been notedwith this intensive annualprocess of reviews. Collecting the necessary evidence and organizing timely interviews has beensomewhat difficult this year. The Independent Review Team (IRT) provides some commentsregarding the organization of the present review and recommendations regarding futureindependentreviewsinsection4.
This year the ToR specified the following key areas for review: a) non-communicable diseases; b)health servicedelivery including the functionalityof thedistricthealth systemand theprogress inprovision of emergency obstetric care (EOC;MDG4 and 5); c) human resource rationalization; d)monitoring and evaluation; e) capital investment; f) good governance and partnerships; and g)healthfinancingandfinancialmanagement.
Thenoverall objectiveof the2009annual review is toprovidean independentassessmentof theprogressmadeintheimplementationofthethreeyearlifespanofthe5YPOW2007-2011.ThelasttwoyearsofthecurrentPOWwillbeincorporatedintothenewMTDP2010-13(beingdeveloped).The present 2009 annual review has been complemented by a retrospective desk review of theimplementationofthe2007and2008POWs.ThelatterispresentedinAnnex3andsummarizedinsection2.2.
Duringthereview(boththedeskreviewandthe2009review)itbecameapparentthatsomeofthemain obstacles of the Ghana health sector to improve performance are in the broad domain ofgovernance. The IRTdecided to focus its effortsmore in this field (and less on thehealth servicedelivery part). As agreed with MoH, the main part of the feedback in this report deals withgovernanceandsummarisesmainsystem-relatedfindings.Specificannexesdealmoreindetailwithspecific elementsof the TOR. Inorder to improve ‘readability’ of the report andaccessibility to awideraudience,themainreporthasbeenkeptshortandfocused.
Section2ofthereportsummarisesthefindingsoftheholisticassessment2009(section2.1)andofthedeskreviewofthe2007and2008processesandachievements.Thefullreportsarepresentedrespectively inannex2and3.Thecoreofthe2009reviewispresentedinsection3ongovernanceandsectororganization.Annexes4to8bringsomeofthedetailsofspecificareasspecified intheTOR. Section 4 discusses the usefulness of the annual review and the main conclusions andrecommendationsaresummarisedinsection5.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 2
2. SectorPerformance
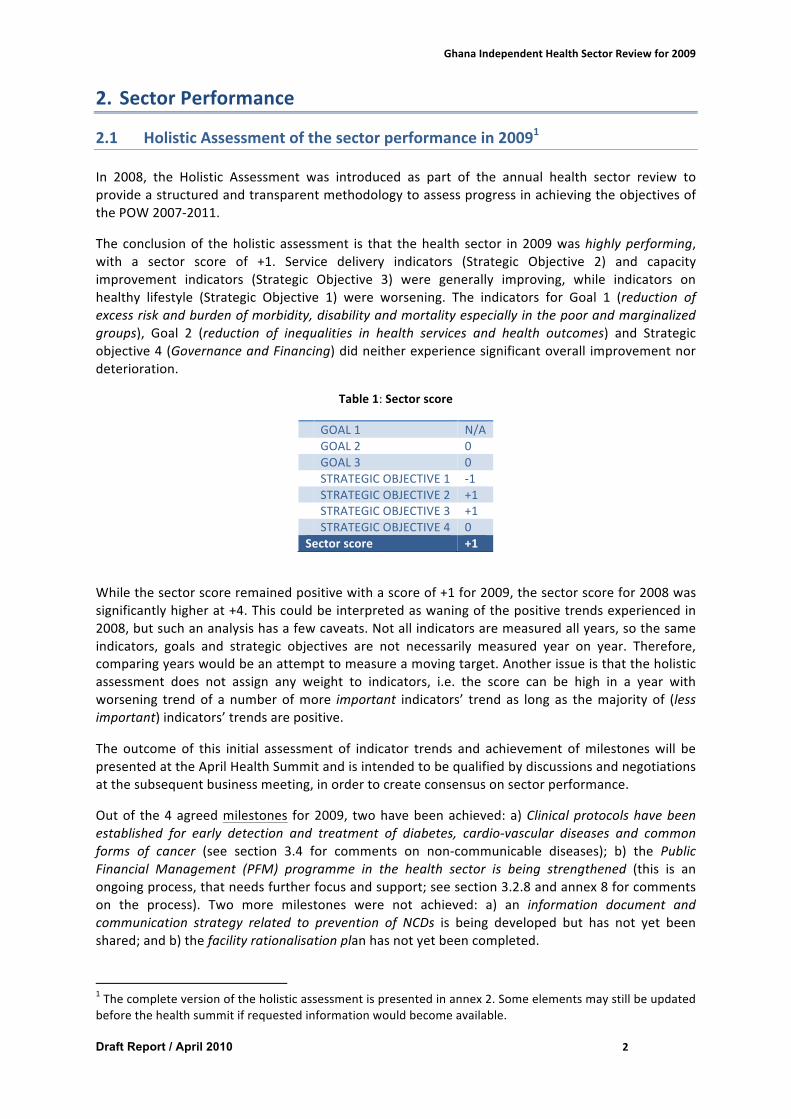
2.1 HolisticAssessmentofthesectorperformancein20091In 2008, the Holistic Assessment was introduced as part of the annual health sector review toprovideastructuredandtransparentmethodologytoassessprogressinachievingtheobjectivesofthePOW2007-2011.
The conclusionof theholistic assessment is that thehealth sector in2009washighlyperforming,with a sector score of +1. Service delivery indicators (Strategic Objective 2) and capacityimprovement indicators (Strategic Objective 3) were generally improving, while indicators onhealthy lifestyle (Strategic Objective 1) were worsening. The indicators for Goal 1 (reduction ofexcessriskandburdenofmorbidity,disabilityandmortalityespeciallyinthepoorandmarginalizedgroups), Goal 2 (reduction of inequalities in health services and health outcomes) and Strategicobjective4(GovernanceandFinancing)didneitherexperiencesignificantoverall improvementnordeterioration.
Table1:Sectorscore
GOAL1 N/A GOAL2 0 GOAL3 0 STRATEGICOBJECTIVE1 -1 STRATEGICOBJECTIVE2 +1 STRATEGICOBJECTIVE3 +1 STRATEGICOBJECTIVE4 0Sectorscore +1
Whilethesectorscoreremainedpositivewithascoreof+1for2009,thesectorscorefor2008wassignificantlyhigherat+4.Thiscouldbeinterpretedaswaningofthepositivetrendsexperiencedin2008,butsuchananalysishasafewcaveats.Notallindicatorsaremeasuredallyears,sothesameindicators, goals and strategic objectives are not necessarily measured year on year. Therefore,comparingyearswouldbeanattempttomeasureamovingtarget.Anotherissueisthattheholisticassessment does not assign any weight to indicators, i.e. the score can be high in a year withworsening trendof a numberofmore important indicators’ trend as long as themajority of (lessimportant)indicators’trendsarepositive.
The outcome of this initial assessment of indicator trends and achievement ofmilestoneswill bepresentedattheAprilHealthSummitandisintendedtobequalifiedbydiscussionsandnegotiationsatthesubsequentbusinessmeeting,inordertocreateconsensusonsectorperformance.
Outof the4agreedmilestones for2009, twohavebeenachieved:a)Clinicalprotocolshavebeenestablished for early detection and treatment of diabetes, cardio-vascular diseases and commonforms of cancer (see section 3.4 for comments on non-communicable diseases); b) the PublicFinancial Management (PFM) programme in the health sector is being strengthened (this is anongoingprocess,thatneedsfurtherfocusandsupport;seesection3.2.8andannex8forcommentson the process). Two more milestones were not achieved: a) an information document andcommunication strategy related to prevention of NCDs is being developed but has not yet beenshared;andb)thefacilityrationalisationplanhasnotyetbeencompleted.
1Thecompleteversionoftheholisticassessmentispresentedinannex2.Someelementsmaystillbeupdatedbeforethehealthsummitifrequestedinformationwouldbecomeavailable.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 3
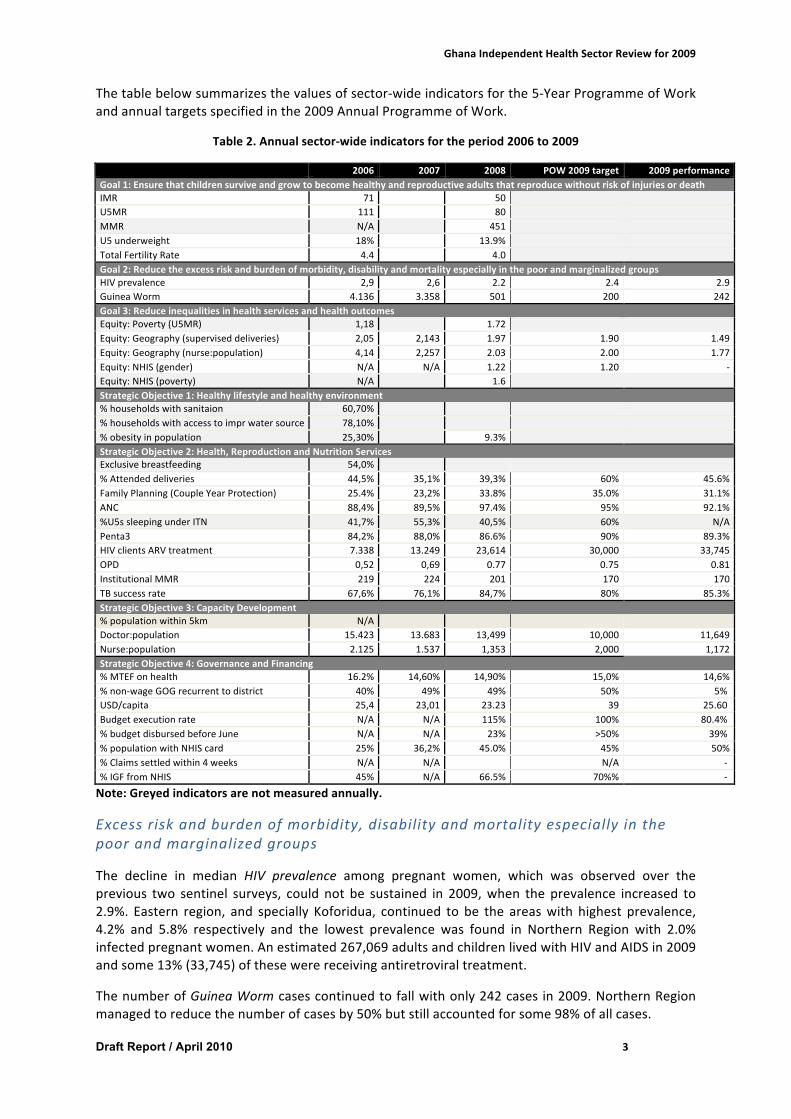
Thetablebelowsummarizesthevaluesofsector-wideindicatorsforthe5-YearProgrammeofWorkandannualtargetsspecifiedinthe2009AnnualProgrammeofWork.
Table2.Annualsector-wideindicatorsfortheperiod2006to2009
2006 2007 2008 POW2009target 2009performanceGoal1:EnsurethatchildrensurviveandgrowtobecomehealthyandreproductiveadultsthatreproducewithoutriskofinjuriesordeathIMR 71 50 U5MR 111 80 MMR N/A 451 U5underweight 18% 13.9% TotalFertilityRate 4.4 4.0 Goal2:Reducetheexcessriskandburdenofmorbidity,disabilityandmortalityespeciallyinthepoorandmarginalizedgroupsHIVprevalence 2,9 2,6 2.2 2.4 2.9GuineaWorm 4.136 3.358 501 200 242Goal3:ReduceinequalitiesinhealthservicesandhealthoutcomesEquity:Poverty(U5MR) 1,18 1.72 Equity:Geography(superviseddeliveries) 2,05 2,143 1.97 1.90 1.49Equity:Geography(nurse:population) 4,14 2,257 2.03 2.00 1.77Equity:NHIS(gender) N/A N/A 1.22 1.20 -Equity:NHIS(poverty) N/A 1.6 StrategicObjective1:Healthylifestyleandhealthyenvironment%householdswithsanitaion 60,70% %householdswithaccesstoimprwatersource 78,10% %obesityinpopulation 25,30% 9.3% StrategicObjective2:Health,ReproductionandNutritionServicesExclusivebreastfeeding 54,0% %Attendeddeliveries 44,5% 35,1% 39,3% 60% 45.6%FamilyPlanning(CoupleYearProtection) 25.4% 23,2% 33.8% 35.0% 31.1%ANC 88,4% 89,5% 97.4% 95% 92.1%%U5ssleepingunderITN 41,7% 55,3% 40,5% 60% N/APenta3 84,2% 88,0% 86.6% 90% 89.3%HIVclientsARVtreatment 7.338 13.249 23,614 30,000 33,745OPD 0,52 0,69 0.77 0.75 0.81InstitutionalMMR 219 224 201 170 170TBsuccessrate 67,6% 76,1% 84,7% 80% 85.3%StrategicObjective3:CapacityDevelopment%populationwithin5km N/A Doctor:population 15.423 13.683 13,499 10,000 11,649Nurse:population 2.125 1.537 1,353 2,000 1,172StrategicObjective4:GovernanceandFinancing%MTEFonhealth 16.2% 14,60% 14,90% 15,0% 14,6%%non-wageGOGrecurrenttodistrict 40% 49% 49% 50% 5%USD/capita 25,4 23,01 23.23 39 25.60Budgetexecutionrate N/A N/A 115% 100% 80.4%%budgetdisbursedbeforeJune N/A N/A 23% >50% 39%%populationwithNHIScard 25% 36,2% 45.0% 45% 50%%Claimssettledwithin4weeks N/A N/A N/A -%IGFfromNHIS 45% N/A 66.5% 70%% -
Note:Greyedindicatorsarenotmeasuredannually.
Excessriskandburdenofmorbidity,disabilityandmortalityespeciallyinthepoorandmarginalizedgroups
The decline in median HIV prevalence among pregnant women, which was observed over theprevious two sentinel surveys, could not be sustained in 2009,when the prevalence increased to2.9%. Eastern region, and specially Koforidua, continued to be the areaswith highest prevalence,4.2% and 5.8% respectively and the lowest prevalence was found in Northern Region with 2.0%infectedpregnantwomen.Anestimated267,069adultsandchildrenlivedwithHIVandAIDSin2009andsome13%(33,745)ofthesewerereceivingantiretroviraltreatment.
ThenumberofGuineaWormcasescontinuedtofallwithonly242casesin2009.NorthernRegionmanagedtoreducethenumberofcasesby50%butstillaccountedforsome98%ofallcases.

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 4
Equity
2009was the firstyear,where itwaspossible toestimate thesurveybasedequity indicators.Theindicatorframeworkholdstwoindicatorsasproxyforgeographicalequity,superviseddeliveriesandnurse to population ratio by region. The indicator for geographical equity of supervised deliverycontinued previous years’ improvement. Not only is the gap between the best and poorestperformingregionclosing,bothregionshavealso improvedoverall coverageandNorthernRegionimproved coverage by almost 40%. Upper West Region saw the most significant reduction incoveragebynearly10%,andisnowclosetotheperformanceofNorthernRegion.
In2009,therewasfurthermoreanimprovementinequitabledistributionofnursesamongGhana’s10regions.UpperWestRegionhadthehighestnumberofnursesperregionalpopulation.AshantiRegioncontinuedtohavethelowestnumberofnursesperpopulation,butsawamarkedincreaseintotalnumberofnursesin2009(26%).
Thedoctor/population ratio increased from2008 to2009by13%.Thehighest relative increase innumberofdoctorswasrecordedinNorthernandBrong-AhafoRegions,butNorthernRegionisstillthe region with lowest number of doctors per population. With a total of 895 doctors, 43% ofGhana’sdoctorswerepracticinginGreaterAccraRegion.The3NorthernRegionshaveatotalof82doctors,whichcorrespondstolessthan4%ofdoctorsinthenation.
The equity indicators forpoverty areU5MR andNHIS cardholders, bywealth quintile. The equityindicator for poverty (U5MR) was measured based on the DHS 2008. The equity indicator isestimatedat1.72. Since2003,Ghanahas seena significant reductionofU5MRnationwide for allwealthquintiles;however, the reduction inU5MRhasbeengreater in thehighestwealthquintilecompare to the lowest. Therefore, the distribution of U5MR by wealth has become increasinglyunequal.TheNHISCardHolderratiobywealthquintilewasmeasuredforthefirsttimebasedontheDHS2008results.Thecalculationshowsthatsignificantlymoreindividualsbelongingtothehighestwealth quintile register compared to the lowest quintile. This is especially evident for the malepopulation.
Healthylifestyleandhealthyenvironment
Obesity (BMI ≥ 30) among women aged 15-49 increased by 15% from 2003 to 2008, and whilealmost10%ofthefemalepopulation15-49isobeseover20%isoverweight.With19.4%ofwomenintheagegroupbeingobeseand25.1%overweight,GreaterAccraRegionhadsignificantlyhigherprevalenceofobesityandoverweightthananyotherregion.
ProvisionofHealth,ReproductionandNutritionServices
Most health service indicators experienced a significant positive trend from 2008 to 2009. Inaccordancewiththetargets for improvedmaternalandneonatalhealthsetout in thePOW2009,theindicatorsforsuperviseddeliveriesandinstitutionalMMRimproved.Thispositivetrendstartedin2007.
From2008 to 2009, the coverage of pregnantwomen,who received one ormoreantenatal carevisits,droppedby5.4%.Inthesameperiod,theproportionofpregnantwomenwhoreceived4ormorevisitsincreasedsignificantlyfrom63.8%to81.6%.Thisindicatesthatthemajority(almost90%)ofwomennowfollowtherecommendedANCcourseofminimum4visits,whichcanbeinterpretedasanoverallimprovementofantenatalservicesinthecountry.
The proportion of deliveries attended by a trained health worker increased by 17%, and hencecontinued the positive trend experienced since 2007. The DHS 2008 estimated the percentagesomewhathigherat58.7%.Adeeperanalysisof theDHS2008data reveals that therewere large
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 5
regional variations in the indicator. In Greater Accra Region 84.3% deliverieswere attended by askilledprovider,whileonly27.2%wereattendedbyaskilledproviderinNorthernRegion.Alsotheroutinehealth information indicates thatNorthernRegionperformed relativelypoorer thanotherregions, the regiondidhoweverachievemajor improvementof this indicatorbyalmost40%from2008to2009.
The institutionalMMR continued thepositive trend,andwas reducedby15% from2008 to2009.Almostall regionsachieved improvementof this indicator,but inUpperWestRegion therewasaseriousincreaseintheMMRby145%from109to267per100,000livebirths.Thetotalnumberofmaternaldeathsrecordedintheregionincreasedfrom19to41.
From2008to2009,contraceptiveprevalenceratedroppedby8%.Whilelongtermcoupleyearsofprotection(CYP)remainedataround142,000,shorttermCYPdroppedby33%from654,072in2008to439,573in2009.TheindicatortrendcorrespondswellwithinformationpresentedtothereviewteamconcerningageneralshortageofshorttermmethodsinGhanaduringthepreviousyear.Thesocialmarketedbrandsofcondoms,e.g.GhanaSocialMarketingFoundationbrand,which in2008constitutedmorethanhalfofallcondomssoldinGhana,havereportedlybeeninparticularshortagein2009.
AfteraslightdropinPenta3coveragein2008,performanceisnowbackontrack,almostreachingthe target of 90% coverage. TheDHS 2008 estimated the percentage of Penta 3 at 87.7%,whichcorrespondswellwithroutinelycollecteddata.AregionalbreakdownoftheroutinedataindicatesthatcoverageinGreaterAccraRegionissignificantlowerthatthenationalcoverage.ThiscouldnotbeconfirmedbyanEPIsurveyfrom2009,whichwasperformedinGreaterAccraRegionandshowedsignificantlyhighercoverageofPenta3at96.1%.
Outpatient(OPD)visitspercapitacontinuedpreviousyears’ increaseandreachedthe2009target.WhileeveryinhabitantofBrongAhafoRegioninaveragevisitstheoutpatientdepartment1.15timesayear,peopleofGreaterAccraandNorthernRegionhaveanaverageutilisationofOPDserviceslessthanhalfofBrongAhafoRegion.
GovernanceandFinancing
Thetotalnumberofcardholders increasedfrom10,417,886in2008to12,123,338in2009.Thisis,however, an accumulated figure of cards issued since health insurance started, and the actualnumber of individuals holding a validNHISmembership card in 2009 is therefore expected to belower due to health insurance dropout (e.g. lack of renewal, death and emigration). It has beenspecifiedbytheNHIAthatthefigurerepresentsanaccumulationofindividualswhowereissuedoneor more cards and not the accumulation of cards issued, i.e. the figure increases every time anindividualrenewshisorhermembershipcard.
Regionofexcellence
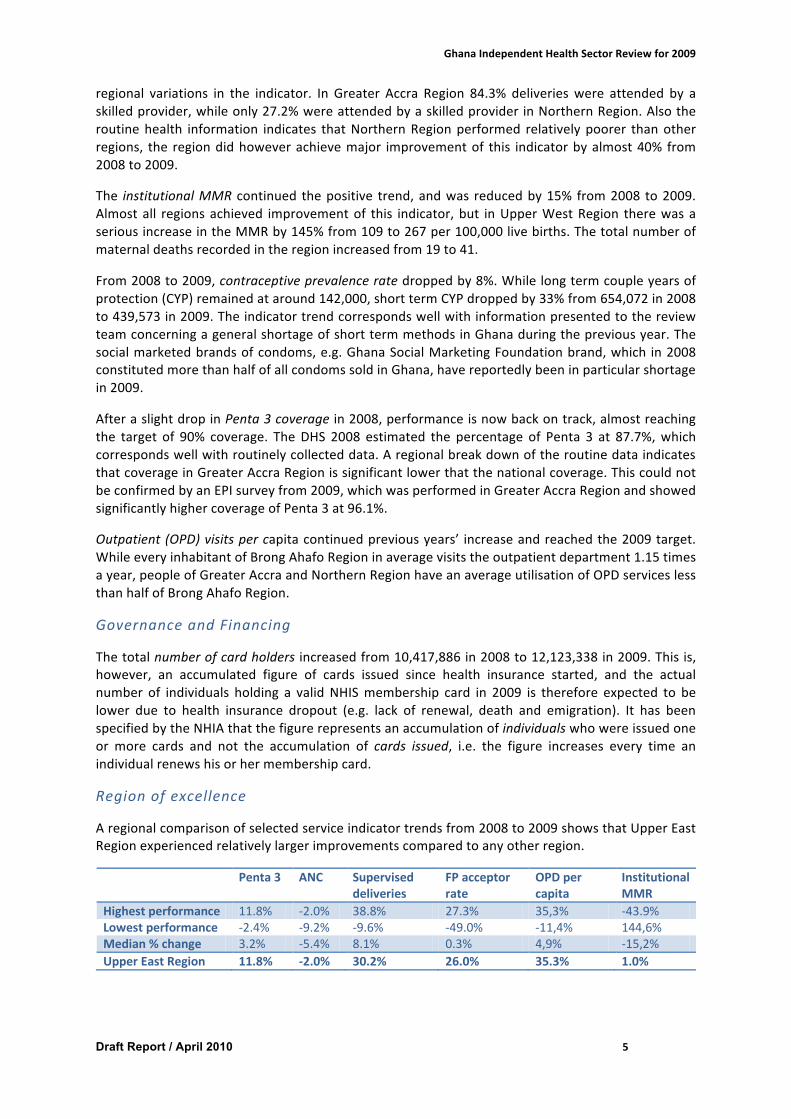
Aregionalcomparisonofselectedserviceindicatortrendsfrom2008to2009showsthatUpperEastRegionexperiencedrelativelylargerimprovementscomparedtoanyotherregion.
Penta3 ANC Superviseddeliveries
FPacceptorrate
OPDpercapita
InstitutionalMMR
Highestperformance 11.8% -2.0% 38.8% 27.3% 35,3% -43.9%Lowestperformance -2.4% -9.2% -9.6% -49.0% -11,4% 144,6%Median%change 3.2% -5.4% 8.1% 0.3% 4,9% -15,2%UpperEastRegion 11.8% -2.0% 30.2% 26.0% 35.3% 1.0%
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 6
Itwouldbe interesting to investigate furtherwhyUERhasmade suchmarked improvements andwhetherlessonscanbelearntforotherregions.
ForadetaileddescriptionoftheHolisticAssessmentToolandunderlyingprincipalsaswellasdetailsofthe2009estimationspleaserefertoannex2.
2.2 MidTermDeskReviewPOW2007-2011Themediumtermreviewtookaspointofdeparture tocompare theoriginal5year strategicplanand ProgrammeofWork (POW) titled ‘wealth throughhealth’with the subsequent annual POWs(2007,2008and2009)andreviews(2007and2008)toanalysewhetherandinwhichwayperceivedand actual priorities have been taken forward from one plan to the other, as evidenced in thevarious reviews. It therefore attempted to measure process and not necessarily progress orachievements thatare the subjectsof theannual independent reviewsandwhereto, if applicable,reference ismade. Themedium term reviewwas hence limited in scope and restricted to a deskreviewofthedifferentdocumentssince2007andtriestocomplementtheindependentreviewfor2009.The full textof thedeskstudy ispresented inannex3while thischapter isonlydevoted toemerging‘redlines’intheprocessoftheimplementationofthe5yearPOW.
More specifically, this desk review has taken ahistorical look at progress, process and actions bycomparingidentifiedintentionsforchangewithactualchangesanditsimpact/effectsonprogress.AdifficultyincomparingthethreesubsequentannualPOWsversustheoriginal5yearPOWistheshiftin2008fromathemebasedapproachtoprogrammingtoanoperationalagencyapproachwhilethesequentialreviewswerebasedonthenperceivedattentionareasfortheMinistryofHealthcausingthemtonotcoverallaspectsofthePOWunderreview.Intermsofoutputandoutcome,however,the availability of a stable set of sector wide indicators allows to draw some conclusions aboutprogress that are captured in the 2009 holistic assessment (see section 2.1) which, as earliermentioned,canbeseenasareviewofthecumulativeoutcomeoftheimplementationofthe5yearPOW.Forajudgementontheprocessofplanningandreviewwithinthesectorthisveryclearshiftintheplanningmodalityflagswhatcouldbeasignificant‘redline’ofincreasingfragmentationwithinandbetweentheactorsinthesector.Itindeedraisesthequestionwhetherthechangetoanagencybased annual POW in 2008 is a symptom of an evident ‘silofication’ of the sector2. Some of theunderlyingreasonsforthiswillbediscussedfurtherinthereport(seesection3).Inadditiontotheinevitableandnatural‘organicdrift’versustheoriginalgoals,objectivesandactivitiesofthe5yearPOW,thisintroducedthreeissuesfortheprogressandfollowupofthesector:
• Programmaticelementsandactivitiesgetlosttofollowup:Thewithdrawalofactivitiesintothedistinct silos - that are sometimes competing for the same resources - has caused the loss ofsynergies for ‘crosscutting’ issues that require sector wide planning. Activities referring topersonalresponsibilitiesandlifestyle(regenerativehealthandnutrition)wouldbeexamples.
• Programmaticelementsandactivitiesthatarewidelyregardedasprioritiesfortheultimategoalofthe5yearPOW(WealththroughHealth)arenotsufficientlytranslatedintoactionbecauseofalackofintra-sectorcollaboration.Theyappearyearafteryearwiththesamerecommendationsinthesubsequentindependentreviews.AnexampleforthisdeviationwouldbetheexpansionofCHPSzones.
• Withdrawalofactivities intoingeneraltechnical inwardlookingdepartmentsandagencieshasskewed thesector towardsbiomedical solutions forhealthwith lessattention to ‘softer’multi-sectorissues.Examplesherewouldbewater,sanitationandnutrition.
2With ‘silofication’wemeanherethecleartrendofantagonisticmanagementof thedifferentdepartmentsandagencies(silos)thatconstitutethe(public)healthsectorandwhichseemstohindertheholisticapproachoftheoriginal5yearstrategyandPOW.

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 7
3. Governanceandhealthsectororganisation
3.1 Ahealthsectorevolvingoverthepastdecadesfromfragmentationtointegrationandagaintofragmentation
The health sector in Ghana has gone through different periods of change which have beenextensivelydocumentedanddiscussedinliterature3,4.Inthe1980stensionexistedbetweenapolicyenvironment aiming at financial decentralisation, strengthening district health systems andintegrated approach to service delivery and the fragmented reality of 13 different healthprogrammes, donor driven projects and balkanisation (donors supporting specific regions). Thesetensions lead in the 1990s to a progressivemove to do business in a different way, aiming at aholistic sectoral approach, using GoG/MoH systems and strengthening institutional capacity. Aprocess was established to discuss and negotiate health sector priorities and interventions andallowing theMoHmore authority on comprehensive resource allocation and utilisation, includingpartofdonorfunds.ThefirstMediumTermHealthStrategy,theFive-YearProgrammeofWorkandtheCommonManagementarrangements(CMA)werereadybytheendof1996,whichleadtothesigning of theMoU betweenMoH and DPs in April 1998. The purchaser-provider split, with thecreation of theGHS,was implemented in the same period. Themain trustwas a single plan andbudget, jointly supported by GoG and DP resources, using common systems; moving from afragmented to a comprehensive, more integrated approach. Reportedly, this process of changemanagementhasbeenfundamental forthehealthsectorand implementedundervariousdegreesof constraints and trust. Thepurchaser-provider split,while a rational choicehasbeena causeoftensions and power struggle in the sector. On the other hand, service delivery improved.Interestingly,we notice todayagain amove away from a comprehensive, sector-wide, integratedapproach regarding health service organisation and health service delivery to an increasinglyfragmentedapproach.Thisisreflectedinseveraldynamicsinthesector,butmainly:a)anincreasingnumber of health (related) agencies without effective communication between agencies andwithout performance based / results based financing; b) a greater complexity/variety in healthfinancing mechanisms; with an increasing tendency to earmarking financial and programmeresources;andmoreemphasisonclinical/curativecarethrougha(relativelynew)healthinsurancefinancing;andc)a lossoffocus intherespectivePOWs,movingfromathemebasedtoanagencybasedfocus(seesection2.2andannex3).
Atthesametime,thesectorisconstrainedbysomemajorinefficiencieswhichinclude:a)thedelaysin funding and in reimbursements; b) the high prices formedicines; and c) the learning by doingprocessofthenationalhealthinsurance.
Other system issues that the IRT has addressed include human resources, health service delivery,informationmanagementandcapitalinvestment.
Someoftheaboveconstraintsmakeit increasinglydifficultforDHMTstocomprehensivelyplanforlocallysetpriorities.
3 Edward Addai& Liz Gaere, Capacity-building and systems development for SWAPs: the experience of theGhanahealthsector,January2001.4DeniseVaillancourt,Dohealthsector-wideapproachesachieveresults?Emergingevidenceandlessonsfromsixcountries(includingGhana),IEGWorkingPaper2009/4.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 8
3.1.1 Fragmentationandpoorcoordinationofessentialgovernancefunctions
In the present organisation of the health sector the central MoH (hereafter called MoH) isresponsible for policy development, regulation, health financing, resource mobilisation andallocation,monitoring and evaluation of sector performance, and engagingwith service providers(GHS,CHAG, teachinghospitals, privateproviders).GHShasover the yearsdevelopedas a strongorganisationresponsibleforallpublicserviceprovision(withtheexceptionoftheteachinghospitals)in closecollaborationwith theCHAGhealth facilitiesand toa lesserextentwithprivateproviders(mainly in urban settings). TheGHShas longbeen the sole ‘main elephant’ in the sector, but hasrecently been complemented by another powerful body, theNHIA,which increasinglymanages asubstantialpartofthesectorresourceenvelope.
ArecenttrendisthatsomeessentialservicefunctionsoftheGHSarebeing‘removed’fromGHSandorganised in separate semi-autonomous agencies. Examples are the National Blood TransfusionServices(NBTS),theNationalAmbulanceServices(NAS),thementalhealthhospitals.ThelistcouldbecomplementedinthefuturebyforexampletheLaboratoryServices,RadiotherapyCentres,etc.asisthecaseinsomecountries.Whiletheremaybearationaleforestablishingsemi-autonomousagencies, the IRThas the followingobservations:a) incountrieswherethis typeoforganisation isbeingpursued,thereisusuallynocomprehensivepublicproviderserviceagencysuchastheGHS;b)it seems that GHS was not always in favour of such separation of functions, which may createtensions between new and existing agencies; c) reportedly newly created agencies do no longercommunicateeffectivelywiththeGHSastheyare‘accountable’totheMoH;andd)theMoHhasnotengagedwithdifferenthealthagenciesthroughaperformanceorresultsbasedcontract,makingitdifficultfortheMoHtoguideandfollow-uponagencyperformance.
Multiplication of (semi) autonomous agencies requires increasingly strong leadership of theMoHandrelevantseniormanagementandtechnicalskillsatcentralMoHtosteer,coordinateandensurethat all agencies implement sector priorities in a complementary and reinforcing way. TheInteragency Leadership Committee 5 (see annex 4 for a more detailed analysis) can fostercoordinationbetweenagenciesbuthasnomandate toenforce collaborationanddecisionsmade.This situation may lead to further fragmentation and increased complexity of the sectororganisation6.
WhiletheMoHhassomeofthecarrotsitdoesnotseemtohaveaneffectivestick.Ontheonehand,the MoH does not seem to be anymore in full control of the sector financial resources. This isreflectedby:a)theapparentlackofauthoritybytheMoHtosteertheNHIAwhichisresponsibleforan increasingly important part of the sector resources (information sharing and communicationbetweentheNHIAandtheMoHseemstobeatbestunsatisfactory);b)theincreasingimportanceofearmarked donor funding versus SBS and previously used flexible health fund; and c) reportedlylimited skills at theMoH to effectively negotiate withMoF. This reality is contrasted by an everincreasing request and competition by all agencies for more resources, as was apparent in thepresentationsmadebymostagenciesduringtheinter-agencymeeting.Ontheotherhand,theMoHhasnot(yet)introducedeffectivemanagementtoolsinordertofollow-uponagencyperformance:a) no performance based or results based contractingwith health agencies7; and b) a reportedly5TheInteragencyLeadershipCommittee,chairedbytheMinister, isanewforumcreatedin2008todiscusscross-cutting issues (e.g. referral services, ambulance services…) on a quarterly basis. It helped agencies‘talkingtoeachother’andseekingconsensusbuthasnodecisionpower.Itwasnotveryactivein2009duetothetransitionbetweengovernments.Meetingsarenotlinkedtotheannualplanandbudgetcycle.6 There is a tendency to remove responsibilities from GHS (blood transfusion, ambulance services, mentalhealth,training,etc.).IsthisaconsciousmovetoreduceGHSpowerortoincreaseefficiency?7Performancecontracting(GHS–Region–District)hasbeen introducedbeforebuthasnotbeenenforced/usedeffectively.Accordingtosomeinformants,erraticGOGfundingtendstomakecontractingineffective.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 9
weakmonitoringandevaluationfunctionattheMoH.Theriskisthatagencyperformanceisthusnoteffectivelymonitored,resultinginlessthanoptimalsectorperformance.
TheNHIAcombinesregulatoryfunctions(e.g.accreditation;servicepackage;resourceallocationandreimbursementpolicy),financing (reimbursementofclaimsand ‘reinsurance’,subsidizingtheMoHfor somepreventionactivitiesand investments,projectsofMemberofParliament, investments inthenationalinsurancefunction,overhead,etc.)andcontrol(numberandtypeofservicesdelivered,prescriptionofmedicines).Somecountrieshaveoptedtoconcentrateallthreefunctionsinasinglepowerfulbody,butforeseechecksandbalancesthroughtransparentandeffectivenegotiationanddecision-making modalities involving civil society, professional bodies, government and privatesectorrepresentatives.Othercountrieshavedecidedtosplitfunctionsbetweendifferentagencies8.Concentratingall threefunctions inonesinglebody,without institutionalisingsufficientchecksandbalances,carriestheriskofshiftingpowerbalancesinthesector.Thisrequireseffectivemechanismsto be in place for coordination, communication, negotiation, guidance and follow-up. From thepresentreviewitisnotevidentthatthosemechanismsaresufficientlywelldevelopedandeffective.Atpresent,theNHIAwouldbenefitfromincreasedtransparencyandeffectivecommunicationwiththeMoH. The perception ismore of competing entities in the sector rather than complementaryagencieswithaspecificmandateandalignedwithagreedcommonsectorpriorities.
Accordingtothepresentlaw,theNHIAisinprincipleaccountabletotheMinisterofHealth,butdefactoNHIAseemstobeaccountabletothePresidentandParliament,reducingtheauthorityoftheMinister to ensure effective complementarity between financing andprovisionof services; and tomonitoringNHIAperformance9.ThenewdraftHIbillspecifiestheestablishmentofaNationalHealthInsurance Commission,with regulatory authority over the National Health Insurance Scheme andany Private andMutual Health Insurance Schemes, and with an expanded membership to covercritical stakeholders. It also aims at ensuring more structured collaborations and interactionsbetweentheMinistryofHealth(MoH),theMinistryofFinanceandEconomicPlanning(MOFEP),theNational Insurance Commission (NHIC) and the National Health Insurance Authority (NHIA) andbetween the Regional and District Offices of the Schemes and the Political and AdministrativeAuthority in the Regions and Districts. Depending on how these decisions are translated intopractice,thenewbillmaygoalongwayinaddressingtheaboveissues10.
It is unclear how the MoH ensures that the national health insurance supports national policy/sector objectives, as being translated into target setting and implementation by some agencies(e.g.GHS). ThereseemtoexistfeweffectiveavenuesforformalcollaborationbetweenMoH,NHIAandGHS/CHAG.AlthoughbylawaccountabletotheMinisterofHealth,theNHIAdataarenoteasilysharedwithMoHseniorstaff11.
8 InMoroccoforexample, theNationalHealth InsuranceAgencyhasmainlyaregulatory function.Financingand control functions are managed separately by specific agencies (for public employees, for privateemployees,forthe informalsector)andthepublicauthorities(MoHandMLGforthesubsidyschemeofthepoor).SimilaranddifferentorganisationalstructuresexistinseveralEuropeancountries.9TheNHIACEOisappointedbythePresidentandreportstotheParliamentarySelectCommittee.TherecentNHIAreportsfor2009werenotavailableatMoHatthetimeofthereview.10 The IRThasonly seen theSeptember2009versionof thedraftbill. Reportedly, some important changesmay still have been inserted in the draft bill that is presently with Cabinet and would be presented toParliament in its next session (May 2010?), more specifically regarding the organisational structure. SomeinformantssuggestthattheideaoftheNHICwouldhavebeenabandoned,whileaseparatefundmanagementteamwouldberesponsibleforadministeringtheNHIF.11 As a consequence theMoHwas not in a position to share up-to-date informationonNHIAwith the IRT.RequestsforspecificdatasubmittedbytheIRTdirectlytoNHIAhavenotbeenhonouredbythetimeofwritingthereport.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 10
Closer collaboration between key agencies is fundamental for effective service delivery. MoHshould continue towork closelywithGHS, CHAG, other health agencies and teaching hospitals indeveloping policy and strategic plans. In addition,MoH should work closely with NHIA on policyissuesregardinghealthfinancingandhealthinsurance.AlsoMoH,GHS,CHAG,THandNHIAshouldwork together at a technical level on issues such as basic package, provider payment systems,provider claimmanagement, control of provider and client behaviour. The above could be donethrough joint technical working groups (linked to the Inter-Agency Leadership Committee orinstitutionalisedattheMoH).
Therather‘insecure’politicalenvironmentinthepastyearsmayhavecontributedtosomeaspectsofthefragmentationdescribedaboveortothefactthatconsequencesfragmentationhaveyettobeaddressed.Whilethechangeofgovernmenthascreatednewpositivedynamics, thereality is thatministers and deputyministers have changed on several occasions over the past years. Also, topmanagement(ChiefDirectorandHeadofPPME)havebeeninactingpositionforquitealongtime.
The upcoming Public Health Act, the new NHIA bill and the CMA provide opportunities toreorganizeandstrengtheneffectivecoordinationofhealthagenciesbytheMoH/GOGwithaviewtoensurethatsectorprioritiesarebeingmet.Itwouldhoweverrequirethatcomplementarityandharmonizationbetweenthethreeinitiativesisbeingensuredbeforetheyarefinalized.
3.1.2 Whiletheresourceenvelopeforhealthcontinuestoincrease,fundingshiftstowardsclinicalcareandlessflexiblefunding
Thetotalresourceenvelopeforthehealthsector(asperbudget)hasmovedfromGHc21percapitain2006toGHc32percapitain2008andGHc38percapitain200912(equivalenttoabout27USDper capita). But sector outputs, although improved, have not followed the same trend. And allagenciesrequestmorefundsandresources.Whilethispercapitaresourceenvelopeisamongthehighest in Sub Saharan Africa, critical sector outputs are rather average. This raises somefundamentalquestions:Wheredoesallthemoneygo?Howcanefficiencyofresourceallocation/usebeenhanced?
12Double-countingofasignificantproportionof IGFswhichisfundedthroughNHIFcouldoverstatethetrueMoHshareofthebudget.Ontheotherhand,substantiallevelsofoff-budgetfinancingarenotincludedinthepresentedfigures(seeannex8).This2009figuremaystillneedtobeadjusted.
Keyrecommendation
TheMoHtoensurestrongsectorleadership,enforcingitsmandate.Thiscouldincludethefollowinginitiatives:
• Implementandmonitorperformance/resultsbasedcontractwithallagencies• StrengthenmonitoringandevaluationfunctionsattheMoH• Strengthen the role of the Inter Agency Leadership Committee (see annex 4, p47 for
specificrecommendations)• Createavenuesforformalcollaborationbetweenagenciesonspecificissues(TWG)• Confirmtoplevel(Acting)managementpositions
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 11
Thenew financingmechanismofhealth insurancehas substantially increased resourceavailabilityfor health,mainly for clinical services13. As discussed further (see section 3.2.4) there is scope forefficiencygainsunderthepresenthealthinsurance.OntheotherhandavailabilityofGOGresourcesfor operations (supervision,monitoring, etc.) and public health and preventive activities seem tohavebeenreduced.Thisismainlyreflectedinthecontinuousunderfundingoftheitem2andmorespecifically item3oftheMoHbudget.This ispartiallyexplainedbythefactthattheserviceclaimsreimbursedbytheNHIcoversomeofthefacilitybasedoperationalcostsandispartiallytheresultofcontinuousoverspendingonitem1.ComplementaryfundingbyDPsthroughSBS/HFandearmarkedfunds ensures that prevention and public health activities remain resourced, but this is in fact afundamentalresponsibilityoftheGoG(publichealthgoods)whichisinsufficientlyresourcedbyowngovernment finances. The latter requires for an informed policy dialogue by DPs and MoH withMoFEP. Proper tracking of expenditures for prevention and public health would allow for moreevidencetoconvinceMoF(seeannex8forasimplifiedflowofhealthfundsunderitem3).
While increasing the overall resource envelope, the new financing mechanism shifts resourceavailability for comprehensive district health planning and implementation away from DHMTs toclinical service providers. Presently, themain source of income for districts is IGF14, largely fromclaims reimbursed by the health insurance, but these resources arewith health facilities (serviceprovision fund and drug revolving fund). Complementary GOG resources for implementation ofdistricthealthplanshaveconsequentlybereduced. InordertocompensateforthisreductionandallowtheDHMTtocoversomedistrictpriorities,somedistrictsrequestfacilitiestoallocateacertainpercentageoftheservicefundtotheDHMTforpublichealthactivities,supervision,etc.(seeannex8).
At present, theNHIF reimbursement for services to providers is not linked to performance targets(clinical care or public health). This means that MoH and GHS cannot steer providers to ensureachieving public health targets with an important part of the sector resources. Many westerncountrieshaveoptedforthistypeofhealthinsurance,traditionallyexcludingpreventionandhealthpromotion,andnotlinkedtoachievingsettargets.However,becauseofresourceconstraints,thereis an upcoming trend to increasingly link individual prevention and lifestyle to cost of healthinsurance. Other countries have chosen to link health insurance to sector and facility based (ortargetgroupbased)clinicaland/orpublichealth targets.Basically,healthprovidershaveaccess toincreased reimbursement or allowanceswhen reaching pre-defined service targets15. Through theNorwegian Trust Fund, the WB is starting up a pilot on a performance-based or result basedpaymentmechanismforprimaryhealthcareservices.Iftheresultsarepositive,itmaydirectpolicydecisions in this domain.Reportedly, theWBproject allows for close collaborationbetweenmainstakeholders,includingMoH,NHIA,GHS,CHAG,etc.
WhilehealthinsuranceclaimsreimbursedtohealthprovidersarefinancialresourcesoverwhichtheDHMT has less control, the other resources available under item 2 and 3 and via specific healthprogrammesare increasinglyearmarked.This includesGFATM,earmarkeddonorfunds,traditionalring-fencing of certain priorities by MoH (such as FP commodities and Guinea Worm activities),specific MoH programmes (e.g. HIRD). Increasingly MoH tend to ‘ring-fence’ GoG/SBS resourcesunderitem3aswell.AlthoughSBSresourcesaresupposedlyflexible,theytendtobecomemoreandmoreearmarkedbefore reaching theoperational level. Thiswasquitedifferentwhen theHealth13Unconfirmeddata suggest total expected revenue forNHIA ofGHc 361.8m for 2009; total payments areexpectedtobeGHc463.7mwithanexpectednetdeficitofGHc206.9mfinancedfromthereservefunds.GHc464mistobecomparedwiththeGHc922mforhealthintheMTEF(morethan50%).14AsimilarpatternappliestoCHAGfacilities(GOGGHc38mofwhich99%PE;IGFGHc21m;DPGHc1.5m).15Egypthaspilottestedthisapproachformanyyearsthroughahealthservicesfundunderthenationalhealthinsurance.Performancetargetsincludedquantitativetargets(e.g.numberofpatientsattendedperhour;EPIcoverage; ANC attendance; etc.) and qualitative targets (patient files updated; patient satisfaction;prescriptionofmedicines;etc.).
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 12
Fundwasstilloperationalandamainsourceofflexiblefundingfordistricts.WhiletheIRTconsidersring fencing for specific priorities acceptable at the national level, comprehensive district healthplanningand localpriority settingbecomesmeaningless ifmost resourcesarebeingearmarkedorring-fencedatthecentrallevel.
3.1.3 Giventhedynamicchangesinthesector,arewelosingfocus?Anddowekeepprioritiesright?
Theshiftinthe2008POWfromathemebasedapproachtoprogrammingtoanoperationalagencyapproachhasprobably contributed to the fact that someaspectsof the5 yearPOWwere lost tofollowup,ornotsufficiently translated intoaction,orwerenot implementedatall.TheMTR(seesection2.2andannex3)discusses this inmoredetail.Verticalisation, fragmentation (of agencies)and its opposite integration have caused overlap and gaps between the respective areas of thePOW. The switch in 2008 to an operational, agency based POW is symptomatic andmight havecontributed, as cause or consequence, to a fragmented approach towards these functionalinterventionareas.Cautiouslya conclusionmightbedrawn that thisorientation towardsagencieshasledtoa‘silofication’ofthehealthsectorwherethedifferentsilosarecompetingforgovernmentresources.
Examples where focus has been lost during the implementation of the present 5Y Strategic Planincludethefollowing:regenerativehealthandnutrition;noncommunicablediseases; intersectoralcollaboration; roll-out of CHPS; use of information for decision-making; and promotion of a localhealthindustry.
IsthefuturepictureoftheGhanahealthsectorahealthcentrewithanexpensivesatellitedishandup-to-date IT environment but no water? Why do we invest in workable high tech solutions atfacilitylevelandlimit itsusetohealthinsurancedatatransferonly?Thesameequipment,withoutadditional investments (except for state of the art anti-virus software), could be used to transferDHIMS data, get regular feedback, introduce telemedicine, facilitate training and continuouseducationandasanincentiveforstaffstayinginisolatedareas(useoftheinternet).
Keyrecommendation
Limitcompartmentalizationofresourcesleadingtofurtherfragmentation:
• Ensuresufficientandtimelyfundingacrossalllevelsandallfinancingmodalitiesincludingforpublichealth/preventiveactivities;andtrackexpendituresforpreventionandpublichealth
• Ensuresufficientflexiblefundssupportingcomprehensivedistricthealthplanning
• StrengthenthepolicydialoguebetweenMoH,DPsandMoFEP:a)toensuresufficientGOGfundingforpublichealth/prevention;b)toensuretimelyreleaseofGOGandSBSfunding;andc)toensurepartialflexiblefunding
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 13
3.2 Asectorfacingincreaseddemandbutconstrainedbyimportantinefficienciesandweaknesses
The IRT did not perform a complete health sector review and only indicates some of the majorinefficienciesthatdirectlyaffectservicedeliveryandneedtobeurgentlyaddressed.
Theseinclude:a)thedelaysinfundingandreimbursements;b)thehighpricesformedicines;c)thelearningbydoingprocessofthenationalhealthinsurance;d)thehumanresourcesforhealth;e)theuseofinformationfordecision-making;f)capitalinvestments;andg)publicfinancemanagement.
3.2.1 Increasingcoverageofhealthinsuranceleadstoincreaseddemandforservices
The introductionoftheNHIShas ledtoasignificant increase inhealthcareutilization. Outpatientutilization increased from 0.52 visits per capita in 2006 to 0.81 in 2009, an increase of 56%16 .Inpatientutilization increasedbyXX%overthesameperiod.TheIRT isnotawareofananalysisoftheprofileofusersandofreasonsforincreasedattendanceandcannotconfirmwhetherincreasedutilizationisbasedonrealneedsandthereforewouldleadtobetterhealth17.
Obviouslysuchan important increaseofutilizationrequiresthehealthsystemtoreact intermsofstaffing, provision of medicines, logistics, etc. It is not clear from the review whether MoH andservice providers had anticipated this change and planned accordingly. The budgets for health,althoughincreasedsubstantially(mainlythroughtheNHIA),donotsuggestasubstantialincreaseofhealth staff, nor for item 3 as discussed previously, nor for capital investments (staff housing,equipment)18.Also,plannedNHIFtransferstoMoH(foritems3&4)havebeenlateandwerelargelybelowexpectationsin2009(seeannex8).Itisthereforeunclearhowthehealthsystemcopeswiththeincreaseddemandforservicesandwiththeincreasedworkloadwhichhasbeenmentionedasaproblematfacilitylevelduringthefieldvisits.
16Asacomparison,whenuserfeeswereabolishedinUganda,OPattendanceincreasedby70%andremainedatthatlevel.Increasedutilisationwassustainedbyasubstantialincreaseinstaffandbudgetsformedicines.17 Increaseddemandforservices isprobablyamixofclient induceddemand,provider induceddemandandreal needs. Further analysis is needed to identify the profile of increased utilisation (who, forwhat type ofservice,essentialversusnon-essential,demand,supplyorDRGdriven,etc.).18 Some categories of staff have increased substantially over the past years such as the CommunityHealthNursesandequipmentbought in2009wasmainly forEOC.Bothare importantbutwouldnotdealwithallaspectsofincreaseddemandforservices.
Keyrecommendation
• The NHIA and MoH / GHS / CHAG to further analyse the profile of the increasedutilizationandworkloadinorderfortheMoH,theNHIAandserviceproviderstoplanandactaccordingly.
• Consequently, ensure sufficient system inputs to coop with increased demand forservices
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 14
3.2.2 Delaysinreleaseoffundingandinreimbursementsconstraineffectiveimplementationandservicedelivery
Theyear2009hasbeenextremelyweakintermsofitem3disbursements.BytheendofJune2009,only 12% of GoG item 3 had been released. The disbursements to the regions and districtsconsequentlywereevenfurtherdelayed.Someofthedistrictsvisitedreportedtheirfirstreceiptoftheyearinthethirdquarter.Unlikeforitem1whereMoFEPusestemporarilyloanswithBoGtopaypersonalemoluments, item3isonlyreleasedwhenthebalanceofaccountispositive.Thissystemseemstobeacceptedasafactoflife:MoHdoesnotactivelynegotiateforfasterdisbursements.
By June 2009 only 43% of SBS item 3 funding was released (only the SBS provided by theNetherlandswasreleased in the firstquarter;DanidaSBS in July;andDFIDSBS inDecember).TheMoHhas to filea separateapplication form to theMoFEP toaccess theSBS.Thisprocess takesalong time. At the beginning of February the MoH applied for the Netherlands SBS which wastransferredtothebankaccounthalfMayi.e.threemonthslater.
Before,whenpartof thehealth fund,DPresourcestendedtocome intime.AccordingtoDHMTs,programmefundsarrived in2009withadelayof3to4months.NoproblemswerementionedbyDHMTsregardingitem2fundingthroughtheDistrictAssemblies.ButallDHMTsandRHMTsvisitedcomplain about delays in fund release from central level and low levels of resources availablethroughitem3,affectingimplementationofplannedactivities.
By December 2009 MoH received only 20% of expected transfers from NHIF, mainly because ofdelaysof inflows inNHIF.Delays in service claimsbeing reimbursedbyDMHIS remains aproblemthroughout most schemes (but some seem to do much better than others). According to someinformants, this raises acute problems of bankruptcy of certain providers and lack of trust bysuppliers.
KeyrecommendationSee3.1.2
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 15
3.2.3 TheaveragepriceofmedicinesinGhanaisonaveragethreetimesthemedianinternationalreferenceprice
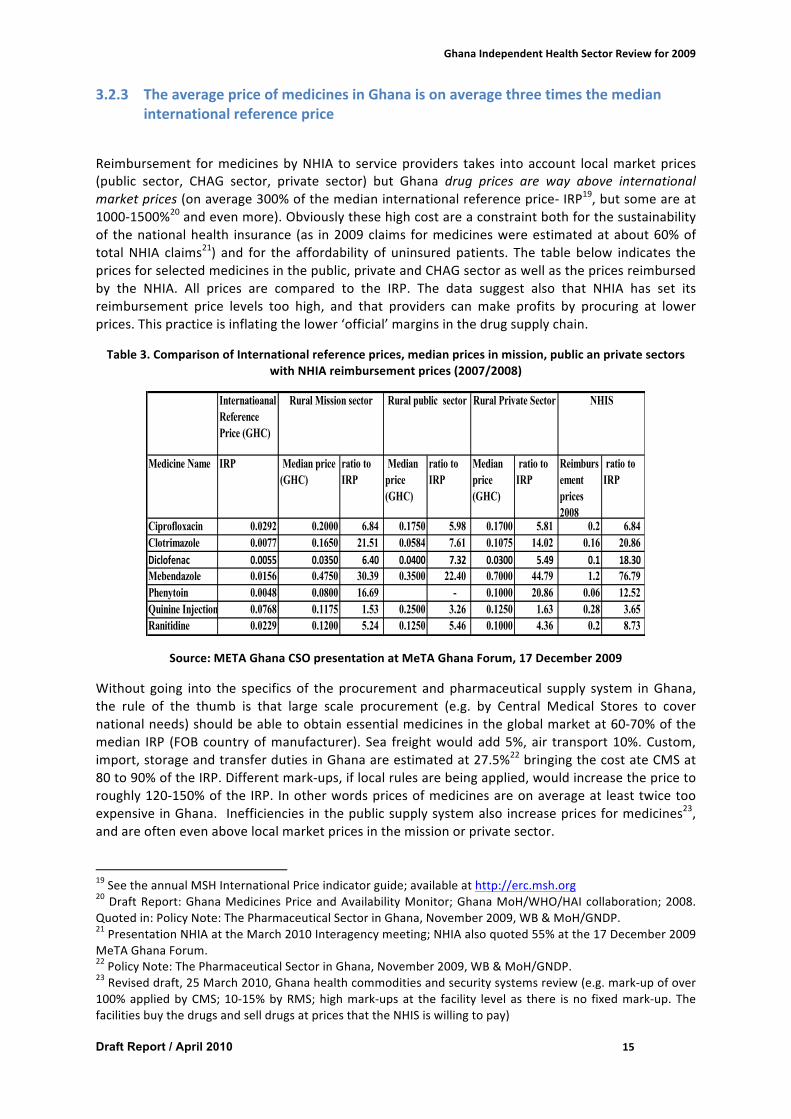
Reimbursement formedicinesbyNHIA to serviceproviders takes intoaccount localmarketprices(public sector, CHAG sector, private sector) but Ghana drug prices are way above internationalmarketprices(onaverage300%ofthemedianinternationalreferenceprice-IRP19,butsomeareat1000-1500%20andevenmore).Obviouslythesehighcostareaconstraintbothforthesustainabilityof thenationalhealth insurance (as in2009claims formedicineswereestimatedatabout60%oftotalNHIA claims21) and for the affordability of uninsuredpatients. The table below indicates thepricesforselectedmedicinesinthepublic,privateandCHAGsectoraswellasthepricesreimbursedby the NHIA. All prices are compared to the IRP. The data suggest also that NHIA has set itsreimbursement price levels too high, and that providers can make profits by procuring at lowerprices.Thispracticeisinflatingthelower‘official’marginsinthedrugsupplychain.
Table3.ComparisonofInternationalreferenceprices,medianpricesinmission,publicanprivatesectorswithNHIAreimbursementprices(2007/2008)
Internatioanal Reference Price (GHC)
Medicine Name IRP Median price (GHC)
ratio to IRP
Median price (GHC)
ratio to IRP
Median price (GHC)
ratio to IRP
Reimbursement prices 2008
ratio to IRP
Ciprofloxacin 0.0292 0.2000 6.84 0.1750 5.98 0.1700 5.81 0.2 6.84 Clotrimazole 0.0077 0.1650 21.51 0.0584 7.61 0.1075 14.02 0.16 20.86 Diclofenac 0.0055 0.0350 6.40 0.0400 7.32 0.0300 5.49 0.1 18.30Mebendazole 0.0156 0.4750 30.39 0.3500 22.40 0.7000 44.79 1.2 76.79 Phenytoin 0.0048 0.0800 16.69 - 0.1000 20.86 0.06 12.52 Quinine Injection 0.0768 0.1175 1.53 0.2500 3.26 0.1250 1.63 0.28 3.65 Ranitidine 0.0229 0.1200 5.24 0.1250 5.46 0.1000 4.36 0.2 8.73
Rural Mission sector Rural public sector Rural Private Sector NHIS
Source:METAGhanaCSOpresentationatMeTAGhanaForum,17December2009
Without going into the specifics of theprocurement andpharmaceutical supply system inGhana,the rule of the thumb is that large scale procurement (e.g. by Central Medical Stores to covernationalneeds)shouldbeabletoobtainessentialmedicinesintheglobalmarketat60-70%ofthemedian IRP (FOBcountryofmanufacturer). Sea freightwouldadd5%,air transport10%.Custom,import,storageandtransferdutiesinGhanaareestimatedat27.5%22bringingthecostateCMSat80to90%oftheIRP.Differentmark-ups,iflocalrulesarebeingapplied,wouldincreasethepricetoroughly120-150%ofthe IRP. Inotherwordspricesofmedicinesareonaverageat leasttwicetooexpensive inGhana. Inefficiencies inthepublicsupplysystemalso increasepricesformedicines23,andareoftenevenabovelocalmarketpricesinthemissionorprivatesector.
19SeetheannualMSHInternationalPriceindicatorguide;availableathttp://erc.msh.org20DraftReport:GhanaMedicinesPriceandAvailabilityMonitor;GhanaMoH/WHO/HAIcollaboration;2008.Quotedin:PolicyNote:ThePharmaceuticalSectorinGhana,November2009,WB&MoH/GNDP.21PresentationNHIAattheMarch2010Interagencymeeting;NHIAalsoquoted55%atthe17December2009MeTAGhanaForum.22PolicyNote:ThePharmaceuticalSectorinGhana,November2009,WB&MoH/GNDP.23Reviseddraft,25March2010,Ghanahealthcommoditiesandsecuritysystemsreview(e.g.mark-upofover100%appliedbyCMS;10-15%byRMS;highmark-upsat the facility levelas there isno fixedmark-up.ThefacilitiesbuythedrugsandselldrugsatpricesthattheNHISiswillingtopay)

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 16
3.2.4 TheNHIAmanagesalargepartofthehealthsectorresourcesbutisconstrainedbyanumberofinefficienciesorweaknesses24
TheNHIAisstillayoungorganisation(4yearsyoung)andislearningbydoing.Thisisincontrastwithsimilar processes in some other countries where an intense period of preparatory studies (e.g.several actuarial studies; testing of different packages; reorganisation of service provision; etc.),developing the regulatory framework as well as continuous debate in civil society have carefullyprepared the progressive introduction of the national health insurance. Ghana has opted for aquicker,moredynamicbutalsomoreriskyprocessofintroducinganeworganisationandfinancingmechanismwhich isyet tobeadaptedalong the road,while learning fromexperience25. It shouldalsobenotedthatGhanahasbeensuccessfulinrapidlycoveringmorethanhalfofthepopulation.Inthatsense,ithasoutpacedspeedofimplementationandcoverageinsomeothercountriesandtoacertainextentisatpresentthevictimofitsownsuccess.
It is thereforeunderstandable that thepresentsystem isperformingatasub-optimal level,butallweaknessesmentionedbelowhave already been identified in different studies, are known to theNHIA and are either being addressed at the time of writing this report, or will most likely beaddressedbythenewbillorarethesubjectoffurtherstudyorpilotprojects.GiventhattheIRThadnoaccesstothelatestversionofthenewdraftbillanddidnotreceiveanyup-top-datedatafromtheNHIA(withtheexceptionofsomeinformationreceivedduringtheinterview),thissectionofthereportisbasedonpreviousstudies,informationfromsomeinformantsandfieldvisits.Someoftheinformationmaythereforenolongerapply.
It is not the purpose of the independent review to do an in-depth study of the national healthinsurance system in Ghana, nor to cover all issues. Many studies have been done and thatinformationaswellasdifferentopinionsarereadilyavailable26.However,giventhe importanceofthe new financing mechanism on the performance of the health sector, on the accessibility to
24Seeannex8forsomemoreanalysisonfinancialaspectsofthehealthinsurancescheme.25 Ghana is not the first country choosing for this approach.Mongolia hasmade the same decision in the1990’s.Rwandahasalsooptedforthe‘fasttrack’.26Forexample,InvestinginHealthinGhana:AReviewofHealthFinancingandtheNationalHealthInsuranceScheme,draft,May2009providesagoodoverviewofthesysteminplace. Ithasbeenused,amongstothersources,forthemainobservationsinthissectionofthereport.
Keyrecommendation
• MoHtoassesstheanalysisandrecommendationsoftherecenthealthcommodityandsecuritysystemsreviewandtodecideonappropriateactiontoaddresstheinefficienciesinthepharmaceuticalsupplysystem
• MoHtoengagewithallstakeholders(private,public,notforprofitandcivilsociety)inamultistakeholderforum(suchastheMedicinesTransparencyAlliance(META)Ghana)toaddressthehightaxes,dutiesandthetoohighpricesformedicinesinGhana;andtakeactiontoaddressthoseissues.

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 17
essentialservices(especiallyforthatpartofthepopulationthattraditionallyhaslimitedaccesssuchas the informal sector and the poor) and the (important and still increasing) size of the resourceenvelope, there isanethical responsibility for theGOG,theNHIAandthecivil society inGhanatoensure that inefficiencies and possible negative consequences are being addressed as soon aspossible.Therefore,theIRTsummarisessomeofthepresentweaknessesofthesystemandprovidessomeoptionsbasedonexperienceselsewhere.
ThefactthattheNHIAhasnodirectauthorityontheDMHISandthatDMHISarenotco-responsible/accountable for the scheme’s financial performance is a structural issue that needs to beaddressed27,28.TheIRTunderstandsthatthenewdraftbillwouldaddressthisorganisationalissue.
Ghana has opted for a broad package of basic clinical / curative services (but excluding someimportantitemssuchasFP,bloodproducts,referralcostsandingeneralprevention),thatissaidtobeexpensive29.Othercountriesoptforamorelimitedbasicpackageandacomplementarypackage.Asindicatedbefore,somecountriesalsoaddselectedindividualpreventiveactivities.
At present, the NHIA pays the same single flat fee for all categories of exempted persons,independentfromexpectedconsumptionprofiles.Theuniqueflat feeprovidesno incentivetotheDMHIStoregistercertainmoreexpensivecategoriessuchasthepoorortheelderly.TheIRTnotesthat the NHIA plans to adjust the flat fee levels, oncemore accurate actuarial data will becomeavailable.
The present system has few incentives to guide provider behaviour (apart from not reimbursingunjustified claims and ad hoc clinical audits). This has lead to numerous examples of change ofprovider behaviour (e.g. claiming more expensive DRGs and polypharmacy30: on averageprescriptionscontainnow6drugsperreceiptascomparedto1.8beforeNHIS; inmonetaryterms,claimsformedicinestotalled60%ofallclaimsin200931)whichunnecessarilyincreasescosts.Thisisawell-knowneffect of health insurance and service-based reimbursement systems. TheNHIAhastheintentiontofurtherdevelopproviderassessmentandcontroltools;andcouldlearnfromothercountryexperienceshowtoaddressproviderbehaviour.
TheG-DRGsystem seemstobecomplex fornon-hospitalbasedprovidersandoutpatientservices,but generally hospital service providers (especially CHAG) consider the hospital fee levels underNHIAmoreappropriate thanprevioushospital fees ifpaid in time.Many (public,CHAG)providersconfirmed that training of prescribers was not appropriate / sufficient. On the other hand, NHIApricesforservicesdeliveredatprimarycarelevel/OPareperceivedbypublicandprivateprovidersasbelowrealcosts,providingincentivestoproviderstofavouruninsured,payingpatients(athigherprices). The IRT notes that the NHIA is considering alternative provider payment systems for OPservices such as capitation payment. Egypt has introduced the concept of registration with apreferred provider and capitation payment under the health insurance. Ghana could learn fromthese(positiveandnegative)experiences.27TheNHIFdoesnot levyfeesfromtheDMHISandtheNHIAdoesnothavesufficientoversighttoinfluencethemanagementofDMHIS.TheDMHISareeachmanagedbytheirownboards.ThereforethedesignoftheNHIScreatesaweakincentiveenvironmentforDMHIStoavoiddeficit.28ItisbeingproposedthatDMHISwouldbecomepartoftheNHIAorganisationasdecentralisedoffices.CriticsquestionwhetherornottheNHIScouldpreservethespiritofcommunityinvolvementthroughitsnewset-up.Thisisanimportantissuethatneedtobeaddressedbythenewbill.29 The IRT is not familiar with any actuarial study that has carefully assessed the cost of the package, theconsumptionpatternofclientgroupsandtheanticipatedchangeofbehaviourunderaninsuranceschemeofprovidersandclients.30 Polypharmacy and rational use of drugs should be monitored and controlled by NHIA and GHS. GHSsupervision systems are weak. Reportedly, a new performance management system is being worked on(meetingwithallMedicalSuperintendentson8-9April).NHIAandGHShavetoagreeontargets.31PresentationbyNHIAattheInter-AgencyMeeting,March2010.

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 18
ClaimmanagementbyDMHISresultsinlongdelaysofreimbursement32(causingcashproblemsforproviders;suppliersmistrustingproviders;depletingdrugstocksatfacilitylevel33)andsometimesinincorrect vetting (refusing to reimburse claims). The field visits toNorthernandVoltaRegionsdidnot confirm improvements in claim reimbursement in 2009 (CHAG, public facilities) but someimprovement was noted in one scheme in Greater Accra Region (but the same schemewas stillconfrontedwithanimportantbacklogofclaims)34.
Premiums,thatvarysubstantiallybetweenschemes(e.g.onaverageGHc10inoneschemeandGhc24inanotherschemevisited)aresaidtokeepsomeusersaway(mainlypartoftheinformalsectorand thepoor)andvariablepremiumsmaycreateproblemsofaccessibility toprovidersoutsideofthesaidscheme.Theonetimepremiummayexacerbateaccessibilitytohealthinsuranceunlessthepriceandexemptionisinlinewithcapacityandwillingnesstopay.Itshouldbenotedthat,becauseof large exemption groups and part of the informal sector and poor staying away from healthinsurance,thecontributionofpremiumstotheoverallhealthinsuranceenvelopeisatpresentlessthan10%.TheIRTisnotawareofanyeconomicmodellingusedbyNHIAtoestimatefuturechangesin membership and contributions. Morocco, with the support of theWB, has developed severalmacro-economicmodelling tools to assess (amongst others) those aspects,which could be useful/adaptedforGhana.
There seem to be ongoing difficulties with managing themembership database, defining activeversus non active card holders. Other problems that have been mentioned concern differentsoftwareprogrammesusedatfacilitylevel;problemswiththeinterfaceandwithuseoftemporarycards.
Asingleorganisationorprocedureforaccreditingallpublicandprivateproviderswouldallowforastandardised approach to quality norm setting, application and monitoring in the sector. ThisrequirestheMoH,GHS,CHAGandthePrivateHospitalsandMaternityHomesBoardtoagreewithNHIAonasingleresponsibleorganisationforaccreditationwithinor(preferably)outsidetheNHIA.
Accessibilityforthepoorisanissueinallnationalhealthinsuranceschemes.AnumberofinitiativesareplannedtoimprovethetargetingofexemptionssuchastheLEAPprogramme,etc.Reportedlythe NHIA has started discussions with the LEAP to develop a common approach / use the samedefinitionandapproach to identify thepoor.But critics cite theadditional costsof increasing thetargetingoftheexemptespeciallyvis-a-visthegoalofmaintainingthefinancialsustainabilityoftheNHIS.Morocco is an interestingexampleasMinistryof LocalGovernmentandMoHarepresentlyimplementingapilottestofmeanstestingandidentifyingthe(‘absolute’and‘relative’poor)inthecontextofthenationalhealthinsurance.Ghanacouldlearnfromtheseexperiences.
32 Delays are partly caused by late submission of providers (up to 1month), delays in vetting of claims byDMHIS(upto3months)anddelaysinpayments(upto2months).Totalperiodcanbeupto5months.IftheDMHIShasnotenoughcashtopay,arequestforreinsuranceissubmittedtoNHIA,whichproceduretakesonaverageanother2months.Today,allDMHISarebeingreinsuredandgetmonthlysubsidiesfromNHIA.33AccordingtoGHS, there is todayamedicinescrisisandGHShasrequestedGoGtocover40%ofessentialmedicines needs to complement medicines availability at facility level. Inefficiency of CMS and lack ofaccountability contributes to the drug crisis. This is a vicious circle: because of unavailability, buying drugsmoreexpensivelyonprivatemarketdepletesbudgetsfordrugsevenmore.34AnecdotalevidencethatprivateprovidersarereimbursedquickerbecauseofdealwithDMHIS

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 19
As indicated, the NHIA is a learning organisation and should be supported in addressing thestructural, conceptual and operational issues in a structured and systematicway. TheNHIA couldprobably benefit from an institutional support or twinning with another social health insurancescheme (as opposed to a private health insurance scheme; and complementary to the technicalsupportalreadyprovidedbyseveralagencies35).
3.2.5 Humanresourcesforbetterhealth36 TheMoHhas implementedseveral interventions tostrengthentheeffectivenessandperformanceof the health workforce in an effort to improve the quality of health care and achieving greaterequityofaccesstohealthservices.ThePOW2007-2011outlinedpriorityinterventionsincludingtoenhance production and utilization, productivity, strengthen human resources management andforgeclosertieswithlocalcommunitiesandvariousotherpartners.
The health workforce and system has recorded significant improvements in education andproduction of health workers especially middle level health cadres, taken steps to improvedeploymentandutilizationandenhancedsalariesandincentivestomotivateworkerswithrecordeddeclineinstaffattrition.
However,someimportantissuesremaintobeaddressed,including:
Existingdisparitiesinhealthworkforcedistribution.Whilethereisacknowledgementoftheexistingdisparity intheequitabledistributionofskilledhealthworkersalongurban–ruralandgeographicalaxis,theprecisepatternisnotclearduetotheabsenceofreliableinformationontheavailabilityofhealthworkers. The sector still lacks a reliableHRH informationmanagement systemandexistingdatabasesarenotregularlyupdated.Thepayrolldataalsohasmanifesteddiscrepancies.Althoughtheholisticassessmenthasindicatedthatequityofdistributionofessentialcadressuchasnursesis35TheNHIAisbeingsupportedbytheWB,PharmAccess,etc.TheIRTisnotawarewhethertheNHIAisbeingsupportedbyanagencythathashealthyinsuranceasitscorebusiness.36Seeannex5foramorein-depthanalysisofhumanresourcesforhealth.
Keyrecommendation
NHIAtobecomeanefficienthealthinsurerinsupportofsectorpriorities:
• AsseswhetherthenewHIbill(RegulatoryCommission–streamliningorganisation–reinforcingcommunicationandcoordinationchannels–clarifyingaccountability)effectivelyaddressestheaboveissues.Pass(andstilladaptifnecessary)thenewbill.
• MoHandagenciestosupportNHIAasalearningorganisationaddressingstructuralandoperationalinefficiencies(NHIAtoconsidertwinningwithanothersocialhealthinsurancescheme).
• Basedonthe(future)pilotexperience,considerintroducingperformance/resultsbasedfinancingandpublichealthtargetingunderNHI.
• NHIAtocollaboratewithMoHandserviceproviderswithaviewtoworktogetherinachievingsectorpriorities
• NHIAtofostertransparencyasabasisformutualcooperationandtrust

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 20
substantially improving (most likelybecauseofeffectivelyaddressing this issuebyMoHandGHS),thedatacaptured in the tablebelow indicatehowdifficult it is toeffectivelyattractandmaintaindoctorsinsomeregions,i.e.theevidenceofrefusalofhealthworkerstoacceptpostingtotheUpperEastRegion.
TrendsinDoctorsPostings,UpperEastRegion:(2001– 2009)
Year #Posted #AssumedDuty
%
2001-2006 16 1 6.3
2007 9 1 11
2008 8 1 12.5
2009 10 1 10
Total 43 4 9.3
HighAttrition of Healthworkers:While the country is grapplingwith the challenge of producingrequiredhealthworkers,thereisacontradictionastheexistingcompulsoryretirementpolicy(of60years) contributes to unacceptable high loss of skilled and experienced health workers. Fromavailableinformation,itwouldappearthattheoverallattritionofprofessionalhealthworkersisonthedeclinedue to the severalpositive interventionsundertakenbygovernmentbetween2001 to2007, including the recent upsurge in production interventions. The recent public payroll analysisalsoconfirmsageneraldeclineinattritionparticularlyafter2006.However,arecentMoHanalysisindicatesthatretirementfromthesectorasagainstotherreasons,standsasthemostconsequentialreasonforattritionbetween2004and2008.Thepictureandtrendisworrisomegiventhatmajorityof thehealthworkersonthepublicpayrollareyoungandrelatively inexperienced (25-35yearsofage), and it is estimated that some 14,439 health workers will reach the mandatory age ofretirementinthenexttenyears.
While related curriculum development is ongoing within the sector, the existing regulatoryframeworkformosthealthcadresremainsanissueofgrowingconcern.Forexamplethereexistsno institutionalised framework for the regulationandaccreditationofmiddle levelhealthworkerswhoconstitutethebulkofthehealthworkforce37.
Under the present administrative arrangement,keyHRHmanagement functions are held by theheadquarters. For example, there is concentration of salary management powers at the centre,coupledwithpowerstoundertakepostinganddeployment,supervisionofstaff,approvaloftrainingand continuous medical education and training. This situation leaves regional and district healthmanagers with little or no influence on these important personnel functions. The existing staffmanagement relationship frequently leads to situationswheremany healthworkers receive theirsalarieswhilenotatpost. Insuchsituation,regionanddistrictauthoritieshave limiteddisciplinaryremediestosanctionoffendingstaff.
37FeedbackfromKeyInformantinterviews.March2010.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 21
Coordinationoftrainingoverpre-serviceeducation inGhana isstill largelycontrolledbytheMoHheadquarters.WhereastheMoHhasindicateditswillingnesstodevolveresponsibilitiestoregionalhealth authorities, officials at the headquarters still exert control over key functions includingknowledgeandstandardsacrossthesectorintermsthepolicydirections,governance,management,curriculumcontents,theteachingenvironment(teachingmaterial,infrastructure,labrequirements,and curriculum contents), funding and expenditure trends. This situation leaves little room forcollaborationbetweentheheadquartersandregionsincrucialareasincludingprovisionofsupportfor shortages in the teaching staff, essential teaching supplies using local resources text books,internetaccess,classroomandhouseaccommodation.
3.2.6 Managinganduseofinformationfordecision-making38
In thedomainof informationaclearpolicyguidelineandstrategyhavebeendeveloped.Over theyears, efforts have been made to synthesize various fragmented information systems andharmonizing datamanagement tools for serving the sectorwith timely information. Nonetheless,theperformanceofinformationsystemsinthesectorhasremainedfarfromsatisfactory.Withthecurrentlevelofpriority,theinformationstrategycannotbeimplementedandwithoutthis,desiredimprovementscannotbeachieved.
Thenationwide implementationoftheDistrictHealth InformationManagementSoftware (DHIMS)is a remarkable start for establishing a single common information system in the country. It hasprovidedaplatform for inputtinganydata that thehealth sector collects. Thoughusers and theirsupervisors have noted numerous problems in DHIMS, those are minor in comparison to theadvantagesthatthesoftwarehasprovidedforthemanagementofthecomplexhealthinformationsystems.Nonetheless,inordertoavoidanyfrustrationonthepartofitsusers,thevariousproblemsthathavealreadybeennotedbeforeshouldbefixedurgently.
The existing systems have adequate tools and guidelines to collect data that are required formanagingindividualcases,managingthehealthunit,andforreportingtohigherlevelstocalculatetheindicators.Whileadmiringthoseaccomplishments,itshouldbenotedthattheformsintroducedforroutinereportingofdiseaseandservicestatisticscontainmorethanrealisticallyrequireddetails.
38Seeannex6foramorein-depthanalysisofinformationmanagement.
Keyrecommendation
• Urgentlyundertakeupwardreviewofthemandatoryretirementagepolicyfrom60to65years, in viewof thepotential lossofhighly skilledandexperiencedhealthworkerswithinthenexttenyears.
• Explore opportunities to devolve HR management functions-(including training,recruitment,deployment,incentives,disciplineandpayrollmanagement).
• Decentralizemanagementandgovernanceofhealthtrainingschools.• Establish a system for effective regulation and accreditation of middle level health
workers: promote investment to address weakness in the curriculum contents, theaccreditationprocess,quality improvements in student/teacher imbalance,provisionofessential learning materials in essential infrastructure, laboratory equipment, andfunctionalutilitiesincludingelectricity,waterprovisionandsystemforHRdatacollectionandanalysis)
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 22
Itdoesnotonlyaddaburdentohealthworkerswhoseprimarydutyistodeliveraqualityservicetothe people, but it also affects the quality of data reported. Monthly reports can be drasticallyshortened while leaving the collection of other details to a special survey such as annual recordreviews.
Dataanalysisanddissemination iswoefullyweakacrossall levels.Mostdataarerarelyanalysedandusedatthepointofcollection.Thedistrictsthatreceivetheplethoraofdataonmonthlyreportsmostly use their time in entering the data into DHIMS and forwarding to the regions. Routineanalysisanddisseminationisnotapriority.ThesameappliestotheregionsandMoHheadquarters.
Contrarytopoorroutineanalysisanddissemination,theproductionofannualreportshasevolvedas a standardpracticeor culture at all administrative levels. Currently, the content and formatofannualreportsarehowevernotuniform. Itwouldbe ideal foreach leveltouseastandardannualreporttemplateasaminimumrequirement.
Visual display on key indicators by means of wall charts and graphs is a powerful tool to drawattentiononkeyissues.Theycanbeusedtokeepone-selfremindedonthepertinentissueaswellastoeducateorinformothers.ExceptaverydetailedcrowdedchartonGuineaWormsurveillancedata,barelyanychartwasfounddisplayedatanyinstitutionthereviewteamvisited.
Theinstitutionalisationofannualreviewsatalllevelsisanotherremarkabledevelopment.Inorderto prevent this process frombecoming only a ritual, a presentation in the reviewmust provide aclearconnectionbetweenwhatwasplannedfortheyear,whathasbeenachieved,andwhatcouldnot be achieved and why. In the recently held inter-agency review meeting, except for a fewpresentations,thislinkwasmissing.
Theholisticassessment introducedintheannualreviewprovidesabird’seyeviewonthesector’sperformance.Moresynergycouldbeachievedbyaddingaleaguetableconcepttoranktheannualperformance of health facilities, districts, regions, and various national programs. It wouldencourageandincitethestakeholdersforbetterperformance.
Keyrecommendations
• Provideaseparatebudgetlineforthehealthinformationsystemandallocateadequateresources(foroperatingandmaintainingthesystem;fortrainingandappropriatelevelsofHR;andforregularreplacement/updatingoftheITenvironment);
• FixtheproblemsinDHIMSandaddthemenudrivenmodulestogeneratedashboardreportandprogramspecificcomprehensivereports.CreateandlinkpivottablestoDHIMS(asinHISPdatabase)andmakethemavailabletothestakeholdersthroughtheMoHwebsite;
• Equiptheinformationunitsatdistrict,region,agencylevelsandatMoHwithfunctionalcomputers,A3printers,antivirussoftware,internetconnection,andanannualbudgettomaintainthesystemandgeneratethedashboard,quarterlyandperiodicreports;
• StrengthenthenecessaryskillsofallHIOstoanalyzedata,generatedashboard,feedback,andcomprehensiveperformancereports,andfurthermosttodisseminatetheinformationtodecisionmakersandfacilitatetheuse.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 23
3.2.7 CapitalinvestmentsinsupportofreachingtheMDGs39
Reportingontotalexpenditurefor2009isstill incompleteatthistime.HoweverthedataavailableforMoHcivilworksandGHStransport,equipmentandICTsuggeststotalexpenditureofGH¢44.94million,representinga28%executionrateofthetotalidentifiedannualbudget.
The analysis of 2009 actual capital expenditure by level (civil works only) shows a significantweighting in favour of the primary level,with 74% of expenditure at the District and Sub-Districtlevel, and a further 8% being spent on infrastructure at the Training Institutions, in linewith theoverallsectorpolicydirection.
IssuesArising
Capitalexpendituredataontransport,equipmentandICTbytheagenciesisnotreadilyavailable,thereisnoroutinereportingonprogressandexpenditure,andnosingleunitordeskisresponsiblefor collectingdata,monitoringand reportingonprogressagainst theCapital InvestmentPlanasawhole.
Forecast inflows fromNHIFdid notmaterialise orwere not captured in reporting, and there hasbeen an increasing reliance (65% of expenditure) on the use of Financial Credits to develop newinfrastructureonturnkeyprojectbasis.
Implementation of the planningmethodology and framework has been restricted, and hence thefacilityrationalisationagendahasstalled.
Capital investmenthasmadeonly a limited contribution towards achieving theMDGs in 2009 -only 300 out of an estimated national requirement of 6,400 CHPS Zones are completed with acompoundfortheCHOs.
3.2.8 Publicfinancemanagement40
The health sector faces anumber of challengeswith regard to public financialmanagement. Thecredibilityofthehealthsectorbudget,thepredictabilityandtimelinessofdisbursementstodifferentlevelsinthesystem,theincompleteinformationondistrict,regionalandNHISexpendituresandtheaccuracyofthefinancialreportingareallfactorscontributingtosub-optimalresultsinhealthsectordelivery.
39Seeannex7foradetailedanalysisofcapitalinvestmentforhealth.40Seeannex8foramorein-depthreviewofhealthfinancingissues.
KeyRecommendation
MoHtoring-fenceGH¢15millionfromitscapitalbudgetperyearforthenextthreeyears,toprovideabout600completeCHPScompoundsovertheperiod,andleveragethisinvestmenttoobtainmatchingsupportfromMLGRDandtheDistrictAssemblies.
Seeannex7,p66forspecificrecommendations.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 24
ThePFMWorkingGroupdevelopedaframeworkforfurtheractionsonPFMstrengtheningincludingan agreed timeline andbudget. Besides the realisationof the long awaited “Accounting, Treasuryand Financial Reporting Rules and Instructions” (ATF), little progress has been made in 2009.Securing funds for the implementation of the activities did not materialise and Working Groupmembersweregenerallytoooccupiedwiththeirregulartaskstoactivelydrivetheagenda.DuringthehealthSummitinNovember2009,concernswereraisedagainaboutthelackofeffectivefinancialmanagementinthesectorincludingcontinuousdelaystostrengthenthisarea.TheseissuesneedtobeseeninthebroadercontextofthefunctioningofthePFMsysteminGhana.Nonetheless,theMoHshouldbeabletotakeappropriateactionswithinitsowndomain.
3.3 Whatarethechallengesthatdistrictfaceinordertodeliver?
Districthealthplansarenotyetfullycomprehensive, largelyexcludingNGOsandprivateproviders.Planning is in principle done on a needs basis, but in reality without respecting budget ceiling(DHMTsreceivebudgetceilingforGOGfundingbutfinditirrelevantasresourceallocationsarenotin linewithceilings), taking intoaccount lastyear’s levelandsourceofresources (e.g. if resourceswere available for HIRD and from GFATM or a specific donor, DHMTs will take this reality intoaccountwhendevelopingnextyear’splan).WhileNGOsandprivateprovidersareoftennotinvolvedintheplanningstageandinprioritysetting,theyaretoacertainextentinvolvedinservicedelivery (e.g.completingDHIMSdata, implementingPMTCT, allowing CHN to provide CWC/EPI services in private clinics, private providers involved intraining, invited to quarterly meetings, etc.). Involvement however varies substantially betweenregions, districts, urban and rural areas based on the local context andmotivation / leadership /interestofindividuals.CollaborationwithDistrictAssembly (DA)seemstoberegularandcontinuous(e.g.participationofall DHMT members in specific DA committees; participation in Head of Department meetings,budgetmeetings,GeneralAssembly,technicalcommittees)andeffective(DAcontributingresourcestohealth:e.g.foritem2,renovation,transport,equipment,feedinghospitalizedpatientsmeetings,ImmunizationDay,communityeducation,problemsolvingincommunities,etc.).ClosecollaborationwithDAallowsforcivilsocietyrepresentationindiscussions.CommunityrepresentativesalsoinvitedatDHMTquarterlymeetings.
KeyRecommendation
AllPFMrecommendationsarealreadylistedinthePFMstrengtheningplan.IMPLEMENTTHEM
• 57activitieshavebeenidentifiedincludingaresponsibleunit,budgetandtimeline.Prioritisethemandidentifyquickwins.
• InstitutionalmeasuresareneededtoassurethatPFMstrengtheningwillstayontheagendain2010.
• DPscouldplayamoresupportiverolebyprovidingtemporaryassistanceinthisarea.

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 25
Workload on reporting up is time consuming (including many different types of reports such asmonthly DHMIS reports and 3 parallel reports; monthly financial reports; quarterly detailed andcumulativeactivityreportstoDAandRHMT;semi-annualandannualreport;plusunderlyingexcelfiles,PPP,etc.).Feedbackisnotstandardizedandregular.Supervision to public health facilities by DHMTs happens regularly (using locally developedchecklists)andasateam.Feedbackisprovided.Frequencyishoweverlow(e.g.quarterlyinAccra)becauseoflackofreliabletransportandlimitedresources.As indicated earlier, there were a number of developments in 2009 which created financialchallengesforservicedeliveryattheregionalanddistrictlevel:• Utilisationandthereforealsocostsofcurativecarefurtherincreased.• The provision of curative services was heavily challenged by the backlog on NHIS claims
processingwhichhascreatedseriousliquidityshortagesatproviderlevel.• The move of some donors from Health Fund to SBS resulted in extra delays in the chain of
disbursements.Thepredictabilityoffundsforitem3deterioratedfurtherin2009.• TheMoH had the tendency to earmark SBS funds to particular Health programmes, thereby
limitingthe‘flexiblefunds’atregionalanddistrictlevel.• Unforeseenexpenditures, likeanadditionalGHc2million for the Influencepandemic in2009,
were taken out of the item 3 budget, thereby further challenging the objectives of the PoWunder item 3. Unforeseen expenditures like these are expected to be paid from the MoFEPcontingencies budget, but access to and slow releases from the contingencies hamper a fastresponseincaseofurgencysothatitem3isusedinstead.
InprincipleSBScanbeallocatedbytheMoHaccordingtoneeds.Whiletherearecertainlypositiveelements on earmarking at this level it is also important to signal that at district level these highvolumesof ringfencing are felt as a big obstructionwhich alsoundermine themeaningof districthealthplanningandbudgeting.Thelimitedandlatereleasesonitem2and3combinedareplacingtheDHAsfurtherunderpressure.In2009,GFATMandHIRDfundswereimportantsourcesatdistrictlevel to keep the system running. This is also reflected in the sector-wide indicators:most sector-wide service indicators monitored under the holistic assessment are indeed HIRD and GFATMrelated service indicators. Overall they have improved substantially in 2009. Thismay create thewrong impression that there is no issue in termsof resource availability and timeliness at districtlevel.The reality is that theearmarked funding forGFATMandHIRDhave indeedbeen the lifelineand allowed districts in 2009 to implement those specific priorities. Other priorities thatwere notresourced such as non-communicable diseases41, regenerative health and nutrition, CHPS42, etc.remained largelyoff the radarofDHMTs.And lackof resourceshas reportedly cutdownonotheractivitiessuchassupervision,addressingreferralsandemergencyservices,etc.Oneofthedistrictsvisitedstartedapilotwithaninnovativeconceptonthe1stofJanuary2010.ThisDistrictAuthorityassists the district health centreswithNHIS claim processing before submission to theDMHIS. Inturn, theDistrictAuthority receives30%of the reimbursedclaims for services (nodrugs)which isusedtosupportthehealthclinicswiththeimplementationofthepublichealthprogrammes.MainchallengesperceivedbyDHMTsare: limitedand latefunding;noflexiblefunding;ageingandunreliable vehicle fleet; lack ofmidwives, especially young ones; poor having no access to healthinsurance;parallelinformationandreportingsystems;fundingde-linkedfromdiseaseburden,localprioritiesandresultingcosts.
41Seesection3.4forcommentsonnoncommunicablediseases.42SeeAnnex9forcommentsonCHPS.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 26
3.4 Andwhathasbeendeliveredintermsofthemain2009servicerelatedpriorities?
Twomain priorities identified in the POW2009 areMDG4& 5 and non communicable diseases.Whathasbeentheachievementgivenontheonehandtheimportantresourceenvelopeavailableforthesectorandthemanyconstraintsdiscussedbefore?
AddressingMaternalandNewbornHealthtowardsAttainingMDGS4&5
Ghanastillfacesanunacceptablehighmaternalmortalityratiocoupledwiththehighcontributionofneonataldeathsdueto(mainly)infantmortality.Thissituationcallsforintensifiedaction.TheMoHhas initiated several interventions to improve the situation. For, example, at the Partners Healthsummit held in April 2008, the HonMinister of Health declaredmaternalmortality as a nationalemergency requiring accelerated action. His Excellency the President also announced the freematernitycarepackageforpregnantwomen,implementedundertheNationalHealthinsurance.FundshavebeenreleasedthroughtheNationalHealth insuranceschemefor theprovisionof freematernalhealthservices43,44.Therearehowever,asdiscussedbefore,emergingchallengeswithre-imbursementof serviceproviders.There iswidespreadconcernamongserviceproviders includingthe private sector that quality of services and sustainabilitymay be difficult to achieve given theimplicationsarisingfromdelayedpaymentofreimbursement.Furthermore,toaddressthematernalandneonatalhealthsituation,anationalconsultativemeetingwasconvened,andamulti-sectoraltaskforce(theMinisterialTaskForce)wasestablishedlate2007to mobilize additional resources and do advocacy regarding MDG 4 & 5 and more specificallyaddress relevant family planning issues, basic emergency obstetric and neonatal care andcomprehensive abortion care. It presented its Action Plan during the April 2008 summit, with anincreased focus onmaternal health in HIRD (more resources for institutional deliveries, outreachservices and staff training). In addition, the GHS had established a safe motherhood task force45undertheReproductiveandChildHealthdepartmentwithinthefamilyHealthDivision.
43GhanaHealthService:DraftHandingOverNotestotheTransitionalTeam,GHS,January2009.44Seealsoannex8onhealthinsurance.45Atechnicaltaskforce,comprisingofdifferentstakeholderssuchasUNagencies,CHAG,NationalPopulationCouncil,etc.
KeyRecommendation
• Mostrecommendationsforimprovingmeaningfulcomprehensivedistricthealthplanninghavebeencapturedunderprevioussections.
• Inaddition,thereisstillscopeforDHMTstomoreinvolveCHAGfacilities,NGOsandprivatesectorprovidersinplanningandprioritysetting.
• Reinforceintegrated‘horizontal’planning:decentralisationstrategies,engagementofcivilsociety
• Ensureholisticplanningforhealth(thematicandmulti-sector)withensuing(ministry)agencyportfolio’s:OpportunityofSMTDPdevelopment
• ImplementrecommendationsofstudyonpartnershipMoH-CHAG• CHAGandGHStoconsiderdevelopinganMoUbetweenbothagencies

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 27
Thereisevidencethatthegovernmenthascatalysedactionatthedistrictandoperational levelstoacceleratemultisectoral response toMDG5. Forexample, theMinisterial task forceonDecember18th 2008 mobilized all regions and districts to assist with transporting pregnant women duringemergencies.TheMinistryofInformationcommittedwithprovidingcommunitieswithinformationon safeMotherhood, the private sector would continue to render valuable clinical and advocacyservices.Itwasalsoagreedthathumanresourcesissuesparticularlythetrainingofandpostingofmidwivesandothercadrestoassistmaternalandnewborncarewouldbeaggressivelypursued.Although theMinisterial Task Force has not been very active in 2009 (only onemeeting) and thefocusmayhavesomewhatshiftedunderthenewminister,the2008actionplanhasinfluenced2009actionsofGHSatoperational leveland through theSafeMotherhoodTaskForce.Over theperiod2007 to 2009, significant progress has been achieved overall, as is confirmed by the sector-wideserviceindicators(seetablebelowandannex2fortheholisticassessment).Whilesignificant,someindicatorsareonlybackatthe2006level(e.g.institutionaldeliveries).AnditisobservedthatfamilyplanningisyettobeincludedintheNationalHealthInsurancesupportedservicepackage.Giventheproven advantage of family planning services to contribute to addressing maternal mortality westrongly suggest inclusionof family planning in theNHIS package in addition to focused action toaddressunderlyingcausesofearlyneonatalandmaternaldeaths.TheHighImpactRapidDelivery(HIRD)approach isbeenimplementedasacomplimentarystrategytoreducematernalandchildmortality.TheHIRDapproachcombinesthekeyprinciplesofvisionanddatadrivenmethodstoachieveimprovedcoverageofkeycost-effectiveinterventions,whichhavebeenproventohaveahighimpact onmaternal andchildmortality. TheHIRDprocesshasresultedintheorganizationofseveralplanningandreviewmeetingsatdifferentlevelsofthehealthsystem,withdisbursementoffundstosupportactivitiesinconsonancewiththenationalguidelines.From the field visits it has been confirmed that maternal health was on the priority agenda ofdistrictsand regions visited. Severaldistricts could indicateprogress in service indicators achievedand innovativestrategies implemented.Severalchallengeshaveemerged includingHIRDplansstillbeingdevelopedandreportedonseparately;inadequatedataforplanningandtargetsetting;weakinvolvement of hospitals in planning and implementation. There has also been complaint ofweaknessinfunding,poorintegrationofactivitiesandweakinvolvementofdistrictstakeholdersinimplementation andmonitoring. Particularly, under funding of hospitals to improve and scale upmaternal services isperceivedasa challenge toexpediteHIRDactivities includingprocurementofequipmentandsupervisionofservices46.TheEOCmappingisongoingandnearcompletion.Limitedresourcesexplainslowimplementationofthe study. Once completed a RoadMap for implementation will be developed.Most equipmentboughtbyGHSunderitem4in2009concernEOC.Asconfirmedbytheholisticassessment(seesection2.1),theproportionofdeliveriesattendedbyatrainedhealthworker increasedby17%,andhencecontinuedthepositivetrendexperiencedsince2007.TheDHS2008estimatedthepercentagesomewhathigherat58.7%.AdeeperanalysisoftheDHS2008data reveals that therewere large regional variations in the indicator. InGreaterAccraRegion84.3%deliverieswereattendedbyaskilledprovider,whileonly27.2%wereattendedbyaskilled provider in Northern Region. Also the routine health information indicates that NorthernRegion performed relatively poorer than other regions, the region did however achieve majorimprovementofthisindicatorbyalmost40%from2008to2009.
The institutionalMMR continued thepositive trend,andwas reducedby15% from2008 to2009.Almostall regionsachieved improvementof this indicator,but inUpperWestRegion therewasa
46MoHGhana:HIRDProgressReport.February2008.
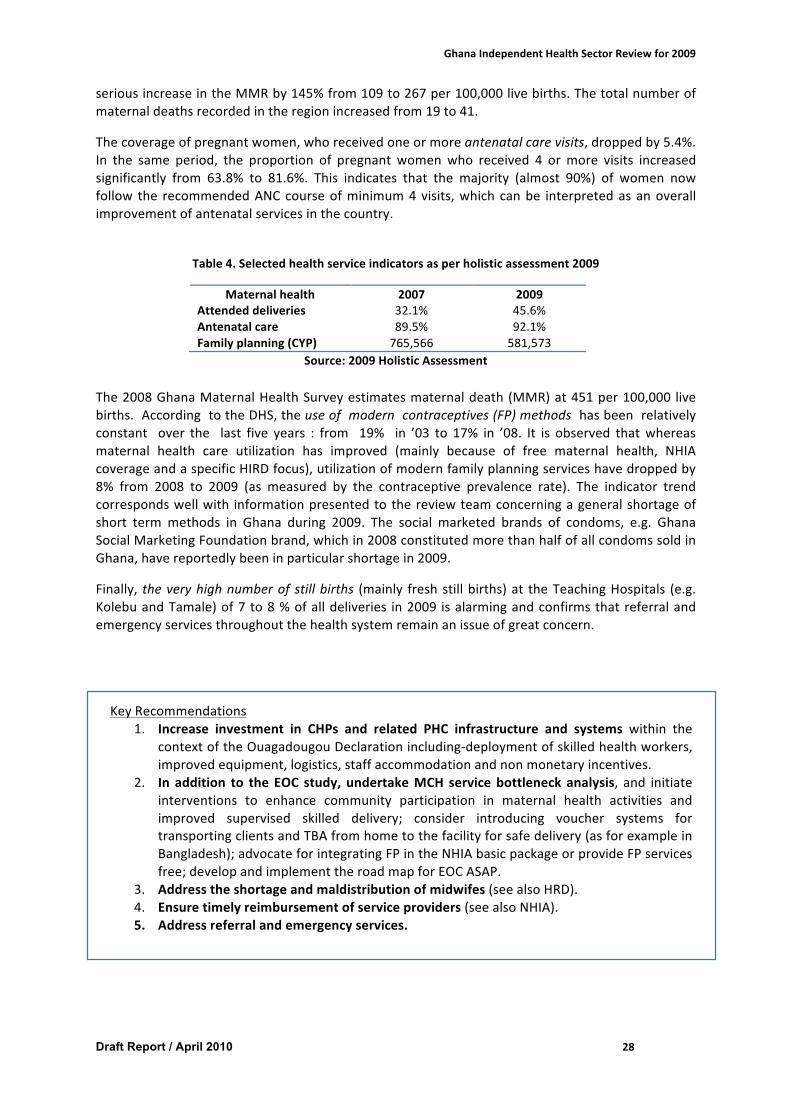
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 28
seriousincreaseintheMMRby145%from109to267per100,000livebirths.Thetotalnumberofmaternaldeathsrecordedintheregionincreasedfrom19to41.
Thecoverageofpregnantwomen,whoreceivedoneormoreantenatalcarevisits,droppedby5.4%.In the same period, the proportion of pregnant womenwho received 4 ormore visits increasedsignificantly from 63.8% to 81.6%. This indicates that the majority (almost 90%) of women nowfollow the recommendedANCcourseofminimum4visits,whichcanbe interpretedasanoverallimprovementofantenatalservicesinthecountry.
Table4.Selectedhealthserviceindicatorsasperholisticassessment2009
Maternalhealth 2007 2009Attendeddeliveries 32.1% 45.6%Antenatalcare 89.5% 92.1%Familyplanning(CYP) 765,566 581,573
Source:2009HolisticAssessmentThe2008GhanaMaternalHealthSurveyestimatesmaternaldeath(MMR)at451per100,000 livebirths.AccordingtotheDHS,theuseofmoderncontraceptives(FP)methodshasbeenrelativelyconstant over the last five years : from 19% in ’03 to 17% in ’08. It is observed thatwhereasmaternal health care utilization has improved (mainly because of free maternal health, NHIAcoverageandaspecificHIRDfocus),utilizationofmodernfamilyplanningserviceshavedroppedby8% from 2008 to 2009 (as measured by the contraceptive prevalence rate). The indicator trendcorrespondswellwith informationpresentedtothereviewteamconcerningageneralshortageofshort termmethods in Ghana during 2009. The social marketed brands of condoms, e.g. GhanaSocialMarketingFoundationbrand,whichin2008constitutedmorethanhalfofallcondomssoldinGhana,havereportedlybeeninparticularshortagein2009.
Finally, theveryhighnumberof stillbirths (mainly freshstillbirths)at theTeachingHospitals (e.g.KolebuandTamale)of7to8%ofalldeliveries in2009 isalarmingandconfirmsthatreferralandemergencyservicesthroughoutthehealthsystemremainanissueofgreatconcern.
KeyRecommendations1. Increase investment in CHPs and related PHC infrastructure and systems within the
contextoftheOuagadougouDeclarationincluding-deploymentofskilledhealthworkers,improvedequipment,logistics,staffaccommodationandnonmonetaryincentives.
2. In addition to theEOC study,undertakeMCH servicebottleneckanalysis, and initiateinterventions to enhance community participation in maternal health activities andimproved supervised skilled delivery; consider introducing voucher systems fortransportingclientsandTBAfromhometothefacilityforsafedelivery(asforexampleinBangladesh);advocateforintegratingFPintheNHIAbasicpackageorprovideFPservicesfree;developandimplementtheroadmapforEOCASAP.
3. Addresstheshortageandmaldistributionofmidwifes(seealsoHRD).4. Ensuretimelyreimbursementofserviceproviders(seealsoNHIA).5. Addressreferralandemergencyservices.
6.

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 29
Addressing awareness towards the reduction of risk factors and improvemanagementofnon-communicablediseases
Noncommunicablediseasesincludeseveralcategoriesofdiseases:a)thetraditionallycalledchronicdiseases such as diabetes, cardiovascular diseases, chronic lung diseases and different forms ofcancer;b)geneticdisorderssuchassicklecellanaemia;c)injurieswithchronicphysicalimpairment;and d) genetic disorders causing impairment such as hearing impairment. Other chronic diseasessuchasmentalhealth,HIV/AIDSandobesityareaddressedbyotherspecificprogrammes.
The POW 2009 mentions two main areas of focus, being: a) creating the necessary awarenesstowards the reductionof the risk factorsofNCDs; andb) addressing service improvements in themanagementofNCDs.
AlthoughmentionedasaspecialfocusinthePOW2009,NCDsdidreceivenomoreemphasisthaninpreviousyears.Thearea isnotconsideredapriority,which is reflectedby the limitedstaff inGHSdealingwithNCDs (2staff,under thediseasecontrolprogramme)and ‘chronic’under funding (nospecificbudgetlinefromGOG;somelimitedfundsfromDPs/MoHandmostlyearmarkedforsicklecell or cancer; in 2009 no additional resources were allocated). District plans follow (promised,anticipated) availability of resources and not the actual disease burden. As a result they tend tofocusprimarilyonspecific,wellresourceddiseasessuchasmalaria,HIV/AIDS,tuberculosisandpolio.
TheGHSChronicDiseasesUnitisfullyawareoftheheavyandincreasingdiseaseburdenduetoNCDs(especially hypertension, diabetes) and cardiovascular diseases being the primary cause of death(40%;morethanmalariaat30%47) inGhana. In2007astudyonriskfactorsforNCDswasdone inAccra. Thedocumenthasnot yetbeendistributed.TheGhanahealth surveys2003covered somedataontobaccoconsumption;theGHS2008onnutritionandalcohol.TheDHSlivingstandards2005(published 2009) included alcohol and tobacco consumption. Ongoing activities include mediaactivities(radiointerviews,trainingofNGOs,prayandtalk,WorldTobaccoDayorganisedbytheHEunit,etc.).
ResourcesforhealtheducationrelatedtoNCDsseemdividedoverseveralunitsinGHSincludingtheCD unit, the HE unit, the PR unit with the Director General, the health research department(tobacco).
The Regenerative Health and Nutrition (RHN) programme falls in principle also under the NCDumbrella but ismanageddirectly by one staff atMoH.As indicated in the 2007-2008MTR, somefocusseemstohavebeenlostovertheyears.TheprogrammewasthepreviousMinister’sinitiative,but has since then been subject to resource competition as most other programmes. Someprogrammemessagessuchasonhealthydiets(vegetarian)arenotalwaysinlinewithotherhealtheducation messages on healthy diet (eggs, meat). Integrating MoH RHN with the GHS Chronicdiseasesunitwouldbemoreefficient.Inaddition,thehealtheducationunitcouldbestrengthenedandsplitbudgetsforhealtheducationconcentratedunderasingleunit.
In 2009 therewas some expectation of funding for sickle cell anaemia and cancer, but it did notcome.However,somepreparatoryworkwasdoneonthosediseases.Forsicklecellanaemia,GHSplanned to take over a project of neonatal screening from the university and appointed a focalperson.However, lack of funding andof consensus betweendifferent parties involvedmean thatnegotiationmeetingsarestillongoing.TheGatesFoundationmayfundsomeofthetransitioncosts;aMoUandPOWhavebeendeveloped.
GHS aims to develop a cross-sectoral cancer control planwith the help of AfrOx (Oxford,UK) butprogresshasbeenslow.Inaddition,a13millionUSDloan,facilitatedbyPACT(ProgrammeofAction
47Source:GHS,diseasecontrolprogramme.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 30
forCancerTherapy)hasbeensecuredwithaviewtosetuptwocancercentreswithradiotherapyunits.PendingonapprovaloftheloanbyParliament,moneywouldbecomeavailablein2011.
Two cancer registry units exist in Accra and Kumasi. Both registries are limited to local data,providedbyeitheroneormorehospital departments. Systematic screening for cancer is not yetimplementedinGhana.Screeningforcervixcancer isdonein3FPcentresandthepapillomavirusvaccine is yet too costly to be accessible on any large scale (some discussions are ongoing withGAVI). Screening for breast cancer is implemented by some NGOs (there are less than 10mammograms inGhanaandonly fewcytologists to interpretbiopsies). PSA forprostate cancer isbeingchecked(butnopolicyforstandardcheck-upexists),whileonlyfewhospitalscanimplementtheappropriatetreatment(Accra,Kumasi,private).
Astrategicframeworkformanagement,preventionandcontrolofNCDsinGhanaisbeingdeveloped(draft,March2010)butwasnotsharedwiththeIRT.Thiswasoneofthe2009milestonesandhasnotbeenachieved.AccordingtotheGHS,theDHIMSdoesnotsufficientlycoverspecificNCDrelateddata.
StandardtreatmentguidelinesformanagingNCDshavebeenupdated(aswasthecasefortheotherdiseases).Thiswasoneofthefouragreedmilestonesfor2009andhasbeenachieved.Howeverthestandardtreatmentguidelinestakeaspecificdiseasefocusratherthanatargetgroup/clientfocus.Reportedly, no guidelines exist on how and when to screen specific target groups, resulting in aseriouslyunderdiagnosisofmanyNCDs(butespeciallydiabetesandcardiovasculardiseases).SomeoftheNHIADRGsmayhavetoberevisedtotakethis intoaccount.Overall,accordingtoGHS,thequalityofdiabeticdiagnosisisanissue.
Summarising,NCDdidnotgettheattentionin2009asplanned.Althoughprevalenceisalarming,thelack of focus on NCDs reflects a continuous (both at a political and professional level)underestimating of the silent effects of NCDs on the general health status andwell-being of theGhanaianpeople,thatarepreventableandmanageable.
Keyrecommendation
• PutNCDshighonthepoliticalagenda,integratedifferentunitsofMoHandGHSdealingwithNCDsinordertocomeupwithoneplanandbudget,concentratehealtheducationbudgetlinesundertheGHSHealthEducationunit,andallocatetheneededhumanandfinancialresources.
• Finalise,resourceandimplementthestrategicframeworkformanagement,preventionandcontrolofNCDs.
• DeveloporupdatescreeningguidelinesforNCDs,focusingonspecifictargetgroups;andnegotiatewithNHIAhowtobestintegrateaNCDscreeningfocusinspecificOP/IPDRGs.
• AlthoughnotmanagedunderthenNCDresponsibility,obesityisanincreasingpublichealthproblem(seeholisticassessment,section2.1)thatneedstobeaddressed
•

GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 31
4. Howcanannualindependentreviewsbestcontribute?TheIRTnoticedacertain‘fatigue’withtheongoingannualreviewprocess.Thiswasclearfromtheinter-agencymeeting where different agencies presented their previous year’s performance withlimitedguidanceonwhatandhowtopresent(nostandardisedformat)andnoleadershiptodiscussmain strategic issues in line with set sector objectives. There is a risk of this event becoming aroutine activity losing its main purpose. In addition, it was difficult for the IRT to collect thenecessarydataandhavetherequestedinterviewsinatimelymanner.WhiletheIRTissupposedtovalidate evidence, the review risks to become a frustrating and time-consuming exercise ofexpensiveexpertssearchingfortheevidencewithlimitedtimeforin-depthanalysisanddiscussion.The2008annualreviewalreadycommentedonseveralaspectsofthereviewprocess.Werefertothat document for aspects of improving of routine systems for data collection and analysis;proposalsforcondensingtheBMCreviewsandplanningprocess;andthelimitedaddedvalueofthepartner’sreviewthroughaself-assessmentquestionnaire.In summary, the reviewprocess is an intenseand time-consumingprocess takingup to4months.Withtheexceptionoftheannual independentreview,theprocess isverymuchlocallyownedandpartandparceloftheannualplanningandevaluationcycle.AlthoughtheIRThasnotparticipatedinthe districts and regional reviews, it considers those essential for evaluating and improvingperformance and part of good management. From discussions held it appears that those peerreview processes are much appreciated at the operational level and catalytic in improvingperformance.However,nostandardSimilarly, the rationale for an annual agency based performance review iswell understood and anecessary event if properly used. However, the review would benefit from a standardisedpresentationofpreviousyearsplansandachievements,constraintsofreachingthesettargetsandhow the next year planwill address those issues. Importantly, itwould be informative if agency-based plans would clearly reflect how they contribute to main sector priorities (e.g. with theexceptionoftheGHSpresentation,noneoftheagencypresentationsindicatedhowtheywould‘dothings differently’ in improvingmaternal and neonatal health; and inmanaging NCDs) and if theinter-agencymeetingwouldbeusedtodiscussthosemainstrategicissuesunderastrongguidancefromMoH.Regarding the annual independent review, the IRT has a number of observations. It can bequestionedwhetherthistypeofintenseindependentreviewisnecessaryandshouldbedoneonanannualbasis.DifferentmodelsusedinothercountriesandannualSWApreviewsmaybeinterestingforGhanatoconsider.TheholisticassessmentshouldbecontinuedonanannualbasisbyMoH. Inordertofullyowntheprocessandthetool,itisrecommendedthatnextyearsassessmentisusedascapacitybuildingofanationalteamorfocalpersoninPPMEtoimplementthetool.Internationaltechnicalsupporttothisexercisecouldbeprogressivelywanedout.
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 32
5. MainconclusionsandrecommendationsTheholisticassessmentfor2009confirmsthatthehealthsectorhasbeenperformingrelativelywellin2009.ThehealthsectorhasachievedsomesubstantialimprovementsinserviceindicatorsrelatedtosomebutnotallHIRDrelatedactivities,includingmaternalhealth;andinsomeequityindicatorsrelated to supervised deliveries and equitable distribution of nurses between regions. Notably,utilisation of health services has continued to increase significantly both as a result of increasedhealth insurancecoverageandexemptionpolicy.Someindicatorssuchasobesityworsenedandingeneral healthy lifestyle, regenerative health and nutrition, NCDs, FP, CHPs and intersectoralcollaboration received less than expected focus. Overall, indicators on governance and financinghavebeenweak.Theoverallpictureofperformanceisthusmixed.Increasing fragmentation of the sector, both in terms of numbers of agencies with a specificmandateandincreasingcomplexityofhealthfinancing,requiresstronganddedicatedleadershiptomanage the sector and ensure sector priorities are beingmet. The sector is constrained by someimportant inefficiencies that have a cross-sectoral impact. These include late release of funds,increasinglylessflexiblefunding,toohighpricesformedicinesandstillsub-optimalperformanceofthe new health insurance financing mechanism. The MTR of the POW 2007-2011 suggests thatincreasedfragmentation,asacauseoraconsequence,hasleadtolessfocusonsomeagreedsectorpriorities over the period of the POW. In order to improve sector performance the above keyconstraintsneedtobeaddressedassoonaspossible.Other areas that require urgent attention include the compulsory retirement policy (of 60 years)which contributes to unacceptable loss of skilled and experienced health workers and the highnumbers of the ageing workforce that soon will need replacement. Funding and resourcing thehealth information system, shifting the attention to use of data for decision making rather than
Themainindependentreviewcouldbeorganiseddifferently.Severaloptionscanbeconsidered:
• Organising the independent review less frequently, for example year 1, 3 and 5 of thestrategicplanningcycle
• Continuingorganizingtheindependentreviewannuallyo but more focused (one priority area); one example is the annual review in
Tanzaniadonebyasmalltechnicalteam(2internationaland2nationalexperts);examplesofrecentfocuswasdistricthealthmanagement;PPME
o maintaining some continuity of experts1 (e.g. keeping a core teamof 2 expertsandaddingoneortwoexpertsasneeded)
o contractinganindependentmonitoringteamforanumberofyears(e.g.ateamof 4 experts hasbeen contracted for aperiodof 5 years tomonitor the sectorperformanceinPapuaNewGuinea;advantagesarecontinuityandflexibility)
• In order to ensure national ownership, it is recommended to have full-time involvednationalconsultantsaspartoftheteam
• Giventheunavailabilityofessentialdataatthetimeofthereview,itcanbequestionedwhethertheindependentreviewisorganisedtooearlyintheprocess?
• Thereportwouldbecomemoreuseful ifsharedwithregionalanddistrict teams;and ifrecommendations are formally translated by the MoH and stakeholders into agreedactionsthatareimplementedandfollowed-upduringthenextannualreview.
•
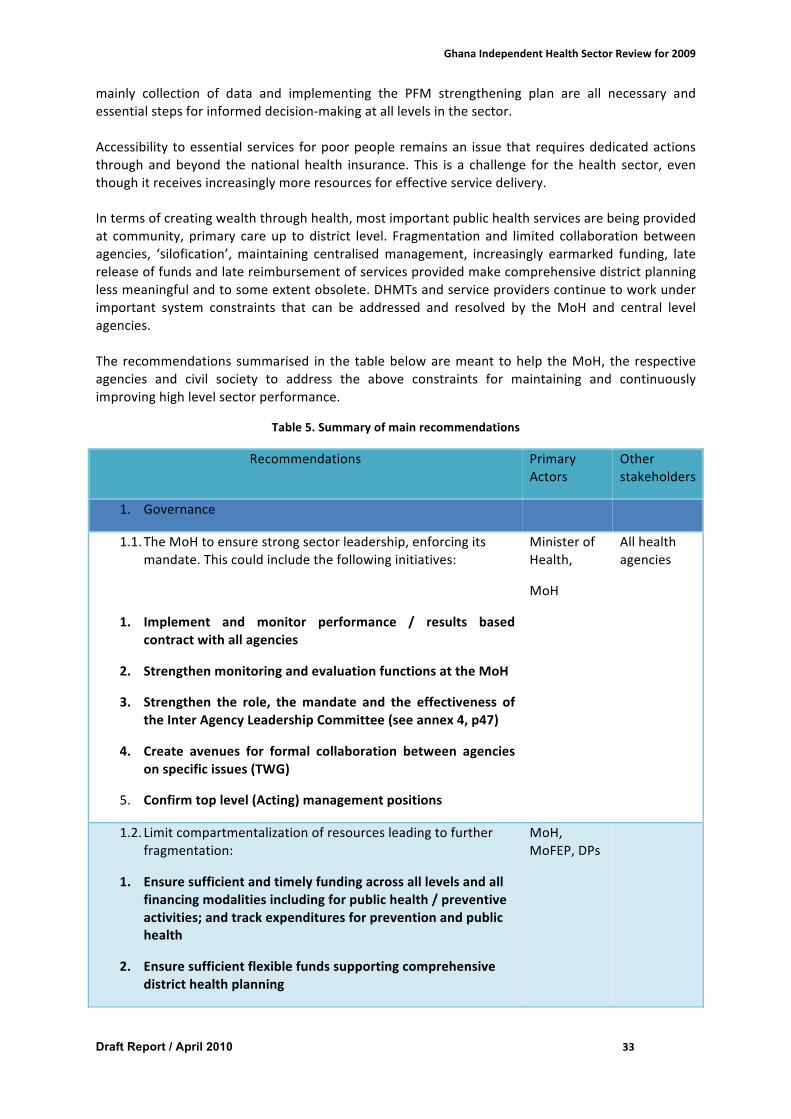
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 33
mainly collection of data and implementing the PFM strengthening plan are all necessary andessentialstepsforinformeddecision-makingatalllevelsinthesector.Accessibility toessential services forpoorpeople remainsan issue that requiresdedicatedactionsthrough andbeyond thenational health insurance. This is a challenge for thehealth sector, eventhoughitreceivesincreasinglymoreresourcesforeffectiveservicedelivery.Intermsofcreatingwealththroughhealth,mostimportantpublichealthservicesarebeingprovidedat community, primary careup todistrict level. Fragmentation and limited collaborationbetweenagencies, ‘silofication’,maintaining centralisedmanagement, increasingly earmarked funding, latereleaseoffundsandlatereimbursementofservicesprovidedmakecomprehensivedistrictplanninglessmeaningfulandtosomeextentobsolete.DHMTsandserviceproviderscontinuetoworkunderimportant system constraints that can be addressed and resolved by the MoH and central levelagencies.The recommendations summarised in the tablebelowaremeant tohelp theMoH, the respectiveagencies and civil society to address the above constraints for maintaining and continuouslyimprovinghighlevelsectorperformance.
Table5.Summaryofmainrecommendations
Recommendations PrimaryActors
Otherstakeholders
1. Governance
1.1. TheMoHtoensurestrongsectorleadership,enforcingitsmandate.Thiscouldincludethefollowinginitiatives:
1. Implement and monitor performance / results basedcontractwithallagencies
2. StrengthenmonitoringandevaluationfunctionsattheMoH
3. Strengthen the role, themandate and the effectiveness oftheInterAgencyLeadershipCommittee(seeannex4,p47)
4. Create avenues for formal collaboration between agenciesonspecificissues(TWG)
5. Confirmtoplevel(Acting)managementpositions
MinisterofHealth,
MoH
Allhealthagencies
1.2. Limitcompartmentalizationofresourcesleadingtofurtherfragmentation:
1. Ensuresufficientandtimelyfundingacrossalllevelsandallfinancingmodalitiesincludingforpublichealth/preventiveactivities;andtrackexpendituresforpreventionandpublichealth
2. Ensuresufficientflexiblefundssupportingcomprehensivedistricthealthplanning
MoH,MoFEP,DPs
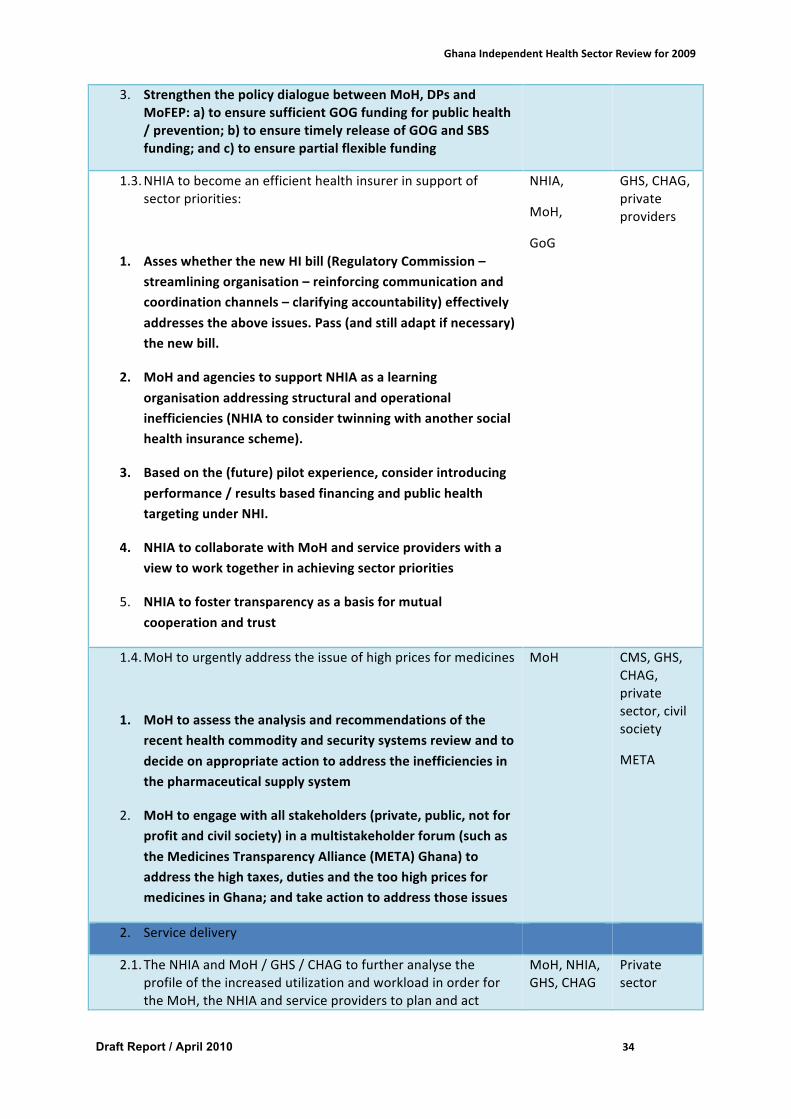
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 34
3. StrengthenthepolicydialoguebetweenMoH,DPsandMoFEP:a)toensuresufficientGOGfundingforpublichealth/prevention;b)toensuretimelyreleaseofGOGandSBSfunding;andc)toensurepartialflexiblefunding
1.3. NHIAtobecomeanefficienthealthinsurerinsupportofsectorpriorities:
1. AsseswhetherthenewHIbill(RegulatoryCommission–streamliningorganisation–reinforcingcommunicationandcoordinationchannels–clarifyingaccountability)effectivelyaddressestheaboveissues.Pass(andstilladaptifnecessary)thenewbill.
2. MoHandagenciestosupportNHIAasalearningorganisationaddressingstructuralandoperationalinefficiencies(NHIAtoconsidertwinningwithanothersocialhealthinsurancescheme).
3. Basedonthe(future)pilotexperience,considerintroducingperformance/resultsbasedfinancingandpublichealthtargetingunderNHI.
4. NHIAtocollaboratewithMoHandserviceproviderswithaviewtoworktogetherinachievingsectorpriorities
5. NHIAtofostertransparencyasabasisformutualcooperationandtrust
NHIA,
MoH,
GoG
GHS,CHAG,privateproviders
1.4. MoHtourgentlyaddresstheissueofhighpricesformedicines
1. MoHtoassesstheanalysisandrecommendationsoftherecenthealthcommodityandsecuritysystemsreviewandtodecideonappropriateactiontoaddresstheinefficienciesinthepharmaceuticalsupplysystem
2. MoHtoengagewithallstakeholders(private,public,notforprofitandcivilsociety)inamultistakeholderforum(suchastheMedicinesTransparencyAlliance(META)Ghana)toaddressthehightaxes,dutiesandthetoohighpricesformedicinesinGhana;andtakeactiontoaddressthoseissues
MoH
CMS,GHS,CHAG,privatesector,civilsociety
META
2. Servicedelivery
2.1. TheNHIAandMoH/GHS/CHAGtofurtheranalysetheprofileoftheincreasedutilizationandworkloadinorderfortheMoH,theNHIAandserviceproviderstoplanandact
MoH,NHIA,GHS,CHAG
Privatesector
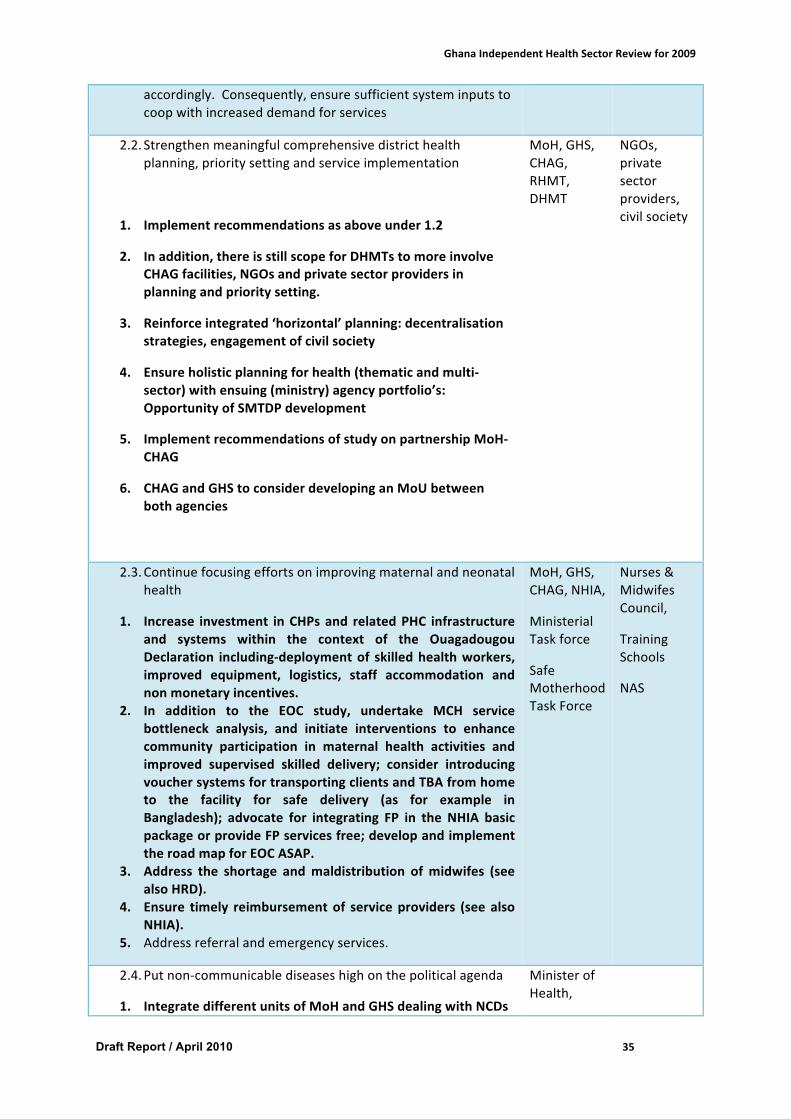
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 35
accordingly.Consequently,ensuresufficientsysteminputstocoopwithincreaseddemandforservices
2.2. Strengthenmeaningfulcomprehensivedistricthealthplanning,prioritysettingandserviceimplementation
1. Implementrecommendationsasaboveunder1.2
2. Inaddition,thereisstillscopeforDHMTstomoreinvolveCHAGfacilities,NGOsandprivatesectorprovidersinplanningandprioritysetting.
3. Reinforceintegrated‘horizontal’planning:decentralisationstrategies,engagementofcivilsociety
4. Ensureholisticplanningforhealth(thematicandmulti-sector)withensuing(ministry)agencyportfolio’s:OpportunityofSMTDPdevelopment
5. ImplementrecommendationsofstudyonpartnershipMoH-CHAG
6. CHAGandGHStoconsiderdevelopinganMoUbetweenbothagencies
MoH,GHS,CHAG,RHMT,DHMT
NGOs,privatesectorproviders,civilsociety
2.3. Continuefocusingeffortsonimprovingmaternalandneonatalhealth
1. Increase investment inCHPsand relatedPHC infrastructureand systems within the context of the OuagadougouDeclaration including-deploymentof skilledhealthworkers,improved equipment, logistics, staff accommodation andnonmonetaryincentives.
2. In addition to the EOC study, undertake MCH servicebottleneck analysis, and initiate interventions to enhancecommunity participation in maternal health activities andimproved supervised skilled delivery; consider introducingvouchersystemsfortransportingclientsandTBAfromhometo the facility for safe delivery (as for example inBangladesh); advocate for integrating FP in the NHIA basicpackageorprovideFPservicesfree;developandimplementtheroadmapforEOCASAP.
3. Address the shortage andmaldistribution ofmidwifes (seealsoHRD).
4. Ensure timely reimbursementof serviceproviders (seealsoNHIA).
5. Addressreferralandemergencyservices.
MoH,GHS,CHAG,NHIA,
MinisterialTaskforce
SafeMotherhoodTaskForce
Nurses&MidwifesCouncil,
TrainingSchools
NAS
2.4. Putnon-communicablediseaseshighonthepoliticalagenda
1. IntegratedifferentunitsofMoHandGHSdealingwithNCDs
MinisterofHealth,
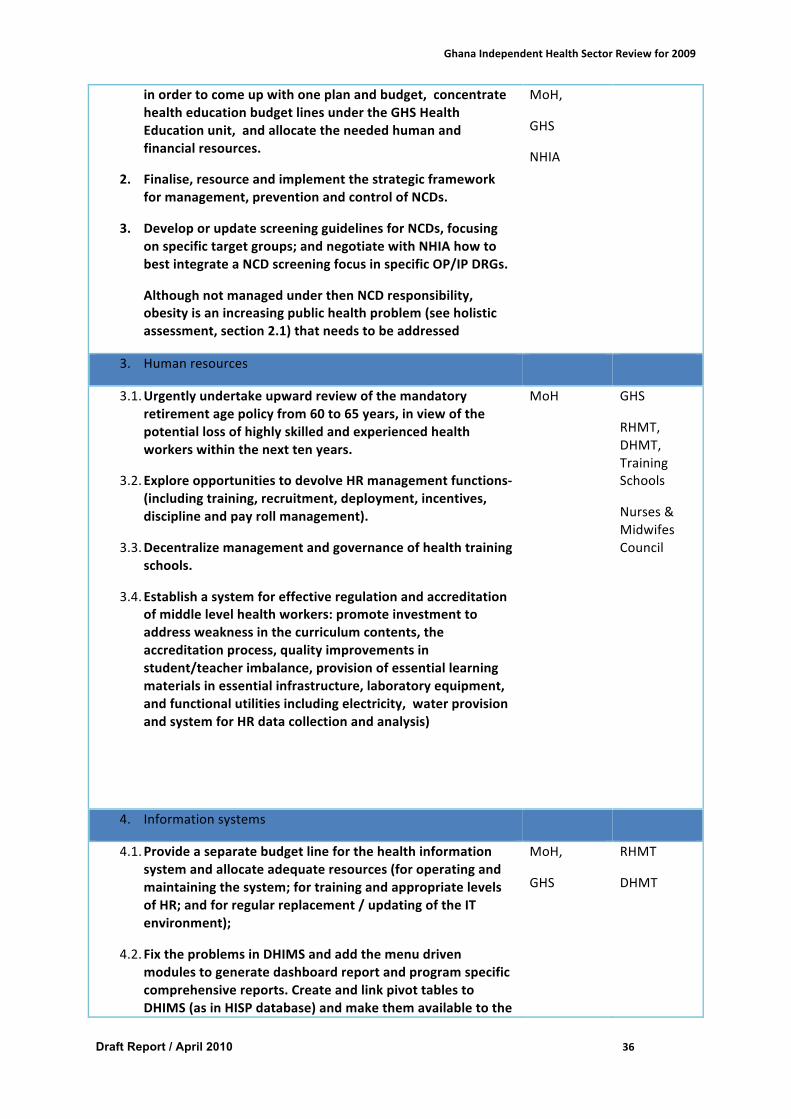
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 36
inordertocomeupwithoneplanandbudget,concentratehealtheducationbudgetlinesundertheGHSHealthEducationunit,andallocatetheneededhumanandfinancialresources.
2. Finalise,resourceandimplementthestrategicframeworkformanagement,preventionandcontrolofNCDs.
3. DeveloporupdatescreeningguidelinesforNCDs,focusingonspecifictargetgroups;andnegotiatewithNHIAhowtobestintegrateaNCDscreeningfocusinspecificOP/IPDRGs.
4. AlthoughnotmanagedunderthenNCDresponsibility,obesityisanincreasingpublichealthproblem(seeholisticassessment,section2.1)thatneedstobeaddressed
MoH,
GHS
NHIA
3. Humanresources
3.1. Urgentlyundertakeupwardreviewofthemandatoryretirementagepolicyfrom60to65years,inviewofthepotentiallossofhighlyskilledandexperiencedhealthworkerswithinthenexttenyears.
3.2. ExploreopportunitiestodevolveHRmanagementfunctions-(includingtraining,recruitment,deployment,incentives,disciplineandpayrollmanagement).
3.3. Decentralizemanagementandgovernanceofhealthtrainingschools.
3.4. Establishasystemforeffectiveregulationandaccreditationofmiddlelevelhealthworkers:promoteinvestmenttoaddressweaknessinthecurriculumcontents,theaccreditationprocess,qualityimprovementsinstudent/teacherimbalance,provisionofessentiallearningmaterialsinessentialinfrastructure,laboratoryequipment,andfunctionalutilitiesincludingelectricity,waterprovisionandsystemforHRdatacollectionandanalysis)
MoH GHS
RHMT,DHMT,TrainingSchools
Nurses&MidwifesCouncil
4. Informationsystems
4.1. Provideaseparatebudgetlineforthehealthinformationsystemandallocateadequateresources(foroperatingandmaintainingthesystem;fortrainingandappropriatelevelsofHR;andforregularreplacement/updatingoftheITenvironment);
4.2. FixtheproblemsinDHIMSandaddthemenudrivenmodulestogeneratedashboardreportandprogramspecificcomprehensivereports.CreateandlinkpivottablestoDHIMS(asinHISPdatabase)andmakethemavailabletothe
MoH,
GHS
RHMT
DHMT
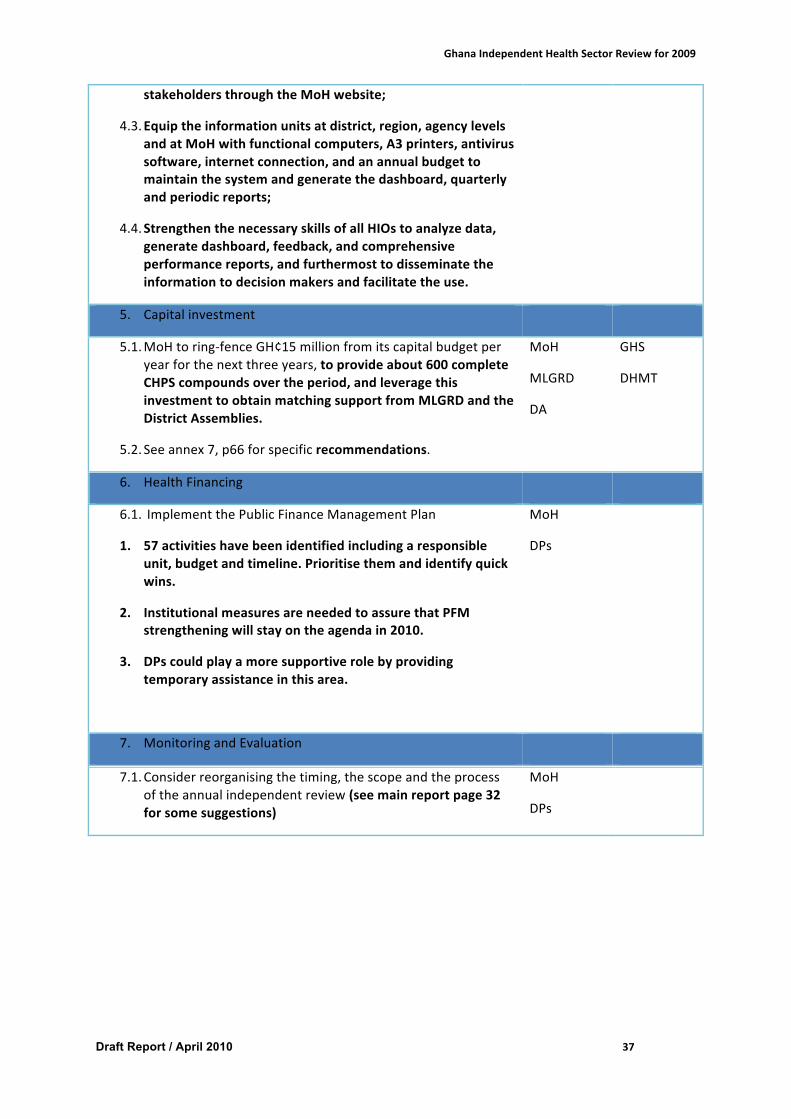
GhanaIndependentHealthSectorReviewfor2009
Draft Report / April 2010 37
stakeholdersthroughtheMoHwebsite;
4.3. Equiptheinformationunitsatdistrict,region,agencylevelsandatMoHwithfunctionalcomputers,A3printers,antivirussoftware,internetconnection,andanannualbudgettomaintainthesystemandgeneratethedashboard,quarterlyandperiodicreports;
4.4. StrengthenthenecessaryskillsofallHIOstoanalyzedata,generatedashboard,feedback,andcomprehensiveperformancereports,andfurthermosttodisseminatetheinformationtodecisionmakersandfacilitatetheuse.
5. Capitalinvestment
5.1. MoHtoring-fenceGH¢15millionfromitscapitalbudgetperyearforthenextthreeyears,toprovideabout600completeCHPScompoundsovertheperiod,andleveragethisinvestmenttoobtainmatchingsupportfromMLGRDandtheDistrictAssemblies.
5.2. Seeannex7,p66forspecificrecommendations.
MoH
MLGRD
DA
GHS
DHMT
6. HealthFinancing
6.1. ImplementthePublicFinanceManagementPlan
1. 57activitieshavebeenidentifiedincludingaresponsibleunit,budgetandtimeline.Prioritisethemandidentifyquickwins.
2. InstitutionalmeasuresareneededtoassurethatPFMstrengtheningwillstayontheagendain2010.
3. DPscouldplayamoresupportiverolebyprovidingtemporaryassistanceinthisarea.
MoH
DPs
7. MonitoringandEvaluation
7.1. Considerreorganisingthetiming,thescopeandtheprocessoftheannualindependentreview(seemainreportpage32forsomesuggestions)
MoH
DPs
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|1
ANNEXESAnnex1.TermsofReference
2009 HEALTH SECTOR REVIEW TERMS OF REFERENCE
January 2010
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|2
Table of CONTENTS 1. BACKGROUND 32. OBJECTIVES 33. FOCUS AND SCOPE OF THE REVIEW 44. METHODOLOGY AND ORGANISATION OF THE REVIEW 4
4.1 Methodology ................................................................................................................................. 44.2 Organization of the review ............................................................................................................ 44.3 Overall coordination of the review process................................................................................... 6
5. KEY AREAS FOR THE INDEPENDENT REVIEW 65.1 Health Services Delivery .............................................................................................................. 75.2 Human Resource Rationalisation .................................................................................................. 75.3 Monitoring and Evaluation ........................................................................................................... 85.4 Capital Investment ........................................................................................................................ 85.5 Good Governance and Partnerships .............................................................................................. 85.6 Health Financing and Financial management ............................................................................... 85.7 Agreed Milestones ........................................................................................................................ 9
6. OUTPUTS 97. TIMETABLE FOR THE REVIEW PROCESS 98. TEAM COMPOSITION 10
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|3
TERMS OF REFERENCE FOR THE 2009 HEALTH SECTOR REVIEW
1.BACKGROUND
The health sector in Ghana undertakes annual reviews of its performance as part of the partnership arrangements. In this context, an independent review is organised annually to provide evidence of performance and to indentify areas requiring attention in subsequent years. The foundations of the annual reviews lie in the performance monitoring systems at the level of budget and management centres (BMCs), which form the backbone of the health service delivery in Ghana. The review also provides a strong basis for decentralised monitoring and management of service delivery. Outputs of the review inform current implementation and guide the planning process for the next programme of work and budget and therefore constitute a critical activity on the health calendar.
The year 2009 represents the third year of the implementation of the current Five-Year Programme of work (2007 - 2011). This has however been truncated as a result of new developments in the Government’s policy development cycle. The new policy development cycle has mandated Ministries, Departments and Agencies (MDAs) to develop four-year Medium Term Development Plans (MTDP) for 2010 – 2013. In this regard the last two years of the current 5YPOW has been incorporated into the MTDP 2010-2013. In view of this, the Ministry will undertake a review of 2009, which in effect marks the end of the current 5YPOW, and also do a retrospective desk review of the implementation of the 2007 and 2008 POWs to assess the overall performance of the health sector for the three-year period.
The review will therefore place emphasis on the systems and structures, including arrangements, put in place to implement programmes outlined in the Five Year Programme of Work and assess results of policies and strategies. In this regard the review will incorporate agreements between Government and Development Partners under the MDBS/PRSC mechanisms. Specifically, the review will assess achievements defined in the MDBS/PRSC performance matrix using the agreed holistic assessment (HA) tool. The holistic assessment as was done for the 2008 review will provide a brief but well-informed, balanced and transparent appraisal of the health sector’s performance and factors that may have influenced such performance. It will also inform the dialogue between Development Partners and Government at sector level and feed into the discussion at MDBS and at Central Government level
2.OBJECTIVES
The overall objective of the 2009 annual review is to provide an independent assessment of the progress made in the implementation of the three-year lifespan of the 5YPOW (2007-2011). Specifically the review will:
1. Provide an overview of the results achieved and the challenges faced in the implementation of the three-year period of the 5YPOW III including highlights of the key challenges.
2. Assess and describe the sector’s performance for the year 2009 to include the holistic assessment.
3. Propose recommendations to address challenges identified.
3.FOCUSANDSCOPEOFTHEREVIEW
The focus of the review is two-fold:
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|4
I. The 2009 Programme of Work. The priorities, targets, resources and responsibilities agreed in the 2009 Programme of Work will be reviewed. A holistic assessment of 2009 will be conducted. The review will also assess the performance of the 2009 MDBS triggers and targets for the health sector.
II. An assessment of the sector’s performance over the three-year life span of the third five-year POW (2007-2011). The performance of the health sector for the three-year period will be placed in the context of the progress made on the milestones, sector-wide indicators and measured against the 2011 targets (the original end point of the 5YPOW) and the Millennium Development Goals.
The review will be sector-wide in scope. All BMCs, National Health Insurance Authority and Development Partners will review their contribution to the sector-wide objectives. The analysis of sector-wide performance will aim to demonstrate the contribution of the various components of the whole sector in the effort to deliver health as well as progress towards the MDGs.
4.METHODOLOGYANDORGANISATIONOFTHEREVIEW
4.1Methodology
The review process will involve a combination of self-assessment by BMCs, desk reviews, in-depth analysis and an independent assessment. The self-assessments will be conducted based on specific guidelines and end with performance hearings.
The desk reviews, in-depth analysis and independent review will be undertaken by a team of external and local consultants to review aspects of the health sector against the agreed terms of reference. The review will largely involve an analysis of documents and reports produced within the health sector. Review teams will undertake field visits to BMCs to validate information generated within the health system but not to collect primary data.
4.2Organizationofthereview
The review will have 6 components. These are:
I. BMC reviews and performance hearings – Each BMC will review its progress in the implementation of the plans and budget for 2009, prepare a 2009 annual report and hold performance hearings which in incorporate an element of peer review. The Agencies responsible for the BMC will coordinate the BMC reviews and consolidate BMC reports into an Agency report. This component of the review is expected to start in January and end in February 2010.
II. Interagency and Health Partners review:
a. The inter-agency review will constitute a technical review to assess progress made in the implementation of the agency-specific programmes, priority health interventions agreed and key service delivery strategies in the 2009 programme of work. Agencies will be required to submit their reports as well as their power-point presentations before the interagency performance hearing.
b. The performance of the Health Partners will also be reviewed in relation to their contributions to the health sector as against the Paris Declaration and Accra Agenda of Action and reports made available to feed into the independent review. An independent assessment would be conducted.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|5
III. In-depth review of key areas: A number of studies were commissioned last year by the Ministry and in collaboration with other health Partners. Some of these studies would be finalised to feed into the 2009 independent review and also be disseminated during the 2010 April Health summit. These include the following:
a. Ghana Health Commodity supplies and security systems review b. Capacity Development Evaluation c. Factors Affecting Motivation for Rural Practices Among Students in Health
Professional and Health Workers in Ghana d. Private Health Sector Assessment e. Research on Interaction of critical Health system functions and Global Fund
supported programs In light of these ongoing studies, the no new in-depth studies will be carried out during the review.
IV. Independent sector review - This component of the process will be a strategic assessment of the performance of the sector. An independent team of national and international experts would be constituted to validate and synthesize the reports from the internal reviews conducted by the MoH, Agencies and Partners as well as the reports from the in depth reviews and ongoing assessments.
The team shall conduct field visits to validate the reports but not to collect primary data. The independent review team will make recommendation for consideration by the MoH and Partners at the health summit. In addition to the review of the 2009 POW, a desk review of the 2007 and 2008 reviews will be undertaken and incorporated into the 2009 Independent review to provide a full three-year assessment of the health sector’s performance. The desk review will emphasis on the objectives and key strategies and use the existing data - DHS, MICS, MMS, DHIMS, SAM, the two previous Review reports (2007 and 2008) and other studies in the area of Child Health, HIRD etc to present the state of the "Nations Health". In addition, the team will how the sector is progressing towards the implementation of the framework for the Ouagadougou Declaration.
This component of the review will be carried out in country between 15th March and 2nd April 2010. The draft report will be submitted to the Chief Director of the Ministry of Health on or before 7th April 2010. It is expected that the leader of the independent review team will make a presentation of the findings of the review at the health summit.
Prior to the independent review, a nationwide data validation and consolidation exercise will be conducted to provide updated information on the sector-wide indicators.
V. Briefing Session for the Parliamentary Select Committee on Health: The Ministry and its agencies will organize a briefing session with the Parliamentary select committee on Health to present the sectors performance for the year 2009. This session is to offer the Ministry the opportunity to provide first hand information on its performance and progress for the year to the Parliamentarians and together discuss challenging facing the sector and how these can be addressed. This will take place from April 8 – 9 2010.
VI. Summit – The review will culminate in a summit to be held from 26-30 April 2010 to discuss findings and recommendations and map out the way forward. During the summit, the independent review and in-depth review reports will be discussed. A business meeting will be held at which the performance of the health sector, including the achievement of triggers and targets defined in the MDBS/PAF matrix. Partners at the end of the summit will sign an aide-memoire. The aide memoire will be shared with the
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|6
MDBS secretariat to form the basis of decisions on whether the health sector has achieved the targets and triggers defined in the MDBS/PAF matrix.
4.3Overallcoordinationofthereviewprocess
A planning committee drawn from the MoH, Agencies, and Partners will be set up to coordinate the review. This committee will agree on the overall orientation for the review, identify and select consultants, ensure that the timetables for Agency and sector-wide activities are harmonized and milestones are met. They will also ensure that the review is adequately funded and of good quality and ensure proper distribution and dissemination of reports. The planning committee will be serviced by a secretariat housed in the Ministry of Health.
5.KEYAREASFORTHEINDEPENDENTREVIEW
• Assess progress and challenges in creating the necessary awareness towards the reduction of the risk factors of non communicable diseases
• Assess progress and challenges towards service improvements in the management of non-communicable diseases.
5.1HealthServicesDelivery
To improve the effectiveness of health service delivery, the Ministry of health in 2009 aimed to do things differently to ensure better results and attainment of agreed targets. In this regard, the sector decided to refocus programmes and activities to increase the chances of meeting the medium term targets and in particular reduces maternal and neonatal deaths. The 2009 POW emphasised on improving maternal and neonatal health, intensify EPI activities to maintain high coverage, improve clinical care and strengthen emergency services; and reposition CHPS to provide maternal health services to be a link in the referral and emergency services.
The review will therefore examine progress made and challenges confronting the sector in these areas. Specifically the review team will:
§ Assess functionality of the district health system with particular reference to: o Planning and budgeting o Support and supervision systems o Referral systems at all levels o The provision of emergency services
§ Assess the progress made with the provision of emergency obstetric care at all levels of the health sector.
o Other interventions aimed at achieving MDG 4 and 5 including the implementation of the free maternal care initiative.
o Assess progress made in addressing neonatal mortality
5.2HumanResourceRationalisation
In 2009, the major challenge identified with HR management was the difficulties in HR planning due to lack of an update staffing norms to reflect the current situation. Staff retention and getting the right mix is still a challenge. The review will:
§ Assess progress made and the challenges in the implementation of the recommendations of Human Resource Forum
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|7
§ Assess mechanisms in place to improve productivity of the health workforce § Assess the progress of the sector on HR management and rationalisation specifically
in the areas of staffing norms related to staff placement, retention, and decentralisation of the management of salaries
§ Assess progress made with the implementation of performance management contracts and challenges associated with moving forward with implementation
§ Assess the progress made with updating the staffing norms.
5.3MonitoringandEvaluation
• Assess progress made and the challenges in the implementation of the single reporting systems and the overall systems for data collection, validation, storage and analysis
• Assess the extent to which data is used for decision making and feedback • Undertake a holistic assessment of the health sector using the HA tool
5.4CapitalInvestment
In 2009, the Capital Investment Programme was guided by the principle of equity and access to care and therefore to focus capital investments on achieving the MDGs.
The review will:
• Assess implementation of the capital Investment plan for 2009. • Assess progress with the implementation of the facility rationalisation agenda
5.5GoodGovernanceandPartnerships
Prior to 2009, the MoH encountered some challenges in the area of coordination and alignment of policies. To curb this, the Inter Agency Leadership Committee was strengthened to serve as a platform for the agencies to discuss and agree on priorities
The review will:
• Assess the existing governance structure within the health sector including the role of the IALC.
• Assess the purchaser – provider arrangements within the health sector • Identify actions to strengthen the partnerships within the sector
5.6HealthFinancingandFinancialmanagement
A sector PFM strengthening plan was developed towards the middle of 2009, though implementation has been constrained by delayed funding releases. Nevertheless, a number of activities have taken place in an attempt to address some of the recognised shortcomings in this area.
The review team will be expected to:
• Assess general progress made in development and implementation of the PFM strengthening plan, and specific progress in monitoring funding flows and budget
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|8
execution, revision of the Accounting, Treasury and Financial rules; and development of the internal audit strategic plan;
o Assess measures taken towards the development of integrated planning at the district level within Ghana Health Service in the light of the 2008 IRR recommendations
o Review changes in the Financial Statement in the light of 2008 IRR recommendations;
o Assess the current situation in reporting of earmarked funding within the context of the overall reporting system at all levels, and make appropriate recommendations for strengthening performance in this area.
• Review measures taken to expand the use of BPEMS in the sector in the light of the current GOG plans for development of an Integrated Financial Management Information System (GIFMIS).
• Measures to improve the management and reimbursement of claims, and to address capacity challenges at all levels in this respect (provider, DMHIS and NHIA);
• Assess the progress in the implementation of NHIS
5.7AgreedMilestones
In addition to the sector wide indicators, the sector agreed on some milestones for 2009. The review team will be expected to assess the implementation of these milestones, which will also feed into the holistic assessment.
• Working group on safe food and water established; implementation plan completed, costed and adopted.
• Clinical protocols established for early detection and treatment of diabetes, cardio-vascular diseases and common forms of cancer.
• Facility rationalisation plan completed and endorsed by health summit and used in the preparation of the 2010 POW.
• Private sector investment opportunities identified and PFM in the health sector strengthened.
6OUTPUTS
The key outputs of the review are the Independent review report and an Aide Memoir signed by the MoH and Development partners. In addition the following will be developed by the MoH as part of the process:
• Agency Review Reports • Partners Review Report • Regional and District Review reports • Report of Health Summit
7.TIMETABLEFORTHEREVIEWPROCESS
Activity Timelines
BMC Performance Hearings January – February 2010
Interagency and Health Partners review March 9 - 11 2010
Parliamentary Briefing April 7-8 2010
Independent sector review March 15 – April 2 2010
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|9
Health Summit April 26 – 30 2010
8.TEAMCOMPOSITION
A team leader will be identified, assisted by independent experts in the key areas of the main review. A team of 6 consultants will be joined by sector resource persons from the MoH and its Agencies.
Suggested areas of required expertise:
1. Health Systems 2. Health Economist / PFM 3. Monitoring and Evaluation 4. Human Resource 5. Capital Investment

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|10
Annex2.HolisticAssessmentofperformanceinthehealthsector2009
Introduction
Theholisticassessmentofperformance inthehealthsector isastructuredmethodologytoassessthequantity,qualityandspeedofprogressinachievingtheobjectivesofthePOW2007-2011.Theprimary objective of the assessment is to provide a brief but well-informed, balanced andtransparentassessmentof the sector’sperformanceand factors thatare likely tohave influencedthisperformance.Theassessmentisbasedonindicatorsandmilestonesspecifiedintheoperationalannual POW, derived from the strategic POW 2007-2011 which is linked with the GPRS II. Morespecifically,theanalysisunderlyingtheholisticassessmentisbasedonthefollowingelements:
- POW2007-2011SectorWideIndicatorsandMilestones- AnnualPOWincludingbudget- AnnualPerformanceReviewReportsfromMoHanditsAgencies- AnnualMoHFinancialStatement- Nationalsurveyreports(GhanaDHS,MICSetc.)
Process
Aninitialassessment,inregardstorealizationofmilestonesandtrendofindicators,isconductedaspartoftheannualindependenthealthsectorreviewprocess,followingapredefinedmethodology.This assessment will be presented at the April Health Summit where overall performance of thesectorwillbediscussed,takingintoconsiderationfactorswhichmayhaveinfluencedperformance.The assessment will be negotiated and agreed upon by Ministry of Health and its DevelopmentPartners during the subsequentBusinessMeeting, informedbydiscussions at theHealth Summit.Theoutcome,regardedastheHolisticAssessmentofperformanceintheHealthSector,willserveasan input into the Performance Assessment Framework (PAF) of theMulti Donor Budget Support(MDBS).Theprocessisexpectedtofacilitateestablishmentofconsensusonthesectorperformance.Such consensus is regarded as important for the constructive sector dialogue and uniformapproachesinbudgetsupportmechanisms.
Method
Theinitialassessmentisinthreesteps:First, each indicator and milestone is assigned a numerical value of -1, 0 or +1 depending onrealizationofmilestonesandtrendofindicators.Indicatorswhichareexpectedtobemeasuredonannualbasisare included ineachyear’sassessment. Indicatorswhicharenotmeasuredonannualbasis (e.g. survey based information like MICS, DHS etc.) are included in the assessment if newinformationisavailable.A milestone is assigned the value +1 if the review team is provided with a statement from therelevantauthoritydocumentingtherealizationofthemilestone;otherwiseitisassignedthevalue-1.Anindicatorisassignedthevalue+1(colourcodedgreen)if
• Theindicatorhasattainedthespecifiedannualtargetregardlessoftrend,or• The indicator has experienced a relative improvement bymore than 5% compared to the
previousyear’svalueAnindicatorisassignedthevalue-1(colourcodedred)if
• Theindicatorhasexperiencedarelativedeteriorationbymorethan5%,or• If nodata is available (only applies to annuallymeasured indicators andnot to survey
indicators)
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|11
Anindicatorisassignedthevalue0(colourcodedyellow)if• Therelativetrendoftheindicatorcomparedtopreviousyeariswithina5%range,or• Theindicatorhasnotpreviouslybeenreported
Second,theindicatorsandmilestonesaregroupedintoGoalsandStrategicObjectivesasdefinedintheProgrammeofWorkand the sumof indicator andmilestone values are calculated.Goals andStrategicObjectiveswithapositivescoreareassignedavalueof+1,-1ifthetotalscoreisnegativeand0ifthetotalscoreis0.Third,afterassigninganumericalscoretoeachoftheGoalsandStrategicObjectivesthescoresareadded together to determine the sector’s score.While a positive sector score is interpreted as ahighlyperformingsector,anegativescoreis interpretedasanunderperformingsectorandascoreofzeroisconsideredtobesustainedperformance.
Results
Step1:Resultsindividualindicatorsandmilestones
Goal1–Ensurethatchildrensurviveandgrowtobecomehealthyandproductiveadultsthatreproducewithoutrisksofinjuriesordeath
Goal1indicatorsarenotmeasuredonannualbasis,andfor2009,thereisnonewinformationavailable.
Infantmortalityrate
2009Performance:Nonewdatafor20092009Target:N/ASource:DHS2008Outcome:N/A
TheDHS2008showedasignificantdeclineinIMRinthefiveyearsrunningupto2008.However,somecautioniscalledfor,asthedatawastakenfromthebirthhistoryintheWomen’sQuestionnaire,andthestudynotedthatwomenmaybereluctanttoreportinfantandchilddeaths,leadingtoanunderestimate.
Under-fivemortalityrate
2009Performance:Nonewdatafor20092009Target:N/ASource:DHS2008Outcome:N/A
Under-fivemortalityrateshavereducedsubstantiallyinthe2008estimates,whichisasignificantgainforGhana,thoughthecautionmentionedundertheIMRsectionaboveshouldbenoted.
Maternalmortalityrate
1998 2003 2008 200957 64 50 -
1998 2003 2008 2009 108 111 80 -
2008 2009
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|12
2009Performance:Nonewdatafor20092009Target:N/ASource:Maternalmortalitysurvey2008Outcome:N/A
ThematernalmortalitysurveyreportedMMRfiguresat451maternaldeathsper100,000livebirthsoverthe7yearsprecedingthesurvey.Thereisnorecentdataavailableforcomparison.
Under-fiveprevalenceoflowweightforage
2009Performance:Nonewdatafor20092009Target:N/ASource:DHS2008Outcome:N/A
TheDHS2008reportshowedasignificantdropof23%intheproportionofchildrenwhoarebelow-2standarddeviationsfromthemedianreferencepopulation.
Totalfertilityrate
2009Performance:Nonewdatafor20092009Target:N/ASource:DHS2008Outcome:N/A
Totalfertilityrateshavereducedoverthepastfiveyearsfrom4.4to4,accordingtotheDHS2008.Thisisadropofsome9%.
Goal2–Reducetheexcessriskandburdenofmorbidity,disabilityandmortalityespeciallyinthepoorandmarginalizedgroups
HIVprevalenceamongpregnantwomen15-24years
2009Performance:2.92009Target:2.4Source:NACP-GHSOutcome:-1
ThedeclineinmedianHIVprevalenceamongpregnantwomen,whichwasobservedovertheprevioustwosentinelsurveys,couldnotbesustainedin2009,wheretheprevalenceincreasedto2.9%.
Easternregion,andspeciallyKoforidua,continuedtobetheareaswithhighestprevalence,4.2%and5.8%respectively.ThelowestprevalencewasfoundinNorthernRegionwith2.0%infectedpregnantwomen.
Thenationalprevalencewasmodelledbasedontheannuallymeasuredsentinelsurveyresult.In2009,themodelledadultnationalHIVprevalence(15-49years)was1.9%,withanestimated267,069adultsandchildrenlivingwithHIVandAIDS.Therewere22,177newinfectionsand20,313AIDSdeaths.Despiteannualvariationsinthesentinelsurveyresults,themodelindicatesthatthenationalprevalenceratehasstabilizedatapproximately1.9%,andsignificantvariationsarenotexpectedfortheyearstocome.
GuineaWorm
451 -
2006 2008 200918% 13.9% -
1998 2003 2008 2009 4.4 4.3 4.0 -
2006 2007 2008 20092.9% 2.6% 2.2% 2.9%
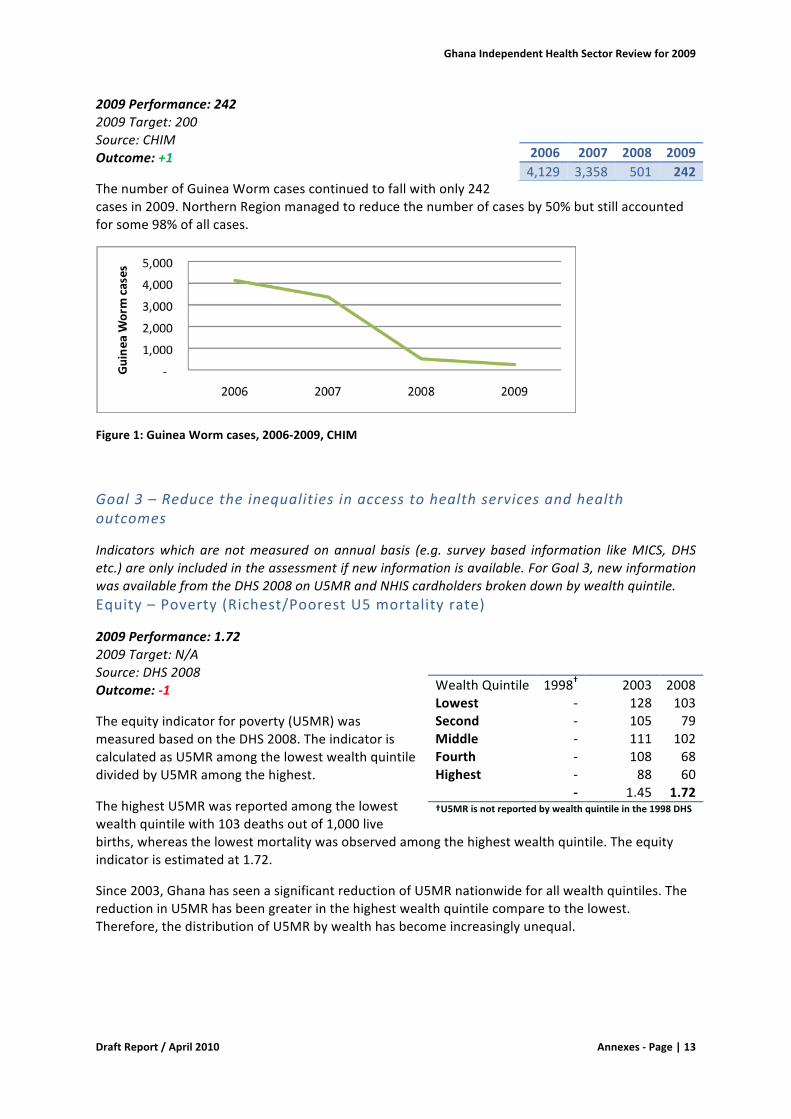
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|13
2009Performance:2422009Target:200Source:CHIMOutcome:+1
ThenumberofGuineaWormcasescontinuedtofallwithonly242casesin2009.NorthernRegionmanagedtoreducethenumberofcasesby50%butstillaccountedforsome98%ofallcases.
Figure1:GuineaWormcases,2006-2009,CHIM
Goal3–Reducetheinequalitiesinaccesstohealthservicesandhealthoutcomes
Indicatorswhich are notmeasured on annual basis (e.g. survey based information likeMICS, DHSetc.)areonlyincludedintheassessmentifnewinformationisavailable.ForGoal3,newinformationwasavailablefromtheDHS2008onU5MRandNHIScardholdersbrokendownbywealthquintile.Equity–Poverty(Richest/PoorestU5mortalityrate)
2009Performance:1.722009Target:N/ASource:DHS2008Outcome:-1
Theequityindicatorforpoverty(U5MR)wasmeasuredbasedontheDHS2008.TheindicatoriscalculatedasU5MRamongthelowestwealthquintiledividedbyU5MRamongthehighest.
ThehighestU5MRwasreportedamongthelowestwealthquintilewith103deathsoutof1,000livebirths,whereasthelowestmortalitywasobservedamongthehighestwealthquintile.Theequityindicatorisestimatedat1.72.
Since2003,GhanahasseenasignificantreductionofU5MRnationwideforallwealthquintiles.ThereductioninU5MRhasbeengreaterinthehighestwealthquintilecomparetothelowest.Therefore,thedistributionofU5MRbywealthhasbecomeincreasinglyunequal.
2006 2007 2008 20094,129 3,358 501 242
WealthQuintile 1998† 2003 2008Lowest - 128 103Second - 105 79Middle - 111 102Fourth - 108 68Highest - 88 60 - 1.45 1.72†U5MRisnotreportedbywealthquintileinthe1998DHS
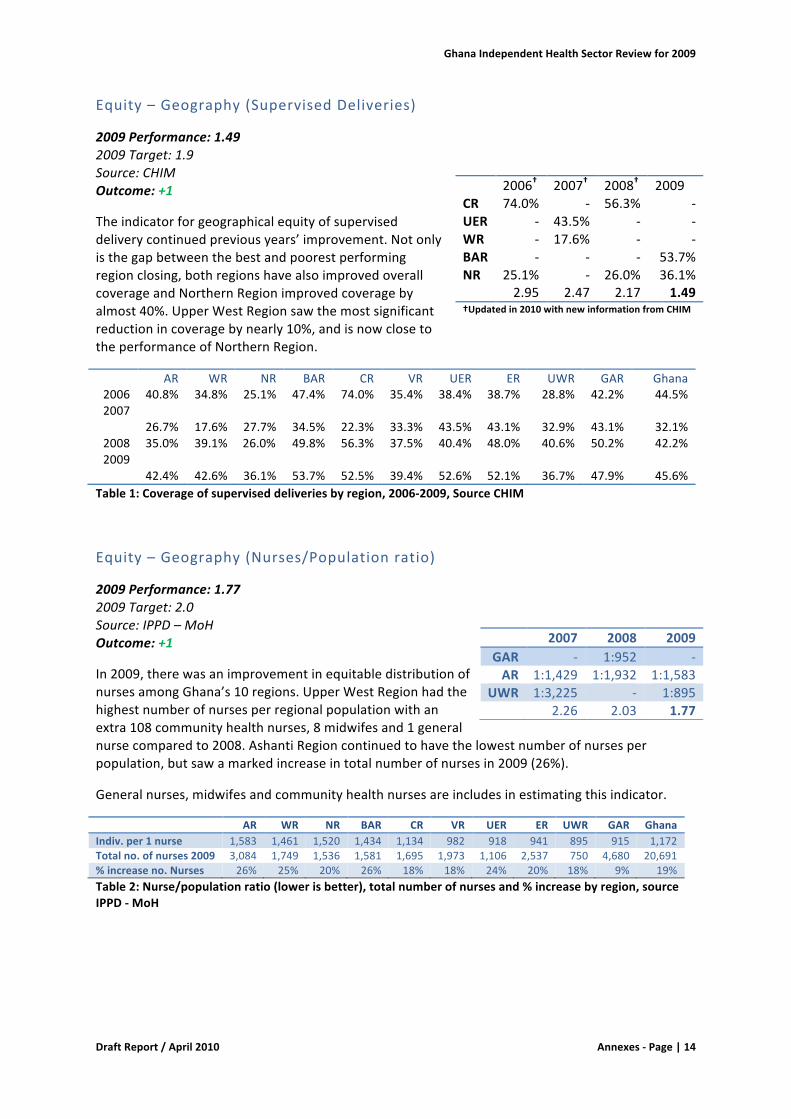
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|14
Equity–Geography(SupervisedDeliveries)
2009Performance:1.492009Target:1.9Source:CHIMOutcome:+1
Theindicatorforgeographicalequityofsuperviseddeliverycontinuedpreviousyears’improvement.Notonlyisthegapbetweenthebestandpoorestperformingregionclosing,bothregionshavealsoimprovedoverallcoverageandNorthernRegionimprovedcoveragebyalmost40%.UpperWestRegionsawthemostsignificantreductionincoveragebynearly10%,andisnowclosetotheperformanceofNorthernRegion.
AR WR NR BAR CR VR UER ER UWR GAR Ghana2006 40.8% 34.8% 25.1% 47.4% 74.0% 35.4% 38.4% 38.7% 28.8% 42.2% 44.5%2007
26.7% 17.6%
27.7% 34.5% 22.3% 33.3% 43.5% 43.1% 32.9% 43.1% 32.1%2008 35.0% 39.1% 26.0% 49.8% 56.3% 37.5% 40.4% 48.0% 40.6% 50.2% 42.2%2009
42.4% 42.6%
36.1% 53.7% 52.5% 39.4% 52.6% 52.1% 36.7% 47.9% 45.6%Table1:Coverageofsuperviseddeliveriesbyregion,2006-2009,SourceCHIM
Equity–Geography(Nurses/Populationratio)
2009Performance:1.772009Target:2.0Source:IPPD–MoHOutcome:+1
In2009,therewasanimprovementinequitabledistributionofnursesamongGhana’s10regions.UpperWestRegionhadthehighestnumberofnursesperregionalpopulationwithanextra108communityhealthnurses,8midwifesand1generalnursecomparedto2008.AshantiRegioncontinuedtohavethelowestnumberofnursesperpopulation,butsawamarkedincreaseintotalnumberofnursesin2009(26%).
Generalnurses,midwifesandcommunityhealthnursesareincludesinestimatingthisindicator.
AR WR NR BAR CR VR UER ER UWR GAR GhanaIndiv.per1nurse 1,583 1,461 1,520 1,434 1,134 982 918 941 895 915 1,172Totalno.ofnurses2009 3,084 1,749 1,536 1,581 1,695 1,973 1,106 2,537 750 4,680 20,691%increaseno.Nurses 26% 25% 20% 26% 18% 18% 24% 20% 18% 9% 19%Table2:Nurse/populationratio(lowerisbetter),totalnumberofnursesand%increasebyregion,sourceIPPD-MoH
2006† 2007† 2008† 2009CR 74.0% - 56.3% -UER - 43.5% - -WR - 17.6% - -BAR - - - 53.7%NR 25.1% - 26.0% 36.1% 2.95 2.47 2.17 1.49†Updatedin2010withnewinformationfromCHIM
2007 2008 2009GAR - 1:952 -AR 1:1,429 1:1,932 1:1,583
UWR 1:3,225 - 1:895 2.26 2.03 1.77
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|15
Equity–Gender(Female/MaleNHISCardHolderratio)
2009Performance:Nodata2009Target:1.2Source:NHIAOutcome:-1
Equity–Poverty(Richest/PoorestNHISCardHolderratio)
2009Performance:1.62009Target:N/ASource:DHS2008Outcome:0
Theequityindicatorforpoverty(NHISCardHolderratio)wasmeasuredforthefirsttimebasedontheDHS2008results,andiscalculatedastheproportionofcardholdersinthehighestwealthquintiledividedbythelowest.Sincethereisnobaselineortargetfortheindicator,theoutcomeis0.
DuetorestrictionsinthesamplingdesignoftheDHS2008,theindicatorhasbeensplitintowomen’sandmen’s’insurancecoverageandonlyincludesindividualsofage15-49.Childrenunder15yearswerenotincluded.
StrategicaObjective1-HealthyLifestyleandHealthyEnvironment
Indicatorswhich are notmeasured on annual basis (e.g. survey based information likeMICS, DHSetc.) are only included in theassessment if new information is available. For strategic objective 1,newinformationwasavailablefromtheDHS2008onobesityinadultpopulation.
Milestone:InformationdocumentandcommunicationstrategyrelatedtopreventionofNCDsdevelopedandshared
2009Performance:NoactiontakenSource:MoHOutcome:-1
Obesityinadultpopulation(womenage15-49years)
2009Performance:9.3%2009Target:N/ASource:DHSOutcome:-1
Obesity(BMI≥30)amongwomenaged15-49increasedby15%from2003to2008,andwhilealmost10%ofthefemalepopulation15-49areobeseover20%areoverweight.With19.4%ofwomenintheagegroupbeingobeseand25.1%overweight,GreaterAccraRegionhadsignificantlyhigherprevalenceofobesityandoverweightthananyotherregion.Westernregionhadthesecondhighestprevalenceofobesityestimatedat9.9%.UpperWestandNorthernRegionhadthelowestprevalencewith2.4%obese,aswellas10.3%and11.5%overweight,respectively.
2006 2007 2008 2009N/A N/A 1.22 -
WealthQuintile Women MenLowest 29.3% 16.6%Second 31.7% 22.5%Middle 37.8% 25.9%Fourth 43.8% 35.2%Highest 47.0% 37.7% 1.6 2.3
1998 2003 2008 2009- 8.1% 9.3% -
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|16
DHS2003 DHS2008BMI<18.5(thin) 9.3% 8.6%BMI25.0-29.9(overweight) 17.2% 20.7%BMI≥30(obese) 8.1% 9.3%Table3:Obesityandoverweightamongwomen15-49,SourceDHS2003andDHS2008
StrategicaObjective2–ProvisionofHealth,ReproductionandNutritionServices
Milestone:Clinicalprotocolsestablishedforearlydetectionandtreatmentofdiabetes,cardio-vasculardiseasesandcommonformsofcancer
2009Performance:ProtocolshavebeenrevisedandcapturedintheStandardTreatmentGuidelineswhichisinprintSource:MoHOutcome:+1
StandardtreatmentguidelinesformanagingNCDshavebeenupdated(aswasthecasefortheotherdiseases).Forthecommonformsofcanceronlybreastcancerhasbeenincluded.Also,thestandardtreatmentguidelinestakeaspecificdiseasefocusratherthanatargetgroup/clientfocus.Reportedly,noguidelinesexistonhowandwhentoscreenspecifictargetgroups,resultinginanunder-diagnosisofmanyNCDs.
%Deliveriesattendedbyatrainedhealthworker
2009Performance:45.6%2009Target:60%Source:CHIMOutcome:+1
Theproportionofdeliveriesattendedbyatrainedhealthworkerincreasedby17%,andhencecontinuedthepositivetrendexperiencedsince2007.Thetargetof60%,however,wasnotmet.
TheDHS2008estimatedthepercentageofbirthassistedbyaskilledproviderat58.7%forGhana.Thisfigureissignificantlyhigherthanthepercentagereportedthroughtheroutinehealthinformationsystem,whichraisesaconcernaboutqualityandcompletenessofroutinereportingonthisindicator.
AdeeperanalysisoftheDHS2008datarevealsthattherewerelargeregionalvariationsintheindicator.InGreaterAccraRegion84.3%deliverieswereattendedbyskilledprovider,whileonly27.2%wereattendedbyskilledproviderinNorthernRegion.
AR WR NR BAR CR VR UER ER UWR GAR GhanaDHS2008 72.6% 61.7% 27.2% 65.5% 54.0% 53.7% 46.7% 60.8% 46.1% 84.3% 58.7%Table4:Percentagedeliveredbyskilledprovider,SourceDHS2008
Regionaldifferencesobservedintheroutinedataarediscussedundertheaboveindicator“Equity–Geography(SupervisedDeliveries)”.
2006 2007 2008 200944.5% 32.1% 39.1% 45.6%
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|17
ContraceptivePrevalenceRate(formodernmethods)
2009Performance:31.1%2009Target:35%Source:CHIMOutcome:-1
From2008to2009,contraceptiveprevalenceratedroppedby8%.Whilelongtermcoupleyearsofprotection(CYP)remainedataround142,000,shorttermCYPdroppedby33%from654,072in2008to439,573in2009.TheindicatortrendcorrespondswellwithinformationpresentedtothereviewteamconcerningageneralshortageofshorttermmethodsinGhanaduringthepreviousyear.Thesocialmarketedbrandsofcondoms,e.g.GhanaSocialMarketingFoundationbrand,whichin2008constitutedmorethanhalfofallcondomssoldinGhana,havereportedlybeeninparticularshortagein2009.
AntenatalCareCoverage
2009Performance:92.1%2009Target:95%Source:CHIMOutcome:-1
From2008to2009,thecoverageofpregnantwomen,whoreceivedoneormoreantenatalcarevisits,droppedby5.4%.Inthesameperiod,theproportionofpregnantwomenwhoreceived4ormorevisitsincreasedsignificantlyfrom62.3%to75.2%.Thisindicatesthatthemajority,almost90%,ofwomennowfollowtherecommendedANCcourseofminimum4visits.
%U5ssleepingunderITN
2009Performance:Nonewdata2009Target:60%Source:-Outcome:N/A
Thepercentageofchildrenunder5yearssleepingunderITNisasurveyindicator,andin2009nosurveywasconducted.
Penta3immunization
2009Performance:89.3%2009Target:90%Source:CHIMOutcome:0
AfteraslightdropinPenta3coveragein2008,performanceisnowbackontrack,almostreachingthetargetof90%coverage.Comparedto2008,however,theimprovementiswithinthe5%rangeindicatingsustainedperformance,henceaneutraloutcome.
AregionalbreakdownoftheindicatorrevealsthatcoverageinGreaterAccraRegion(72.7%)issignificantlowerthattheaverageof89.3%andthemedianof90.1%.AnEPIsurveyfrom2009performedinGreaterAccraRegionshowssignificantlyhighercoverageofPentathreeat96.1%andpercentagefullyimmunizedat90.0%.
2006 2007 2008 200925.4% 23.2% 33.8% 31.1%
2006 2007 2008 200988.4% 89.5% 97.4% 92.1%
2006 2007 2008 200941.7% 55.3% 40.5% -
2006 2007 2008 200984.2% 88.0% 86.6% 89.3%
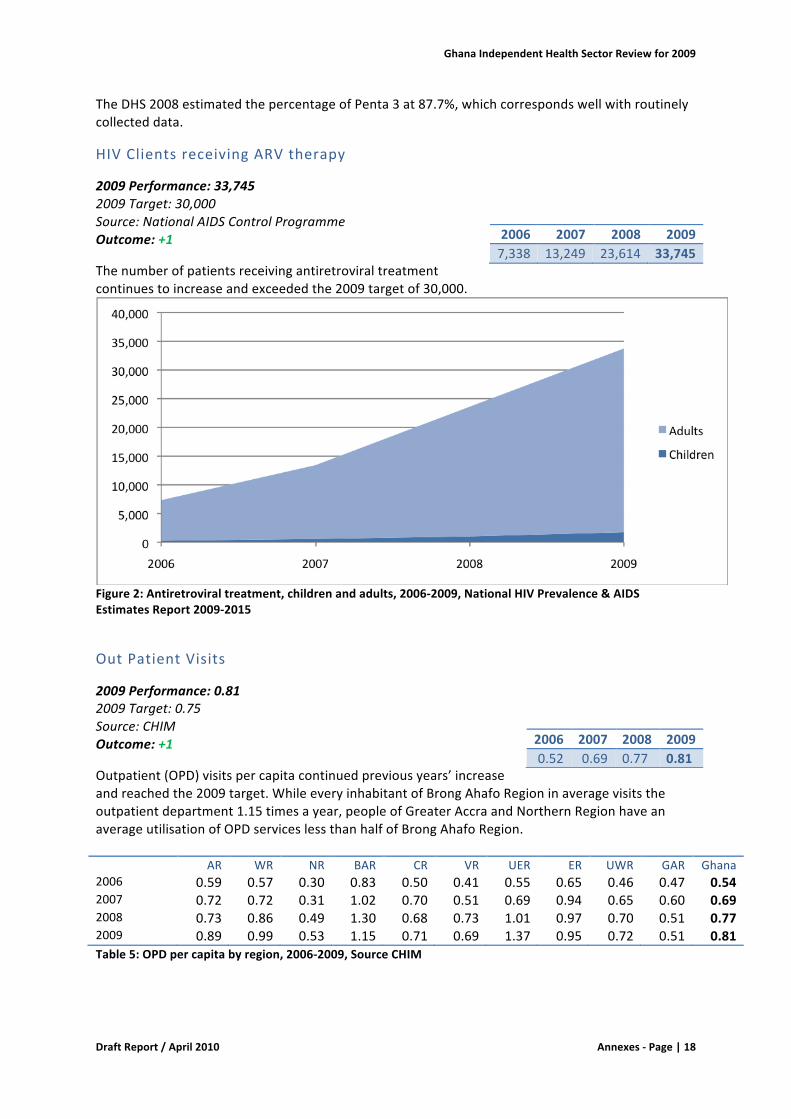
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|18
TheDHS2008estimatedthepercentageofPenta3at87.7%,whichcorrespondswellwithroutinelycollecteddata.
HIVClientsreceivingARVtherapy
2009Performance:33,7452009Target:30,000Source:NationalAIDSControlProgrammeOutcome:+1
Thenumberofpatientsreceivingantiretroviraltreatmentcontinuestoincreaseandexceededthe2009targetof30,000.
Figure2:Antiretroviraltreatment,childrenandadults,2006-2009,NationalHIVPrevalence&AIDSEstimatesReport2009-2015
OutPatientVisits
2009Performance:0.812009Target:0.75Source:CHIMOutcome:+1
Outpatient(OPD)visitspercapitacontinuedpreviousyears’increaseandreachedthe2009target.WhileeveryinhabitantofBrongAhafoRegioninaveragevisitstheoutpatientdepartment1.15timesayear,peopleofGreaterAccraandNorthernRegionhaveanaverageutilisationofOPDserviceslessthanhalfofBrongAhafoRegion. AR WR NR BAR CR VR UER ER UWR GAR Ghana2006 0.59 0.57 0.30 0.83 0.50 0.41 0.55 0.65 0.46 0.47 0.542007 0.72 0.72 0.31 1.02 0.70 0.51 0.69 0.94 0.65 0.60 0.692008 0.73 0.86 0.49 1.30 0.68 0.73 1.01 0.97 0.70 0.51 0.772009 0.89 0.99 0.53 1.15 0.71 0.69 1.37 0.95 0.72 0.51 0.81Table5:OPDpercapitabyregion,2006-2009,SourceCHIM
2006 2007 2008 20097,338 13,249 23,614 33,745
2006 2007 2008 20090.52 0.69 0.77 0.81
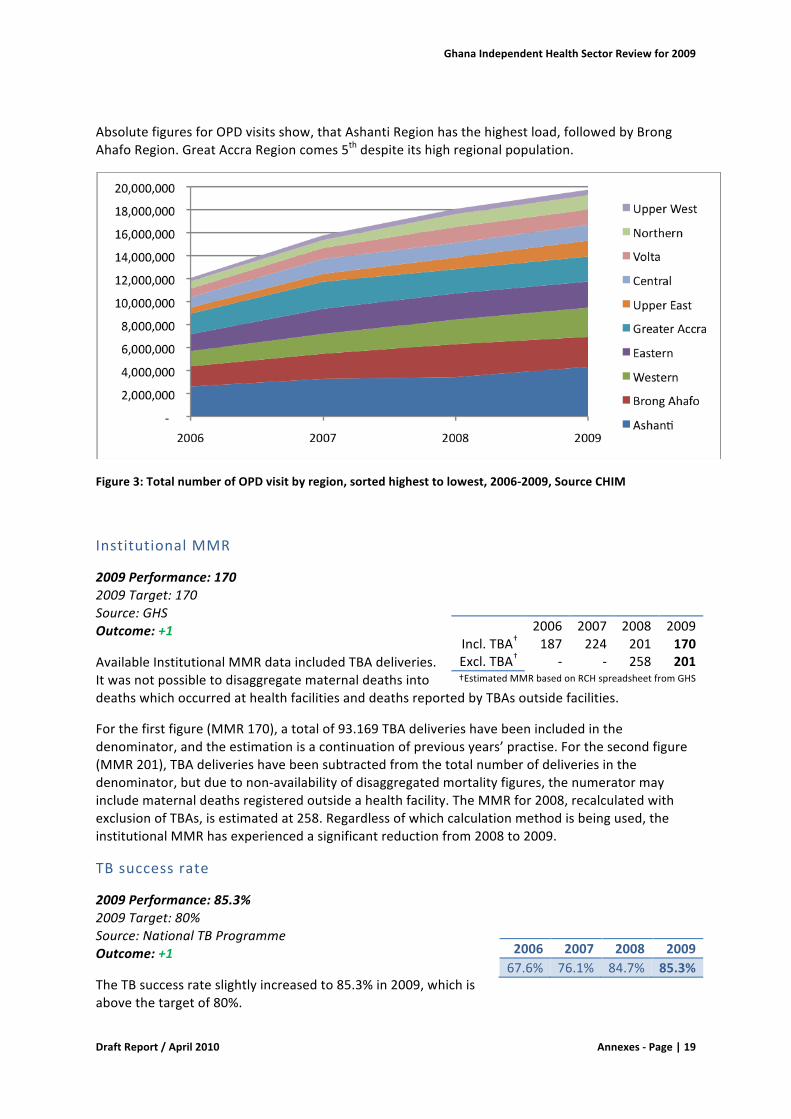
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|19
AbsolutefiguresforOPDvisitsshow,thatAshantiRegionhasthehighestload,followedbyBrongAhafoRegion.GreatAccraRegioncomes5thdespiteitshighregionalpopulation.
Figure3:TotalnumberofOPDvisitbyregion,sortedhighesttolowest,2006-2009,SourceCHIM
InstitutionalMMR
2009Performance:1702009Target:170Source:GHSOutcome:+1
AvailableInstitutionalMMRdataincludedTBAdeliveries.ItwasnotpossibletodisaggregatematernaldeathsintodeathswhichoccurredathealthfacilitiesanddeathsreportedbyTBAsoutsidefacilities.
Forthefirstfigure(MMR170),atotalof93.169TBAdeliverieshavebeenincludedinthedenominator,andtheestimationisacontinuationofpreviousyears’practise.Forthesecondfigure(MMR201),TBAdeliverieshavebeensubtractedfromthetotalnumberofdeliveriesinthedenominator,butduetonon-availabilityofdisaggregatedmortalityfigures,thenumeratormayincludematernaldeathsregisteredoutsideahealthfacility.TheMMRfor2008,recalculatedwithexclusionofTBAs,isestimatedat258.Regardlessofwhichcalculationmethodisbeingused,theinstitutionalMMRhasexperiencedasignificantreductionfrom2008to2009.
TBsuccessrate
2009Performance:85.3%2009Target:80%Source:NationalTBProgrammeOutcome:+1
TheTBsuccessrateslightlyincreasedto85.3%in2009,whichisabovethetargetof80%.
2006 2007 2008 2009Incl.TBA† 187 224 201 170Excl.TBA† - - 258 201†EstimatedMMRbasedonRCHspreadsheetfromGHS
2006 2007 2008 200967.6% 76.1% 84.7% 85.3%
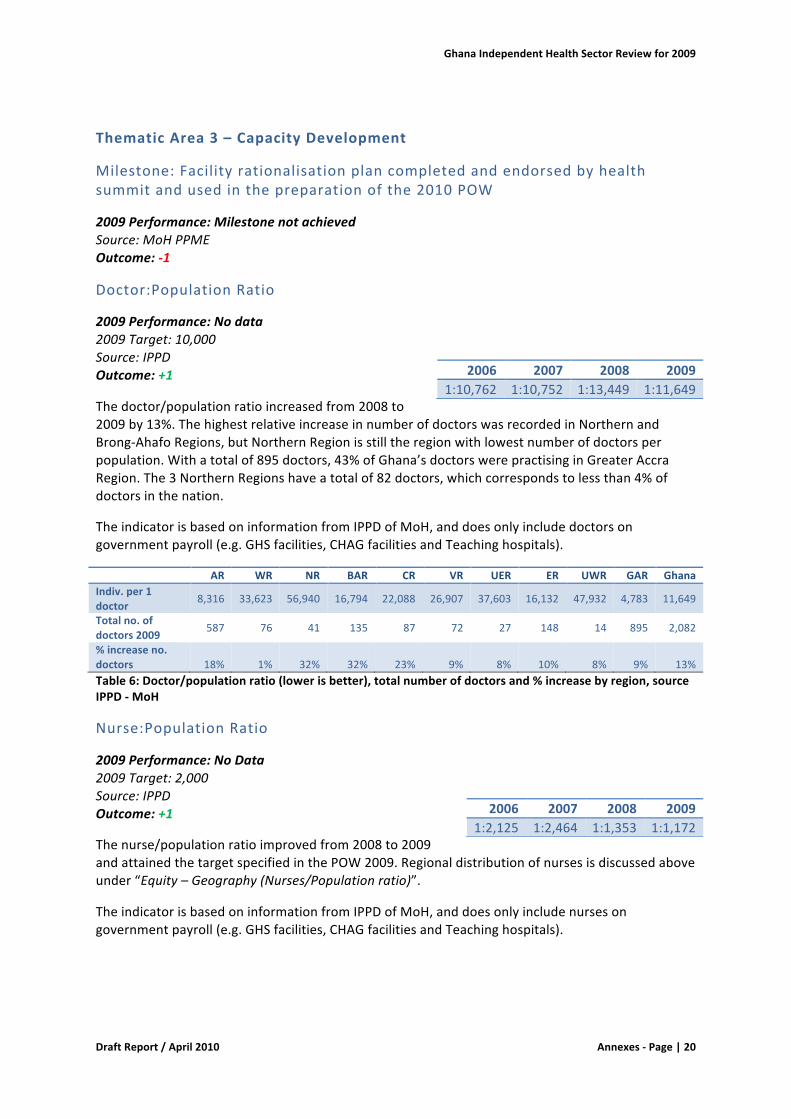
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|20
ThematicArea3–CapacityDevelopment
Milestone:Facilityrationalisationplancompletedandendorsedbyhealthsummitandusedinthepreparationofthe2010POW
2009Performance:MilestonenotachievedSource:MoHPPMEOutcome:-1
Doctor:PopulationRatio
2009Performance:Nodata2009Target:10,000Source:IPPDOutcome:+1
Thedoctor/populationratioincreasedfrom2008to2009by13%.ThehighestrelativeincreaseinnumberofdoctorswasrecordedinNorthernandBrong-AhafoRegions,butNorthernRegionisstilltheregionwithlowestnumberofdoctorsperpopulation.Withatotalof895doctors,43%ofGhana’sdoctorswerepractisinginGreaterAccraRegion.The3NorthernRegionshaveatotalof82doctors,whichcorrespondstolessthan4%ofdoctorsinthenation.
TheindicatorisbasedoninformationfromIPPDofMoH,anddoesonlyincludedoctorsongovernmentpayroll(e.g.GHSfacilities,CHAGfacilitiesandTeachinghospitals).
AR WR NR BAR CR VR UER ER UWR GAR GhanaIndiv.per1doctor 8,316 33,623 56,940 16,794 22,088 26,907 37,603 16,132 47,932 4,783 11,649
Totalno.ofdoctors2009 587 76 41 135 87 72 27 148 14 895 2,082
%increaseno.doctors 18% 1% 32% 32% 23% 9% 8% 10% 8% 9% 13%Table6:Doctor/populationratio(lowerisbetter),totalnumberofdoctorsand%increasebyregion,sourceIPPD-MoH
Nurse:PopulationRatio
2009Performance:NoData2009Target:2,000Source:IPPDOutcome:+1
Thenurse/populationratioimprovedfrom2008to2009andattainedthetargetspecifiedinthePOW2009.Regionaldistributionofnursesisdiscussedaboveunder“Equity–Geography(Nurses/Populationratio)”.
TheindicatorisbasedoninformationfromIPPDofMoH,anddoesonlyincludenursesongovernmentpayroll(e.g.GHSfacilities,CHAGfacilitiesandTeachinghospitals).
2006 2007 2008 20091:10,762 1:10,752 1:13,449 1:11,649
2006 2007 2008 20091:2,125 1:2,464 1:1,353 1:1,172
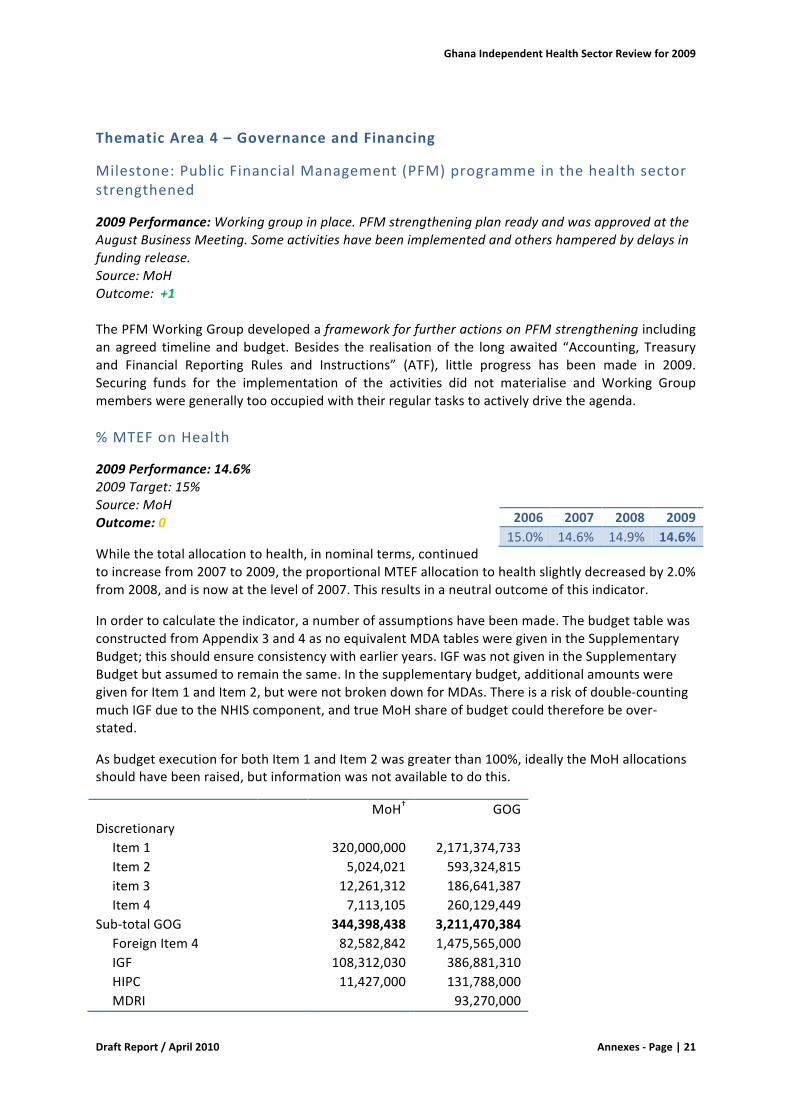
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|21
ThematicArea4–GovernanceandFinancing
Milestone:PublicFinancialManagement(PFM)programmeinthehealthsectorstrengthened
2009Performance:Workinggroupinplace.PFMstrengtheningplanreadyandwasapprovedattheAugustBusinessMeeting.Someactivitieshavebeenimplementedandothershamperedbydelaysinfundingrelease.Source:MoHOutcome:+1ThePFMWorkingGroupdevelopedaframeworkforfurtheractionsonPFMstrengtheningincludingan agreed timeline andbudget. Besides the realisationof the long awaited “Accounting, Treasuryand Financial Reporting Rules and Instructions” (ATF), little progress has been made in 2009.Securing funds for the implementation of the activities did not materialise and Working Groupmembersweregenerallytoooccupiedwiththeirregulartaskstoactivelydrivetheagenda.%MTEFonHealth
2009Performance:14.6%2009Target:15%Source:MoHOutcome:0
Whilethetotalallocationtohealth,innominalterms,continuedtoincreasefrom2007to2009,theproportionalMTEFallocationtohealthslightlydecreasedby2.0%from2008,andisnowatthelevelof2007.Thisresultsinaneutraloutcomeofthisindicator.
Inordertocalculatetheindicator,anumberofassumptionshavebeenmade.ThebudgettablewasconstructedfromAppendix3and4asnoequivalentMDAtablesweregivenintheSupplementaryBudget;thisshouldensureconsistencywithearlieryears.IGFwasnotgivenintheSupplementaryBudgetbutassumedtoremainthesame.Inthesupplementarybudget,additionalamountsweregivenforItem1andItem2,butwerenotbrokendownforMDAs.Thereisariskofdouble-countingmuchIGFduetotheNHIScomponent,andtrueMoHshareofbudgetcouldthereforebeover-stated.
AsbudgetexecutionforbothItem1andItem2wasgreaterthan100%,ideallytheMoHallocationsshouldhavebeenraised,butinformationwasnotavailabletodothis.
MoH† GOGDiscretionary Item1 320,000,000 2,171,374,733 Item2 5,024,021 593,324,815 item3 12,261,312 186,641,387 Item4 7,113,105 260,129,449Sub-totalGOG 344,398,438 3,211,470,384 ForeignItem4 82,582,842 1,475,565,000 IGF 108,312,030 386,881,310 HIPC 11,427,000 131,788,000 MDRI 93,270,000
2006 2007 2008 200915.0% 14.6% 14.9% 14.6%
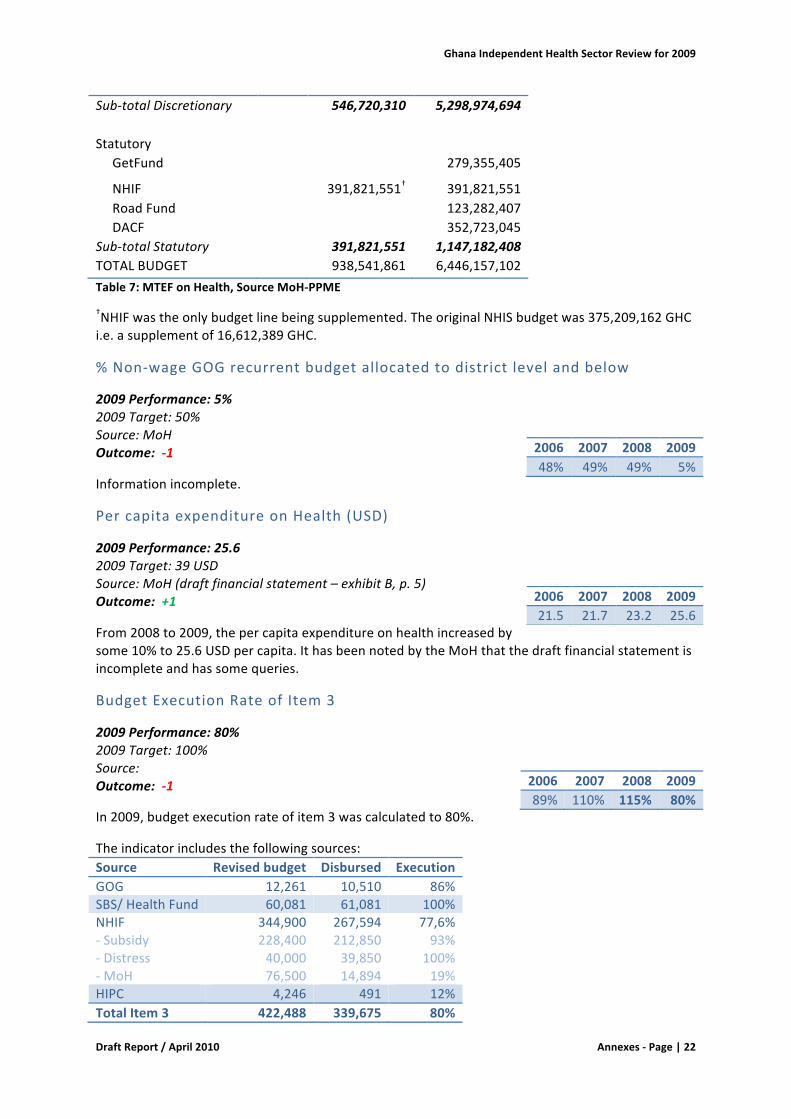
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|22
Sub-totalDiscretionary 546,720,310 5,298,974,694 Statutory GetFund 279,355,405
NHIF 391,821,551† 391,821,551 RoadFund 123,282,407 DACF 352,723,045Sub-totalStatutory 391,821,551 1,147,182,408TOTALBUDGET 938,541,861 6,446,157,102Table7:MTEFonHealth,SourceMoH-PPME
†NHIFwastheonlybudgetlinebeingsupplemented.TheoriginalNHISbudgetwas375,209,162GHCi.e.asupplementof16,612,389GHC.
%Non-wageGOGrecurrentbudgetallocatedtodistrictlevelandbelow
2009Performance:5%2009Target:50%Source:MoHOutcome:-1
Informationincomplete.
PercapitaexpenditureonHealth(USD)
2009Performance:25.62009Target:39USDSource:MoH(draftfinancialstatement–exhibitB,p.5)Outcome:+1
From2008to2009,thepercapitaexpenditureonhealthincreasedbysome10%to25.6USDpercapita.IthasbeennotedbytheMoHthatthedraftfinancialstatementisincompleteandhassomequeries.
BudgetExecutionRateofItem3
2009Performance:80%2009Target:100%Source:Outcome:-1
In2009,budgetexecutionrateofitem3wascalculatedto80%.
Theindicatorincludesthefollowingsources:Source Revisedbudget Disbursed ExecutionGOG 12,261 10,510 86%SBS/HealthFund 60,081 61,081 100%NHIF-Subsidy-Distress-MoH
344,900228,40040,00076,500
267,594212,85039,85014,894
77,6%93%
100%19%
HIPC 4,246 491 12%TotalItem3 422,488 339,675 80%
2006 2007 2008 200948% 49% 49% 5%
2006 2007 2008 200921.5 21.7 23.2 25.6
2006 2007 2008 200989% 110% 115% 80%
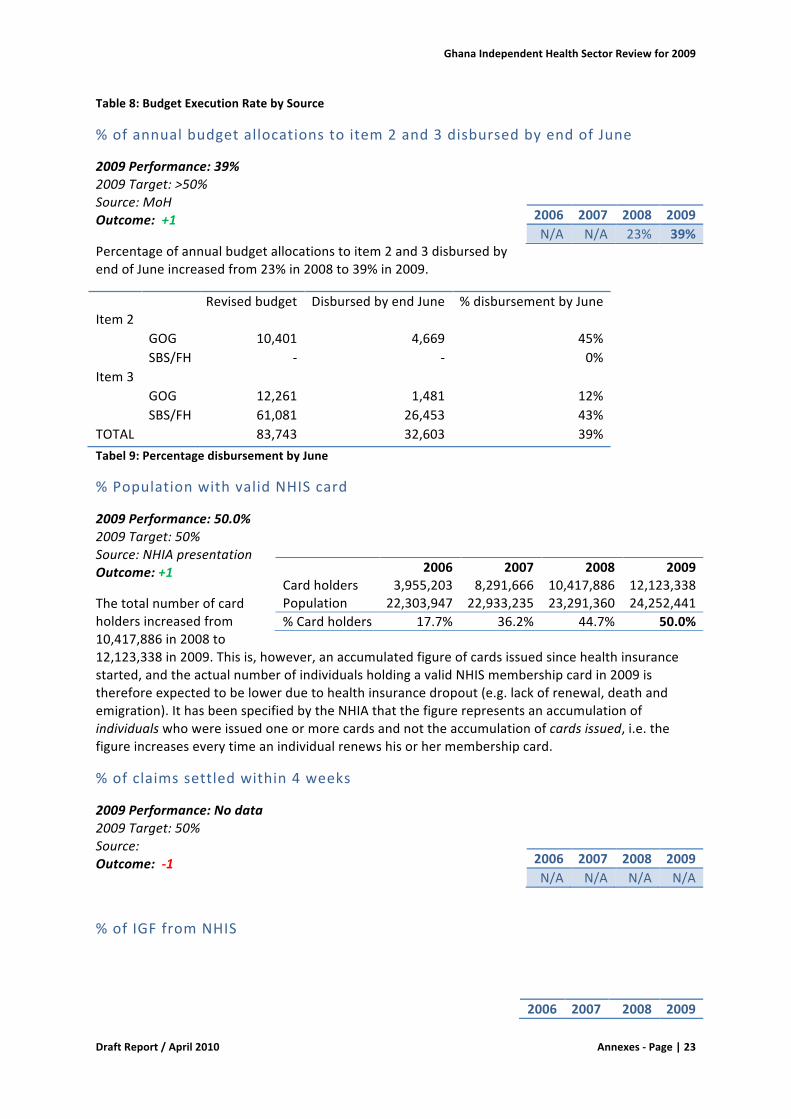
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|23
Table8:BudgetExecutionRatebySource
%ofannualbudgetallocationstoitem2and3disbursedbyendofJune
2009Performance:39%2009Target:>50%Source:MoHOutcome:+1
Percentageofannualbudgetallocationstoitem2and3disbursedbyendofJuneincreasedfrom23%in2008to39%in2009.
Revisedbudget DisbursedbyendJune %disbursementbyJuneItem2 GOG 10,401 4,669 45% SBS/FH - - 0%Item3 GOG 12,261 1,481 12% SBS/FH 61,081 26,453 43%TOTAL 83,743 32,603 39%Tabel9:PercentagedisbursementbyJune
%PopulationwithvalidNHIScard
2009Performance:50.0%2009Target:50%Source:NHIApresentationOutcome:+1
Thetotalnumberofcardholdersincreasedfrom10,417,886in2008to12,123,338in2009.Thisis,however,anaccumulatedfigureofcardsissuedsincehealthinsurancestarted,andtheactualnumberofindividualsholdingavalidNHISmembershipcardin2009isthereforeexpectedtobelowerduetohealthinsurancedropout(e.g.lackofrenewal,deathandemigration).IthasbeenspecifiedbytheNHIAthatthefigurerepresentsanaccumulationofindividualswhowereissuedoneormorecardsandnottheaccumulationofcardsissued,i.e.thefigureincreaseseverytimeanindividualrenewshisorhermembershipcard.
%ofclaimssettledwithin4weeks
2009Performance:Nodata2009Target:50%Source:Outcome:-1
%ofIGFfromNHIS
2006 2007 2008 2009N/A N/A 23% 39%
2006 2007 2008 2009Cardholders 3,955,203 8,291,666 10,417,886 12,123,338Population 22,303,947 22,933,235 23,291,360 24,252,441%Cardholders 17.7% 36.2% 44.7% 50.0%
2006 2007 2008 2009N/A N/A N/A N/A
2006 2007 2008 2009
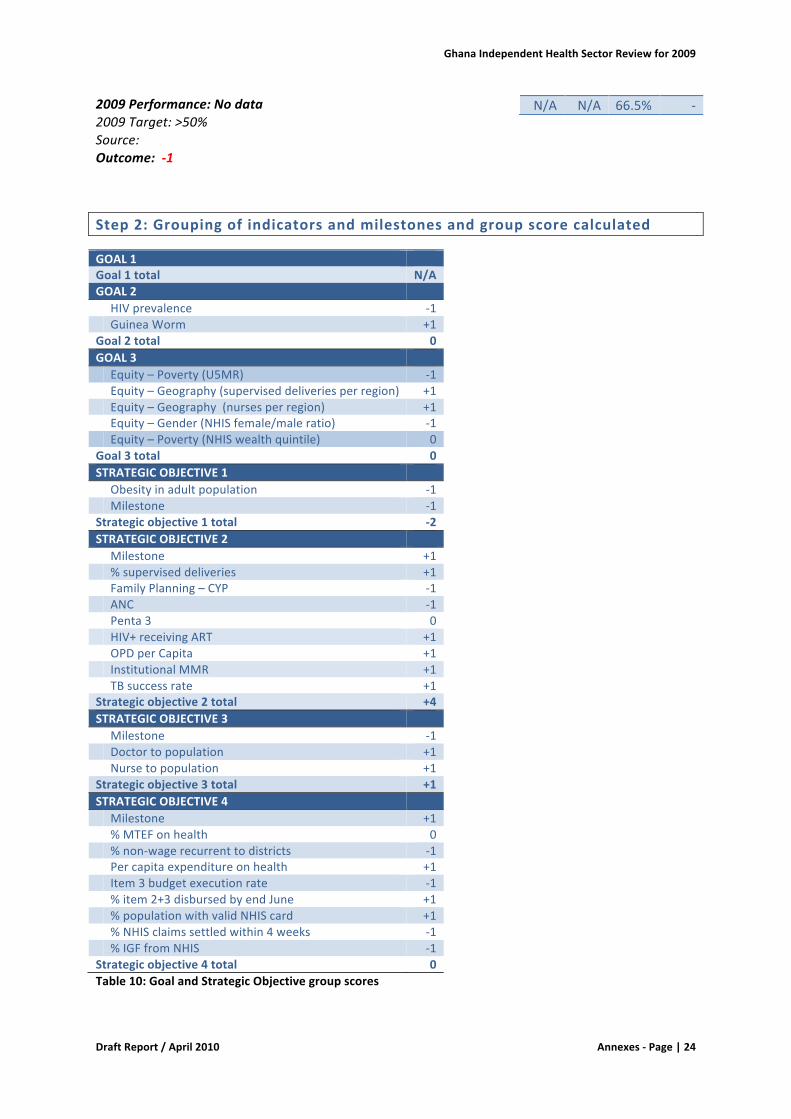
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|24
2009Performance:Nodata2009Target:>50%Source:Outcome:-1
Step2:Groupingofindicatorsandmilestonesandgroupscorecalculated
GOAL1 Goal1total N/AGOAL2 HIVprevalence -1 GuineaWorm +1Goal2total 0GOAL3 Equity–Poverty(U5MR) -1 Equity–Geography(superviseddeliveriesperregion) +1 Equity–Geography(nursesperregion) +1 Equity–Gender(NHISfemale/maleratio) -1 Equity–Poverty(NHISwealthquintile) 0Goal3total 0STRATEGICOBJECTIVE1 Obesityinadultpopulation -1 Milestone -1Strategicobjective1total -2STRATEGICOBJECTIVE2 Milestone +1 %superviseddeliveries +1 FamilyPlanning–CYP -1 ANC -1 Penta3 0 HIV+receivingART +1 OPDperCapita +1 InstitutionalMMR +1 TBsuccessrate +1Strategicobjective2total +4STRATEGICOBJECTIVE3 Milestone -1 Doctortopopulation +1 Nursetopopulation +1Strategicobjective3total +1STRATEGICOBJECTIVE4 Milestone +1 %MTEFonhealth 0 %non-wagerecurrenttodistricts -1 Percapitaexpenditureonhealth +1 Item3budgetexecutionrate -1 %item2+3disbursedbyendJune +1 %populationwithvalidNHIScard +1 %NHISclaimssettledwithin4weeks -1 %IGFfromNHIS -1Strategicobjective4total 0Table10:GoalandStrategicObjectivegroupscores
N/A N/A 66.5% -
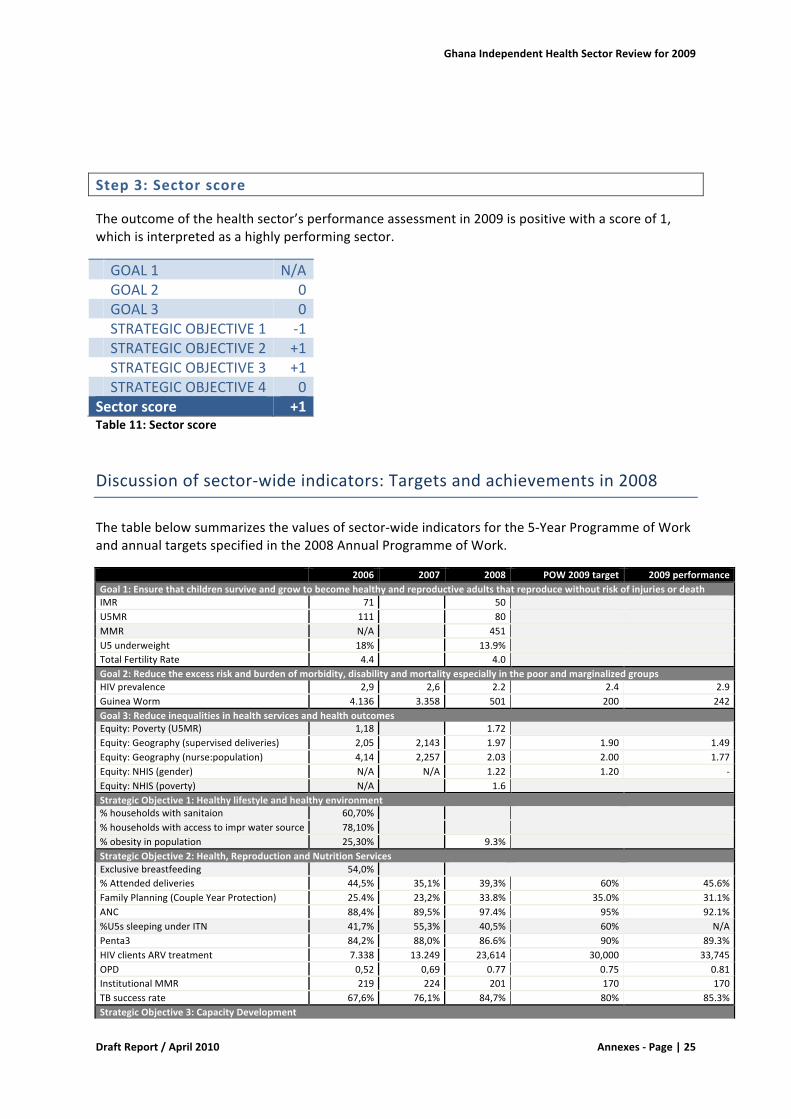
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|25
Step3:Sectorscore
Theoutcomeofthehealthsector’sperformanceassessmentin2009ispositivewithascoreof1,whichisinterpretedasahighlyperformingsector.
GOAL1 N/A GOAL2 0 GOAL3 0 STRATEGICOBJECTIVE1 -1 STRATEGICOBJECTIVE2 +1 STRATEGICOBJECTIVE3 +1 STRATEGICOBJECTIVE4 0Sectorscore +1Table11:Sectorscore
Discussionofsector-wideindicators:Targetsandachievementsin2008
Thetablebelowsummarizesthevaluesofsector-wideindicatorsforthe5-YearProgrammeofWorkandannualtargetsspecifiedinthe2008AnnualProgrammeofWork.
2006 2007 2008 POW2009target 2009performanceGoal1:EnsurethatchildrensurviveandgrowtobecomehealthyandreproductiveadultsthatreproducewithoutriskofinjuriesordeathIMR 71 50 U5MR 111 80 MMR N/A 451 U5underweight 18% 13.9% TotalFertilityRate 4.4 4.0 Goal2:Reducetheexcessriskandburdenofmorbidity,disabilityandmortalityespeciallyinthepoorandmarginalizedgroupsHIVprevalence 2,9 2,6 2.2 2.4 2.9GuineaWorm 4.136 3.358 501 200 242Goal3:ReduceinequalitiesinhealthservicesandhealthoutcomesEquity:Poverty(U5MR) 1,18 1.72 Equity:Geography(superviseddeliveries) 2,05 2,143 1.97 1.90 1.49Equity:Geography(nurse:population) 4,14 2,257 2.03 2.00 1.77Equity:NHIS(gender) N/A N/A 1.22 1.20 -Equity:NHIS(poverty) N/A 1.6 StrategicObjective1:Healthylifestyleandhealthyenvironment%householdswithsanitaion 60,70% %householdswithaccesstoimprwatersource 78,10% %obesityinpopulation 25,30% 9.3% StrategicObjective2:Health,ReproductionandNutritionServicesExclusivebreastfeeding 54,0% %Attendeddeliveries 44,5% 35,1% 39,3% 60% 45.6%FamilyPlanning(CoupleYearProtection) 25.4% 23,2% 33.8% 35.0% 31.1%ANC 88,4% 89,5% 97.4% 95% 92.1%%U5ssleepingunderITN 41,7% 55,3% 40,5% 60% N/APenta3 84,2% 88,0% 86.6% 90% 89.3%HIVclientsARVtreatment 7.338 13.249 23,614 30,000 33,745OPD 0,52 0,69 0.77 0.75 0.81InstitutionalMMR 219 224 201 170 170TBsuccessrate 67,6% 76,1% 84,7% 80% 85.3%StrategicObjective3:CapacityDevelopment
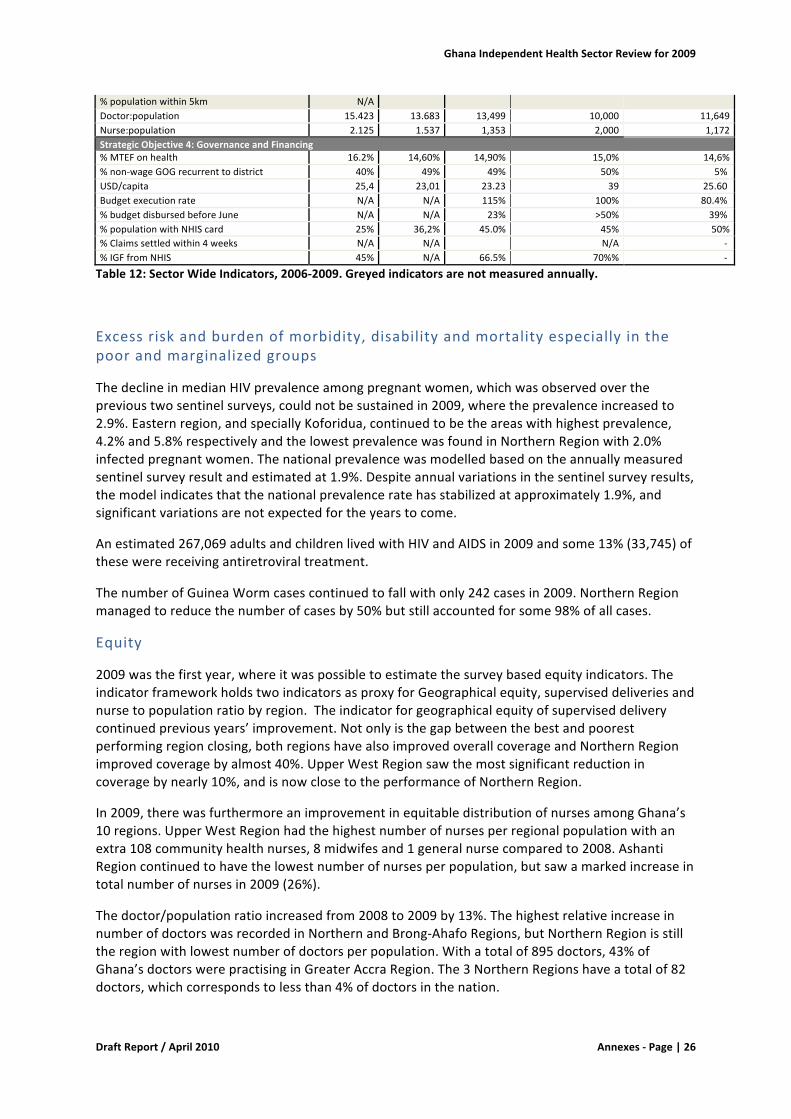
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|26
%populationwithin5km N/A Doctor:population 15.423 13.683 13,499 10,000 11,649Nurse:population 2.125 1.537 1,353 2,000 1,172StrategicObjective4:GovernanceandFinancing%MTEFonhealth 16.2% 14,60% 14,90% 15,0% 14,6%%non-wageGOGrecurrenttodistrict 40% 49% 49% 50% 5%USD/capita 25,4 23,01 23.23 39 25.60Budgetexecutionrate N/A N/A 115% 100% 80.4%%budgetdisbursedbeforeJune N/A N/A 23% >50% 39%%populationwithNHIScard 25% 36,2% 45.0% 45% 50%%Claimssettledwithin4weeks N/A N/A N/A -%IGFfromNHIS 45% N/A 66.5% 70%% -
Table12:SectorWideIndicators,2006-2009.Greyedindicatorsarenotmeasuredannually.
Excessriskandburdenofmorbidity,disabilityandmortalityespeciallyinthepoorandmarginalizedgroups
ThedeclineinmedianHIVprevalenceamongpregnantwomen,whichwasobservedovertheprevioustwosentinelsurveys,couldnotbesustainedin2009,wheretheprevalenceincreasedto2.9%.Easternregion,andspeciallyKoforidua,continuedtobetheareaswithhighestprevalence,4.2%and5.8%respectivelyandthelowestprevalencewasfoundinNorthernRegionwith2.0%infectedpregnantwomen.Thenationalprevalencewasmodelledbasedontheannuallymeasuredsentinelsurveyresultandestimatedat1.9%.Despiteannualvariationsinthesentinelsurveyresults,themodelindicatesthatthenationalprevalenceratehasstabilizedatapproximately1.9%,andsignificantvariationsarenotexpectedfortheyearstocome.
Anestimated267,069adultsandchildrenlivedwithHIVandAIDSin2009andsome13%(33,745)ofthesewerereceivingantiretroviraltreatment.
ThenumberofGuineaWormcasescontinuedtofallwithonly242casesin2009.NorthernRegionmanagedtoreducethenumberofcasesby50%butstillaccountedforsome98%ofallcases.
Equity
2009wasthefirstyear,whereitwaspossibletoestimatethesurveybasedequityindicators.TheindicatorframeworkholdstwoindicatorsasproxyforGeographicalequity,superviseddeliveriesandnursetopopulationratiobyregion.Theindicatorforgeographicalequityofsuperviseddeliverycontinuedpreviousyears’improvement.Notonlyisthegapbetweenthebestandpoorestperformingregionclosing,bothregionshavealsoimprovedoverallcoverageandNorthernRegionimprovedcoveragebyalmost40%.UpperWestRegionsawthemostsignificantreductionincoveragebynearly10%,andisnowclosetotheperformanceofNorthernRegion.
In2009,therewasfurthermoreanimprovementinequitabledistributionofnursesamongGhana’s10regions.UpperWestRegionhadthehighestnumberofnursesperregionalpopulationwithanextra108communityhealthnurses,8midwifesand1generalnursecomparedto2008.AshantiRegioncontinuedtohavethelowestnumberofnursesperpopulation,butsawamarkedincreaseintotalnumberofnursesin2009(26%).
Thedoctor/populationratioincreasedfrom2008to2009by13%.ThehighestrelativeincreaseinnumberofdoctorswasrecordedinNorthernandBrong-AhafoRegions,butNorthernRegionisstilltheregionwithlowestnumberofdoctorsperpopulation.Withatotalof895doctors,43%ofGhana’sdoctorswerepractisinginGreaterAccraRegion.The3NorthernRegionshaveatotalof82doctors,whichcorrespondstolessthan4%ofdoctorsinthenation.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|27
TheequityindicatorsforpovertyareU5MRandNHIScardholders,bywealthquintile.Theequityindicatorforpoverty(U5MR)wasmeasuredbasedontheDHS2008.ThehighestU5MRwasreportedamongthelowestwealthquintilewith103deathsoutof1,000livebirths,whereasthelowestmortalitywasobservedamongthehighestwealthquintile.Theequityindicatorisestimatedat1.72.Since2003,GhanahasseenasignificantreductionofU5MRnationwideforallwealthquintiles;however,thereductioninU5MRhasbeengreaterinthehighestwealthquintilecomparetothelowest.Therefore,thedistributionofU5MRbywealthhasbecomeincreasinglyunequal.TheNHISCardHolderratiobywealthquintilewasmeasuredforthefirsttimebasedontheDHS2008results.Thecalculationshowsthatsignificantlymoreindividualsbelongingtothehighestwealthquintileregistercomparedtothelowestquintile.Thisisespeciallyevidentforthemalepopulation.
Healthylifestyleandhealthyenvironment
Obesity(BMI≥30)amongwomenaged15-49increasedby15%from2003to2008,andwhilealmost10%ofthefemalepopulation15-49areobeseover20%areoverweight.With19.4%ofwomenintheagegroupbeingobeseand25.1%overweight,GreaterAccraRegionhadsignificantlyhigherprevalenceofobesityandoverweightthananyotherregion.Westernregionhadthesecondhighestprevalenceofobesityestimatedat9.9%.UpperWestandNorthernRegionhadthelowestprevalencewith2.4%obese,aswellas10.3%and11.5%overweight,respectively.ComparedtotheDHS2003survey,obesityhasincreasedby15%from8.1%to9.3%inthefemalepopulationaged15-49years.
Themilestonespecifiedinthe5YPOWforimprovementofhealthylifestyleandenvironmentrelatedtothedevelopmentofaninformationdocumentandcommunicationstrategytopreventNCDs.Thismilestonewasnotrealised.
ProvisionofHealth,ReproductionandNutritionServices
Mosthealthserviceindicatorsexperiencedasignificantpositivetrendfrom2008to2009.InaccordancewiththetargetsforimprovedmaternalandneonatalhealthsetoutinthePOW2009,theindicatorsforsuperviseddeliveriesandinstitutionalMMRimproved.
From2008to2009,thecoverageofpregnantwomen,whoreceivedoneormoreantenatalcarevisits,droppedby5.4%.Inthesameperiod,theproportionofpregnantwomenwhoreceived4ormorevisitsincreasedsignificantlyfrom63.8%to81.6%.Thisindicatesthatthemajority(almost90%)ofwomennowfollowtherecommendedANCcourseofminimum4visits,whichcanbeinterpretedasanoverallimprovementofantenatalservicesinthecountry.
Theproportionofdeliveriesattendedbyatrainedhealthworkerincreasedby17%,andhencecontinuedthepositivetrendexperiencedsince2007.TheDHS2008estimatedthepercentagesomewhathigherat58.7%.AdeeperanalysisoftheDHS2008datarevealsthattherewerelargeregionalvariationsintheindicator.InGreaterAccraRegion84.3%deliverieswereattendedbyskilledprovider,whileonly27.2%wereattendedbyskilledproviderinNorthernRegion.AlsotheroutinehealthinformationindicatesthatNorthernRegionperformedrelativelypoorerthanotherregions,theregiondidhoweverachievemajorimprovementofthisindicatorbyalmost40%from2008to2009.
TheinstitutionalMMRcontinuedthepositivetrend,andwasreducedby15%from2008to2009.Almostallregionsachievedimprovementofthisindicator,butinUpperWestRegiontherewasaseriousincreaseintheMMRby145%from109to267per100,000livebirths.Thetotalnumberofmaternaldeathsrecordedintheregionincreasedfrom19to41.
From2008to2009,contraceptiveprevalenceratedroppedby8%.Whilelongtermcoupleyearsofprotection(CYP)remainedataround142,000,shorttermCYPdroppedby33%from654,072in2008
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|28
to439,573in2009.TheindicatortrendcorrespondswellwithinformationpresentedtothereviewteamconcerningageneralshortageofshorttermmethodsinGhanaduringthepreviousyear.Thesocialmarketedbrandsofcondoms,e.g.GhanaSocialMarketingFoundationbrand,whichin2008constitutedmorethanhalfofallcondomssoldinGhana,havereportedlybeeninparticularshortagein2009.
AfteraslightdropinPenta3coveragein2008,performanceisnowbackontrack,almostreachingthetargetof90%coverage.TheDHS2008estimatedthepercentageofPenta3at87.7%,whichcorrespondswellwithroutinelycollecteddata.AregionalbreakdownoftheroutinedataindicatesthatcoverageinGreaterAccraRegionissignificantlowerthatthenationalcoverage.ThiscouldnotbeconfirmedbyanEPIsurveyfrom2009,whichwasperformedinGreaterAccraRegionandshowedsignificantlyhighercoverageofPenta3at96.1%.
Outpatient(OPD)visitspercapitacontinuedpreviousyears’increaseandreachedthe2009target.WhileeveryinhabitantofBrongAhafoRegioninaveragevisitstheoutpatientdepartment1.15timesayear,peopleofGreaterAccraandNorthernRegionhaveanaverageutilisationofOPDserviceslessthanhalfofBrongAhafoRegion.AbsolutefiguresforOPDvisitsshow,thatAshantiRegionhasthehighestload,followedbyBrongAhafoRegion.GreatAccraRegioncomes5thdespiteitshighregionalpopulation.
GovernanceandFinancing
Thetotalnumberofcardholdersincreasedfrom10,417,886in2008to12,123,338in2009.Thisis,however,anaccumulatedfigureofcardsissuedsincehealthinsurancestarted,andtheactualnumberofindividualsholdingavalidNHISmembershipcardin2009isthereforeexpectedtobelowerduetohealthinsurancedropout(e.g.lackofrenewal,deathandemigration).IthasbeenspecifiedbytheNHIAthatthefigurerepresentsanaccumulationofindividualswhowereissuedoneormorecardsandnottheaccumulationofcardsissued,i.e.thefigureincreaseseverytimeanindividualrenewshisorhermembershipcard.
HolisticassessmentoftheHealthSectorperformancein2009
In2008,theHolisticAssessmentwasintroducedaspartoftheannualhealthsectorreviewtoprovideastructuredandtransparentmethodologytoassessprogressinachievingtheobjectivesofthePOW2007-2011.
Theconclusionoftheholisticassessmentisthatthehealthsectorin2009washighlyperforming,withasectorscoreof+1.Servicedeliveryindicators(StrategicObjective2)andcapacityimprovementindicators(StrategicObjective3)weregenerallyimproving,whileindicatorsonhealthylifestyle(StrategicObjective1)wereworsening.TheindicatorsforGoal1(reductionofexcessriskandburdenofmorbidity,disabilityandmortalityespeciallyinthepoorandmarginalizedgroups),Goal2(reductionofinequalitiesinhealthservicesandhealthoutcomes)andStrategicobjective4(GovernanceandFinancing)didneitherexperiencesignificantoverallimprovementnordeterioration.
Whilethesectorscoreremainedpositivewithascoreof+1for2009,thesectorscorefor2008wassignificantlyhigherat+4.Thiscouldbeinterpretedaswaningofthepositivetrendsexperiencedin2008,butsuchananalysishasafewcaveats.Notallindicatorsaremeasuredallyears,sothesameindicators,goalsandstrategicobjectivesarenotnecessarilymeasuredyearonyear.Therefore,comparingyearswouldbeanattempttomeasureamovingtarget.Anotherissueisthattheholisticassessmentdoesnotassignanyweighttoindicators,i.e.thescorecanbehighinayearwithworseningtrendofanumberofmoreimportantindicators’trendaslongasthemajorityof(lessimportant)indicators’trendsarepositive.
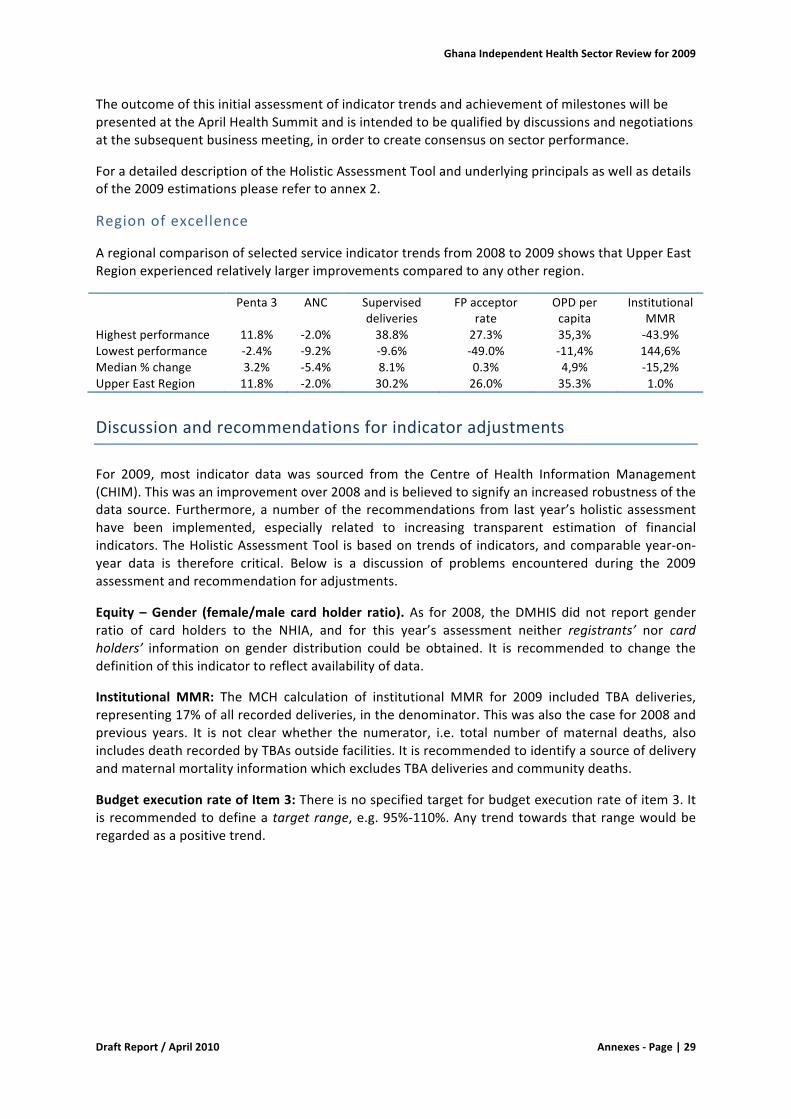
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|29
TheoutcomeofthisinitialassessmentofindicatortrendsandachievementofmilestoneswillbepresentedattheAprilHealthSummitandisintendedtobequalifiedbydiscussionsandnegotiationsatthesubsequentbusinessmeeting,inordertocreateconsensusonsectorperformance.
ForadetaileddescriptionoftheHolisticAssessmentToolandunderlyingprincipalsaswellasdetailsofthe2009estimationspleaserefertoannex2.
Regionofexcellence
Aregionalcomparisonofselectedserviceindicatortrendsfrom2008to2009showsthatUpperEastRegionexperiencedrelativelylargerimprovementscomparedtoanyotherregion.
Penta3 ANC Superviseddeliveries
FPacceptorrate
OPDpercapita
InstitutionalMMR
Highestperformance 11.8% -2.0% 38.8% 27.3% 35,3% -43.9%Lowestperformance -2.4% -9.2% -9.6% -49.0% -11,4% 144,6%Median%change 3.2% -5.4% 8.1% 0.3% 4,9% -15,2%UpperEastRegion 11.8% -2.0% 30.2% 26.0% 35.3% 1.0%
Discussionandrecommendationsforindicatoradjustments
For 2009, most indicator data was sourced from the Centre of Health InformationManagement(CHIM).Thiswasanimprovementover2008andisbelievedtosignifyanincreasedrobustnessofthedata source. Furthermore, anumberof the recommendations from last year’sholistic assessmenthave been implemented, especially related to increasing transparent estimation of financialindicators.TheHolisticAssessmentTool isbasedontrendsof indicators,andcomparableyear-on-year data is therefore critical. Below is a discussion of problems encountered during the 2009assessmentandrecommendationforadjustments.
Equity –Gender (female/male card holder ratio).As for 2008, theDMHIS did not report genderratio of card holders to the NHIA, and for this year’s assessment neither registrants’ nor cardholders’ information on gender distribution could be obtained. It is recommended to change thedefinitionofthisindicatortoreflectavailabilityofdata.
Institutional MMR: The MCH calculation of institutional MMR for 2009 included TBA deliveries,representing17%ofallrecordeddeliveries,inthedenominator.Thiswasalsothecasefor2008andprevious years. It is not clearwhether the numerator, i.e. total number ofmaternal deaths, alsoincludesdeathrecordedbyTBAsoutsidefacilities.ItisrecommendedtoidentifyasourceofdeliveryandmaternalmortalityinformationwhichexcludesTBAdeliveriesandcommunitydeaths.
BudgetexecutionrateofItem3:Thereisnospecifiedtargetforbudgetexecutionrateofitem3.Itis recommendedtodefineatargetrange,e.g.95%-110%.Anytrendtowardsthatrangewouldberegardedasapositivetrend.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|30
AnnexA:Definitionsandcalculationsfor2009assessment
Indicator
Numerator
Denominator
Source
Calculation2009
HIVPrevalenceamongpregnantwomen15-24years
N/A
N/A
NationalAIDSControlProgramme.SentinelSurveillancereport.
Calculationwasdoneintheannualsentinelsurveyreport.
IncidenceofGuineaWorm
Newcases
N/A
CHIM
N/A
EquityIndex:Pov
U5MRamon
U5MRam
DHS2008
103/60
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|31
erty(Richest/PoorestU5mortalityrate)
gchildrenoflowestwealthquintile
ongchildrenofhighestwealthquintile
EquityIndex:Geography(superviseddeliveries)
Proportionofdeliveriesattendedbyatrainedhealthworkerinbestperformingregion
Proportionofdeliveriesattendedbyatrainedhealthworkerinpoorestperformin
CHIM
33,714/93,382
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|32
gregion
EquityIndex:Geography(nurses:population)
Numberofnursesbytotalpopulationinbestperformingregion
Numberofnursesbytotalpopulationinpoorestperformingregion
IPPD–MinistryofHealth.PopulationdatafromCHIM
2,442/4,881,428
EquityIndex:Gender(NHISregistration)
NumberofwomenregisteredwithNHIS
NumberofmenregisteredwithNHIS
NHIA
N/A
Equity
%NH
%N
DHS
37.7%/16.6%
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|33
Index:Poverty(NHISregistration)
IScardholdersamonghighestwealthquintile
HIScardholdersamonglowestwealthquintile
2008
%deliveriesattendedbyatrainedhealthworker
Nationalnumberofdeliveriessupervisedbytrainedhealthworker
Nationalnumberofexpecteddeliveries
MaternalandChildHealthUnitannualreport
442,766/970,097
Contracepti
New+
Target
MCH
1,811,777/5,820,585

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|34
vePrevalenceRate
continuingFPacceptors
population(0.24xtotalpopulation)
spreadsheet
Antenatalcarecoverage
NumberofpregnantwomenregisteredtoreceivedANC
Expectednumberofpregnancies
MCHspreadsheet/CHIM
893,747/970,097
Antenatalcarecoverage
Numberofpregnantwomenwith4ormo
Expectednumberofpregnancies
MCHspreadsheet/CHIM
729,403/970,097
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|35
reANCvisits
%U5ssleepingunderITNs
NumberofsurveyedU5ssleepingunderITNthepreviousnight
Numberofsurveyedchildren
N/A
N/A
%ChildrenreceivingPenta3
NumberofchildrenwhoreceivedPenta3
Expectednumberofchildren0-12months
CHIM
Notspecified.CalculationdonebyCHIM.
HIVposi
HIV
N/A
NAC
N/A
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|36
tiveindividualsreceivingART
positiveindividualsreceivingART
Pannualreport
Outpatientattendancepercapita
NumberofOPDencounters(GHS,CHAG,TeachingHospitals)
TotalpopulationprovidedbyCHIM-GHS
CHIM–GhanaHealthService
19,747,839/24,252,441
InstitutionalMaternalMortalityRatio
Numberofmaternaldeathsatgovernmen
Numberoflivebirthsingovernm
MCHSpreadsheet
889/523,110(MCHcalculationincludingTBAdeliveries)
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|37
tandCHAGinstitutions,excludingTBAdeliveries
entandCHAGinstitutions,excludingTBAdeliveries
TBsuccessrate
NumberofpatientsproventobecuredofTBaftercompletionoftherapy
Numberofpatientcommencinganti-TBtherapy
NationalTBProgrammeannualreport
RateprovidedbyNTP
Doctor:Pop
Number
Totalpo
IPPD
1,835/24,252,441
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|38
ulationratio
ofdoctorsregisteredatIPPD/MoH
pulationprovidedbyCHIM
–MoH.PopulationdatafromCHIM
Nurse:Populationratio
NumberofnursesregisteredatIPPD/MoH
TotalpopulationprovidedbyCHIM
IPPD–MoH.PopulationdatafromCHIM
17,427/24,252,441
%totalMTEFonHealth
MTEFallocatedtohealth.Sources:GO
TotalMTEFforGOG
Currentyear’sGOGAnnualBu
6,446,157,102
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|39
G+Donor+IGF+HIPC+NHIS
dgetStatement
%non-wageGOGrecurrentbudgetallocatedtodistrictlevelandbelow
PerCapitaExpenditureonHealth
TotalexpenditureonhealthinUSD,exchan
TotalpopulationprovidedbyCHIM-GHS
MoHFinancialStatements.Populatio
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|40
geratefromBankofGhanaper01.07.2008
ndatafromCHIM
BudgetExecutionRateofItem3
Item3disbursementsfromGOG+SBS+HF+HIPC+NHIS(subsidies+distress+MoHalloc
POWitem3budget(samesources).
PPME–MoH
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|41
ation)
%ofannualbudgetallocationstoitems2and3disbursedbyendofJune
Disbursementsforitem2and3byendofJune.Sources:GOGandSBS.
Totalbudgetallocationsforitem2and3(samesources)
PPME–MoH
%PopulationwithvalidNHISMembership
TotalnumberofactiveNHISmembers(validNHIScardholders)
TotalpopulationprovidedbyCHIM-GHS
NHIAannualreport.PopulationdatafromCHIM
24,252,441
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|42
Proportionofclaimssettledwithin4weeks
Numberofclaimsreimbursed(disbursedfromDMHISaccounts)within4weeksofreceptionbyDMHIS
TotalnumberofclaimsreceivedbyDMHIS
NHIAannualreport.
N/A
%IGFfromNHIS
TotalclaimsamountpaidbyDM
TotalIGF
NHIAannualreport.MoHfin
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|43
HIS ancialstatements.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|44
Annex3.MidTermDeskReviewPOW2007-2011
Introduction
TheMinistryofHealthanditsDevelopmentPartnersdecidedtoletthemediumtermreviewofthehealthsectorprogrammeofwork2007–2011coincidewiththeannualindependentreviewofthePOW2009.
TheannualreviewprovidesanindepthanalysisofprogressagainstthePOW2009,thatinitselfcanbeseenasacontinuationofthepreviousannualPOWsbuildingonandadjustingaccordingtothetwopreviousannualreviewsandtheirrecommendations.ItwillprovidesomeinsightintotheprogressionagainstthefiveyearPOWobjectivesandmilestonesand,assuch,ispartofacumulativeprocess.Themediumtermreview,however,willtakeadifferentpointofdeparture.ItsetsouttocomparethesubsequentPOWswiththesubsequentreviewstoanalysewhetherandinwhichwayperceivedandactualprioritieshavebeentakenforwardfromoneplantotheother,asevidencedinthevariousreviews.Itwillthereforeattempttomeasureprocessandnotprogressorachievementsthat,asearliermentionedarethesubjectsoftheannualindependentreviewsandwhereto,ifapplicable,referencewillbemade.
Themediumtermreviewishencelimitedinscopeandrestrictedtoadeskreviewofthedifferentdocumentssince2007andtriestocomplementthevariousannualreviews.
TheHealthSectorProgrammeofWork2007-2011;CreatingWealththroughHealth
2009-2010marksthemidpointofthisProgrammeofWork.Thetitleoftheworkprogramme,“Creatingwealththroughhealth”,placesthehealthsectorwithintheoverallnationaldevelopmentagendaasfollows:
• Improvingthehealthofthepopulace,particularlythroughpreventionandpromotionleadstosavingsintimeandmoneyspentonhealthcare
• ImprovinghealthimprovesproductivityincurrentgenerationofworkersandimprovedIQandlearninginchildrenandhenceproductivityinfuturegeneration
• CreatingJobswithinthehealthsectorcouldleadto(i)economicempowermentofemployees,(ii)importsubstitutionandreductionintheuseofscarceforeignexchangeearningsforimporteddrugsand(iii)generationofforeignexchangethroughtheexportofstandardizedqualityproducts.
WhiletakingcognisanceoftheMillenniumDevelopmentGoalstheprogrammederivesitsobjectivesfromthe“physiologicalfactthattheprimarycauseofdiseaseisnotthebacteriaorvirus,buttheweakenedresistancebroughtaboutbyhealthdestroyinglivinghabits,physicalandemotionalstress,ageingandenvironmentalsanitation”.Thereforethestrategicapproachdefinesfourthemes:
• Healthylifestylesandhealthyenvironments• Health,reproductionandnutritionservices• Capacityforhealthdevelopment• Governanceandfinancing
Withinthenationalvisionofattainingmiddleincomestatuswithaminimumof1000USDpercapitabytheyear2015,thesectorhasdefineditscontributingvisionas:“Creatingwealththroughhealth”.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|45
Thisissubstantiatedbytheministry’smissionstatementthattheMinistryofHealthaimstocontributetosocio-economicdevelopmentandwealthcreationbypromotinghealthandvitality,ensuringaccesstoqualityhealth,populationandnutritionservicesforallpeoplelivinginGhanaandpromotingthedevelopmentofalocalhealthindustry.Theultimategoalofthehealthsectoristoensureahealthyandproductivepopulationthatreproducesitselfsafely.Thisgoalcanthereforebeseenasproxyforoverarchingwealthcreationandmutatismutandistheobjectivesthatwouldachievethisgoalastheyardsticksagainstwhichprogresswillbemeasured:
1. Ensuringhealthiermothersandchildrenthroughthescalingupimplementationofhighimpactandrapiddeliveryhealthinterventions
2. Promotinggoodnutritionandregenerativehealthacrossthelifespan3. CombatingcommunicablediseasessuchasHIV/AIDS,Malaria,Tuberculosis,epidemicprone
diseasesanddiseasesthatalmostexclusivelyaffectthepoorsuchasBuruliulcer,Guineaworm,Leishmaniasis,lymphaticfilariasis,etc.
ThefollowingareasofactionweredefinedaspointofdeparturefordevelopingthesubsequentdetailedannualProgrammesofWork:
• Promotinghealthylifestylesandhealthyenvironments• Providinghealth,populationandnutritionServices• Investingequitablyincapacitydevelopmentofthehealthsector• PromotingtheuseofInformationforplanningandmanagementofthehealthsector• EnsuringsustainableandequitableFinancing• Promotingalocalhealthindustry• Ensuinggoodgovernanceandpartnership
Thecontextofthehealthsectorhasalonghistoryofpartnershipandcoordinationwithnationalandinternationalbodiesforthedevelopmentofhealthandhealthservices.Governanceandpartnershipsareimportantfortheeffectivefunctioningofthehealthsystemandachievinghealthsectorobjectives.Governancearrangementsinclude:(i)institutionsandtheirorganizationalstructures,(ii)managerialprocessesincludingpolicyformulation,prioritysetting,resourceallocation,planning,monitoringandevaluation,(iii)coordinationmechanisms(iv)performanceassessmentandaccountabilityand(iv)regulation.Withregardstopartners,thereisafirmcommitmenttotheParisdeclarationandtheensuingconfirmationthereofintheAAA.Atthebeginningofthe5yearPOWthiswas,however,notfullytranslatedandthereforemadeintegraltothePOWsdevelopmentagenda.
Theharmonisationandalignmentintermsoffinancesforthehealthsectorwillbeaddressedthroughtheplanningandbudgetcycle.The5yearPOWsetsouttointroducesectorwideprogrammebudgetingwithinafirmgovernmentMediumTermExpenditureFrameworkandtodevelopacomprehensivestrategyforresourcemobilisationfrombothdomesticandinternationalsources.TheNationalHealthInsuranceisforeseentoincreasecoveragewhileensuringfinancialsustainabilityincludingareviewofthesubsidies,premium,tariffstructureandadministrativecost.Multi-sectorandmulti-stakeholderprocesswillbeestablishedandstrengthenedandsystemsandprogrammeswillbeimplementedtoensurealignment,harmonisationandpredictability.
Monitoringandevaluationofthefive-yearprogrammewillinvolveasystematicprocessofcollecting,analyzingandusingdatatoimproveprogrammemanagementandguideresourceallocation.Themonitoringandevaluationexercisewillbeintegraltothemanagementprocessandwillsupportlearninganddecisionmaking.Monitoringasaprocesswillbecloselylinkedtotheimplementationoftheprogrammeofwork.Itinvolvesquarterlycollectionandassessmentofthe

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|46
performanceofthedifferentcomponentsoftheprogrammeofwork.Specificallyitwillaimatdeterminingwhetheractivitiesarebeingimplementedasplanned,milestonesarebeingachievedandoutputsarebeingdelivered.Monitoringwillalsoinvolvestrackingprogresstowardsgoalsandobjectives.Managementteams,CouncilsandtheMinistryofHealthwilltraditionallyresponsibleformonitoringtheimplementationofprogrammeofwork.Inadditiontothequarterlymonitoringandreportingsystem,theMinistryandAgencywillinstitutesystemsjointmonitoringvisitstoprovidetechnicalsupporttoAgencies,andBMCs.Thesesupportvisitswillbestructuredandtargetedprimarilyatassistinghealthsectorimproveperformanceinareaswhereperformanceislessthanoptimal.Annualreviewsandevaluationswillbeconductedbyexternalteams.Indepthreviewofkeyareaswillbeconductedonaselectivebasisinresponsetoindividualtermsofreferencerelatedtospecificissues,concernsandthemesrelevanttooneormorecomponentoftheprogrammeofwork.Thereviewswillinvolvein-depthanalysisofcontextandvariablesaffectingperformancewillaimatassistingthesectortomakejudgmentontherelevance,efficiency,effectiveness,adequacy,sustainabilityandimpactofcomponentsofthe(orthewhole)programmeofwork.
ThedialoguewithdevelopmentPartnersfollowsasimilarpattern.Therearequarterly‘business’meetingsbetweengovernmentandpartnerswhereprogressagainstthePOWisdiscussedandmonitored.Ontwooftheseoccasionsthesemeetingsarecombinedwitha‘summit’allowingawideraudiencetoinputintheplanning(onesummit)andreview(theothersummit)ofthesector.A‘rolling‘matrixofactionpointsandresponsibilitiesismaintainedandupdatedduringthebusinessmeetings.
Processversusprogress
Aswasearliermentionedthesequentialannualreviewsprovideacumulativepictureofprogressagainststatedtargetsassummarisedbythesectorwideindicators.Theyfurtherprovideananalysisoftheunderlyingsystemsandprogrammesthatledtotheseachievements(orlackthereof).Thisdeskreviewtakesahistoricallookatthisprogress,processandactionsbycomparingidentifiedintentionsforchangewithactualchangesanditsimpact/effectsonprogressasoutlinedinthe5yearPOW.AdifficultyincomparingthethreesubsequentPOWsversustheoriginal5yearPOWistheshiftin2008fromathemebasedapproachtoprogrammingtoanoperationalagencyapproach.Thishascausedthatsomeaspectsofthe5yearPOWwerelosttofollowup.ThesequentialreviewswerebasedonthenperceivedattentionareasfortheMinistryofHealthcausingthemtonotcoverallaspectsofthePOWunderreview.Thisdemonstratesthelimitationsofadeskreviewinthatsomeaspectsofactualprogressonespeciallyongoing(system)processescannotbecovered.Intermsofoutputandoutcome,however,theavailabilityofastablesetofsectorwideindicatorsallowstodrawsomeconclusionsaboutprogressthatarecapturedinthe2009POWreviewwhich,asearliermentioned,canbeseenasareviewofthecumulativeoutcomeoftheimplementationofthe5yearPOW.
Healthylifestyleandenvironment
1. Regenerativehealthandnutrition
AlthoughalotofemphasisisplacedonthisthemeintheoriginalfiveyearsPOW-itisindeedthecoreoftheunderlyingstrategyembodiedinregenerativeandnutritionhealthobjectivesandtargets-itappearstodisappearofftheradarasadiscreteprogrammeelementafterthefirstyearofimplementation.InthefirstPOW(2007)distinctivementionismadeoftheparadigmshifttoregenerativehealthandnutrition.Althoughthereviewofthe2007POWmentionsthatastrategicplanwasfinalisedtoscaleuptheregenerativehealthandnutritionprogramme,thesubsequentagencybasedPOWsreferonlycursorytothemulti-sectorandpersonalphysicalfitnessaspectsofitwhilebiomedicalpublichealthaspectsseemtobemaintained.Itmightbearguedthatthisineffectindicatesthemainstreamingofthistheme,butimportantreferraltopersonalhealthylifestylesis
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|47
missed.Nobaselinefortheindicatorsproposedforthisthemehasbeenestablished.ThelackofprogressmighthavetodowithsomeoftheissuesidentifiedinthereviewofthePOW2007whenitrefersamongotherstoaseeminglylackoftargeting,lackofconsultationwithMoHandGHSstaffonnutrition,lackofinvolvementofDHMTs,theperceptionofaverticalintervention,lackofimpactmonitoringandinsufficientanchoringwithinamulti-sectorcontext.Thereviewofthe2008POWremarksthatitdifficulttoassessperformancesincenoreportsareavailableovertheactualworkdoneintheprogrammeandseesasawayforwardanintegrationintheGHSpublichealthactivities.Inthe2009POW,however,nodirectactivitiesrelatingtoregenerativehealthandnutritioncanbefoundbesidesatangentialreferraltopublicawarenessonfoodsafety,improvementofdataonriskfactorsofspecificdiseasesandtheintentiontoconductscreeningprogrammesforspecificNCDs(breastandprostatecancer).
2. Publichealthlegislation
Althoughthe5yearPOWmentionsthereviewandpromulgationofthepublichealthlaw,the2007reviewremarksthatitisuncleartowhatextenttheseactivitieshavebeentakenforward.NospecificmentionofthepublichealthlawismadeinthesubsequentPOWsandreviews.Ourunderstandingisthatthereviewofthepublichealthactisnowinitsfinalstagestobepassedintolawsoon.
3. Inter-sectorcollaboration
Thisaspectoftheoriginal5yearPOWhadspecificactionpointsonthenationalandperipherallevelthat,accordingtothePOW2007review,wereunclearinthewaytheyweretakenforward.ThesubsequentPOWsonlymakementionofsectorcollaborationintheiractivitymatriceswhereonecolumnreferstothecollaboratorsconcerningspecificagencies,ministriesandotherpartners.The2008POWreviewmakesnomentiononprogressintermsofcollaborationbetweendifferentsectors,althoughthereissomecursorymentionofmulti-sectoractivitiesintherecommendationswhereitconcernsintegrationofthenon-functionalregenerativehealthandnutritionprogramme,comprehensivedistricthealthplanningandNHISaccreditationandcostcontainment.
Coverageofhighqualityhealth,reproductionandnutritionservices
Healthinterventionsaredeliveredthroughacombinationoffamilyorientedcommunitybasedservices,populationandoutreachorientedschedulableservicesandindividualorientedclinicalservices.Theservicedeliverymodesdeterminewhere,howandoperationalstrategiesforthedeliveryofhealthservices.Ingeneral,interventionsdeliveredinthesamewayusuallyusethesamesetofinputsandfacesimilarconstraints.Forthisreason,strengtheningthehealthsystemasawholetendstobenefitthedeliveryofhealthinterventions.InthisvainthefollowingwilldiscussthedifferentactivitiesdeployedbythehealthsectorinGhanainrelationwiththeunderlyingdeliverysystemsandtheir(lackof/insufficient)integrationandcollaboration.
The5yearPOWidentifiestheprovisionofhealthservicesasgenerallynotadaptedtosocio-culturalneeds,valuesandpractices.Healthfacilitiesinboththepublicandprivatesectorsoperateasdiscreteentitiesratherthanaspartofanetworkofproviders.Thereferralsystemis(2007)nonfunctionalleadingtoincreasedcosttoclients,providersandgovernmentandrelativelypoorhealthoutcomes.
Traditionalandalternativemedicinepracticeareusedbythepopulationandyetnotadequatelysupportedandregulated.Thesectorhasbeenunabletoadoptaholisticdeliveryapproachtoservicedeliveryconsistentwiththelocaldemand,choicesandpracticesinvolvingtheuseofallkindsofprovidersincludingallopathic,traditionalandalternativepractitioners(5yearPOW2007-2011).
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|48
Thekeyobjectiveidentifiedforthisthemewastoensureequitableaccesstogoodquality,safeandaffordablehealth,reproductiveandnutritionservicesthatimprovehealthoutcomes,respondtopeople’slegitimateexpectationsandarefinanciallyfair.
Thefollowinginterventionareaswereidentifiedinthe5yearPOWandprogressineachisdiscussedbelow,althoughverticalisation,fragmentation(ofagencies)anditsoppositeintegrationhavecausedoverlapandgapsbetweentherespectiveareas.Theswitchin2008toanoperational,agencybasedPOWissymptomaticandmighthavecontributed,ascauseorconsequence,toafragmentedapproachtowardsthesefunctionalinterventionareas.Cautiouslyaconclusionmightbedrawnthatthisorientationtowardsagencieshasledtoa‘silofication’ofthehealthsectorwherethedifferentsilosarecompetingforgovernmentresources.Inordertosatisfycounterpartfundingtospecificprogrammes(seelater)moregovernmentresourceshave(therefore?)beenringfencedbytheMinistryofHealthleadingtocomplaintsofagenciesregardingtheirroomtomanoeuvre.
1. Communicablediseasecontrol
TheHighImpactRapidDelivery(HIRD)strategieshavebeenscaleduptocoveralldistrictsinGhana,however,the2007reviewnoticesthattheirplanningrunsparallelwithroutinedistricthealthplanning,presumablybecauseofweakcapacityforplanningatthatlevel.Forthe2008POWacontinuationofHIRDwasplannedwithoutaddressingthisissue.InOctober2008GHSincollaborationwithUnicefandtheWHOevaluatedtheHIRDinitiativeandaffirmedthevalueofHIRDforchildhealthbutconcludedthatitisinitiatedbydiseasecontrol,childhealthandnutritionprogrammesthathavetheirownsourcesoffunding,ownproceduresandownmethodsofwork.HIRDhasnotmanagedsufficientlytopulltheseprogrammestogether,partlybecausefundingcomesverticallyfromdifferentfundingsources.Ithasbecomeaverticalprogrammeinitsownright,themonitoringsystemsareweakandinformationishardlyanalysed.Nonintegrationwithdistrictplanningremainsandunpredictabilityinterfereswithotheractivitiesatthatlevel.The2009POWmakesnomentionofHIRDundertheservicedeliverychapter.ThiscouldindicatethatitnowconstitutesanintegralpartoftheGHSservices,butleavesindoubtwhetherthesameisthecaseatthedistrictplanninglevel.
TheEPIinterventionwasgearedtomaintainandincreasetheexistinghighcoveragerates.Evidenceindicates,however,thatPenta3coverageremainsstaticatbest.ThePOW2008reviewstatesthatthereisnoreasonforcomplacencywithregardtothesuccessoftheEPIprogramme.AswithHIRD,EPIstillremainsaverticalisedinterventionwithitsownreportingchannels.
OtherdiseasespecificinterventionsasforHIV,tuberculosis,malaria,nutrition,reproductivehealthandneglecteddiseaseshaveinadditiontotheabovementionedledtohightransactioncostattheperipheral,districtlevelandregionallevel(review2008POW),whiletheseinefficienciesarenoteasilyrecognisedatthenationallevel,whereprogrammeofficersarefocussedontheirownprogrammeandonaccountabilitytowardstheirdevelopmentpartners.
The2007POWmakesnomentionofCommunityHealthServicesandPlanning(CHPS)asastrategytoimplementhealthservicedeliverybutafirstneedsassessmentwasmadebyGHStorollouttheinitiative.ThereviewofthePOW2007identifiesCHPSasakeyissueandconcludesthatitisimportanttorevisitthestrategyandtorolloutCHPSinthecontextofincreasingsuperviseddeliveriesbyskilledattendants.CHPSappearsfirstinthePOW2008asaspecificstrategybutalthoughanintensificationoftheexpansionofCHPScompoundswasforeseenthereviewofthe2008POWstillrecommendsthemappingandanalysisofbestpracticesinCHPSforharmonizingthecommunityhealthapproach.The2009POWreiteratesthattherolloutofCHPShasbeenextremelyslow,butnoevidenceintheactivitymatrixofaspecificrolloutfortheinterventionispresent.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|49
2. Noncommunicablediseasecontrol
The5yearPOWstatestheimportanceofstrengtheningtheprogrammeforthecontrolofnon-communicablediseases(NCD)throughtheestablishmentofacancerregistry,theestablishmentofscreeningprogrammesandthestrengtheningofthementalhealthprogramme.Althoughthedesignandimplementationofscreeningprogrammesappearsinthe2007POWtheseareonlyrepeatedinthesubsequentPOWs,whilenoreferencetothemismadeinthereviewreport.ThisleadstothebeliefthatnorealprogressismadeinthisimportantareaandthatalthoughtheimportanceofNCDsisincreasingwhileGhanaisgoingthroughanepidemiologicaltransitionthepointofgravityofthehealthservicedeliverysystemremainsstronglybiasedtowardscommunicablediseases.
3. Reproductivehealthandsexualhealthrights
TheMaternalMortalityRatioremainsveryhigh.Althoughthisassessmentwasuntil2008onlybasedoninstitutionalGHSdatathatgiveatbestadoubtfulindicationoftherealsituationwhenalotofdeliveriestakeplaceathome,thiswaslateraffirmedinthe2007MaternalHealthSurveythatmeasuredatotalMMRof451inthefiveprecedingyears.Antenatalcoveragehasremainedhighduringthethreeprogrammeyearsataround90%ofallpregnantwomen,butthetargetforMDG5remainsoutofreach.The2007POWcontainsthethreeelementsoffamilyplanning,deliverycareandreferralandPostAbortionCare(PAC),the2007POWreviewreportslargeregionalandsocio-economicdisparities,financialbarrierstoreceivematernalcare,socio-culturalfactors,poorqualityandnonavailabilityofservicesasreasonsfortheunacceptableperformance.During2008thethenMinisterofHealthdeclaredmaternalmortalityanemergencyandrenewedemphasiswasplacedonmaternalhealthwiththeestablishmentofaministerialtaskforce.Thistaskforceformulatedfourpriorityareas:Familyplanning,emergencyobstetriccare,adolescenthealthandPAC.Therequesttoformulateatimedandcostedimplementationframeworkcould,however,notbehonoured.During2008pregnantwomenweredeclaredexemptforenrolmentfeesfortheNHIS.Thishaspresumablyledtoasignificantincreaseinassisteddeliveries.FurthermoreplanstoextendBasicEmergencyObstetricCare(BEOC)totheCHPSlevelareinanadvancedstageofdevelopment.BecauseofitsnaturetheMMRindicatorcanonlybemeasuredtoreduceintheyearstocome.
Becauseoftheagencycentrednatureofthe2008and2009POWsthefamilyplanning(FP)componentseemstodisappearfromtheradarinthesetwodocumentsalthoughrepositioningFPismentionedinthe2007POWandtheactivitymatrixofthe2009POW.Thetworeviewsof2007and2008bothindicatealargeunmetdemandformodernmethodswithaslowlydecreasingfertilityrate.Inthe2007reviewalackofmaleinvolvement,lackofintegrationofservices,socio-culturalfactors,providerbiasandforemostinsufficientcommoditysuppliesasunderlyingcauses.Althoughastudyin2008recommendedtheinclusionoflongtermmethodsundertheNHIS(withsavingsinthelongterm)andthe2007reviewrecommendedthesame,noprogressismadetothisrespect.
4. Nutrition
Aswasearliermentionedthenutritionprogrammeinthehealthsectorshowsinsufficientlinkagewiththeregenerativehealthandnutritionprogramme,althoughthisisastatedactivityareaofthe5yearPOW.Furtheractivityareaswererehabilitation(therapeuticfeeding)ansupplementaryfeeding,collaborationwiththeMinistryofEducationforthebenefitsoftheschoolfeedingprogramme,inclusionofnutritioninthecurriculumofhealthworkersandestablishinganin-servicetrainingprogramme.Althoughthe2007POWreiteratestheseareasofactivitiesandaddsthestrengtheningofHIRDintermsofnutritioninterventionsaswellasprogrammestocontrolmicro-nutrientdeficiencies,theagencybasedPOWsof2008and2009makenomention.Thereviewofthe2008POWconcludesthatalthoughthepercentageofunderweightedchildrenunder5isreducingto15%in2008stuntingwith30%andseverestuntingwith11%remainsunacceptablyhigh.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|50
5. Emergencypreparednessandresponse
Ambulanceserviceshavetakencentrestageunderthisissueinthefirstthreeyearsofimplementingthe5yearPOW.Theintentionwastoscaleupambulanceservicesbyinteralialinkingthefacilitybasedambulanceswiththenationalambulanceservice(NAS)andtoconsolidatethescalinguptotheregionallevel.Inter-sectorcollaborationwiththeMinistryofTransport,thePoliceService,theGhana@50CommitteeandtheCAN2008wasmentioned.The2008POWputsfigurestotheseactivityareaandaimstoestablish6additionalambulancestationsandtostrengthenthecommunicationlinksbetweenNAS,facilitybasedambulanceandhealthfacilities.ANASbillisthenunderpreparation.Althoughthereviewofthe2007POWmentionsthedeteriorationofthehealthsectorvehiclefleet,ofwhichonly75%isoperational,itdoesnotsplitthisoutspecificallyforambulance.Itisthereforedifficulttofollowuponthe2007activities-forinstancehowmanyadditionalstationshavebeenestablished-butthe2009POWtalksagainaboutadditional(10)stations.Whetherthiswouldthenmakeupthetotaloverthethreeyears16additionalstationsisnotclear.
Ingeneralthereisnostandardemergencyresponsesystem;theresponsetooutbreaksisinthehandsoftheGHS.Thereisafunctionaldiseasesurveillancesystemwhichhasworkedwellformeningitisandpolio.TheNationalDisasterManagementOrganisationhasanEpidemicSubcommitteeandintheMoHthereisaMinisterialMedicalEmergencyServicesCommittee,butsofarthecommitteeisnotcoveringepidemicoutbreaks.
6. Clinicalcare
Likewithotherissuesfromtheoriginal5yearPOWdetailsoftheprogressinthisactivityareaarelosttofollowupwhentheannualPOWchangestoanagencybaseddocument.Recurrentissuesseemtobehumanresourcesbothinquantity,qualityanddistribution(thisisdiscussedinaseparatechapterofthisreport)andcommoditysupplyanddistribution(acomprehensivereportisexpectedin2010).PerhapsthemostimportantfactorimpactingonclinicalcarehasbeenthesteadyincreasingenrolmentofthepopulationunderNHIS.OPDandIPDutilisationhaveincreasedsignificantly.However,forexampletheexistenceoftwodifferentdruglistsindicatesaninherenttensionbetweenthemainfinancers(NHIS)andthemainimplementersofhealthservices(GHS)inGhana.TheeffectsoftheresourcesavailedthroughtheNHIStothehealthsectorwillbediscussedseparatelylater.
7. Traditionalandalternativemedicinepractice
The5yearPOWclearlystatesthedevelopmentofatraditionalandalternativemedicinesectorthatintegratesintothegeneralhealthsystem.WhilethePOW2007takestheissuesoutofthe5yearPOWalmostliterallyforward,thesubsequentPOWsof2008and2009listspecificactivities,mostofthemreflectsystemsandcapacitybuildingfortheTraditionalMedicinePracticeCouncilandonlycursorymentioningtheintegrationofalternativemedicineinthehealthservicedeliverysystemofGhana.Activitiesdifferfromyeartoyearandthesubsequentreviewsoffernoinsightinactualprogressionwithinthisactivityarea.
8. Rehabilitation
TheonlyaspectoftherehabilitationactivityareathatcanbesomewhatreliablyfollowedupthroughoutthesequentialPOWsandreviewsarementalhealthissuesadeclaredpriorityofgovernment.AkeyissuehereseemstobethepassingofthementalhealthbillwhichismentionedinallPOWsseeminglywithoutprogresshamperingthefurtheringofthedevelopmentofthesector.Thereseemtobecontinuingissueswiththebalancebetweenhospitalisedandcommunitycareandalackofqualifiedhumanresources.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|51
StrengtheningHealthSystemscapacity
Capacityreferstothestockofcapabilitiesavailabletothehealthsystemforhealthdelivery.Itincludesamixoftechnical,managerialandlogisticcapacityrequiredtopromote,protectandimprovehealth.Capacitydevelopmentwillemphasizethecreation,expansionorupgradingofcapabilitiesinthehealthsystemtofillcapacityandservicegaps,improveindividualandinstitutionalperformance,andachieveobjectivesofthehealthsector.
1. Investingequitablyincapacitydevelopmentofthehealthsector
Humanresources
Theoriginal5yearPOWdescribesactivityareasthatcouldconvenientlybesummarisedas:
• Expandingtheworkforceandadaptcurriculatorealitiesinthefield• Enhancehumanresourceplanning• Developanddeployhumanresourcepolicies,incentivesandadvocacytoretaincriticalmass• Decentralisemanagementofhumanresources
Initiallythe2007POWsetsofftoincreasetheproductionofmiddlelevelcadre,tocontinuouslyrefinestrategiesforretentionandequitabledistributionandtoenhanceproductivity.ImportantaspectsweretheestablishmentofaHRHconsultativegroupandstocktakingofthethencurrentsituation.ThereviewofthePOW2007concludedthatapolicyframeworkandprojectionofstaffrequirementsforthe5yearPOWwereachievedandthatsalaryrationalisationprovidedaplatformfortheintroductionofperformancemanagement.Theheadcountledtoacleanedpayrollandtherewasadownwardtrendinattrition.PerformancemanagementwouldbecomeoneofthepriorityareasforthePOW2008.Itissurprising,however,thatnosuchactivitycanbefoundinthe2008POW,insteaditsmajorpolicythrustistoensureanequitabledistributionoftherightnumbersandmixofstaffandtointroducestaffimprovementprogrammesontheanalysisthatthenewsalarypackagedidnottranslateintoanincreasedproductivityofthehealthworkforce.Thereviewofthe2008POWobservedthatthefocusontheproductionofmiddlelevelcadrewasmaintainedbutthatthesectormightbesacrificingqualityforquantityriskingoverproduction.Concerningthedistributionofstaffitremarkedthat,althoughtherearestillsignificantinequitiesinthedistributionofhealthworkers,apositivestephasbeentakenbytheInter-MinisterialPostingCommitteethatbecamecloselyengagedindecisionsofdistributionwhiletheMoHhadremoveditselffromoperationaldistributionandtheagenciesdidgettheautonomytoaffectinternalpostings.However,re-distributionofstaffbetweenagenciesremainedachallenge.Thekeychallengeofrecognisedwastheabsenceofagreedstaffingnorms.Thereisnocleardirectionastowhatconstituteshealthworkforceproductivityanddefinitemodelsofmeasuringperformanceareyettobedeveloped,althoughtheGHShasintroducedastaffperformanceappraisalsystemin2008.Staffperformancemanagementisstillanissue,butdifferentmodelsareontrial.Thewagebillcontinuestoescalateandin2008adeficitbudgetwasgenerated.Itseemsthatthesectorbecomingtopheavy(largenumbersofstaffoccupyingthetopendoftheirgrades),thatproducedhealthworkersareexpectedtobeemployedbytheMoHanditsagenciesandthattheexplosionofrecruitmentofmiddlelevelcadrehasledtothisescalation.Thereviewrecommendeddevelopingcriteriaandmodelsforagenciestoworktowardsthesuccessfulimplementationofdecentralisedstaffmanagement.The2009POWfocusesspecificallyonproductivityandperformancethrougheffectiveandefficientmanagement,takingforwardissuesidentifiedinthetwoprecedingyears.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|52
Infrastructuredevelopment
The5yearPOWsetouttodeployanintegratedcapitalinvestmentplanningmodelbasedonneedandnationalstandardsofthehealthsectorinthedevelopmentofaprioritizedfiveyearcapitalinvestmentplan2007-2011andanannualcapitalinvestmentplan.TheconstructionofCHPScompoundwasseenasapriorityaswellashospitalsandhealthcentresinunder-servedareas.
The2007POWmentionsthecompletionoftheheathservicesplanningmethodologyandframeworkforcapitalinvestmentandthemobilisingoffinancesfortheestablishmentof80CHPScompounds.ItspeaksofcollaborationwithDPstodevelopandinstitutearoutineprogressandexpendituretrackingsystemforcapitalinvestmenttobeoperationalin2007.Acapitalinvestmentplanwasdulydevelopedin2007(CIPIII)outliningthreescenariosofmaintenanceofthecurrentsystem,limitedexpansionandfullneedsbasedexpansion.Prudentmanagementreducedthecapitalinvestmentdebtto0byearly2008.Inpracticethismeantthatonlyprojectsrequiringcounterpartfunding,projectsunderICBwithlegalimplicationfordelayedpayments,paymentofoutstandingbills,projectsearmarkedforcompletionin2007andprojectsurgentlyrequiredindeprivedareaswerehonoured.NomentionismadeinthereviewofthePOWoftheforeseenCHPSexpansion.ThesameprudentapproachwastakeninthePOW2008withafocusonthecompletionofongoingprojectswithprioritytoprojectswithsignificantcontributiontoenhancingqualityandequitableaccesstohealthcarewhilecommencingthemajorrehabilitationofTamaleTeachingHospital,constructionofBekwai,Nkawie(ORETfunding)andTarkwadistricthospitalsandtheSunyaniRegionalHospitalstaffaccommodationproject.ThetargetfortheestablishmentsofCHPScompoundswassetat50.Apartfromtheseprioritiesalistforcompletionofongoingprojectsaswellasthecommissioningofnewprojectswasmentioned.
Thereviewofthe2008POWdidnotincludeelementsofinfrastructuredevelopmentandsofollowupofplansislost.ThePOWfor2009largelyincludesunfinishedbusinessfrom2008andthecommissioningoffurtherdistricthospitalsinWa,Kumasi,Madina,Weija,Kumasi,Tepa,Salaga,Wenchi,Konongo-OdumasiandTwifo-Praso.Nodetailsonfinancialinvestmentareavailableapartfromtotalfiguresthatmightbequestionedforinclusiveness.
Suppliesandlogisticsmanagement
Theoriginal5yearPOWfocusesonproduction,procurement,supply,distributionandrationaluseofmedicine(traditionalandmodern)andvehiclereplacementandpreventivemaintenance.The2007POWtakesthisforwardwithafocusontheimplementationofaframeworktoaddressaffordability,sustainablefinancing,safety,qualityandefficacyofmedicines.InteraliatheharmonizationofthestandardtreatmentguidelinesandessentialmedicineswiththeNHIS.Consideringtwostillexistingdruglistsin2009,littleprogresshasbeenbookedagainstthisactivityarea.Furthermorethe2007POWindicatesthemobilisationofresourcesforvehiclereplacementandtoimprovethemanagementandpreventivemaintenanceofthefleet.
Thereviewofthe2007POWreportsapoorstateofmaintenanceofthesector’svehicleswithonly75%ofthe399vehiclesroadworthywithsignificantregionaldisparitiesintheavailabilityofvehicles.Itreportsfurtheraneffectivelogisticssystemforessentialmedicinesandsupplieswithonlyminorstockoutsatthefacilitylevel.
The2008POWonlymentionsinverygeneraltermstheprocurementoftransportforspecificallythedistrictlevelwithoutgivinganytargets.Itremainsquietabouttheprocurementofdrugsandmedicalcommodities,apartfromaannexedprocurementplanthatprovideslittleinsightinefficacy,efficiencyandeffectivenessoftheeffort.Thereviewofthe2008POWmakesnoreferencetotheprocurementofdrugs.The2009POWhasagainnotargetswithrespecttovehiclesandthecapitalinvestmentbudgetonlystatesballparktotalfigures.Toaddressthe(medicine)supplychainthis
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|53
POWfocusesonthefacilitationofvisiblefollowthroughonprocurementpracticesandbroadstakeholderengagement.Theresultisbroadlyformulatedasimprovedmedicinesandlogisticssupplysecurity.Acomprehensivecommoditysecuritystudywascommissionedin2009ofwhichtheresultsareexpectedinthefirstquarterof2010.
2. Promotingtheuseofinformationforplanningandmanagementofthehealthsector
Healthinformationhassixcomponents:ResourcescomprisinghumanandICT,indicators,datasourcesincludingpopulationbasedandadministrativedatasources,systemsfordatamanagement,informationproductsanddisseminationanduse.
Thehealthsectorhasestablishedarobustandstableframeworkofsectorwideindicatorstomonitorprogress.Asubsetoftheseindicatorsconstitutesaholisticperformanceassessmentthatisnowafirmstartingpointforthesectordebateandprioritisationandplanningofservices.AtthecoreofthesectorwideindicatorsliesanowunifiedDHMISthatisalsoadoptedbythesecondlargestproviderofservices,CHAG.However,thereisconcernthatdatacollectionisstilltootimeconsumingforserviceimplementers,whileutilisationatthedistrictlevelandbelowremainsquestionable.Theearliermentioned‘vertical’programmesaddtothedatacollectionburdenbyrequiringspecificdataformonitoring,andtheunifiedDHMIS,whichreceivedmuchattentioninthefirstfewyearsofimplementingthe5yearPOWremainsunderthreatthroughthesedifferentdemandsthatareincreasingwithfurtherfragmentationofthehealthdeliverysystem.
Comprehensivedistricthealthplansareconceivedthroughabottomupneedsbasedprocesswhichinvokesinherentlytensionswiththetopdown,resourcebasedplanningfromthecentre.Sincealotofdistrictpublichealthinterventionsareimplementedinacentralisedtopdownmannerfollowedbyresources,integrateddistrictplanningisoftennotadheredto;adhocplanningforsuccinctinterventionsismorerulethanexception.Thisinturnhasalsoledtoinsufficientuseofdatatoappropriatelyplanlocally.
3. Promotingalocalhealthindustry
Theoriginal5yearPOWmentionsthedevelopmentofmicro-enterpriseforpublichealthinterventionsthroughcollaborationwiththeprivatesectorinconcurrencewiththeMinistryofTradeandIndustrytoavailcapita/micro-creditsforpotentialinvestors.AlthoughinthePOW2007theintentionisexpressedtocreateabetterunderstandingofthehealthindustryasabasisforenhancingthecapacityandsustainabilityofthehealthsystemandcontributetothenationaleconomy,thisislosttofollowupinthesubsequentagencybasedPOWs.
Promotegoodgovernance,partnershipsandsustainablefinancing
1. Ensuringsustainableandequitablefinancing
FaroutthemostimportantinitiativeinthefinancingofhealthservicesinGhanahasbeentheintroductionoftheNHISandthesteadyincreaseoftheenrolmentofthepopulation.Attheendof2008theNHIFwasproviding41%ofthetotalpublicresourceenvelopeforhealth.Thesustainabilityoftheschemeishoweverthreatenedbyseveralfactors;currentpaymentsystems(tariffcreep,incentivesonoverprescription),absenceofco-paymentswithinherentmoralhazard,acomprehensivebenefitspackagethatcovers95%ofallhealthinterventions,poorgate-keeping,poormonitoringandcontrol,lowpremiumsfortheinformalsector(notbasedonactuarialanalysis)andahighproportionofexemptedgroups.Currentlythehealthinsuranceactsaswellasthepremium/NHILsystemsareunderreviewandaclearerpictureofthefutureofNHISisexpectedin
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|54
2010.Thiswouldsitsquarelywithintheintentionsofthenewgovernmenttointroduceaoneoffpremiumpayment.
Arecurrentdiscussionissueisthepro-pooraspectoftheinsuranceschemeandthedifferenceofdefinitionsusedbytheNHISandforexamplethelivelihoodsentinelsurveystoidentifythepoor.TheopinionoftheMoHistodefinethepooraccordingtodefinitionsappliedbytheMinistryofSocialWelfareanddirectsubsidiesforexemptgroupsaccordingly,althoughsomevoicespleadforgeographictargetingofthepoor.Howthepoorargumentisaffectedbytheoneoffpaymentisstillhanginginthebalanceandwilldependonandiswaitingforthenewlegislationandtariffstructure.
AsearliermentionedtheexemptionofpregnantwomenunderNHIShasincreasedthenumberofassisteddeliveriessignificantly.However,duetothecharacterofinterventionsarounddeliverycostwilloutstripthesubsidisedpremiumwhichwillbringfurthersustainabilityissuestothefore.TheintentionoftheNHIAtodecoupleunder18childrenfromtheirparentsandthusrealiseadefactoexemptionofthewholeunder18populationofGhanahasyettobematerialised.
WithNHIS,moneyfollowsinfrastructure.Therewillthereforebeatendencyforhigherfacilitiestocapturereimbursementsdisproportionallyandsimilarareaswhichhavehigherlevelsofinfrastructure.Aseparateconcernisthebalancebetweenpreventiveandcurativeservices.AtpresentthosefacilitiesgeneratingrevenuefromtheNHISbecomeincreasinglyfinanciallyindependent,whilefundsforpublichealthactivitiesarestagnant.Thishaschangethepowerbalancebetweenhospitalsinparticularandhealthmanagersatdistrictregionalandnationallevel.Thereisnoevidenceofredistributionfromhospitalstohealthadministrations.
OneoftheequityconcernsrelatingtotheNHISishowithasaffectedthenon-insured.Whenthenewtariffswereintroducedin2008itaffectedthecashandcarrypricesaswell.Assessingtowhatextendthenon-insuredhavebeensqueezedoutofthemarketisnotstraightforward,butthefactthatthemajorityofIGFisgeneratedbytheNHIS,whileitsmembershipisrelativelybelowthatinputsuggestthatthenon-insuredareusingfewerand/orlessexpensiveservices.
2. Ensuinggoodgovernanceandpartnership
Asredlinessomeissuesarerecurringthroughoutthedifferentthemesoftheoriginal5yearPOWimportantforgoodgovernanceandpartnership:
• Thefragmentationofthehealthdeliverypackagecausedbyaprogrammaticagencybasedapproachanddonorearmarking.
• Skewingofservicestowardscurativecare(andmoreingeneralbio-medicalsolutions)atthedetrimentofpublichealthactivitiesandlocalhorizontalmanagementofservicesandcausedbythechangingmodalitiesoffinancingthesector.ConnectedwiththisisthefeelingthattheNHISismoreandmoresettingtheagendaforhealthservicesbecausetheyineffectcontrolaccreditation,qualitycontrolandimplementationofhealthservices.
• Geographicandincomeinequitiesofaccesstohealthservices.
TheseissueshavetheattentionoftheMoHanddevelopmentpartners,andsomeongoingdebateswilladdresspossibleremedialaction.NewCommonManagementArrangementsorunderconstructionthatwillencompassallstakeholdersinthesectorpossiblyaddressingthefragmentationofthesector;AstrengtheningoftheInterAgencyLeadingCommitteethatmightaddressthe‘silofication’ofthesector;and,thenewpublichealthactsandhealthinsurancelegislationthatmightallowamorestrategicapproachtowardsNHISexpenditures.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|55
AtthesametimewiththestrengtheningoftheCHPSapproachandtheopportunitiesofferedbyprogrammes(e.g.GFTAM,GAVI)toinvestinsystembuildingandcapacityatthedistrictandregionallevelappropriatelocalplanningmightbecomemoreachievable,butrequiresamoreintegrated‘horizontal’approach,asopposedtoagencybased,towardsplanningatthedifferentlevels.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|56
Annex4.NoteonInter-AgencyLeadershipCommittee
1. BackgroundAshealthserviceshavegrownmorecomplexoverthepastdecades,theMinistryofHealthandGovernmentofGhanahaverespondedbycreatingagencies (currentlynumbering17)responsible for coordinating, providing and/or regulating various aspects of the nationalsystemthroughoutthenation’s [165]districts.Communicationandcollaborationbetweenthese agencies is instrumental to the realization of the objectives set out in the GhanaHealthSectorMediumTermDevelopmentPlans(SMTDPs).TheHeadsofAgencieshavehada history of collectively meeting with the Ministry of Health sporadically over the pastseveral years, although generally thesemeetings have been infrequent. In total,minuteswerefoundtobedocumentedforonlynineHeadsofAgencymeetingsfrom2002to2007.Inearly2008,adecisionwas taken to revitalise thepreviousHeadsofAgenciesmeetingsintotheGhanaHealthSectorInter-AgencyLeadershipCommittee(Inter-AgencyLeadershipCommittee, or IALC). The primary purpose of this committee is to institutionalize a keyleadershipstructureacrosstheMinistryofHealthanditsAgencies.Thisteamof leadersisalsointendedtoactasa“MinisterialAdvisoryCommittee”andbythatcanbeconsideredas“acabinet”fortheMinisterofHealth.TheInter-AgencyLeadershipCommitteehasthefollowingcollectivegoals:
1. Tojointlyagreeonsectorwidepriorities,policiesandgoalsasateam;
2. To ensure alignment of Agency and Inter-Agency activities with health sectorpriorities,goalsandobjectives;
3. Todiscuss progress,makedecisions and resolve issues for keyAgency and Inter-Agency activities, as well as any other critical health issues or situations thatrequirethebenefitofanInter-Agencycollaborativeproblemsolvingapproachthatresults in clear action items including person(s) responsible and timeframedeadlines;
4. To create operational synergies between agencies to improve the efficiency andeffectiveness of the sector as a whole, and to avoid duplication of services oractivitiesbetweenAgencies;
5. To act as the health sector advisor/ “cabinet” to the Minister and provideinput/directionintoMoHpolicies;
6. Todistributekeyinformationconcerningcurrentpressingsectoralissuesacrossthesector and downward through each agency to support the implementation ofhealthsectorpoliciesandstrategicdirectiveswithinthescopeoftheIALC.
7. To leverage collaboration venues (such as Health Summits) to share informationwith other stakeholders and intersectoral partners to ensure alignment withspecialtyworkstreamsrunbyAgenciesandtheirpartners.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|57
8. Tobeaccountableforhealthsectorperformancebyreviewingindicatormetricsofpeer agencies and/or health priority areas and making recommendations anddecisionsonhowtoaddressanygapsinresults.
The Inter-Agency Leadership Committee is intended to convene four times per year(quarterly) for ongoing governance planning, strategic decisionmaking, and performanceoversight,andtodiscusscurrentpressingissues.TheCommitteemembersdevelopasharedagenda,andperiodicallyevaluatetheagendastructuretoensurethatthereisanemphasisoncrosscuttingareasbestaddressedthroughcollaborationofhealthsectorleadership.Core membership of the Committee is comprised of theMinister of Health, the DeputyMinisters, the Heads of Agencies, and the Chief Director. Other guests (i.e. training andresearch institutions, development partners, civil society, the private sector, otherMinistries,Agencyboardmembers,healthsectorspecialistsetc)areinvitedasparticipantson an ad hoc basis when asked to speak to particular agenda items or support anycommitteemembertomakedecisionsonaspecificagendaitem.TheMoHPPMEsecretariatis responsible forcoordinatingagendasandmeetingmaterials,andthereforealsoattendseachmeeting.
2. FindingsA surveyof the first full yearof IALCmeetings found thataverageattendance in the fourquarterlyIALCmeetingsin2008successfullyexceededitstargetof80%,withanoverallrateof82%.Itisnoted,however,thatattendancedidfallfromthefirstmeetingandreachedalowof71%inthe3rdmeeting.Thesurveyresultsalsoindicatedthatattendancecouldbestrengthenedmovingforwardby
a) ensuringattendancebytheMinister;b) reinforcing team “norms” established at the October 15/16 2008 Portfolio
ManagementWorkshop;andc) emphasizing the importance of the meetings as convening the leadership
teamofthehealthsector,andasateamofadvisorstotheminister.AnalysisoftheMinutesoflastDecember’smeetingindicatesthatin20093meetingswereheld,andthefirstmeetingof2010onlytookplaceon24thMarch,suggestingthattheIALCmayhavedifficulty inmeeting its targetof 4meetings in the calendar year. Ensuring theattendanceoftheMinister,whichwasflaggedasakeyrequirementinthereviewof2008,appearstocontinuetohindertheconveningofmeetingsonanannuallyplannedbasis.Another factor impeding the effective functioning of the IALC is the attendance or non-attendanceofkeyagencies,inparticulartheGHSandtheNHIA.Bothoftheseagencieswereabsent from the March 2010 meeting, which limited the ability of IALC to agree onimplementationmechanismsforthedecisionsreached,suchasthenewtariffstructurefortheNationalAmbulanceService(NAS).Itappearedthatthelatenotificationofthemeetingdate,whichclashedwithpre-arrangedactivitiesforbothagencies,wasresponsiblefortheirnon-attendance.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|58
Thediscussionof thenewNAStariff structureat theMarch2010meetingprovidedsomeevidenceoftheIALC’sabilitytofollowthroughonissuesdiscussedatearliermeetings–theissuehadbeenraisedattheDecember2009meeting,andNAShadbeentaskedtoprepareaproposalforreviewatthefollowingmeeting.
3. Recommendations1 To be truly effective as the key forum in the health sector for resolving issues and
makingaction-orienteddecisions,theIALCneedstohavelegalbackingfromCabinettoinstitutionaliseitasapermanentstructurewithinthesector.Italsorequiresaspartofthis legal backing a clear mandate to enforce collaboration, in the event of thecommittee’sinabilitytoreachavoluntaryconsensusonspecificissues.
2 To ensure IALC’s ability to re-align agencies’ activities with sector priorities and
objectives,thereneedstobeaclearlydefinedandcommunicatedlinkagebetweentheIALC’smeetingschedulesandagendas,andthesector’sestablishedplanning,budgetingand review cycle. Without such a linkage, the decisions of the IALC cannot beoperationalisedonatimelybasis,anditrisksbecomingamere‘talkingshop’,lackingtheabilitytoinfluenceimplementationofitsrecommendations.
3 The issue of the MoH’s authority (or lack thereof) to direct the NHIA, which is
increasinglybecomingthesinglemostsignificantfundingsourceforthesector,onpolicyissuesisonethatthreatenstheeffectivenessandcredibilityofthewholeIALCinitiative.NHIAdoesnotappeartoregarditselfasanagencyoftheMinistry,andonlyreluctantlyacceptstheMinister’spersonaloversightofitsoperations.UnlessanduntiltheNHIAisbroughtfullyintothehealthsectorundertheauthorityoftheMinistryofHealth,itsfullparticipationintheIALCmayneverberealised.
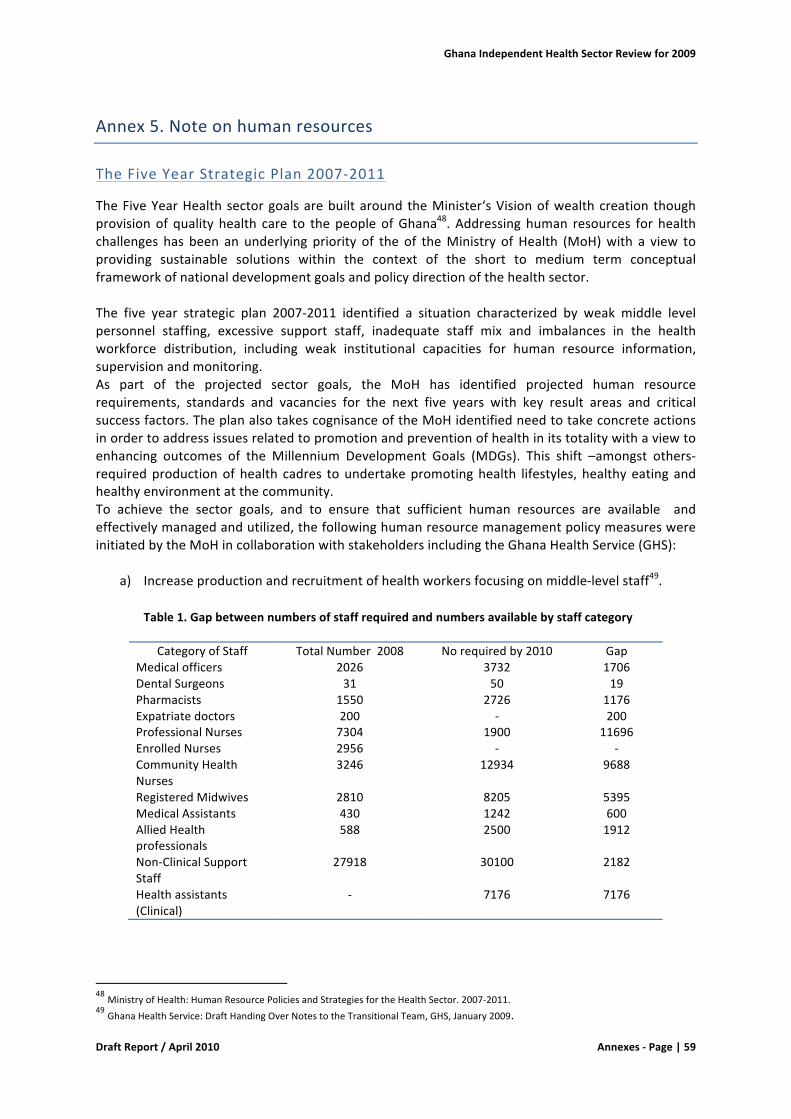
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|59
Annex5.Noteonhumanresources
TheFiveYearStrategicPlan2007-2011
TheFiveYearHealthsectorgoalsarebuiltaround theMinister‘sVisionofwealthcreation thoughprovisionof quality health care to thepeopleofGhana48. Addressinghuman resources for healthchallenges has been an underlying priority of the of theMinistry of Health (MoH)with a view toproviding sustainable solutions within the context of the short to medium term conceptualframeworkofnationaldevelopmentgoalsandpolicydirectionofthehealthsector.The five year strategic plan 2007-2011 identified a situation characterized by weak middle levelpersonnel staffing, excessive support staff, inadequate staff mix and imbalances in the healthworkforce distribution, including weak institutional capacities for human resource information,supervisionandmonitoring.As part of the projected sector goals, the MoH has identified projected human resourcerequirements, standards and vacancies for the next five years with key result areas and criticalsuccessfactors.TheplanalsotakescognisanceoftheMoHidentifiedneedtotakeconcreteactionsinordertoaddressissuesrelatedtopromotionandpreventionofhealthinitstotalitywithaviewtoenhancing outcomes of the Millennium Development Goals (MDGs). This shift –amongst others-requiredproductionofhealth cadres toundertakepromotinghealth lifestyles, healthyeatingandhealthyenvironmentatthecommunity.To achieve the sector goals, and to ensure that sufficient human resources are available andeffectivelymanagedandutilized,thefollowinghumanresourcemanagementpolicymeasureswereinitiatedbytheMoHincollaborationwithstakeholdersincludingtheGhanaHealthService(GHS):
a) Increaseproductionandrecruitmentofhealthworkersfocusingonmiddle-levelstaff49.Table1.Gapbetweennumbersofstaffrequiredandnumbersavailablebystaffcategory
CategoryofStaff TotalNumber2008 Norequiredby2010 GapMedicalofficers 2026 3732 1706DentalSurgeons 31 50 19Pharmacists 1550 2726 1176Expatriatedoctors 200 - 200ProfessionalNurses 7304 1900 11696EnrolledNurses 2956 - -CommunityHealthNurses
3246 12934 9688
RegisteredMidwives 2810 8205 5395MedicalAssistants 430 1242 600AlliedHealthprofessionals
588 2500 1912
Non-ClinicalSupportStaff
27918 30100 2182
Healthassistants(Clinical)
- 7176 7176
48MinistryofHealth:HumanResourcePoliciesandStrategiesfortheHealthSector.2007-2011.49GhanaHealthService:DraftHandingOverNotestotheTransitionalTeam,GHS,January2009.
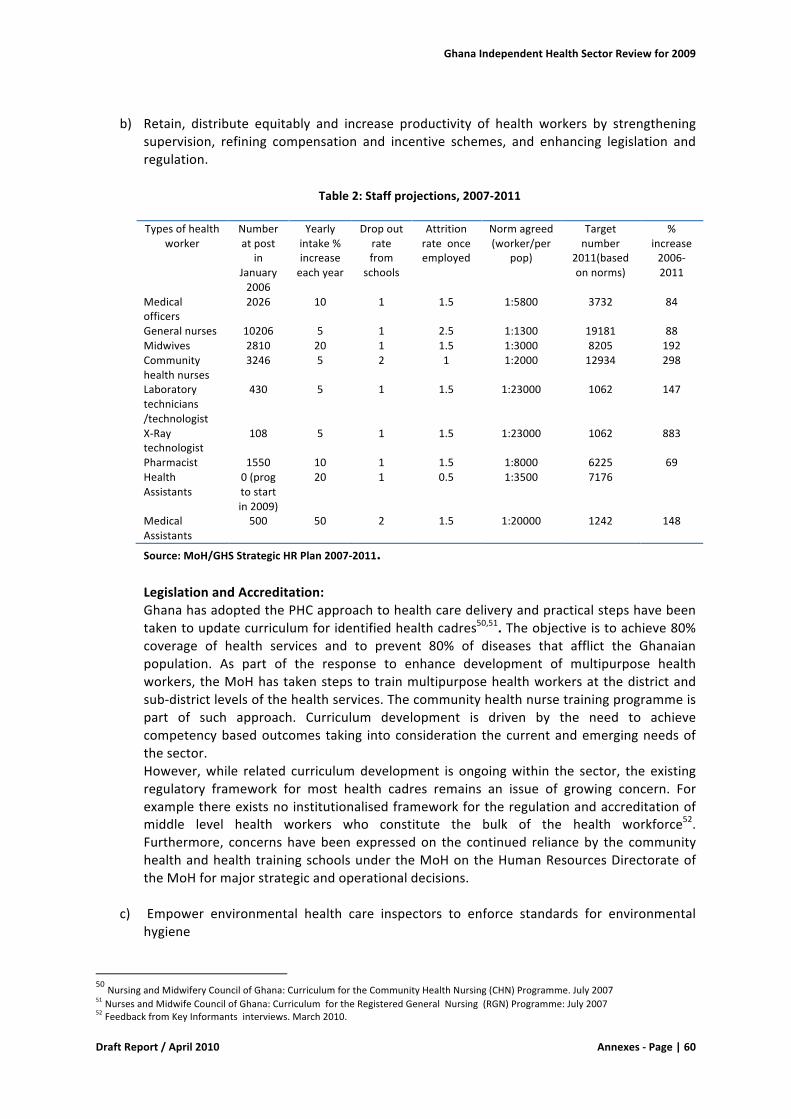
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|60
b) Retain, distribute equitably and increase productivity of health workers by strengthening
supervision, refining compensation and incentive schemes, and enhancing legislation andregulation.
Table2:Staffprojections,2007-2011
Typesofhealthworker
Numberatpost
inJanuary2006
Yearlyintake%increaseeachyear
Dropoutratefrom
schools
Attritionrateonceemployed
Normagreed(worker/per
pop)
Targetnumber
2011(basedonnorms)
%increase2006-2011
Medicalofficers
2026 10 1 1.5 1:5800 3732 84
Generalnurses 10206 5 1 2.5 1:1300 19181 88Midwives 2810 20 1 1.5 1:3000 8205 192Communityhealthnurses
3246 5 2 1 1:2000 12934 298
Laboratorytechnicians/technologist
430 5 1 1.5 1:23000 1062 147
X-Raytechnologist
108 5 1 1.5 1:23000 1062 883
Pharmacist 1550 10 1 1.5 1:8000 6225 69HealthAssistants
0(progtostartin2009)
20 1 0.5 1:3500 7176
MedicalAssistants
500 50 2 1.5 1:20000 1242 148
Source:MoH/GHSStrategicHRPlan2007-2011.LegislationandAccreditation:GhanahasadoptedthePHCapproachtohealthcaredeliveryandpracticalstepshavebeentakentoupdatecurriculumforidentifiedhealthcadres50,51.Theobjectiveistoachieve80%coverage of health services and to prevent 80% of diseases that afflict the Ghanaianpopulation. As part of the response to enhance development of multipurpose healthworkers, theMoHhastakenstepstotrainmultipurposehealthworkersatthedistrictandsub-districtlevelsofthehealthservices.Thecommunityhealthnursetrainingprogrammeispart of such approach. Curriculum development is driven by the need to achievecompetencybasedoutcomes taking intoconsideration thecurrentandemergingneedsofthesector.However,while related curriculumdevelopment is ongoingwithin the sector, the existingregulatory framework for most health cadres remains an issue of growing concern. Forexamplethereexistsnoinstitutionalisedframeworkfortheregulationandaccreditationofmiddle level health workers who constitute the bulk of the health workforce52.Furthermore, concerns havebeenexpressedon the continued relianceby the communityhealthandhealthtrainingschoolsundertheMoHontheHumanResourcesDirectorateoftheMoHformajorstrategicandoperationaldecisions.
c) Empower environmental health care inspectors to enforce standards for environmentalhygiene
50NursingandMidwiferyCouncilofGhana:CurriculumfortheCommunityHealthNursing(CHN)Programme.July200751NursesandMidwifeCouncilofGhana:CurriculumfortheRegisteredGeneralNursing(RGN)Programme:July200752FeedbackfromKeyInformantsinterviews.March2010.
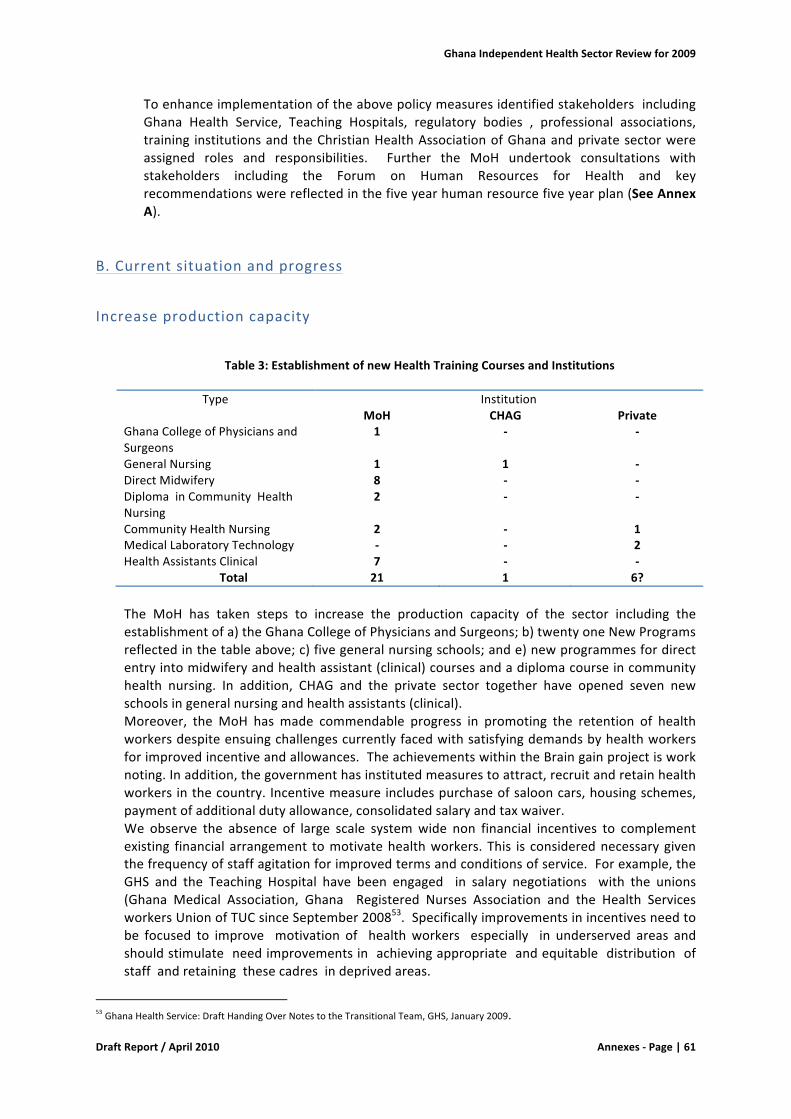
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|61
ToenhanceimplementationoftheabovepolicymeasuresidentifiedstakeholdersincludingGhana Health Service, Teaching Hospitals, regulatory bodies , professional associations,training institutionsandtheChristianHealthAssociationofGhanaandprivatesectorwereassigned roles and responsibilities. Further the MoH undertook consultations withstakeholders including the Forum on Human Resources for Health and keyrecommendationswerereflectedinthefiveyearhumanresourcefiveyearplan(SeeAnnexA).
B.Currentsituationandprogress
Increaseproductioncapacity
Table3:EstablishmentofnewHealthTrainingCoursesandInstitutions
Type Institution MoH CHAG Private
GhanaCollegeofPhysiciansandSurgeons
1 - -
GeneralNursing 1 1 -DirectMidwifery 8 - -DiplomainCommunityHealthNursing
2 - -
CommunityHealthNursing 2 - 1MedicalLaboratoryTechnology - - 2HealthAssistantsClinical 7 - -
Total 21 1 6?
The MoH has taken steps to increase the production capacity of the sector including theestablishmentofa)theGhanaCollegeofPhysiciansandSurgeons;b)twentyoneNewProgramsreflectedinthetableabove;c)fivegeneralnursingschools;ande)newprogrammesfordirectentryintomidwiferyandhealthassistant(clinical)coursesandadiplomacourseincommunityhealth nursing. In addition, CHAG and the private sector together have opened seven newschoolsingeneralnursingandhealthassistants(clinical).Moreover, the MoH has made commendable progress in promoting the retention of healthworkersdespiteensuingchallengescurrentlyfacedwithsatisfyingdemandsbyhealthworkersforimprovedincentiveandallowances.TheachievementswithintheBraingainprojectisworknoting.Inaddition,thegovernmenthasinstitutedmeasurestoattract,recruitandretainhealthworkersinthecountry.Incentivemeasureincludespurchaseofsalooncars,housingschemes,paymentofadditionaldutyallowance,consolidatedsalaryandtaxwaiver.We observe the absence of large scale systemwide non financial incentives to complementexisting financial arrangement tomotivatehealthworkers. This is considerednecessarygiventhefrequencyofstaffagitationforimprovedtermsandconditionsofservice.Forexample,theGHS and the Teaching Hospital have been engaged in salary negotiations with the unions(Ghana Medical Association, Ghana Registered Nurses Association and the Health ServicesworkersUnionofTUCsinceSeptember200853.Specificallyimprovementsinincentivesneedtobe focused to improve motivation of healthworkers especially in underserved areas andshouldstimulateneedimprovementsinachievingappropriateandequitabledistributionofstaffandretainingthesecadresindeprivedareas.
53GhanaHealthService:DraftHandingOverNotestotheTransitionalTeam,GHS,January2009.
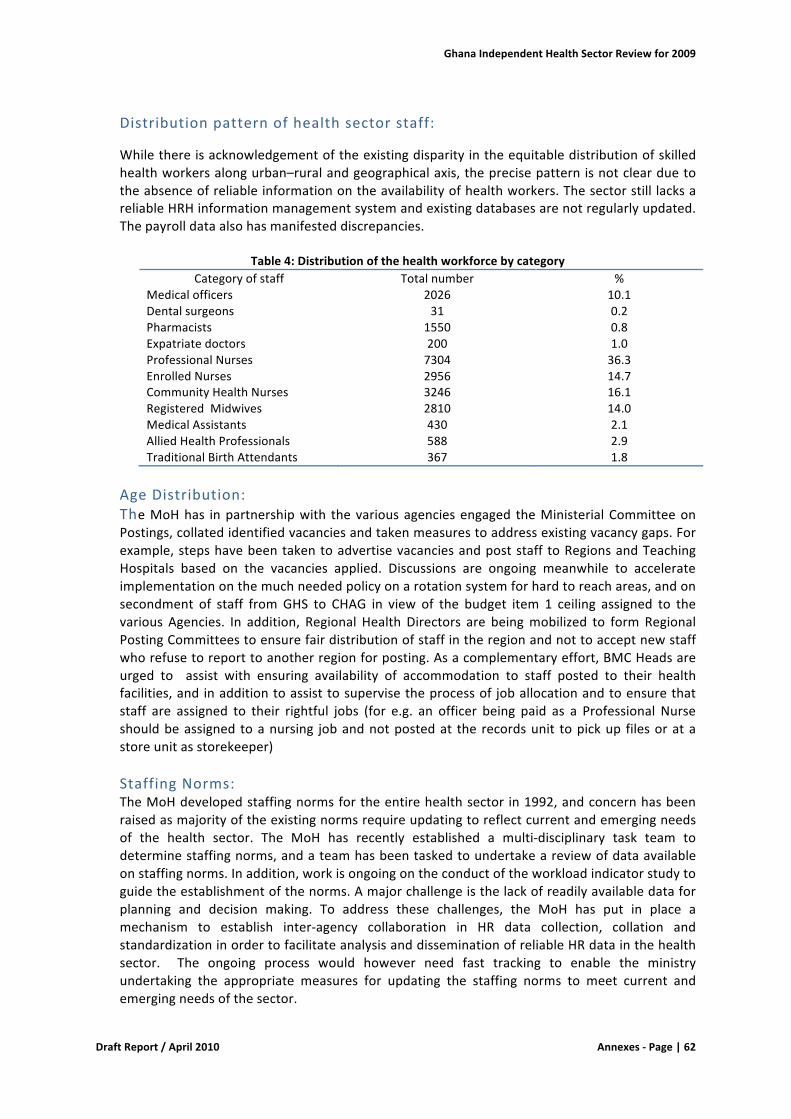
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|62
Distributionpatternofhealthsectorstaff:
Whilethereisacknowledgementoftheexistingdisparityintheequitabledistributionofskilledhealthworkersalongurban–ruralandgeographicalaxis,theprecisepatternisnotclearduetotheabsenceofreliableinformationontheavailabilityofhealthworkers.Thesectorstill lacksareliableHRHinformationmanagementsystemandexistingdatabasesarenotregularlyupdated.Thepayrolldataalsohasmanifesteddiscrepancies.
Table4:DistributionofthehealthworkforcebycategoryCategoryofstaff Totalnumber %
Medicalofficers 2026 10.1Dentalsurgeons 31 0.2Pharmacists 1550 0.8Expatriatedoctors 200 1.0ProfessionalNurses 7304 36.3EnrolledNurses 2956 14.7CommunityHealthNurses 3246 16.1RegisteredMidwives 2810 14.0MedicalAssistants 430 2.1AlliedHealthProfessionals 588 2.9TraditionalBirthAttendants 367 1.8
AgeDistribution:TheMoHhas inpartnershipwith thevariousagenciesengaged theMinisterialCommitteeonPostings,collatedidentifiedvacanciesandtakenmeasurestoaddressexistingvacancygaps.Forexample,stepshavebeentakentoadvertisevacanciesandpoststaff toRegionsandTeachingHospitals based on the vacancies applied. Discussions are ongoing meanwhile to accelerateimplementationonthemuchneededpolicyonarotationsystemforhardtoreachareas,andonsecondment of staff fromGHS to CHAG in view of the budget item 1 ceiling assigned to thevarious Agencies. In addition, Regional Health Directors are beingmobilized to form RegionalPostingCommitteestoensurefairdistributionofstaffintheregionandnottoacceptnewstaffwhorefusetoreporttoanotherregionforposting.Asacomplementaryeffort,BMCHeadsareurged to assist with ensuring availability of accommodation to staff posted to their healthfacilities,andinadditiontoassisttosupervisetheprocessof joballocationandtoensurethatstaff are assigned to their rightful jobs (for e.g. an officer being paid as a Professional Nurseshouldbeassigned toanursing jobandnotpostedat the recordsunit topickup filesoratastoreunitasstorekeeper)StaffingNorms:TheMoHdevelopedstaffingnormsfortheentirehealthsector in1992,andconcernhasbeenraisedasmajorityoftheexistingnormsrequireupdatingtoreflectcurrentandemergingneedsof the health sector. The MoH has recently established a multi-disciplinary task team todeterminestaffingnorms,andateamhasbeentaskedtoundertakeareviewofdataavailableonstaffingnorms.Inaddition,workisongoingontheconductoftheworkloadindicatorstudytoguidetheestablishmentofthenorms.Amajorchallengeisthelackofreadilyavailabledataforplanning and decision making. To address these challenges, the MoH has put in place amechanism to establish inter-agency collaboration in HR data collection, collation andstandardizationinordertofacilitateanalysisanddisseminationofreliableHRdatainthehealthsector. The ongoing process would however need fast tracking to enable the ministryundertaking the appropriate measures for updating the staffing norms to meet current andemergingneedsofthesector.
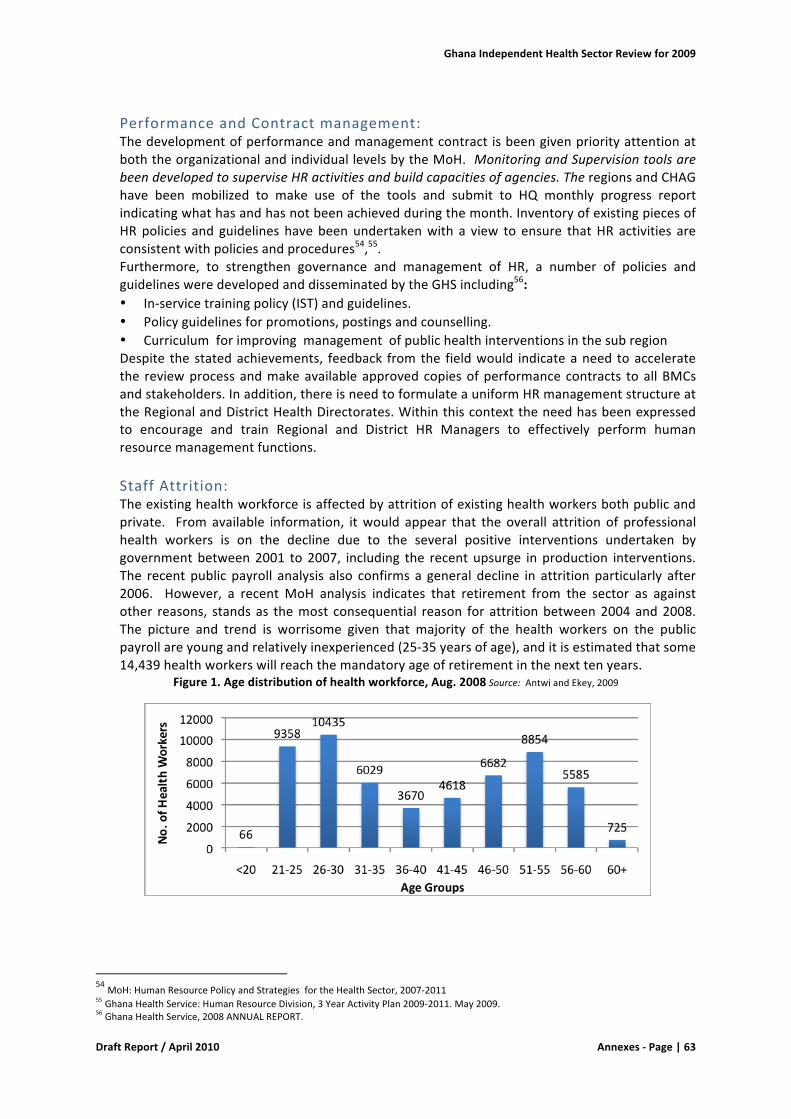
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|63
PerformanceandContractmanagement:ThedevelopmentofperformanceandmanagementcontractisbeengivenpriorityattentionatboththeorganizationalandindividuallevelsbytheMoH.MonitoringandSupervisiontoolsarebeendevelopedtosuperviseHRactivitiesandbuildcapacitiesofagencies.TheregionsandCHAGhave been mobilized to make use of the tools and submit to HQ monthly progress reportindicatingwhathasandhasnotbeenachievedduringthemonth.InventoryofexistingpiecesofHRpolicies and guidelines havebeenundertakenwith a view to ensure thatHR activities areconsistentwithpoliciesandprocedures54,55.Furthermore, to strengthen governance and management of HR, a number of policies andguidelinesweredevelopedanddisseminatedbytheGHSincluding56:• In-servicetrainingpolicy(IST)andguidelines.• Policyguidelinesforpromotions,postingsandcounselling.• CurriculumforimprovingmanagementofpublichealthinterventionsinthesubregionDespite thestatedachievements, feedback fromthe fieldwould indicateaneed toacceleratethe reviewprocessandmakeavailableapprovedcopiesofperformancecontracts toallBMCsandstakeholders.Inaddition,thereisneedtoformulateauniformHRmanagementstructureattheRegionalandDistrictHealthDirectorates.Withinthiscontexttheneedhasbeenexpressedto encourage and train Regional and District HR Managers to effectively perform humanresourcemanagementfunctions.StaffAttrition:Theexistinghealthworkforceisaffectedbyattritionofexistinghealthworkersbothpublicandprivate. Fromavailable information, itwould appear that the overall attrition of professionalhealth workers is on the decline due to the several positive interventions undertaken bygovernmentbetween2001 to2007, including the recentupsurge inproduction interventions.The recent public payroll analysis also confirms a general decline in attritionparticularly after2006. However, a recentMoH analysis indicates that retirement from the sector as againstother reasons, standsas themost consequential reason forattritionbetween2004and2008.The picture and trend is worrisome given that majority of the health workers on the publicpayrollareyoungandrelativelyinexperienced(25-35yearsofage),anditisestimatedthatsome14,439healthworkerswillreachthemandatoryageofretirementinthenexttenyears.
Figure1.Agedistributionofhealthworkforce,Aug.2008Source:AntwiandEkey,2009
54MoH:HumanResourcePolicyandStrategiesfortheHealthSector,2007-201155GhanaHealthService:HumanResourceDivision,3YearActivityPlan2009-2011.May2009.56GhanaHealthService,2008ANNUALREPORT.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|64
Conclusions:
Thefiveyearprogrammeofworkoutlinedclearstrategies to improvetheworkforceeffectivenessand performance. TheMoH has taken bold strides towards attaining the stated objectives in thePOW2007-2011 including taking actions to improvehealthworkersmotivation, formationof taskteam to streamline policy on training and granting of study leave, quota system for study leave,creationofestablishmentforpostbasiccourses(Postbasicnursing,inEye,ENT,andintensivecare)review of staff grading structure and promotion system for the variousMoH agencies to ensureharmonization. Already the MoH and its agencies have also taken positive steps to increaseproduction of healthworkers especiallymiddle level cadres and ongoing efforts are on course tobetterequipandenhancetheoperationaleffectivenessofhealthworkers.While commendable achievements have been recorded, three important challenges requiringurgentattentionarenoted.Firstly,thescarceavailabilityofreliabledataforaccurateplanningandanalysistoachieveacomprehensivepictureofissuesandrequirements.Secondly,unconfirmeddataon impending retirements seem to indicate that the health workforce is still faced with hugeattritionarisingfromthemandatoryretirementageof60years.Thistrendisworrisomegiventhatmajority of the healthworkers on the public payroll are young and relatively inexperienced. It isestimatedthatsome14,439healthworkerswillreachthemandatoryageofretirementinthenextten.Inaddition,weobservetheabsenceofanapprovedplantoaddressdeploymentdisparitiesinthehealthworkforcedistributionanddevolutionofHRmanagementfunctionstodistricts.Recommendations:
Thefollowingarethemainconclusionsfromthisreview:
• Thereisanurgentneedtoundertakeupwardreviewthemandatoryretirementagepolicyfrom60 to65years, in viewof thepotential lossofhighly skilledandexperiencedhealthworkerswithinthenexttenyears.
• Explore opportunities to devolve HR management functions-(including training,recruitment,deployment,incentives,disciplineandpayrollmanagement).
• Decentralizemanagementandgovernanceofhealthtrainingschools.• Establish a system for effective regulation and accreditation of middle level health
workers: promote investment to address weakness in the curriculum contents, theaccreditation process, quality improvements in student/teacher imbalance, provision ofessentiallearningmaterialsinessentialinfrastructure,laboratoryequipment,andfunctionalutilitiesincludingelectricity,waterprovisionandsystemforHRdatacollectionandanalysis)
Toachievetheaboverecommendation,majorincreaseinfundingbothrecurrentfundingandcapitalinvestmenttoscaleupqualityofeducationandinfrastructureforprimaryhealthcareisenvisagedasessentialtoachievestatedgoalsandobjectivesoftheMoHpolicydocumentof2007–theHRHPolicies,StrategiesandPlans(2007-2011).
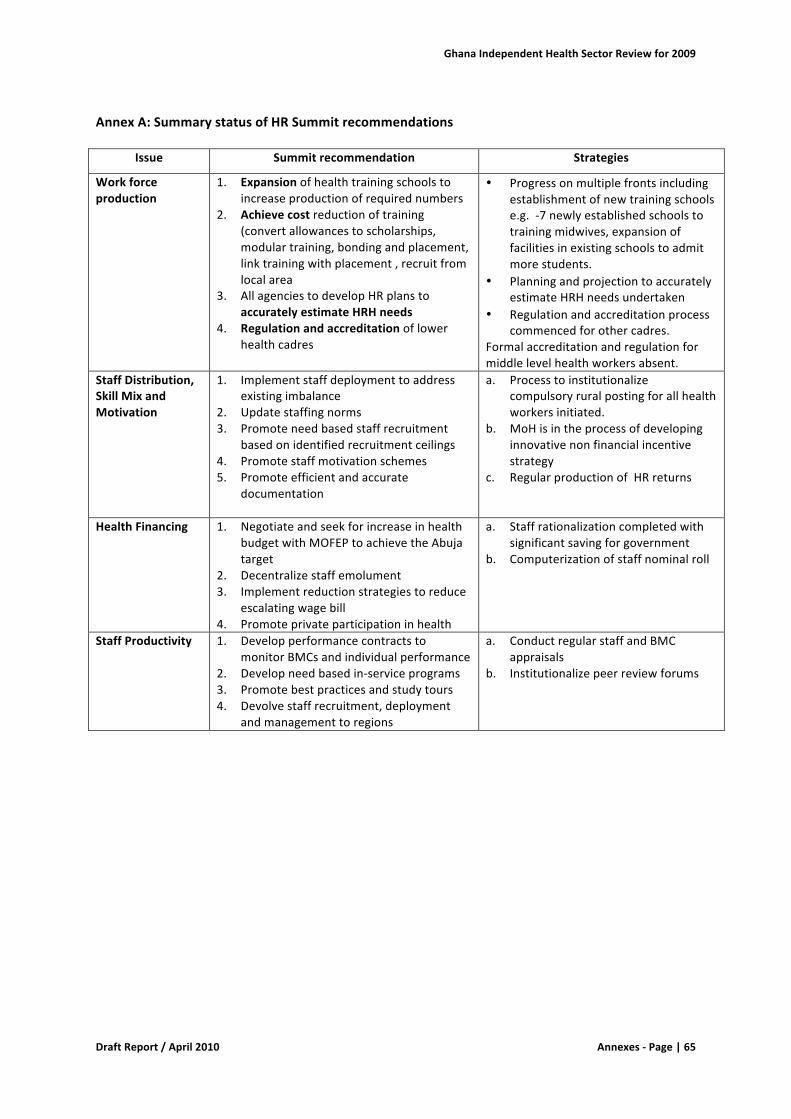
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|65
AnnexA:SummarystatusofHRSummitrecommendations
Issue Summitrecommendation Strategies
Workforceproduction
1. Expansionofhealthtrainingschoolstoincreaseproductionofrequirednumbers
2. Achievecostreductionoftraining(convertallowancestoscholarships,modulartraining,bondingandplacement,linktrainingwithplacement,recruitfromlocalarea
3. AllagenciestodevelopHRplanstoaccuratelyestimateHRHneeds
4. Regulationandaccreditationoflowerhealthcadres
• Progressonmultiplefrontsincludingestablishmentofnewtrainingschoolse.g.-7newlyestablishedschoolstotrainingmidwives,expansionoffacilitiesinexistingschoolstoadmitmorestudents.
• PlanningandprojectiontoaccuratelyestimateHRHneedsundertaken
• Regulationandaccreditationprocesscommencedforothercadres.
Formalaccreditationandregulationformiddlelevelhealthworkersabsent.
StaffDistribution,SkillMixandMotivation
1. Implementstaffdeploymenttoaddressexistingimbalance
2. Updatestaffingnorms3. Promoteneedbasedstaffrecruitment
basedonidentifiedrecruitmentceilings4. Promotestaffmotivationschemes5. Promoteefficientandaccurate
documentation
a. Processtoinstitutionalizecompulsoryruralpostingforallhealthworkersinitiated.
b. MoHisintheprocessofdevelopinginnovativenonfinancialincentivestrategy
c. RegularproductionofHRreturns
HealthFinancing
1. NegotiateandseekforincreaseinhealthbudgetwithMOFEPtoachievetheAbujatarget
2. Decentralizestaffemolument3. Implementreductionstrategiestoreduce
escalatingwagebill4. Promoteprivateparticipationinhealth
a. Staffrationalizationcompletedwithsignificantsavingforgovernment
b. Computerizationofstaffnominalroll
StaffProductivity
1. DevelopperformancecontractstomonitorBMCsandindividualperformance
2. Developneedbasedin-serviceprograms3. Promotebestpracticesandstudytours4. Devolvestaffrecruitment,deployment
andmanagementtoregions
a. ConductregularstaffandBMCappraisals
b. Institutionalizepeerreviewforums
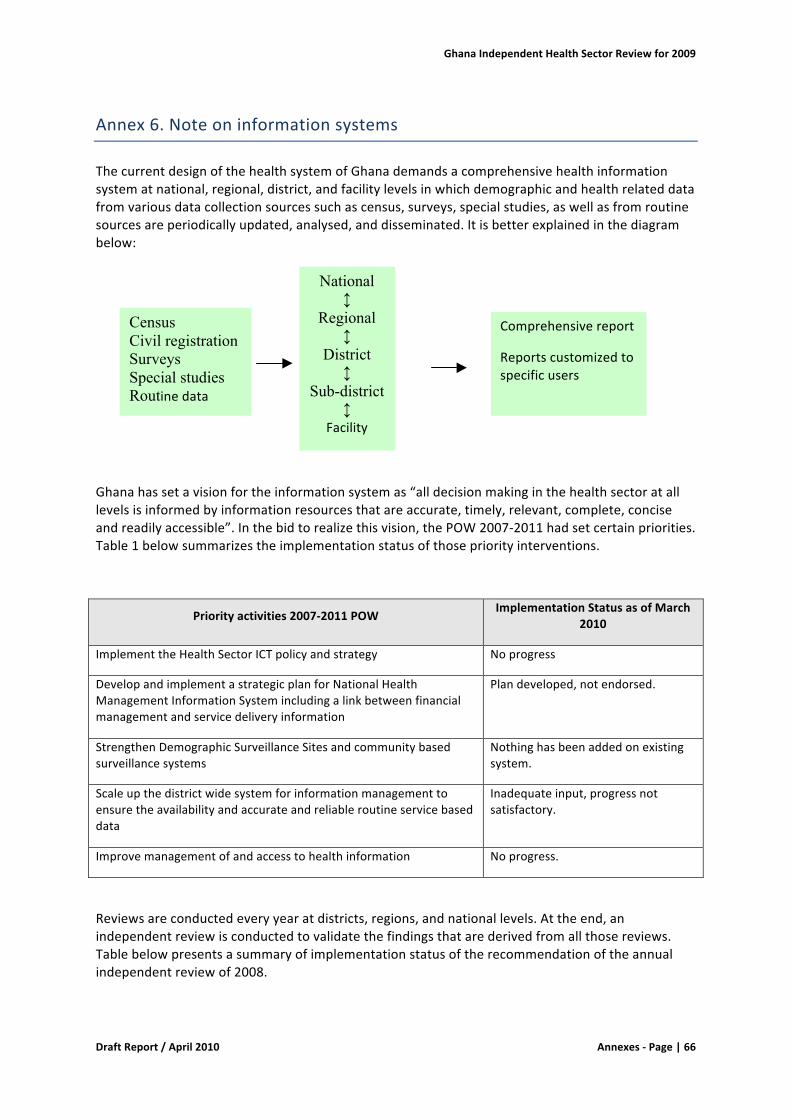
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|66
Annex6.Noteoninformationsystems
ThecurrentdesignofthehealthsystemofGhanademandsacomprehensivehealthinformationsystematnational,regional,district,andfacilitylevelsinwhichdemographicandhealthrelateddatafromvariousdatacollectionsourcessuchascensus,surveys,specialstudies,aswellasfromroutinesourcesareperiodicallyupdated,analysed,anddisseminated.Itisbetterexplainedinthediagrambelow:
Ghanahassetavisionfortheinformationsystemas“alldecisionmakinginthehealthsectoratalllevelsisinformedbyinformationresourcesthatareaccurate,timely,relevant,complete,conciseandreadilyaccessible”.Inthebidtorealizethisvision,thePOW2007-2011hadsetcertainpriorities.Table1belowsummarizestheimplementationstatusofthosepriorityinterventions.
Priorityactivities2007-2011POWImplementationStatusasofMarch
2010
ImplementtheHealthSectorICTpolicyandstrategy Noprogress
DevelopandimplementastrategicplanforNationalHealthManagementInformationSystemincludingalinkbetweenfinancialmanagementandservicedeliveryinformation
Plandeveloped,notendorsed.
StrengthenDemographicSurveillanceSitesandcommunitybasedsurveillancesystems
Nothinghasbeenaddedonexistingsystem.
Scaleupthedistrictwidesystemforinformationmanagementtoensuretheavailabilityandaccurateandreliableroutineservicebaseddata
Inadequateinput,progressnotsatisfactory.
Improvemanagementofandaccesstohealthinformation Noprogress.
Reviewsareconductedeveryyearatdistricts,regions,andnationallevels.Attheend,anindependentreviewisconductedtovalidatethefindingsthatarederivedfromallthosereviews.Tablebelowpresentsasummaryofimplementationstatusoftherecommendationoftheannualindependentreviewof2008.
National ↕
Regional ↕
District ↕
Sub-district ↕
Facility
Comprehensivereport
Reportscustomizedtospecificusers
Census Civil registration Surveys Special studies Routinedata
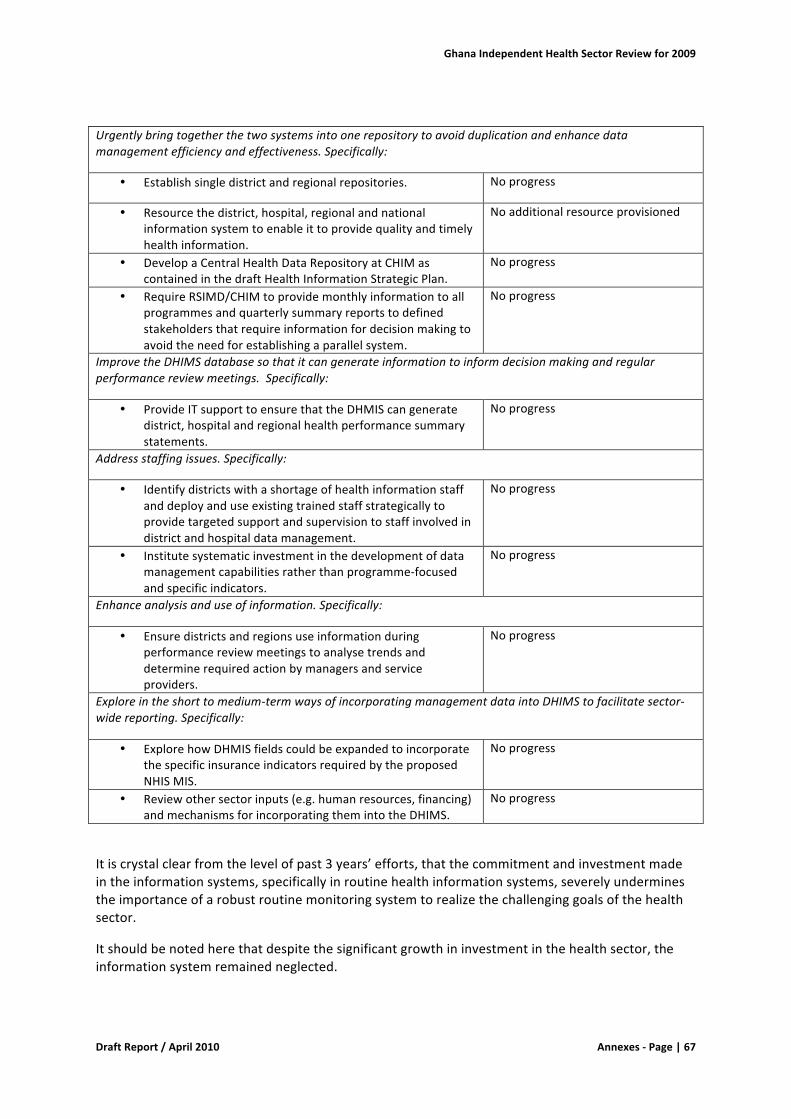
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|67
Urgentlybringtogetherthetwosystemsintoonerepositorytoavoidduplicationandenhancedatamanagementefficiencyandeffectiveness.Specifically:
• Establishsingledistrictandregionalrepositories. Noprogress
• Resourcethedistrict,hospital,regionalandnationalinformationsystemtoenableittoprovidequalityandtimelyhealthinformation.
Noadditionalresourceprovisioned
• DevelopaCentralHealthDataRepositoryatCHIMascontainedinthedraftHealthInformationStrategicPlan.
Noprogress
• RequireRSIMD/CHIMtoprovidemonthlyinformationtoallprogrammesandquarterlysummaryreportstodefinedstakeholdersthatrequireinformationfordecisionmakingtoavoidtheneedforestablishingaparallelsystem.
Noprogress
ImprovetheDHIMSdatabasesothatitcangenerateinformationtoinformdecisionmakingandregularperformancereviewmeetings.Specifically:
• ProvideITsupporttoensurethattheDHMIScangeneratedistrict,hospitalandregionalhealthperformancesummarystatements.
Noprogress
Addressstaffingissues.Specifically:
• Identifydistrictswithashortageofhealthinformationstaffanddeployanduseexistingtrainedstaffstrategicallytoprovidetargetedsupportandsupervisiontostaffinvolvedindistrictandhospitaldatamanagement.
Noprogress
• Institutesystematicinvestmentinthedevelopmentofdatamanagementcapabilitiesratherthanprogramme-focusedandspecificindicators.
Noprogress
Enhanceanalysisanduseofinformation.Specifically:
• Ensuredistrictsandregionsuseinformationduringperformancereviewmeetingstoanalysetrendsanddeterminerequiredactionbymanagersandserviceproviders.
Noprogress
Exploreintheshorttomedium-termwaysofincorporatingmanagementdataintoDHIMStofacilitatesector-widereporting.Specifically:
• ExplorehowDHMISfieldscouldbeexpandedtoincorporatethespecificinsuranceindicatorsrequiredbytheproposedNHISMIS.
Noprogress
• Reviewothersectorinputs(e.g.humanresources,financing)andmechanismsforincorporatingthemintotheDHIMS.
Noprogress
Itiscrystalclearfromthelevelofpast3years’efforts,thatthecommitmentandinvestmentmadeintheinformationsystems,specificallyinroutinehealthinformationsystems,severelyunderminestheimportanceofarobustroutinemonitoringsystemtorealizethechallenginggoalsofthehealthsector.
Itshouldbenotedherethatdespitethesignificantgrowthininvestmentinthehealthsector,theinformationsystemremainedneglected.

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|68
Thenexttwosectionsofthischapterpresentthebriefdiscussionon“theachievementsandconstraintsinoverallinformationmanagement”followedby“howwelltheavailableinformationisbeingusedindecisionmaking”.
a)Progressmadeandchallengesofsinglereportingsystemsandoverallsystemsfordatacollection,validation,storageandanalysis
Duringthelasttwodecades,theinformationmanagementinthehealthsectorhasbeenthesubjectofseveralreviews,development,andimprovement.Yet,themanagementofroutinehealthinformation(thatincludesdiseaseandservicestatistics,humanresource,finance,logisticsandsupplies,physicalassets,etc.)facesthesamechallenge.Thesystemdoesnothaveappropriatehumanresources,reasonablebudgetsupport,andappropriateequipmentandmaterials.
DistrictHealthInformationManagementSoftware(DHIMS):
TheDistrictHealthInformationManagementSoftware(DHIMS)aimsatintegratingtheinformationmanagementatthedistrictlevel.Itprovidesaplatformforinputtinganydatathatthehealthsectorgathers.NationwiderolloutofDHIMSindeedwasaremarkableachievementinthehistoryofdevelopmentofhealthinformationsystemsinthecountry.However,theDHIMShasseveraldeficiencies.ItdoesnotincludeTBandHIVdata.ItdoesnotcapturesomeRCHdata,whichhasbeenmadeacaseforjustifyingaparallelreporting.Itappearsthatthereareproblemsinmalaria,nutrition,andmorbiditymodules.TheselatterissuesaresimpleandstraightforwardandbeingfixedbyCHIMwithafinancialsupportfromtheMalariacontrolprogram.ThemainweaknessinDHIMSisthelackofmenudrivenreportmodulestogeneratecomprehensivereport,dashboardreports,andprogramspecificcustomizedreports.Intheabsenceofthesefeatures,theutilityofDHIMShasbeenconfinedtodatastorage.
Despiteseveralrecommendationsmadeinthepast,theinformationsystemisstillsufferingfromlackofappropriateICTequipmentandothersupplies.
Maximizingtheuseofavailableresourcesisanothermissedopportunityobservedyearafteryear.SatellitedishesinstallednationwideatfacilitylevelcouldbeusedmoreeffectivelythanonlytransferringdatatoNHIA.Itcanbeusedfortelemedicine,distanceeducation,generalcommunication,andtransferringthehealthinformation.
DataCollection
Datarequiredformanagingtheindividualcases,managingthehealthunit,andmanagingthehealthsystemiswellcapturedinthedatacollectioninstruments(registers,cards,forms).TheDHIMSdatabasealreadycontainsawealthofpermanentandsemi-permanentdata.Thecurrentdatacollectiontoolsandsystemsareadequateforaddressingtheinformationneedsofthesector.
Reporting
Informationneededformanagingthehealthsectorisgatheredfromvariousnon-routineandroutinedatasources.Theseincludecensus,periodicsurveys,adhocstudies,androutinereportsofhealthfacilities.Eachsourcehasitsspecificpurposeanditslimitations.Dataisroutinelygatheredtomonitorkeyperformanceindicatorsandtosupportongoingmanagementofhealthprograms.Variouskindsofsurveysareconductedtogatheradditionaldatawhichcannotbegatheredthroughroutinesources.Contrarytothisprinciple,mostmonthlyreportingformshavebeendesignedtocollectdataintediousdetailthatarerarelyusedinroutinemonitoringandongoingmanagementofthehealthsystem.Asaresult,healthworkersareoverburdened,dataqualityisdeterioratingandreportingdeadlinesaremissed.Dataonvariousagegroups,genderandothervariablesthatmight

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|69
beusefulinpolicyandstrategicplanningcanbegatheredmoreefficientlyandscientificallythroughannualorbiannualreviewoffacilitybasedrecords.
Dataquality
Dataonthecollectiontoolsaregenerallycomplete.However,errorsareoftenmadewhilecompilingdataintovariousvariablesandtranscribingthemintoreportforms.Compilationofdataontoomanyvariablesistediousandhighlyerrorprone.
Errorsarealsomadeathigherlevelswhileaggregatingdatafrommultiplesources.Differentdatavaluesaregeneratedfromdifferentdepartmentswhilethesourceofthedataisthesame.Thisremainsunresolvedaslongasmorethanonereportingchannelismaintainedforreportingthesamedata.
AmostimportantfeatureinDHIMSisthatdatavalueenteredatdistrictlevelcannotbechangedatregionalornationallevels.Ifacorrectionisrequired,ithastobedoneatthepointoforiginalentry.Further,DHIMSmaintainsdisaggregationofdatabyhealthfacilityorspecificprovidermakingitpossibletoverifyareportedvalueatanylevelatanytime.
DataanalysisandDissemination
Dataanalysisanddisseminationiswoefullyweakacrossalllevels.Mostdataarerarelyanalysedandusedatthepointofcollection.ThedistrictsthatreceivetheplethoraofdataonmonthlyreportsmostlyusetheirtimeinenteringthedataintoDHIMSandforwardingtotheregions.Routineanalysisanddisseminationisnotapriority.ThesameappliestotheregionsandMoHheadquarters.
Areportproducedatanylevelhasnevercoveredmorethan25percentofdataavailableonthereportingforms.Itclearlyindicatesthatalotofdataisgatheredwhichisneveranalysedandused.
Contrarytopoorroutineanalysisanddissemination,theproductionofannualreportshasevolvedasastandardpracticeorcultureatalladministrativelevels.Currently,thecontentandformatofannualreportsarenotuniform.Itwouldbeidealforeachleveltouseastandardannualreporttemplateasaminimumrequirement.
Visualdisplayonkeyindicatorsbymeansofwallchartsandgraphsisapowerfultooltodrawattentiononkeyissues.Theycanbeusedtokeepone-selfremindedonthepertinentissueaswellastoeducateorinformothers.ExceptaverydetailedcrowdedchartonGuineaWormsurveillancedata,barelyanychartwasfounddisplayedatanyinstitutionthereviewteamvisited.
TheMoHwhostartedpublishingthehealthinformationbulletinin2000stoppedpublishingafterafewerraticpublicationsupto2004.Thetitleofthebulletin“informationforaction”wasappropriate,thoughthecontentandlevelofanalysiswasmoreacademicthanquickactionable.Regardless,itwasanoblestartofinformationdissemination.Theministrymustreinstateperiodicpublicationwithmoresimplifiedgraphsandchartsandlesstextualdescriptionsmakingitsuitabletoitspurpose“informationforaction”.
b)ExtenttowhichdataisusedinDecisionmakingandfeedback
Annualreview
Annualjoint/peerreviewshavebeeninstitutionalisedatalllevels.Datafromvarioussourcesarecompiledandpresentedinthereviews.However,thosereviewsareconsideredhigherlevelrequirementsratherthananopportunitytoreflectonownperformance.

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|70
Theindependentreviewteamhadanopportunitytoobservetheinteragencylevelreviewwhereallnationalstakeholderswereexpectedtotakepart.Itisnotedthatmostpresentationsdidnotfollowthereviewguidelines.Planswerenotlinkedtoachievementsandexplanationsregardingperformancewerelargelymissing.Manystakeholderswereabsentduringvariouspresentations.
Routinemonitoring
Routinedataisprimarilymeantforongoingmonitoringandtakingcorrectiveactions.Correctiveactionstimelyintroducedcouldhelpachieveplannedresults.Ifroutinelycollecteddataarenotusedintrackingprogressandtakingcorrectivemeasures,nootherreasoncanjustifythecollectionofroutinedata.Routinedataismoreexpensivethanthedatacollectedfromcensusorsurveys.Thereportingforms,humanresources,healthworkerstimeandITenvironmentaltogetherconsumesalotofresources.
Awellstructuredandproperlyusedroutinemonitoringsystemcanmaketremendousdifferencesinservicedeliveryifthedeliverypointhassomeresourcesatitsdiscretion.Sincefacilitiesgeneratesomeresources,asimplesystematicmonitoringsysteminstitutedathealthfacilitiescanmakeimportantimpact.
Exceptionally,andbecauseofpoliticalfocus,someindicatorssuchasmaternaldeathsandguineawormcasesarebeingstrictlymonitoredatalllevels.Butgenerallydistricts,regionsandnationalprogramsareequallyweakinroutinemonitoringandtakingcorrectivemeasures.Despitetheplethoraofdataavailableinthecurrentroutinereportingsystem,theiruseinongoingmonitoringofperformanceisextremelylow.Infact,thehealthfacilitieslacknecessarytoolsandguidelines.
Holisticassessmentversussub-district,districtandregionalleaguetables
Aholisticassessmentconcepthasbeenintroducedaspartoftheannualperformancereviewwithapositive,neutralandnegativescorebasedonachievementornon-achievementofsetmilestonesandsector-wideindicators.Then,allscoresaresummeduptoderiveasinglesummarymeasure.Thisisgoodforassessingtheglobalperformanceofthesector.Tomaketheresultantscoreusefulfortakingactionsatsub-nationallevels,itwouldbeveryappropriatetointroducealeaguetableconcepttoranktheannualperformanceofhealthfacilities,districts,regions,andvariousnationalprograms.Itwouldencourageandincitethestakeholdersforbetterperformance.
Cautionshouldbeexercisedwhileselectingtheindicatorsfortheleaguetableandassigningthevaluetoeachofthem.Leaguetablesshouldusefivetosevenindicatorsfromthelistusedfortheholisticassessment.Itshouldcovertheindicatorsofvariousperformancedomainssuchasusersatisfaction,coverageofservice,qualityofservice,efficiency,andequity.Itmustrevealwhoisdoingbest–andworst–tomeetinghealthneedsofthepopulation;andwhohasachievedthegreatestchangeovertheyearunderreview.
Feedbackonindividualreport
Thefeedbackprocessshouldstartrightatthehealthfacility.Oncetheresponsiblepersonsubmitsamonthlyreporttothefacilityin-charge,aninternalreviewandfeedbackmeetingshouldbeorganized.Atthedistrict,thepersonresponsibleforreceivingthefacilityreportsshouldbrowsethroughthereportfordataconsistencyandmakeafollow-upwiththeconcernedfacilityforanyerrorsandomissions.ThenthedatashouldbeenteredintoDHIMS,analyzed,comparativechartscreatedonkeyindicators,thedashboardreportgeneratedanddiscussedintheDHMT,andsentbacktothehealthfacilities.Thefacilitydatacouldbeusedfordiscussiononinterpretationandactionstobetakenduringafollow-upsupervisoryvisitatthefacility.Thesameproceduresshouldberepeatedattheregionalandnationallevel.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|71
Theabovefeedbackprocessisnothappeningformanyreasons.Firstly,thisconceptisnotunderstoodbythosewhoaresupposedtopracticeit.Secondly,theresourcesrequiredtosendwrittenfeedbackarenotavailable.
Recommendations
1. Provideaseparatebudgetlineforthehealthinformationsystemandallocateadequateresources(foroperatingandmaintainingthesystem;fortrainingandappropriatelevelsofHR;andforregularreplacement/updatingoftheITenvironment);
2. FixtheproblemsinDHIMSandaddthemenudrivenmodulestogeneratedashboardreportandprogramspecificcomprehensivereports.CreateandlinkpivottablestoDHIMS(asinHISPdatabase)andmakethemavailabletothestakeholdersthroughtheMoHwebsite;
3. Equiptheinformationunitatdistrict,region,agencylevelsandatMoHwithfunctionalcomputers,A3printers,antivirussoftware,internetconnection,andanannualbudgettomaintainthesystemandgeneratethedashboard,quarterlyandperiodicreports;
4. StrengthenthenecessaryskillsofallHIOstoanalysedata,generatedashboard,feedback,andcomprehensiveperformancereports,andfurthermosttodisseminatetheinformationtodecisionmakersandfacilitatetheuse.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|72
Annex7.Noteoncapitalinvestment
1. BackgroundReviewsundertakenin2006ontheCapitalInvestmentPlanII(2002–2006)assessedthesectorasoverdevelopingfacilitiesandequipmentinsomelocationsandunder-investinginotherareas,whilstexpandingthepubliclyprovidedhealthservicesbeyondthe limitsofavailableoperatingfundsandprofessional staffing. Added to these challenges were changes in the political and economicenvironment,includingthemovementofsomeDPstoMultiDonorBudgetSupport(MDBS),andtheintroductionoftheGrowthandPovertyReductionStrategy(GPRSII).InpreparingtheCapitalInvestmentPlanIII(CIPIII,2007–2011),thestrategyofequityandaccesstoqualityhealthcarestillremainedtheprimaryfocus,asameanstoachievingtheMDGs.Themajorobjectiveof theCIP IIIwasdefinedas focusingon increasinggeographicalaccess,wellmaintainedhealthfacilitiesandhealthenhancinginfrastructurewithemphasisondeprivedandperi-urbanareas.Thisobjectivewasderived fromStrategicObjective3of theoverall sector2007-2011POW,whichaimed at strengthening health system capacity to expand, manage and sustain high coverage ofservicesThelong-terminvestmentframeworkfortheCIPIIIwasbuiltonthefollowingkeyelements:
1) Over time, to re-appraise and subsequently to re-prioritise ongoing and proposed newprojects, so as to adequately link investment policy and planning with the objective ofimprovingservicedelivery;
2) ToengineerashiftinresourceallocationstowardstheprimarylevelandtheachievementoftheMDGs,basedonclearandobjectiveprocessesandcriteriaappliedbytheregionalanddistricthealthauthorities;
3) Tomoveaway from the centralizedplanningmodel thathasbeenappliedover theyears,andgreatlyimprovingcollaborationwiththepoliticalauthoritiesatthedecentralizedlevel;and
4) To promote the use of alternative financing mechanisms, based on increased levels ofprivate sector participation, for the upgrading and expansion of regional and teachinghospitals,aswellastheconstructionoffacilitiesforstatutorybodies.
Basedongrowthrates fromActualexpenditureduring theCIP IIperiod, theCIP IIIprojectedtotalresources available of $511million for the five-year CIP III period, an average capital investmentinflow of about $100 million per year. However funding constraints encountered in 2008 hadresulted in a 50% cut in the GOG capital investment budget allocation for that year, and aconsequentaccumulationofunpaidbillstocontractors.Againstthisbackground,theannualCIPfor2009defineditsexpenditureprioritiesasfollows:• CommitmentssuchasMatchingFundsrequiredforprojectsfundedundermixedcredits/grants
andpaymentofaccumulateddebtsfrom2008;• Projectswith100%secured/earmarkedfunding;• Ongoingprojectsprocuredunderinternationalcompetitivetenderingwithlegalimplicationsfor
GOGarisingfromdelaysinpayments;• Ongoingprojectswithhighlevelofcompletionandsubstantialsunkcostthatcanbecompleted
in2009;
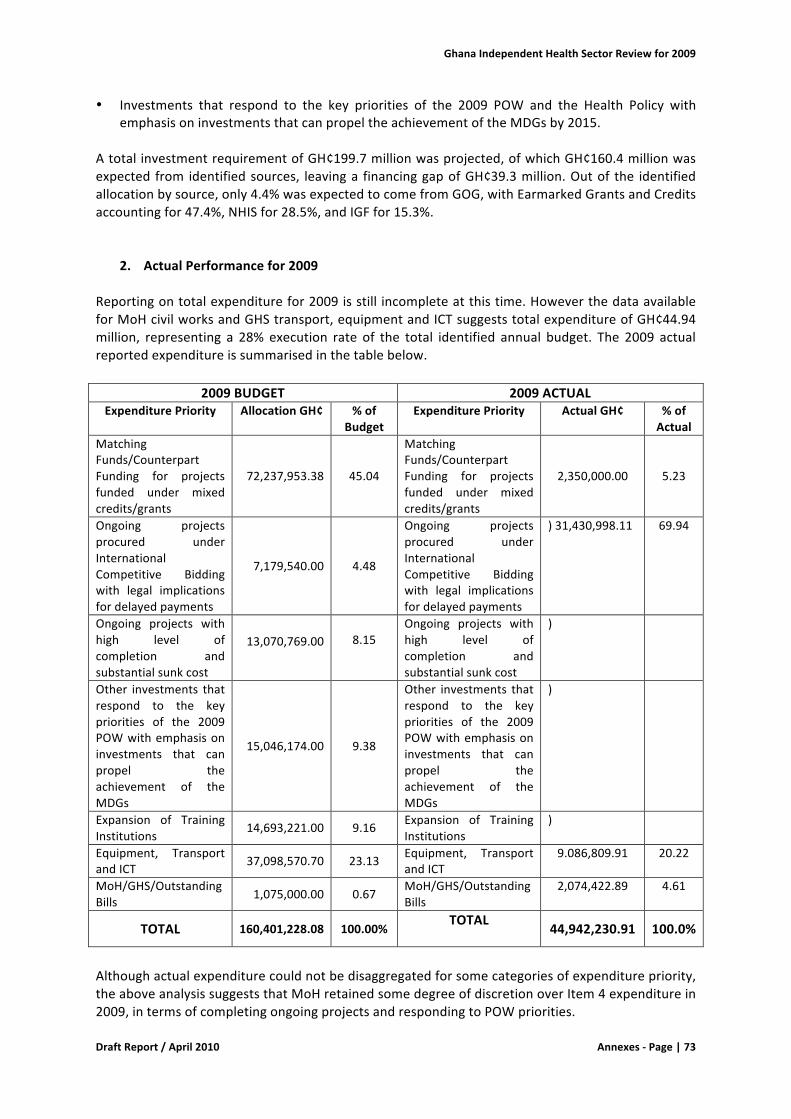
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|73
• Investments that respond to the key priorities of the 2009 POW and the Health Policy withemphasisoninvestmentsthatcanpropeltheachievementoftheMDGsby2015.
AtotalinvestmentrequirementofGH¢199.7millionwasprojected,ofwhichGH¢160.4millionwasexpected from identifiedsources, leavinga financinggapofGH¢39.3million.Outof the identifiedallocationbysource,only4.4%wasexpectedtocomefromGOG,withEarmarkedGrantsandCreditsaccountingfor47.4%,NHISfor28.5%,andIGFfor15.3%.
2. ActualPerformancefor2009Reportingontotalexpenditurefor2009isstill incompleteatthistime.HoweverthedataavailableforMoHcivilworksandGHStransport,equipmentandICTsuggeststotalexpenditureofGH¢44.94million, representing a 28% execution rate of the total identified annual budget. The 2009 actualreportedexpenditureissummarisedinthetablebelow.
2009BUDGET 2009ACTUALExpenditurePriority AllocationGH¢ %of
BudgetExpenditurePriority ActualGH¢ %of
ActualMatchingFunds/CounterpartFunding for projectsfunded under mixedcredits/grants
72,237,953.38 45.04
MatchingFunds/CounterpartFunding for projectsfunded under mixedcredits/grants
2,350,000.00
5.23
Ongoing projectsprocured underInternationalCompetitive Biddingwith legal implicationsfordelayedpayments
7,179,540.00
4.48
Ongoing projectsprocured underInternationalCompetitive Biddingwith legal implicationsfordelayedpayments
)31,430,998.11 69.94
Ongoing projects withhigh level ofcompletion andsubstantialsunkcost
13,070,769.00 8.15
Ongoing projects withhigh level ofcompletion andsubstantialsunkcost
)
Other investments thatrespond to the keypriorities of the 2009POWwithemphasisoninvestments that canpropel theachievement of theMDGs
15,046,174.00
9.38
Other investments thatrespond to the keypriorities of the 2009POWwithemphasisoninvestments that canpropel theachievement of theMDGs
)
Expansion of TrainingInstitutions
14,693,221.00 9.16 Expansion of TrainingInstitutions
)
Equipment, TransportandICT 37,098,570.70 23.13 Equipment, Transport
andICT 9.086,809.91 20.22
MoH/GHS/OutstandingBills 1,075,000.00 0.67
MoH/GHS/OutstandingBills
2,074,422.89 4.61
TOTAL 160,401,228.08 100.00%TOTAL
44,942,230.91 100.0%
Althoughactualexpenditurecouldnotbedisaggregatedforsomecategoriesofexpenditurepriority,theaboveanalysissuggeststhatMoHretainedsomedegreeofdiscretionoverItem4expenditurein2009,intermsofcompletingongoingprojectsandrespondingtoPOWpriorities.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|74
The analysis of 2009 actual capital expenditure by level (civil works only) shows a significantweighting in favour of the primary level,with 74% of expenditure at the District and Sub-Districtlevel, and a further 8% being spent on infrastructure at the Training Institutions, in linewith theoverallsectorpolicydirection.2009Achievement–CivilWorksAchievementsincivilworksaregroupedunderthreeheadings,namelyinitiationofturnkeyprojects;full completion of ongoing projects; completion of preparatory works for turnkey and bilateralsponsoredprojects;andreactivationofabandonedprojectsintheAccra–TemaMetropolis.Initiationofmajorturnkeyprojects:Constructionof100-bedHospitalwithMalariaResearchCentreat Teshie, Accra with Chinese Government funding; Construction of 5 Polyclinics with specializedmaternityfacilitiesinNorthernRegionatKaraga,Buipe,Kpandai,Tatale,JangaandChereponiwithfinancial support from the Austrian Government; Construction of District Hospital at BekwaiwithADBfunding;andConstructionofWinnebaDistrictHospitalwithDutchORETfunding.Fullcompletionofongoingprojects:FeasibilitystudyandfundmobilizationforthedevelopmentofaMaternityandChildren’sHospitalatRidgeHospital,Accra;10newHealthCentreswithfundingfromOPEC; GHS Head Office complex at Limb Fitting Centre, Accra; Facilities in the following Nurses’Training Colleges: Tamale NTC, Akim Oda CHNTS, Ashanti-Mampong MTS/HATS; and Phase 1 ofBolgatangaRegionalHospital.Completion of preparatory works including Value For Money Audits, negotiations and Statutoryapprovals for the implementation of the following proposed turnkey and bilateral-sponsoredprojects:MajorrehabilitationandupgradingofTamaleTeachingHospitalwithDutchORETfunding;Re-equippingof13laundryfacilitiesinselectednationwidehospitalswithBelgian/KBCBankfunding;ExpansionofRadiotherapyandNuclearMedicinefacilityatKATHandKBTHwithOPECandBADEAfunding; Development of 2 Regional Hospitals and staff housing atWa and Kumasi with Eurogetfinancing; Development of District Hospitals and staff housing at Madina/Adenta in Accra, Tepa,Salaga,Nsawkaw,Konongo-Odumasi,andTwifo-Praso;Phase2ofBolgatangaRegionalHospital;and5 new Health Centres nationwide and 3 District Hospitals with Abu Dhabi and OPEC fundingrespectively.Reactivation of abandoned projects in the Accra – Tema Metropolis: Usher Polyclinic Theatre;MaternityBlockatAchimotaHospital;UpgradingofMaamobi,KaneshieandMamprobiPolyclinics;andMaternityandChildren’sBlockatTemaGeneralHospital.2009Achievements-TransportThemain achievements for transport were the procurement of 4,000motorbikes, funded in themain through earmarked funds (Malaria, TB, HIV/AIDS, etc). Due to their funding sources, thedeploymentofthesemotorbikeshastargetedpublichealthprogrammes,leavingouthospitals.Thelatter,togetherwiththeDHMTs,arebeingencouragedtotakeuptheopportunityofacquiringpick-upsthroughahirepurchaseschemearrangedbytheMinistry,underwhichMoHhaspaidtheinitial30% of the cost while the beneficiaries are expected to pay the balance at a monthly cost ofGH¢1,500pervehicle.
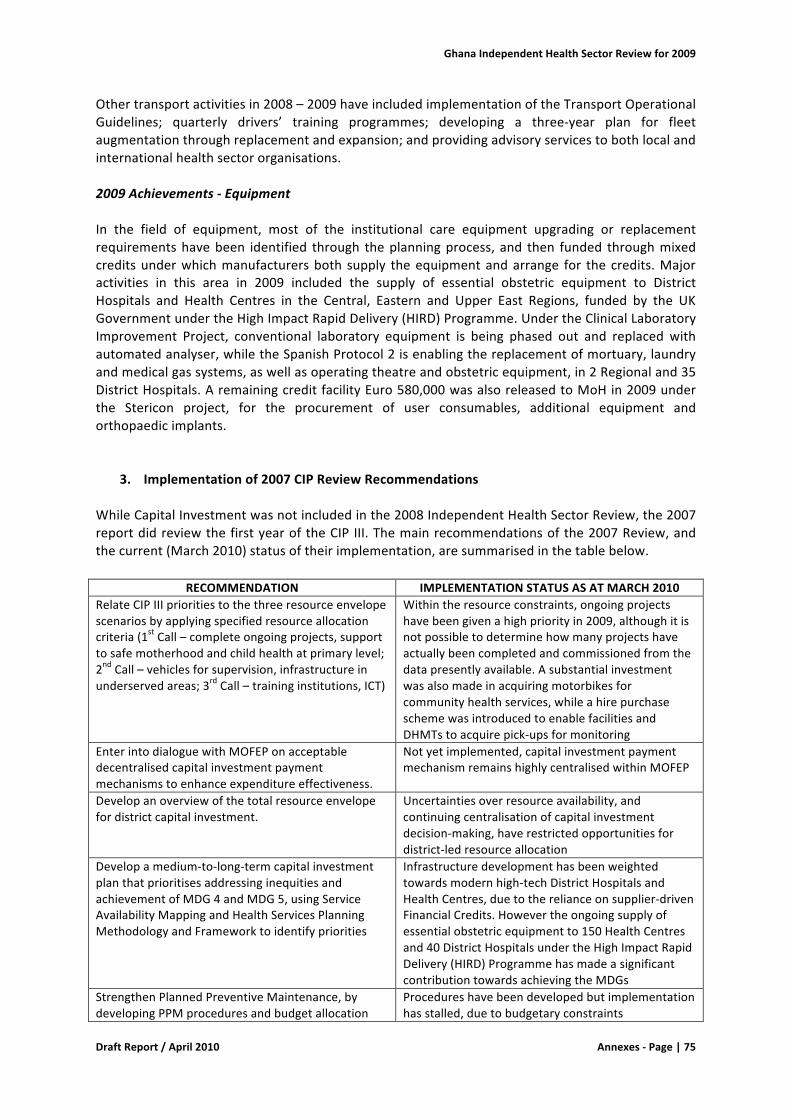
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|75
Othertransportactivitiesin2008–2009haveincludedimplementationoftheTransportOperationalGuidelines; quarterly drivers’ training programmes; developing a three-year plan for fleetaugmentationthroughreplacementandexpansion;andprovidingadvisoryservicestobothlocalandinternationalhealthsectororganisations.2009Achievements-EquipmentIn the field of equipment, most of the institutional care equipment upgrading or replacementrequirementshavebeen identified through theplanningprocess, and then funded throughmixedcreditsunderwhichmanufacturersboth supply theequipmentandarrange for the credits.Majoractivities in this area in 2009 included the supply of essential obstetric equipment to DistrictHospitals and Health Centres in the Central, Eastern and Upper East Regions, funded by the UKGovernmentundertheHighImpactRapidDelivery(HIRD)Programme.UndertheClinicalLaboratoryImprovement Project, conventional laboratory equipment is being phased out and replaced withautomatedanalyser,whiletheSpanishProtocol2isenablingthereplacementofmortuary,laundryandmedicalgassystems,aswellasoperatingtheatreandobstetricequipment,in2Regionaland35DistrictHospitals.AremainingcreditfacilityEuro580,000wasalsoreleasedtoMoHin2009underthe Stericon project, for the procurement of user consumables, additional equipment andorthopaedicimplants.
3. Implementationof2007CIPReviewRecommendationsWhileCapitalInvestmentwasnotincludedinthe2008IndependentHealthSectorReview,the2007reportdidreviewthefirstyearoftheCIP III.Themainrecommendationsofthe2007Review,andthecurrent(March2010)statusoftheirimplementation,aresummarisedinthetablebelow.
RECOMMENDATION IMPLEMENTATIONSTATUSASATMARCH2010RelateCIPIIIprioritiestothethreeresourceenvelopescenariosbyapplyingspecifiedresourceallocationcriteria(1stCall–completeongoingprojects,supporttosafemotherhoodandchildhealthatprimarylevel;2ndCall–vehiclesforsupervision,infrastructureinunderservedareas;3rdCall–traininginstitutions,ICT)
Withintheresourceconstraints,ongoingprojectshavebeengivenahighpriorityin2009,althoughitisnotpossibletodeterminehowmanyprojectshaveactuallybeencompletedandcommissionedfromthedatapresentlyavailable.Asubstantialinvestmentwasalsomadeinacquiringmotorbikesforcommunityhealthservices,whileahirepurchaseschemewasintroducedtoenablefacilitiesandDHMTstoacquirepick-upsformonitoring
EnterintodialoguewithMOFEPonacceptabledecentralisedcapitalinvestmentpaymentmechanismstoenhanceexpenditureeffectiveness.
Notyetimplemented,capitalinvestmentpaymentmechanismremainshighlycentralisedwithinMOFEP
Developanoverviewofthetotalresourceenvelopefordistrictcapitalinvestment.
Uncertaintiesoverresourceavailability,andcontinuingcentralisationofcapitalinvestmentdecision-making,haverestrictedopportunitiesfordistrict-ledresourceallocation
Developamedium-to-long-termcapitalinvestmentplanthatprioritisesaddressinginequitiesandachievementofMDG4andMDG5,usingServiceAvailabilityMappingandHealthServicesPlanningMethodologyandFrameworktoidentifypriorities
Infrastructuredevelopmenthasbeenweightedtowardsmodernhigh-techDistrictHospitalsandHealthCentres,duetotherelianceonsupplier-drivenFinancialCredits.Howevertheongoingsupplyofessentialobstetricequipmentto150HealthCentresand40DistrictHospitalsundertheHighImpactRapidDelivery(HIRD)ProgrammehasmadeasignificantcontributiontowardsachievingtheMDGs
StrengthenPlannedPreventiveMaintenance,bydevelopingPPMproceduresandbudgetallocation
Procedureshavebeendevelopedbutimplementationhasstalled,duetobudgetaryconstraints
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|76
guidelines,implementandmonitor
4. 2007-2009IssuesArisingCapitalexpendituredataon transport,equipmentand ICTby theagencies isnot readilyavailable,reflecting inadequate information flow between GHS and MoH, and laterally within eachorganisation.With theexceptionof thereportsoncivilworksproducedby theCapital InvestmentManagementUnitofMoH-PPME,thereisnoroutinereportingonprogressandexpenditure,andnosingleunitordesk is responsible forcollectingdata,monitoringandreportingonprogressagainsttheCapitalInvestmentPlanasawhole.Problems have arisen in trying to reconcile operational data with with MoH annual FinancialStatements. Estimated totalMoH/GHS2009 Item4 expenditure ofGHC44.94million (per PPMEsand SSDMdata), is significantly lower than theGHC 204.70million recorded for Item 4 per draft2009FinancialStatement–thefinancialdataincludesloanagreementsthathavebeenenteredintobut not yet disbursed, and credits of GH¢196 million at the DHA level for recurrent costs ofProgrammeactivities,therebyoverstatingexpenditure.ForecastinflowsfromNHIF(46%ofthetotalCIPIIIresourceenvelope,and7.5%ofthe2009Budget)didnotmaterialiseorwerenotcapturedinreporting.Therehasbeenanincreasingrelianceontheuse of Financial Credits to develop new infrastructure, often on turnkey project basiswhich goesagainsteffortstobuildcapacitywithinMoH/GHS-65%ofactualinflowswerefromFinancialCredits,mostlyatthelevelofDistrictHospitals.TherewasverylimitedinvestmentofGOGfundsatthesub-districtlevel,withonly3newCHPSCompoundsactuallyfundedbyMoHin2009.Implementation of the planningmethodology and framework has been restricted, and hence thefacilityrationalisationagendahasstalled–Districtscontinuetodevelopproposalsforinvestments,but funding for implementation is limited, and decisions on capital investments are sometimesbased on political considerations and funding availability rather than technical grounds. Oneexample of this is the Austrian-funded project for construction of Polyclinics/Health Centres –althoughtheselectionoflocationswasdirectedtowardstheNorthernRegionbyuseoftheServiceAvailabilityMapping in the first phase, it has beenmoved to the Upper East Region in the nextphase,althoughtheNorthernRegioncontinuestobeunderserved.CapitalinvestmenthasmadeonlyalimitedcontributiontowardsachievingtheMDGsin2009.Outofanestimated6,400CHPSzonesrequirednationwide,over2,300havebeendemarcatedbutonly500made functional,outofwhichamere300are completedwitha compound for theCHOs.DistrictAssemblies’budgetsareincreasinglyconstrainedintheireffortstoprovideCHPSinfrastructure,andtheNovember2009JointMoH–PartnersBusinessMeetingnotedthat“intheabsenceofsufficientcompounds, CHOs are being placed at health centres, thereby defeating the purpose of theirtraining”.Theapproachof‘staffbeforeinfrastructure’thereforeappearstolimittheCHOs’abilitytoundertakesustainedprimarycareworkinthecommunities.DHMTs and facilities at the District level appear to be using their own initiative to acquire smallitems of medical equipment and ICT equipment through their IGF surpluses, although these aremostly reported as Item 2 expenditure, in order to get around the central control on Item 4expenditure(thismayaccountforsomeoftheapparentover-expenditureonItem2).MobilityattheDistrictlevelappearstohavebeenconsiderablyenhancedbytheacquisitionof4,000motorbikes in 2008–2009. The hire purchase scheme for acquisition of pick-ups has generated
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|77
considerableinterestfromDHMTsandfacilities,althoughthereareuncertaintiesoverhowtheywillbeabletomeetthemonthlypayments.Itappearsthat littleattention isbeingpaidtotherecurrentmaintenancecost implicationsofnewcapital investments, especially for the modern Polyclinics and District Hospitals currently beingconstructedinaneraofincreasinglylimitedavailabilityofItem2funds.
5. Recommendations• The MoH should hold regular high level meeting with MLGRD and NDPC with a view to
improving collaboration on the CHPS, as recommended by the November 2009 BusinessMeeting Aide Memoir. Without a concerted effort to ensure the presence of CHOs in thecommunities,GhanawillstruggletoachievetheMDGs.
• As its contribution to the substantial investment needed nationwide, MoH should ring-fence
GH¢15million from its capitalbudgetper year for thenext threeyears, toprovideabout600complete CHPS compounds over the period. MoH will then be seen to be making a realcommitment to implementing the CHPS programme, and will be in a stronger position todemandcontributionsfromDistrictAssembliesformoreofthesefacilities.
• Theproblemofmonitoringphysicalprogressandreportingonfinancialexpenditureforcapital
investment (including transport, equipment and ICT) persists. The earlier well-functioningsystemsformonitoring inthepast,havefallen intodisuseandhavenotbeenreplacedbyanyalternativesystems.ItisrecommendedthattheCapitalInvestmentManagementUnit(CIMU)ofthe MoH PPME should be tasked to coordinate quarterly monitoring and reporting to theDirectorofPPMEonprogressandexpenditureonallcapitalinvestment.Thisinformationshouldbe validated by quarterly monitoring visits to the Districts by MoH and partners, to assessbudgetimplementation.

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|78
Annex8.Noteonhealthfinancingandhealthinsurance
1PFMinthehealthsector
The health sector faces a number of challengeswith regard to public financialmanagement. Thecredibilityofthehealthsectorbudget,thepredictabilityandtimelinessofdisbursementstodifferentlevelsinthesystem,theincompleteinformationondistrict,regionalandNHISexpendituresandtheaccuracyofthefinancialreportingareallfactorscontributingtosub-optimalresultsinhealthsectordelivery.TheseissuesneedtobeseeninthebroadercontextofthefunctioningofthePFMsysteminGhana (all sectors).Nonetheless, theMoHshouldbeable to takeappropriateactionswithin itsowndomain.
PFMworkinggroup
The move from DFID, the Netherlands and Danida from pooling funds into the Health Fund toprovidingSBSfrom2008onwardshastosomeextendformalisedtheissuetostrengthenPFMinthehealthsector.TheFrameworkMemorandumforSBSpartnerscommitstheGoGtocontinuedeffortstostrengthenPFM,asfollows:“StrengtheningPublicFinancialManagement(PFM)isarequirementof budget support programmes. Within the existing framework of the MOFEP PFM programme,signatoryMinistriesandsignatoryDPswilljointlydevelopaprogrammeforPFMstrengtheninginthehealthsectorinthefirstsixmonthsofimplementationofthisFM.TheprogrammewillbesequencedandintegratedintotheAPOWsstartingin2009atthelatest.”
Box1.KeyfindingsonPFMinthehealthsector• The health sector still leads in PFM but without a conscious effort to build and
maintain the fundamentals. • The pre-requisites for effective financial management in the health sector need
immediate attention to ensure a sound foundation for investments in improvements. • A coordinated effort to clarify roles and linkages across the sector for ensuring
accountability must be made and sustained. • A structured approach to performance management that rides on the existing rigorous
annual planning and review process must be put in place. This system must be decentralised across agencies, levels and BMCs and tied to an incentive and sanction system
• A well structured institutional mechanism for environmental scanning and risk management.
• A systematic and structured model for identifying capacity needs in a manner that is linked to policy priorities and targets and coordinated such as to improve outputs.
Source: PFM issues paper, December 2008

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|79
A formal process in this direction started in June 2008 when interested stakeholders formed aWorkingGroupandagreedonatwophasedapproach.Phase1 involvedtheproductionofaMoHPublic Financial Management Strengthening Issues Paper with the objective to 1) map currentactivities related to PFM strengthening both within the MoH and her agencies at central anddecentralised levels; 2) identify outstanding concerns, and 3) to propose actions necessary toaddressthoseconcerns. Thisstudy,carriedoutwithexternaltechnicalassistance,wasfinalised inDecember2008.Aspartofphase2,thePFMIssuesPaperwasdiscussedandcommentedonamongstakeholders inApril 2009. TheWorkingGroupmeton a coupleof occasions in 2009 for furtherdiscussions on PFM-related concerns. The Working Group’s main achievement in 2009 was thedevelopmentofa framework for furtheractions, listing57 (non-prioritised)activities includingtheresponsibleunit,atimelineandbudget.Beyondthismilestone(oneoftherecommendationsoflastyear’sreview),implementationoftheidentifiedactivitiesweregenerallyslow.
One of the PFM-related outputs that materialised in 2009 is the finalisation and printing of theupdatedversionofthe“Accounting,TreasuryandFinancialReportingRulesandInstructions”(ATF)which became effective from January 2010. The AFT will standardize and improve the financialmanagementproceduresandprocesseswithinthesectorandguidefinancialauditingandreporting.Theupdatewasneededtoincorporatelegalacts(e.g.thePublicProcurementActandtheInternalAuditAgencyAct)andpolicychanges(introductionofNHIS,HIRDprogramme)afterthepublicationofthefirstATFin1997.AtrainingprogrammeontheATFstartedinthefirstquarterof2010.
BesidestherealisationofthelongawaitedATF,littleprogresshasbeenmade.ThemembersoftheWorkingGroupwerehamperedbythelackofbudgetreleasesandweregenerallytoooccupiedwiththeir regular tasks to actively drive the agenda. During the Health Summit in November 2009,concernswereraisedagainaboutthelackofeffectivefinancialmanagementinthesectorincludingcontinuous delays to strengthen this area. It is therefore recommended to take institutionalmeasurestoassurethatthePFMstrengtheningplanwillstayontheagendain2010.DPscouldplayamoreactive roleby supporting temporaryassistance in thisarea.Further, it is recommended toprioritise between the 57 activities. The sector will benefit for instance from improving the linkbetween the MTEF (on-budget) with the PoW (on-plan) and the FS (on-account) to be able toprovide budget performance feedback. But besides themore complicatedmatters, theWorkingGroupcanfocusonsomequickwins:SectorBudgetCommitteemeetingstotakeplace,solvingtheIGF double counting in the MTEF and sharing of information on the budget allocation formulabetweenNHIS,GHSandMoH.
2.Allocationstohealth
Based on the corrected Annual (Supplementary) Budget Statement, the allocation to the healthsectorasapercentageofthetotalfiscalspacefor2009is14.6percent(seealsoholisticassessmentindicator27 foranexplanatorynote).Double-countingofa significantproportionof IGFswhich isfunded through NHIF could overstate the true MoH share of the budget. On the other hand,substantial levels of off-budget financing are not included in the presented figures. All in all, theallocationstohealthgrewinnominaltermswith25%;about7%inrealtermsbasedonanaverageinflationrateof18%in2009. InrelativetermsasaproportionoftheMTEFallocationtherewasaslight decline of 2%. The total allocation is considered relatively stable and in themargin of theAbuja-targetof15percent.
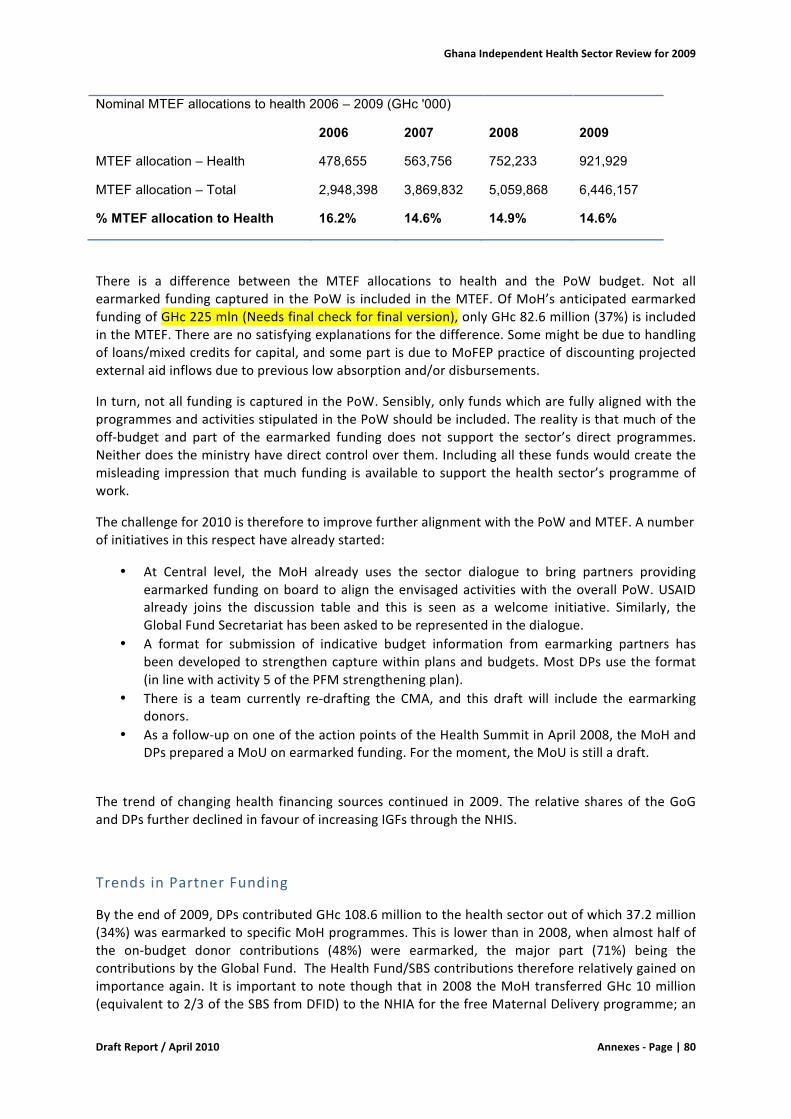
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|80
Nominal MTEF allocations to health 2006 – 2009 (GHc '000)
2006 2007 2008 2009
MTEF allocation – Health 478,655 563,756 752,233 921,929
MTEF allocation – Total 2,948,398 3,869,832 5,059,868 6,446,157
% MTEF allocation to Health 16.2% 14.6% 14.9% 14.6%
There is a difference between the MTEF allocations to health and the PoW budget. Not allearmarkedfundingcaptured inthePoWis included intheMTEF.OfMoH’santicipatedearmarkedfundingofGHc225mln(Needsfinalcheckforfinalversion),onlyGHc82.6million(37%)isincludedintheMTEF.Therearenosatisfyingexplanationsforthedifference.Somemightbeduetohandlingofloans/mixedcreditsforcapital,andsomepartisduetoMoFEPpracticeofdiscountingprojectedexternalaidinflowsduetopreviouslowabsorptionand/ordisbursements.
Inturn,notallfundingiscapturedinthePoW.Sensibly,onlyfundswhicharefullyalignedwiththeprogrammesandactivitiesstipulatedinthePoWshouldbeincluded.Therealityisthatmuchoftheoff-budget and part of the earmarked funding does not support the sector’s direct programmes.Neitherdoestheministryhavedirectcontroloverthem.Includingallthesefundswouldcreatethemisleading impressionthatmuchfunding isavailabletosupport thehealthsector’sprogrammeofwork.
Thechallengefor2010isthereforetoimprovefurtheralignmentwiththePoWandMTEF.Anumberofinitiativesinthisrespecthavealreadystarted:
• At Central level, the MoH already uses the sector dialogue to bring partners providingearmarked fundingonboard toalign theenvisagedactivitieswith theoverallPoW.USAIDalready joins the discussion table and this is seen as a welcome initiative. Similarly, theGlobalFundSecretariathasbeenaskedtoberepresentedinthedialogue.
• A format for submission of indicative budget information from earmarking partners hasbeendevelopedtostrengthencapturewithinplansandbudgets.MostDPsusetheformat(inlinewithactivity5ofthePFMstrengtheningplan).
• There is a team currently re-drafting the CMA, and this draft will include the earmarkingdonors.
• Asafollow-upononeoftheactionpointsoftheHealthSummitinApril2008,theMoHandDPspreparedaMoUonearmarkedfunding.Forthemoment,theMoUisstilladraft.
The trendof changinghealth financing sources continued in2009.The relative sharesof theGoGandDPsfurtherdeclinedinfavourofincreasingIGFsthroughtheNHIS.
TrendsinPartnerFunding
Bytheendof2009,DPscontributedGHc108.6milliontothehealthsectoroutofwhich37.2million(34%)wasearmarkedtospecificMoHprogrammes.Thisislowerthanin2008,whenalmosthalfofthe on-budget donor contributions (48%) were earmarked, the major part (71%) being thecontributionsbytheGlobalFund.TheHealthFund/SBScontributionsthereforerelativelygainedonimportanceagain. It is importanttonotethoughthat in2008theMoHtransferredGHc10million(equivalentto2/3oftheSBSfromDFID)totheNHIAforthefreeMaternalDeliveryprogramme;an
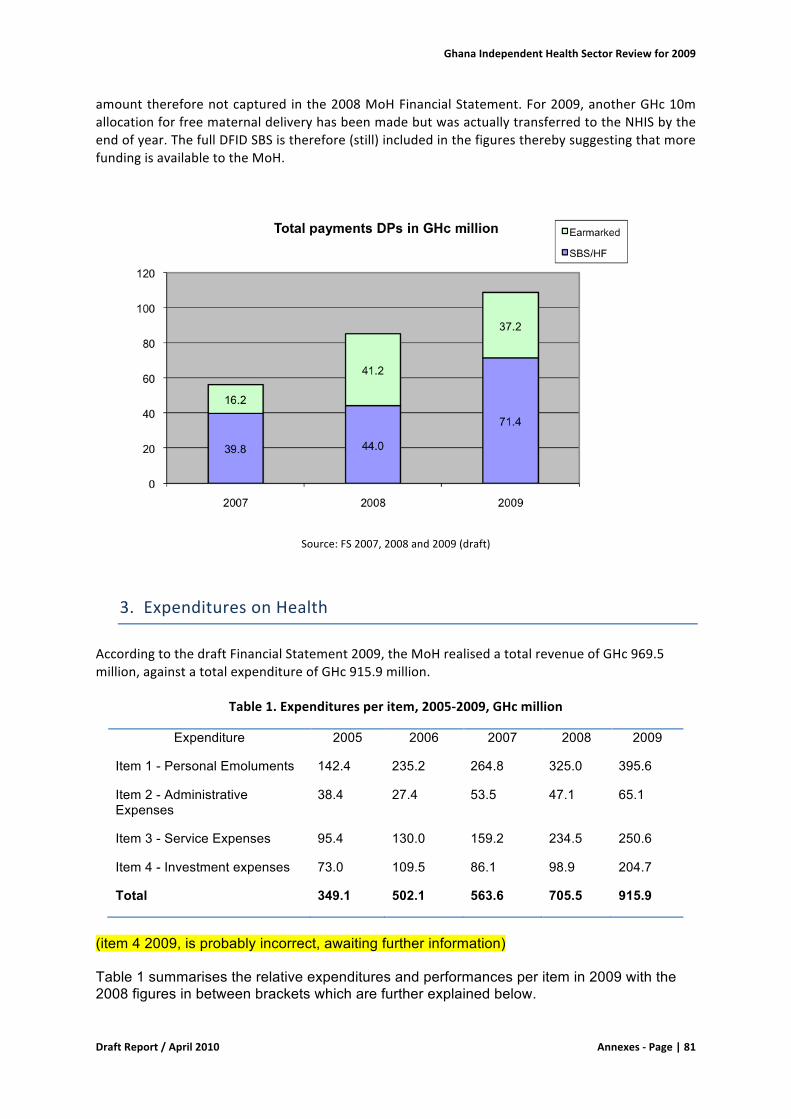
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|81
amountthereforenotcaptured inthe2008MoHFinancialStatement.For2009,anotherGHc10mallocationforfreematernaldeliveryhasbeenmadebutwasactuallytransferredtotheNHISbytheendofyear.ThefullDFIDSBSistherefore(still)includedinthefigurestherebysuggestingthatmorefundingisavailabletotheMoH.
Source:FS2007,2008and2009(draft)
3. ExpendituresonHealth
AccordingtothedraftFinancialStatement2009,theMoHrealisedatotalrevenueofGHc969.5million,againstatotalexpenditureofGHc915.9million.
Table1.Expendituresperitem,2005-2009,GHcmillion
Expenditure 2005 2006 2007 2008 2009
Item 1 - Personal Emoluments 142.4 235.2 264.8 325.0 395.6
Item 2 - Administrative Expenses
38.4 27.4 53.5 47.1 65.1
Item 3 - Service Expenses 95.4 130.0 159.2 234.5 250.6
Item 4 - Investment expenses 73.0 109.5 86.1 98.9 204.7
Total 349.1 502.1 563.6 705.5 915.9
(item 4 2009, is probably incorrect, awaiting further information) Table 1 summarises the relative expenditures and performances per item in 2009 with the 2008 figures in between brackets which are further explained below.
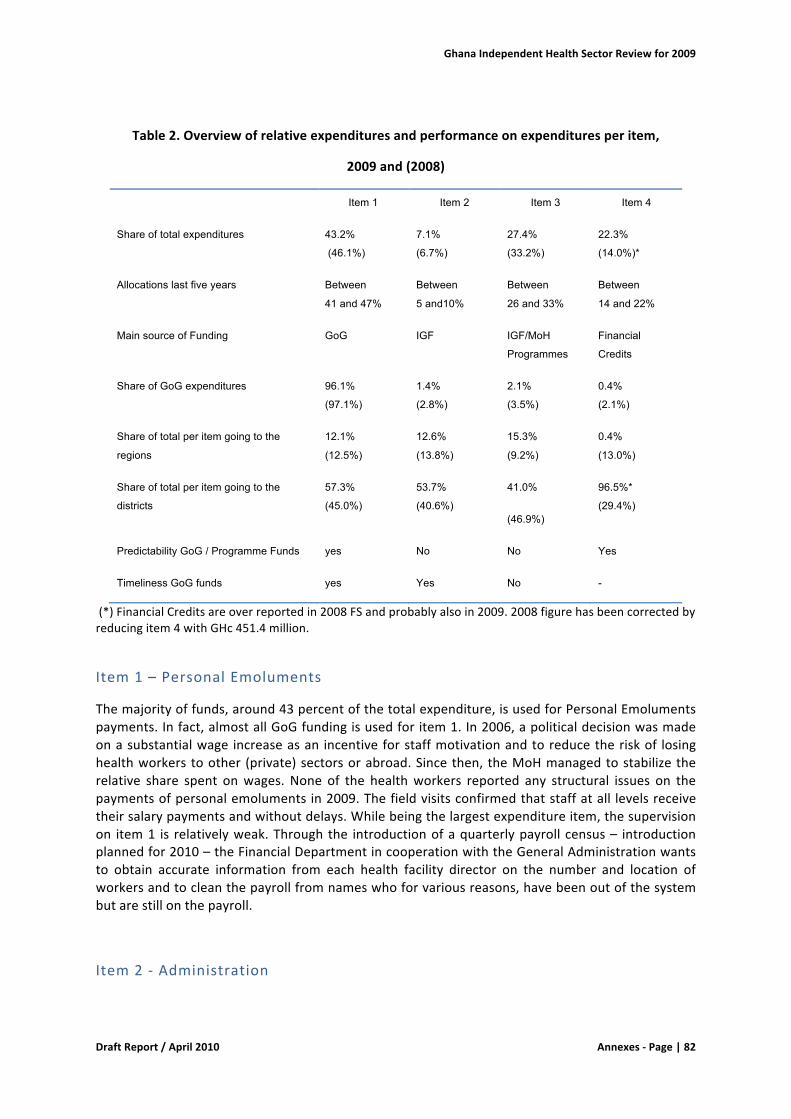
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|82
Table2.Overviewofrelativeexpendituresandperformanceonexpendituresperitem,
2009and(2008)
Item 1 Item 2 Item 3 Item 4
Share of total expenditures 43.2%
(46.1%)
7.1%
(6.7%)
27.4%
(33.2%)
22.3%
(14.0%)*
Allocations last five years Between
41 and 47%
Between
5 and10%
Between
26 and 33%
Between
14 and 22%
Main source of Funding GoG IGF IGF/MoH
Programmes
Financial
Credits
Share of GoG expenditures 96.1%
(97.1%)
1.4%
(2.8%)
2.1%
(3.5%)
0.4%
(2.1%)
Share of total per item going to the
regions
12.1%
(12.5%)
12.6%
(13.8%)
15.3%
(9.2%)
0.4%
(13.0%)
Share of total per item going to the
districts
57.3%
(45.0%)
53.7%
(40.6%)
41.0%
(46.9%)
96.5%*
(29.4%)
Predictability GoG / Programme Funds yes No No Yes
Timeliness GoG funds yes Yes No -
(*)FinancialCreditsareoverreportedin2008FSandprobablyalsoin2009.2008figurehasbeencorrectedbyreducingitem4withGHc451.4million.
Item1–PersonalEmoluments
Themajorityoffunds,around43percentofthetotalexpenditure,isusedforPersonalEmolumentspayments.Infact,almostallGoGfundingisusedforitem1.In2006,apoliticaldecisionwasmadeonasubstantialwage increaseasan incentiveforstaffmotivationandtoreducetheriskof losinghealthworkerstoother (private)sectorsorabroad.Sincethen,theMoHmanagedtostabilizetherelative share spent onwages. None of the healthworkers reported any structural issues on thepaymentsofpersonalemolumentsin2009.Thefieldvisitsconfirmedthatstaffatall levelsreceivetheirsalarypaymentsandwithoutdelays.Whilebeingthelargestexpenditureitem,thesupervisionon item1 is relativelyweak.Throughthe introductionofaquarterlypayroll census– introductionplannedfor2010–theFinancialDepartmentincooperationwiththeGeneralAdministrationwantsto obtain accurate information from each health facility director on the number and location ofworkersandtocleanthepayrollfromnameswhoforvariousreasons,havebeenoutofthesystembutarestillonthepayroll.
Item2-Administration

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|83
One of the consequences of the high expenditures on wages is that it leaves limited resourcesavailableforothernon-salaryrecurrentexpenditures.Thefundsavailableforadministrationattheregional and district health authorities seem to fluctuate heavily year-to-year, scoring badly onpredictability. In 2008, shortfalls on the overall health budget were settled by reallocating thebudgetfromitems2and3toitem1tosafeguardsalarypayments.In2009,item2sawabudgetcutof around50%when the final budgetwas approved in aroundMarch. Thiswas supposed to cutdown on “waste and inefficiencies” but was not realistic and MoFEP ended up paying out ofcontingencythroughasupplementarybudget.Theseshiftsinexpendituresharescauseconsiderabledifficulties at regional and district level. Since these budget reallocations are not monitored onactivity level in the financial statement, it is important to signal the growing imbalance betweensalaryandnon-salaryexpendituresandhowthisaffectsservicedeliveryreportedelsewhere.
Item3-Services
The figurebelow illustrates the flowof fundsunder item3.Bothpreventiveandcurativecarearepaidfromitem3.Thecurrentstructureofthefinancialstatementmakesitimpossibletodistinguishbetweenpreventiveandcurativecareexpenditures.
Curativeservicesaresolelycoveredfromthefacility’sIGFsthroughtheNHISandCashandCarry.Inaddition, theMoHallocated(butnotyet transferred)GHc10million (equivalentto2/3of theSBSfromDFID)topartiallysubsidizetheNHIA’sfreeMaternalDeliveryprogramme.
Preventive health services are paid directly from the MoH Budget. The NHIS contributes to thepromotion of preventive care (allocated to public health programmes as well as certaininfrastructureimprovements)byallocatingacertainamountofNHISrevenuestotheMoH.In2008,theNHIScontributionwasGHc42.5million.TherearenorulestodeterminetheNHIScontributionto theMoH;availablebudgetary space seems tobe themain criteria. Thiswouldalsoexplain thelowerplannedcontributionofGHc30.3millionin2009.
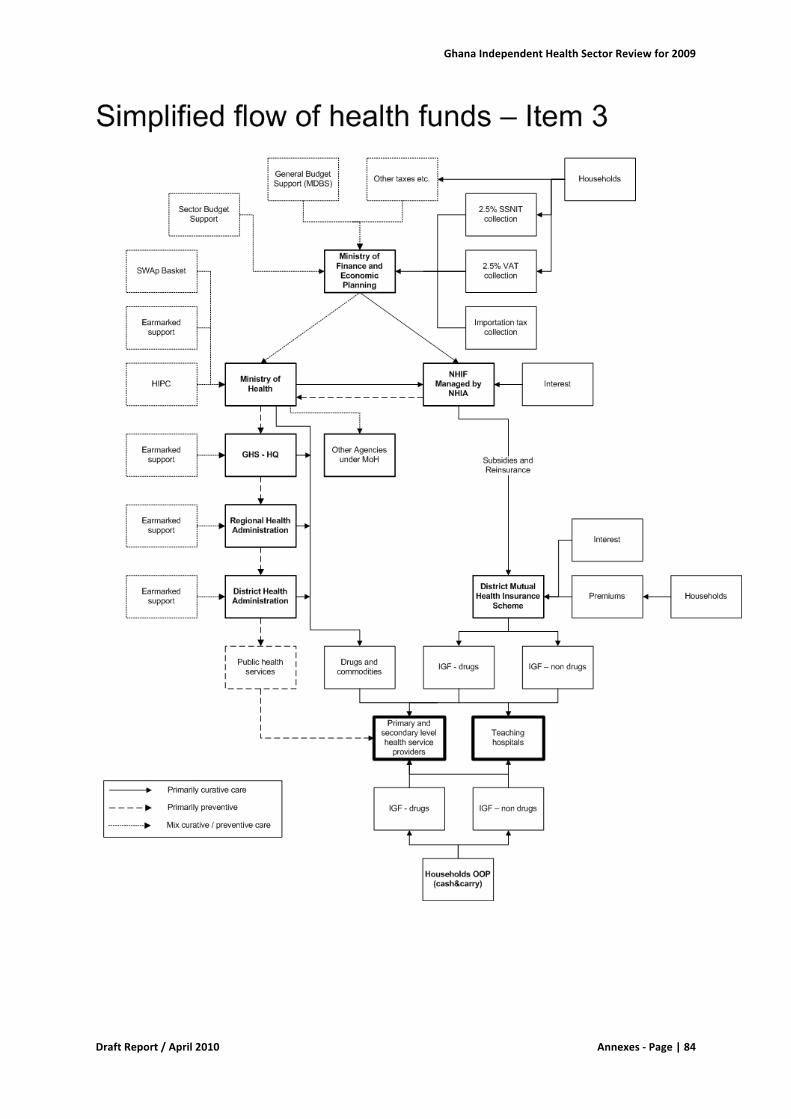
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|84
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|85
GHShasthetechnicalresponsibilityfortheimplementationoftheMoHpublichealthprogrammes(including theHIRD strategy) and uses allocation formulas to distribute the funds to the RegionalHealthAuthoritieswhichinturnallocatethefundstothedistricts.TheMoHProgrammebudget issupplementedby(earmarked)donorsupportwhichentersthesystemsatdifferentlevels.ThemaincontributorsofearmarkedfundingaretheGlobalFundforHIV/AIDS,TBandMalariaandUSAID,thelatter is not included in the national financial reporting system. Although not substantiated byfigures, the feeling exists that preventive care is loosing ground compared to curative care,especially since the introduction of the NHIA and IGF. If true, this is would be an alarmingdevelopmentthatneedstobealtered.Moreinformationandanalysisisneededinthisregard.
There were a number of developments in 2009 which created financial challenges for servicedeliveryattheregionalanddistrictlevel:
• Utilisationandthereforealsocostsofcurativecarefurtherincreased.• The provision of curative services was heavily challenged by the backlog on NHIS claims
processingwhichhascreatedseriousliquidityshortagesatproviderlevel.• ThemoveofsomedonorsfromHealthFundtoSBSresultedinextradelays inthechainof
disbursementsinparticularfromtheMoFEPtotheMoH.Thepredictabilityoffundsforitem3deterioratedfurtherin2009.
• The MoH had the tendency to earmark high volumes of SBS funds to particular Healthprogrammes,therebylimitingthe‘flexiblefunds’atregionalanddistrictlevel.
• Unforeseen expenditures, like an additional GHc 2 million for the Influenza pandemic in2009,weretakenoutoftheitem3budget,therebyfurtherchallengingtheobjectivesofthePoWunder item3.Unforeseen expenditures like these are expected to be paid from theMoFEP contingencies budget, but access to and slow releases from the contingencieshamperafastresponseincaseofurgencysothatitem3isusedinstead.
Themainissuesarefurtherdiscussedbelow:
TimelinessofGoGdisbursements
The year 2009 has been extremelyweak in terms of item 3 disbursements. The first GoG item 3tranchewithaWarrantDateof3Februarywas receivedat theBankofGhanaaccounton28thofApril.BytheendofJune2009,only12%ofGoGitem3hadbeenreleased.Thedisbursementstotheregionsanddistrictsconsequentlywereevenfurtherdelayed.Someofthedistrictsvisitedreportedtheirfirstreceiptoftheyearinthethirdquarter.
MoFEP and MoH see the change of Government as the main explanation for the delays indisbursements,butthefactthat item3isbasedoncashmanagementisanotherimportantfactor.Unlikeforitem1whereMoFEPusestemporarilyloanswithBoGtopaypersonalemoluments,item3is only releasedwhen thebalanceof account is positive. This system is accepted as a fact of life;MoHdoesnotactivelynegotiateforfasterdisbursements.
TimelinessandallocationsofSectorBudgetSupport
SBSas anewaidmodality is not yet fullyunderstood. SBS is keptona separateaccount and stillreportedandtrackedseparatelyintheMTEF,PoWandFSwhileitshouldactuallybetreatedasGoGfunds.TheMoHhastofileaseparateapplicationformtotheMoFEPtoaccesstheSBS.Thisprocesstakesalongtime.AtthebeginningofFebruarytheMoHappliedfortheNetherlandsSBSwhichwastransferredtothebankaccounthalfMayi.e.threemonthslater.TheDanidaSBStookevenlongerwithanapplicationdateattheendofAprilandalodgementdateinthebeginningofOctober.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|86
BecauseSBSisnotintegratedintotheGoGfunds,itispossibletotrackinthePoWhowtheMoHhasallocatedtheSBSfunds.Interestingly,onlyGHc1.5millionoutofGHc54.9million(lessthan3%)isavailable for operational costs for MoH and its agencies (excluding NHIA). The remaining part isintendedtosecure:
1) thecentralprocurementofcommodities(likevaccines,contraceptives,ITNsanddrugs)2) theimplementationofpublichealthprogrammes(likeMCHcampaigns)3) HealthSystemStrengthening;4) PublicFinanceManagementstrengthening;5) Equipmentmaintenanceandreagents.
Thelatterring-fenceditemshouldactuallybepaidbythefacilitiesfromIGFs,butsomeofthelargerequipmentmanufacturershavenegotiatedthattheirmaintenancecontractsaredirectlypaidbytheMoHandnotbythefacilities.Thetotalvalueofthesecontracts isGHc10.4million,about19%oftotalSBS.
DistrictPlanning
As stated above, the current reporting structure allows commenting on the allocations of SBS. Inprinciple SBS can be allocated by theMoH according to needs.While there are certainly positiveelements on earmarking at this level it is also important to signal that at district level these highvolumesof earmarkingare felt as abigobstructionwhichalsoundermine themeaningofdistricthealthplanningandbudgeting.Thelimitedandlatereleasesonitem2and3combinedareplacingtheDHAsfurtherunderpressure.In2009,GFATMandHIRDfundswereimportantsourcesatdistrictlevel to keep the system running. One of the district visited started a pilot with an innovativeconcept on the 1st of January 2010. This District Authority assists the district health centreswithNHISclaimprocessingbeforesubmissiontotheDMHIS.Inturn,theDistrictAuthorityandthedistricthealthcentreshaveagreedthattheDAkeepsthevalueof30%ofthereimbursedclaimsforservices(nodrugs)whichisusedtosupportthehealthclinicswiththeimplementationofthepublichealthprogrammes.
4. NationalHealthinsuranceScheme
TheNHISdidnotprovidemembershiporfinancialdata.Instead,theteamusedprovisionalestimatesfromtheAllocationFormula2010(versionOctober2009),providedbytheMoH.AnalysingNHISenrolmentiscomplicatedbecauseonlythenumbersofregisteredexemptgroupsareavailable. There is no information available on the number of premium paying registrants. Inaddition, NHIS membership needs to be renewed on an annual basis and there is no overviewavailableonvalidcardholders.Withthisimportantremarkinmind,theavailableestimatesdoshowasignificantgrowth.ThetotalregistrationsofexemptgroupsbytheendofOctober2009were9.7millioncomparedto8.8millionin2008(+10%).
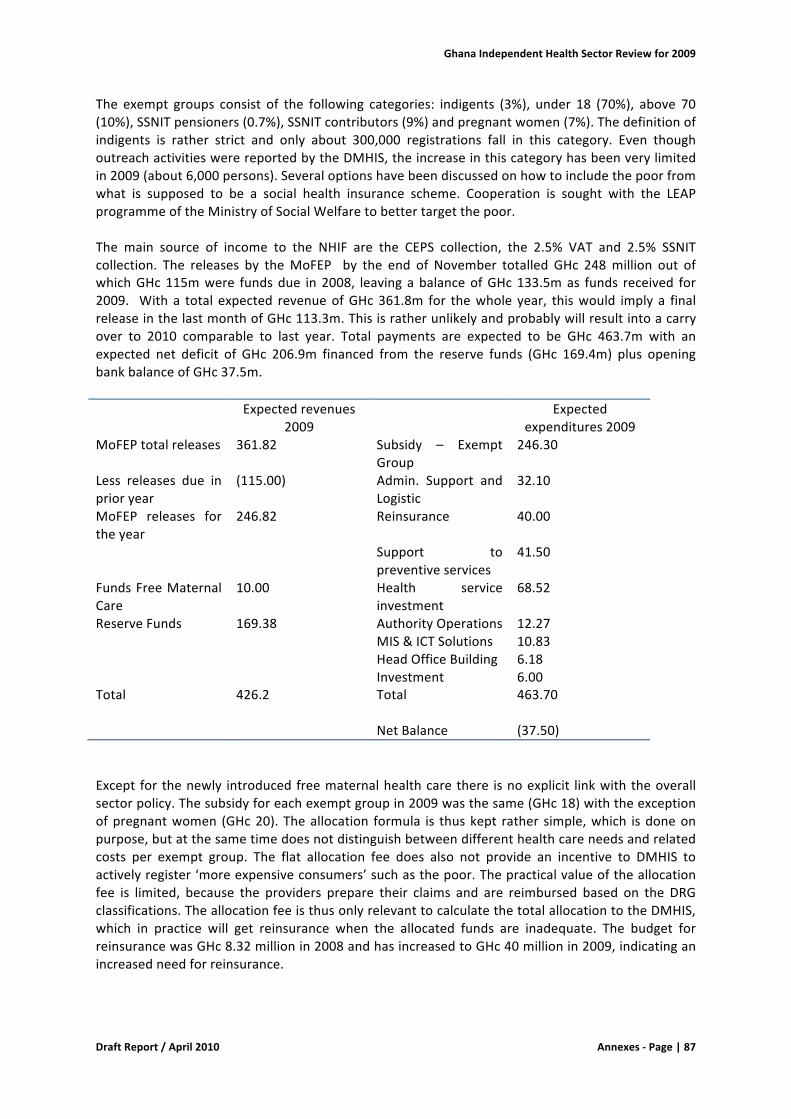
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|87
The exempt groups consist of the following categories: indigents (3%), under 18 (70%), above 70(10%),SSNITpensioners(0.7%),SSNITcontributors(9%)andpregnantwomen(7%).Thedefinitionofindigents is rather strict and only about 300,000 registrations fall in this category. Even thoughoutreachactivitieswerereportedbytheDMHIS,theincreaseinthiscategoryhasbeenverylimitedin2009(about6,000persons).Severaloptionshavebeendiscussedonhowtoincludethepoorfromwhat is supposed to be a social health insurance scheme. Cooperation is sought with the LEAPprogrammeoftheMinistryofSocialWelfaretobettertargetthepoor.The main source of income to the NHIF are the CEPS collection, the 2.5% VAT and 2.5% SSNITcollection. The releases by theMoFEP by the end of November totalled GHc 248million out ofwhichGHc115mwere fundsdue in2008, leavingabalanceofGHc133.5mas funds received for2009. With a total expected revenueofGHc361.8m for thewhole year, thiswould imply a finalreleaseinthelastmonthofGHc113.3m.Thisisratherunlikelyandprobablywillresultintoacarryover to 2010 comparable to last year. Total payments are expected to be GHc 463.7m with anexpected net deficit of GHc 206.9m financed from the reserve funds (GHc 169.4m) plus openingbankbalanceofGHc37.5m. Expectedrevenues
2009 Expected
expenditures2009MoFEPtotalreleases 361.82 Subsidy – Exempt
Group246.30
Less releases due inprioryear
(115.00) Admin. Support andLogistic
32.10
MoFEP releases fortheyear
246.82 Reinsurance 40.00
Support topreventiveservices
41.50
FundsFreeMaternalCare
10.00 Health serviceinvestment
68.52
ReserveFunds 169.38 AuthorityOperations 12.27 MIS&ICTSolutions 10.83 HeadOfficeBuilding 6.18 Investment 6.00Total 426.2 Total 463.70 NetBalance (37.50)Except for thenewly introducedfreematernalhealthcarethere isnoexplicit linkwiththeoverallsectorpolicy.Thesubsidyforeachexemptgroupin2009wasthesame(GHc18)withtheexceptionofpregnantwomen (GHc20).Theallocation formula is thuskept rather simple,which isdoneonpurpose,butatthesametimedoesnotdistinguishbetweendifferenthealthcareneedsandrelatedcosts per exempt group. The flat allocation fee does also not provide an incentive to DMHIS toactivelyregister‘moreexpensiveconsumers’suchasthepoor.Thepracticalvalueoftheallocationfee is limited, because the providers prepare their claims and are reimbursed based on the DRGclassifications.TheallocationfeeisthusonlyrelevanttocalculatethetotalallocationtotheDMHIS,which in practice will get reinsurance when the allocated funds are inadequate. The budget forreinsurancewasGHc8.32millionin2008andhasincreasedtoGHc40millionin2009,indicatinganincreasedneedforreinsurance.

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|88
TheactualexpendituresonexemptgroupstillOctober2009wereGHc212.9m,asignificantincreaseof64%comparedtotheGHc129.7min2008,yet,withinthebudgetofGHc246.3for2009.Auditedfinancial statements are needed to be able to make more comprehensive conclusions on thefinancialsituationandsustainabilityofthesystem.
Claimprocessing
As clearly outlined in last year’s review, there are considerable delays in the chain of claimprocessing,bothupwardsfromtheproviderspreparingandsubmittingtheirclaimstotheDMHISaswellasdownwards insubsidypayments,reinsuranceandreimbursementsofclaims.Attheendof2008, thehealth facilitieshadoutstandingclaimsworthGHc49million.Theoutstandingclaimsattheendof2009arenotavailablebutallqualitativeinformationsuggestsafurtherincrease.
A large proportion of claims is still handled manually. The introduction of the DRG system isgenerally felt as an improvement, at least for inpatient services and when compared with theprevious user fee system, though there are still some ICT-related hick-ups to overcome. For OPservicesandfirstlinefacilities,itisfeltthattheDRGsystemmaybetoocomplicated.RegardingICT-related hiccups, there are for instance delays in receiving a validmembership card, duringwhichperiodtheDMHISisallowedtoissuetemporarycards,butclaimsfrommemberswithatemporarycardcan’tbevettedthroughtheautomaticsystem.
Duetothesubstantialgrowthinmembershipandutilisationofservices,theDMHISdon’thavethecapacitytohandleallclaimsintime.Duringoneofthefieldvisits,theschememanageroftheDMHISpointedouttoreceiveabout30,000claimsamonth.Withanaveragecapacitytovet30claimsadayperstaffmemberandwithonly2staffmembersavailableforvetting,theschemehasastructuralproblemwhichiscurrentlyaddressedwithassistancefromtheregionalNHIAofficeandbyovertimeworkbutforwhichnolong-termsolutionissought,hangingthenewHealthInsuranceAct.
The DMHISs lose a lot of time on filtering for wrong or false claims. Examples of these rejectedclaimsareforinstancecasesinwhichthe:
• ClaimhasnoID-number• Claimlistsprescribeddrugsoutsidethemedicines listandalsochargeabovetheapproved
pricesfordrugs• Claimisfiledasthoughthepatientwasaninpatientwhileheactuallyvisitedtheoutpatient
department• Claimfilestreatmentsnotmeritingthediagnosedailmentandisnotincompliancewiththe
standardguidelinesfortreatment.
Inparticularthelattercategorycausesfrustrationattheproviderslevelwhofeelthatthestandardguidelines are too strict, leaving no room for different medical interpretations for the patient’ssickness.Thereisalsonoclearcutsolutiononthesekindofrejectedclaims.Inprincipal,theyshouldbereturnedtotheproviderforcorrectionbutitisuncleartowhichextendthisishappening.Claimsrejectedbythemutualresultasbaddebtonthebalancesheetoftheprovider.
SustainabilityofNHIS
Aspartof theWB-fundedHealth InsuranceProject, anactuarial studyon the sustainabilityof theNHIS isongoing.Preliminary results conclude thatat thismoment in time, theNHIS is sustainablethoughthesituationstartsgettingcritical.Thestudyismodellingdifferentscenariosincludingsomemacro-economicdevelopmentsthatmayinfluencetherevenuegeneratingcapacityoftheNHIS.Forinstance, the NHISmay benefit indirectly from higher volumes of VAT income through increasedconsumptionlevelsfromfutureoilrevenuesordirectlybyincreasingtheVATlevy.Whilethesekind

GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|89
of scenariosare interesting to investigate, thenumberofassumptions is toohigh to relyon.As itstandsnow,onlydemographicgrowthmayalreadyturnthebalance.Therefore,thesectorneedstofocuson rapidactions to rationaliseuseof services, control volumeandpriceofdrugsprescribedanddetectfraudandabusebyprovidersorpatients.
Currently,therearenoimbeddedmechanismsintheNHIStoimposegoodqualityofcare.ThroughtheNorwegianTrustFund,theWBisstartingupapilotonaresults-basedfinancingmechanismforprimaryhealthcareservices.Iftheresultsarepositive,itmaydirectpolicydecisionsforupscalingtootherdistricts.
Other ongoing research and activities concern the rationalisation of drugs. The NHIA has put inplacesomecontrolmeasureslikeaformularybasedontheEssentialDrugListwithreimbursementpricesbasedonmedianpricesobservedinthemarket,aswellasprescribingguidelinesforcommonconditions. The investments in a nationwide IT system should further provide the possibility todetectindicationsofirrationaluse,over-useandfraudbypatientsorproviders.
ChangestotheproposedHealthInsuranceBill
Growing unease of the NHIA on the functioning of the DMHIS as independent, autonomous anddecentralisedcompanieswiththeirowngoverningboards,subsidisedbytheNHIAbutwithoutclearsupervisionor administrativeand financial controlmechanismshas led theNHIA to commissionastudywhich informed a revisionofAct 650on thehealth insurance law.. Simultaneously, theActcoversissueslikethebenefitpackage,tariffstructure,qualityofcareetc.Box2belowsummarisesthemainchangesproposedbytherevisedAct.Atthetimeofwriting,theDraftActhasbeensenttoParliament.
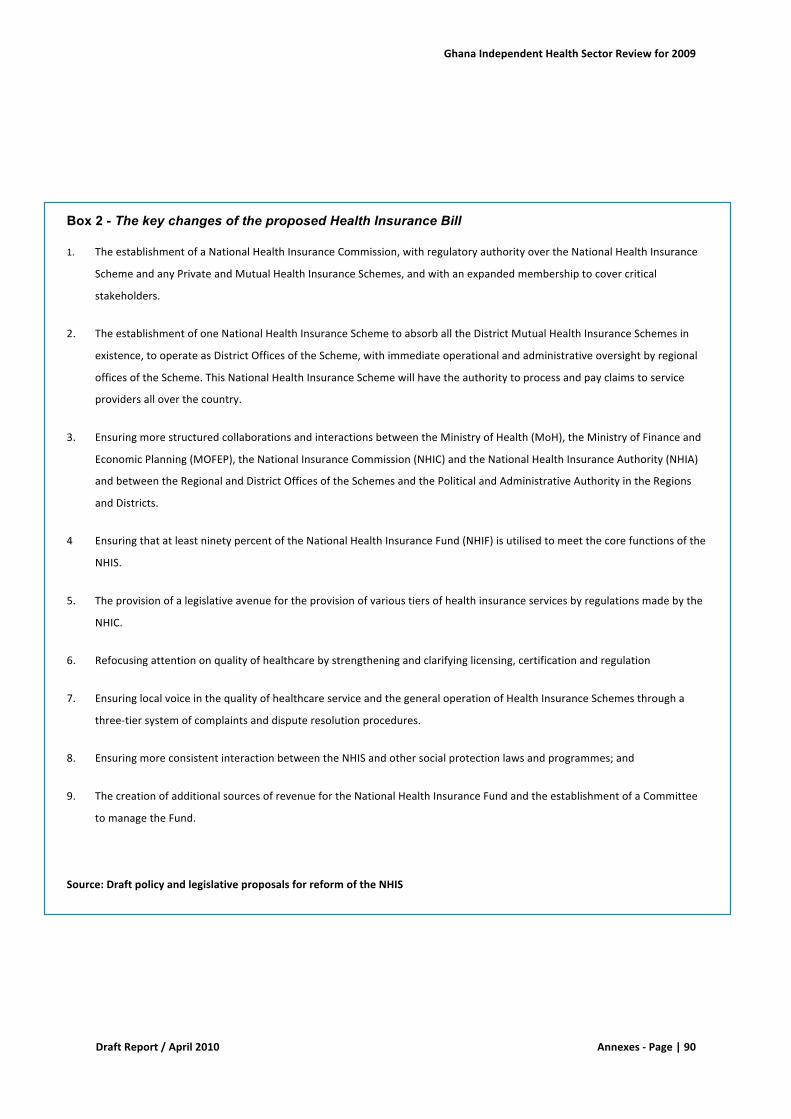
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|90
Box 2 - The key changes of the proposed Health Insurance Bill
1. TheestablishmentofaNationalHealthInsuranceCommission,withregulatoryauthorityovertheNationalHealthInsurance
SchemeandanyPrivateandMutualHealthInsuranceSchemes,andwithanexpandedmembershiptocovercritical
stakeholders.
2. TheestablishmentofoneNationalHealthInsuranceSchemetoabsorballtheDistrictMutualHealthInsuranceSchemesin
existence,tooperateasDistrictOfficesoftheScheme,withimmediateoperationalandadministrativeoversightbyregional
officesoftheScheme.ThisNationalHealthInsuranceSchemewillhavetheauthoritytoprocessandpayclaimstoservice
providersalloverthecountry.
3. EnsuringmorestructuredcollaborationsandinteractionsbetweentheMinistryofHealth(MoH),theMinistryofFinanceand
EconomicPlanning(MOFEP),theNationalInsuranceCommission(NHIC)andtheNationalHealthInsuranceAuthority(NHIA)
andbetweentheRegionalandDistrictOfficesoftheSchemesandthePoliticalandAdministrativeAuthorityintheRegions
andDistricts.
4 EnsuringthatatleastninetypercentoftheNationalHealthInsuranceFund(NHIF)isutilisedtomeetthecorefunctionsofthe
NHIS.
5. Theprovisionofalegislativeavenuefortheprovisionofvarioustiersofhealthinsuranceservicesbyregulationsmadebythe
NHIC.
6. Refocusingattentiononqualityofhealthcarebystrengtheningandclarifyinglicensing,certificationandregulation
7. EnsuringlocalvoiceinthequalityofhealthcareserviceandthegeneraloperationofHealthInsuranceSchemesthrougha
three-tiersystemofcomplaintsanddisputeresolutionprocedures.
8. EnsuringmoreconsistentinteractionbetweentheNHISandothersocialprotectionlawsandprogrammes;and
9. ThecreationofadditionalsourcesofrevenuefortheNationalHealthInsuranceFundandtheestablishmentofaCommittee
tomanagetheFund.
Source:DraftpolicyandlegislativeproposalsforreformoftheNHIS
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|91
Annex9.NoteonCHPS
TheCommunity-basedHealthPlanningandServices(CHPS)initiativeisaprogramstrategyadoptedbytheMoHasanationalprogrammetobridgethegapinhealthcareaccess.CHIPSisdesignedtotranslate innovations fromanexperimentalstudyof theNavrongoHealthResearchCentre (NHRC)intoanationalprogramfor improvingtheaccessibility,efficiency,andqualityofhealthandfamilyplanning services (Binkaetal.1995;Penceetal.2001;Debpuuretal.2002).Within theFiveYearProgramme of Work 2007-2011, the CHPs implementation is designed to guide national healthreformstosupportcommunity-basedprimaryhealthcareascomponentofthepro-poorservices57.CHPSwas launchedbytheMoHwithaviewto improvingaccessibilitytoprimaryhealthcare.Thiswasagainstabackgroundthatdespitetheexistencefortwodecadesof“healthforall”policies, in1990morethan70percentofallGhanaiansstilllivedmorethaneightkilometresfromthenearestprovider, and rural infantmortality rateswere 50 percent higher than corresponding urban rates(MoH1998).Henceimprovingaccesstohealth-caredelivery,therefore,remainedaprimarygoalofhealth-sectorreforminthe1990s.At itscore, theGhanaCommunity-basedHealthPlanningandServices initiativebroughttoanendvariousverticalprogramsandestablishedmechanismsforthedecentralizedadministrationofhealthcare. This initiative involves a process of evidence-based organizational change for extending thelogicofthesector-wideapproachtothecommunitylevel.Among the essential elements of the CHPs intervention is the creation of community healthcompounds. Community health services require a simple facility that provides a room for thecommunityhealthofficer’slivingareaandanotherforaclinic.Developingsuchfacilitiescontributestocommunityownershipof theCHPS initiativeby involving local leaders inplanningandresourcemobilizationandvolunteersforconstructionwork.Inaddition,CHIPalsopromotesprocurementofessential equipments for primary health care services and logistics (including bicycles andmotorbikes),pluspostingcommunityhealthofficerstothecompounds.Thepostedofficersareexpectedtocarryoutclinicalandcommunityoutreachservices includingmakinghouseholdvisitstoprovidefamilyplanningservices,healtheducation,andambulatorycareandoutreachclinics forchildhoodimmunization. The CHIP outreach is designed to serve as a vital referral link between the healthfacilitiesandcommunity.CurrentStatusofCHPs:An in-depth reviewof theCHIPSwasundertakenaspartof theannualhealth sector review2008withmixedresultshighlightedbelow58:
• CHPS involved six general implementation activities “CHPSMilestones” includingplanning,community entry, community compound construction, communityhealthofficer, essentialequipmentandvolunteers.CompletionofthesesixmilestonesheraldsafunctionalCHPS.• EvidencesuggestthatthedefinitionandunderstandingofCHPsisnotconsistentacrossboard,andhencemost of theCHPSprogrammes werefocusing onbuilding compoundsfor curative services and little outreach services to the detriment of preventive andpromotiveprogrammes.• CHIPs compounds have grown from 19 in 2000 to 401 in 2008 though overallimplementation of the programme of the CHPS programme nationwide has been belowaverage(only31%oftheplannedoutput).
57FrankNyator,J.KokuAwonor-Williamsetal“Thecommunitybasedplanningandservicesinitiative(CHIPS):Fosteringevidencebasedorganizationalinitiativeinaresourcesconstrainedsetting”;2003.No180.PopulationCouncil58In-depthReviewoftheCommunity–basedHealthPlanningservices(CHPS):AReportofoftheAnnualhealthSectorReview2008.FinalReport,Accra,April2009.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|92
• Thenecessarypartnershipamongstakeholders(localgovernment,communities,NGOsanddevelopment partners) and required buy-in for the effective commencement of the CHPShasinpracticalsensenotmaterialized.• TrainingoftheCommunityhealthNurseshasbeenverysuccessfulwithaschoolestablishedin each region. While about 1500 CHN have been absorbed into the GHS, the adequatedeploymentsofmidwivesremainachallenge.• Limited community mobilization skill for CHOs, hence community participation andmobilization component of CHPS is weak leading to more static and curative servicesprovision.
Conclusionandimplications:CHPs initiative isan innovativeevidencebased interventionwithpotential toenhanceaccessibilityandownershipofPHCservicesbycommunities.GhanahasmadeabolddecisionininvestinginCHPsinfrastructure.Afteran initial surge inmomentumespecially in theperiod from1999to2005, theplannedrolloutof theCHPsappears tobe losingmomentum.Hence to revitalize theprogrammetheMoHshouldreaffirmtheCHPSstrategyandprovidetherequiredleadership,settingrealisticrollouttargets,budgetsandcoordination.Onthepositiveside,whereasoverallprogressinscalingupCHPsisbelowexpectations,thereisthepotential opportunity by the MoH to explore avenues within component 4 of the health sectorbudgettoenhanceinvestmentinCHPsinfrastructuresandservices.Toachievethisobjectivethereisneed for advocacy at the district and regional levels to mobilize social groups and traditionalinstitutions to participate in CHP activities. In view of the envisaged increase in skilled healthworkers required for effective delivery of services, this process would benefit from a closermonitoring of the current expansion of production of health workers with a view to trackingemerging human resource requirements to achieve stated objectives including maternal andneonatalhealthtargets.GiventhewidevarietyinexperienceswithCHPS(differentmodels,dependingondifferentfunders)andtheveryslowuptakeinsomeregions,differentinnovativemodelsand/orapproachesmayneedtobeexploredbyregionandurbanversusruralareas.
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|93
Annex10.Listofkeyinformants
Name Position Tel e-mail
SylvesterAniemana MoH,ChiefDirector GeorgDakpallah MoH,DirectorPPME JanetKwansah MoH,PPME,HeadofM&E 0243340760 [email protected] MoH,Director,DepartmentofResearch,
Statistics,InformationManagement
AppiahDenkyira MoH,DirectorHumanResources 020-8199413
HermanDusu MoH,FinancialController 0208164945 [email protected] MoH,HeadFinancialReporting 0244685150 SallyLake MoH,ChiefAdvisor,EconomicsandPFM 0248815352 [email protected]
MoHPPME,CIMU 0242383921 [email protected]
Mr.J.G.K.Abankwa MoHPPME,Head,CIMU Dr.N.K.Gebe Head,BioMedicalEngineeringUnit,MoH
PPME0275697828 [email protected]
AlhajiSaakaDumba MoH,HeadofTransport 0208240923 [email protected] MoH,HealthEconomist,TA EliasKavinahSory GHS,DirectorGeneral 662014 GorgeAmofah GHS,DeputyDirector 0244322843 [email protected] GHS,DirectorPPMEDivision 0206010001 [email protected] GHS,DirectorofFinance 021684809 [email protected]
Mr.DanOsei GHS,DeputyDirectorPPME? [email protected]
Dr.CarolineJehu-Appiah GHS,DeputyDirectorPPME 021681367 [email protected]
PhilipAkanzingeN.Asenah GHS,ChiefAdministrator,NHIS 021662014 [email protected] GHS,ProgrammeManager,NCDs 0244379199 [email protected] GHS,ReproductiveHealth DanielDarko GHS,Head,CentreforHealth
InformationManagement
Dedzo GHS,HRD SaidAl-Hussain GHS,DeputyDirectorHRTraining&
Development
JustinaKAnsah GHS,? 0208162812020666429
Mr.Yahya GHS,Head,EstatesManagementUnit Dr.N.Adjebu GHS,Head,BioMedicalEngineeringUnit Mr.EboHammond GHS,DeputyDirector,Transport 0208118563 [email protected] GHS,Director,HASS Mr.K.Addai-Donkoh GHS,Director,SSDM PhilipK.Amoo KorlebuTeachingHospital,Head
PublicHealth0243238188 [email protected]
BenAnnan KorlebuTeachingHospital,DirectormedicalAffairs
0208127176
KombianKambarin KorlebuTeachingHospital,Ag.DirectorofAdminstration
0208129057 [email protected]
IreneAkuaAgyepong RegionalDirector,GreaterAccraRegion 0208133850 [email protected] DistrictDirector,DHMTGhanaWest(and
allDHMTmembers)0244121272 [email protected]
GeorginaAmankwa DistrictDirector,DHMT,Ledzokuku-Krowor,Accra(andallmembersofthe
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|94
DHMT)IsaacLartev HIO,NortherRegionalHealth
Directorate,Tamale
ImoroAhmedMuhusina HIO,Savelegu-NontonDHMT,NorthernRegion
AkwesiTsumasi RegionalDirector,NorthernRegion Tawiah DDH–Do- JacobMahama DDPH–Do_ Lartey DDH-Do_ AwonorWilliams RegionalDirectorNorthUpperWest Margaret AgDHS,SavulangeNanton
0208244284 P.OBox45Savulange–Nanton
JohnBorah VPNursingandMidwivestrainingschool,Tamale
KenSagoe CEO,TamaleTeachingHospital,Tamale
JamesBoateng CHAG,Projectsmanager 0244150229 [email protected] CHAG,TA FelixNyante NursingandMidwiferyCouncil,Deputy
Registrar0244251638 [email protected]
NicholasA.Tweneboa NHIA,DirectorofOperations 0208150401 [email protected] NBTS,Director 0208162812 Ms.BenedictaKwame MoF,healthfocalpoint 0243659633 Mr.EmmanuelAdjololo MoF,healthofficer DanielKertesz WHO,Representative 024434200 [email protected] UNAIDS,CountryCoordinator 0244330626 [email protected] WB,SeniorEconomist(Health) 021229681 [email protected] EmbassyoftheKingdomofthe
Netherlands,HealthAdviser0540667501 [email protected]
RuudvanderHelm EmbassyoftheKingdomoftheNetherlands,FirstSecretary,SeniorEconomicAdvisor
021214350 [email protected]
TheophlusAyugane EmbassyoftheKingdomoftheNetherlands,HealthAdviser
AnitaD’Almeida DanishEmbassy SelassiD’Almeida WHO [email protected] UNFPA AndreasGrub NetworkofMutualHealthOrganisations
ofGhana0264329394 [email protected]
JanBorg HSAO,TA,Danida
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|95
Annex11.Referencesanddocumentsconsulted
MoH,FinancialStatement2006,2007,2008and2009(draft)MoH,Accounting,TreasuryandFinancialReportingRulesandInstructions,2009MoH,AnnualProgrammeofWorks2007,2008,2009and2010MoH,IndependentReviewsofthehealthsectorprogrammeofwork2007and2008MoH,PublicFinancialManagementStrengtheningIssuesPaper,December2008MoH,PFMStrengtheningactionframework,2009MoH,HumanResourcePoliciesandStrategiesfortheHealthSector2007-2011MoH,HumanResourcePolicyandStrategiesfortheHealthSector,2007-2011MoH,CapitalInvestmentPlanIII(2007–2011)–CIMUofthePPMEMoH,ProgressReportonImplementationof2007CapitalInvestmentPlanMoH,2008AnnualReportonImplementationof5-yearPOWIIIMoH,Accounting,TreasuryandFinancialReportingRulesandInstructions(Jan2010Revision)MoH,2009Performance/AnnualReport–CapitalInvestmentManagementUnit,PPMEMoH,2009CapitalInvestmentPlan–CapitalInvestmentManagementUnit,PPMEMoH,Reporton2009BudgetExecution–CapitalInvestmentManagementUnit,PPMEMoH,Reporton2009EquipmentProjects–BioMedicalEngineeringUnit,PPMEMoH,DraftFinancialStatementforYearEnded31stDecember2009–FinanceDirectorateMoH,AuditedFinancialStatementforYearEnded31stDecember2008–FinanceDirectorateMoH,DataRepositoryFramework(draft)MoH,LegalandPolicyFrameworkforHealthInformationandHealthDataReporting(Draft)MoH/HMN,HealthInformationManagementStrategicPlan2007TO2011(draft)MoH,NationalHealthPolicy,2007MoH,HealthResearchAgenda,2007(draft)MoH/HMN,GhanaHealthInformationSystem:NationalLevelReviewandAssessmentReport,2006
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|96
MoH,ABulletinofHealthInformation:InformationForAction,2001(2),2004(1)MoH/GHS/CHIM.InformationforAction:UsingDataforDecisionMaking.AannualonuseofinformationfordecisionsupportatdistrictlevelGHS,AnnualReport,2008GHS,AnnualReport,2008GHS,BudgetGuidelines,2009GHS,DraftHandingOverNotestotheTransitionalTeam,GHS,January2009GHS,DraftHandingOverNotestotheTransitionalTeam,GHS,January2009GHS,HumanResourceDivision,3YearActivityPlan2009-2011,May2009GHS,March2010ReportonPrimaryHealthCareServices–PPMEGHS,RegionalPlansforRollingOutCHPS–PPMEGHS,ReportonPercentofPopulationCoveredbyFunctional/CompletedZonesasat31stDecember2009–PPMENHIS,AllocationFormula2009and2010(draftOctober2009)NHIS,Conceptpaper,PolicyandLegislativeReviewoftheNationalHealthInsuranceScheme,October2009NHIS,DraftpolicyandlegislativeproposalsforreformoftheNationalHealthInsuranceSchemes,October2009MoF,AnnualBudgetStatement2009MoUonearmarkedfunding(draft)AideMemoire,JointMinistryofHealth-PartnersBusinessMeeting,GIMPA,Accra,16thto18thNovember2009AideMemoire,WorldBank,Ghana-HealthInsuranceProject,Mid-TermReviewMissionDecember7-17,2009CentreforHealthandSocialService,Dr.SamAdjeietal.LiteraturereviewofthekeyissuesandsuggestedareasforfurtherresearchinGhana,2010(draft)WorldBank,InvestinginHealthinGhana:AReviewofHealthFinancingandtheNationalHealthInsuranceScheme,May2009(draft)WorldBank,ExternalReviewofPublicExpendituresandFinancialManagement,VolumeIandII,May2009
GhanaIndependentHealthSectorReviewfor2009
DraftReport/April2010 Annexes-Page|97
NursingandMidwiferyCouncilofGhana:CurriculumfortheCommunityHealthNursing(CHN)Programme.July2007NursesandMidwifeCouncilofGhana:CurriculumfortheRegisteredGeneralNursing(RGN)Programme:July20072009AnnualReport–VoltaRegionalHospital,HoReviewoftheCapitalInvestmentManagementProgrammeII–DESERV-JMAssociatesforMoHNovember2008AideMemoir–MoHandHealthPartners





























