Embed Size (px)
Citation preview
Hindawi Publishing CorporationRehabilitation Research and PracticeVolume 2013, Article ID 305249, 10 pageshttp://dx.doi.org/10.1155/2013/305249
Review ArticlePhysiotherapy Treatment in Patients with Hemophilia andChronic Ankle Arthropathy: A Systematic Review
Rubén Cuesta-Barriuso,1 Antonia Gómez-Conesa,1 and José Antonio López-Pina2
1 Research Group in Physiotherapy and Health Promotion, Regional Campus of International Excellence “Campus Mare Nostrum”,University of Murcia, 30100 Murcia, Spain
2Department of Basic Psychology and Methodology, Faculty of Medicine, Espinardo Campus, University of Murcia,30100 Murcia, Spain
Correspondence should be addressed to Ruben Cuesta-Barriuso; [email protected]
Received 27 January 2013; Revised 10 June 2013; Accepted 2 July 2013
Academic Editor: Felipe Querol
Copyright © 2013 Ruben Cuesta-Barriuso et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Haemophilic arthropathy of the ankle causes pain and deterioration in gait, causing disability. Although some physiotherapymodalities are effective in the management of acute bleeding, the results are unknown in chronic arthropathy. Our objective wasto determine the most effective physiotherapy procedures for treating the haemophilic arthropathy of the ankle and to assess themethodological quality of the studies. A systematic review was carried out in the Cochrane Database, PubMed,MEDLINE, ISIWebof Knowledge, PEDro, TESEO, and specialized journals (Haemophilia and Haematologica). It included articles with at least onegroup undergoing any kind of physiotherapy treatment and with pretest and posttest evaluation, published before April 2013. Ananalysis of variables was performed and assessed the methodological quality of studies. Five studies met the criteria for inclusion.Hydrotherapy treatments, strength training and balance strength, balance training, and sports therapy, have improved range ofmovement, pain, balance, and subjective physical performance. The proposed methodological analysis was not possible due to thelow quality of the studies. Although the results are positive, they lack rigorous evidence on the effects of treatments. Studies areneeded to establish the efficacy of the various forms of physiotherapy in the haemophilic arthropathy of the ankle.
1. Introduction
Hemophilia is a blood-clotting disorder caused by a defi-ciency in factor VIII (FVIII) or factor IX (FIX), whichmanifests itself through bleeding in the muscles and joints[1].There are three categories, depending on the percentage ofthe blood-clotting factor: severe hemophilia (<1% FVIII/IX),characterised by spontaneous bleeding;moderate hemophilia(1–5% FVIII/FIX), with bleeding from slight injuries; andmild hemophilia (>5–40% FVIII/FIX) with bleeding duringsurgical procedures or from severe injuries [2, 3].
Eighty percent of the episodes in hemophiliac patientsinvolve bleeding in the joints, or haemarthrosis [4, 5], withthe ankle being the third most frequently affected joint [6].The symptoms of intra-articular ankle bleeding are severepain, limited range of motion, inflammation, and synovialinvolvement.Without proper treatment, capsular and tendoncontractures can develop in the joints [7].
Although experiments on animals cannot be directlyrelated to the humans, Hooiveld et al. [8] observed in a caninemodel that weight-bearing joints, as opposed to non-weight-bearing joints with haemarthrosis, suffered progressive anddegenerative damage after a bleeding episode. Also analysingthe effects of haemarthrosis, Hakobyan et al. [9] tested in amurine model the effect of the ferric component of blood, invitro, on the development of chronic synovitis.
Excess blood inside the joint results in inflammation ofthe synovial membrane, which eventually leads to chronichaemophilic synovitis and a vicious cycle of haemarthrosis-synovitis-haemarthrosis [15].
When synovitis becomes chronic, the condition is wors-ened by the recurrent haemarthrosis episodes, acceleratingthe degenerative process known as haemophilic arthropathy,which leads to alterations of the joints, pain, muscular atro-phy, and functional impairment [16]. Chronic arthropathy isa major cause of morbidity in patients with haemophilia [17].

2 Rehabilitation Research and Practice
Due to the progression of haemophilic arthropathy andthe resulting deterioration of the joint, deformities such asthe restriction of motion, valgus hindfoot, alteration of thesubtalar and tibiofibular-astragalar joints, or plano-valgusfoot [18] occur. Likewise, the chronic pain associated withhaemophilic arthropathy is a good predictor of disability inpatients with severe haemophilia [19].
Current pharmacological treatments prophylactic withFVIII or FIX significantly reduce the frequency of haemar-throsis in hemophilia. This decrease in the incidence of jointand muscle bleeding, spontaneous and posttraumatic, hasdelayed the incidence of haemophilic arthropathy [20, 21].When arthropathy is already instituted, this treatment canonly slow the joint deterioration but not prevent it [22, 23].
On the other hand, the 80% of hemophilia patients haveno access to pharmacological therapy [24], and part of theremaining 20% only receive treatment after a bleeding epi-sode (on demand treatment). In both cases, patients developphysical consequences before reaching adulthood, thatrequire physiotherapy treatment to improve and maintainjoint function [25].
Physiotherapy through theRICEmethod (Rest, Ice, Com-pression, and Elevation) has been described for the improve-ment of acute joint injuries [26], as well as in themanagementof hemarthrosis in patients with hemophilia [27].
Treatment of the ankle with physical therapy is compli-cated because it involves a small joint surface that bears sig-nificant ranges of body weight and the joint limitation altersbiomechanical movement during walking. A treatment com-bining strength and proprioception exercises improved func-tionality in a group of 31 patients with haemophilic arthropa-thy on knee and ankle [10].
Likewise, for the ankle joint, the guide of the World Fed-eration of Haemophilia recommends exercises to range ofmovement, strength, and balance [28], while these recom-mendations are not based on any clinical study.
Even though it is a joint with a high prevalence of degen-erative lesions [29], it is not known how significant or effi-cacious physical therapy is in managing arthropathy of theankle.
The main objective of this work is to learn from theexisting literature about the effectiveness of physical therapyprocedures in treating chronic arthropathy of the ankle inpatients with hemophilia. It will also analyse themethodolog-ical quality of the studies and propose new lines of research.
2. Methods
2.1. Data Sources and Searches. The literature search was per-formed according to the search strategy described by Dick-ersin et al. [30].
Combined processes were developed for the study search,establishing the following steps: (I) the following databases ofspecialised literature were consulted: Cochrane, MEDLINE,PubMed, PEDro, TESEO and ISI Web of Knowledge; (II) thesearch ended in May of 2013; (III) the medical subjects head-ing included “hemophilia” AND “ankle” AND “arthropa-thy” AND “rehabilitation” OR “physiotherapy” OR “physical
therapy” OR “TENS” OR “transcutaneous” OR “hydrother-apy” OR “kinesiotherapy” OR “manual therapy” in the arti-cle, and specialised electronic magazines were consulted:HaemophiliaandHaematologica.
We also reviewed bibliographies of relevant papers,conference messages, dissertations, and consultations withexperts. Two authors reviewed the abstracts and full texts ofthe publications found in the databases and journals, and ifin doubt, the eligibility of any of the articles was determinedby consensus.
2.2. Study Selection. The studies selected met the followingcriteria: (I) they use physical therapy treatments and (II)clinical trials; (III) they include at least one treatment groupwith pretest and posttest evaluations; (IV) the size of thesample in the posttest is a minimum of five individuals pergroup; (V) years considered: without restrictions in the yearof publication; the study had to have been published prior toApril 2013; (VI) the studies included are restricted to thosein Spanish, French, English, Italian, and Portuguese, (VII)studies without limit of age, and (VIII) articles publishedin scientific journals or in process of publication; (IX) casestudies are excluded, (X) as are those in which the individ-uals were not diagnosed with hemophilia A or B, or (XI)those in which the physical therapy treatment used was notexplained.
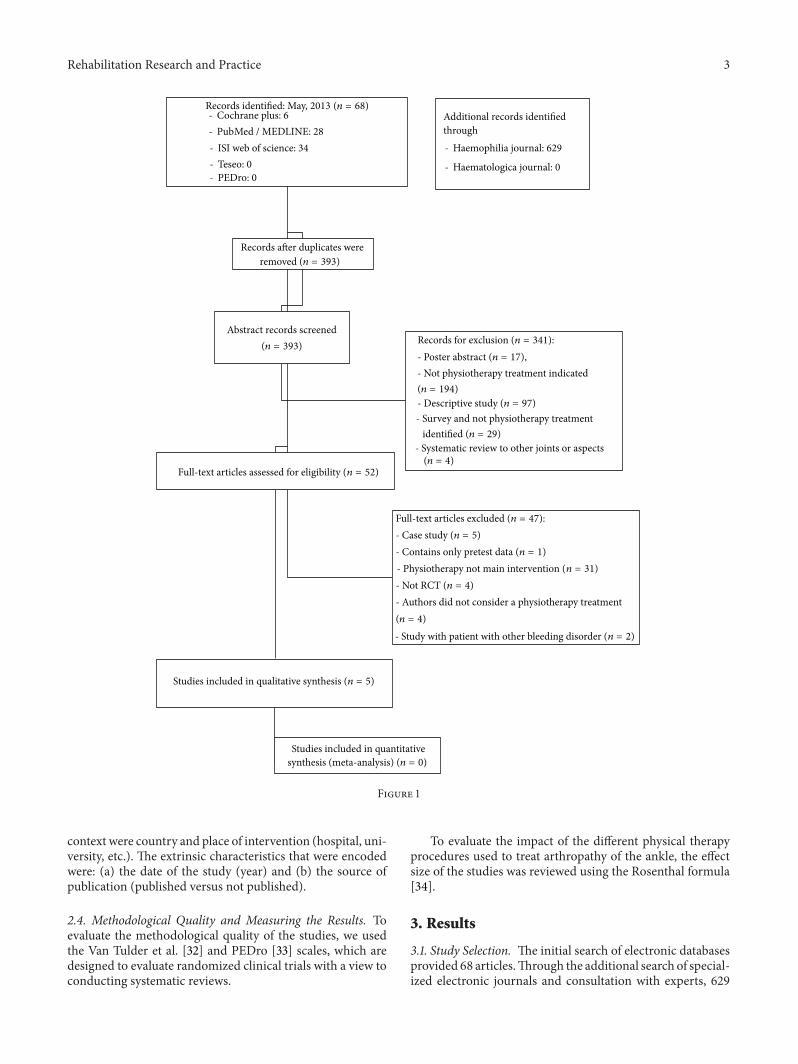
After the search, in which more than 600 references wereconsulted, a total of five articles [10–14] fulfilled the inclusioncriteria. Figure 1 shows the results of the search and selectionprocess.
2.3. Encoding of the Variables. It was performed according tothe procedure for coding the studies of the Meta-AnalysisUnit of Murcia University (http://www.um.es/metaanalysis/presentation.php/).
The characteristics of the five selected studies wereencoded. The moderating variables were grouped in threecategories in accordance with the Lipsey et al. [31] classifi-cation system: substantive variables (treatment, context, andindividual involved), methodological variables, and extrinsicvariables.
The encoded characteristics of the treatment were thefollowing: the type of physical therapy treatment (muscularstrength, proprioception training, hydrotherapy, and sportstherapy); the duration of treatment (in weeks); the intensityof the treatment (number of hours for session); the extentof the treatment (total number of hours per patient); thenumber of sessions; inclusion of the follow-up programme(in weeks); the uniformity of the treatments (patients fromthe same group receive the same treatment); the mode ofintervention: direct (applied by a physiotherapist), indirect(under the supervision of a physiotherapist), or mixed; andinformed consent.
The encoded characteristics of the individuals were thefollowing: the average age (in years) of the individuals in thesample; the type of hemophilia; the severity of the hemo-philia; and whether or not prophylactic drug treatment withFVIII/FIX was used. The encoded characteristics of the
Rehabilitation Research and Practice 3
- Cochrane plus: 6- PubMed / MEDLINE: 28- ISI web of science: 34- Teseo: 0- PEDro: 0
Abstract records screened
Additional records identified through - Haemophilia journal: 629
- Haematologica journal: 0
removed (n = 393)
(n = 393)
Full-text articles assessed for eligibility (n = 52)
Records for exclusion (n = 341):- Poster abstract (n = 17),- Not physiotherapy treatment indicated(n = 194)- Descriptive study (n = 97)- Survey and not physiotherapy treatment
- Systematic review to other joints or aspects
Studies included in qualitative synthesis (n = 5)
Studies included in quantitativesynthesis (meta-analysis) (n = 0)
Full-text articles excluded (n = 47):- Case study (n = 5)- Contains only pretest data (n = 1)- Physiotherapy not main intervention (n = 31)- Not RCT (n = 4)- Authors did not consider a physiotherapy treatment(n = 4)
(n = 4)
Records identified: May, 2013 (n = 68)
Records after duplicates were
identified (n = 29)
- Study with patient with other bleeding disorder (n = 2)
Figure 1
context were country and place of intervention (hospital, uni-versity, etc.). The extrinsic characteristics that were encodedwere: (a) the date of the study (year) and (b) the source ofpublication (published versus not published).
2.4. Methodological Quality and Measuring the Results. Toevaluate the methodological quality of the studies, we usedthe Van Tulder et al. [32] and PEDro [33] scales, which aredesigned to evaluate randomized clinical trials with a view toconducting systematic reviews.
To evaluate the impact of the different physical therapyprocedures used to treat arthropathy of the ankle, the effectsize of the studies was reviewed using the Rosenthal formula[34].
3. Results
3.1. Study Selection. The initial search of electronic databasesprovided 68 articles.Through the additional search of special-ized electronic journals and consultation with experts, 629

4 Rehabilitation Research and Practice
articles were located. We reviewed 393 abstracts of which 52went to full-text review. Finally, 5 studies met all inclusioncriteria.
3.2. Participants. Finally, they were 94 patients with hemo-philia and 47 people without congenital coagulopathies. Allpatients were males, diagnosed with hemophilia A or B, withdifferent phenotypes of gravity, based on the percentage ofFVIII/FIX in blood.
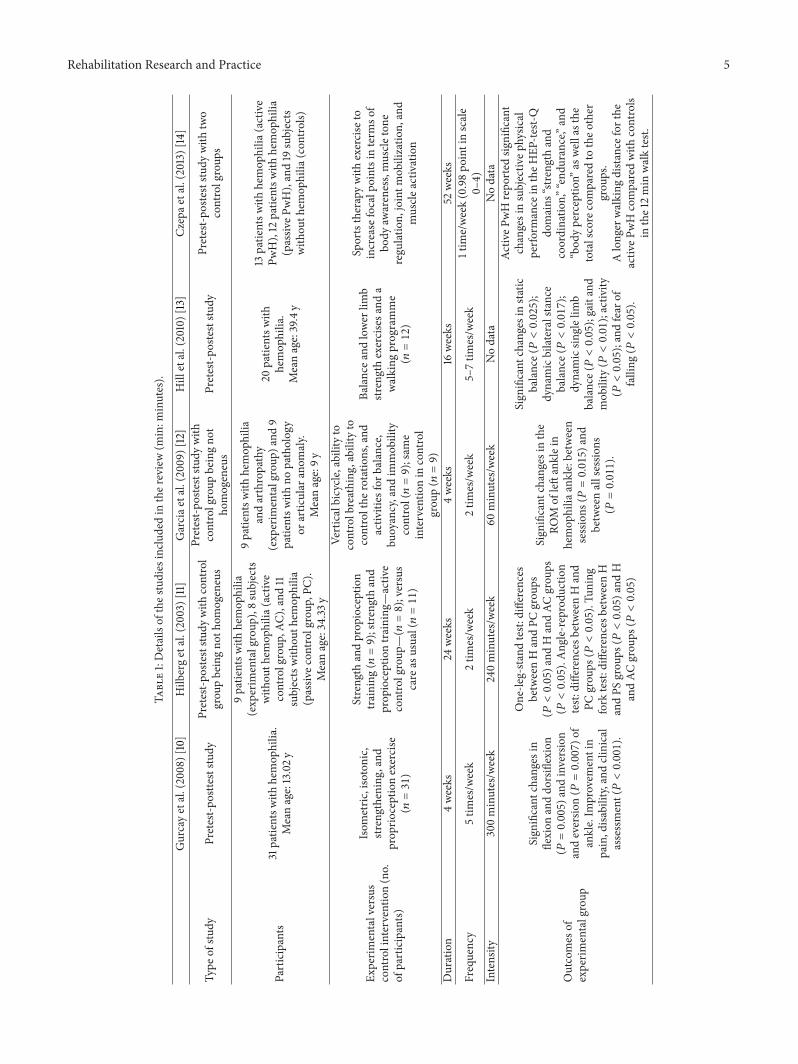
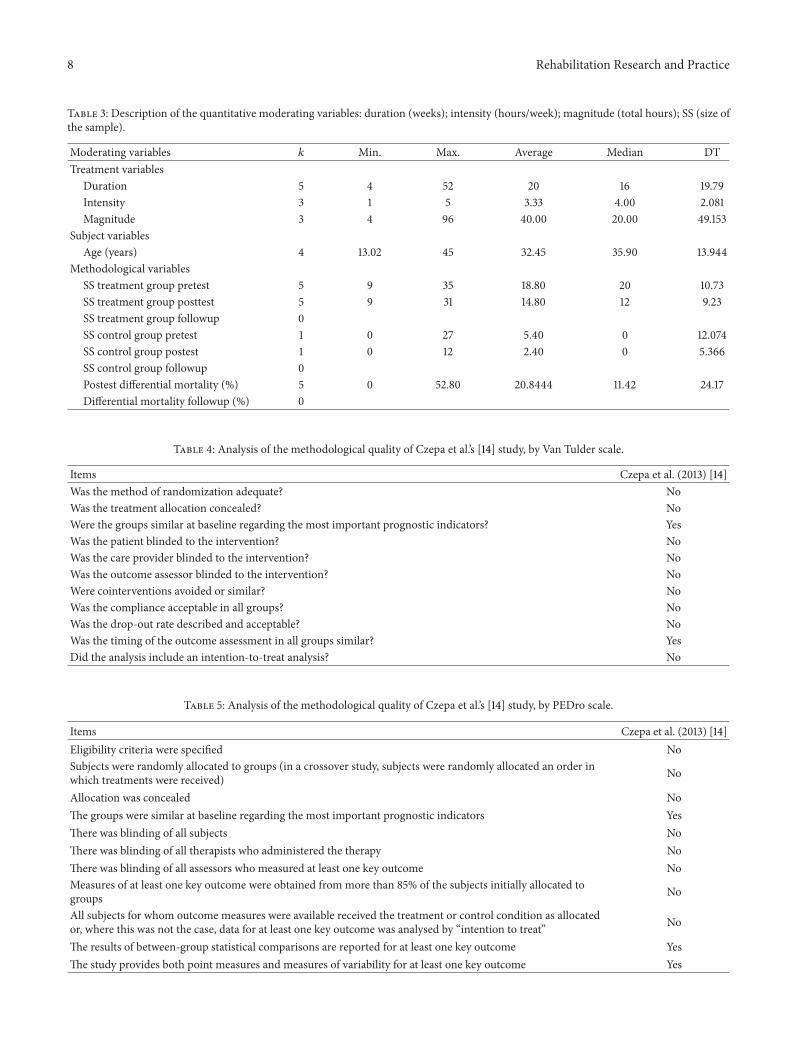
3.3. Characteristics of the Studies. Weanalysed the five studiesthat met the inclusion criteria. Table 1 contains the mostrelevant results of the studies analysed, and the characteristicsof the potentially moderating variables are presented inTables 2 and 3.
Regarding the treatment variables, we found differenttypes of intervention, distinguishing between a combinationof muscle strength training and proprioception [10, 11, 13],hydrotherapy [12] and sports therapy [14].
With respect to the quantitative treatment variables, theintervention lasted an average of 20 weeks; each individualreceived an average of 10 hours of treatment per week, andeach individual received treatment totalling an average of 120hours.
Regarding the variables for the individuals, just three ofthe studies [10, 13, 14] indicated the type and severity of thehemophilia in the sample. The Hill et al. [13] study examined19 patients with hemophilia A and one with hemophilia B,of whom 14 had the severe, four had the moderate, and onehad the mild phenotype. In the Gurcay et al. [10] sample, onthe other hand, there were 25 patients with hemophilia A andsix with hemophilia B, of whom 21 had the moderate, sixhad the severe, and four had the mild phenotype. Czepaet al. [14] examined 24 patients with hemophilia A and onewith hemophilia B, of whom 21 had the severe and 3 hadthe moderate phenotype. The prophylactic treatment wascovered by the authors in two articles [10, 13]. In the Czepaet al. [14] study, patients were on pharmacological regimenprovided for their haematologist (12/25).
Regarding the extrinsic characteristics, all of the studiesare from journal articles. One study was conducted in 2003[11] and the other four in 2008, 2009, 2010, and 2013 [10, 12–14].
3.4.Methodological Quality andMeasuring the Results. Of thefive studies, two had no control group [10, 13], and in theother two, the control group consisted of individuals whowere either healthy [11] or with no ankle pathology [12].Thesestudies have no control group with the same characteristicsthat the treatment group (patients with hemophilia and anklearthropathy), and none of the scales anticipated in the designof this review could be applied (Van Tulder and PEDro).
In the study of Czepa et al. [14], the control group (passivePWH) had the same characteristics that the active group.Tables 4 and 5 show assessment of these articles with VanTulder and PEDro scales.
The size effect could not be calculated as anticipatedbecause of the lack of a control group or because of the latter’scharacteristics.
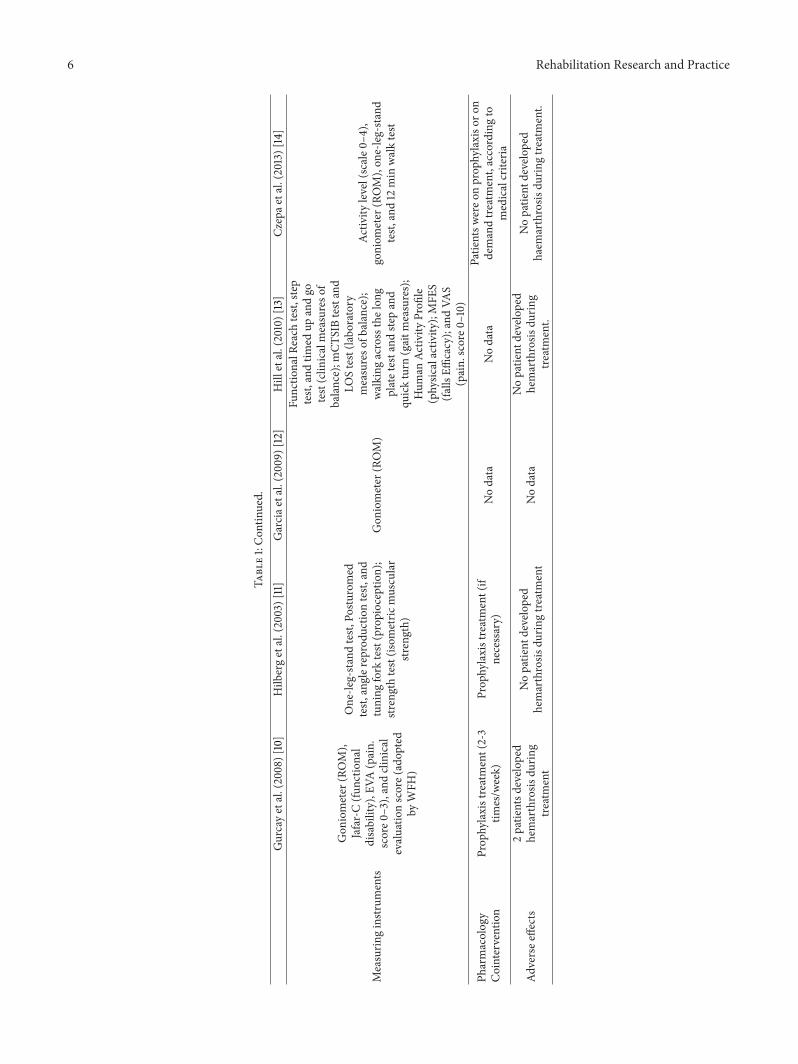
3.5. Measuring Instruments. The studies selected for thisreview used a wide variety of clinimetric measures to detect ameasurable change after the physiotherapy treatment. Gurcayet al. [10] evaluated ROM (with a universal goniometer); per-ception of pain (scale of joint pain, score 0–3): functionalincapacity (Juvenile Arthritis Functional Assessment Reportfor Children; JAFAR-C questionnaire); and the clinical evalu-ation (evaluation scale adopted by the Orthopaedic AdvisoryCommittee of the World Federation of Haemophilia).
The Hilberg et al. [11] study evaluated proprioception(test: One-Leg Stand, angle reproduction, tuning fork, andPosturomed) and isometric muscular strength (test: kneeextensor, and leg press). Garcia et al. [12] evaluated ROM(with a universal goniometer). Finally, the Hill et al. [13]study evaluated proprioception (Functional Reach test, steptest, timed up and go, modified Clinical Test of SensoryInteraction on Balance-mCTSIB test and Limits of stability-LOS test); walking (test: Walking across the long plate andStep and quick turn); physical activity (Human ActivityProfile questionnaire); fear of falling (modified Falls EfficacyScale—MFES questionnaire); and the perception of pain(Visual Analogue Scale, or VAS). Czepa et al. [14] evaluatedactivity level (scale from 0-not active to 4-active more thanthree times/week); ROM of knee, ankle, and elbow (with auniversal goniometer); One-Leg Stand test; and 12min walktest.
Pretest and posttest evaluations were performed in thefive studies [10–14], and Garcia et al. [12] measured ROMbefore and after each session.
3.6. Adverse Effects. Gurcay et al. [10] showed that duringtreatment with strength and proprioception, there were twopatients with hemophilia who developed joint bleeds, whiletreatments ofHilberg et al. [11], Hill et al. [13], andCzepa et al.[14] did not cause haemarthrosis during the study period, andGarcia et al. [12] provided no data on this respect.
4. Discussion
This review explored the changes in objective measuresof physical therapy treatments in patients with hemophiliaand chronic arthropathy of the ankle. The five studies wereselected because they provided pretest/posttest data in atreatment group. The studies reviewed examined the impactof different physical therapy treatments on the clinical mani-festations of chronic arthropathy of the ankle (reduced ROM,loss of strength, pain, and alteration of proprioception) inpatients with hemophilia. Three studies were conducted in ahospital setting [10–12] and two in hospital and in the home[13, 14].
The studies are very heterogeneous with respect to theduration, intensity, and extent of the treatments. The treat-ments lasted for four weeks [10, 12], sixteen weeks [13], twen-ty-four weeks [11], and fifty-two weeks [14]; and the numberof hours per week for each patient was one hour [12], fourhours [11], or five hours [10].
The treatments administered were strength training and,proprioception [10, 11, 13], hydrotherapy [12], and sports ther-apy [14].
Rehabilitation Research and Practice 5
Table1:Detailsof
thes
tudies
inclu
dedin
ther
eview(m
in:m
inutes).
Gurcayetal.(2008)[10]
Hilb
ergetal.(2003)[11]
Garciae
tal.(200
9)[12]
Hill
etal.(2010)[13]
Czepae
tal.(2013)
[14]
Type
ofstu
dyPretest-p
ostte
ststu
dyPretest-p
osteststu
dywith
control
grou
pbeingno
thom
ogeneus
Pretest-p
osteststu
dywith
controlgroup
beingno
tho
mogeneus
Pretest-p
osteststu
dyPretest-p
osteststu
dywith
two
controlgroup
s
Participants
31patie
ntsw
ithhemop
hilia.
Meanage:13.02y
9patie
ntsw
ithhemop
hilia
(exp
erim
entalgroup
),8subjects
with
outh
emop
hilia
(active
controlgroup
,AC)
,and
11subjectswith
outh
emop
hilia
(passiv
econ
trolgroup
,PC)
.Meanage:34.33
y
9patie
ntsw
ithhemop
hilia
andarthropathy
(exp
erim
entalgroup
)and
9patie
ntsw
ithno
patholog
yor
artic
ular
anom
aly.
Meanage:9y
20patie
ntsw
ithhemop
hilia.
Meanage:39.4y
13patie
ntsw
ithhemop
hilia
(active
PwH),12
patie
ntsw
ithhemop
hilia
(passiv
ePwH),and19
subjects
with
outh
emop
hilia
(con
trols)
Experim
entalversus
controlintervention(no.
ofparticipants)
Isom
etric
,isotonic,
streng
thening,and
prop
rioceptionexercise
(𝑛=31)
Streng
thandprop
ioception
training
(𝑛=9);str
engthand
prop
ioceptiontraining
—activ
econtrolgroup
—(𝑛=8);versus
care
asusual(𝑛=11)
Verticalbicycle
,abilityto
controlbreathing
,abilityto
controlthe
rotatio
ns,and
activ
ities
forb
alance,
buoyancy,and
immob
ility
control(𝑛=9);same
interventio
nin
control
grou
p(𝑛=9)
Balancea
ndlower
limb
streng
thexercisesa
nda
walking
programme
(𝑛=12)
Sportstherapywith
exercise
toincrease
focalp
ointsinterm
sof
body
awareness,muscle
tone
regu
latio
n,jointm
obilizatio
n,and
muscle
activ
ation
Duration
4weeks
24weeks
4weeks
16weeks
52weeks
Frequency
5tim
es/w
eek
2tim
es/w
eek
2tim
es/w
eek
5–7tim
es/w
eek
1tim
e/week(0.98po
intinscale
0–4)
Intensity
300minutes/w
eek
240minutes/w
eek
60minutes/w
eek
Nodata
Nodata
Outcomes
ofexperim
entalgroup
Sign
ificant
changesin
flexion
anddo
rsiflexion
(𝑃=0.005)a
ndinversion
andeversio
n(𝑃=0.007)o
fankle.Im
provem
entin
pain,disa
bility,andclinical
assessment(𝑃<0.001).
One-le
g-standtest:
differences
betweenHandPC
grou
ps(𝑃<0.05)a
ndHandAC
grou
ps(𝑃<0.05).Ang
le-reprodu
ction
test:
differences
betweenHand
PCgrou
ps(𝑃<0.05).Tu
ning
fork
test:
differences
betweenH
andPS
grou
ps(𝑃<0.05)a
ndH
andAC
grou
ps(𝑃<0.05)
Sign
ificant
changesinthe
ROM
ofleftanklein
hemop
hilia
ankle:between
sessions
(𝑃=0.015)a
ndbetweenallsessio
ns(𝑃=0.011).
Sign
ificant
changesinstatic
balance(𝑃<0.025);
dynamicbilateralsta
nce
balance(𝑃<0.017);
dynamicsin
glelim
bbalance(𝑃<0.05);gaitand
mob
ility(𝑃<0.01);activ
ity(𝑃<0.05);andfear
offalling
(𝑃<0.05).
Activ
ePwHrepo
rted
significant
changesinsubjectiv
ephysic
alperfo
rmance
intheH
EP-te
st-Q
domains
“stre
ngth
and
coordinatio
n,”“end
urance,”and
“bod
yperceptio
n”as
wellasthe
totalscore
comparedto
theo
ther
grou
ps.
Alonger
walking
dista
ncefor
the
activ
ePwHcomparedwith
controls
inthe12min
walktest.
6 Rehabilitation Research and Practice
Table1:Con
tinued.
Gurcayetal.(2008)[10]
Hilb
ergetal.(2003)[11]
Garciae
tal.(200
9)[12]
Hill
etal.(2010)[13]
Czepae
tal.(2013)
[14]
Measurin
ginstr
uments
Gon
iometer
(ROM),
Jafar-C(fu
nctio
nal
disability),E
VA(pain.
score0
–3),andclinical
evaluatio
nscore(adop
ted
byWFH
)
One-le
g-standtest,
Postu
romed
test,
angler
eprodu
ctiontest,
and
tuning
fork
test(propioceptio
n);
strengthtest(isom
etric
muscular
strength)
Gon
iometer
(ROM)
Functio
nalR
each
test,
step
test,
andtim
edup
andgo
test(clin
icalmeasureso
fbalance);m
CTSIBtestand
LOStest(la
boratory
measureso
fbalance);
walking
acrossthelon
gplatetestand
stepand
quickturn
(gaitm
easures);
Hum
anAc
tivity
Profi
le(physic
alactiv
ity);MFE
S(fa
llsEffi
cacy);andVA
S(pain.
score0
–10)
Activ
itylevel(scale0
–4),
goniom
eter
(ROM),on
e-leg-stand
test,
and12
min
walktest
Pharmacolog
yCointervention
Prop
hylaxistreatment(2-3
times/w
eek)
Prop
hylaxistreatment(if
necessary)
Nodata
Nodata
Patie
ntsw
ereo
nprop
hylaxiso
ron
demandtre
atment,accordingto
medicalcriteria
Adversee
ffects
2patie
ntsd
evelo
ped
hemarthrosis
durin
gtre
atment
Nopatie
ntdeveloped
hemarthrosis
durin
gtre
atment
Nodata
Nopatie
ntdeveloped
hemarthrosis
durin
gtre
atment.
Nopatie
ntdeveloped
haem
arthrosis
durin
gtre
atment.

Rehabilitation Research and Practice 7
Table 2: Description of the qualitative moderating variables.
Variables 𝑘 Frequency %Treatment variables
Type of treatment 5ST + PT 3 60
H 1 20SPORT 1 20
Mode of application 5Direct 2 40Indirect 2 40Mixed 1 20
Informed consent 5 Yes 3 50No 2 50
Context variables
Country 5
Germany 2 25Brazil 1 25
Australia 1 25Turkey 1 25
Place 5 Hospital 3 75Domiciliary 2 25
Methodological variables
Pretest 5 Yes 5 100No 0 0
Assignment 5 Random 0 0Not random 5 100
Control group 5 Yes 1 0No 4 100
Date 5 2003 1 252005–2013 4 75
Published 5 Yes 5 100No 0 0
Source 5 Journal article 5 100𝑘: number of studies; ST: strength training; PT: proprioception training; H:hydrotherapy; SPORT: sports therapy.
Regarding the occurrence of joint bleeding as a resultof physical therapy treatments, in three trials there was nohaemarthrosis of the ankle [11, 13, 14] which indicates thesafety of the strengthening treatments and sports therapywith exercises adapted to the patients’ health status in pre-venting recurrent bleeding.
These results agree with those of Koch et al. [35] thatafter treatment with strength training in young people withhemophilia from 12 to 14 years, improvement was noted inquadriceps muscle strength with a decrease in the frequencyof haemarthrosis in the knee joint and in the results ofPelletier et al. [36] in a patient with hemophilic arthropathy ofthe knee treated with isometric exercises. Other authors havealso noted that physical activity can improve muscle strengthand flexibility and reduce the number of bleeding, synovitisand joint destruction in patients with hemophilia [37].
Development of arthropathy affects the proprioceptionof patients with haemophilia [38]. After the treatmentsdescribed in the studies, proprioception improves as a resultof strength and proprioception training programmes for thelower limbs [11, 13].
In the ROM evaluation, described by Harris and Bog-gio [39] as a measure of joint deterioration in patientswith hemophilia, significant improvement was found in the
evaluation of the ankle after treatment with strength andproprioception exercises [10] and hydrotherapy [12].
Perception of pain is one of the main causes of incapac-ity in patients with hemophilia [24]; there was significantimprovement after strength and proprioception treatment[10, 13].
The treatments of the Gurcay et al. [10] and Hill et al. [13]studies seem to havemore effectiveness, with improvement ina larger number of clinimetricmeasures, although theGurcayet al. [10] study achieves good results in less time: four weeksas opposed to the 16 required by Hill et al. [13]. However, dueto the lack of follow-up periods in the studies of this review, itwas not possible to learn whether the effect of the treatmentsholds up over time.
In the study of Czepa et al. [14], 47.9% of patients dropoutthe study due to irregular training frequencies, operationsduring intervention period, private reasons, or patient whoentered later into the study. In the study byHill et al. [13], 40%of patients discontinued due to lack of time, other diseasesthat affect their ability to participate, lack of motivation orinterest in the program, or not believing in the benefits oftreatment.The dropout rate is similar to that described in thestudy by Mulvany et al. [40] who developed physiotherapytreatments for improving muscle strength and flexibility, andcardiovascular function in 33 patients with congenital coag-ulopathies (hemophilia and von Willebrand disease), andhad a 39% dropout due to problems with transportation andschedules and the disease, although no patient reported anyadverse effects as a result of treatment. By contrast, there wasa lower experimental mortality rate (17.85%) in the study byHilberg et al. [11], and no patient stopped treatment in theother two studies [10, 12].
4.1. Methodological Quality and Measuring the Results. Withrespect to methodological quality and measuring the results,the analysis of the methodological quality using the VanTulder and PEDro scales and of effect size, is precluded bythe fact there is no control group in the studies with thesame characteristics as the experimental group (hemophiliaand ankle arthropathy). Only it was possible to assess themethodological quality of the article by Czepa et al. [14] with2 and 3 points in Van Tulder and PEDro scales, respectively.
Among the articles on physiotherapy treatment of hae-mophilic arthropathy of the ankle excluded from this reviewbecause they did not meet the selection criteria, there are twounique cases [22, 41] one that did not involve posttreatmentevaluation [42] and two articles that evaluated the isolatedplacement of a plantar orthoses [43] and performance ofsports without supervision of physiotherapist [39]. Althoughacupuncture has been used as a treatment of physiotherapy,the article of Lambing et al. [44] has not been included in thisreview because the authors do not apply it as a physiotherapytreatment. Two articles [40, 45], despite their good method-ological quality, include patients with other coagulationdeficits (von Willebrand disease-vWD).
Similarly, despite the good methodological quality of thestudy of Von Mackensen et al’s [46], this article was notincluded in this review because the authors did not assess anyphysical variable in ankles with hemophilic arthropathy.
8 Rehabilitation Research and Practice
Table 3: Description of the quantitative moderating variables: duration (weeks); intensity (hours/week); magnitude (total hours); SS (size ofthe sample).
Moderating variables 𝑘 Min. Max. Average Median DTTreatment variables
Duration 5 4 52 20 16 19.79Intensity 3 1 5 3.33 4.00 2.081Magnitude 3 4 96 40.00 20.00 49.153
Subject variablesAge (years) 4 13.02 45 32.45 35.90 13.944
Methodological variablesSS treatment group pretest 5 9 35 18.80 20 10.73SS treatment group posttest 5 9 31 14.80 12 9.23SS treatment group followup 0SS control group pretest 1 0 27 5.40 0 12.074SS control group postest 1 0 12 2.40 0 5.366SS control group followup 0Postest differential mortality (%) 5 0 52.80 20.8444 11.42 24.17Differential mortality followup (%) 0
Table 4: Analysis of the methodological quality of Czepa et al.’s [14] study, by Van Tulder scale.
Items Czepa et al. (2013) [14]Was the method of randomization adequate? NoWas the treatment allocation concealed? NoWere the groups similar at baseline regarding the most important prognostic indicators? YesWas the patient blinded to the intervention? NoWas the care provider blinded to the intervention? NoWas the outcome assessor blinded to the intervention? NoWere cointerventions avoided or similar? NoWas the compliance acceptable in all groups? NoWas the drop-out rate described and acceptable? NoWas the timing of the outcome assessment in all groups similar? YesDid the analysis include an intention-to-treat analysis? No
Table 5: Analysis of the methodological quality of Czepa et al.’s [14] study, by PEDro scale.
Items Czepa et al. (2013) [14]Eligibility criteria were specified NoSubjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order inwhich treatments were received) No
Allocation was concealed NoThe groups were similar at baseline regarding the most important prognostic indicators YesThere was blinding of all subjects NoThere was blinding of all therapists who administered the therapy NoThere was blinding of all assessors who measured at least one key outcome NoMeasures of at least one key outcome were obtained from more than 85% of the subjects initially allocated togroups No
All subjects for whom outcome measures were available received the treatment or control condition as allocatedor, where this was not the case, data for at least one key outcome was analysed by “intention to treat” No
The results of between-group statistical comparisons are reported for at least one key outcome YesThe study provides both point measures and measures of variability for at least one key outcome Yes

Rehabilitation Research and Practice 9
4.2. Limits of the Review. There were a number of limitsplaced on this review. The lack of precision in the studiesin describing the physical therapy methods and techniquesused, as well as the sample data, raised doubts for us duringthe encoding process. Moreover, the lack of data on moder-ating variables (randomisation of the sample, masking, andthe treatment application method) limited the possibilitiesfor obtaining detailed results on this review.
The lowmethodological quality of the studies did not per-mit a detailed analysis of them, nor could outcome measuresbe extracted to calculate the effect size.
4.3. Implications for the Clinical Practice. Results of thissystematic review confirm the need for treatment of phys-iotherapy in the multidisciplinary approach to patients withhemophilia, raised previously by other authors [24, 36].However, a clear indication about the most efficacious typeof treatment is limited by the lack of controlled studies.
Physical therapy treatments must combine variousaspects. On the one hand, there must be efficacious treatmentof the problems caused by arthropathy of the ankle [42], suchas restrictions on range of motion, loss of muscular strength,pain, and alteration of proprioception. On the other hand,the treatment must not cause haemarthrosis.
4.4. Implication for Future Studies. Properly designed ran-domised clinical studies must be developed for physical ther-apy treatment in patients with hemophilic arthropathy ofthe ankle. Furthermore, the study samples must be as broadas possible, and the outcome measures must be valid andreliable.
Studies with a follow-up period are necessary to establishthe efficacy of the treatment in the medium term.
Future studies must describe the characteristics of theindividuals with respect to age, weight, the joints affected,the degree of joint impairment, and so forth; the treatmentscharacteristics (procedures, duration, intensity, etc.); and thepotential adverse effects in the locomotor system as a resultof the treatment.
5. Conclusion
There is little uniformity in the studies reviewed with respectto duration, intensity, extent, and types of treatment.
Treatments with strength and proprioception training,hydrotherapy, and sports therapy improve some clinicalaspects in patients with hemophilic arthropathy of the anklebefore and after comparison.
There is no rigorous evidence on the effects of thetreatments.
Methodological quality of the studies is low.
Conflict of Interests
The authors declare that they do not have any conflict ofinterests.
References
[1] P. Molho, N. Rolland, T. Lebrun et al., “Epidemiological surveyof the orthopaedic status of severe haemophilia A andB patientsin France,” Haemophilia, vol. 6, no. 1, pp. 23–32, 2000.
[2] R. R. Montgomery and J. P. Scott, “Hemostasis: diseases of theXuid phase,” in Hematology of Infancy and Childhood, D. G.Nathan and F. A. Oski, Eds., pp. 1605–1620, Saunders, Philadel-phia, Pa, USA, 1992.
[3] K. S. Upchurch and D. B. Brettler, “Hemophilic arthropathy,” inKelley’s Textbook of Rheumatology, S. Ruddy, E. D.Harris, andC.B. Sledge, Eds., pp. 1567–1574, Saunders, Philadelphia, Pa, USA,2001.
[4] R. B. Duthie, J. Matthews, and C. Rizza, The Management ofMusculoskeletal Problems in the Haemophilias, Blackwell Scien-tific Publications, Oxford, UK, 1972.
[5] E. C. Rodriguez-Merchan, “Effects of hemophilia on articula-tions of children and adults,” Clinical Orthopaedics and RelatedResearch, vol. 328, pp. 7–13, 1996.
[6] J. Hoskinson and R. B. Duthie, “Management of musculoskele-tal problems in the hemophilias,” Orthopedic Clinics of NorthAmerica, vol. 9, no. 2, pp. 455–480, 1978.
[7] W. J. Ribbans and J. L. Rees, “Management of equinus contrac-tures of the ankle in haemophilia,” Haemophilia, vol. 5, supple-ment 1, pp. 46–52, 1999.
[8] M. J. J. Hooiveld, G. Roosendaal, K. M. G. Jacobs et al., “Ini-tiation of degenerative joint damage by experimental bleedingcombined with loading of the joint: a possible mechanism ofhemophilic arthropathy,”Arthritis and Rheumatism, vol. 50, no.6, pp. 2024–2031, 2004.
[9] N. Hakobyan, T. Kazarian, A. A. Jabbar, K. J. Jabbar, and L. A.Valentino, “Pathobiology of hemophilic synovitis I: overexpres-sion of mdm2 oncogene,” Blood, vol. 104, no. 7, pp. 2060–2064,2004.
[10] E. Gurcay, E. Eksioglu, U. Ezer, B. Cakir, and A. Cakci, “A pro-spective series of musculoskeletal system rehabilitation ofarthropathic joints in young male hemophilic patients,” Rheu-matology International, vol. 28, no. 6, pp. 541–545, 2008.
[11] T. Hilberg, M. Hersbsleb, C. Puta, H. H. W. Gabriel, andW. Schramm, “Physical training increases isometric muscularstrength and proprioceptive performance in haemophilic sub-jects,” Haemophilia, vol. 9, no. 1, pp. 86–93, 2003.
[12] M. K. Garcia, A. Capusso, D. Montans, E. Massad, and L. R.Battistella, “Variations of the articular mobility of elbows, kneesand ankles in patientswith severe haemophilia submitted to freeactivemovimentation in a pool with warmwater,”Haemophilia,vol. 15, no. 1, pp. 386–389, 2009.
[13] K. Hill, M. Fearn, S. Williams et al., “Effectiveness of a balancetraining home exercise programme for adultswith haemophilia:a pilot study,” Haemophilia, vol. 16, no. 1, pp. 162–169, 2010.
[14] D. Czepa, S. von Mackensen, and T. Hilberg, “Haemophilia& Exercise Project (HEP): the impact of 1-year sports therapyprogramme on physical performance in adult haemophiliapatients,” Haemophilia, vol. 19, pp. 194–199, 2013.
[15] E. C. Rodriguez-Merchan, “The haemophilic ankle,” Haemo-philia, vol. 12, no. 4, pp. 337–344, 2006.
[16] D. Stephensen, R. Tait, N. Brodie et al., “Changing patterns ofbleeding in patients with severe haemophilia A,” Haemophilia,vol. 15, no. 6, pp. 1210–1214, 2009.
[17] M. Funk, H. Schmidt, C. Escuriola-Ettingshausen et al., “Radi-ological and orthopedic score in pediatric hemophilic patients
10 Rehabilitation Research and Practice
with early and late prophylaxis,” Annals of Hematology, vol. 77,no. 4, pp. 171–174, 1998.
[18] M. S. Pearce, M. A. Smith, and G. F. Savidge, “Supramalleolartrial osteotomy for haemophilic arthropathy of the ankle,” Jour-nal of Bone and Joint Surgery Series B, vol. 76, no. 6, pp. 947–950,1994.
[19] F. R. van Genderen, K. Fischer, L. Heijnen et al., “Pain andfunctional limitations in patients with severe haemophilia,”Haemophilia, vol. 12, no. 2, pp. 147–153, 2006.
[20] K. Fischer, J. G. Van Der Bom, P. Molho et al., “Prophylacticversus on-demand treatment strategies for severe haemophilia:a comparison of costs and long-term outcome,” Haemophilia,vol. 8, no. 6, pp. 745–752, 2002.
[21] S. Royal, W. Schramm, E. Berntorp et al., “Quality-of-life differ-ences between prophylactic and on-demand factor replacementtherapy in European haemophilia patients,”Haemophilia, vol. 8,no. 1, pp. 44–50, 2002.
[22] R. Tiktinsky, B. Falk, M. Heim, and U. Martinovitz, “The effectof resistance training on the frequency of bleeding in haemo-philia patients: a pilot study,” Haemophilia, vol. 8, no. 1, pp. 22–27, 2002.
[23] L. M. Aledort, R. H. Haschmeyer, and H. Pettersson, “A longi-tudinal study of orthopaedic outcomes for severe factor-VIII-deficient haemophiliacs,” Journal of Internal Medicine, vol. 236,no. 4, pp. 391–399, 1994.
[24] B. M. Buzzard, “Physiotherapy for the prevention of articularcontraction in haemophilia,”Haemophilia, vol. 5, supplement 1,pp. 10–15, 1999.
[25] J. A. Aznar, M. Magallon, F. Querol, E. Gorina, and J. M. Tusell,“The orthopaedic status of severe haemophiliacs in Spain,”Haemophilia, vol. 6, no. 3, pp. 170–176, 2000.
[26] C. M. Bleakley, S. O’Connor, M. A. Tully, L. G. Rocke, D. C.MacAuley, and S. M. McDonough, “The PRICE study (Pro-tection Rest Ice Compression Elevation): design of a ran-domised controlled trial comparing standard versus cryokineticice applications in the management of acute ankle sprain[ISRCTN13903946],” BMC Musculoskeletal Disorders, vol. 8,article 125, 2007.
[27] C. Hermans, P. De Moerloose, K. Fischer et al., “Managementof acute haemarthrosis in haemophilia A without inhibitors:literature review, European survey and recommendations,”Haemophilia, vol. 17, no. 3, pp. 383–392, 2011.
[28] K. Mulder, Exercise for People with Hemophilia, World Federa-tion of Hemophilia, Montreal, Canada, 2006.
[29] J. G. Gamble, J. Bellah, L. A. Rinsky, and B. Glader, “Arthropathyof the ankle in hemophilia,” Journal of Bone and Joint SurgerySeries A, vol. 73, no. 7, pp. 1008–1015, 1991.
[30] K. Dickersin, R. Scherer, and C. Lefebvre, “Identifying relevantstudies for systematic reviews,” BritishMedical Journal, vol. 309,pp. 1286–1291, 1994.
[31] M. W. Lipsey, “Identifying interesting variables and analysisopportunities,” in The Handbook of Research Synthesis andMeta-Analysis, H. M. Cooper, L. V. Hedges, and J. C. Valentine,Eds., pp. 147–158, Sage, New York, NY, USA, 2009.
[32] M. Van Tulder, A. Furlan, C. Bombardier, and L. Bouter,“Updated method guidelines for systematic reviews in theCochrane Collaboration Back ReviewGroup,” Spine, vol. 28, no.12, pp. 1290–1299, 2003.
[33] C. G. Maher, C. Sherrington, R. D. Herbert, A. M. Moseley, andM. Elkins, “Reliability of the PEDro scale for rating quality ofrandomized controlled trials,” Physical Therapy, vol. 83, no. 8,pp. 713–721, 2003.
[34] R. Rosenthal, Meta-Analytic Procedures for Social Research,Sage, Beverly Hills, Calif, USA, 1984.
[35] B. Koch, S. Cohen, N. C. Luban, and G. Eng, “Hemophiliacknee: rehabilitation techniques,” Archives of Physical Medicineand Rehabilitation, vol. 63, no. 8, pp. 379–382, 1982.
[36] J. R. Pelletier, T. W. Findley, and S. A. Gemma, “Isometric exer-cise for an individual with hemophilic arthropathy,” PhysicalTherapy, vol. 67, no. 9, pp. 1359–1364, 1987.
[37] A.-M. Nazzaro, S. Owens, W. K. Hoots, and K. L. Larson,“Knowledge, attitudes, and behaviors of youths in the UShemophilia population: results of a national survey,” AmericanJournal of Public Health, vol. 96, no. 9, pp. 1618–1622, 2006.
[38] T. Hilberg, M. Herbsleb, H. H. W. Gabriel, D. Jeschke, and W.Schramm, “Proprioception and isometric muscular strength inhaemophilic subjects,” Haemophilia, vol. 7, no. 6, pp. 582–588,2001.
[39] S. Harris and L. N. Boggio, “Exercise may decrease furtherdestruction in the adult haemophilic joint,” Haemophilia, vol.12, pp. 237–240, 2006.
[40] R. Mulvany, A. R. Zucker-Levin, M. Jeng et al., “Effects of a 6-Week, individualized, supervised exercise program for peoplewith bleeding disorders and hemophilic arthritis,” PhysicalTherapy, vol. 90, no. 4, pp. 509–526, 2010.
[41] M. Luterek, M. Baranowski, W. Zakiewicz, A. Biel, and P.Pedzisz, “PNF-based rehabilitation in patients with severehaemophilic arthropathy—case study,” Ortopedia Traumatolo-gia Rehabilitacja, vol. 11, no. 3, pp. 280–289, 2009.
[42] L. Heijnen and P. de Kleijn, “Physiotherapy for the treatmentof articular contractures in haemophilia,” Haemophilia, vol. 5,supplement 1, pp. 16–19, 1999.
[43] D. J. Filho, L. R. Battistella, and C. Lourenco, “Computerizedpedobarography in the characterization of ankle-foot instabil-ities of haemophilic patients,” Haemophilia, vol. 12, no. 2, pp.140–146, 2006.
[44] A. Lambing, B. Kohn-Converse, S. Hanagavadi, and V. Varma,“Use of acupuncture in themanagement of chronic haemophiliapain,” Haemophilia, vol. 18, pp. 613–617, 2012.
[45] I. A. d’Young, “Domiciliary application of CryoCuff in severehaemophilia: qualitative questionnaire and clinical audit,”Haemophilia, vol. 14, no. 4, pp. 823–827, 2008.
[46] S. Von Mackensen, B. Eifrig, D. Zach, J. Kalnins, A. Wieloch,and W. Zeller, “The impact of a specific aqua-training for adulthaemophilic patients—results of theWATERCISE study (WAT-QoL),” Haemophilia, vol. 18, pp. 714–721, 2012.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com





























