Embed Size (px)
Citation preview

Review ArticleThe Physiological and Biochemical Outcomes Associated witha Reflexology Treatment: A Systematic Review
J. E. M. McCullough, S. D. Liddle, M. Sinclair, C. Close, and C. M. Hughes
Institute of Nursing and Health Research, University of Ulster, Jordanstown Campus, Shore Road,Newtownabbey, County Antrim BT37 0QB, UK
Correspondence should be addressed to C. M. Hughes; [email protected]
Received 21 November 2013; Accepted 10 March 2014; Published 5 May 2014
Academic Editor: Peter Mackereth
Copyright © 2014 J. E. M. McCullough et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. Reflexology is one of the top forms of complementary and alternative medicine in the UK and is used for healthcare bya diverse range of people. However, it is offered by few healthcare providers as little scientific evidence is available explaining howit works or any health benefits it may confer. The aim of this review was to assess the current evidence available from reflexologyrandomised controlled trials (RCTs) that have investigated changes in physiological or biochemical outcomes.Methods. Guidelinesfrom the Cochrane Handbook of Systematic Reviews of Interventions were followed: the following databases were searched frominception toDecember 2013: AMED, CAMQuest, CINAHLPlus, Cochrane Central Register of Controlled Trials, Embase,MedlineOvid, Proquest, and Pubmed. Risk of bias was assessed independently by two members of the review team and overall strength ofthe evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation guidelines. Results.Seventeen eligible RCTsmet all inclusion criteria. A total of 34 objective outcomemeasures were analysed. Although twelve studiesshowed significant changes within the reflexology group, only three studies investigating blood pressure, cardiac index, and salivaryamylase resulted in significant between group changes in favour of reflexology. The overall quality of the studies was low.
1. Introduction
Reflexology is considered to be a form of complementaryand alternative medicine (CAM). CAM refers to treatmentsused either as an adjunct to, or instead of conventionalmedical care. The House of Lords Select Committee forScience and Technology [1] has placed reflexology in grouptwo, categorised as therapies used mostly to complementconventional medicine. Its popularity has increased in recentyears as the public seek more holistic ways to maintain goodhealth and well-being [2]. In fact CAM is increasingly beingconsidered as a safe and effective way of reducing the causesand impacts of pain and disease.
Reflexology is one of the top six forms of CAMused in theUK [3] and, according to a survey by McDonough et al. [4],it is the second most popular form of CAM used in NorthernIreland. In 2007 a national survey in the USA reported that38% of adults and 12% of children were using some form of
CAM [5] and in the same year a Norwegian survey indicatedthat 5.6% of the population had used reflexology in thepreceding twelve months [6]. In support, a national surveycarried out in Denmark in 2005 showed that 21% of thepopulation had used reflexology at some point in their livesand 6% had used it within the previous year [7]. In the UKthere are thought to be over 40,000 complementary therapistsand the sector is expected to grow by over 30% from £213million in 2009 to £282 million by 2014 [8].
While the general population is spending large sums ofmoney on CAM, health care professionals are reluctant topromote any benefits for such treatments. Reflexology hascome under much criticism based predominantly on thedearth of high quality evidence supporting a clear scientificmechanism of action for the treatment. Most of the researchcarried out in this area has investigated the psychologicaloutcomes from reflexology focusing on qualitative outcomes.Researchers have repeatedly shown that reflexology has a
Hindawi Publishing CorporationEvidence-Based Complementary and Alternative MedicineVolume 2014, Article ID 502123, 16 pageshttp://dx.doi.org/10.1155/2014/502123

2 Evidence-Based Complementary and Alternative Medicine
Table 1: GRADE evaluation guidelines [29].
Study limitationsThe quality of the evidence was downgraded if serious study limitations existed such as a lack of allocationconcealment, lack of blinding, large loss to follow-up, or randomized trials stopped early for benefit or theselective reporting of outcomes.
Inconsistency The quality of the evidence was downgraded if there was inconsistency in the results, for example, if studiesshowed varying or different effects of the same intervention.
IndirectnessThe quality of the evidence was downgraded if there was a level of indirectness in the studies, for example, ifinterventions had not been compared directly to one another or if the studies investigated a restricted version ofthe main review question in terms of population, intervention, or outcomes.
Imprecision The quality of the evidence was downgraded if the studies were imprecise in any respect, for example, if theyincluded few participants and few events and thus had wide confidence intervals.
Publication bias The quality of the evidence was downgraded if some element of reporting bias was evident, for example, authorsfailed to report all the outcomes they set out to or perhaps only reported the positive findings of their study.
positive effect on quality of life, stress, anxiety, and pain [9–12]. However, few studies have attempted to correlate theseresults with any quantitative physiological or biochemicaloutcomes.
To date six literature reviews of reflexology have beencarried out [13–18] and three further reviews on reflexologyfor cancer care [19], pain and fatigue [2], and pain man-agement [11] are also available. None of these have focusedspecifically on the quantitative aspect of the results available,although the overwhelming opinion from the authors is thatthere is not enough high quality RCTs to produce significantscientific data for recommending reflexology as an evidence-based treatment option.
The exact mechanism of action of reflexology has yetto be confirmed; however, various theories have been pro-posed and Tiran and Chummun [20] have detailed manyof the current theories in their paper. One of the earliest isthe haemodynamic theory which suggests that reflexologystimulation enhances blood flow to the corresponding organor body part [21]. The findings of an investigation usingcolour Doppler sonography [22] showed a significant effecton blood flow to the kidney during reflexology and aninvestigation by Jones et al. [3] displayed some evidence tosupport this theory. Recent research has also indicated thatchanges in the dermal layer structures and luminosity of theskin at specific reflex points on the feet may give rise tothe changes felt by therapists during a treatment [23]. The“nerve impulse theory” proposes that stimulation applied tospecific reflex points on the feet enhance nervous connectionto the corresponding body parts [24]. This is currently themost promising theory and suggests that the benefits ofreflexology may be brought about by modulation of theautonomic nervous system (ANS). The ANS regulates bodysystems that are under unconscious control such as breathing,heart rate, and blood pressure.These parameters are sensitiveto stressors and fluctuate according to the physical or psy-chological changes experienced by an individual, via vagalmodulation which controls calming and restful changes andregular functioning or sympathetic modulation, responsiblefor controlling arousal and the “fight or flight” response. ANSmodulation has also been supported by Hughes et al. [25]and Sliz et al. [26]. A commonly held belief, often cited by
reflexologists and suggested by Poole et al. [27] and Tiran[28], states that reflexology may work by stimulating therelease of endorphins and in this waymay help to reduce painand increase feelings of wellbeing and relaxation.
2. The Review
2.1. Aim. This systematic review aimed to assess the quality ofevidence fromRCTs that have tested changes in physiologicalor biochemical outcome parameters as a result of reflexology.
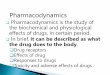
2.2. Design. The Cochrane guidelines for conducting sys-tematic reviews were followed throughout this review. Aninclusion and exclusion protocol was devised to determinewhich studies were included for evaluation, and the risk ofbias (ROB) of each eligible RCT was assessed independentlyby two members of the review team.The PRISMA guidelines[43] were used (Figure 1) and the methodological quality ofeach trial was determined by carrying out an ROB assess-ment following guidelines in the Cochrane Handbook forSystematic Reviews [44].The strength of the evidence for theRCTs was assessed according to the constructs of the GRADE(Grading of Recommendations, Assessment, Development,and Evaluation) tool [29] adapted to suit this review (Table 1).
2.3. Search Methods. The following databases were searchedfrom their inception to December 2013: AMED, CAMQuest,CINAHL Plus, Cochrane Central Register of ControlledTrials, Embase,MedlineOvid, Proquest, and Pubmed. Searchterms used in various combinations were “reflexology, blood,urine, saliva, plasma, electrolyte, hormone, neurotransmitter,neuroregulator, immune response, lymph, lymphatic sys-tem, respiratory function, respiratory function tests, bloodpressure, heart rate, foetal heart rate, fetal heart rate andendorphin”. Hand searches of relevant journals and refer-ence lists along with citation tracking were undertaken toensure comprehensive coverage of all relevant literature.The references of all articles were hand searched. Identifiedpublications were read either as abstracts or full texts.

Evidence-Based Complementary and Alternative Medicine 3
Elig
ibili
tySc
reen
ing
Iden
tifica
tion
Inclu
ded
17 studies included for review
Duplicates removed
Articles assessed for eligibility
Screened
Hand searchDatabase screening
Removed
No physiological/biochemical
Full text articles excluded
Combination of therapies used
Not English (translation not available)
(Brygge, 2002)
n = 19332 n = 5
n = 19337
irrelevant n = 19193
outcome n = 47
n = 70
n = 27
n = 45No full text n = 2
n = 1
Not trials n = 5
Figure 1: Systematic literature search PRISMA flow diagram.
2.4. Search Outcome. A total of 19337 articles were retrievedvia the initial database and hand searches. Twenty-threestudies remained after the exclusion of irrelevant studies(19193), those with no biochemical or physiological outcomemeasure (47), those articles not available in English (27),duplicates (45), and those where the full text was not available(2). Another five studieswere excluded as theywere not RCTs,and one further RCTwas excluded as it used a combination ofreflexology plus backmassage for the intervention group [45].Therefore, 17 papers were extracted for systematic review andcritical appraisal. The risk of bias is detailed in Table 2.
2.5. Data Abstraction and Synthesis. All results were screenedby two independent reviewers and differences in opinionwere resolved through discussion to reach a consensus.Exclusions were applied using the criteria in Table 3. Inaddition, when insufficient information was available fromthe paper, the review team contacted the study authors.
Owing to the consistent use of blood pressure (BP) andheart rate as outcomemeasures in the studies collated, ameta-analysis was conducted using Review Manager 5.2 to gain
further insight into the effects of reflexology across a widerange of populations (Figures 2, 3, and 4).
3. Results
Twelve randomised controlled trials and five feasibility orpilot randomised controlled trials, involving a total of 697participants, were reviewed (Table 4). The trial participantsranged from healthy volunteers to those suffering from awide range of musculoskeletal, neurological, and systemicconditions including people with breast cancer, coronaryartery bypass graft (CABG), chronic heart failure (CHF),nursing home residents with dementia and cancer, chronicobstructive pulmonary disease (COPD), multiple sclerosis(MS), pregnant women, and women failing to ovulate.
In total, 34 physiological or biochemical outcome mea-sures were analysed in the 17 included studies. Significantwithin reflexology group changes were recorded for 11 out-come measures. These were blood pressure in five studies,heart rate in three studies, cortisol in two studies, sali-vary amylase, lymphocyte production, heart rate variability

4 Evidence-Based Complementary and Alternative Medicine
Table2:Risk
ofbias
(ROB)
analysis.
Stud
yTy
peof
study
Adequate
sequ
ence
generatio
n
Allo
catio
nconcealm
ent
Adequate
blinding
-participant
Adequate
blinding
-clinician
Adequate
blinding
-ou
tcom
eassessor
Incomplete
outcom
edata
assessment
Selective
repo
rtingbias
Other
bias
Risk
ofbias
Jonese
tal.,2013
[30]
RCT
Low
Low
Low
High
Low
Low
Low
Low
Low
Hod
gson
andLafferty,2012
[31]
Pilot
Unclear
Unclear
High
High
Low
Low
Low
Low
Unclear
Jonese
tal.,2012
[3]
RCT
Low
Low
Low
High
Low
Unclear
Low
Low
Low
Ruiz-Padialetal.,2012
[32]
RCT
Unclear
Unclear
Low
High
Unclear
Low
Low
Low
Unclear
Slizetal.,2012
[26]
RCT
Low
Low
High
High
Unclear
Low
Low
Low
Low
Hug
hese
tal.,2011[25]
Pilot
Low
Low
Low
High
Low
Low
Low
Low
Low
Luetal.,2011[33]
RCT
Unclear
Unclear
Low
Unclear
Unclear
Low
Unclear
Unclear
Unclear
Moeinietal.,2011[34]
RCT
Low
High
High
High
High
Unclear
Low
Low
Unclear
Green
etal.,2010
[35]
RCT
Low
Low
High
High
Unclear
Low
Low
Unclear
Low
Holtetal.,2009
[36]
RCT
Low
Low
Low
High
Low
Low
Low
Low
Low
Mackereth
etal.,2009
[37]
RCT
Low
Low
High
High
Unclear
High
Low
Unclear
Unclear
Hod
gson
andAnd
ersen,
2008
[38]
RCT
High
High
High
High
Low
Unclear
High
Unclear
High
Gun
narsdo
ttira
ndJonsdo
ttir,2007
[39]
Pilot
Unclear
Unclear
Unclear
High
High
Unclear
Low
Low
Unclear
McV
icar
etal.,2007[40]
Pilot
Unclear
Unclear
High
High
High
High
High
Low
High
Wilk
insonetal.,2006
[41]
RCT
Unclear
Unclear
High
High
Unclear
High
High
High
High
Mollart,2003[10]
Unclear
High
High
High
High
High
High
Unclear
High
Frankel,1997
[42]
Pilot
Unclear
Low
Unclear
High
Unclear
Low
Low
Low
Unclear

Evidence-Based Complementary and Alternative Medicine 5
Table 3: Systematic literature search inclusion and exclusion crite-ria.
Inclusion criteria Exclusion criteriaFoot reflexology treatmentonly
Self-treatmentonly
A quantitative biochemicaloutcome measure
Qualitative outcomemeasure only
A quantitative physiologicaloutcome measure
Full text notavailable
Randomised controlledtrials
Full article not available inEnglish
Pilot studies Duplicate
(HRV), R-R interval, pulse pressure, cardiac output, cardiacindex (CI), and blood oxygen level dependant (BOLD)response, in one study each (Table 4). However, only fouroutcome measures showed significant changes between thereflexology and control group: salivary amylase [38], systolicanddiastolic blood pressure [34], andCI [3]. Ruiz-Padial et al.[32] demonstrated significant changes in blood pressure as afactor of time, treatment number, and intervention. Eight ofthe studies compared reflexology to an active CAM controlinstead of sham treatment and eleven used a control measurewhich involved touching the participants feet. In one studythe same reflexology treatmentwas compared in two differentparticipant groups [33].
4. GRADE Analysis
The strength of the evidence presented by the 17 includedRCTs was assessed using the GRADE criteria which resultedin the quality of evidence being rated as very low (Table 5).However, assessment must be viewed with caution. TheGRADE start score was four, the maximum available, whichindicated that all the studies included had an RCT designwhich is considered the gold standard [44]. Study limitationssurrounding blinding were considered serious (−2). How-ever, blinding of participants, therapists, and outcome asses-sors in reflexology trials is extremely challenging as shamtreatment to the feet that mimics reflexology is difficult toachievewithout some active stimulation of reflexology points.Neither can any therapist be truly blinded as they must haveprior knowledge of protocols and whether a true or shamtreatment is to be employed. Table 2 shows the trend towardshigh ROB for blinding of participants and, in particular,therapists. The GRADE score was further marked down forserious inconsistencies between studies and indirectness ofresults (−1). However, due to the nature of this review, studieswere not comparable given that different outcome measuresand populations were assessed. All included studies had smallsample sizes which resulted in a further downgrade due toimprecision.
5. Physiological Outcome Measures
5.1. Cardiac Parameters. The physiological parameter mostcommonly investigated within reflexology studies was BP,
with 13 studies including this as an outcome measure. BPresponded in a positive manner to reflexology in half of thestudies: Mollart [10], Mc Vicar et al. [40], Mackereth et al.[37], Hughes et al. [25], Lu et al. [33], and Moeini et al. [34].The work by Moeini et al. [34] was the only trial to showa significant difference between the treatment and controlgroups.
Contrary to all of the other studies in this review Ruiz-Padial et al. [32] found that BP increased following reflex-ology, foot massage, and sitting quietly in a room. However,average BP results at baseline were different for each of thethree study groups and the results presented were as a func-tion of time, treatment number, and treatment interactionwhich made them difficult to interpret.
Changes in heart rate (HR) were investigated in ninestudies and positive results were demonstrated by Mc Vicaret al. [40], Wilkinson et al. [41], and Mackereth et al. [37];however, none were statistically significant.
Jones et al. [3] investigated a wide range of cardiac param-eters with cardiac index (CI) only having a significant changebetween the active and control groups. A within reflexologygroup change in cardiac output (CO), the volume of bloodbeing pumped by the heart per minute, was significantcompared with baseline.
5.2. Functional Magnetic Resonance Imaging (fMRI). fMRIinvolves the use of MRI to detect visible changes that occurin the brain as a result of some external stimuli. Sliz etal. [26] investigated the effects of foot treatments on brainactivity using fMRI and evaluated the findings using theblood oxygen level demand (BOLD) response which relatesto changes in blood flow to the brain during activation.The results showed positive BOLD responses for reflexology,Swedish massage and the rest only control group, but not inresponse to massage with a wooden roller massager.
6. Biochemical Outcome Measures
A total of seven studies investigated a biochemical response toreflexology.These studies tended to focus on stress hormonesandwere correlatedwith qualitative data on stress and anxietylevels.
Significant within group decreases in cortisol were foundby Mackereth et al. [37] and Hodgson and Lafferty [31] butnot by Mc Vicar et al. [40]. However, no between groupdifferences were found in these studies. No changes wereobserved for melatonin [40] or progesterone [36]. However,Hodgson and Andersen [38] found significant reductions insalivary amylase within the reflexology group. Green et al.[35] found a significant increase in CD25+ cells, involved incancer cell death and tumour growth inhibition, within thereflexology and control massage groups.
7. Meta-Analysis
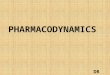
Ameta-analysis was performed on seven papers investigatingBP and HR [3, 25, 30, 34, 37, 38, 40]. The study by Wilkinsonet al. [41] was not included as only one participant completed

6 Evidence-Based Complementary and Alternative Medicine
Table4:Tableo
fstudy
characteris
tics.
Stud
yParticipants
Interventio
nCom
paris
onDropo
uts
Outcomem
easure
Adverse
effects
Results
Com
ments
Jonese
tal.,2013
[30]
(Scotland
,UK)
Dou
ble-blind
RCT
12patie
ntsw
ithstablechronic
heartfailure
4.5m
ins
reflexology
toheartreflex
area
(activeh
eart
point)(In
gham
Metho
d)
4.5m
ins
reflexology
ongrossh
eelarea
Nodrop
outs
occurred
Beat-to
-beat
cardiovascular
parametersH
R,BP
,stroke
index(SI),cardiac
output
(CO),cardiac
index(C
I),total
perip
heralresistance
(TPR
),baroreceptor
up/dow
nevents
(BarUpE
v)/barDwEv
),andheartratev
ariability
(HRV
)
Non
eNosig
.difference
fora
nyou
tcom
efor
either
grou
p
Thea
utho
rssta
tethat
participantsmedication
may
have
maskedany
potentialbenefit
Hod
gson
and
Lafferty,2012
[31]
(USA
)Pilotcrossover
RCTwith
one
week’s
washo
ut
18olderc
ancer
survivorsin
nursingho
mes
4×20mins
reflexology
(Ingh
amMetho
d)
4×20mins
Swedish
massage
tofeet
Nodrop
outs
occurred
Salivarycortiso
lNon
erepo
rted
Sig.change
forb
oth
grou
ps,
nosig
.difference
between
grou
p
Nodetails
regarding
whether
cortiso
llevels
returned
tobaselin
edu
ringthew
asho
utperio
dwereg
iven
Jonese
tal.,2012
[3]
(Scotland
,UK)
Dou
ble-blind
RCT
16healthy
volunteers
4.5m
ins
reflexology
toheartreflex
area
(activeh
eart
point)(In
gham
metho
d)
4.5m
ins
reflexology
ongrossh
eelarea
1due
todata
collectionissue
Beat-to
-beat
cardiovascular
parametersH
R,BP
,stroke
index(SI),cardiac
output
(CO),cardiac
index(C
I),total
perip
heralresistance
(TPR
),baroreceptor
up/dow
nevents
(BarUpE
v)/(Ba
rDwEv
),heartratev
ariability
(HRV
)
Non
erepo
rted
Sig.decrease
inCI
for
interventio
ngrou
p,sig
.changeinCO
from
baselin
efor
interventio
ngrou
p,no
othersig.results,
sig.betweengrou
pdifferencefor
CI
Suggestsalinkbetween
reflexology
stimulation
totheh
eartreflexarea
andcardiacb
lood
flow
andcirculation
Ruiz-Padialet
al.,2012
[32]
(Spain)
RCT
41healthy
volunteers
3×40mins
reflexology
(Ingh
amMetho
d)
3×40mins
(1)N
on-
professio
nalfoo
tmassage
(2)S
eatedin
adarkened
room
Non
ereported
BP,B
RS,H
RV,Inter-beat
interval(IBI)
Somep
ain
repo
rted
for
reflexology
grou
p
Increasesininterbeat
interval,H
RVandBR
Sin
allgroup
s.Sig.increase
inBP
inreflexology
grou
pas
afun
ctionof
time
Thea
utho
rssta
tethat
theincreaseinBP
inthe
reflexology
grou
psuggesta
“co-activ
ation
ofthetwo
branches
oftheA
NS,”
namely
,the
sympatheticand
parasympathetic
pathways

Evidence-Based Complementary and Alternative Medicine 7
Table4:Con
tinued.
Stud
yParticipants
Interventio
nCom
paris
onDropo
uts
Outcomem
easure
Adverse
effects
Results
Com
ments
Slizetal.,2012
[26]
(Canada)
RCT
40healthy
volunteersused
amentalstre
sstestto
increase
stresslevels
1×8.5mins
reflexology
torig
htfoot
only
1×8.5mins
(1)S
wedish
foot
massage
(2)F
oot
massage
with
awoo
denob
ject
tomim
icSw
edish
massage
(3)R
est
Non
ereported
fMRI,blood
oxygen
leveld
ependent
(BOLD
)respon
se(in
dicated
bloo
dflo
wto
areaso
factiv
ation)
Non
erepo
rted
PositiveB
OLD
respon
sein
ACCandPC
Cbrain
region
forreflexolog
y,Sw
edish
massage
and
control,
nosig
.difference
between
grou
ps
TheA
CCandPC
Cregion
softhe
brainare
thou
ghttobe
linkedto
emotionalrespo
nse,
learning
,and
mem
ory
andarea
lsoinvolved
inmajor
depressiv
edisorders(Dervetsetal.,
2008)
Hug
hese
tal.,
2011[25]
(Northern
Ireland,UK)
FeasibilityRC
T
25healthy
volunteersusing
amentalstre
sstestto
increase
stresslevels
1×20mins
reflexology
1×20mins
relaxatio
nand
foot
hold
Nodrop
outsoccurred
BP,H
RNon
erepo
rted
Sig.redu
ctionin
SBPfor
interventio
nandcontrol
grou
ps,
sig.reductio
nin
DBP
ininterventio
ngrou
p,no
sig.changeinHR,
nosig
.difference
between
grou
ps
Luetal.,2011
[33]
(Taiwan)
RCT
37participants
1×60mins
reflexology
(FatherJosef
Metho
d)CA
Dpatie
nts
1×60mins
reflexology
(FatherJosef
Metho
d)healthy
patie
nts
Non
ereported
ECG,B
P,HRV
,PP,RR
INon
erepo
rted
Sig.redu
ctionin
BPand
PPforb
othgrou
ps,sig
increase
inRR
Iin
reflexology
grou
p.Sig.change
inHRV
inbo
thgrou
ps,
nosig
.difference
between
grou
ps
HRV
benefitslasted
longer
forC
ADpatie
nts
(60m
ins)compared
with
controls(30m
ins)
Moeinietal.,
2011[34]
(Iran)
RCT
50CA
BGpatie
nts
1×30mins
reflexotherapy
pre-surgery
Usualcare
Non
ereported
BP,H
R,respira
tory
rate
Non
erepo
rted
Sigredu
ctionin
SBPand
DBP
inreflexology
grou
p,no
nsignificantreductio
nin
HRandrespira
tionrate
forreflexolog
y,sig
.betweengrou
psdifferenceinSB
PandDBP
Green
etal.,
2010
[35]
(UK)
RCT
183Ea
rlysta
gebreastcancer
(6weeks
post-
surgery)
8×tre
atment
(weeklysession
duratio
nun
know
n)
(1)S
elf-initiated
supp
ort
(2)8
treatments
atweekly
intervalso
fSIS
with
head
massage
Fulldatasetswere
obtained
for8
7participants,
intentionto
treatwas
carriedou
t
Bloo
dlymph
ocytes
(CD
profi
les)cytokine
prod
uctio
n(Th
1,Th
2),
prolactin
,cortisol,
grow
thho
rmon
e
Non
erepo
rted
Sig.increase
inCD
25+
cells
inreflexandmassage
grou
pcomparedwith
baselin
e.Sig.increase
inCD
25+cells
between
massage
andSIS,
noothersig.results,
nosig
.difference
between
grou
ps
Results
foro
nly47.5%of
thep
artic
ipantswere
repo
rted
duetoalosso
fbloo
dsampleinthe
analysisprocess

8 Evidence-Based Complementary and Alternative Medicine
Table4:Con
tinued.
Stud
yParticipants
Interventio
nCom
paris
onDropo
uts
Outcomem
easure
Adverse
effects
Results
Com
ments
Holtetal.,2009
[36]
(UK)
RCT
49Wom
enwith
anovulation7×60mins
reflexology
Sham
reflexology
9drop
outs
Serum
progesterone
Non
erepo
rted
Ovulationoccurred
ininterventio
n(42%
)and
sham
grou
ps(46%
),Pregnancyoccurred
ininterventio
n(15%
)and
sham
grou
ps(9%),
nosig
.difference
between
grou
ps
Thea
utho
rssta
tedthat
ther
ateo
fovulatio
nin
thistrialw
asdo
ublethat
expected
giving
riseto
anidea
thatthes
ham
treatmentm
ayalso
have
hadan
effecto
nthe
outcom
emeasures
Mackereth
etal.,
2009
[37]
(UK)
CrossoverR
CTwith
4-week
washo
ut
53MSpatie
nts
6×40mins
weekly
reflexology
(Ingh
amMetho
d)
Progressive
muscle
relaxatio
n(PRM
)training
3drop
outs
HRandBP
,salivary
cortiso
lNon
erepo
rted
Sig.decrease
before
and
after
treatmentand
before
andaft
erweeks
1–6for
cortiso
lwith
inreflexology
grou
p,sig
.decreaseinSB
Pand
HRforb
othgrou
ps,
nosig
.chang
einDBP
,no
sig.difference
between
grou
ps
Thev
ariableo
finterest
failedto
return
toinitial
levelsresulting
inprob
lemsrela
tingto
the
orderin
gof
the
treatmentsandthese
interactions
made
analysisvery
difficultto
determ
ine
Hod
gson
and
And
ersen,
2008
[38]
(USA
)Cr
ossoverR
CTwith
nowasho
utperio
d
21dementia
sufferersin
nursingho
mes
4×30mins
weeklyhand
orfoot
reflexology
4×30min
weeklyfriend
lyvisit
Not
stated
BP,pulse,salivary
𝛼-amylase
Non
erepo
rted
Sig.decrease
insalivary
𝛼-amylaseinreflexology
grou
p,no
othersig.results,
significantb
etween
grou
psdifferencein
amylase
Thea
utho
rsdidno
tconsider
theimpactof
thea
bsence
ofaw
asho
utperio
don
results.A
lso,
nodetails
ornu
mbersof
patie
ntsreceiving
hand
orfoot
reflexology
were
given
Gun
narsdo
ttir
andJonsdo
ttir,
2007
[39]
(Iceland)
PilotR
CT
9Coron
ary
artery
bypass
graft
patie
nts
5×30mins
reflexology
(Ingh
amMetho
d)pre
and
post-
surgery
Cream
applicationto
feet(1min)+
30minsrest
2du
etopo
stsurgery
complication
BP,H
R,respira
tionrate
Non
erepo
rted
Sigredu
ctionin
SBPin
controlgroup
,no
sig.difference
between
grou
ps
Anx
ietylevelsin
the
controlgroup
were
consistently
lower
inthe
controlgroup
and
authorsa
ttributeh
igher
anxietyscores
toa
potentiallackof
valid
ityof
SAItotheIceland
icpo
pulatio
n

Evidence-Based Complementary and Alternative Medicine 9
Table4:Con
tinued.
Stud
yParticipants
Interventio
nCom
paris
onDropo
uts
Outcomem
easure
Adverse
effects
Results
Com
ments
McV
icar
etal.,
2007
[40]
(UK)
Pilotcrossover
RCTwith
3-day
washo
ut
30healthy
volunteers
3×60mins
pragmatic
reflexology
Sitting
asa
grou
pin
aquiet
room
Not
stated
Salivarymelaton
in&
cortiso
l,BP
,pulse
rate
Non
erepo
rted
Sign
ificant
redu
ctionin
pulse
andSB
Din
reflexology
grou
p,no
sig.chang
einDBP
,no
sig.chang
eincortiso
lor
melaton
in,
nosig
.difference
between
grou
ps
Authorsstatedthatcarry
over
effectsandordero
ftre
atmentsdu
etostu
dydesig
nmay
have
affected
results.Th
eyalso,
suggestthatsittingin
aroom
asag
roup
may
have
resultedin
anxiety
forsom
econ
trol
participants
Wilk
insonetal.,
2006
[41]
(UK)
RCT
20Ch
ronic
Obstructiv
ePu
lmon
ary
Dise
ase(CO
PD)
patie
nts
4×50min
sessions
Friend
lyvisits
19participantsdidno
tcompletea
llof
the
study
BP,H
R,respira
tionrate,
oxygen
saturatio
n,FV
C,FE
V,vitalcapacity,peak
flow
Non
erepo
rted
Sign
ificant
pre-po
stdecreaseinHR
with
inreflexology
grou
p,no
sig.improvem
entin
HRandPE
Fin
control
grou
p,no
sig,difference
between
grou
ps
Peak
flowsw
ere
self-repo
rted
andas
only
onep
artic
ipant
completed
allofthe
study,these
results
are
open
tobias
Mollart,2003
[10]
(Australia)
Sing
le-blin
dRC
T
69Pregnant
wom
en30
weeks
+gestationwith
foot
oedema
3×15mins
session
lymph
atic
reflexology
(1)R
elaxing
reflexology
(2)R
est
Only20
participants
completed
all3
sessions
BP,ank
le,andfoot
circum
ference
measurements
Non
erepo
rted
Non
significantreductio
nin
BPfora
llgrou
ps,
nonsignificantd
ecreases
inanklea
ndfoot
measurements
Results
from
thefi
rst
treatmentsessio
non
lywerea
nalyseddu
eto
drop
outs
Frankel,1997
[42]
(UK)
PilotR
CT
24healthy
participants
1×45mins
reflexology
(Ingh
amMetho
d)
(1)F
ootm
assage
(2)N
ointerventio
nNon
ereported
Baroreceptor
reflex
sensitivity(BRS
),BP
,sin
usarrhythm
ia(SA)
Non
erepo
rted
Non
significantreductio
nin
BRSforreflexolog
yand
FM(60%
)com
paredwith
notre
atment(50%),
nonsignificantincreasein
SAfre
quency
for
reflexology
andFM
,no
nsignificantd
ifference
betweengrou
ps
Author
suggestsa
“Neuro
theory”m
ayexplainthem
echanism
ofactio
nas
BRSisun
der
ANScontrol
ACC:
anterio
rcingu
latecortex;A
NS:autono
micnervou
ssystem;BarDwEv
:baroreceptord
ownevents;
BarU
pEv:baroreceptor
upevents;
BOLD
:blood
oxygen
leveldependent;BP:bloo
dpressure;BRS
:baroreceptor
reflexs
ensitivity
;CABG
:coron
arya
rteryb
ypassg
raft;CA
D:coron
arya
rteryd
isease;CH
F:chronich
eartfailu
re;C
I:cardiacind
ex;C
O:cardiac
output;C
OPD
:chron
icob
structiv
epulmon
aryd
isease;DBP
:diasto
licbloo
dpressure;ECG
:electrocardiogram
;FEV
:forcedexpiratio
nvolume;FM
:foo
tmassage;fMRI:fun
ctionalm
agnetic
resonanceimaging;FV
C:forced
vitalcapacity
;HR:
heartrate;HRV
:heartratevaria
bility;IBI:
interbeatinterval;PC
C:po
sterio
rcingulatecortex;P
EF:p
eakexpiratory
flow;P
MR:
progressivemuscle
relaxatio
n;PP
:pulse
pressure;R
CT:rando
mise
dcontrolledtrial;RR
I:R-Rinterval;SA:sinus
arrhythm
ia;
SAI:SpielbergersStateA
nxietyInventory;SB
P:systo
licbloo
dpressure;SI:Stroke
Index;SIS:self-initiated
supp
ort;TP
R:totalp
eripheralresistance.

10 Evidence-Based Complementary and Alternative Medicine
Table5:As
sessmento
fqualityusingtheG
RADEsyste
m.
Num
bero
fstudies
andparticipants
Stud
ylim
itatio
nsCon
sistencyof
results
Dire
ctnessof
thee
vidence
Precision
Repo
rtingbias
Overallqu
ality
ofthe
evidence
17RC
Tsandpilot
studies
(697
participants)
startscore=
4
−2serio
uslim
itatio
nsdu
etoprob
lemsw
ithblinding
−2serio
usinconsistency
inresults
between
studies
−1som
eind
irectnessas
moststudies
not
comparable
−1som
eimprecision
dueto
lowparticipantn
umbers
Unlikely
aspo
sitivea
ndnegativ
eeffectsfou
ndVe
rylow

Evidence-Based Complementary and Alternative Medicine 11
Experimental Control Mean difference Mean difference
Hodgson & Andersen 2008
Study or subgroupMean SDTotal MeanSD Total
WeightIV, fixed, 95% CI IV, fixed, 95% CI
−100 −50 0 50 100
Favours (experimental) Favours (control)
124 124 100.0%Total (95% CI)
121
114.9
133.9
123.9
129.04
122.5
122.2
9.9
11.8
16
17.1
16.25
14.207
15.67
10
13
15
12
25
24
25
121
116.5
131.8
129.2
124.16
123
130.8
10.3
10.1
14.8
15.1
17.93
14.207
10.77
11
12
15
12
25
24
25
15.6%15.8%9.6%7.0%13.0%18.0%21.0%
0.00 [−8.64, 8.64]−1.60 [−10.19, 6.99]2.10 [−8.93, 13.13]−5.30 [−18.21, 7.61]4.88 [−4.61, 14.37]
−8.60 [−16.05, −1.15]
Test for overall effect: Z = 0.97 (P = 0.33)
−0.50 [−8.54, 7.54]
Hughes et al. 2011Jones et al. 2012Jones et al. 2013Mackereth et al. 2009McVicar et al. 2007Moeini et al. 2011
Heterogeneity: 𝜒2 = 6.13, df = 6 (P = 0.41); I2 = 2%
−1.69 [−5.10,1.73]
Figure 2: Meta-analysis and forest plot of systolic blood pressure.
72.6
74.3
86.7
79
78.92
72.6
78.4
5.5
7.8
12.6
13
10.95
8.3283
8.74
10
13
15
12
25
24
25
73
76.6
84.3
82.6
78.84
70.7
84.52
7
8.2
14.3
8.7
8.4
8.8182
10.2
11
12
15
12
25
24
25
17.7%12.9%5.5%6.5%17.4%21.6%18.4%
−0.40 [−5.76, 4.96]−2.30 [−8.59, 3.99]2.40 [−7.25, 12.05]−3.60 [−12.45, 5.25]0.08 [−5.33, 5.49]1.90 [−2.95, 6.75]−6.12 [−11.39, −0.85]
−100 −50 0 50 100
Favours (experimental) Favours (control)
Test for overall effect: Z = 1.02 (P = 0.31)
124 124 100.0%−1.17 [−3.43, 1.09]Total (95% CI)
Experimental Control Mean difference Mean difference
Hodgson & Andersen 2008
Study or subgroupMean SDTotal MeanSD Total
WeightIV, fixed, 95% CI IV, fixed, 95% CI
Hughes et al. 2011Jones et al. 2012Jones et al. 2013Mackereth et al. 2009McVicar et al. 2007Moeini et al. 2011
Heterogeneity: 𝜒2 = 6.16, df = 6 (P = 0.41); I2 = 3%
Figure 3: Meta-analysis and forest plot of diastolic blood pressure.
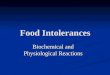
all parts of the study, Mollart [10] presented no data and wastherefore, excluded, and Gunnarsdottir and Jonsdottir [39]and Ruiz-Padial et al. [32] were also excluded as no resultsmeans or standard deviations were available to the researchteam. Mackereth et al. [37] provided results for both armsof their crossover trial; however, since results did not returnto baseline during the washout period, only data from theexperiment which delivered the reflexology treatment firstwas included in the meta-analysis. The forest plots showestimated effect for systolic BP as 1.69 (Figure 2), diastolic BPas 1.17 (Figure 3), and heart rate as 0.97 (Figure 4) all in favourof reflexology.
8. Discussion
The focus of this paper was to review the evidence availablefrom RCTs investigating any quantitative physiological orbiochemical outcome measure as a result of reflexologyas there has been minimal evaluation to date. Seventeenstudies were included for review from a total of 19337 articlesidentified. A notable limitation, however, is the exclusion of
studies not available in English, owing to a lack of availabilityof translation of these papers, along with these not havingsufficient data to perform a meta-analysis; this would haveundoubtedly further informed the review outcomes.
Only three RCTs in this review represented a significantchange between the reflexology intervention and the controlgroup [3, 34, 38]. These studies showed few similarities;however, Hodgson and Andersen [38] and Moeini et al. [34]employed a control measure that involved no touch, whichmay have reduced the incidence of the placebo effect, orpatient therapist interaction in the control group that couldotherwise have reduced the difference between groups. Joneset al. [3] investigated a wide range of cardiac parameters inhealthy volunteerswith onlyCI showing a significant betweengroups difference. However, using the same methodology inheart failure patients resulted in no changes.Thismay suggestthat the positive effects achieved in healthy individuals in onetreatment may require multiple treatments in participantswith health conditions or that the treatment may not betransferable between the different populations. InterestinglyGunnarsdottir and Jonsdottir [39] used a similar participant

12 Evidence-Based Complementary and Alternative Medicine
−100 −50 0 50 100
Favours (experimental) Favours (control)
124 124 100.0%Total (95% CI)
77.9
74.9
66
67.8
72.64
63
68.12
5.5
10.9
7.9
20.5
8.98
5.39
8.42
10
13
15
12
25
24
25
78.7
74
67.3
68.1
71.8
63.9
71.6
6
13.4
10.1
21.8
6.47
7.35
7.86
11
12
15
12
25
24
25
16.1%4.2%9.2%1.4%20.7%29.3%19.1%
−0.80 [−5.72, 4.12]0.90 [−8.72, 10.52]−1.30 [−7.79, 5.19]−0.30 [−17.23, 16.63]
−0.90 [−4.55, 2.75]−3.48 [−8.00, 1.04]
−0.97 [−2.94, 1.00]
Test for overall effect: Z = 0.96 (P = 0.34)
Experimental Control Mean difference Mean difference
Hodgson & Andersen 2008
Study or subgroupMean SDTotal MeanSD Total
WeightIV, fixed, 95% CI IV, fixed, 95% CI
Hughes et al. 2011Jones et al. 2012Jones et al. 2013Mackereth et al. 2009McVicar et al. 2007Moeini et al. 2011
Heterogeneity: 𝜒2 = 2.02, df = 6 (P = 0.92); I2 = 0%
0.84 [−3.50, 5.18]
Figure 4: Meta-analysis and forest plot of heart rate.
group and study design toMoeini et al. [34] but no significantbetween group changes were determined (a significant reduc-tion in systolic BP within the control group was reported).These results show that the effects of reflexology are notrepeatable across all groups.
Within group significant changes were observed for eightoutcomemeasures across a range of ten studies, and a furtherfour studies resulted in no significant changes for eitherthe intervention or control group (Table 4). Importantly,significant within group changes that do not achieve enoughstrength to lead to between group changes may be due toseveral external factors and therefore must be viewed in lightof this. Reasons for within group changes may be due toa regression to the mean, an unknown difference betweengroups at baseline, the normal effect of time or participantsbecoming accustomed to the treatment, therapist, or setting,or a change in health status of the participants. Interestingly,the studies by Mc Vicar et al. [40] and Mackereth et al. [37]both employed a crossover design and both showed a withingroup change for HR and BP which may have influencedbaseline data and results in the reflexology group.
Reflexology is an area which has seen much growthwithin the private sector; however, little work has been car-ried out to determine a possible “mode of action” or howit may be best incorporated into mainstream medical carefrom ameasurable, quantitative perspective informed by highquality evidence.This reviewhighlights thatwhile reflexologyhas seen minimal investigation over the past 20 years, thehypothesised mechanism of action has been focused on themodulation of the ANS. However, the scope of the researchhas been very broad, therefore making it difficult to draw anyfirm conclusions due to the lack of consistency in participantgroups, outcome measures, methodologies, and evaluationtechniques.
The studies considered in this review were undertakenin a range of countries demonstrating that reflexology isconsidered to be worthy of investigation and also a sociallyacceptable form of treatment globally. Nine studies werecarried out in the UK, six of which were performed inNational Health Service (NHS) hospitals. In total, ten trialswere completed in hospitals, four in universities, and three in
nursing homes in the following countries: UK (nine studies),USA (two studies), and one each in the following coun-tries: Australia, Canada, Iceland, Iran, Spain, and Taiwan.Although half of the studies carried out in the UK had a lowROB, neither country nor location had any discernible effecton the ROB.
To date relatively small studies have been carried out, withthe mean number of participants per study being 41; in awell-designed, 3-armed trial this would result in less than 14participants per group. Only five of the named studies carriedout power calculations prior to recruitment. Mackereth et al.[37] determined a total requirement of 46 participants anda total of 53 patients were recruited resulting in statisticallysignificant results in BP and cortisol levels. Hughes et al. [25]included ten participants per group for their feasibility study.The authors went on to complete a post hoc analysis whichindicated that 180 participants would be required for a fullypowered study to achieve 90% power. Mollart [10] estimateda required sample size of 120, which was later reduced to 60,determined by a smaller initial population than first expected.Holt et al. [36] stated that a post hoc analysis found thatat least 600 participants would be necessary to determineany connection between reflexology and ovulation. Joneset al. [30] based their calculation of twelve participants onprevious research using the same protocol and a healthypopulation. This would indicate that, in general, the lack ofsolid statistically significant data is the result of small studysizes (imprecision); therefore larger trials are required toadequately test the effects of reflexology.
Studies involving reflexology have investigated a widerange of outcome parameters using a range of measurementmethods. Treatments have been applied to various groups ofdifferent ethnicity and gender and with different illnesses,using a wide range of experimental designs, measurements,and analyses. This has led to a very low quality evidenceas stated earlier, demonstrating that the RCTs that havebeen carried out in this area and the results should betreated with caution. It has also demonstrated that overall,with respect to reflexology, low quality studies have beencarried out and those where the ROB was low were smalland yielded few statistically significant results. However, it

Evidence-Based Complementary and Alternative Medicine 13
is important to note that high ROB is largely due to thelack of participant and therapist blinding. Importantly ROBanalysis has demonstrated that studies involving reflexology,and indeed any touch therapy, are complex and difficult todesign in order to maintain adequate blinding status forthe participants, therapists, and assessors alike. Ultimately,if statistically significant between groups differences fromlow ROB studies are analysed, this would give rise to onlyone study [3] demonstrating the effectiveness of reflexology,which is a very weak body of evidence for 17 years’ worth ofresearch activity.
In the six studies with a low ROB for participantblinding (Table 2) this was achieved in each case by usinga comparison treatment that was an alternative form ofreflexology. All of the studies reviewed showed a high ROBfor clinician blinding. This highlights the difficulty of usingan adequate control treatment that renders the participantblind to the treatment received and the therapist impartial tothe allocation of treatment. These difficulties in participantblinding persisted even where an alternative foot massagetreatment was used as the control measure [26, 31]. Inter-estingly participants in the intervention group in the studycarried out by Frankel [42] were reported as not havinghad reflexology before. They were given either true or shamreflexology, although no data on blinding index was reported.More recently, Hughes et al. [25] excluded volunteers whohad previous experience of reflexology. However, 66.7% ofthe control group receiving the foot hold control measurereported that they were in the control group. This mayillustrate that the general population is becomingmore awareof reflexology and what it involves, thus allowing them toreliably assert whether they are receiving true reflexology ornot.Therefore, future RCTs involving CAMwill requiremorecomplex designs with greater emphasis on comparing andcontrasting different treatments.
Indeed it is a limitation of any study involving reflexologyto employ a suitable sham treatment that will allow theparticipants to remain blind to the intervention but haveno therapeutic effect, as even gentle pressure on the feetmay give rise to stimulation of a reflex point of interest.Eleven of the RCTs used a control treatment which alsoinvolved touching the feet. The results of those studies,which used sham reflexology, foot hold, cream application,nonprofessional massage, or Swedish massage, showed fewerdifferences between groups. Conversely studies where thecontrol measure involved no touch showed more statisti-cally significant changes between groups and more positivechanges in outcome measures suggesting that touch plays anintegral part in the response to reflexology.
The number of treatments participants received rangedfrom one 4.5-minute treatment to seven separate one-hourtreatments.The duration and frequency of treatments did nothave any effect on the results. Likewise, the type of reflexologyperformed did not appear to have any effect.
A major difficulty for researchers and therapists alike isthe various different types of reflexology used. This currentreview demonstrated this with six different types of reflexol-ogy employed, including the Bayly method, Inghammethod,Father Josef method, a gentle method developed at Anglia
RuskinUniversity, UK, byMcVicar et al. [40], reflexotherapy,and hand reflexology. The most commonly cited protocolin seven studies was the Ingham method or a derivation ofthis; however, only five studies stated any precise reflexologyroutine. As with other therapies, research and experiencehave resulted in generic reflexology evolving into specificforms particular to a school of thought, or the practicesand findings of individual therapists. Also each reflexologymap may have subtle differences leading to difficulties inpinpointing specific reflexes. The points which seem to mostcommonly come into question are the heart, solar plexus, andpituitary gland. This lack of precision and agreement mayresult in a perceived lack of validity of reflexology amongmedical professionals and other health care providers. Hodg-son and Andersen [38] stated that patients received handor foot reflexology; however, no further data on numberswas given which may have offered valuable insight into theeffects of two different types of reflexology within the samepopulation. In accordance with most texts, reflexology ismost usually carried out right foot first; interestingly, intheir study, Moeini et al. [34] treated the left foot first. Theabsence of written details about the routines used duringresearch studies renders them impossible to repeat by otherresearchers keen to investigate the method or critique it inthe light of changing trends in reflexology application. Futurestudies should aim to provide detailedmethods of treatmentscarried out. Furthermore, a lack of consistent terminologyexists within the field of reflexology and CAM modalities ingeneral [38], adding a further level of confusion to therapists,researchers, and medical professionals alike.
A further potential confounder for these studies may liein the number of therapists providing reflexology treatmentsduring trials. During the research for this review one studyboasted 32 therapists taking part; however, the authors didnot cite this as a possible limitation of the study. A singlereflexologist delivering treatments may generally use thesame technique and employ the same treatment type andschedule per client; however, in only seven of the 17 RCTs inthis review was it stated that a single therapist carried out allthe treatments. Small fluctuations in treatment type or eventhemannerisms of the therapist may have an important effecton treatment outcomes.
Only two studies stated whether music was played duringtreatments [3, 40]. Relaxing music is commonly playedduring the delivery of reflexology. Music therapy is an alliedhealth profession. A Cochrane Heart Group review [46]states that listening to music may have a beneficial effect onblood pressure, heart rate, respiratory rate, anxiety, and painin persons with coronary heart disease (CHD). Therefore,as it may have a positive effect on treatment outcomes, itis important to standardise the use of music during trialsinvestigating complementary therapies.
While this review focused on the physiological and bio-chemical outcomes recorded for reflexology interventions,the literature available clearly shows that for all of the articlesevaluated, whether a significant change was identified ornot, reflexology had a positive effect on the health and well-being, quality of life, stress, anxiety, and pain levels of theparticipants involved. Hodgson and Lafferty [31] indicated

14 Evidence-Based Complementary and Alternative Medicine
that cortisol reduction correlated with a reduction in painand stress and Hodgson and Andersen [38] found salivaryamylase to be significantly reduced between the reflexologyand control group, corresponding to a significant reductionin pain. This is in keeping with the ethos that reflexology isa therapy that aims to promote harmony of mind, body, andsoul. Reflexology reduces stress and anxiety levels [3, 32, 36–38, 40] and increases feelings of well-being and quality of life[35].Thepaper byHolt et al. [36] revealed promising evidencefor reflexology. The participants in the control arm receivedsham reflexology and the study had a lowROB for participantblinding. In this study the Hospital Anxiety and Depression(HAD) scale results also showed a significant between groupsreduction in favour of “true” reflexology suggesting someadded value with “true” reflexology. Swedish massage to thefeet has been shown to reduce stress [26] by activation ofthe sACC region of the brain and this may go some way toexplain how reflexology helps to reduce stress levels, giventhat massage is an integral part of a complete reflexologytreatment. No papers were found that investigated any otherbiochemical related to stress or pain.
This review is the first to carry out a meta-analysisof papers investigating BP and HR. These were the mostcommonly analysed outcome measures, likely due to theease and noninvasive nature of recording these parameters.While the forest plots appear to show positive benefits infavour of reflexology, cautious interpretation of the results isneeded. The clinical heterogeneity of the studies, the mix ofhealthy and non-healthy populations, the variation in controlinterventions and the low number of participants (124) wouldresult in a low quality evidence. Furthermore the confidenceintervals for all results cross zero and, therefore, the resultsmust not be viewed as significant at this stage until more databecomes available and further analyses can be carried out.
Overall, the review indicates that only three studiesresulted in significant between group differences [3, 34, 38]suggesting that reflexology can result in a significant reduc-tion in cardiac index (CI) in healthy volunteers, salivary amy-lase in elderly dementia patients, and BP in patients preparedfor coronary artery bypass graft (CABG). These results aresupported by the meta-analyses; however it does not provideany firm conclusions. CI is a measure of how well the heartis functioning to pump blood around the body, suggestinga link between reflexology stimulation and cardiac bloodflow and circulation. These parameters are also functions ofstress and regulated by the ANS. Overall, had the studiesbeen larger a more significant change in quantitative stressoutcome measures may have been demonstrated correlatingwith the overwhelming evidence for a reduction in qualitativeindicators.Therefore, reflexology should be promoted for anymedical condition where stress is contraindicated.
While no firm scientific evidence for the effective andefficacious use or “mode of action” of reflexology has beenestablished, it is nonetheless currently being used in health-care settings around the world including hospices, nursinghomes, andmaternity departments. Inmany countries reflex-ology is associated with the beauty industry or traditionalunorthodox medicine. However, attitudes to CAM therapiesare shifting towards their use as secondarymedical healthcare
and integrating them into mainstream medicine. Ten studiesin this review were carried out in hospitals suggesting a morepositive attitude of health professionals towards the use ofCAM therapies as potential adjuncts to mainstream medicalhealthcare. Thus, this review has implications globally for allhealth professionals seeking innovative and novel methodsfor patient care.
There were no serious adverse effects related to any ofthe treatments for any of the studies. Ruiz-Padial et al. [32]stated that the participants in the reflexology interventionexperienced more discomfort that those receiving a footmassage; however, both groups rated the pleasantness of thetreatments they received as high. Commonly reflexologymaycause some discomfort if the particular body part or organcorresponding to the reflex point being worked is out ofbalance, or in a state of disease [47, 48]. However, care shouldbe taken by the therapist to avoid causing any unnecessarypain or discomfort during treatments as this would have anegative effect on the outcomes of the treatment. Reflexologyis deemed suitable for almost all individuals. It has beenshown to reduce stress in the elderly with life limiting disease[31] and thereforemay be an effective adjunct to palliative carefor patients, their carers, and their families. It also reduces BP,which the National Institute of Health and Care Excellence(NICE) estimated cost the NHS one billion pounds in 2006in drug charges alone [49]. It is considered to be a safe,noninvasive, and inexpensive form of healthcare accessibleby the vast majority of the population including children,the very elderly, terminally ill patients, and pregnant women[48]. Therefore, in the current economic climate investing inresearch into reflexology may prove dividends for health andthe provision of healthcare globally.
Overall reflexology has a positive effect on health, reduc-ing physiological and psychological stress. However, it is asyet unclear how this specialised foot massage exerts its actionand whether physiological stress parameters are reduced dueto a reduction in psychological stress or vice versa.
9. Conclusions
This systematic literature review is the first, to our combinedknowledge, to specifically analyse the existing data availablefrom RCTs investigating the physiological and biochemicalchanges associated with reflexology, and it has demonstratedthat a range of positive effects can be attributed to thetreatment, specifically a reduction in stress parameters. Thiswill inform health care professionals of the evidence base forknown benefits and will enhance evidence based decisionmaking at clinical level. It is important to note that, in allof the studies included in this review, where psychologicalparameters were assessed, a significant improvement inhealth and well-being was determined and this factor alonehad a positive effect on disease outcomes, prognosis, andrehabilitation. None of the studies in this review investigatedany long-term effects through follow-up with participants.Therefore, this is an aspect of CAM study design that mustbe addressed in the future.
It is still unclear from this review precisely how reflex-ology impacts physiological and biochemical parameters.

Evidence-Based Complementary and Alternative Medicine 15
It illustrates the need for further research into the use,efficacy, andmode of action of reflexologywithwell designed,high quality RCTs, if indeed RCTs are a suitable mode ofinvestigation. Also, this review highlights the need for furtherresearch into the measurable physiological and biochemicaleffects of reflexology in order to address the concerns ofhealthcare professionals and thus allowing all patients tobenefit from any positive outcomes afforded by this inex-pensive, noninvasive, and nonpharmacological therapy. It ismore than likely, however, that a number of factors are atwork, both of a physiological and psychological nature andthat reflexology is what it attests to be, a treatment that seeksto enhance and harmonise the mind, body, and spirit.
Conflict of Interests
No conflict of interests has been declared by the authors.
References
[1] “House of lords select committee on science and technologysixth report (2000),” 2012, http://www.publications.parliament.uk/pa/ld199900/ldselect/ldsctech/123/12301.htm.
[2] J. Lee, M. Han, Y. Chung, J. Kim, and J. Choi, “Effects of footreflexology on fatigue, sleep and pain: a systematic review andmeta-analysis,” Journal of Korean Academy of Nursing, vol. 41,no. 6, pp. 821–833, 2011.
[3] J. Jones, P. Thomson, W. Lauder, K. Howie, and S. J. Leslie,“Reflexology has an acute (immediate) haemodynamic effect inhealthy volunteers: a double-blind randomised controlled trial,”Complementary Therapies in Clinical Practice, vol. 18, pp. 204–211, 2012.
[4] S. McDonough, P. Devine, and D. Baxter, “Research update:complementary and alternative medicine: patterns of use inNorthern Ireland,” 2007, http://www.ark.ac.uk/publications/up-dates/update50.pdf.
[5] C. L. Ventola, “Current issues regarding complementary andalternative medicine (CAM) in the United States—part 1: thewidespread use of CAM and the need for better-informedhealth care professionals to provide patient counseling,” Phar-macy andTherapeutics, vol. 35, no. 8, pp. 461–468, 2010.
[6] NIFAB-undersøkelsen 2007, http://www.nifab.no/om alternati-v behandling/tall og fakta/nifab undersoekelsen 2007.
[7] DanishMinistry of Health, Knowledge and Research Center forAlternative Medicine, 2012, http://www.srab.dk/uk/alternative+medicine/reflexology.
[8] British Library, http://www.bl.uk/bipc/aboutus/news/compthe-rapy.html.
[9] H. Hodgson, “Does reflexology impact on cancer patients’ qua-lity of life?” Nursing Standard, vol. 14, no. 31, pp. 33–38, 2000.
[10] L. Mollart, “Single-blind trial addressing the differential effectsof two reflexology techniques versus rest, on ankle and footoedema in late pregnancy,”ComplementaryTherapies inNursingand Midwifery, vol. 9, no. 4, pp. 203–208, 2003.
[11] N. L.N. Stephenson and J. A.Dalton, “Using reflexology for painmanagement. A review,” Journal of Holistic Nursing, vol. 21, no.2, pp. 179–191, 2003.
[12] G.Wyatt, A. Sikorskii, M. A. Rahbar, D. Victorson, andM. You,“Health-related quality-of-life outcomes: a reflexology trial withpatients with advanced stage breast cancer,” Oncology NursingForum, vol. 39, no. 6, pp. 568–577, 2012.
[13] D. Botting, “Review of literature on the effectiveness of reflexol-ogy,” Complementary Therapies in Nursing & Midwifery, vol. 3,no. 5, pp. 123–130, 1997.
[14] E. Ernst and K. Koder, “An overview of reflexology,” EuropeanJournal of General Practice, vol. 3, no. 2, pp. 52–57, 1997.
[15] M.-Y. Wang, P.-S. Tsai, P.-H. Lee, W.-Y. Chang, and C.-M.Yang, “The efficacy of reflexology: systematic review,” Journalof Advanced Nursing, vol. 62, no. 5, pp. 512–520, 2008.
[16] E. Ernst, “Is reflexology an effective intervention? A systematicreview of randomised controlled trials,”Medical Journal of Aus-tralia, vol. 191, no. 5, pp. 263–265, 2009.
[17] E. Ernst, P. Posadzki, andM. S. Lee, “Reflexology: an update of asystematic review of randomised clinical trials,”Maturitas, vol.68, no. 2, pp. 116–120, 2011.
[18] J. Jones, P.Thomson, K. Irvine, and S. J. Leslie, “Is there a specifichaemodynamic effect in reflexology? A systematic review ofrandomised controlled trials,” The Journal of Alternative andComplementary Medicine, vol. 19, no. 4, pp. 319–328, 2013.
[19] J. I. Kim, M. S. Lee, J. W. Kang, D. Y. Choi, and E. Ernst,“Reflexology for the symptomatic treatment of breast cancer: asystematic review,” Integrative CancerTherapies, vol. 9, no. 4, pp.326–330, 2010.
[20] D. Tiran and H. Chummun, “The physiological basis of reflex-ology and its use as a potential diagnostic tool,” ComplementaryTherapies in Clinical Practice, vol. 11, no. 1, pp. 58–64, 2005.
[21] E. Ingham, Stories the Feet Can Tell Thru Reflexology, Storiesthe Feet Have Told Thru Reflexology, Ingham Publishing, StPetersburg, Fla, USA, 1984.
[22] I. Sudmeier, G. Bodner, I. Egger, E. Mur, H. Ulmer, and M.Herold, “Changes of renal blood flow during organ-associatedfoot reflexology measured by colour doppler sonography,” Fors-chende Komplementarmedizin, vol. 6, no. 3, pp. 129–134, 1999.
[23] K. Dalal, D. Elanchezhiyan, R. Das et al., “Noninvasive cha-racterisation of foot reflexology areas by swept source-opticalcoherence tomography in patients with low back pain,” Evi-dence-Based Complementary and Alternative Medicine, vol.2013, Article ID 983769, 11 pages, 2013.
[24] Universal College of Reflexology, 2012, http://www.universalref-lex.com/article.php/20040309175204417.
[25] C. M. Hughes, S. Krirsnakriengkrai, S. Kumar, and S. M.McDonough, “The effect of reflexology on the autonomicnervous system in healthy adults: a feasibility study,”AlternativeTherapies in Health and Medicine, vol. 17, no. 3, pp. 32–37, 2011.
[26] D. Sliz, A. Smith, C. Wiebking, G. Northoff, and S. Hayley,“Neural correlates of a single-session massage treatment,” BrainImaging and Behavior, vol. 6, no. 1, pp. 77–87, 2012.
[27] H. Poole, S. Glenn, and P. Murphy, “A randomised controlledstudy of reflexology for the management of chronic low backpain,” European Journal of Pain, vol. 11, no. 8, pp. 878–887, 2007.
[28] D. Tiran, Reflexology in Pregnancy and Childbirth, ChurchillLivingstone Elsevier, London, UK, 2010.
[29] H. G. Guyatt, A. D. Oxman, G. E. Vist et al., “GRADE: an eme-rging consensus on rating quality of the evidence and strengthof recommendations,” British Medical Journal, vol. 336, no.7650, pp. 924–926, 2008.
[30] J. Jones, P. Thomson, W. Lauder, K. Howie, and S. J. Leslie,“Reflexology has no immediate haemodynamic effect inpatients with chronic heart failure: a double-blind randomisedcontrolled trial,” Complementary Therapies in Clinical Practice,vol. 19, pp. 133–138, 2013.

16 Evidence-Based Complementary and Alternative Medicine
[31] N. A. Hodgson and D. Lafferty, “Reflexology versus Swedishmassage to reduce physiologic stress and pain and improvemood in nursing home residents with cancer: a pilot trial,”Evidence-Based Complementary and Alternative Medicine, vol.2012, Article ID 456897, 5 pages, 2012.
[32] E. Ruiz-Padial, N. Torres-Lopez, J. Luna-Bujaldon, I. Espadas-Villanueva, and G. R. del Paso, “Cardiovascular effects of reflex-ology in healthy individuals: evidence for a specific increase inblood pressure,” Alternative Medicine Studies, vol. 2, no. e4, pp.10–17, 2012.
[33] W. A. Lu, G. Y. Chen, and C. D. Kuo, “Foot reflexology can inc-rease vagal modulation, decrease sympathetic modulation, andlower blood pressure in healthy subjects and patients withcoronary artery disease,” Alternative Therapies in Health andMedicine, vol. 17, no. 4, pp. 8–14, 2011.
[34] M.Moeini, L. S. Kahangi, M. Valiani, and R. Heshmat, “The eff-ect of reflexotherapy on patients’ vital signs before coronaryartery bypass graft surgery,” Iranian Journal of Nursing andMidwifery Research, vol. 16, no. 1, pp. 8–12, 2011.
[35] V. L. Green, A. Alexandropoulou, M. B. Walker et al., “Alter-ations in the Th1/Th2 balance in breast cancer patients usingreflexology and scalp massage,” Experimental and TherapeuticMedicine, vol. 1, no. 1, pp. 97–108, 2010.
[36] J. Holt, J. Lord, U. Acharya et al., “The effectiveness of footreflexology in inducing ovulation: a sham-controlled random-ized trial,” Fertility and Sterility, vol. 91, no. 6, pp. 2514–2519,2009.
[37] P. A. Mackereth, K. Booth, V. F. Hillier, and A. L. Caress, “Refl-exology and progressive muscle relaxation training for peoplewith multiple sclerosis: a crossover trial,” Complementary Ther-apies in Clinical Practice, vol. 15, no. 1, pp. 14–21, 2009.
[38] N. A. Hodgson and S. Andersen, “The clinical efficacy of refl-exology in nursing home residents with dementia,” Journal ofAlternative andComplementaryMedicine, vol. 14, no. 3, pp. 269–275, 2008.
[39] T. J. Gunnarsdottir and H. Jonsdottir, “Does the experimentaldesign capture the effects of complementary therapy? A studyusing reflexology for patients undergoing coronary artery byp-ass graft surgery,” Journal of Clinical Nursing, vol. 16, no. 4, pp.777–785, 2007.
[40] A. J. Mc Vicar, C. R. Greenwood, F. Fewell, V. D’arcy, S. Chan-drasekharan, and L. C. Alldridge, “Evaluation of anxiety, sali-vary cortisol and melatonin secretion following reflexologytreatment: a pilot study in healthy individuals,” ComplementaryTherapies in Clinical Practice, vol. 13, no. 3, pp. 137–145, 2007.
[41] I. S. A. Wilkinson, S. Prigmore, and C. F. Rayner, “A rando-mised-controlled trail examining the effects of reflexology ofpatients with chronic obstructive pulmonary disease (COPD),”Complementary Therapies in Clinical Practice, vol. 12, no. 2, pp.141–147, 2006.
[42] B. S. M. Frankel, “The effect of reflexology on baroreceptorreflex sensitivity, blood pressure and sinus arrhythmia,” Com-plementary Therapies in Medicine, vol. 5, no. 2, pp. 80–84, 1997.
[43] D. Moher, A. Liberati, J. Tetzlaff, and D. G. Altman, “Preferredreporting for systematic reviews and meta-analyses,” PLoSMedicine, vol. 6, no. 7, Article ID e10000097, 2009.
[44] J. P. T. Higgins and S. Green, Eds., Cochrane Handbook forSystematic Reviews of Interventions Version 5.1.0, The CochraneCollaboration, Oxford, UK, 2011, https://www.cochrane-handbook.org.
[45] T. Brygge, J. H. Heinig, P. Collins et al., “Reflexology and bron-chial asthma,” Respiratory Medicine, vol. 95, no. 3, pp. 173–179,2001.
[46] J. Bradt and C. Dileo, “Music for stress and anxiety reduction incoronary heart disease patients,” Cochrane Database of System-atic Reviews, no. 2, Article ID CD006577, 2009.
[47] H.Marquardt,Reflex ZoneTherapy of the Feet: A ComprehensiveGuide forHealth Professionals, HealingArts Press, Rochester, Vt,USA, 2007.
[48] D. Tiran and P. A. Mackereth, Clinical Reflexology: A Guide forIntegrated Practice, Churchill Livingstone Elsevier, Edinburgh,Scotland, 2011.
[49] National Institute for Health and Care Excellence (NICE),“Clinical guidelines hypertension: clinical management of pri-mary hypertension in adults,” 2013, http://publications.nice.org.uk/hypertension-cg127

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com