Embed Size (px)
Citation preview

Hindawi Publishing CorporationThe Scientific World JournalVolume 2013 Article ID 170576 9 pageshttpdxdoiorg1011552013170576
Review ArticleOral Anticoagulant Therapy in Patients ReceivingHaemodialysis Is It Time to Abandon It
Marek Saracyn Dorota Brodowska-Kania and StanisBaw Niemczyk
Department of Internal Diseases Nephrology and Dialysis Military Institute of Medicine Szaserow Street 128 04-141 Warsaw Poland
Correspondence should be addressed to Marek Saracyn msaracyninteriapl
Received 13 September 2013 Accepted 28 October 2013
Academic Editors F Hinoshita and R Sakai
Copyright copy 2013 Marek Saracyn et alThis is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Oral anticoagulant (OAC) therapy in haemodialysis patients causes a great deal of controversy This is because a number of pro-and anticoagulant factors play an important role in end-stage renal failure due to the nature of the disease itself In these conditionsthe pharmacokinetic and pharmacodynamic properties of the OACs used change as well In the case of the treatment of venousthromboembolism the only remaining option is OAC treatment according to regimens used for the general population Preventionof HD vascular access thrombosis with the use of OACs is not very effective and can be dangerous However OAC treatment inpatients with atrial fibrillation in dialysis population may be associated with an increase in the incidence of stroke and mortalityDoubts should be dispelled by prospective randomised studies at the moment there is no justification for routine use of OACs inthe above-mentioned indications In selected cases of OAC therapy in this group of patients it is absolutely necessary to controland monitor the applied treatment thoroughly Indications for the use of OACs in patients with end-stage renal disease includinghaemodialysis patients should be currently limited
1 Introduction
Chronic kidney disease (CKD) constitutes an increasinglyserious challenge for modern medicine both in its strictlyclinical aspect and in the epidemiological one According todifferent but essentially consistent estimates it is assumedthat its various stages currently affect more than 600 millionpeople worldwide including 10 million patients with its endstage and 2 million patients undergoing various forms ofrenal replacement therapyThe high incidence andmorbidityin the terminal stages of CKD are also associated with ahigh mortality rate which is almost 19 of all patientsundergoing different forms of dialysis treatment [1] Themost common causes of death in this population of patientsinclude cardiovascular diseases (CVDs) (39) infections(12) stroke (103) and neoplastic diseases (10) [2] Thehigh epidemiological indices result from both the agingof the population and other concomitant diseases (such ascardiovascular diseases diabetes and arterial hypertension)increasingly and commonly occurring also in this group ofpatients Epidemiological data fully justify the statement that
CKD has become a serious social issue and like the above-mentioned conditions another lifestyle disease
As the incidence and prevalence of CKD and its endstages in particular increase the number of patients under-going various forms of renal replacement therapy also con-stantly increases Of the three basic treatment methodshaemodialysis (HD) therapy is the one that is most com-monly applied This is because according to global datamore than 68 of patients requiring renal replacement ther-apy undergo haemodialysis patients after renal transplantaccount for approximately 23 of the discussed populationwhile patients treated with peritoneal dialysis constitute lessthan 9 [3] Prognoses for the next few years suggest a furtherincrease in the number of patients requiring different formsof renal replacement therapy including patients receivinghaemodialysis especially among patients with diabetes arte-rial hypertension as well as the elderly ones [4]
In recent years the indications for treatment with oralanticoagulants (OACs) as well as their use have increasedsignificantly [5] This phenomenon included both the entirepopulation of patients with CKD and patients receiving
2 The Scientific World Journal
Table 1 Factors conducive to coagulation disorders in patients with end-stage renal disease and receiving haemodialysis [8ndash13]
Factors conducive to bleeding events Factors conducive to thrombosisDirectlyPlatelet adhesion disordersmdashdecreased activity of von Willebrandfactor and receptor GPIb increased release of PGI2 NOPlatelet aggregation disordersmdashdecreased activity of GPIIbIIIareceptor impaired binding of fibrinogen to plateletsPlatelet secretion disordersmdashdecreased production of thromboxaneA2 serotonin and ADP decreased release of 120573-thromboglobulinand impaired Ca++ mobilizationReduced number and volume of platelets
Accelerated atherosclerotic processes damaged endotheliumDefective GPIb expression on the surface of plateletsDisorders of protein C metabolism decreased concentration ofprotein C and antithrombin IIIElevated concentrations of plasminogen activator inhibitor-1(PAI-1)
IndirectlyAnaemiamdashaltered rheological features of blood impaired plateletaggregationUraemic toxinsmdashfor example PTHMedicationsmdashantiplatelet anticoagulant cephalosporinsantitubercular inhibitors of lipid absorption NSAIDsConcomitant diseasesmdashfor example affecting the gastrointestinaltractInvasive proceduresmdashcannulations biopsies vascular accessGP glycoprotein PGI2 prostacyclin NO nitric oxide ADP adenosine diphosphate Ca calcium ions PTH parathormone NSAIDs non-steroidal anti-inflammatory drugs
haemodialysis [6] The continuously growing population ofpatients receiving haemodialysis as a result of the increas-ing prevalence of the aforementioned lifestyle diseases orsocial and demographic factors associated with them hasan undoubted impact on this fact Attempts to find newapplications for OACs in this group of patients are howevernot less important Although they are based on a number ofprospective randomised studies in the general populationthere are no such studies in the group of patients receivinghaemodialysis [7] Attempts to apply the results of studiescarried out in the general population from which patientswith end-stage renal failure are usually excluded to beginwith to patients receiving haemodialysis are not only unjusti-fied but sometimes have downright negative influence on theeffectiveness of treatment and patientsrsquo safety
2 Chronic Kidney Disease andHaemostasis Disorders
As renal failure progresses increasingly significant distur-bances occur in the process of blood coagulation At the ini-tial stages ofCKDmostly as a result of disorders of the plasmacoagulation system and fibrinolysis (eg decreased levelsof protein C and antithrombin III elevated concentrationsof fibrinogen von Willebrand factor factor VIII elevatedconcentration of plasminogen activator inhibitor-1 (PAI-1)decreased concentration of tissue plasminogen activator (t-PA)) prothrombotic processes clinically expressed as hyper-coagulation dominate [8 9] As glomerular filtration rate(GFR) decreases and renal failure progresses uraemic bleed-ing diathesis characteristic of end-stage renal failure andpatients during dialysis therapy worsens At the end stages ofCKD the accumulating uraemic toxins both low-molecular-weight (eg urea phenol and guanidinosuccinic acid) andmedium-molecular-weight ones (eg RGD polypeptides)
affect mostly platelet function inhibiting their adhesionand aggregation and releasing platelet factors such as sero-tonin or thromboxane A
2[10 11] These phenomena mostly
lead to platelet haemostasis disorders Uraemic toxins andproinflammatory cytokines frequently co-occurring lipiddisorders or arterial hypertension damage endothelium andin this way disrupt also vascular haemostasis As a result oftheir stimulation endothelial cells produce large amounts ofprostacyclin (PGI
2) and nitric oxide (NO) [12] The former
is a strong inhibitor of platelet aggregation and the latter ofplatelet adhesion Their elevated concentrations thereforeincrease the existing haemorrhagic diathesis
A clear bleeding tendency does not exclude of coursea simultaneous state of increased prothrombotic suscepti-bility even in the same patient The peculiar competitionbetween these two antagonistic systems is presented inTable 1 which includes factors that occur as renal failureprogresses predisposing the patient to bleeding events andon the other hand to the formation of thrombi [13] Thefactors conducive to bleeding mentioned in the table as wecan see mostly disrupt platelet haemostasis they disruptvascular haemostasis to a lesser extent mainly those thatdo not take part in the process of coagulation directlyOn the other hand prothrombotic factors include apartfrom those affecting plasma haemostasis first and foremostthe state of endothelium and accelerated atheroscleroticprocesses inextricably linked with end-stage renal failure[14] Most frequently this dynamic equilibrium is slightlyshifted towards haemorrhagic diathesis which is suggestedby the clinical characteristics of the haemodialysed patientthe results of his or her additional tests usually increasedbleeding time with usually normal APTT and INR Thisstate of equilibrium is however extremely unstable and theslightest additional factor affecting the processes of bloodcoagulationfibrinolysis shifts it to either of the sides
The Scientific World Journal 3
3 Chronic Kidney Disease andOral Anticoagulant Treatment
The applied medications are a factor which frequently andsignificantly disturbs the above-described equilibrium Vita-min K antagonists are still the most commonly used oralanticoagulant medications (incidentally the erroneous nameldquoantagonistsrdquo has been adopted though they do not haveantagonist effects on vitaminK only inhibitory ones so to beprecise they are its inhibitors) The first medicine from thisgroup was dicoumarol isolated by Karl Link at the Universityof Wisconsin in 1941 [15] However they really started tobe commonly used in 1950 when a more effective andbioavailable medicine was introducedmdashwarfarin [16] Theirmechanism of action consists in inhibiting the activity of thevitaminK reductase complex whichmakes the carboxylationof the residues of glutamic acid in the N-terminal fragmentsof different proteins impossible This way the activity offour key factors of the blood coagulation system factorsII VII IX X is inhibited [17] It is a strong anticoagulantactivity because key factors both to the auxiliary endogenouspathway and first and foremost to the exogenous pathwayfundamental to the coagulation system are inhibited Attherapeutic doses the inhibition of the aforementioned coag-ulation factors should range from 30 to 50 [18] This verynarrow therapeutic window can on the one hand result inthe ineffectiveness of treatment and on the other in frequentserious adverse reactions mostly severe bleeding eventsOACs in the blood strongly bind to albumins but the activefree fraction fluctuates in a fairly wide range (from 05 to 3)[19] Elimination occurs via hepatic metabolism by variouscytochromes for each of the isomers of the active ingredientof the medicine its inactive metabolites are excreted by thekidneys [20]The half-life is from 18 to 70 hours [21] It wouldseem that the hepatic metabolism of coumarin derivativesjustifies the use of these medications in patients with end-stage renal failure and receiving haemodialysis following thesame rules and at the same doses as in the general pop-ulation However the above-described pharmacodynamicand pharmacokinetic properties make treatment with OACsin patients receiving haemodialysis extremely difficult Thetherapeutic window becomes even narrower the concen-trations of the free fraction of the medicine fluctuate evenmore depending on changes in peridialytic volaemia and theamount of fraction bound to albumins decreases as a resultof malnutrition or patient cachexia [22] Moreover thereare a number of known nutritional limitations associatedwith using OACs restrictions in the treatment of elderlyindividuals (slower hepatic metabolism) or their numerousinteractions with other medicines (especially antiplateletones) [23] In the conditions of advanced CKD the impactof all these factors is much greater [24]
Maruyama et al [25] evaluating INR and albumin valuesbefore and after HD procedures demonstrated a significantdecrease in the value of INR following HD in comparisonwith its levels determined prior to HD while albumin con-centrations increased significantly following the procedure inrelation to values prior to dialysis What is more the authorsalso showed a significant negative correlation between both
of the above-described parameters during haemodialysisAbe et al [26] apart from similar changes regarding INRand proteins during HD demonstrated a significant risein warfarin concentrations post-HD versus pre-HD bothwith respect to the more potent S-isomer and the weakerR-isomer Interestingly multifactorial analysis revealed thestrongest links between peridialytic values of INR and albu-min concentrations The ability of blood proteins especiallyalbumin to bind warfarin is very strong and thereforechanges in their concentration duringHD result in significantchanges in the concentrations of the active ingredient of themedicine INR and consequently treatment complicationsIn a retrospective study of 142 haemodialysed patients whoreceived acenocoumarol for typical indications at a dose of1mg a day for a year Gompou et al [27] demonstratedthat 30 of the INR values determined at this time werebelow target values 37 were in the therapeutic range andnearly 33 exceeded therapeutic values Admittedly thereis no information regarding the severe complications ofsuch treatment in the report but the fact that OACs wereoverdosed in 13 of the cases seems alarming
So far among patients with end-stage renal failure andpatients receiving haemodialysis no prospective randomisedstudies evaluating the effectiveness and safety of OACs havebeen conducted In spite of that in this group of patientsthese medications are attempted to be used according to theirtypical indications taking however special precautions inusing them due to the considerably increased risk of adversereactions [28] Indeed the literature includes a number ofreports of such reactions including very severe and fatalones [29ndash31] It is also interesting to read the official con-traindications for the use of OACs approved in registrationdocuments by regulatory bodies authorised to do that [32](eg the FDA) (Table 2) On the list presented in Table 2almost every other item (eg 1 3 5 7 and the last one) refersto patients with end-stage renal failure including patientsreceiving haemodialysis Admittedly chronic renal failure isnot explicitly listed but the items enumerated above referdirectly to it In any case most of them overlap with factorspredisposing to bleeding events in patients with end-stagerenal failure and receiving haemodialysis as described earlier(Table 1) As we can see platelet function disorders otherthrombocytopathies the risk of gastrointestinal bleedingurinary tract bleeding falls or lack of adequate collaborationin this specific treatment are especially significant in thisrespect After all it is a picture of patients that we see innephrology units or at dialysis centres on a daily basis Istherefore OAC treatment according to its typical indica-tions in patients with end-stage CKD or in those receivinghaemodialysis an off-label use an experimental one andtherefore is it justified these questions remain open
4 OACs in Patients with End-Stage RenalDisease in Clinical Practice
Attempts to use OACs in patients at the end stages of CKDand receiving haemodialysis encounter a number of diffi-culties Practically all prospective controlled randomised
4 The Scientific World Journal
Table 2 Contraindications for the use of oral anticoagulants [32]
(i) Increased risk of bleeding eventsmdashplatelet function disorders thrombocytopenia vonWillebrand disease and haemophilia(ii) Recent intracranial bleeding Conditions predisposing to intracranial bleedingmdashcerebral artery aneurysms(iii) Conditions predisposing to gastrointestinal urinary and respiratory tract bleeding(iv) Surgical procedures within the central nervous system or the eye(v) Increased risk of frequent fallsmdashcaused by a neurological or another condition(vi) Severe liver failure cirrhosis(vii) Untreated or poorly controlled arterial hypertension(viii) Pregnancy(ix) Infective endocarditis or pericardial effusion(x) Hypersensitivity to the active substance or any of the excipients(xi)Dementia psychoses alcoholism and other conditions in which compliance may not be satisfactory andwhen anticoagulant treatment cannot be safely administeredEnd-stage renal-disease-associated items are bold
studies which evaluated the effectiveness and safety of OACsin the general population carried out so far excluded patientswith creatinine clearance lt30mLmin Applying the resultsof these studies to the population with advanced renal failureshould not therefore be automatic because their simple usenot only may prove to be ineffective in this group of patientsbut what is worse may be dangerous to them as well
41 OACs in the Treatment of Venous Thromboembolism inPatients with CKD The prevalence of pulmonary embolismin the population of patients receiving haemodialysis isseveral times higher than its prevalence in the generalpopulation The annual incidence of pulmonary embolismin this group of patients is approximately 15100000 versus25100000 patients in the general population [33] Howeverthere are no evidence-based studies evaluating the use ofOACs in this disease and in this population The remainingoption therefore is beginning treatment with unfractionatedheparin usually on an inpatient basis then changing it overthe next several days and continuing the OAC treatmentwhile monitoring INR which is the treatment acceptedgenerally for the population without renal failure [34] Dueto the lack of relevant research the length of therapy depend-ing on the aetiology of the disease the individual risk ofthrombosisbleeding events for a given patient and often thedecision of the patient him- or herself regarding the appliedOAC treatment remain to be evaluated In the case of absolutecontraindications for OACs implantation of a filter in theinferior vena cava could be an alternative therapy but thereare no such studies for patients receiving haemodialysis inthe available literature and they are inconclusive even in thegeneral population [35]
42 OACs in Preventing Thrombosis of Vascular Access forHaemodialysis It is estimated that the causes of almost 13of cases requiring hospitalisation among patients receivinghaemodialysis are associatedwith vascular access failure [40]The likelihood of the occurrence of vascular access failuredue to thrombosis in over a year-long observation of patientsreceiving haemodialysis is approximately 15 in the case of
autologous arteriovenous fistulae and two times higher in thecase of vascular grafts [41] It would therefore seem thatOACscan be an effective treatment option in reducing this risk
Several such prospective controlled studies (some ofwhich were even randomised) have been conducted thoughon small groups of patients Their results however proved tonot be very encouraging In a group of 75 patients receivinghaemodialysis OAC treatment whose therapeutic target wasINR 15ndash20 was found to be only slightly more effective inthe prevention of thrombotic complications in comparisonwith the control group in which OAC treatment was notinitiated (66 versus 57) but the recorded difference wasnot statistically significant [42] What is more in spite ofthe unchanging study protocol the target INR values wereachieved in only a half of the subjects While serious bleedingevents were not recorded the target INR range was not highIn another randomised study on a group of 144 patientsreceiving haemodialysis Colı et al [43] used OACs with alittle higher therapeutic range of INR (18ndash25) Statisticallysignificant differences between the study group and thecontrol group not treated with OACs were observed onlyafter taking the time at which OAC treatment was initiatedinto consideration In the group in which this treatmentwas initiated in the first 24 hours after the implantation ofa vascular catheter vascular complications were found in alittle more than 10 of patients in comparison with patientswho received OACs after their first thrombotic event wherethe proportion of complications was a little over 50 Inanother study carried out on a group of 63 patients receivinghaemodialysis the use of OACs whose therapeutic aim wasINR of 20-30 was proved to be significantly more effectivein preventing thrombosis than in the group of patients notreceiving such treatment [44] However when the resultsof the group treated with OACs were compared with thegroup in which acetylsalicylic acid at a dose of 325mgdaywas used differences in the effectiveness regarding vascu-lar access thrombosis were not observed Serious bleedingevents which significantly more frequently occurred in thegroup receiving OACs were the only significant differencebetween these groups
The Scientific World Journal 5
Table 3 Mortality risk in haemodialysis patients with atrial fibrillation treated with warfarin
Study Population (119899) Period (y) Mortality (HR)Knoll et al [36] 119899mdash235 pts 3 years HRmdash080 (95 CI 028ndash229 119875 lt 067)Chan et al [37] 119899mdash1671 pts 1 year HRmdash110 (094ndash130)
Wizemann et al [38] 119899mdash17513 pts(AFmdash125) 7 years
All ages HRmdash116 (95 CI 108ndash125 119875 lt 0001)Age lt 65 HRmdash129 (95 CI 045ndash368 119875 lt 063)Age 65ndash75 HRmdash135 (95 CI 069ndash263 119875 lt 039)Age gt 75 HRmdash217 (95 CI 104ndash453 119875 lt 004)
Chan et al [39]
119899mdash41425 pts
11 yearsWarfarinmdash83 HRmdash173 (95 CI 162ndash185)Clopidogrelmdash10 HRmdash150 (95 CI 139ndash162)Acetylsalicylicacidmdash304 HRmdash117 (95 CI 112ndash122)
Acetylsalicylic acidand warfarinmdash8 HRmdash111 (95 CI 103ndash186)
HR hazard ratio CI confidence interval 119899 number of patients
How effective is therefore the application of OACs inthis group of patients As the few not very reliable studiessuggest it admittedly increaseswith the increase in the targetINR but at the price of significant adverse reactions in theform of serious bleeding events Moreover in the last ofthe cited studies which confirmed such effectiveness similareffectiveness was recorded with the use of acetylsalicylic acidwithout severe complicationsThe results of the above studiesand the opinions of experts in the area do not allow thereforea routine use of OACs due to the discussed indications [45]This is because a target safe INR range for this group ofpatients has not been established the effectiveness of themedications is doubtful and the risk for the patient is highfurthermore there are alternative methods that are no lesseffective and as it appears are safer [44]
43 OACs in the Prevention ofThromboembolic ComplicationsAssociated with Atrial Fibrillation Atrial fibrillation (AF) isthe most common cardiac dysrhythmia It is estimated that itaffects several percent of the population over the age of 65 andthe proportion increases with age [46] However in the groupof patients with end-stage renal failure this proportion ismuch higher and reaches according to various studies from10 to as high as 30 [47] The annual mortality rate amongthese patients is approximately 25 in the general populationand almost 30 in patients receiving haemodialysis [48]Theprevalence of stroke in patients with atrial fibrillationwithoutrenal failure is on the other hand close to that in patientsreceiving haemodialysis (17 versus 15 resp) [49 50]Similarly studies evaluating the risk of stroke among patientsreceiving haemodialysis depending on the presence of AF orsinus rhythm are inconclusive Some of them show a several-fold increase in the incidence of stroke in the group with AFwhile others do not record such a correlation [50 51] Thesetwo factors among other things are probably responsible forthe inconclusive results of studies evaluating the effectivenessand safety of OAC treatment due to AF in the group ofpatients with end-stage renal failure and patients receiving
haemodialysis The confusion in the literature regardingthe plausibility and significance of the discussed issue isincreased however mostly by the fact that there are simplyno prospective controlled randomised studies in this group
First let us look at the impact of the use of OACs in thisgroup of patients on the hard end-point which is patientmortality (Table 3) Knoll et al [36] carrying out a studyon a group of 235 haemodialysed patients with AF receivingOACs recorded a slightly lower mortality rate than thatwhich characterised the control group not receiving OACsalthough not significant Chan et al [37] in a retrospectivestudy conducted on more than 1600 patients with AFreceiving haemodialysis showed that the use of warfarin inthe prevention of thromboembolic events is not associatedwith all-cause mortality or an increase in the number ofhospitalisations In turn Wizemann et al [38] observed aclear increase in mortality rate in patients receiving warfarinfor the same reasons as in haemodialysed ones which wasespecially apparent in the older population (gt75 years old)Another study confirmed the negative impact of OACs usedfor the same indications on themortality rate in patients withend-stage renal failure in comparison with the control groupwhich did not receive such treatment [39]
Data regarding effectiveness in decreasing the risk ofstroke in patients with AF receiving haemodialysis are alsoinconclusive In one of the latest of such studies Olesenet al [52] in a group of more than 900 patients in whomwarfarin was used in fewer than 20 of cases observed for aperiod of 11 years and found a statistically significant decreasein the risk of the occurrence of stroke or another systemicthromboembolic event However in several other studiessuch an effect was not observed what is more the effect ofusing OACs was decidedly negative In the study cited aboveChan et al [37] recorded a two times higher risk of strokein the group treated with warfarin than in the control groupnot receiving OACs Furthermore there was an increase inthe risk of both haemorrhagic and ischaemic stroke (HR 22and 18 resp) Similar results were presented by Wizemann
6 The Scientific World Journal
et al [38] in a group of 3245 patients participating inDOPPS I and DOPPS II (Dialysis Outcomes and PracticePatterns Study) In this study the patientsrsquo age was the factordifferentiating the risk In the oldest group (gt75 years old)warfarin treatment was associated with a significant morethan twofold increase in the risk of stroke in younger groups(65ndash75 and lt65) the increase in the risk of stroke wasevident but statistically insignificant In another study whichcovered 2313 haemodialysed patients with newly diagnosedAF and treated with warfarin for the first time Winkelmayeret al [53] observed an over twofold increase in the risk ofhaemorrhagic stroke such a relationshipwas not found in thecase of ischaemic stroke
The risk of adverse reactions including severe bleed-ing events during OAC treatment in patients receivinghaemodialysis rises considerably Previous studies in whichOACs were used for different indications had alreadyreported that [54] In the case of the treatment of AF thesituation looks similar most reports suggest a several-foldincrease in this risk The results of the study by Chan etal [39] suggest a significant almost threefold increase inthe risk of severe bleeding events during OAC treatmentin haemodialysed patients due to AF In the same studyclopidogrel was associated with a more than 25-fold (higher)risk of significant haemorrhagic complications what is inter-esting is that the use of acetylsalicylic acid also increasedthis risk but not significantly Holden et al [55] in turnobserved an increase in such risk which was more thanthreefold in the case of warfarin and over fourfold in thecase of acetylsalicylic acid the use of these medications incombinationwas associated withmore than a sixfold increasein this risk Other studies also suggested a significant risk ofsevere bleeding events associated with the use of OACs inthe prevention of thromboembolic complications due to AF[52 56]
Is therefore OAC treatment for the above indications inpatients receiving haemodialysis effective and safe Do thebenefits of using OACs outweigh the risk of severe bleedingevents in patients with end-stage renal failure
All of the above study results should be treated cautiouslyAs we have mentioned there are no large-scale controlledprospective randomised studies here Only on the basis ofsuch studies would it be possible to present guidelines orrecommendations regarding OAC treatment in this groupof patients Most of them are studies conducted on smallgroups observational retrospective groups only a few ofthemwere prospective but not randomised It is also difficultto perform a reliable meta-analysis because the individualstudies sometimes differ in their design specific assumptionsmethods of collecting data ormethods of analysis [37 38 53]Decisions regarding the initiation of OAC treatment andthe time when it occurred depended mostly on the patientrsquosclinical data and the physicianrsquos experience Some studies alsoexcluded patients taking OACs or patients with AF that haddeveloped before renal failure All these circumstances makeit necessary to evaluate these studies cautiously
Moreover let us look at two epidemiological issues [49ndash51]The prevalence of stroke in patients with atrial fibrillationwithout renal failure in comparison with that in patients
receiving haemodialysis turned out to be comparable in theabove-cited studies However the evaluation of the risk ofstroke in patients receiving haemodialysis depending on thepresence of AF or sinus rhythm proved to be inconclusive Iftherefore there is no such risk what role are OACs supposedto play Perhaps a significant portion of the causes of strokein the group with end-stage renal failure are vascular onesand atherosclerosis considerably accelerated in this group ofpatients In this situation OACs would not change such risksignificantly
In turn the increase in the risk of death and the increasein the incidence of stroke in haemodialysed patients treatedwith OACs may be explained by two things The first oneis of course inappropriate management of anticoagulationor rather the time during which the patient remains in thedesired INR range After all its deviation towards higher orlower values is associated with an increase in morbidity oradverse reactions On a daily basis in nephrology units ordialysis centres we can see how difficult it is to keep INR insuch a therapeutic range in patients receiving haemodialysisIt is associated with the fact that chronic renal failureand haemodialysis therapy to an even larger extent are asignificant and independent factors that may decrease theperiod in which the desired value of INR is maintained [57]Anyway the above-cited data regarding the increase in therisk of bleeding events during OAC treatment in patientsreceiving haemodialysis most likely result from the samecause The described impact of vitamin K antagonists onthe processes of vascular calcification and calciphylaxis isanother noteworthy potential factor As a number of studiesboth experimental and clinical show vitamin K inhibitionfor example by OACs inhibits the activity of matrix Glaprotein (MGP) an important protein playing a preventiverole in vascular calcification [58 59] OACs can thereforedirectly interfere and accelerate the process of vascularcalcification already increased in end-stage renal failureIs it a causative factor significantly raising the incidenceof ischaemic stroke and mortality among haemodialysedpatients receiving OACsThis question must be answered byfuture studies
Patients with end-stage renal failure including above allthose who receive haemodialysis are a group of patients withexceptionally many concomitant diseases [60] Considerablyaccelerated atherosclerotic processes vascular calcificationchronic inflammation lipid disorders and malnutrition areinherent characteristics of this population of patients CanOACs have an impact on the risk of stroke in haemodialysedpatients with AF in these conditions and with the existingvascular changes also within the central nervous systemmdashthis Question remains open However the results of the citedstudies do not allow us to use OACs routinely for theseindications in this group of patients
5 Conclusions
The population of patients with CKD including patientsreceiving haemodialysis keeps growing all over the world
The Scientific World Journal 7
Table 4 Potential indications for oral anticoagulants in patientswith end-stage renal disease and receiving haemodialysis
(i) Status after prosthetic heart valve implantation(ii) Antiphospholipid syndrome(iii) Secondary prevention of severe thromboembolic events (forexample pulmonary embolism)(iv) Atrial fibrillation with a high risk of stroke
However OAC treatment in this group of patients irrespec-tive of its indications causes a great deal of controversy Thisis because a number of pro- and anticoagulant factors playan important role in end-stage renal failure due to the natureof the disease itself In these conditions the pharmacokineticand especially pharmacodynamic properties of the OACsused change as well All these factors make proper anticoagu-lation in these patients more difficult and most importantlythey decrease the time during which patients remain inthe therapeutic range of INR In the case of the treatmentof venous thromboembolism the only remaining option isOAC treatment according to regimens used for the generalpopulation as there are no relevant studies concerning thegroup of patients receiving haemodialysis Prevention of HDvascular access thrombosis with the use of OACs accordingto the presented studies and expertsrsquo opinions is not veryeffective and can additionally be very dangerous HoweverOAC treatment in haemodialysed patientswithAF in order toprevent thromboembolic events according to some authorsis associated with an increase in the incidence of stroke andmortality
Is the provocative question included in the title justifiedDoubts should be dispelled by prospective controlled ran-domised studies at the moment there is no justification forroutine use of OACs in the above-mentioned indications Inselected cases of OAC treatment in this group of patients it isabsolutely necessary to control andmonitor the applied treat-ment thoroughly According to the authors and the opinionsalready partially reported in the literature [45] indicationsfor the use of OACs in patients with end-stage renal failureincluding patients receiving haemodialysis should be limitedto those included in Table 4
References
[1] S I Hallan J Coresh B C Astor et al ldquoInternational compari-son of the relationship of chronic kidney disease prevalence andESRD riskrdquo Journal of the American Society of Nephrology vol17 no 8 pp 2275ndash2284 2006
[2] B Rutkowski ldquoChanging pattern of end-stage renal disease incentral and eastern Europerdquo Nephrology Dialysis Transplanta-tion vol 15 no 2 pp 156ndash160 2000
[3] J J Snyder R N Foley and A J Collins ldquoPrevalence of CKDin the United States a sensitivity analysis using the NationalHealth and Nutrition Examination Survey (NHANES) 1999ndash2004rdquo American Journal of Kidney Diseases vol 53 no 2 pp218ndash228 2009
[4] E Krol B Rutkowski P Czarniak et al ldquoEarly detection ofchronic kidney disease results of the PolNef studyrdquo AmericanJournal of Nephrology vol 29 no 3 pp 264ndash273 2009
[5] S Ghanny and M Crowther ldquoTreatment with novel oralanticoagulants indications efficacy and risksrdquo Current Opinionin Hematology vol 20 pp 430ndash436 2013
[6] T Kruger V Brandenburg G Schlieper et al ldquoSailing betweenScylla andCharybdis oral long-term anticoagulation in dialysispatientsrdquo Nephrology Dialysis Transplantation vol 28 pp 534ndash541 2013
[7] S Genovesi and A Santoro ldquoAnticoagulants renal failure andatrial fibrillationrdquo Expert Opinion on Drug Safety vol 12 pp 1ndash3 2013
[8] N Leung ldquoHematologic manifestations of kidney diseaserdquoSeminars in Hematology vol 50 pp 207ndash215 2013
[9] J A Milburn K Cassar I Ford N Fluck and J BrittendenldquoProthrombotic changes in platelet endothelial and coagulationfunction following hemodialysisrdquo International Journal of Arti-ficial Organs vol 34 no 3 pp 280ndash287 2011
[10] D I Jalal M Chonchol andG Targher ldquoDisorders of hemosta-sis associated with chronic kidney diseaserdquo Seminars inThrom-bosis and Hemostasis vol 36 no 1 pp 34ndash40 2010
[11] D Kaw and D Malhotra ldquoPlatelet dysfunction and end-stagerenal diseaserdquo Seminars in Dialysis vol 19 no 4 pp 317ndash3222006
[12] M A de Sa Siqueira T M C Brunini N R Pereira et alldquoIncreased nitric oxide production in platelets from severechronic renal failure patientsrdquo Canadian Journal of Physiologyand Pharmacology vol 89 no 2 pp 97ndash102 2011
[13] P Boccardo G Remuzzi and M Galbusera ldquoPlatelet dysfunc-tion in renal failurerdquo Seminars in Thrombosis and Hemostasisvol 30 no 5 pp 579ndash589 2004
[14] A S Gangji A S Sohal D Treleaven and M A CrowtherldquoBleeding in patients with renal insufficiency a practical guideto clinicalmanagementrdquoThrombosis Research vol 118 no 3 pp423ndash428 2006
[15] J C McCarter J B Bingham and O O Meyer ldquoStudies on thehemorrhagic agent 3 31015840-methylenebis (4-Hydroxycoumarin)IV The pathologic findings after the administration ofdicumarolrdquo The American Journal of Pathology vol 20 pp651ndash659 1944
[16] D V Clatanoff P O Triggs and O O Meyer ldquoClinical expe-rience with coumarin anticoagulants warfarin and warfarinrdquoArchives of Internal Medicine vol 94 no 2 pp 213ndash220 1954
[17] C Becattini M C Vedovati and G Agnelli ldquoOld and neworal anticoagulants for venous thromboembolism and atrialfibrillation a review of the literaturerdquoThrombosis Research vol129 no 3 pp 392ndash400 2012
[18] E A Nutescu ldquoOral anticoagulant therapies balancing therisksrdquoAmerican Journal of Health-System Pharmacy vol 70 no10 supplement 1 pp S3ndashS11 2013
[19] M Zacchigna G di Luca F Cateni and V Maurich ldquoImprove-ment of warfarin biopharmaceutics by conjugation with poly(ethylene glycol)rdquo European Journal of Pharmaceutical Sciencesvol 23 no 4-5 pp 379ndash384 2004
[20] G F Pineo and R D Hull ldquoVitamin K antagonists and directthrombin inhibitors present and futurerdquoHematologyOncologyClinics of North America vol 19 no 1 pp 69ndash85 2005
[21] B F Gage and P E Milligan ldquoPharmacology and pharma-cogenetics of warfarin and other coumarins when used withsupplementsrdquo Thrombosis Research vol 117 no 1-2 pp 55ndash592005
[22] K S Brimble A J Ingram J W Eikelboom et al ldquoAntico-agulants in patients with atrial fibrillation and end-stage renaldiseaserdquo Postgraduate Medicine vol 124 pp 17ndash25 2012
8 The Scientific World Journal
[23] S Benmira Z K Banda and V Bhattacharya ldquoOld versusnew anticoagulants focus on pharmacologyrdquo Recent Patents onCardiovascular Drug Discovery vol 5 no 2 pp 120ndash137 2010
[24] N A Limdi M A Limdi L Cavallari et al ldquoWarfarin dosingin patients with impaired kidney functionrdquoAmerican Journal ofKidney Diseases vol 56 no 5 pp 823ndash831 2010
[25] N Maruyama M Abe K Okada et al ldquoChanges to pro-thrombin international normalized ratio in patients receivinghemodialysisrdquo International Journal of Clinical PharmacologyandTherapeutics vol 51 pp 283ndash287 2013
[26] M Abe N Maruyama H Suzuki et al ldquoInternational nor-malized ratio decreases after hemodialysis treatment in patientstreated with warfarinrdquo Journal of Cardiovascular Pharmacologyvol 60 pp 502ndash507 2012
[27] AGompou I Griveas I Kyritsis I AgroyannisMTsakoniatisand B Agroyannis ldquoINR deviations in hemodialyzed patientsunder low dose oral anticoagulant therapyrdquo International Jour-nal of Artificial Organs vol 32 no 10 pp 752ndash755 2009
[28] J C van Blijderveen K M Verhamme R Zietse et alldquoOveranticoagulation is associated with renal function declinerdquoJournal of Nephrology vol 26 pp 691ndash698 2013
[29] M M Sood M Larkina J R Thumma et al ldquoMajor bleed-ing events and risk stratification of antithrombotic agents inhemodialysis results from the DOPPSrdquo Kidney Internationalvol 84 pp 600ndash608 2013
[30] M Monge I Vaida S S Modeliar et al ldquoRetroperitonealhematoma compressing a single functioning kidney an unusualcause of obstructive renal failurerdquo Clinical Nephrology vol 67no 5 pp 318ndash320 2007
[31] M Dugo E la Torre F Farneti et al ldquoA case of intrarenalhematoma role of ultrasonography in the early diagnosisof possible complication of anticoagulant therapyrdquo GiornaleItaliano di Nefrologia vol 29 pp 616ndash620 2012
[32] httpwwwaccessdatafdagovdrugsatfda docslabel2011009218s107lblpdf
[33] D P Tveit I O Hypolite P Hshieh et al ldquoChronic dialysispatients have high risk for pulmonary embolismrdquo AmericanJournal of Kidney Diseases vol 39 no 5 pp 1011ndash1017 2002
[34] C Kearon S R Kahn G Agnelli S Goldhaber G E RaskobandA J Comerota ldquoAntithrombotic therapy for venous throm-boembolic disease American College of Chest Physiciansevidence-based clinical practice guidelines (8th edition)rdquoChestvol 133 no 6 pp 454Sndash545S 2008
[35] H Decousus A Leizerovicz F Parent et al ldquoA clinical trialof vena cava filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave StudyGrouprdquoTheNew England Journal ofMedicine vol 338 pp 409ndash415 1998
[36] F Knoll G Sturm C Lamina et al ldquoCoumarins and survival inincident dialysis patientsrdquo Nephrology Dialysis Transplantationvol 27 no 1 pp 332ndash337 2012
[37] K E Chan J Michael Lazarus R Thadhani and R MHakim ldquoWarfarin use associates with increased risk for strokein hemodialysis patients with atrial fibrillationrdquo Journal of theAmerican Society of Nephrology vol 20 no 10 pp 2223ndash22332009
[38] V T L Wizemann S Satayathum A Disney et al ldquoAtrialfibrillation in hemodialysis patients clinical features and asso-ciations with anticoagulant therapyrdquo Kidney International vol77 no 12 pp 1098ndash1106 2010
[39] K E Chan J M Lazarus R Thadhani and R M HakimldquoAnticoagulant and antiplatelet usage associates with mortalityamong hemodialysis patientsrdquo Journal of the American Societyof Nephrology vol 20 no 4 pp 872ndash881 2009
[40] J A Chazan M R London and L M Pomo ldquoLong-termsurvival of vascular accesses in a large chronic hemodialysispopulationrdquo Nephron vol 69 no 3 pp 228ndash233 1995
[41] D N Churchill D W Taylor R J Cook et al ldquoCanadianhemodialysis morbidity studyrdquo American Journal of KidneyDiseases vol 19 no 3 pp 214ndash234 1992
[42] M Zellweger J Bouchard S Raymond-Carrier A Laforest-Renald S Querin and F Madore ldquoSystemic anticoagulationand prevention of hemodialysis catheter malfunctionrdquo Amer-ican Society for Artificial Internal Organs Journal vol 51 no 4pp 360ndash365 2005
[43] L Colı G Donati G Cianciolo et al ldquoAnticoagulation therapyfor the prevention of hemodialysis tunneled cuffed catheter(TCC) thrombosisrdquo Journal of Vascular Access vol 7 no 3 pp118ndash122 2006
[44] C I Obialo A C Conner and L F Lebon ldquoMaintainingpatency of tunneled hemodialysis cathetersmdashefficacy of aspirincompared to warfarinrdquo Scandinavian Journal of Urology andNephrology vol 37 no 2 pp 172ndash176 2003
[45] M Cozzolino and V Brandenburg ldquoWarfarin to use or not touse in chronic kidney disease patientsrdquo Journal of Nephrologyvol 23 no 6 pp 648ndash652 2010
[46] L Friberg and L Bergfeldt ldquoAtrial fibrillation prevalence revis-itedrdquo Journal of Internal Medicine vol 274 no 5 pp 461ndash4682013
[47] I Atar D Konas S Acikel et al ldquoFrequency of atrial fibrillationand factors related to its development in dialysis patientsrdquoInternational Journal of Cardiology vol 106 pp 47ndash51 2006
[48] E Vazquez C Sanchez-Perales F Borrego et al ldquoInfluenceof atrial fibrillation on the morbido-mortality of patients onhemodialysisrdquo American Heart Journal vol 140 no 6 pp 886ndash890 2000
[49] S A Lubitz C Moser L Sullivan et al ldquoAtrial fibrillationpatterns and risks of subsequent stroke heart failure or deathin the communityrdquo Journal of the American Heart Associationvol 2 Article ID e000126 2013
[50] U S Renal DATA System USRDS 200520062007 AnnualData Report Atlas of End-Stage Renal Disease in the UnitedStates Bethesda National Institutes of Health NationalInstitute of Diabetes and Digestive and Kidney Diseaseshttpwwwusrdsorgarchiveaspx
[51] S Genovesi A Vincenti E Rossi et al ldquoAtrial fibrillation andmorbidity and mortality in a cohort of long-term hemodialysispatientsrdquoAmerican Journal of Kidney Diseases vol 51 no 2 pp255ndash262 2008
[52] J Olesen G Lip A L Kamper et al ldquoStroke and bleeding inatrial fibrillation with chronic kidney diseaserdquoTheNewEnglandJournal of Medicine vol 367 pp 625ndash635 2012
[53] W C Winkelmayer J Liu S Setoguchi and N K ChoudhryldquoEffectiveness and safety of warfarin initiation in olderhemodialysis patients with incident atrial fibrillationrdquo ClinicalJournal of the American Society of Nephrology vol 6 no 11 pp2662ndash2668 2011
[54] M J Elliott D Zimmerman and R M Holden ldquoWarfarinanticoagulation in hemodialysis patients a systematic review ofbleeding ratesrdquoAmerican Journal of Kidney Diseases vol 50 no3 pp 433ndash440 2007
The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 The Scientific World Journal
Table 1 Factors conducive to coagulation disorders in patients with end-stage renal disease and receiving haemodialysis [8ndash13]
Factors conducive to bleeding events Factors conducive to thrombosisDirectlyPlatelet adhesion disordersmdashdecreased activity of von Willebrandfactor and receptor GPIb increased release of PGI2 NOPlatelet aggregation disordersmdashdecreased activity of GPIIbIIIareceptor impaired binding of fibrinogen to plateletsPlatelet secretion disordersmdashdecreased production of thromboxaneA2 serotonin and ADP decreased release of 120573-thromboglobulinand impaired Ca++ mobilizationReduced number and volume of platelets
Accelerated atherosclerotic processes damaged endotheliumDefective GPIb expression on the surface of plateletsDisorders of protein C metabolism decreased concentration ofprotein C and antithrombin IIIElevated concentrations of plasminogen activator inhibitor-1(PAI-1)
IndirectlyAnaemiamdashaltered rheological features of blood impaired plateletaggregationUraemic toxinsmdashfor example PTHMedicationsmdashantiplatelet anticoagulant cephalosporinsantitubercular inhibitors of lipid absorption NSAIDsConcomitant diseasesmdashfor example affecting the gastrointestinaltractInvasive proceduresmdashcannulations biopsies vascular accessGP glycoprotein PGI2 prostacyclin NO nitric oxide ADP adenosine diphosphate Ca calcium ions PTH parathormone NSAIDs non-steroidal anti-inflammatory drugs
haemodialysis [6] The continuously growing population ofpatients receiving haemodialysis as a result of the increas-ing prevalence of the aforementioned lifestyle diseases orsocial and demographic factors associated with them hasan undoubted impact on this fact Attempts to find newapplications for OACs in this group of patients are howevernot less important Although they are based on a number ofprospective randomised studies in the general populationthere are no such studies in the group of patients receivinghaemodialysis [7] Attempts to apply the results of studiescarried out in the general population from which patientswith end-stage renal failure are usually excluded to beginwith to patients receiving haemodialysis are not only unjusti-fied but sometimes have downright negative influence on theeffectiveness of treatment and patientsrsquo safety
2 Chronic Kidney Disease andHaemostasis Disorders
As renal failure progresses increasingly significant distur-bances occur in the process of blood coagulation At the ini-tial stages ofCKDmostly as a result of disorders of the plasmacoagulation system and fibrinolysis (eg decreased levelsof protein C and antithrombin III elevated concentrationsof fibrinogen von Willebrand factor factor VIII elevatedconcentration of plasminogen activator inhibitor-1 (PAI-1)decreased concentration of tissue plasminogen activator (t-PA)) prothrombotic processes clinically expressed as hyper-coagulation dominate [8 9] As glomerular filtration rate(GFR) decreases and renal failure progresses uraemic bleed-ing diathesis characteristic of end-stage renal failure andpatients during dialysis therapy worsens At the end stages ofCKD the accumulating uraemic toxins both low-molecular-weight (eg urea phenol and guanidinosuccinic acid) andmedium-molecular-weight ones (eg RGD polypeptides)
affect mostly platelet function inhibiting their adhesionand aggregation and releasing platelet factors such as sero-tonin or thromboxane A
2[10 11] These phenomena mostly
lead to platelet haemostasis disorders Uraemic toxins andproinflammatory cytokines frequently co-occurring lipiddisorders or arterial hypertension damage endothelium andin this way disrupt also vascular haemostasis As a result oftheir stimulation endothelial cells produce large amounts ofprostacyclin (PGI
2) and nitric oxide (NO) [12] The former
is a strong inhibitor of platelet aggregation and the latter ofplatelet adhesion Their elevated concentrations thereforeincrease the existing haemorrhagic diathesis
A clear bleeding tendency does not exclude of coursea simultaneous state of increased prothrombotic suscepti-bility even in the same patient The peculiar competitionbetween these two antagonistic systems is presented inTable 1 which includes factors that occur as renal failureprogresses predisposing the patient to bleeding events andon the other hand to the formation of thrombi [13] Thefactors conducive to bleeding mentioned in the table as wecan see mostly disrupt platelet haemostasis they disruptvascular haemostasis to a lesser extent mainly those thatdo not take part in the process of coagulation directlyOn the other hand prothrombotic factors include apartfrom those affecting plasma haemostasis first and foremostthe state of endothelium and accelerated atheroscleroticprocesses inextricably linked with end-stage renal failure[14] Most frequently this dynamic equilibrium is slightlyshifted towards haemorrhagic diathesis which is suggestedby the clinical characteristics of the haemodialysed patientthe results of his or her additional tests usually increasedbleeding time with usually normal APTT and INR Thisstate of equilibrium is however extremely unstable and theslightest additional factor affecting the processes of bloodcoagulationfibrinolysis shifts it to either of the sides
The Scientific World Journal 3
3 Chronic Kidney Disease andOral Anticoagulant Treatment
The applied medications are a factor which frequently andsignificantly disturbs the above-described equilibrium Vita-min K antagonists are still the most commonly used oralanticoagulant medications (incidentally the erroneous nameldquoantagonistsrdquo has been adopted though they do not haveantagonist effects on vitaminK only inhibitory ones so to beprecise they are its inhibitors) The first medicine from thisgroup was dicoumarol isolated by Karl Link at the Universityof Wisconsin in 1941 [15] However they really started tobe commonly used in 1950 when a more effective andbioavailable medicine was introducedmdashwarfarin [16] Theirmechanism of action consists in inhibiting the activity of thevitaminK reductase complex whichmakes the carboxylationof the residues of glutamic acid in the N-terminal fragmentsof different proteins impossible This way the activity offour key factors of the blood coagulation system factorsII VII IX X is inhibited [17] It is a strong anticoagulantactivity because key factors both to the auxiliary endogenouspathway and first and foremost to the exogenous pathwayfundamental to the coagulation system are inhibited Attherapeutic doses the inhibition of the aforementioned coag-ulation factors should range from 30 to 50 [18] This verynarrow therapeutic window can on the one hand result inthe ineffectiveness of treatment and on the other in frequentserious adverse reactions mostly severe bleeding eventsOACs in the blood strongly bind to albumins but the activefree fraction fluctuates in a fairly wide range (from 05 to 3)[19] Elimination occurs via hepatic metabolism by variouscytochromes for each of the isomers of the active ingredientof the medicine its inactive metabolites are excreted by thekidneys [20]The half-life is from 18 to 70 hours [21] It wouldseem that the hepatic metabolism of coumarin derivativesjustifies the use of these medications in patients with end-stage renal failure and receiving haemodialysis following thesame rules and at the same doses as in the general pop-ulation However the above-described pharmacodynamicand pharmacokinetic properties make treatment with OACsin patients receiving haemodialysis extremely difficult Thetherapeutic window becomes even narrower the concen-trations of the free fraction of the medicine fluctuate evenmore depending on changes in peridialytic volaemia and theamount of fraction bound to albumins decreases as a resultof malnutrition or patient cachexia [22] Moreover thereare a number of known nutritional limitations associatedwith using OACs restrictions in the treatment of elderlyindividuals (slower hepatic metabolism) or their numerousinteractions with other medicines (especially antiplateletones) [23] In the conditions of advanced CKD the impactof all these factors is much greater [24]
Maruyama et al [25] evaluating INR and albumin valuesbefore and after HD procedures demonstrated a significantdecrease in the value of INR following HD in comparisonwith its levels determined prior to HD while albumin con-centrations increased significantly following the procedure inrelation to values prior to dialysis What is more the authorsalso showed a significant negative correlation between both
of the above-described parameters during haemodialysisAbe et al [26] apart from similar changes regarding INRand proteins during HD demonstrated a significant risein warfarin concentrations post-HD versus pre-HD bothwith respect to the more potent S-isomer and the weakerR-isomer Interestingly multifactorial analysis revealed thestrongest links between peridialytic values of INR and albu-min concentrations The ability of blood proteins especiallyalbumin to bind warfarin is very strong and thereforechanges in their concentration duringHD result in significantchanges in the concentrations of the active ingredient of themedicine INR and consequently treatment complicationsIn a retrospective study of 142 haemodialysed patients whoreceived acenocoumarol for typical indications at a dose of1mg a day for a year Gompou et al [27] demonstratedthat 30 of the INR values determined at this time werebelow target values 37 were in the therapeutic range andnearly 33 exceeded therapeutic values Admittedly thereis no information regarding the severe complications ofsuch treatment in the report but the fact that OACs wereoverdosed in 13 of the cases seems alarming
So far among patients with end-stage renal failure andpatients receiving haemodialysis no prospective randomisedstudies evaluating the effectiveness and safety of OACs havebeen conducted In spite of that in this group of patientsthese medications are attempted to be used according to theirtypical indications taking however special precautions inusing them due to the considerably increased risk of adversereactions [28] Indeed the literature includes a number ofreports of such reactions including very severe and fatalones [29ndash31] It is also interesting to read the official con-traindications for the use of OACs approved in registrationdocuments by regulatory bodies authorised to do that [32](eg the FDA) (Table 2) On the list presented in Table 2almost every other item (eg 1 3 5 7 and the last one) refersto patients with end-stage renal failure including patientsreceiving haemodialysis Admittedly chronic renal failure isnot explicitly listed but the items enumerated above referdirectly to it In any case most of them overlap with factorspredisposing to bleeding events in patients with end-stagerenal failure and receiving haemodialysis as described earlier(Table 1) As we can see platelet function disorders otherthrombocytopathies the risk of gastrointestinal bleedingurinary tract bleeding falls or lack of adequate collaborationin this specific treatment are especially significant in thisrespect After all it is a picture of patients that we see innephrology units or at dialysis centres on a daily basis Istherefore OAC treatment according to its typical indica-tions in patients with end-stage CKD or in those receivinghaemodialysis an off-label use an experimental one andtherefore is it justified these questions remain open
4 OACs in Patients with End-Stage RenalDisease in Clinical Practice
Attempts to use OACs in patients at the end stages of CKDand receiving haemodialysis encounter a number of diffi-culties Practically all prospective controlled randomised
4 The Scientific World Journal
Table 2 Contraindications for the use of oral anticoagulants [32]
(i) Increased risk of bleeding eventsmdashplatelet function disorders thrombocytopenia vonWillebrand disease and haemophilia(ii) Recent intracranial bleeding Conditions predisposing to intracranial bleedingmdashcerebral artery aneurysms(iii) Conditions predisposing to gastrointestinal urinary and respiratory tract bleeding(iv) Surgical procedures within the central nervous system or the eye(v) Increased risk of frequent fallsmdashcaused by a neurological or another condition(vi) Severe liver failure cirrhosis(vii) Untreated or poorly controlled arterial hypertension(viii) Pregnancy(ix) Infective endocarditis or pericardial effusion(x) Hypersensitivity to the active substance or any of the excipients(xi)Dementia psychoses alcoholism and other conditions in which compliance may not be satisfactory andwhen anticoagulant treatment cannot be safely administeredEnd-stage renal-disease-associated items are bold
studies which evaluated the effectiveness and safety of OACsin the general population carried out so far excluded patientswith creatinine clearance lt30mLmin Applying the resultsof these studies to the population with advanced renal failureshould not therefore be automatic because their simple usenot only may prove to be ineffective in this group of patientsbut what is worse may be dangerous to them as well
41 OACs in the Treatment of Venous Thromboembolism inPatients with CKD The prevalence of pulmonary embolismin the population of patients receiving haemodialysis isseveral times higher than its prevalence in the generalpopulation The annual incidence of pulmonary embolismin this group of patients is approximately 15100000 versus25100000 patients in the general population [33] Howeverthere are no evidence-based studies evaluating the use ofOACs in this disease and in this population The remainingoption therefore is beginning treatment with unfractionatedheparin usually on an inpatient basis then changing it overthe next several days and continuing the OAC treatmentwhile monitoring INR which is the treatment acceptedgenerally for the population without renal failure [34] Dueto the lack of relevant research the length of therapy depend-ing on the aetiology of the disease the individual risk ofthrombosisbleeding events for a given patient and often thedecision of the patient him- or herself regarding the appliedOAC treatment remain to be evaluated In the case of absolutecontraindications for OACs implantation of a filter in theinferior vena cava could be an alternative therapy but thereare no such studies for patients receiving haemodialysis inthe available literature and they are inconclusive even in thegeneral population [35]
42 OACs in Preventing Thrombosis of Vascular Access forHaemodialysis It is estimated that the causes of almost 13of cases requiring hospitalisation among patients receivinghaemodialysis are associatedwith vascular access failure [40]The likelihood of the occurrence of vascular access failuredue to thrombosis in over a year-long observation of patientsreceiving haemodialysis is approximately 15 in the case of
autologous arteriovenous fistulae and two times higher in thecase of vascular grafts [41] It would therefore seem thatOACscan be an effective treatment option in reducing this risk
Several such prospective controlled studies (some ofwhich were even randomised) have been conducted thoughon small groups of patients Their results however proved tonot be very encouraging In a group of 75 patients receivinghaemodialysis OAC treatment whose therapeutic target wasINR 15ndash20 was found to be only slightly more effective inthe prevention of thrombotic complications in comparisonwith the control group in which OAC treatment was notinitiated (66 versus 57) but the recorded difference wasnot statistically significant [42] What is more in spite ofthe unchanging study protocol the target INR values wereachieved in only a half of the subjects While serious bleedingevents were not recorded the target INR range was not highIn another randomised study on a group of 144 patientsreceiving haemodialysis Colı et al [43] used OACs with alittle higher therapeutic range of INR (18ndash25) Statisticallysignificant differences between the study group and thecontrol group not treated with OACs were observed onlyafter taking the time at which OAC treatment was initiatedinto consideration In the group in which this treatmentwas initiated in the first 24 hours after the implantation ofa vascular catheter vascular complications were found in alittle more than 10 of patients in comparison with patientswho received OACs after their first thrombotic event wherethe proportion of complications was a little over 50 Inanother study carried out on a group of 63 patients receivinghaemodialysis the use of OACs whose therapeutic aim wasINR of 20-30 was proved to be significantly more effectivein preventing thrombosis than in the group of patients notreceiving such treatment [44] However when the resultsof the group treated with OACs were compared with thegroup in which acetylsalicylic acid at a dose of 325mgdaywas used differences in the effectiveness regarding vascu-lar access thrombosis were not observed Serious bleedingevents which significantly more frequently occurred in thegroup receiving OACs were the only significant differencebetween these groups
The Scientific World Journal 5
Table 3 Mortality risk in haemodialysis patients with atrial fibrillation treated with warfarin
Study Population (119899) Period (y) Mortality (HR)Knoll et al [36] 119899mdash235 pts 3 years HRmdash080 (95 CI 028ndash229 119875 lt 067)Chan et al [37] 119899mdash1671 pts 1 year HRmdash110 (094ndash130)
Wizemann et al [38] 119899mdash17513 pts(AFmdash125) 7 years
All ages HRmdash116 (95 CI 108ndash125 119875 lt 0001)Age lt 65 HRmdash129 (95 CI 045ndash368 119875 lt 063)Age 65ndash75 HRmdash135 (95 CI 069ndash263 119875 lt 039)Age gt 75 HRmdash217 (95 CI 104ndash453 119875 lt 004)
Chan et al [39]
119899mdash41425 pts
11 yearsWarfarinmdash83 HRmdash173 (95 CI 162ndash185)Clopidogrelmdash10 HRmdash150 (95 CI 139ndash162)Acetylsalicylicacidmdash304 HRmdash117 (95 CI 112ndash122)
Acetylsalicylic acidand warfarinmdash8 HRmdash111 (95 CI 103ndash186)
HR hazard ratio CI confidence interval 119899 number of patients
How effective is therefore the application of OACs inthis group of patients As the few not very reliable studiessuggest it admittedly increaseswith the increase in the targetINR but at the price of significant adverse reactions in theform of serious bleeding events Moreover in the last ofthe cited studies which confirmed such effectiveness similareffectiveness was recorded with the use of acetylsalicylic acidwithout severe complicationsThe results of the above studiesand the opinions of experts in the area do not allow thereforea routine use of OACs due to the discussed indications [45]This is because a target safe INR range for this group ofpatients has not been established the effectiveness of themedications is doubtful and the risk for the patient is highfurthermore there are alternative methods that are no lesseffective and as it appears are safer [44]
43 OACs in the Prevention ofThromboembolic ComplicationsAssociated with Atrial Fibrillation Atrial fibrillation (AF) isthe most common cardiac dysrhythmia It is estimated that itaffects several percent of the population over the age of 65 andthe proportion increases with age [46] However in the groupof patients with end-stage renal failure this proportion ismuch higher and reaches according to various studies from10 to as high as 30 [47] The annual mortality rate amongthese patients is approximately 25 in the general populationand almost 30 in patients receiving haemodialysis [48]Theprevalence of stroke in patients with atrial fibrillationwithoutrenal failure is on the other hand close to that in patientsreceiving haemodialysis (17 versus 15 resp) [49 50]Similarly studies evaluating the risk of stroke among patientsreceiving haemodialysis depending on the presence of AF orsinus rhythm are inconclusive Some of them show a several-fold increase in the incidence of stroke in the group with AFwhile others do not record such a correlation [50 51] Thesetwo factors among other things are probably responsible forthe inconclusive results of studies evaluating the effectivenessand safety of OAC treatment due to AF in the group ofpatients with end-stage renal failure and patients receiving
haemodialysis The confusion in the literature regardingthe plausibility and significance of the discussed issue isincreased however mostly by the fact that there are simplyno prospective controlled randomised studies in this group
First let us look at the impact of the use of OACs in thisgroup of patients on the hard end-point which is patientmortality (Table 3) Knoll et al [36] carrying out a studyon a group of 235 haemodialysed patients with AF receivingOACs recorded a slightly lower mortality rate than thatwhich characterised the control group not receiving OACsalthough not significant Chan et al [37] in a retrospectivestudy conducted on more than 1600 patients with AFreceiving haemodialysis showed that the use of warfarin inthe prevention of thromboembolic events is not associatedwith all-cause mortality or an increase in the number ofhospitalisations In turn Wizemann et al [38] observed aclear increase in mortality rate in patients receiving warfarinfor the same reasons as in haemodialysed ones which wasespecially apparent in the older population (gt75 years old)Another study confirmed the negative impact of OACs usedfor the same indications on themortality rate in patients withend-stage renal failure in comparison with the control groupwhich did not receive such treatment [39]
Data regarding effectiveness in decreasing the risk ofstroke in patients with AF receiving haemodialysis are alsoinconclusive In one of the latest of such studies Olesenet al [52] in a group of more than 900 patients in whomwarfarin was used in fewer than 20 of cases observed for aperiod of 11 years and found a statistically significant decreasein the risk of the occurrence of stroke or another systemicthromboembolic event However in several other studiessuch an effect was not observed what is more the effect ofusing OACs was decidedly negative In the study cited aboveChan et al [37] recorded a two times higher risk of strokein the group treated with warfarin than in the control groupnot receiving OACs Furthermore there was an increase inthe risk of both haemorrhagic and ischaemic stroke (HR 22and 18 resp) Similar results were presented by Wizemann
6 The Scientific World Journal
et al [38] in a group of 3245 patients participating inDOPPS I and DOPPS II (Dialysis Outcomes and PracticePatterns Study) In this study the patientsrsquo age was the factordifferentiating the risk In the oldest group (gt75 years old)warfarin treatment was associated with a significant morethan twofold increase in the risk of stroke in younger groups(65ndash75 and lt65) the increase in the risk of stroke wasevident but statistically insignificant In another study whichcovered 2313 haemodialysed patients with newly diagnosedAF and treated with warfarin for the first time Winkelmayeret al [53] observed an over twofold increase in the risk ofhaemorrhagic stroke such a relationshipwas not found in thecase of ischaemic stroke
The risk of adverse reactions including severe bleed-ing events during OAC treatment in patients receivinghaemodialysis rises considerably Previous studies in whichOACs were used for different indications had alreadyreported that [54] In the case of the treatment of AF thesituation looks similar most reports suggest a several-foldincrease in this risk The results of the study by Chan etal [39] suggest a significant almost threefold increase inthe risk of severe bleeding events during OAC treatmentin haemodialysed patients due to AF In the same studyclopidogrel was associated with a more than 25-fold (higher)risk of significant haemorrhagic complications what is inter-esting is that the use of acetylsalicylic acid also increasedthis risk but not significantly Holden et al [55] in turnobserved an increase in such risk which was more thanthreefold in the case of warfarin and over fourfold in thecase of acetylsalicylic acid the use of these medications incombinationwas associated withmore than a sixfold increasein this risk Other studies also suggested a significant risk ofsevere bleeding events associated with the use of OACs inthe prevention of thromboembolic complications due to AF[52 56]
Is therefore OAC treatment for the above indications inpatients receiving haemodialysis effective and safe Do thebenefits of using OACs outweigh the risk of severe bleedingevents in patients with end-stage renal failure
All of the above study results should be treated cautiouslyAs we have mentioned there are no large-scale controlledprospective randomised studies here Only on the basis ofsuch studies would it be possible to present guidelines orrecommendations regarding OAC treatment in this groupof patients Most of them are studies conducted on smallgroups observational retrospective groups only a few ofthemwere prospective but not randomised It is also difficultto perform a reliable meta-analysis because the individualstudies sometimes differ in their design specific assumptionsmethods of collecting data ormethods of analysis [37 38 53]Decisions regarding the initiation of OAC treatment andthe time when it occurred depended mostly on the patientrsquosclinical data and the physicianrsquos experience Some studies alsoexcluded patients taking OACs or patients with AF that haddeveloped before renal failure All these circumstances makeit necessary to evaluate these studies cautiously
Moreover let us look at two epidemiological issues [49ndash51]The prevalence of stroke in patients with atrial fibrillationwithout renal failure in comparison with that in patients
receiving haemodialysis turned out to be comparable in theabove-cited studies However the evaluation of the risk ofstroke in patients receiving haemodialysis depending on thepresence of AF or sinus rhythm proved to be inconclusive Iftherefore there is no such risk what role are OACs supposedto play Perhaps a significant portion of the causes of strokein the group with end-stage renal failure are vascular onesand atherosclerosis considerably accelerated in this group ofpatients In this situation OACs would not change such risksignificantly
In turn the increase in the risk of death and the increasein the incidence of stroke in haemodialysed patients treatedwith OACs may be explained by two things The first oneis of course inappropriate management of anticoagulationor rather the time during which the patient remains in thedesired INR range After all its deviation towards higher orlower values is associated with an increase in morbidity oradverse reactions On a daily basis in nephrology units ordialysis centres we can see how difficult it is to keep INR insuch a therapeutic range in patients receiving haemodialysisIt is associated with the fact that chronic renal failureand haemodialysis therapy to an even larger extent are asignificant and independent factors that may decrease theperiod in which the desired value of INR is maintained [57]Anyway the above-cited data regarding the increase in therisk of bleeding events during OAC treatment in patientsreceiving haemodialysis most likely result from the samecause The described impact of vitamin K antagonists onthe processes of vascular calcification and calciphylaxis isanother noteworthy potential factor As a number of studiesboth experimental and clinical show vitamin K inhibitionfor example by OACs inhibits the activity of matrix Glaprotein (MGP) an important protein playing a preventiverole in vascular calcification [58 59] OACs can thereforedirectly interfere and accelerate the process of vascularcalcification already increased in end-stage renal failureIs it a causative factor significantly raising the incidenceof ischaemic stroke and mortality among haemodialysedpatients receiving OACsThis question must be answered byfuture studies
Patients with end-stage renal failure including above allthose who receive haemodialysis are a group of patients withexceptionally many concomitant diseases [60] Considerablyaccelerated atherosclerotic processes vascular calcificationchronic inflammation lipid disorders and malnutrition areinherent characteristics of this population of patients CanOACs have an impact on the risk of stroke in haemodialysedpatients with AF in these conditions and with the existingvascular changes also within the central nervous systemmdashthis Question remains open However the results of the citedstudies do not allow us to use OACs routinely for theseindications in this group of patients
5 Conclusions
The population of patients with CKD including patientsreceiving haemodialysis keeps growing all over the world
The Scientific World Journal 7
Table 4 Potential indications for oral anticoagulants in patientswith end-stage renal disease and receiving haemodialysis
(i) Status after prosthetic heart valve implantation(ii) Antiphospholipid syndrome(iii) Secondary prevention of severe thromboembolic events (forexample pulmonary embolism)(iv) Atrial fibrillation with a high risk of stroke
However OAC treatment in this group of patients irrespec-tive of its indications causes a great deal of controversy Thisis because a number of pro- and anticoagulant factors playan important role in end-stage renal failure due to the natureof the disease itself In these conditions the pharmacokineticand especially pharmacodynamic properties of the OACsused change as well All these factors make proper anticoagu-lation in these patients more difficult and most importantlythey decrease the time during which patients remain inthe therapeutic range of INR In the case of the treatmentof venous thromboembolism the only remaining option isOAC treatment according to regimens used for the generalpopulation as there are no relevant studies concerning thegroup of patients receiving haemodialysis Prevention of HDvascular access thrombosis with the use of OACs accordingto the presented studies and expertsrsquo opinions is not veryeffective and can additionally be very dangerous HoweverOAC treatment in haemodialysed patientswithAF in order toprevent thromboembolic events according to some authorsis associated with an increase in the incidence of stroke andmortality
Is the provocative question included in the title justifiedDoubts should be dispelled by prospective controlled ran-domised studies at the moment there is no justification forroutine use of OACs in the above-mentioned indications Inselected cases of OAC treatment in this group of patients it isabsolutely necessary to control andmonitor the applied treat-ment thoroughly According to the authors and the opinionsalready partially reported in the literature [45] indicationsfor the use of OACs in patients with end-stage renal failureincluding patients receiving haemodialysis should be limitedto those included in Table 4
References
[1] S I Hallan J Coresh B C Astor et al ldquoInternational compari-son of the relationship of chronic kidney disease prevalence andESRD riskrdquo Journal of the American Society of Nephrology vol17 no 8 pp 2275ndash2284 2006
[2] B Rutkowski ldquoChanging pattern of end-stage renal disease incentral and eastern Europerdquo Nephrology Dialysis Transplanta-tion vol 15 no 2 pp 156ndash160 2000
[3] J J Snyder R N Foley and A J Collins ldquoPrevalence of CKDin the United States a sensitivity analysis using the NationalHealth and Nutrition Examination Survey (NHANES) 1999ndash2004rdquo American Journal of Kidney Diseases vol 53 no 2 pp218ndash228 2009
[4] E Krol B Rutkowski P Czarniak et al ldquoEarly detection ofchronic kidney disease results of the PolNef studyrdquo AmericanJournal of Nephrology vol 29 no 3 pp 264ndash273 2009
[5] S Ghanny and M Crowther ldquoTreatment with novel oralanticoagulants indications efficacy and risksrdquo Current Opinionin Hematology vol 20 pp 430ndash436 2013
[6] T Kruger V Brandenburg G Schlieper et al ldquoSailing betweenScylla andCharybdis oral long-term anticoagulation in dialysispatientsrdquo Nephrology Dialysis Transplantation vol 28 pp 534ndash541 2013
[7] S Genovesi and A Santoro ldquoAnticoagulants renal failure andatrial fibrillationrdquo Expert Opinion on Drug Safety vol 12 pp 1ndash3 2013
[8] N Leung ldquoHematologic manifestations of kidney diseaserdquoSeminars in Hematology vol 50 pp 207ndash215 2013
[9] J A Milburn K Cassar I Ford N Fluck and J BrittendenldquoProthrombotic changes in platelet endothelial and coagulationfunction following hemodialysisrdquo International Journal of Arti-ficial Organs vol 34 no 3 pp 280ndash287 2011
[10] D I Jalal M Chonchol andG Targher ldquoDisorders of hemosta-sis associated with chronic kidney diseaserdquo Seminars inThrom-bosis and Hemostasis vol 36 no 1 pp 34ndash40 2010
[11] D Kaw and D Malhotra ldquoPlatelet dysfunction and end-stagerenal diseaserdquo Seminars in Dialysis vol 19 no 4 pp 317ndash3222006
[12] M A de Sa Siqueira T M C Brunini N R Pereira et alldquoIncreased nitric oxide production in platelets from severechronic renal failure patientsrdquo Canadian Journal of Physiologyand Pharmacology vol 89 no 2 pp 97ndash102 2011
[13] P Boccardo G Remuzzi and M Galbusera ldquoPlatelet dysfunc-tion in renal failurerdquo Seminars in Thrombosis and Hemostasisvol 30 no 5 pp 579ndash589 2004
[14] A S Gangji A S Sohal D Treleaven and M A CrowtherldquoBleeding in patients with renal insufficiency a practical guideto clinicalmanagementrdquoThrombosis Research vol 118 no 3 pp423ndash428 2006
[15] J C McCarter J B Bingham and O O Meyer ldquoStudies on thehemorrhagic agent 3 31015840-methylenebis (4-Hydroxycoumarin)IV The pathologic findings after the administration ofdicumarolrdquo The American Journal of Pathology vol 20 pp651ndash659 1944
[16] D V Clatanoff P O Triggs and O O Meyer ldquoClinical expe-rience with coumarin anticoagulants warfarin and warfarinrdquoArchives of Internal Medicine vol 94 no 2 pp 213ndash220 1954
[17] C Becattini M C Vedovati and G Agnelli ldquoOld and neworal anticoagulants for venous thromboembolism and atrialfibrillation a review of the literaturerdquoThrombosis Research vol129 no 3 pp 392ndash400 2012
[18] E A Nutescu ldquoOral anticoagulant therapies balancing therisksrdquoAmerican Journal of Health-System Pharmacy vol 70 no10 supplement 1 pp S3ndashS11 2013
[19] M Zacchigna G di Luca F Cateni and V Maurich ldquoImprove-ment of warfarin biopharmaceutics by conjugation with poly(ethylene glycol)rdquo European Journal of Pharmaceutical Sciencesvol 23 no 4-5 pp 379ndash384 2004
[20] G F Pineo and R D Hull ldquoVitamin K antagonists and directthrombin inhibitors present and futurerdquoHematologyOncologyClinics of North America vol 19 no 1 pp 69ndash85 2005
[21] B F Gage and P E Milligan ldquoPharmacology and pharma-cogenetics of warfarin and other coumarins when used withsupplementsrdquo Thrombosis Research vol 117 no 1-2 pp 55ndash592005
[22] K S Brimble A J Ingram J W Eikelboom et al ldquoAntico-agulants in patients with atrial fibrillation and end-stage renaldiseaserdquo Postgraduate Medicine vol 124 pp 17ndash25 2012
8 The Scientific World Journal
[23] S Benmira Z K Banda and V Bhattacharya ldquoOld versusnew anticoagulants focus on pharmacologyrdquo Recent Patents onCardiovascular Drug Discovery vol 5 no 2 pp 120ndash137 2010
[24] N A Limdi M A Limdi L Cavallari et al ldquoWarfarin dosingin patients with impaired kidney functionrdquoAmerican Journal ofKidney Diseases vol 56 no 5 pp 823ndash831 2010
[25] N Maruyama M Abe K Okada et al ldquoChanges to pro-thrombin international normalized ratio in patients receivinghemodialysisrdquo International Journal of Clinical PharmacologyandTherapeutics vol 51 pp 283ndash287 2013
[26] M Abe N Maruyama H Suzuki et al ldquoInternational nor-malized ratio decreases after hemodialysis treatment in patientstreated with warfarinrdquo Journal of Cardiovascular Pharmacologyvol 60 pp 502ndash507 2012
[27] AGompou I Griveas I Kyritsis I AgroyannisMTsakoniatisand B Agroyannis ldquoINR deviations in hemodialyzed patientsunder low dose oral anticoagulant therapyrdquo International Jour-nal of Artificial Organs vol 32 no 10 pp 752ndash755 2009
[28] J C van Blijderveen K M Verhamme R Zietse et alldquoOveranticoagulation is associated with renal function declinerdquoJournal of Nephrology vol 26 pp 691ndash698 2013
[29] M M Sood M Larkina J R Thumma et al ldquoMajor bleed-ing events and risk stratification of antithrombotic agents inhemodialysis results from the DOPPSrdquo Kidney Internationalvol 84 pp 600ndash608 2013
[30] M Monge I Vaida S S Modeliar et al ldquoRetroperitonealhematoma compressing a single functioning kidney an unusualcause of obstructive renal failurerdquo Clinical Nephrology vol 67no 5 pp 318ndash320 2007
[31] M Dugo E la Torre F Farneti et al ldquoA case of intrarenalhematoma role of ultrasonography in the early diagnosisof possible complication of anticoagulant therapyrdquo GiornaleItaliano di Nefrologia vol 29 pp 616ndash620 2012
[32] httpwwwaccessdatafdagovdrugsatfda docslabel2011009218s107lblpdf
[33] D P Tveit I O Hypolite P Hshieh et al ldquoChronic dialysispatients have high risk for pulmonary embolismrdquo AmericanJournal of Kidney Diseases vol 39 no 5 pp 1011ndash1017 2002
[34] C Kearon S R Kahn G Agnelli S Goldhaber G E RaskobandA J Comerota ldquoAntithrombotic therapy for venous throm-boembolic disease American College of Chest Physiciansevidence-based clinical practice guidelines (8th edition)rdquoChestvol 133 no 6 pp 454Sndash545S 2008
[35] H Decousus A Leizerovicz F Parent et al ldquoA clinical trialof vena cava filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave StudyGrouprdquoTheNew England Journal ofMedicine vol 338 pp 409ndash415 1998
[36] F Knoll G Sturm C Lamina et al ldquoCoumarins and survival inincident dialysis patientsrdquo Nephrology Dialysis Transplantationvol 27 no 1 pp 332ndash337 2012
[37] K E Chan J Michael Lazarus R Thadhani and R MHakim ldquoWarfarin use associates with increased risk for strokein hemodialysis patients with atrial fibrillationrdquo Journal of theAmerican Society of Nephrology vol 20 no 10 pp 2223ndash22332009
[38] V T L Wizemann S Satayathum A Disney et al ldquoAtrialfibrillation in hemodialysis patients clinical features and asso-ciations with anticoagulant therapyrdquo Kidney International vol77 no 12 pp 1098ndash1106 2010
[39] K E Chan J M Lazarus R Thadhani and R M HakimldquoAnticoagulant and antiplatelet usage associates with mortalityamong hemodialysis patientsrdquo Journal of the American Societyof Nephrology vol 20 no 4 pp 872ndash881 2009
[40] J A Chazan M R London and L M Pomo ldquoLong-termsurvival of vascular accesses in a large chronic hemodialysispopulationrdquo Nephron vol 69 no 3 pp 228ndash233 1995
[41] D N Churchill D W Taylor R J Cook et al ldquoCanadianhemodialysis morbidity studyrdquo American Journal of KidneyDiseases vol 19 no 3 pp 214ndash234 1992
[42] M Zellweger J Bouchard S Raymond-Carrier A Laforest-Renald S Querin and F Madore ldquoSystemic anticoagulationand prevention of hemodialysis catheter malfunctionrdquo Amer-ican Society for Artificial Internal Organs Journal vol 51 no 4pp 360ndash365 2005
[43] L Colı G Donati G Cianciolo et al ldquoAnticoagulation therapyfor the prevention of hemodialysis tunneled cuffed catheter(TCC) thrombosisrdquo Journal of Vascular Access vol 7 no 3 pp118ndash122 2006
[44] C I Obialo A C Conner and L F Lebon ldquoMaintainingpatency of tunneled hemodialysis cathetersmdashefficacy of aspirincompared to warfarinrdquo Scandinavian Journal of Urology andNephrology vol 37 no 2 pp 172ndash176 2003
[45] M Cozzolino and V Brandenburg ldquoWarfarin to use or not touse in chronic kidney disease patientsrdquo Journal of Nephrologyvol 23 no 6 pp 648ndash652 2010
[46] L Friberg and L Bergfeldt ldquoAtrial fibrillation prevalence revis-itedrdquo Journal of Internal Medicine vol 274 no 5 pp 461ndash4682013
[47] I Atar D Konas S Acikel et al ldquoFrequency of atrial fibrillationand factors related to its development in dialysis patientsrdquoInternational Journal of Cardiology vol 106 pp 47ndash51 2006
[48] E Vazquez C Sanchez-Perales F Borrego et al ldquoInfluenceof atrial fibrillation on the morbido-mortality of patients onhemodialysisrdquo American Heart Journal vol 140 no 6 pp 886ndash890 2000
[49] S A Lubitz C Moser L Sullivan et al ldquoAtrial fibrillationpatterns and risks of subsequent stroke heart failure or deathin the communityrdquo Journal of the American Heart Associationvol 2 Article ID e000126 2013
[50] U S Renal DATA System USRDS 200520062007 AnnualData Report Atlas of End-Stage Renal Disease in the UnitedStates Bethesda National Institutes of Health NationalInstitute of Diabetes and Digestive and Kidney Diseaseshttpwwwusrdsorgarchiveaspx
[51] S Genovesi A Vincenti E Rossi et al ldquoAtrial fibrillation andmorbidity and mortality in a cohort of long-term hemodialysispatientsrdquoAmerican Journal of Kidney Diseases vol 51 no 2 pp255ndash262 2008
[52] J Olesen G Lip A L Kamper et al ldquoStroke and bleeding inatrial fibrillation with chronic kidney diseaserdquoTheNewEnglandJournal of Medicine vol 367 pp 625ndash635 2012
[53] W C Winkelmayer J Liu S Setoguchi and N K ChoudhryldquoEffectiveness and safety of warfarin initiation in olderhemodialysis patients with incident atrial fibrillationrdquo ClinicalJournal of the American Society of Nephrology vol 6 no 11 pp2662ndash2668 2011
[54] M J Elliott D Zimmerman and R M Holden ldquoWarfarinanticoagulation in hemodialysis patients a systematic review ofbleeding ratesrdquoAmerican Journal of Kidney Diseases vol 50 no3 pp 433ndash440 2007
The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

The Scientific World Journal 3
3 Chronic Kidney Disease andOral Anticoagulant Treatment
The applied medications are a factor which frequently andsignificantly disturbs the above-described equilibrium Vita-min K antagonists are still the most commonly used oralanticoagulant medications (incidentally the erroneous nameldquoantagonistsrdquo has been adopted though they do not haveantagonist effects on vitaminK only inhibitory ones so to beprecise they are its inhibitors) The first medicine from thisgroup was dicoumarol isolated by Karl Link at the Universityof Wisconsin in 1941 [15] However they really started tobe commonly used in 1950 when a more effective andbioavailable medicine was introducedmdashwarfarin [16] Theirmechanism of action consists in inhibiting the activity of thevitaminK reductase complex whichmakes the carboxylationof the residues of glutamic acid in the N-terminal fragmentsof different proteins impossible This way the activity offour key factors of the blood coagulation system factorsII VII IX X is inhibited [17] It is a strong anticoagulantactivity because key factors both to the auxiliary endogenouspathway and first and foremost to the exogenous pathwayfundamental to the coagulation system are inhibited Attherapeutic doses the inhibition of the aforementioned coag-ulation factors should range from 30 to 50 [18] This verynarrow therapeutic window can on the one hand result inthe ineffectiveness of treatment and on the other in frequentserious adverse reactions mostly severe bleeding eventsOACs in the blood strongly bind to albumins but the activefree fraction fluctuates in a fairly wide range (from 05 to 3)[19] Elimination occurs via hepatic metabolism by variouscytochromes for each of the isomers of the active ingredientof the medicine its inactive metabolites are excreted by thekidneys [20]The half-life is from 18 to 70 hours [21] It wouldseem that the hepatic metabolism of coumarin derivativesjustifies the use of these medications in patients with end-stage renal failure and receiving haemodialysis following thesame rules and at the same doses as in the general pop-ulation However the above-described pharmacodynamicand pharmacokinetic properties make treatment with OACsin patients receiving haemodialysis extremely difficult Thetherapeutic window becomes even narrower the concen-trations of the free fraction of the medicine fluctuate evenmore depending on changes in peridialytic volaemia and theamount of fraction bound to albumins decreases as a resultof malnutrition or patient cachexia [22] Moreover thereare a number of known nutritional limitations associatedwith using OACs restrictions in the treatment of elderlyindividuals (slower hepatic metabolism) or their numerousinteractions with other medicines (especially antiplateletones) [23] In the conditions of advanced CKD the impactof all these factors is much greater [24]
Maruyama et al [25] evaluating INR and albumin valuesbefore and after HD procedures demonstrated a significantdecrease in the value of INR following HD in comparisonwith its levels determined prior to HD while albumin con-centrations increased significantly following the procedure inrelation to values prior to dialysis What is more the authorsalso showed a significant negative correlation between both
of the above-described parameters during haemodialysisAbe et al [26] apart from similar changes regarding INRand proteins during HD demonstrated a significant risein warfarin concentrations post-HD versus pre-HD bothwith respect to the more potent S-isomer and the weakerR-isomer Interestingly multifactorial analysis revealed thestrongest links between peridialytic values of INR and albu-min concentrations The ability of blood proteins especiallyalbumin to bind warfarin is very strong and thereforechanges in their concentration duringHD result in significantchanges in the concentrations of the active ingredient of themedicine INR and consequently treatment complicationsIn a retrospective study of 142 haemodialysed patients whoreceived acenocoumarol for typical indications at a dose of1mg a day for a year Gompou et al [27] demonstratedthat 30 of the INR values determined at this time werebelow target values 37 were in the therapeutic range andnearly 33 exceeded therapeutic values Admittedly thereis no information regarding the severe complications ofsuch treatment in the report but the fact that OACs wereoverdosed in 13 of the cases seems alarming
So far among patients with end-stage renal failure andpatients receiving haemodialysis no prospective randomisedstudies evaluating the effectiveness and safety of OACs havebeen conducted In spite of that in this group of patientsthese medications are attempted to be used according to theirtypical indications taking however special precautions inusing them due to the considerably increased risk of adversereactions [28] Indeed the literature includes a number ofreports of such reactions including very severe and fatalones [29ndash31] It is also interesting to read the official con-traindications for the use of OACs approved in registrationdocuments by regulatory bodies authorised to do that [32](eg the FDA) (Table 2) On the list presented in Table 2almost every other item (eg 1 3 5 7 and the last one) refersto patients with end-stage renal failure including patientsreceiving haemodialysis Admittedly chronic renal failure isnot explicitly listed but the items enumerated above referdirectly to it In any case most of them overlap with factorspredisposing to bleeding events in patients with end-stagerenal failure and receiving haemodialysis as described earlier(Table 1) As we can see platelet function disorders otherthrombocytopathies the risk of gastrointestinal bleedingurinary tract bleeding falls or lack of adequate collaborationin this specific treatment are especially significant in thisrespect After all it is a picture of patients that we see innephrology units or at dialysis centres on a daily basis Istherefore OAC treatment according to its typical indica-tions in patients with end-stage CKD or in those receivinghaemodialysis an off-label use an experimental one andtherefore is it justified these questions remain open
4 OACs in Patients with End-Stage RenalDisease in Clinical Practice
Attempts to use OACs in patients at the end stages of CKDand receiving haemodialysis encounter a number of diffi-culties Practically all prospective controlled randomised
4 The Scientific World Journal
Table 2 Contraindications for the use of oral anticoagulants [32]
(i) Increased risk of bleeding eventsmdashplatelet function disorders thrombocytopenia vonWillebrand disease and haemophilia(ii) Recent intracranial bleeding Conditions predisposing to intracranial bleedingmdashcerebral artery aneurysms(iii) Conditions predisposing to gastrointestinal urinary and respiratory tract bleeding(iv) Surgical procedures within the central nervous system or the eye(v) Increased risk of frequent fallsmdashcaused by a neurological or another condition(vi) Severe liver failure cirrhosis(vii) Untreated or poorly controlled arterial hypertension(viii) Pregnancy(ix) Infective endocarditis or pericardial effusion(x) Hypersensitivity to the active substance or any of the excipients(xi)Dementia psychoses alcoholism and other conditions in which compliance may not be satisfactory andwhen anticoagulant treatment cannot be safely administeredEnd-stage renal-disease-associated items are bold
studies which evaluated the effectiveness and safety of OACsin the general population carried out so far excluded patientswith creatinine clearance lt30mLmin Applying the resultsof these studies to the population with advanced renal failureshould not therefore be automatic because their simple usenot only may prove to be ineffective in this group of patientsbut what is worse may be dangerous to them as well
41 OACs in the Treatment of Venous Thromboembolism inPatients with CKD The prevalence of pulmonary embolismin the population of patients receiving haemodialysis isseveral times higher than its prevalence in the generalpopulation The annual incidence of pulmonary embolismin this group of patients is approximately 15100000 versus25100000 patients in the general population [33] Howeverthere are no evidence-based studies evaluating the use ofOACs in this disease and in this population The remainingoption therefore is beginning treatment with unfractionatedheparin usually on an inpatient basis then changing it overthe next several days and continuing the OAC treatmentwhile monitoring INR which is the treatment acceptedgenerally for the population without renal failure [34] Dueto the lack of relevant research the length of therapy depend-ing on the aetiology of the disease the individual risk ofthrombosisbleeding events for a given patient and often thedecision of the patient him- or herself regarding the appliedOAC treatment remain to be evaluated In the case of absolutecontraindications for OACs implantation of a filter in theinferior vena cava could be an alternative therapy but thereare no such studies for patients receiving haemodialysis inthe available literature and they are inconclusive even in thegeneral population [35]
42 OACs in Preventing Thrombosis of Vascular Access forHaemodialysis It is estimated that the causes of almost 13of cases requiring hospitalisation among patients receivinghaemodialysis are associatedwith vascular access failure [40]The likelihood of the occurrence of vascular access failuredue to thrombosis in over a year-long observation of patientsreceiving haemodialysis is approximately 15 in the case of
autologous arteriovenous fistulae and two times higher in thecase of vascular grafts [41] It would therefore seem thatOACscan be an effective treatment option in reducing this risk
Several such prospective controlled studies (some ofwhich were even randomised) have been conducted thoughon small groups of patients Their results however proved tonot be very encouraging In a group of 75 patients receivinghaemodialysis OAC treatment whose therapeutic target wasINR 15ndash20 was found to be only slightly more effective inthe prevention of thrombotic complications in comparisonwith the control group in which OAC treatment was notinitiated (66 versus 57) but the recorded difference wasnot statistically significant [42] What is more in spite ofthe unchanging study protocol the target INR values wereachieved in only a half of the subjects While serious bleedingevents were not recorded the target INR range was not highIn another randomised study on a group of 144 patientsreceiving haemodialysis Colı et al [43] used OACs with alittle higher therapeutic range of INR (18ndash25) Statisticallysignificant differences between the study group and thecontrol group not treated with OACs were observed onlyafter taking the time at which OAC treatment was initiatedinto consideration In the group in which this treatmentwas initiated in the first 24 hours after the implantation ofa vascular catheter vascular complications were found in alittle more than 10 of patients in comparison with patientswho received OACs after their first thrombotic event wherethe proportion of complications was a little over 50 Inanother study carried out on a group of 63 patients receivinghaemodialysis the use of OACs whose therapeutic aim wasINR of 20-30 was proved to be significantly more effectivein preventing thrombosis than in the group of patients notreceiving such treatment [44] However when the resultsof the group treated with OACs were compared with thegroup in which acetylsalicylic acid at a dose of 325mgdaywas used differences in the effectiveness regarding vascu-lar access thrombosis were not observed Serious bleedingevents which significantly more frequently occurred in thegroup receiving OACs were the only significant differencebetween these groups
The Scientific World Journal 5
Table 3 Mortality risk in haemodialysis patients with atrial fibrillation treated with warfarin
Study Population (119899) Period (y) Mortality (HR)Knoll et al [36] 119899mdash235 pts 3 years HRmdash080 (95 CI 028ndash229 119875 lt 067)Chan et al [37] 119899mdash1671 pts 1 year HRmdash110 (094ndash130)
Wizemann et al [38] 119899mdash17513 pts(AFmdash125) 7 years
All ages HRmdash116 (95 CI 108ndash125 119875 lt 0001)Age lt 65 HRmdash129 (95 CI 045ndash368 119875 lt 063)Age 65ndash75 HRmdash135 (95 CI 069ndash263 119875 lt 039)Age gt 75 HRmdash217 (95 CI 104ndash453 119875 lt 004)
Chan et al [39]
119899mdash41425 pts
11 yearsWarfarinmdash83 HRmdash173 (95 CI 162ndash185)Clopidogrelmdash10 HRmdash150 (95 CI 139ndash162)Acetylsalicylicacidmdash304 HRmdash117 (95 CI 112ndash122)
Acetylsalicylic acidand warfarinmdash8 HRmdash111 (95 CI 103ndash186)
HR hazard ratio CI confidence interval 119899 number of patients
How effective is therefore the application of OACs inthis group of patients As the few not very reliable studiessuggest it admittedly increaseswith the increase in the targetINR but at the price of significant adverse reactions in theform of serious bleeding events Moreover in the last ofthe cited studies which confirmed such effectiveness similareffectiveness was recorded with the use of acetylsalicylic acidwithout severe complicationsThe results of the above studiesand the opinions of experts in the area do not allow thereforea routine use of OACs due to the discussed indications [45]This is because a target safe INR range for this group ofpatients has not been established the effectiveness of themedications is doubtful and the risk for the patient is highfurthermore there are alternative methods that are no lesseffective and as it appears are safer [44]
43 OACs in the Prevention ofThromboembolic ComplicationsAssociated with Atrial Fibrillation Atrial fibrillation (AF) isthe most common cardiac dysrhythmia It is estimated that itaffects several percent of the population over the age of 65 andthe proportion increases with age [46] However in the groupof patients with end-stage renal failure this proportion ismuch higher and reaches according to various studies from10 to as high as 30 [47] The annual mortality rate amongthese patients is approximately 25 in the general populationand almost 30 in patients receiving haemodialysis [48]Theprevalence of stroke in patients with atrial fibrillationwithoutrenal failure is on the other hand close to that in patientsreceiving haemodialysis (17 versus 15 resp) [49 50]Similarly studies evaluating the risk of stroke among patientsreceiving haemodialysis depending on the presence of AF orsinus rhythm are inconclusive Some of them show a several-fold increase in the incidence of stroke in the group with AFwhile others do not record such a correlation [50 51] Thesetwo factors among other things are probably responsible forthe inconclusive results of studies evaluating the effectivenessand safety of OAC treatment due to AF in the group ofpatients with end-stage renal failure and patients receiving
haemodialysis The confusion in the literature regardingthe plausibility and significance of the discussed issue isincreased however mostly by the fact that there are simplyno prospective controlled randomised studies in this group
First let us look at the impact of the use of OACs in thisgroup of patients on the hard end-point which is patientmortality (Table 3) Knoll et al [36] carrying out a studyon a group of 235 haemodialysed patients with AF receivingOACs recorded a slightly lower mortality rate than thatwhich characterised the control group not receiving OACsalthough not significant Chan et al [37] in a retrospectivestudy conducted on more than 1600 patients with AFreceiving haemodialysis showed that the use of warfarin inthe prevention of thromboembolic events is not associatedwith all-cause mortality or an increase in the number ofhospitalisations In turn Wizemann et al [38] observed aclear increase in mortality rate in patients receiving warfarinfor the same reasons as in haemodialysed ones which wasespecially apparent in the older population (gt75 years old)Another study confirmed the negative impact of OACs usedfor the same indications on themortality rate in patients withend-stage renal failure in comparison with the control groupwhich did not receive such treatment [39]
Data regarding effectiveness in decreasing the risk ofstroke in patients with AF receiving haemodialysis are alsoinconclusive In one of the latest of such studies Olesenet al [52] in a group of more than 900 patients in whomwarfarin was used in fewer than 20 of cases observed for aperiod of 11 years and found a statistically significant decreasein the risk of the occurrence of stroke or another systemicthromboembolic event However in several other studiessuch an effect was not observed what is more the effect ofusing OACs was decidedly negative In the study cited aboveChan et al [37] recorded a two times higher risk of strokein the group treated with warfarin than in the control groupnot receiving OACs Furthermore there was an increase inthe risk of both haemorrhagic and ischaemic stroke (HR 22and 18 resp) Similar results were presented by Wizemann
6 The Scientific World Journal
et al [38] in a group of 3245 patients participating inDOPPS I and DOPPS II (Dialysis Outcomes and PracticePatterns Study) In this study the patientsrsquo age was the factordifferentiating the risk In the oldest group (gt75 years old)warfarin treatment was associated with a significant morethan twofold increase in the risk of stroke in younger groups(65ndash75 and lt65) the increase in the risk of stroke wasevident but statistically insignificant In another study whichcovered 2313 haemodialysed patients with newly diagnosedAF and treated with warfarin for the first time Winkelmayeret al [53] observed an over twofold increase in the risk ofhaemorrhagic stroke such a relationshipwas not found in thecase of ischaemic stroke
The risk of adverse reactions including severe bleed-ing events during OAC treatment in patients receivinghaemodialysis rises considerably Previous studies in whichOACs were used for different indications had alreadyreported that [54] In the case of the treatment of AF thesituation looks similar most reports suggest a several-foldincrease in this risk The results of the study by Chan etal [39] suggest a significant almost threefold increase inthe risk of severe bleeding events during OAC treatmentin haemodialysed patients due to AF In the same studyclopidogrel was associated with a more than 25-fold (higher)risk of significant haemorrhagic complications what is inter-esting is that the use of acetylsalicylic acid also increasedthis risk but not significantly Holden et al [55] in turnobserved an increase in such risk which was more thanthreefold in the case of warfarin and over fourfold in thecase of acetylsalicylic acid the use of these medications incombinationwas associated withmore than a sixfold increasein this risk Other studies also suggested a significant risk ofsevere bleeding events associated with the use of OACs inthe prevention of thromboembolic complications due to AF[52 56]
Is therefore OAC treatment for the above indications inpatients receiving haemodialysis effective and safe Do thebenefits of using OACs outweigh the risk of severe bleedingevents in patients with end-stage renal failure
All of the above study results should be treated cautiouslyAs we have mentioned there are no large-scale controlledprospective randomised studies here Only on the basis ofsuch studies would it be possible to present guidelines orrecommendations regarding OAC treatment in this groupof patients Most of them are studies conducted on smallgroups observational retrospective groups only a few ofthemwere prospective but not randomised It is also difficultto perform a reliable meta-analysis because the individualstudies sometimes differ in their design specific assumptionsmethods of collecting data ormethods of analysis [37 38 53]Decisions regarding the initiation of OAC treatment andthe time when it occurred depended mostly on the patientrsquosclinical data and the physicianrsquos experience Some studies alsoexcluded patients taking OACs or patients with AF that haddeveloped before renal failure All these circumstances makeit necessary to evaluate these studies cautiously
Moreover let us look at two epidemiological issues [49ndash51]The prevalence of stroke in patients with atrial fibrillationwithout renal failure in comparison with that in patients
receiving haemodialysis turned out to be comparable in theabove-cited studies However the evaluation of the risk ofstroke in patients receiving haemodialysis depending on thepresence of AF or sinus rhythm proved to be inconclusive Iftherefore there is no such risk what role are OACs supposedto play Perhaps a significant portion of the causes of strokein the group with end-stage renal failure are vascular onesand atherosclerosis considerably accelerated in this group ofpatients In this situation OACs would not change such risksignificantly
In turn the increase in the risk of death and the increasein the incidence of stroke in haemodialysed patients treatedwith OACs may be explained by two things The first oneis of course inappropriate management of anticoagulationor rather the time during which the patient remains in thedesired INR range After all its deviation towards higher orlower values is associated with an increase in morbidity oradverse reactions On a daily basis in nephrology units ordialysis centres we can see how difficult it is to keep INR insuch a therapeutic range in patients receiving haemodialysisIt is associated with the fact that chronic renal failureand haemodialysis therapy to an even larger extent are asignificant and independent factors that may decrease theperiod in which the desired value of INR is maintained [57]Anyway the above-cited data regarding the increase in therisk of bleeding events during OAC treatment in patientsreceiving haemodialysis most likely result from the samecause The described impact of vitamin K antagonists onthe processes of vascular calcification and calciphylaxis isanother noteworthy potential factor As a number of studiesboth experimental and clinical show vitamin K inhibitionfor example by OACs inhibits the activity of matrix Glaprotein (MGP) an important protein playing a preventiverole in vascular calcification [58 59] OACs can thereforedirectly interfere and accelerate the process of vascularcalcification already increased in end-stage renal failureIs it a causative factor significantly raising the incidenceof ischaemic stroke and mortality among haemodialysedpatients receiving OACsThis question must be answered byfuture studies
Patients with end-stage renal failure including above allthose who receive haemodialysis are a group of patients withexceptionally many concomitant diseases [60] Considerablyaccelerated atherosclerotic processes vascular calcificationchronic inflammation lipid disorders and malnutrition areinherent characteristics of this population of patients CanOACs have an impact on the risk of stroke in haemodialysedpatients with AF in these conditions and with the existingvascular changes also within the central nervous systemmdashthis Question remains open However the results of the citedstudies do not allow us to use OACs routinely for theseindications in this group of patients
5 Conclusions
The population of patients with CKD including patientsreceiving haemodialysis keeps growing all over the world
The Scientific World Journal 7
Table 4 Potential indications for oral anticoagulants in patientswith end-stage renal disease and receiving haemodialysis
(i) Status after prosthetic heart valve implantation(ii) Antiphospholipid syndrome(iii) Secondary prevention of severe thromboembolic events (forexample pulmonary embolism)(iv) Atrial fibrillation with a high risk of stroke
However OAC treatment in this group of patients irrespec-tive of its indications causes a great deal of controversy Thisis because a number of pro- and anticoagulant factors playan important role in end-stage renal failure due to the natureof the disease itself In these conditions the pharmacokineticand especially pharmacodynamic properties of the OACsused change as well All these factors make proper anticoagu-lation in these patients more difficult and most importantlythey decrease the time during which patients remain inthe therapeutic range of INR In the case of the treatmentof venous thromboembolism the only remaining option isOAC treatment according to regimens used for the generalpopulation as there are no relevant studies concerning thegroup of patients receiving haemodialysis Prevention of HDvascular access thrombosis with the use of OACs accordingto the presented studies and expertsrsquo opinions is not veryeffective and can additionally be very dangerous HoweverOAC treatment in haemodialysed patientswithAF in order toprevent thromboembolic events according to some authorsis associated with an increase in the incidence of stroke andmortality
Is the provocative question included in the title justifiedDoubts should be dispelled by prospective controlled ran-domised studies at the moment there is no justification forroutine use of OACs in the above-mentioned indications Inselected cases of OAC treatment in this group of patients it isabsolutely necessary to control andmonitor the applied treat-ment thoroughly According to the authors and the opinionsalready partially reported in the literature [45] indicationsfor the use of OACs in patients with end-stage renal failureincluding patients receiving haemodialysis should be limitedto those included in Table 4
References
[1] S I Hallan J Coresh B C Astor et al ldquoInternational compari-son of the relationship of chronic kidney disease prevalence andESRD riskrdquo Journal of the American Society of Nephrology vol17 no 8 pp 2275ndash2284 2006
[2] B Rutkowski ldquoChanging pattern of end-stage renal disease incentral and eastern Europerdquo Nephrology Dialysis Transplanta-tion vol 15 no 2 pp 156ndash160 2000
[3] J J Snyder R N Foley and A J Collins ldquoPrevalence of CKDin the United States a sensitivity analysis using the NationalHealth and Nutrition Examination Survey (NHANES) 1999ndash2004rdquo American Journal of Kidney Diseases vol 53 no 2 pp218ndash228 2009
[4] E Krol B Rutkowski P Czarniak et al ldquoEarly detection ofchronic kidney disease results of the PolNef studyrdquo AmericanJournal of Nephrology vol 29 no 3 pp 264ndash273 2009
[5] S Ghanny and M Crowther ldquoTreatment with novel oralanticoagulants indications efficacy and risksrdquo Current Opinionin Hematology vol 20 pp 430ndash436 2013
[6] T Kruger V Brandenburg G Schlieper et al ldquoSailing betweenScylla andCharybdis oral long-term anticoagulation in dialysispatientsrdquo Nephrology Dialysis Transplantation vol 28 pp 534ndash541 2013
[7] S Genovesi and A Santoro ldquoAnticoagulants renal failure andatrial fibrillationrdquo Expert Opinion on Drug Safety vol 12 pp 1ndash3 2013
[8] N Leung ldquoHematologic manifestations of kidney diseaserdquoSeminars in Hematology vol 50 pp 207ndash215 2013
[9] J A Milburn K Cassar I Ford N Fluck and J BrittendenldquoProthrombotic changes in platelet endothelial and coagulationfunction following hemodialysisrdquo International Journal of Arti-ficial Organs vol 34 no 3 pp 280ndash287 2011
[10] D I Jalal M Chonchol andG Targher ldquoDisorders of hemosta-sis associated with chronic kidney diseaserdquo Seminars inThrom-bosis and Hemostasis vol 36 no 1 pp 34ndash40 2010
[11] D Kaw and D Malhotra ldquoPlatelet dysfunction and end-stagerenal diseaserdquo Seminars in Dialysis vol 19 no 4 pp 317ndash3222006
[12] M A de Sa Siqueira T M C Brunini N R Pereira et alldquoIncreased nitric oxide production in platelets from severechronic renal failure patientsrdquo Canadian Journal of Physiologyand Pharmacology vol 89 no 2 pp 97ndash102 2011
[13] P Boccardo G Remuzzi and M Galbusera ldquoPlatelet dysfunc-tion in renal failurerdquo Seminars in Thrombosis and Hemostasisvol 30 no 5 pp 579ndash589 2004
[14] A S Gangji A S Sohal D Treleaven and M A CrowtherldquoBleeding in patients with renal insufficiency a practical guideto clinicalmanagementrdquoThrombosis Research vol 118 no 3 pp423ndash428 2006
[15] J C McCarter J B Bingham and O O Meyer ldquoStudies on thehemorrhagic agent 3 31015840-methylenebis (4-Hydroxycoumarin)IV The pathologic findings after the administration ofdicumarolrdquo The American Journal of Pathology vol 20 pp651ndash659 1944
[16] D V Clatanoff P O Triggs and O O Meyer ldquoClinical expe-rience with coumarin anticoagulants warfarin and warfarinrdquoArchives of Internal Medicine vol 94 no 2 pp 213ndash220 1954
[17] C Becattini M C Vedovati and G Agnelli ldquoOld and neworal anticoagulants for venous thromboembolism and atrialfibrillation a review of the literaturerdquoThrombosis Research vol129 no 3 pp 392ndash400 2012
[18] E A Nutescu ldquoOral anticoagulant therapies balancing therisksrdquoAmerican Journal of Health-System Pharmacy vol 70 no10 supplement 1 pp S3ndashS11 2013
[19] M Zacchigna G di Luca F Cateni and V Maurich ldquoImprove-ment of warfarin biopharmaceutics by conjugation with poly(ethylene glycol)rdquo European Journal of Pharmaceutical Sciencesvol 23 no 4-5 pp 379ndash384 2004
[20] G F Pineo and R D Hull ldquoVitamin K antagonists and directthrombin inhibitors present and futurerdquoHematologyOncologyClinics of North America vol 19 no 1 pp 69ndash85 2005
[21] B F Gage and P E Milligan ldquoPharmacology and pharma-cogenetics of warfarin and other coumarins when used withsupplementsrdquo Thrombosis Research vol 117 no 1-2 pp 55ndash592005
[22] K S Brimble A J Ingram J W Eikelboom et al ldquoAntico-agulants in patients with atrial fibrillation and end-stage renaldiseaserdquo Postgraduate Medicine vol 124 pp 17ndash25 2012
8 The Scientific World Journal
[23] S Benmira Z K Banda and V Bhattacharya ldquoOld versusnew anticoagulants focus on pharmacologyrdquo Recent Patents onCardiovascular Drug Discovery vol 5 no 2 pp 120ndash137 2010
[24] N A Limdi M A Limdi L Cavallari et al ldquoWarfarin dosingin patients with impaired kidney functionrdquoAmerican Journal ofKidney Diseases vol 56 no 5 pp 823ndash831 2010
[25] N Maruyama M Abe K Okada et al ldquoChanges to pro-thrombin international normalized ratio in patients receivinghemodialysisrdquo International Journal of Clinical PharmacologyandTherapeutics vol 51 pp 283ndash287 2013
[26] M Abe N Maruyama H Suzuki et al ldquoInternational nor-malized ratio decreases after hemodialysis treatment in patientstreated with warfarinrdquo Journal of Cardiovascular Pharmacologyvol 60 pp 502ndash507 2012
[27] AGompou I Griveas I Kyritsis I AgroyannisMTsakoniatisand B Agroyannis ldquoINR deviations in hemodialyzed patientsunder low dose oral anticoagulant therapyrdquo International Jour-nal of Artificial Organs vol 32 no 10 pp 752ndash755 2009
[28] J C van Blijderveen K M Verhamme R Zietse et alldquoOveranticoagulation is associated with renal function declinerdquoJournal of Nephrology vol 26 pp 691ndash698 2013
[29] M M Sood M Larkina J R Thumma et al ldquoMajor bleed-ing events and risk stratification of antithrombotic agents inhemodialysis results from the DOPPSrdquo Kidney Internationalvol 84 pp 600ndash608 2013
[30] M Monge I Vaida S S Modeliar et al ldquoRetroperitonealhematoma compressing a single functioning kidney an unusualcause of obstructive renal failurerdquo Clinical Nephrology vol 67no 5 pp 318ndash320 2007
[31] M Dugo E la Torre F Farneti et al ldquoA case of intrarenalhematoma role of ultrasonography in the early diagnosisof possible complication of anticoagulant therapyrdquo GiornaleItaliano di Nefrologia vol 29 pp 616ndash620 2012
[32] httpwwwaccessdatafdagovdrugsatfda docslabel2011009218s107lblpdf
[33] D P Tveit I O Hypolite P Hshieh et al ldquoChronic dialysispatients have high risk for pulmonary embolismrdquo AmericanJournal of Kidney Diseases vol 39 no 5 pp 1011ndash1017 2002
[34] C Kearon S R Kahn G Agnelli S Goldhaber G E RaskobandA J Comerota ldquoAntithrombotic therapy for venous throm-boembolic disease American College of Chest Physiciansevidence-based clinical practice guidelines (8th edition)rdquoChestvol 133 no 6 pp 454Sndash545S 2008
[35] H Decousus A Leizerovicz F Parent et al ldquoA clinical trialof vena cava filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave StudyGrouprdquoTheNew England Journal ofMedicine vol 338 pp 409ndash415 1998
[36] F Knoll G Sturm C Lamina et al ldquoCoumarins and survival inincident dialysis patientsrdquo Nephrology Dialysis Transplantationvol 27 no 1 pp 332ndash337 2012
[37] K E Chan J Michael Lazarus R Thadhani and R MHakim ldquoWarfarin use associates with increased risk for strokein hemodialysis patients with atrial fibrillationrdquo Journal of theAmerican Society of Nephrology vol 20 no 10 pp 2223ndash22332009
[38] V T L Wizemann S Satayathum A Disney et al ldquoAtrialfibrillation in hemodialysis patients clinical features and asso-ciations with anticoagulant therapyrdquo Kidney International vol77 no 12 pp 1098ndash1106 2010
[39] K E Chan J M Lazarus R Thadhani and R M HakimldquoAnticoagulant and antiplatelet usage associates with mortalityamong hemodialysis patientsrdquo Journal of the American Societyof Nephrology vol 20 no 4 pp 872ndash881 2009
[40] J A Chazan M R London and L M Pomo ldquoLong-termsurvival of vascular accesses in a large chronic hemodialysispopulationrdquo Nephron vol 69 no 3 pp 228ndash233 1995
[41] D N Churchill D W Taylor R J Cook et al ldquoCanadianhemodialysis morbidity studyrdquo American Journal of KidneyDiseases vol 19 no 3 pp 214ndash234 1992
[42] M Zellweger J Bouchard S Raymond-Carrier A Laforest-Renald S Querin and F Madore ldquoSystemic anticoagulationand prevention of hemodialysis catheter malfunctionrdquo Amer-ican Society for Artificial Internal Organs Journal vol 51 no 4pp 360ndash365 2005
[43] L Colı G Donati G Cianciolo et al ldquoAnticoagulation therapyfor the prevention of hemodialysis tunneled cuffed catheter(TCC) thrombosisrdquo Journal of Vascular Access vol 7 no 3 pp118ndash122 2006
[44] C I Obialo A C Conner and L F Lebon ldquoMaintainingpatency of tunneled hemodialysis cathetersmdashefficacy of aspirincompared to warfarinrdquo Scandinavian Journal of Urology andNephrology vol 37 no 2 pp 172ndash176 2003
[45] M Cozzolino and V Brandenburg ldquoWarfarin to use or not touse in chronic kidney disease patientsrdquo Journal of Nephrologyvol 23 no 6 pp 648ndash652 2010
[46] L Friberg and L Bergfeldt ldquoAtrial fibrillation prevalence revis-itedrdquo Journal of Internal Medicine vol 274 no 5 pp 461ndash4682013
[47] I Atar D Konas S Acikel et al ldquoFrequency of atrial fibrillationand factors related to its development in dialysis patientsrdquoInternational Journal of Cardiology vol 106 pp 47ndash51 2006
[48] E Vazquez C Sanchez-Perales F Borrego et al ldquoInfluenceof atrial fibrillation on the morbido-mortality of patients onhemodialysisrdquo American Heart Journal vol 140 no 6 pp 886ndash890 2000
[49] S A Lubitz C Moser L Sullivan et al ldquoAtrial fibrillationpatterns and risks of subsequent stroke heart failure or deathin the communityrdquo Journal of the American Heart Associationvol 2 Article ID e000126 2013
[50] U S Renal DATA System USRDS 200520062007 AnnualData Report Atlas of End-Stage Renal Disease in the UnitedStates Bethesda National Institutes of Health NationalInstitute of Diabetes and Digestive and Kidney Diseaseshttpwwwusrdsorgarchiveaspx
[51] S Genovesi A Vincenti E Rossi et al ldquoAtrial fibrillation andmorbidity and mortality in a cohort of long-term hemodialysispatientsrdquoAmerican Journal of Kidney Diseases vol 51 no 2 pp255ndash262 2008
[52] J Olesen G Lip A L Kamper et al ldquoStroke and bleeding inatrial fibrillation with chronic kidney diseaserdquoTheNewEnglandJournal of Medicine vol 367 pp 625ndash635 2012
[53] W C Winkelmayer J Liu S Setoguchi and N K ChoudhryldquoEffectiveness and safety of warfarin initiation in olderhemodialysis patients with incident atrial fibrillationrdquo ClinicalJournal of the American Society of Nephrology vol 6 no 11 pp2662ndash2668 2011
[54] M J Elliott D Zimmerman and R M Holden ldquoWarfarinanticoagulation in hemodialysis patients a systematic review ofbleeding ratesrdquoAmerican Journal of Kidney Diseases vol 50 no3 pp 433ndash440 2007
The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 The Scientific World Journal
Table 2 Contraindications for the use of oral anticoagulants [32]
(i) Increased risk of bleeding eventsmdashplatelet function disorders thrombocytopenia vonWillebrand disease and haemophilia(ii) Recent intracranial bleeding Conditions predisposing to intracranial bleedingmdashcerebral artery aneurysms(iii) Conditions predisposing to gastrointestinal urinary and respiratory tract bleeding(iv) Surgical procedures within the central nervous system or the eye(v) Increased risk of frequent fallsmdashcaused by a neurological or another condition(vi) Severe liver failure cirrhosis(vii) Untreated or poorly controlled arterial hypertension(viii) Pregnancy(ix) Infective endocarditis or pericardial effusion(x) Hypersensitivity to the active substance or any of the excipients(xi)Dementia psychoses alcoholism and other conditions in which compliance may not be satisfactory andwhen anticoagulant treatment cannot be safely administeredEnd-stage renal-disease-associated items are bold
studies which evaluated the effectiveness and safety of OACsin the general population carried out so far excluded patientswith creatinine clearance lt30mLmin Applying the resultsof these studies to the population with advanced renal failureshould not therefore be automatic because their simple usenot only may prove to be ineffective in this group of patientsbut what is worse may be dangerous to them as well
41 OACs in the Treatment of Venous Thromboembolism inPatients with CKD The prevalence of pulmonary embolismin the population of patients receiving haemodialysis isseveral times higher than its prevalence in the generalpopulation The annual incidence of pulmonary embolismin this group of patients is approximately 15100000 versus25100000 patients in the general population [33] Howeverthere are no evidence-based studies evaluating the use ofOACs in this disease and in this population The remainingoption therefore is beginning treatment with unfractionatedheparin usually on an inpatient basis then changing it overthe next several days and continuing the OAC treatmentwhile monitoring INR which is the treatment acceptedgenerally for the population without renal failure [34] Dueto the lack of relevant research the length of therapy depend-ing on the aetiology of the disease the individual risk ofthrombosisbleeding events for a given patient and often thedecision of the patient him- or herself regarding the appliedOAC treatment remain to be evaluated In the case of absolutecontraindications for OACs implantation of a filter in theinferior vena cava could be an alternative therapy but thereare no such studies for patients receiving haemodialysis inthe available literature and they are inconclusive even in thegeneral population [35]
42 OACs in Preventing Thrombosis of Vascular Access forHaemodialysis It is estimated that the causes of almost 13of cases requiring hospitalisation among patients receivinghaemodialysis are associatedwith vascular access failure [40]The likelihood of the occurrence of vascular access failuredue to thrombosis in over a year-long observation of patientsreceiving haemodialysis is approximately 15 in the case of
autologous arteriovenous fistulae and two times higher in thecase of vascular grafts [41] It would therefore seem thatOACscan be an effective treatment option in reducing this risk
Several such prospective controlled studies (some ofwhich were even randomised) have been conducted thoughon small groups of patients Their results however proved tonot be very encouraging In a group of 75 patients receivinghaemodialysis OAC treatment whose therapeutic target wasINR 15ndash20 was found to be only slightly more effective inthe prevention of thrombotic complications in comparisonwith the control group in which OAC treatment was notinitiated (66 versus 57) but the recorded difference wasnot statistically significant [42] What is more in spite ofthe unchanging study protocol the target INR values wereachieved in only a half of the subjects While serious bleedingevents were not recorded the target INR range was not highIn another randomised study on a group of 144 patientsreceiving haemodialysis Colı et al [43] used OACs with alittle higher therapeutic range of INR (18ndash25) Statisticallysignificant differences between the study group and thecontrol group not treated with OACs were observed onlyafter taking the time at which OAC treatment was initiatedinto consideration In the group in which this treatmentwas initiated in the first 24 hours after the implantation ofa vascular catheter vascular complications were found in alittle more than 10 of patients in comparison with patientswho received OACs after their first thrombotic event wherethe proportion of complications was a little over 50 Inanother study carried out on a group of 63 patients receivinghaemodialysis the use of OACs whose therapeutic aim wasINR of 20-30 was proved to be significantly more effectivein preventing thrombosis than in the group of patients notreceiving such treatment [44] However when the resultsof the group treated with OACs were compared with thegroup in which acetylsalicylic acid at a dose of 325mgdaywas used differences in the effectiveness regarding vascu-lar access thrombosis were not observed Serious bleedingevents which significantly more frequently occurred in thegroup receiving OACs were the only significant differencebetween these groups
The Scientific World Journal 5
Table 3 Mortality risk in haemodialysis patients with atrial fibrillation treated with warfarin
Study Population (119899) Period (y) Mortality (HR)Knoll et al [36] 119899mdash235 pts 3 years HRmdash080 (95 CI 028ndash229 119875 lt 067)Chan et al [37] 119899mdash1671 pts 1 year HRmdash110 (094ndash130)
Wizemann et al [38] 119899mdash17513 pts(AFmdash125) 7 years
All ages HRmdash116 (95 CI 108ndash125 119875 lt 0001)Age lt 65 HRmdash129 (95 CI 045ndash368 119875 lt 063)Age 65ndash75 HRmdash135 (95 CI 069ndash263 119875 lt 039)Age gt 75 HRmdash217 (95 CI 104ndash453 119875 lt 004)
Chan et al [39]
119899mdash41425 pts
11 yearsWarfarinmdash83 HRmdash173 (95 CI 162ndash185)Clopidogrelmdash10 HRmdash150 (95 CI 139ndash162)Acetylsalicylicacidmdash304 HRmdash117 (95 CI 112ndash122)
Acetylsalicylic acidand warfarinmdash8 HRmdash111 (95 CI 103ndash186)
HR hazard ratio CI confidence interval 119899 number of patients
How effective is therefore the application of OACs inthis group of patients As the few not very reliable studiessuggest it admittedly increaseswith the increase in the targetINR but at the price of significant adverse reactions in theform of serious bleeding events Moreover in the last ofthe cited studies which confirmed such effectiveness similareffectiveness was recorded with the use of acetylsalicylic acidwithout severe complicationsThe results of the above studiesand the opinions of experts in the area do not allow thereforea routine use of OACs due to the discussed indications [45]This is because a target safe INR range for this group ofpatients has not been established the effectiveness of themedications is doubtful and the risk for the patient is highfurthermore there are alternative methods that are no lesseffective and as it appears are safer [44]
43 OACs in the Prevention ofThromboembolic ComplicationsAssociated with Atrial Fibrillation Atrial fibrillation (AF) isthe most common cardiac dysrhythmia It is estimated that itaffects several percent of the population over the age of 65 andthe proportion increases with age [46] However in the groupof patients with end-stage renal failure this proportion ismuch higher and reaches according to various studies from10 to as high as 30 [47] The annual mortality rate amongthese patients is approximately 25 in the general populationand almost 30 in patients receiving haemodialysis [48]Theprevalence of stroke in patients with atrial fibrillationwithoutrenal failure is on the other hand close to that in patientsreceiving haemodialysis (17 versus 15 resp) [49 50]Similarly studies evaluating the risk of stroke among patientsreceiving haemodialysis depending on the presence of AF orsinus rhythm are inconclusive Some of them show a several-fold increase in the incidence of stroke in the group with AFwhile others do not record such a correlation [50 51] Thesetwo factors among other things are probably responsible forthe inconclusive results of studies evaluating the effectivenessand safety of OAC treatment due to AF in the group ofpatients with end-stage renal failure and patients receiving
haemodialysis The confusion in the literature regardingthe plausibility and significance of the discussed issue isincreased however mostly by the fact that there are simplyno prospective controlled randomised studies in this group
First let us look at the impact of the use of OACs in thisgroup of patients on the hard end-point which is patientmortality (Table 3) Knoll et al [36] carrying out a studyon a group of 235 haemodialysed patients with AF receivingOACs recorded a slightly lower mortality rate than thatwhich characterised the control group not receiving OACsalthough not significant Chan et al [37] in a retrospectivestudy conducted on more than 1600 patients with AFreceiving haemodialysis showed that the use of warfarin inthe prevention of thromboembolic events is not associatedwith all-cause mortality or an increase in the number ofhospitalisations In turn Wizemann et al [38] observed aclear increase in mortality rate in patients receiving warfarinfor the same reasons as in haemodialysed ones which wasespecially apparent in the older population (gt75 years old)Another study confirmed the negative impact of OACs usedfor the same indications on themortality rate in patients withend-stage renal failure in comparison with the control groupwhich did not receive such treatment [39]
Data regarding effectiveness in decreasing the risk ofstroke in patients with AF receiving haemodialysis are alsoinconclusive In one of the latest of such studies Olesenet al [52] in a group of more than 900 patients in whomwarfarin was used in fewer than 20 of cases observed for aperiod of 11 years and found a statistically significant decreasein the risk of the occurrence of stroke or another systemicthromboembolic event However in several other studiessuch an effect was not observed what is more the effect ofusing OACs was decidedly negative In the study cited aboveChan et al [37] recorded a two times higher risk of strokein the group treated with warfarin than in the control groupnot receiving OACs Furthermore there was an increase inthe risk of both haemorrhagic and ischaemic stroke (HR 22and 18 resp) Similar results were presented by Wizemann
6 The Scientific World Journal
et al [38] in a group of 3245 patients participating inDOPPS I and DOPPS II (Dialysis Outcomes and PracticePatterns Study) In this study the patientsrsquo age was the factordifferentiating the risk In the oldest group (gt75 years old)warfarin treatment was associated with a significant morethan twofold increase in the risk of stroke in younger groups(65ndash75 and lt65) the increase in the risk of stroke wasevident but statistically insignificant In another study whichcovered 2313 haemodialysed patients with newly diagnosedAF and treated with warfarin for the first time Winkelmayeret al [53] observed an over twofold increase in the risk ofhaemorrhagic stroke such a relationshipwas not found in thecase of ischaemic stroke
The risk of adverse reactions including severe bleed-ing events during OAC treatment in patients receivinghaemodialysis rises considerably Previous studies in whichOACs were used for different indications had alreadyreported that [54] In the case of the treatment of AF thesituation looks similar most reports suggest a several-foldincrease in this risk The results of the study by Chan etal [39] suggest a significant almost threefold increase inthe risk of severe bleeding events during OAC treatmentin haemodialysed patients due to AF In the same studyclopidogrel was associated with a more than 25-fold (higher)risk of significant haemorrhagic complications what is inter-esting is that the use of acetylsalicylic acid also increasedthis risk but not significantly Holden et al [55] in turnobserved an increase in such risk which was more thanthreefold in the case of warfarin and over fourfold in thecase of acetylsalicylic acid the use of these medications incombinationwas associated withmore than a sixfold increasein this risk Other studies also suggested a significant risk ofsevere bleeding events associated with the use of OACs inthe prevention of thromboembolic complications due to AF[52 56]
Is therefore OAC treatment for the above indications inpatients receiving haemodialysis effective and safe Do thebenefits of using OACs outweigh the risk of severe bleedingevents in patients with end-stage renal failure
All of the above study results should be treated cautiouslyAs we have mentioned there are no large-scale controlledprospective randomised studies here Only on the basis ofsuch studies would it be possible to present guidelines orrecommendations regarding OAC treatment in this groupof patients Most of them are studies conducted on smallgroups observational retrospective groups only a few ofthemwere prospective but not randomised It is also difficultto perform a reliable meta-analysis because the individualstudies sometimes differ in their design specific assumptionsmethods of collecting data ormethods of analysis [37 38 53]Decisions regarding the initiation of OAC treatment andthe time when it occurred depended mostly on the patientrsquosclinical data and the physicianrsquos experience Some studies alsoexcluded patients taking OACs or patients with AF that haddeveloped before renal failure All these circumstances makeit necessary to evaluate these studies cautiously
Moreover let us look at two epidemiological issues [49ndash51]The prevalence of stroke in patients with atrial fibrillationwithout renal failure in comparison with that in patients
receiving haemodialysis turned out to be comparable in theabove-cited studies However the evaluation of the risk ofstroke in patients receiving haemodialysis depending on thepresence of AF or sinus rhythm proved to be inconclusive Iftherefore there is no such risk what role are OACs supposedto play Perhaps a significant portion of the causes of strokein the group with end-stage renal failure are vascular onesand atherosclerosis considerably accelerated in this group ofpatients In this situation OACs would not change such risksignificantly
In turn the increase in the risk of death and the increasein the incidence of stroke in haemodialysed patients treatedwith OACs may be explained by two things The first oneis of course inappropriate management of anticoagulationor rather the time during which the patient remains in thedesired INR range After all its deviation towards higher orlower values is associated with an increase in morbidity oradverse reactions On a daily basis in nephrology units ordialysis centres we can see how difficult it is to keep INR insuch a therapeutic range in patients receiving haemodialysisIt is associated with the fact that chronic renal failureand haemodialysis therapy to an even larger extent are asignificant and independent factors that may decrease theperiod in which the desired value of INR is maintained [57]Anyway the above-cited data regarding the increase in therisk of bleeding events during OAC treatment in patientsreceiving haemodialysis most likely result from the samecause The described impact of vitamin K antagonists onthe processes of vascular calcification and calciphylaxis isanother noteworthy potential factor As a number of studiesboth experimental and clinical show vitamin K inhibitionfor example by OACs inhibits the activity of matrix Glaprotein (MGP) an important protein playing a preventiverole in vascular calcification [58 59] OACs can thereforedirectly interfere and accelerate the process of vascularcalcification already increased in end-stage renal failureIs it a causative factor significantly raising the incidenceof ischaemic stroke and mortality among haemodialysedpatients receiving OACsThis question must be answered byfuture studies
Patients with end-stage renal failure including above allthose who receive haemodialysis are a group of patients withexceptionally many concomitant diseases [60] Considerablyaccelerated atherosclerotic processes vascular calcificationchronic inflammation lipid disorders and malnutrition areinherent characteristics of this population of patients CanOACs have an impact on the risk of stroke in haemodialysedpatients with AF in these conditions and with the existingvascular changes also within the central nervous systemmdashthis Question remains open However the results of the citedstudies do not allow us to use OACs routinely for theseindications in this group of patients
5 Conclusions
The population of patients with CKD including patientsreceiving haemodialysis keeps growing all over the world
The Scientific World Journal 7
Table 4 Potential indications for oral anticoagulants in patientswith end-stage renal disease and receiving haemodialysis
(i) Status after prosthetic heart valve implantation(ii) Antiphospholipid syndrome(iii) Secondary prevention of severe thromboembolic events (forexample pulmonary embolism)(iv) Atrial fibrillation with a high risk of stroke
However OAC treatment in this group of patients irrespec-tive of its indications causes a great deal of controversy Thisis because a number of pro- and anticoagulant factors playan important role in end-stage renal failure due to the natureof the disease itself In these conditions the pharmacokineticand especially pharmacodynamic properties of the OACsused change as well All these factors make proper anticoagu-lation in these patients more difficult and most importantlythey decrease the time during which patients remain inthe therapeutic range of INR In the case of the treatmentof venous thromboembolism the only remaining option isOAC treatment according to regimens used for the generalpopulation as there are no relevant studies concerning thegroup of patients receiving haemodialysis Prevention of HDvascular access thrombosis with the use of OACs accordingto the presented studies and expertsrsquo opinions is not veryeffective and can additionally be very dangerous HoweverOAC treatment in haemodialysed patientswithAF in order toprevent thromboembolic events according to some authorsis associated with an increase in the incidence of stroke andmortality
Is the provocative question included in the title justifiedDoubts should be dispelled by prospective controlled ran-domised studies at the moment there is no justification forroutine use of OACs in the above-mentioned indications Inselected cases of OAC treatment in this group of patients it isabsolutely necessary to control andmonitor the applied treat-ment thoroughly According to the authors and the opinionsalready partially reported in the literature [45] indicationsfor the use of OACs in patients with end-stage renal failureincluding patients receiving haemodialysis should be limitedto those included in Table 4
References
[1] S I Hallan J Coresh B C Astor et al ldquoInternational compari-son of the relationship of chronic kidney disease prevalence andESRD riskrdquo Journal of the American Society of Nephrology vol17 no 8 pp 2275ndash2284 2006
[2] B Rutkowski ldquoChanging pattern of end-stage renal disease incentral and eastern Europerdquo Nephrology Dialysis Transplanta-tion vol 15 no 2 pp 156ndash160 2000
[3] J J Snyder R N Foley and A J Collins ldquoPrevalence of CKDin the United States a sensitivity analysis using the NationalHealth and Nutrition Examination Survey (NHANES) 1999ndash2004rdquo American Journal of Kidney Diseases vol 53 no 2 pp218ndash228 2009
[4] E Krol B Rutkowski P Czarniak et al ldquoEarly detection ofchronic kidney disease results of the PolNef studyrdquo AmericanJournal of Nephrology vol 29 no 3 pp 264ndash273 2009
[5] S Ghanny and M Crowther ldquoTreatment with novel oralanticoagulants indications efficacy and risksrdquo Current Opinionin Hematology vol 20 pp 430ndash436 2013
[6] T Kruger V Brandenburg G Schlieper et al ldquoSailing betweenScylla andCharybdis oral long-term anticoagulation in dialysispatientsrdquo Nephrology Dialysis Transplantation vol 28 pp 534ndash541 2013
[7] S Genovesi and A Santoro ldquoAnticoagulants renal failure andatrial fibrillationrdquo Expert Opinion on Drug Safety vol 12 pp 1ndash3 2013
[8] N Leung ldquoHematologic manifestations of kidney diseaserdquoSeminars in Hematology vol 50 pp 207ndash215 2013
[9] J A Milburn K Cassar I Ford N Fluck and J BrittendenldquoProthrombotic changes in platelet endothelial and coagulationfunction following hemodialysisrdquo International Journal of Arti-ficial Organs vol 34 no 3 pp 280ndash287 2011
[10] D I Jalal M Chonchol andG Targher ldquoDisorders of hemosta-sis associated with chronic kidney diseaserdquo Seminars inThrom-bosis and Hemostasis vol 36 no 1 pp 34ndash40 2010
[11] D Kaw and D Malhotra ldquoPlatelet dysfunction and end-stagerenal diseaserdquo Seminars in Dialysis vol 19 no 4 pp 317ndash3222006
[12] M A de Sa Siqueira T M C Brunini N R Pereira et alldquoIncreased nitric oxide production in platelets from severechronic renal failure patientsrdquo Canadian Journal of Physiologyand Pharmacology vol 89 no 2 pp 97ndash102 2011
[13] P Boccardo G Remuzzi and M Galbusera ldquoPlatelet dysfunc-tion in renal failurerdquo Seminars in Thrombosis and Hemostasisvol 30 no 5 pp 579ndash589 2004
[14] A S Gangji A S Sohal D Treleaven and M A CrowtherldquoBleeding in patients with renal insufficiency a practical guideto clinicalmanagementrdquoThrombosis Research vol 118 no 3 pp423ndash428 2006
[15] J C McCarter J B Bingham and O O Meyer ldquoStudies on thehemorrhagic agent 3 31015840-methylenebis (4-Hydroxycoumarin)IV The pathologic findings after the administration ofdicumarolrdquo The American Journal of Pathology vol 20 pp651ndash659 1944
[16] D V Clatanoff P O Triggs and O O Meyer ldquoClinical expe-rience with coumarin anticoagulants warfarin and warfarinrdquoArchives of Internal Medicine vol 94 no 2 pp 213ndash220 1954
[17] C Becattini M C Vedovati and G Agnelli ldquoOld and neworal anticoagulants for venous thromboembolism and atrialfibrillation a review of the literaturerdquoThrombosis Research vol129 no 3 pp 392ndash400 2012
[18] E A Nutescu ldquoOral anticoagulant therapies balancing therisksrdquoAmerican Journal of Health-System Pharmacy vol 70 no10 supplement 1 pp S3ndashS11 2013
[19] M Zacchigna G di Luca F Cateni and V Maurich ldquoImprove-ment of warfarin biopharmaceutics by conjugation with poly(ethylene glycol)rdquo European Journal of Pharmaceutical Sciencesvol 23 no 4-5 pp 379ndash384 2004
[20] G F Pineo and R D Hull ldquoVitamin K antagonists and directthrombin inhibitors present and futurerdquoHematologyOncologyClinics of North America vol 19 no 1 pp 69ndash85 2005
[21] B F Gage and P E Milligan ldquoPharmacology and pharma-cogenetics of warfarin and other coumarins when used withsupplementsrdquo Thrombosis Research vol 117 no 1-2 pp 55ndash592005
[22] K S Brimble A J Ingram J W Eikelboom et al ldquoAntico-agulants in patients with atrial fibrillation and end-stage renaldiseaserdquo Postgraduate Medicine vol 124 pp 17ndash25 2012
8 The Scientific World Journal
[23] S Benmira Z K Banda and V Bhattacharya ldquoOld versusnew anticoagulants focus on pharmacologyrdquo Recent Patents onCardiovascular Drug Discovery vol 5 no 2 pp 120ndash137 2010
[24] N A Limdi M A Limdi L Cavallari et al ldquoWarfarin dosingin patients with impaired kidney functionrdquoAmerican Journal ofKidney Diseases vol 56 no 5 pp 823ndash831 2010
[25] N Maruyama M Abe K Okada et al ldquoChanges to pro-thrombin international normalized ratio in patients receivinghemodialysisrdquo International Journal of Clinical PharmacologyandTherapeutics vol 51 pp 283ndash287 2013
[26] M Abe N Maruyama H Suzuki et al ldquoInternational nor-malized ratio decreases after hemodialysis treatment in patientstreated with warfarinrdquo Journal of Cardiovascular Pharmacologyvol 60 pp 502ndash507 2012
[27] AGompou I Griveas I Kyritsis I AgroyannisMTsakoniatisand B Agroyannis ldquoINR deviations in hemodialyzed patientsunder low dose oral anticoagulant therapyrdquo International Jour-nal of Artificial Organs vol 32 no 10 pp 752ndash755 2009
[28] J C van Blijderveen K M Verhamme R Zietse et alldquoOveranticoagulation is associated with renal function declinerdquoJournal of Nephrology vol 26 pp 691ndash698 2013
[29] M M Sood M Larkina J R Thumma et al ldquoMajor bleed-ing events and risk stratification of antithrombotic agents inhemodialysis results from the DOPPSrdquo Kidney Internationalvol 84 pp 600ndash608 2013
[30] M Monge I Vaida S S Modeliar et al ldquoRetroperitonealhematoma compressing a single functioning kidney an unusualcause of obstructive renal failurerdquo Clinical Nephrology vol 67no 5 pp 318ndash320 2007
[31] M Dugo E la Torre F Farneti et al ldquoA case of intrarenalhematoma role of ultrasonography in the early diagnosisof possible complication of anticoagulant therapyrdquo GiornaleItaliano di Nefrologia vol 29 pp 616ndash620 2012
[32] httpwwwaccessdatafdagovdrugsatfda docslabel2011009218s107lblpdf
[33] D P Tveit I O Hypolite P Hshieh et al ldquoChronic dialysispatients have high risk for pulmonary embolismrdquo AmericanJournal of Kidney Diseases vol 39 no 5 pp 1011ndash1017 2002
[34] C Kearon S R Kahn G Agnelli S Goldhaber G E RaskobandA J Comerota ldquoAntithrombotic therapy for venous throm-boembolic disease American College of Chest Physiciansevidence-based clinical practice guidelines (8th edition)rdquoChestvol 133 no 6 pp 454Sndash545S 2008
[35] H Decousus A Leizerovicz F Parent et al ldquoA clinical trialof vena cava filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave StudyGrouprdquoTheNew England Journal ofMedicine vol 338 pp 409ndash415 1998
[36] F Knoll G Sturm C Lamina et al ldquoCoumarins and survival inincident dialysis patientsrdquo Nephrology Dialysis Transplantationvol 27 no 1 pp 332ndash337 2012
[37] K E Chan J Michael Lazarus R Thadhani and R MHakim ldquoWarfarin use associates with increased risk for strokein hemodialysis patients with atrial fibrillationrdquo Journal of theAmerican Society of Nephrology vol 20 no 10 pp 2223ndash22332009
[38] V T L Wizemann S Satayathum A Disney et al ldquoAtrialfibrillation in hemodialysis patients clinical features and asso-ciations with anticoagulant therapyrdquo Kidney International vol77 no 12 pp 1098ndash1106 2010
[39] K E Chan J M Lazarus R Thadhani and R M HakimldquoAnticoagulant and antiplatelet usage associates with mortalityamong hemodialysis patientsrdquo Journal of the American Societyof Nephrology vol 20 no 4 pp 872ndash881 2009
[40] J A Chazan M R London and L M Pomo ldquoLong-termsurvival of vascular accesses in a large chronic hemodialysispopulationrdquo Nephron vol 69 no 3 pp 228ndash233 1995
[41] D N Churchill D W Taylor R J Cook et al ldquoCanadianhemodialysis morbidity studyrdquo American Journal of KidneyDiseases vol 19 no 3 pp 214ndash234 1992
[42] M Zellweger J Bouchard S Raymond-Carrier A Laforest-Renald S Querin and F Madore ldquoSystemic anticoagulationand prevention of hemodialysis catheter malfunctionrdquo Amer-ican Society for Artificial Internal Organs Journal vol 51 no 4pp 360ndash365 2005
[43] L Colı G Donati G Cianciolo et al ldquoAnticoagulation therapyfor the prevention of hemodialysis tunneled cuffed catheter(TCC) thrombosisrdquo Journal of Vascular Access vol 7 no 3 pp118ndash122 2006
[44] C I Obialo A C Conner and L F Lebon ldquoMaintainingpatency of tunneled hemodialysis cathetersmdashefficacy of aspirincompared to warfarinrdquo Scandinavian Journal of Urology andNephrology vol 37 no 2 pp 172ndash176 2003
[45] M Cozzolino and V Brandenburg ldquoWarfarin to use or not touse in chronic kidney disease patientsrdquo Journal of Nephrologyvol 23 no 6 pp 648ndash652 2010
[46] L Friberg and L Bergfeldt ldquoAtrial fibrillation prevalence revis-itedrdquo Journal of Internal Medicine vol 274 no 5 pp 461ndash4682013
[47] I Atar D Konas S Acikel et al ldquoFrequency of atrial fibrillationand factors related to its development in dialysis patientsrdquoInternational Journal of Cardiology vol 106 pp 47ndash51 2006
[48] E Vazquez C Sanchez-Perales F Borrego et al ldquoInfluenceof atrial fibrillation on the morbido-mortality of patients onhemodialysisrdquo American Heart Journal vol 140 no 6 pp 886ndash890 2000
[49] S A Lubitz C Moser L Sullivan et al ldquoAtrial fibrillationpatterns and risks of subsequent stroke heart failure or deathin the communityrdquo Journal of the American Heart Associationvol 2 Article ID e000126 2013
[50] U S Renal DATA System USRDS 200520062007 AnnualData Report Atlas of End-Stage Renal Disease in the UnitedStates Bethesda National Institutes of Health NationalInstitute of Diabetes and Digestive and Kidney Diseaseshttpwwwusrdsorgarchiveaspx
[51] S Genovesi A Vincenti E Rossi et al ldquoAtrial fibrillation andmorbidity and mortality in a cohort of long-term hemodialysispatientsrdquoAmerican Journal of Kidney Diseases vol 51 no 2 pp255ndash262 2008
[52] J Olesen G Lip A L Kamper et al ldquoStroke and bleeding inatrial fibrillation with chronic kidney diseaserdquoTheNewEnglandJournal of Medicine vol 367 pp 625ndash635 2012
[53] W C Winkelmayer J Liu S Setoguchi and N K ChoudhryldquoEffectiveness and safety of warfarin initiation in olderhemodialysis patients with incident atrial fibrillationrdquo ClinicalJournal of the American Society of Nephrology vol 6 no 11 pp2662ndash2668 2011
[54] M J Elliott D Zimmerman and R M Holden ldquoWarfarinanticoagulation in hemodialysis patients a systematic review ofbleeding ratesrdquoAmerican Journal of Kidney Diseases vol 50 no3 pp 433ndash440 2007
The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

The Scientific World Journal 5
Table 3 Mortality risk in haemodialysis patients with atrial fibrillation treated with warfarin
Study Population (119899) Period (y) Mortality (HR)Knoll et al [36] 119899mdash235 pts 3 years HRmdash080 (95 CI 028ndash229 119875 lt 067)Chan et al [37] 119899mdash1671 pts 1 year HRmdash110 (094ndash130)
Wizemann et al [38] 119899mdash17513 pts(AFmdash125) 7 years
All ages HRmdash116 (95 CI 108ndash125 119875 lt 0001)Age lt 65 HRmdash129 (95 CI 045ndash368 119875 lt 063)Age 65ndash75 HRmdash135 (95 CI 069ndash263 119875 lt 039)Age gt 75 HRmdash217 (95 CI 104ndash453 119875 lt 004)
Chan et al [39]
119899mdash41425 pts
11 yearsWarfarinmdash83 HRmdash173 (95 CI 162ndash185)Clopidogrelmdash10 HRmdash150 (95 CI 139ndash162)Acetylsalicylicacidmdash304 HRmdash117 (95 CI 112ndash122)
Acetylsalicylic acidand warfarinmdash8 HRmdash111 (95 CI 103ndash186)
HR hazard ratio CI confidence interval 119899 number of patients
How effective is therefore the application of OACs inthis group of patients As the few not very reliable studiessuggest it admittedly increaseswith the increase in the targetINR but at the price of significant adverse reactions in theform of serious bleeding events Moreover in the last ofthe cited studies which confirmed such effectiveness similareffectiveness was recorded with the use of acetylsalicylic acidwithout severe complicationsThe results of the above studiesand the opinions of experts in the area do not allow thereforea routine use of OACs due to the discussed indications [45]This is because a target safe INR range for this group ofpatients has not been established the effectiveness of themedications is doubtful and the risk for the patient is highfurthermore there are alternative methods that are no lesseffective and as it appears are safer [44]
43 OACs in the Prevention ofThromboembolic ComplicationsAssociated with Atrial Fibrillation Atrial fibrillation (AF) isthe most common cardiac dysrhythmia It is estimated that itaffects several percent of the population over the age of 65 andthe proportion increases with age [46] However in the groupof patients with end-stage renal failure this proportion ismuch higher and reaches according to various studies from10 to as high as 30 [47] The annual mortality rate amongthese patients is approximately 25 in the general populationand almost 30 in patients receiving haemodialysis [48]Theprevalence of stroke in patients with atrial fibrillationwithoutrenal failure is on the other hand close to that in patientsreceiving haemodialysis (17 versus 15 resp) [49 50]Similarly studies evaluating the risk of stroke among patientsreceiving haemodialysis depending on the presence of AF orsinus rhythm are inconclusive Some of them show a several-fold increase in the incidence of stroke in the group with AFwhile others do not record such a correlation [50 51] Thesetwo factors among other things are probably responsible forthe inconclusive results of studies evaluating the effectivenessand safety of OAC treatment due to AF in the group ofpatients with end-stage renal failure and patients receiving
haemodialysis The confusion in the literature regardingthe plausibility and significance of the discussed issue isincreased however mostly by the fact that there are simplyno prospective controlled randomised studies in this group
First let us look at the impact of the use of OACs in thisgroup of patients on the hard end-point which is patientmortality (Table 3) Knoll et al [36] carrying out a studyon a group of 235 haemodialysed patients with AF receivingOACs recorded a slightly lower mortality rate than thatwhich characterised the control group not receiving OACsalthough not significant Chan et al [37] in a retrospectivestudy conducted on more than 1600 patients with AFreceiving haemodialysis showed that the use of warfarin inthe prevention of thromboembolic events is not associatedwith all-cause mortality or an increase in the number ofhospitalisations In turn Wizemann et al [38] observed aclear increase in mortality rate in patients receiving warfarinfor the same reasons as in haemodialysed ones which wasespecially apparent in the older population (gt75 years old)Another study confirmed the negative impact of OACs usedfor the same indications on themortality rate in patients withend-stage renal failure in comparison with the control groupwhich did not receive such treatment [39]
Data regarding effectiveness in decreasing the risk ofstroke in patients with AF receiving haemodialysis are alsoinconclusive In one of the latest of such studies Olesenet al [52] in a group of more than 900 patients in whomwarfarin was used in fewer than 20 of cases observed for aperiod of 11 years and found a statistically significant decreasein the risk of the occurrence of stroke or another systemicthromboembolic event However in several other studiessuch an effect was not observed what is more the effect ofusing OACs was decidedly negative In the study cited aboveChan et al [37] recorded a two times higher risk of strokein the group treated with warfarin than in the control groupnot receiving OACs Furthermore there was an increase inthe risk of both haemorrhagic and ischaemic stroke (HR 22and 18 resp) Similar results were presented by Wizemann
6 The Scientific World Journal
et al [38] in a group of 3245 patients participating inDOPPS I and DOPPS II (Dialysis Outcomes and PracticePatterns Study) In this study the patientsrsquo age was the factordifferentiating the risk In the oldest group (gt75 years old)warfarin treatment was associated with a significant morethan twofold increase in the risk of stroke in younger groups(65ndash75 and lt65) the increase in the risk of stroke wasevident but statistically insignificant In another study whichcovered 2313 haemodialysed patients with newly diagnosedAF and treated with warfarin for the first time Winkelmayeret al [53] observed an over twofold increase in the risk ofhaemorrhagic stroke such a relationshipwas not found in thecase of ischaemic stroke
The risk of adverse reactions including severe bleed-ing events during OAC treatment in patients receivinghaemodialysis rises considerably Previous studies in whichOACs were used for different indications had alreadyreported that [54] In the case of the treatment of AF thesituation looks similar most reports suggest a several-foldincrease in this risk The results of the study by Chan etal [39] suggest a significant almost threefold increase inthe risk of severe bleeding events during OAC treatmentin haemodialysed patients due to AF In the same studyclopidogrel was associated with a more than 25-fold (higher)risk of significant haemorrhagic complications what is inter-esting is that the use of acetylsalicylic acid also increasedthis risk but not significantly Holden et al [55] in turnobserved an increase in such risk which was more thanthreefold in the case of warfarin and over fourfold in thecase of acetylsalicylic acid the use of these medications incombinationwas associated withmore than a sixfold increasein this risk Other studies also suggested a significant risk ofsevere bleeding events associated with the use of OACs inthe prevention of thromboembolic complications due to AF[52 56]
Is therefore OAC treatment for the above indications inpatients receiving haemodialysis effective and safe Do thebenefits of using OACs outweigh the risk of severe bleedingevents in patients with end-stage renal failure
All of the above study results should be treated cautiouslyAs we have mentioned there are no large-scale controlledprospective randomised studies here Only on the basis ofsuch studies would it be possible to present guidelines orrecommendations regarding OAC treatment in this groupof patients Most of them are studies conducted on smallgroups observational retrospective groups only a few ofthemwere prospective but not randomised It is also difficultto perform a reliable meta-analysis because the individualstudies sometimes differ in their design specific assumptionsmethods of collecting data ormethods of analysis [37 38 53]Decisions regarding the initiation of OAC treatment andthe time when it occurred depended mostly on the patientrsquosclinical data and the physicianrsquos experience Some studies alsoexcluded patients taking OACs or patients with AF that haddeveloped before renal failure All these circumstances makeit necessary to evaluate these studies cautiously
Moreover let us look at two epidemiological issues [49ndash51]The prevalence of stroke in patients with atrial fibrillationwithout renal failure in comparison with that in patients
receiving haemodialysis turned out to be comparable in theabove-cited studies However the evaluation of the risk ofstroke in patients receiving haemodialysis depending on thepresence of AF or sinus rhythm proved to be inconclusive Iftherefore there is no such risk what role are OACs supposedto play Perhaps a significant portion of the causes of strokein the group with end-stage renal failure are vascular onesand atherosclerosis considerably accelerated in this group ofpatients In this situation OACs would not change such risksignificantly
In turn the increase in the risk of death and the increasein the incidence of stroke in haemodialysed patients treatedwith OACs may be explained by two things The first oneis of course inappropriate management of anticoagulationor rather the time during which the patient remains in thedesired INR range After all its deviation towards higher orlower values is associated with an increase in morbidity oradverse reactions On a daily basis in nephrology units ordialysis centres we can see how difficult it is to keep INR insuch a therapeutic range in patients receiving haemodialysisIt is associated with the fact that chronic renal failureand haemodialysis therapy to an even larger extent are asignificant and independent factors that may decrease theperiod in which the desired value of INR is maintained [57]Anyway the above-cited data regarding the increase in therisk of bleeding events during OAC treatment in patientsreceiving haemodialysis most likely result from the samecause The described impact of vitamin K antagonists onthe processes of vascular calcification and calciphylaxis isanother noteworthy potential factor As a number of studiesboth experimental and clinical show vitamin K inhibitionfor example by OACs inhibits the activity of matrix Glaprotein (MGP) an important protein playing a preventiverole in vascular calcification [58 59] OACs can thereforedirectly interfere and accelerate the process of vascularcalcification already increased in end-stage renal failureIs it a causative factor significantly raising the incidenceof ischaemic stroke and mortality among haemodialysedpatients receiving OACsThis question must be answered byfuture studies
Patients with end-stage renal failure including above allthose who receive haemodialysis are a group of patients withexceptionally many concomitant diseases [60] Considerablyaccelerated atherosclerotic processes vascular calcificationchronic inflammation lipid disorders and malnutrition areinherent characteristics of this population of patients CanOACs have an impact on the risk of stroke in haemodialysedpatients with AF in these conditions and with the existingvascular changes also within the central nervous systemmdashthis Question remains open However the results of the citedstudies do not allow us to use OACs routinely for theseindications in this group of patients
5 Conclusions
The population of patients with CKD including patientsreceiving haemodialysis keeps growing all over the world
The Scientific World Journal 7
Table 4 Potential indications for oral anticoagulants in patientswith end-stage renal disease and receiving haemodialysis
(i) Status after prosthetic heart valve implantation(ii) Antiphospholipid syndrome(iii) Secondary prevention of severe thromboembolic events (forexample pulmonary embolism)(iv) Atrial fibrillation with a high risk of stroke
However OAC treatment in this group of patients irrespec-tive of its indications causes a great deal of controversy Thisis because a number of pro- and anticoagulant factors playan important role in end-stage renal failure due to the natureof the disease itself In these conditions the pharmacokineticand especially pharmacodynamic properties of the OACsused change as well All these factors make proper anticoagu-lation in these patients more difficult and most importantlythey decrease the time during which patients remain inthe therapeutic range of INR In the case of the treatmentof venous thromboembolism the only remaining option isOAC treatment according to regimens used for the generalpopulation as there are no relevant studies concerning thegroup of patients receiving haemodialysis Prevention of HDvascular access thrombosis with the use of OACs accordingto the presented studies and expertsrsquo opinions is not veryeffective and can additionally be very dangerous HoweverOAC treatment in haemodialysed patientswithAF in order toprevent thromboembolic events according to some authorsis associated with an increase in the incidence of stroke andmortality
Is the provocative question included in the title justifiedDoubts should be dispelled by prospective controlled ran-domised studies at the moment there is no justification forroutine use of OACs in the above-mentioned indications Inselected cases of OAC treatment in this group of patients it isabsolutely necessary to control andmonitor the applied treat-ment thoroughly According to the authors and the opinionsalready partially reported in the literature [45] indicationsfor the use of OACs in patients with end-stage renal failureincluding patients receiving haemodialysis should be limitedto those included in Table 4
References
[1] S I Hallan J Coresh B C Astor et al ldquoInternational compari-son of the relationship of chronic kidney disease prevalence andESRD riskrdquo Journal of the American Society of Nephrology vol17 no 8 pp 2275ndash2284 2006
[2] B Rutkowski ldquoChanging pattern of end-stage renal disease incentral and eastern Europerdquo Nephrology Dialysis Transplanta-tion vol 15 no 2 pp 156ndash160 2000
[3] J J Snyder R N Foley and A J Collins ldquoPrevalence of CKDin the United States a sensitivity analysis using the NationalHealth and Nutrition Examination Survey (NHANES) 1999ndash2004rdquo American Journal of Kidney Diseases vol 53 no 2 pp218ndash228 2009
[4] E Krol B Rutkowski P Czarniak et al ldquoEarly detection ofchronic kidney disease results of the PolNef studyrdquo AmericanJournal of Nephrology vol 29 no 3 pp 264ndash273 2009
[5] S Ghanny and M Crowther ldquoTreatment with novel oralanticoagulants indications efficacy and risksrdquo Current Opinionin Hematology vol 20 pp 430ndash436 2013
[6] T Kruger V Brandenburg G Schlieper et al ldquoSailing betweenScylla andCharybdis oral long-term anticoagulation in dialysispatientsrdquo Nephrology Dialysis Transplantation vol 28 pp 534ndash541 2013
[7] S Genovesi and A Santoro ldquoAnticoagulants renal failure andatrial fibrillationrdquo Expert Opinion on Drug Safety vol 12 pp 1ndash3 2013
[8] N Leung ldquoHematologic manifestations of kidney diseaserdquoSeminars in Hematology vol 50 pp 207ndash215 2013
[9] J A Milburn K Cassar I Ford N Fluck and J BrittendenldquoProthrombotic changes in platelet endothelial and coagulationfunction following hemodialysisrdquo International Journal of Arti-ficial Organs vol 34 no 3 pp 280ndash287 2011
[10] D I Jalal M Chonchol andG Targher ldquoDisorders of hemosta-sis associated with chronic kidney diseaserdquo Seminars inThrom-bosis and Hemostasis vol 36 no 1 pp 34ndash40 2010
[11] D Kaw and D Malhotra ldquoPlatelet dysfunction and end-stagerenal diseaserdquo Seminars in Dialysis vol 19 no 4 pp 317ndash3222006
[12] M A de Sa Siqueira T M C Brunini N R Pereira et alldquoIncreased nitric oxide production in platelets from severechronic renal failure patientsrdquo Canadian Journal of Physiologyand Pharmacology vol 89 no 2 pp 97ndash102 2011
[13] P Boccardo G Remuzzi and M Galbusera ldquoPlatelet dysfunc-tion in renal failurerdquo Seminars in Thrombosis and Hemostasisvol 30 no 5 pp 579ndash589 2004
[14] A S Gangji A S Sohal D Treleaven and M A CrowtherldquoBleeding in patients with renal insufficiency a practical guideto clinicalmanagementrdquoThrombosis Research vol 118 no 3 pp423ndash428 2006
[15] J C McCarter J B Bingham and O O Meyer ldquoStudies on thehemorrhagic agent 3 31015840-methylenebis (4-Hydroxycoumarin)IV The pathologic findings after the administration ofdicumarolrdquo The American Journal of Pathology vol 20 pp651ndash659 1944
[16] D V Clatanoff P O Triggs and O O Meyer ldquoClinical expe-rience with coumarin anticoagulants warfarin and warfarinrdquoArchives of Internal Medicine vol 94 no 2 pp 213ndash220 1954
[17] C Becattini M C Vedovati and G Agnelli ldquoOld and neworal anticoagulants for venous thromboembolism and atrialfibrillation a review of the literaturerdquoThrombosis Research vol129 no 3 pp 392ndash400 2012
[18] E A Nutescu ldquoOral anticoagulant therapies balancing therisksrdquoAmerican Journal of Health-System Pharmacy vol 70 no10 supplement 1 pp S3ndashS11 2013
[19] M Zacchigna G di Luca F Cateni and V Maurich ldquoImprove-ment of warfarin biopharmaceutics by conjugation with poly(ethylene glycol)rdquo European Journal of Pharmaceutical Sciencesvol 23 no 4-5 pp 379ndash384 2004
[20] G F Pineo and R D Hull ldquoVitamin K antagonists and directthrombin inhibitors present and futurerdquoHematologyOncologyClinics of North America vol 19 no 1 pp 69ndash85 2005
[21] B F Gage and P E Milligan ldquoPharmacology and pharma-cogenetics of warfarin and other coumarins when used withsupplementsrdquo Thrombosis Research vol 117 no 1-2 pp 55ndash592005
[22] K S Brimble A J Ingram J W Eikelboom et al ldquoAntico-agulants in patients with atrial fibrillation and end-stage renaldiseaserdquo Postgraduate Medicine vol 124 pp 17ndash25 2012
8 The Scientific World Journal
[23] S Benmira Z K Banda and V Bhattacharya ldquoOld versusnew anticoagulants focus on pharmacologyrdquo Recent Patents onCardiovascular Drug Discovery vol 5 no 2 pp 120ndash137 2010
[24] N A Limdi M A Limdi L Cavallari et al ldquoWarfarin dosingin patients with impaired kidney functionrdquoAmerican Journal ofKidney Diseases vol 56 no 5 pp 823ndash831 2010
[25] N Maruyama M Abe K Okada et al ldquoChanges to pro-thrombin international normalized ratio in patients receivinghemodialysisrdquo International Journal of Clinical PharmacologyandTherapeutics vol 51 pp 283ndash287 2013
[26] M Abe N Maruyama H Suzuki et al ldquoInternational nor-malized ratio decreases after hemodialysis treatment in patientstreated with warfarinrdquo Journal of Cardiovascular Pharmacologyvol 60 pp 502ndash507 2012
[27] AGompou I Griveas I Kyritsis I AgroyannisMTsakoniatisand B Agroyannis ldquoINR deviations in hemodialyzed patientsunder low dose oral anticoagulant therapyrdquo International Jour-nal of Artificial Organs vol 32 no 10 pp 752ndash755 2009
[28] J C van Blijderveen K M Verhamme R Zietse et alldquoOveranticoagulation is associated with renal function declinerdquoJournal of Nephrology vol 26 pp 691ndash698 2013
[29] M M Sood M Larkina J R Thumma et al ldquoMajor bleed-ing events and risk stratification of antithrombotic agents inhemodialysis results from the DOPPSrdquo Kidney Internationalvol 84 pp 600ndash608 2013
[30] M Monge I Vaida S S Modeliar et al ldquoRetroperitonealhematoma compressing a single functioning kidney an unusualcause of obstructive renal failurerdquo Clinical Nephrology vol 67no 5 pp 318ndash320 2007
[31] M Dugo E la Torre F Farneti et al ldquoA case of intrarenalhematoma role of ultrasonography in the early diagnosisof possible complication of anticoagulant therapyrdquo GiornaleItaliano di Nefrologia vol 29 pp 616ndash620 2012
[32] httpwwwaccessdatafdagovdrugsatfda docslabel2011009218s107lblpdf
[33] D P Tveit I O Hypolite P Hshieh et al ldquoChronic dialysispatients have high risk for pulmonary embolismrdquo AmericanJournal of Kidney Diseases vol 39 no 5 pp 1011ndash1017 2002
[34] C Kearon S R Kahn G Agnelli S Goldhaber G E RaskobandA J Comerota ldquoAntithrombotic therapy for venous throm-boembolic disease American College of Chest Physiciansevidence-based clinical practice guidelines (8th edition)rdquoChestvol 133 no 6 pp 454Sndash545S 2008
[35] H Decousus A Leizerovicz F Parent et al ldquoA clinical trialof vena cava filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave StudyGrouprdquoTheNew England Journal ofMedicine vol 338 pp 409ndash415 1998
[36] F Knoll G Sturm C Lamina et al ldquoCoumarins and survival inincident dialysis patientsrdquo Nephrology Dialysis Transplantationvol 27 no 1 pp 332ndash337 2012
[37] K E Chan J Michael Lazarus R Thadhani and R MHakim ldquoWarfarin use associates with increased risk for strokein hemodialysis patients with atrial fibrillationrdquo Journal of theAmerican Society of Nephrology vol 20 no 10 pp 2223ndash22332009
[38] V T L Wizemann S Satayathum A Disney et al ldquoAtrialfibrillation in hemodialysis patients clinical features and asso-ciations with anticoagulant therapyrdquo Kidney International vol77 no 12 pp 1098ndash1106 2010
[39] K E Chan J M Lazarus R Thadhani and R M HakimldquoAnticoagulant and antiplatelet usage associates with mortalityamong hemodialysis patientsrdquo Journal of the American Societyof Nephrology vol 20 no 4 pp 872ndash881 2009
[40] J A Chazan M R London and L M Pomo ldquoLong-termsurvival of vascular accesses in a large chronic hemodialysispopulationrdquo Nephron vol 69 no 3 pp 228ndash233 1995
[41] D N Churchill D W Taylor R J Cook et al ldquoCanadianhemodialysis morbidity studyrdquo American Journal of KidneyDiseases vol 19 no 3 pp 214ndash234 1992
[42] M Zellweger J Bouchard S Raymond-Carrier A Laforest-Renald S Querin and F Madore ldquoSystemic anticoagulationand prevention of hemodialysis catheter malfunctionrdquo Amer-ican Society for Artificial Internal Organs Journal vol 51 no 4pp 360ndash365 2005
[43] L Colı G Donati G Cianciolo et al ldquoAnticoagulation therapyfor the prevention of hemodialysis tunneled cuffed catheter(TCC) thrombosisrdquo Journal of Vascular Access vol 7 no 3 pp118ndash122 2006
[44] C I Obialo A C Conner and L F Lebon ldquoMaintainingpatency of tunneled hemodialysis cathetersmdashefficacy of aspirincompared to warfarinrdquo Scandinavian Journal of Urology andNephrology vol 37 no 2 pp 172ndash176 2003
[45] M Cozzolino and V Brandenburg ldquoWarfarin to use or not touse in chronic kidney disease patientsrdquo Journal of Nephrologyvol 23 no 6 pp 648ndash652 2010
[46] L Friberg and L Bergfeldt ldquoAtrial fibrillation prevalence revis-itedrdquo Journal of Internal Medicine vol 274 no 5 pp 461ndash4682013
[47] I Atar D Konas S Acikel et al ldquoFrequency of atrial fibrillationand factors related to its development in dialysis patientsrdquoInternational Journal of Cardiology vol 106 pp 47ndash51 2006
[48] E Vazquez C Sanchez-Perales F Borrego et al ldquoInfluenceof atrial fibrillation on the morbido-mortality of patients onhemodialysisrdquo American Heart Journal vol 140 no 6 pp 886ndash890 2000
[49] S A Lubitz C Moser L Sullivan et al ldquoAtrial fibrillationpatterns and risks of subsequent stroke heart failure or deathin the communityrdquo Journal of the American Heart Associationvol 2 Article ID e000126 2013
[50] U S Renal DATA System USRDS 200520062007 AnnualData Report Atlas of End-Stage Renal Disease in the UnitedStates Bethesda National Institutes of Health NationalInstitute of Diabetes and Digestive and Kidney Diseaseshttpwwwusrdsorgarchiveaspx
[51] S Genovesi A Vincenti E Rossi et al ldquoAtrial fibrillation andmorbidity and mortality in a cohort of long-term hemodialysispatientsrdquoAmerican Journal of Kidney Diseases vol 51 no 2 pp255ndash262 2008
[52] J Olesen G Lip A L Kamper et al ldquoStroke and bleeding inatrial fibrillation with chronic kidney diseaserdquoTheNewEnglandJournal of Medicine vol 367 pp 625ndash635 2012
[53] W C Winkelmayer J Liu S Setoguchi and N K ChoudhryldquoEffectiveness and safety of warfarin initiation in olderhemodialysis patients with incident atrial fibrillationrdquo ClinicalJournal of the American Society of Nephrology vol 6 no 11 pp2662ndash2668 2011
[54] M J Elliott D Zimmerman and R M Holden ldquoWarfarinanticoagulation in hemodialysis patients a systematic review ofbleeding ratesrdquoAmerican Journal of Kidney Diseases vol 50 no3 pp 433ndash440 2007
The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 The Scientific World Journal
et al [38] in a group of 3245 patients participating inDOPPS I and DOPPS II (Dialysis Outcomes and PracticePatterns Study) In this study the patientsrsquo age was the factordifferentiating the risk In the oldest group (gt75 years old)warfarin treatment was associated with a significant morethan twofold increase in the risk of stroke in younger groups(65ndash75 and lt65) the increase in the risk of stroke wasevident but statistically insignificant In another study whichcovered 2313 haemodialysed patients with newly diagnosedAF and treated with warfarin for the first time Winkelmayeret al [53] observed an over twofold increase in the risk ofhaemorrhagic stroke such a relationshipwas not found in thecase of ischaemic stroke
The risk of adverse reactions including severe bleed-ing events during OAC treatment in patients receivinghaemodialysis rises considerably Previous studies in whichOACs were used for different indications had alreadyreported that [54] In the case of the treatment of AF thesituation looks similar most reports suggest a several-foldincrease in this risk The results of the study by Chan etal [39] suggest a significant almost threefold increase inthe risk of severe bleeding events during OAC treatmentin haemodialysed patients due to AF In the same studyclopidogrel was associated with a more than 25-fold (higher)risk of significant haemorrhagic complications what is inter-esting is that the use of acetylsalicylic acid also increasedthis risk but not significantly Holden et al [55] in turnobserved an increase in such risk which was more thanthreefold in the case of warfarin and over fourfold in thecase of acetylsalicylic acid the use of these medications incombinationwas associated withmore than a sixfold increasein this risk Other studies also suggested a significant risk ofsevere bleeding events associated with the use of OACs inthe prevention of thromboembolic complications due to AF[52 56]
Is therefore OAC treatment for the above indications inpatients receiving haemodialysis effective and safe Do thebenefits of using OACs outweigh the risk of severe bleedingevents in patients with end-stage renal failure
All of the above study results should be treated cautiouslyAs we have mentioned there are no large-scale controlledprospective randomised studies here Only on the basis ofsuch studies would it be possible to present guidelines orrecommendations regarding OAC treatment in this groupof patients Most of them are studies conducted on smallgroups observational retrospective groups only a few ofthemwere prospective but not randomised It is also difficultto perform a reliable meta-analysis because the individualstudies sometimes differ in their design specific assumptionsmethods of collecting data ormethods of analysis [37 38 53]Decisions regarding the initiation of OAC treatment andthe time when it occurred depended mostly on the patientrsquosclinical data and the physicianrsquos experience Some studies alsoexcluded patients taking OACs or patients with AF that haddeveloped before renal failure All these circumstances makeit necessary to evaluate these studies cautiously
Moreover let us look at two epidemiological issues [49ndash51]The prevalence of stroke in patients with atrial fibrillationwithout renal failure in comparison with that in patients
receiving haemodialysis turned out to be comparable in theabove-cited studies However the evaluation of the risk ofstroke in patients receiving haemodialysis depending on thepresence of AF or sinus rhythm proved to be inconclusive Iftherefore there is no such risk what role are OACs supposedto play Perhaps a significant portion of the causes of strokein the group with end-stage renal failure are vascular onesand atherosclerosis considerably accelerated in this group ofpatients In this situation OACs would not change such risksignificantly
In turn the increase in the risk of death and the increasein the incidence of stroke in haemodialysed patients treatedwith OACs may be explained by two things The first oneis of course inappropriate management of anticoagulationor rather the time during which the patient remains in thedesired INR range After all its deviation towards higher orlower values is associated with an increase in morbidity oradverse reactions On a daily basis in nephrology units ordialysis centres we can see how difficult it is to keep INR insuch a therapeutic range in patients receiving haemodialysisIt is associated with the fact that chronic renal failureand haemodialysis therapy to an even larger extent are asignificant and independent factors that may decrease theperiod in which the desired value of INR is maintained [57]Anyway the above-cited data regarding the increase in therisk of bleeding events during OAC treatment in patientsreceiving haemodialysis most likely result from the samecause The described impact of vitamin K antagonists onthe processes of vascular calcification and calciphylaxis isanother noteworthy potential factor As a number of studiesboth experimental and clinical show vitamin K inhibitionfor example by OACs inhibits the activity of matrix Glaprotein (MGP) an important protein playing a preventiverole in vascular calcification [58 59] OACs can thereforedirectly interfere and accelerate the process of vascularcalcification already increased in end-stage renal failureIs it a causative factor significantly raising the incidenceof ischaemic stroke and mortality among haemodialysedpatients receiving OACsThis question must be answered byfuture studies
Patients with end-stage renal failure including above allthose who receive haemodialysis are a group of patients withexceptionally many concomitant diseases [60] Considerablyaccelerated atherosclerotic processes vascular calcificationchronic inflammation lipid disorders and malnutrition areinherent characteristics of this population of patients CanOACs have an impact on the risk of stroke in haemodialysedpatients with AF in these conditions and with the existingvascular changes also within the central nervous systemmdashthis Question remains open However the results of the citedstudies do not allow us to use OACs routinely for theseindications in this group of patients
5 Conclusions
The population of patients with CKD including patientsreceiving haemodialysis keeps growing all over the world
The Scientific World Journal 7
Table 4 Potential indications for oral anticoagulants in patientswith end-stage renal disease and receiving haemodialysis
(i) Status after prosthetic heart valve implantation(ii) Antiphospholipid syndrome(iii) Secondary prevention of severe thromboembolic events (forexample pulmonary embolism)(iv) Atrial fibrillation with a high risk of stroke
However OAC treatment in this group of patients irrespec-tive of its indications causes a great deal of controversy Thisis because a number of pro- and anticoagulant factors playan important role in end-stage renal failure due to the natureof the disease itself In these conditions the pharmacokineticand especially pharmacodynamic properties of the OACsused change as well All these factors make proper anticoagu-lation in these patients more difficult and most importantlythey decrease the time during which patients remain inthe therapeutic range of INR In the case of the treatmentof venous thromboembolism the only remaining option isOAC treatment according to regimens used for the generalpopulation as there are no relevant studies concerning thegroup of patients receiving haemodialysis Prevention of HDvascular access thrombosis with the use of OACs accordingto the presented studies and expertsrsquo opinions is not veryeffective and can additionally be very dangerous HoweverOAC treatment in haemodialysed patientswithAF in order toprevent thromboembolic events according to some authorsis associated with an increase in the incidence of stroke andmortality
Is the provocative question included in the title justifiedDoubts should be dispelled by prospective controlled ran-domised studies at the moment there is no justification forroutine use of OACs in the above-mentioned indications Inselected cases of OAC treatment in this group of patients it isabsolutely necessary to control andmonitor the applied treat-ment thoroughly According to the authors and the opinionsalready partially reported in the literature [45] indicationsfor the use of OACs in patients with end-stage renal failureincluding patients receiving haemodialysis should be limitedto those included in Table 4
References
[1] S I Hallan J Coresh B C Astor et al ldquoInternational compari-son of the relationship of chronic kidney disease prevalence andESRD riskrdquo Journal of the American Society of Nephrology vol17 no 8 pp 2275ndash2284 2006
[2] B Rutkowski ldquoChanging pattern of end-stage renal disease incentral and eastern Europerdquo Nephrology Dialysis Transplanta-tion vol 15 no 2 pp 156ndash160 2000
[3] J J Snyder R N Foley and A J Collins ldquoPrevalence of CKDin the United States a sensitivity analysis using the NationalHealth and Nutrition Examination Survey (NHANES) 1999ndash2004rdquo American Journal of Kidney Diseases vol 53 no 2 pp218ndash228 2009
[4] E Krol B Rutkowski P Czarniak et al ldquoEarly detection ofchronic kidney disease results of the PolNef studyrdquo AmericanJournal of Nephrology vol 29 no 3 pp 264ndash273 2009
[5] S Ghanny and M Crowther ldquoTreatment with novel oralanticoagulants indications efficacy and risksrdquo Current Opinionin Hematology vol 20 pp 430ndash436 2013
[6] T Kruger V Brandenburg G Schlieper et al ldquoSailing betweenScylla andCharybdis oral long-term anticoagulation in dialysispatientsrdquo Nephrology Dialysis Transplantation vol 28 pp 534ndash541 2013
[7] S Genovesi and A Santoro ldquoAnticoagulants renal failure andatrial fibrillationrdquo Expert Opinion on Drug Safety vol 12 pp 1ndash3 2013
[8] N Leung ldquoHematologic manifestations of kidney diseaserdquoSeminars in Hematology vol 50 pp 207ndash215 2013
[9] J A Milburn K Cassar I Ford N Fluck and J BrittendenldquoProthrombotic changes in platelet endothelial and coagulationfunction following hemodialysisrdquo International Journal of Arti-ficial Organs vol 34 no 3 pp 280ndash287 2011
[10] D I Jalal M Chonchol andG Targher ldquoDisorders of hemosta-sis associated with chronic kidney diseaserdquo Seminars inThrom-bosis and Hemostasis vol 36 no 1 pp 34ndash40 2010
[11] D Kaw and D Malhotra ldquoPlatelet dysfunction and end-stagerenal diseaserdquo Seminars in Dialysis vol 19 no 4 pp 317ndash3222006
[12] M A de Sa Siqueira T M C Brunini N R Pereira et alldquoIncreased nitric oxide production in platelets from severechronic renal failure patientsrdquo Canadian Journal of Physiologyand Pharmacology vol 89 no 2 pp 97ndash102 2011
[13] P Boccardo G Remuzzi and M Galbusera ldquoPlatelet dysfunc-tion in renal failurerdquo Seminars in Thrombosis and Hemostasisvol 30 no 5 pp 579ndash589 2004
[14] A S Gangji A S Sohal D Treleaven and M A CrowtherldquoBleeding in patients with renal insufficiency a practical guideto clinicalmanagementrdquoThrombosis Research vol 118 no 3 pp423ndash428 2006
[15] J C McCarter J B Bingham and O O Meyer ldquoStudies on thehemorrhagic agent 3 31015840-methylenebis (4-Hydroxycoumarin)IV The pathologic findings after the administration ofdicumarolrdquo The American Journal of Pathology vol 20 pp651ndash659 1944
[16] D V Clatanoff P O Triggs and O O Meyer ldquoClinical expe-rience with coumarin anticoagulants warfarin and warfarinrdquoArchives of Internal Medicine vol 94 no 2 pp 213ndash220 1954
[17] C Becattini M C Vedovati and G Agnelli ldquoOld and neworal anticoagulants for venous thromboembolism and atrialfibrillation a review of the literaturerdquoThrombosis Research vol129 no 3 pp 392ndash400 2012
[18] E A Nutescu ldquoOral anticoagulant therapies balancing therisksrdquoAmerican Journal of Health-System Pharmacy vol 70 no10 supplement 1 pp S3ndashS11 2013
[19] M Zacchigna G di Luca F Cateni and V Maurich ldquoImprove-ment of warfarin biopharmaceutics by conjugation with poly(ethylene glycol)rdquo European Journal of Pharmaceutical Sciencesvol 23 no 4-5 pp 379ndash384 2004
[20] G F Pineo and R D Hull ldquoVitamin K antagonists and directthrombin inhibitors present and futurerdquoHematologyOncologyClinics of North America vol 19 no 1 pp 69ndash85 2005
[21] B F Gage and P E Milligan ldquoPharmacology and pharma-cogenetics of warfarin and other coumarins when used withsupplementsrdquo Thrombosis Research vol 117 no 1-2 pp 55ndash592005
[22] K S Brimble A J Ingram J W Eikelboom et al ldquoAntico-agulants in patients with atrial fibrillation and end-stage renaldiseaserdquo Postgraduate Medicine vol 124 pp 17ndash25 2012
8 The Scientific World Journal
[23] S Benmira Z K Banda and V Bhattacharya ldquoOld versusnew anticoagulants focus on pharmacologyrdquo Recent Patents onCardiovascular Drug Discovery vol 5 no 2 pp 120ndash137 2010
[24] N A Limdi M A Limdi L Cavallari et al ldquoWarfarin dosingin patients with impaired kidney functionrdquoAmerican Journal ofKidney Diseases vol 56 no 5 pp 823ndash831 2010
[25] N Maruyama M Abe K Okada et al ldquoChanges to pro-thrombin international normalized ratio in patients receivinghemodialysisrdquo International Journal of Clinical PharmacologyandTherapeutics vol 51 pp 283ndash287 2013
[26] M Abe N Maruyama H Suzuki et al ldquoInternational nor-malized ratio decreases after hemodialysis treatment in patientstreated with warfarinrdquo Journal of Cardiovascular Pharmacologyvol 60 pp 502ndash507 2012
[27] AGompou I Griveas I Kyritsis I AgroyannisMTsakoniatisand B Agroyannis ldquoINR deviations in hemodialyzed patientsunder low dose oral anticoagulant therapyrdquo International Jour-nal of Artificial Organs vol 32 no 10 pp 752ndash755 2009
[28] J C van Blijderveen K M Verhamme R Zietse et alldquoOveranticoagulation is associated with renal function declinerdquoJournal of Nephrology vol 26 pp 691ndash698 2013
[29] M M Sood M Larkina J R Thumma et al ldquoMajor bleed-ing events and risk stratification of antithrombotic agents inhemodialysis results from the DOPPSrdquo Kidney Internationalvol 84 pp 600ndash608 2013
[30] M Monge I Vaida S S Modeliar et al ldquoRetroperitonealhematoma compressing a single functioning kidney an unusualcause of obstructive renal failurerdquo Clinical Nephrology vol 67no 5 pp 318ndash320 2007
[31] M Dugo E la Torre F Farneti et al ldquoA case of intrarenalhematoma role of ultrasonography in the early diagnosisof possible complication of anticoagulant therapyrdquo GiornaleItaliano di Nefrologia vol 29 pp 616ndash620 2012
[32] httpwwwaccessdatafdagovdrugsatfda docslabel2011009218s107lblpdf
[33] D P Tveit I O Hypolite P Hshieh et al ldquoChronic dialysispatients have high risk for pulmonary embolismrdquo AmericanJournal of Kidney Diseases vol 39 no 5 pp 1011ndash1017 2002
[34] C Kearon S R Kahn G Agnelli S Goldhaber G E RaskobandA J Comerota ldquoAntithrombotic therapy for venous throm-boembolic disease American College of Chest Physiciansevidence-based clinical practice guidelines (8th edition)rdquoChestvol 133 no 6 pp 454Sndash545S 2008
[35] H Decousus A Leizerovicz F Parent et al ldquoA clinical trialof vena cava filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave StudyGrouprdquoTheNew England Journal ofMedicine vol 338 pp 409ndash415 1998
[36] F Knoll G Sturm C Lamina et al ldquoCoumarins and survival inincident dialysis patientsrdquo Nephrology Dialysis Transplantationvol 27 no 1 pp 332ndash337 2012
[37] K E Chan J Michael Lazarus R Thadhani and R MHakim ldquoWarfarin use associates with increased risk for strokein hemodialysis patients with atrial fibrillationrdquo Journal of theAmerican Society of Nephrology vol 20 no 10 pp 2223ndash22332009
[38] V T L Wizemann S Satayathum A Disney et al ldquoAtrialfibrillation in hemodialysis patients clinical features and asso-ciations with anticoagulant therapyrdquo Kidney International vol77 no 12 pp 1098ndash1106 2010
[39] K E Chan J M Lazarus R Thadhani and R M HakimldquoAnticoagulant and antiplatelet usage associates with mortalityamong hemodialysis patientsrdquo Journal of the American Societyof Nephrology vol 20 no 4 pp 872ndash881 2009
[40] J A Chazan M R London and L M Pomo ldquoLong-termsurvival of vascular accesses in a large chronic hemodialysispopulationrdquo Nephron vol 69 no 3 pp 228ndash233 1995
[41] D N Churchill D W Taylor R J Cook et al ldquoCanadianhemodialysis morbidity studyrdquo American Journal of KidneyDiseases vol 19 no 3 pp 214ndash234 1992
[42] M Zellweger J Bouchard S Raymond-Carrier A Laforest-Renald S Querin and F Madore ldquoSystemic anticoagulationand prevention of hemodialysis catheter malfunctionrdquo Amer-ican Society for Artificial Internal Organs Journal vol 51 no 4pp 360ndash365 2005
[43] L Colı G Donati G Cianciolo et al ldquoAnticoagulation therapyfor the prevention of hemodialysis tunneled cuffed catheter(TCC) thrombosisrdquo Journal of Vascular Access vol 7 no 3 pp118ndash122 2006
[44] C I Obialo A C Conner and L F Lebon ldquoMaintainingpatency of tunneled hemodialysis cathetersmdashefficacy of aspirincompared to warfarinrdquo Scandinavian Journal of Urology andNephrology vol 37 no 2 pp 172ndash176 2003
[45] M Cozzolino and V Brandenburg ldquoWarfarin to use or not touse in chronic kidney disease patientsrdquo Journal of Nephrologyvol 23 no 6 pp 648ndash652 2010
[46] L Friberg and L Bergfeldt ldquoAtrial fibrillation prevalence revis-itedrdquo Journal of Internal Medicine vol 274 no 5 pp 461ndash4682013
[47] I Atar D Konas S Acikel et al ldquoFrequency of atrial fibrillationand factors related to its development in dialysis patientsrdquoInternational Journal of Cardiology vol 106 pp 47ndash51 2006
[48] E Vazquez C Sanchez-Perales F Borrego et al ldquoInfluenceof atrial fibrillation on the morbido-mortality of patients onhemodialysisrdquo American Heart Journal vol 140 no 6 pp 886ndash890 2000
[49] S A Lubitz C Moser L Sullivan et al ldquoAtrial fibrillationpatterns and risks of subsequent stroke heart failure or deathin the communityrdquo Journal of the American Heart Associationvol 2 Article ID e000126 2013
[50] U S Renal DATA System USRDS 200520062007 AnnualData Report Atlas of End-Stage Renal Disease in the UnitedStates Bethesda National Institutes of Health NationalInstitute of Diabetes and Digestive and Kidney Diseaseshttpwwwusrdsorgarchiveaspx
[51] S Genovesi A Vincenti E Rossi et al ldquoAtrial fibrillation andmorbidity and mortality in a cohort of long-term hemodialysispatientsrdquoAmerican Journal of Kidney Diseases vol 51 no 2 pp255ndash262 2008
[52] J Olesen G Lip A L Kamper et al ldquoStroke and bleeding inatrial fibrillation with chronic kidney diseaserdquoTheNewEnglandJournal of Medicine vol 367 pp 625ndash635 2012
[53] W C Winkelmayer J Liu S Setoguchi and N K ChoudhryldquoEffectiveness and safety of warfarin initiation in olderhemodialysis patients with incident atrial fibrillationrdquo ClinicalJournal of the American Society of Nephrology vol 6 no 11 pp2662ndash2668 2011
[54] M J Elliott D Zimmerman and R M Holden ldquoWarfarinanticoagulation in hemodialysis patients a systematic review ofbleeding ratesrdquoAmerican Journal of Kidney Diseases vol 50 no3 pp 433ndash440 2007
The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

The Scientific World Journal 7
Table 4 Potential indications for oral anticoagulants in patientswith end-stage renal disease and receiving haemodialysis
(i) Status after prosthetic heart valve implantation(ii) Antiphospholipid syndrome(iii) Secondary prevention of severe thromboembolic events (forexample pulmonary embolism)(iv) Atrial fibrillation with a high risk of stroke
However OAC treatment in this group of patients irrespec-tive of its indications causes a great deal of controversy Thisis because a number of pro- and anticoagulant factors playan important role in end-stage renal failure due to the natureof the disease itself In these conditions the pharmacokineticand especially pharmacodynamic properties of the OACsused change as well All these factors make proper anticoagu-lation in these patients more difficult and most importantlythey decrease the time during which patients remain inthe therapeutic range of INR In the case of the treatmentof venous thromboembolism the only remaining option isOAC treatment according to regimens used for the generalpopulation as there are no relevant studies concerning thegroup of patients receiving haemodialysis Prevention of HDvascular access thrombosis with the use of OACs accordingto the presented studies and expertsrsquo opinions is not veryeffective and can additionally be very dangerous HoweverOAC treatment in haemodialysed patientswithAF in order toprevent thromboembolic events according to some authorsis associated with an increase in the incidence of stroke andmortality
Is the provocative question included in the title justifiedDoubts should be dispelled by prospective controlled ran-domised studies at the moment there is no justification forroutine use of OACs in the above-mentioned indications Inselected cases of OAC treatment in this group of patients it isabsolutely necessary to control andmonitor the applied treat-ment thoroughly According to the authors and the opinionsalready partially reported in the literature [45] indicationsfor the use of OACs in patients with end-stage renal failureincluding patients receiving haemodialysis should be limitedto those included in Table 4
References
[1] S I Hallan J Coresh B C Astor et al ldquoInternational compari-son of the relationship of chronic kidney disease prevalence andESRD riskrdquo Journal of the American Society of Nephrology vol17 no 8 pp 2275ndash2284 2006
[2] B Rutkowski ldquoChanging pattern of end-stage renal disease incentral and eastern Europerdquo Nephrology Dialysis Transplanta-tion vol 15 no 2 pp 156ndash160 2000
[3] J J Snyder R N Foley and A J Collins ldquoPrevalence of CKDin the United States a sensitivity analysis using the NationalHealth and Nutrition Examination Survey (NHANES) 1999ndash2004rdquo American Journal of Kidney Diseases vol 53 no 2 pp218ndash228 2009
[4] E Krol B Rutkowski P Czarniak et al ldquoEarly detection ofchronic kidney disease results of the PolNef studyrdquo AmericanJournal of Nephrology vol 29 no 3 pp 264ndash273 2009
[5] S Ghanny and M Crowther ldquoTreatment with novel oralanticoagulants indications efficacy and risksrdquo Current Opinionin Hematology vol 20 pp 430ndash436 2013
[6] T Kruger V Brandenburg G Schlieper et al ldquoSailing betweenScylla andCharybdis oral long-term anticoagulation in dialysispatientsrdquo Nephrology Dialysis Transplantation vol 28 pp 534ndash541 2013
[7] S Genovesi and A Santoro ldquoAnticoagulants renal failure andatrial fibrillationrdquo Expert Opinion on Drug Safety vol 12 pp 1ndash3 2013
[8] N Leung ldquoHematologic manifestations of kidney diseaserdquoSeminars in Hematology vol 50 pp 207ndash215 2013
[9] J A Milburn K Cassar I Ford N Fluck and J BrittendenldquoProthrombotic changes in platelet endothelial and coagulationfunction following hemodialysisrdquo International Journal of Arti-ficial Organs vol 34 no 3 pp 280ndash287 2011
[10] D I Jalal M Chonchol andG Targher ldquoDisorders of hemosta-sis associated with chronic kidney diseaserdquo Seminars inThrom-bosis and Hemostasis vol 36 no 1 pp 34ndash40 2010
[11] D Kaw and D Malhotra ldquoPlatelet dysfunction and end-stagerenal diseaserdquo Seminars in Dialysis vol 19 no 4 pp 317ndash3222006
[12] M A de Sa Siqueira T M C Brunini N R Pereira et alldquoIncreased nitric oxide production in platelets from severechronic renal failure patientsrdquo Canadian Journal of Physiologyand Pharmacology vol 89 no 2 pp 97ndash102 2011
[13] P Boccardo G Remuzzi and M Galbusera ldquoPlatelet dysfunc-tion in renal failurerdquo Seminars in Thrombosis and Hemostasisvol 30 no 5 pp 579ndash589 2004
[14] A S Gangji A S Sohal D Treleaven and M A CrowtherldquoBleeding in patients with renal insufficiency a practical guideto clinicalmanagementrdquoThrombosis Research vol 118 no 3 pp423ndash428 2006
[15] J C McCarter J B Bingham and O O Meyer ldquoStudies on thehemorrhagic agent 3 31015840-methylenebis (4-Hydroxycoumarin)IV The pathologic findings after the administration ofdicumarolrdquo The American Journal of Pathology vol 20 pp651ndash659 1944
[16] D V Clatanoff P O Triggs and O O Meyer ldquoClinical expe-rience with coumarin anticoagulants warfarin and warfarinrdquoArchives of Internal Medicine vol 94 no 2 pp 213ndash220 1954
[17] C Becattini M C Vedovati and G Agnelli ldquoOld and neworal anticoagulants for venous thromboembolism and atrialfibrillation a review of the literaturerdquoThrombosis Research vol129 no 3 pp 392ndash400 2012
[18] E A Nutescu ldquoOral anticoagulant therapies balancing therisksrdquoAmerican Journal of Health-System Pharmacy vol 70 no10 supplement 1 pp S3ndashS11 2013
[19] M Zacchigna G di Luca F Cateni and V Maurich ldquoImprove-ment of warfarin biopharmaceutics by conjugation with poly(ethylene glycol)rdquo European Journal of Pharmaceutical Sciencesvol 23 no 4-5 pp 379ndash384 2004
[20] G F Pineo and R D Hull ldquoVitamin K antagonists and directthrombin inhibitors present and futurerdquoHematologyOncologyClinics of North America vol 19 no 1 pp 69ndash85 2005
[21] B F Gage and P E Milligan ldquoPharmacology and pharma-cogenetics of warfarin and other coumarins when used withsupplementsrdquo Thrombosis Research vol 117 no 1-2 pp 55ndash592005
[22] K S Brimble A J Ingram J W Eikelboom et al ldquoAntico-agulants in patients with atrial fibrillation and end-stage renaldiseaserdquo Postgraduate Medicine vol 124 pp 17ndash25 2012
8 The Scientific World Journal
[23] S Benmira Z K Banda and V Bhattacharya ldquoOld versusnew anticoagulants focus on pharmacologyrdquo Recent Patents onCardiovascular Drug Discovery vol 5 no 2 pp 120ndash137 2010
[24] N A Limdi M A Limdi L Cavallari et al ldquoWarfarin dosingin patients with impaired kidney functionrdquoAmerican Journal ofKidney Diseases vol 56 no 5 pp 823ndash831 2010
[25] N Maruyama M Abe K Okada et al ldquoChanges to pro-thrombin international normalized ratio in patients receivinghemodialysisrdquo International Journal of Clinical PharmacologyandTherapeutics vol 51 pp 283ndash287 2013
[26] M Abe N Maruyama H Suzuki et al ldquoInternational nor-malized ratio decreases after hemodialysis treatment in patientstreated with warfarinrdquo Journal of Cardiovascular Pharmacologyvol 60 pp 502ndash507 2012
[27] AGompou I Griveas I Kyritsis I AgroyannisMTsakoniatisand B Agroyannis ldquoINR deviations in hemodialyzed patientsunder low dose oral anticoagulant therapyrdquo International Jour-nal of Artificial Organs vol 32 no 10 pp 752ndash755 2009
[28] J C van Blijderveen K M Verhamme R Zietse et alldquoOveranticoagulation is associated with renal function declinerdquoJournal of Nephrology vol 26 pp 691ndash698 2013
[29] M M Sood M Larkina J R Thumma et al ldquoMajor bleed-ing events and risk stratification of antithrombotic agents inhemodialysis results from the DOPPSrdquo Kidney Internationalvol 84 pp 600ndash608 2013
[30] M Monge I Vaida S S Modeliar et al ldquoRetroperitonealhematoma compressing a single functioning kidney an unusualcause of obstructive renal failurerdquo Clinical Nephrology vol 67no 5 pp 318ndash320 2007
[31] M Dugo E la Torre F Farneti et al ldquoA case of intrarenalhematoma role of ultrasonography in the early diagnosisof possible complication of anticoagulant therapyrdquo GiornaleItaliano di Nefrologia vol 29 pp 616ndash620 2012
[32] httpwwwaccessdatafdagovdrugsatfda docslabel2011009218s107lblpdf
[33] D P Tveit I O Hypolite P Hshieh et al ldquoChronic dialysispatients have high risk for pulmonary embolismrdquo AmericanJournal of Kidney Diseases vol 39 no 5 pp 1011ndash1017 2002
[34] C Kearon S R Kahn G Agnelli S Goldhaber G E RaskobandA J Comerota ldquoAntithrombotic therapy for venous throm-boembolic disease American College of Chest Physiciansevidence-based clinical practice guidelines (8th edition)rdquoChestvol 133 no 6 pp 454Sndash545S 2008
[35] H Decousus A Leizerovicz F Parent et al ldquoA clinical trialof vena cava filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave StudyGrouprdquoTheNew England Journal ofMedicine vol 338 pp 409ndash415 1998
[36] F Knoll G Sturm C Lamina et al ldquoCoumarins and survival inincident dialysis patientsrdquo Nephrology Dialysis Transplantationvol 27 no 1 pp 332ndash337 2012
[37] K E Chan J Michael Lazarus R Thadhani and R MHakim ldquoWarfarin use associates with increased risk for strokein hemodialysis patients with atrial fibrillationrdquo Journal of theAmerican Society of Nephrology vol 20 no 10 pp 2223ndash22332009
[38] V T L Wizemann S Satayathum A Disney et al ldquoAtrialfibrillation in hemodialysis patients clinical features and asso-ciations with anticoagulant therapyrdquo Kidney International vol77 no 12 pp 1098ndash1106 2010
[39] K E Chan J M Lazarus R Thadhani and R M HakimldquoAnticoagulant and antiplatelet usage associates with mortalityamong hemodialysis patientsrdquo Journal of the American Societyof Nephrology vol 20 no 4 pp 872ndash881 2009
[40] J A Chazan M R London and L M Pomo ldquoLong-termsurvival of vascular accesses in a large chronic hemodialysispopulationrdquo Nephron vol 69 no 3 pp 228ndash233 1995
[41] D N Churchill D W Taylor R J Cook et al ldquoCanadianhemodialysis morbidity studyrdquo American Journal of KidneyDiseases vol 19 no 3 pp 214ndash234 1992
[42] M Zellweger J Bouchard S Raymond-Carrier A Laforest-Renald S Querin and F Madore ldquoSystemic anticoagulationand prevention of hemodialysis catheter malfunctionrdquo Amer-ican Society for Artificial Internal Organs Journal vol 51 no 4pp 360ndash365 2005
[43] L Colı G Donati G Cianciolo et al ldquoAnticoagulation therapyfor the prevention of hemodialysis tunneled cuffed catheter(TCC) thrombosisrdquo Journal of Vascular Access vol 7 no 3 pp118ndash122 2006
[44] C I Obialo A C Conner and L F Lebon ldquoMaintainingpatency of tunneled hemodialysis cathetersmdashefficacy of aspirincompared to warfarinrdquo Scandinavian Journal of Urology andNephrology vol 37 no 2 pp 172ndash176 2003
[45] M Cozzolino and V Brandenburg ldquoWarfarin to use or not touse in chronic kidney disease patientsrdquo Journal of Nephrologyvol 23 no 6 pp 648ndash652 2010
[46] L Friberg and L Bergfeldt ldquoAtrial fibrillation prevalence revis-itedrdquo Journal of Internal Medicine vol 274 no 5 pp 461ndash4682013
[47] I Atar D Konas S Acikel et al ldquoFrequency of atrial fibrillationand factors related to its development in dialysis patientsrdquoInternational Journal of Cardiology vol 106 pp 47ndash51 2006
[48] E Vazquez C Sanchez-Perales F Borrego et al ldquoInfluenceof atrial fibrillation on the morbido-mortality of patients onhemodialysisrdquo American Heart Journal vol 140 no 6 pp 886ndash890 2000
[49] S A Lubitz C Moser L Sullivan et al ldquoAtrial fibrillationpatterns and risks of subsequent stroke heart failure or deathin the communityrdquo Journal of the American Heart Associationvol 2 Article ID e000126 2013
[50] U S Renal DATA System USRDS 200520062007 AnnualData Report Atlas of End-Stage Renal Disease in the UnitedStates Bethesda National Institutes of Health NationalInstitute of Diabetes and Digestive and Kidney Diseaseshttpwwwusrdsorgarchiveaspx
[51] S Genovesi A Vincenti E Rossi et al ldquoAtrial fibrillation andmorbidity and mortality in a cohort of long-term hemodialysispatientsrdquoAmerican Journal of Kidney Diseases vol 51 no 2 pp255ndash262 2008
[52] J Olesen G Lip A L Kamper et al ldquoStroke and bleeding inatrial fibrillation with chronic kidney diseaserdquoTheNewEnglandJournal of Medicine vol 367 pp 625ndash635 2012
[53] W C Winkelmayer J Liu S Setoguchi and N K ChoudhryldquoEffectiveness and safety of warfarin initiation in olderhemodialysis patients with incident atrial fibrillationrdquo ClinicalJournal of the American Society of Nephrology vol 6 no 11 pp2662ndash2668 2011
[54] M J Elliott D Zimmerman and R M Holden ldquoWarfarinanticoagulation in hemodialysis patients a systematic review ofbleeding ratesrdquoAmerican Journal of Kidney Diseases vol 50 no3 pp 433ndash440 2007
The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
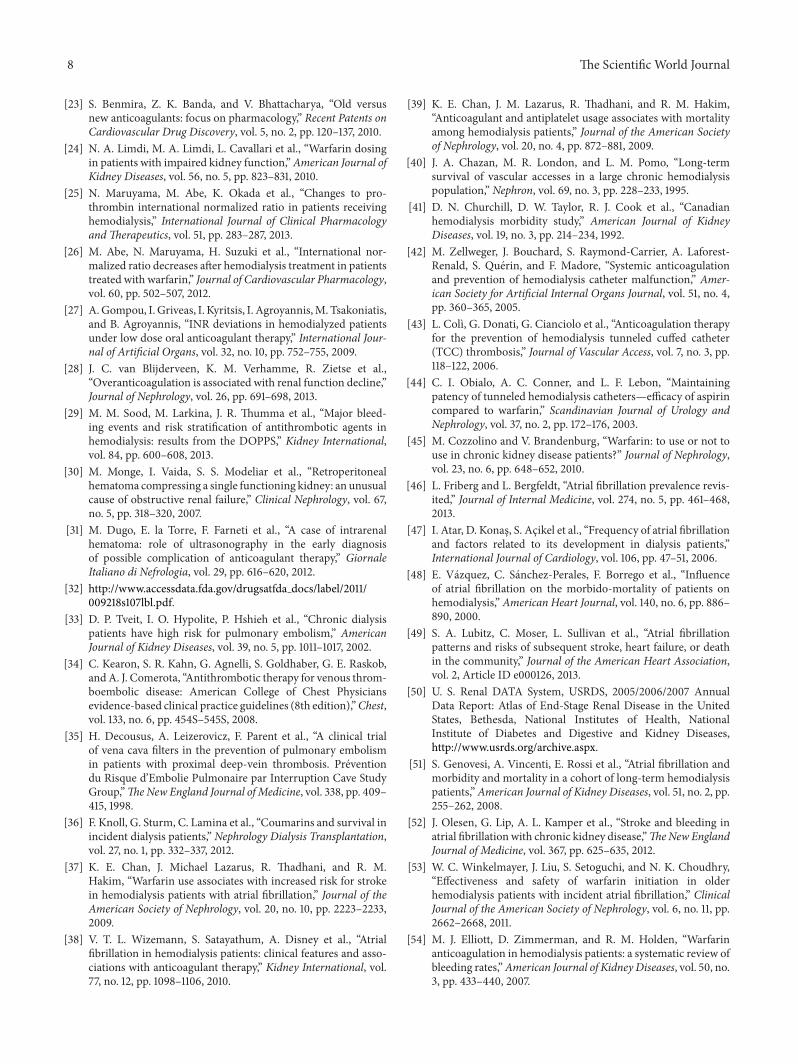
8 The Scientific World Journal
[23] S Benmira Z K Banda and V Bhattacharya ldquoOld versusnew anticoagulants focus on pharmacologyrdquo Recent Patents onCardiovascular Drug Discovery vol 5 no 2 pp 120ndash137 2010
[24] N A Limdi M A Limdi L Cavallari et al ldquoWarfarin dosingin patients with impaired kidney functionrdquoAmerican Journal ofKidney Diseases vol 56 no 5 pp 823ndash831 2010
[25] N Maruyama M Abe K Okada et al ldquoChanges to pro-thrombin international normalized ratio in patients receivinghemodialysisrdquo International Journal of Clinical PharmacologyandTherapeutics vol 51 pp 283ndash287 2013
[26] M Abe N Maruyama H Suzuki et al ldquoInternational nor-malized ratio decreases after hemodialysis treatment in patientstreated with warfarinrdquo Journal of Cardiovascular Pharmacologyvol 60 pp 502ndash507 2012
[27] AGompou I Griveas I Kyritsis I AgroyannisMTsakoniatisand B Agroyannis ldquoINR deviations in hemodialyzed patientsunder low dose oral anticoagulant therapyrdquo International Jour-nal of Artificial Organs vol 32 no 10 pp 752ndash755 2009
[28] J C van Blijderveen K M Verhamme R Zietse et alldquoOveranticoagulation is associated with renal function declinerdquoJournal of Nephrology vol 26 pp 691ndash698 2013
[29] M M Sood M Larkina J R Thumma et al ldquoMajor bleed-ing events and risk stratification of antithrombotic agents inhemodialysis results from the DOPPSrdquo Kidney Internationalvol 84 pp 600ndash608 2013
[30] M Monge I Vaida S S Modeliar et al ldquoRetroperitonealhematoma compressing a single functioning kidney an unusualcause of obstructive renal failurerdquo Clinical Nephrology vol 67no 5 pp 318ndash320 2007
[31] M Dugo E la Torre F Farneti et al ldquoA case of intrarenalhematoma role of ultrasonography in the early diagnosisof possible complication of anticoagulant therapyrdquo GiornaleItaliano di Nefrologia vol 29 pp 616ndash620 2012
[32] httpwwwaccessdatafdagovdrugsatfda docslabel2011009218s107lblpdf
[33] D P Tveit I O Hypolite P Hshieh et al ldquoChronic dialysispatients have high risk for pulmonary embolismrdquo AmericanJournal of Kidney Diseases vol 39 no 5 pp 1011ndash1017 2002
[34] C Kearon S R Kahn G Agnelli S Goldhaber G E RaskobandA J Comerota ldquoAntithrombotic therapy for venous throm-boembolic disease American College of Chest Physiciansevidence-based clinical practice guidelines (8th edition)rdquoChestvol 133 no 6 pp 454Sndash545S 2008
[35] H Decousus A Leizerovicz F Parent et al ldquoA clinical trialof vena cava filters in the prevention of pulmonary embolismin patients with proximal deep-vein thrombosis Preventiondu Risque drsquoEmbolie Pulmonaire par Interruption Cave StudyGrouprdquoTheNew England Journal ofMedicine vol 338 pp 409ndash415 1998
[36] F Knoll G Sturm C Lamina et al ldquoCoumarins and survival inincident dialysis patientsrdquo Nephrology Dialysis Transplantationvol 27 no 1 pp 332ndash337 2012
[37] K E Chan J Michael Lazarus R Thadhani and R MHakim ldquoWarfarin use associates with increased risk for strokein hemodialysis patients with atrial fibrillationrdquo Journal of theAmerican Society of Nephrology vol 20 no 10 pp 2223ndash22332009
[38] V T L Wizemann S Satayathum A Disney et al ldquoAtrialfibrillation in hemodialysis patients clinical features and asso-ciations with anticoagulant therapyrdquo Kidney International vol77 no 12 pp 1098ndash1106 2010
[39] K E Chan J M Lazarus R Thadhani and R M HakimldquoAnticoagulant and antiplatelet usage associates with mortalityamong hemodialysis patientsrdquo Journal of the American Societyof Nephrology vol 20 no 4 pp 872ndash881 2009
[40] J A Chazan M R London and L M Pomo ldquoLong-termsurvival of vascular accesses in a large chronic hemodialysispopulationrdquo Nephron vol 69 no 3 pp 228ndash233 1995
[41] D N Churchill D W Taylor R J Cook et al ldquoCanadianhemodialysis morbidity studyrdquo American Journal of KidneyDiseases vol 19 no 3 pp 214ndash234 1992
[42] M Zellweger J Bouchard S Raymond-Carrier A Laforest-Renald S Querin and F Madore ldquoSystemic anticoagulationand prevention of hemodialysis catheter malfunctionrdquo Amer-ican Society for Artificial Internal Organs Journal vol 51 no 4pp 360ndash365 2005
[43] L Colı G Donati G Cianciolo et al ldquoAnticoagulation therapyfor the prevention of hemodialysis tunneled cuffed catheter(TCC) thrombosisrdquo Journal of Vascular Access vol 7 no 3 pp118ndash122 2006
[44] C I Obialo A C Conner and L F Lebon ldquoMaintainingpatency of tunneled hemodialysis cathetersmdashefficacy of aspirincompared to warfarinrdquo Scandinavian Journal of Urology andNephrology vol 37 no 2 pp 172ndash176 2003
[45] M Cozzolino and V Brandenburg ldquoWarfarin to use or not touse in chronic kidney disease patientsrdquo Journal of Nephrologyvol 23 no 6 pp 648ndash652 2010
[46] L Friberg and L Bergfeldt ldquoAtrial fibrillation prevalence revis-itedrdquo Journal of Internal Medicine vol 274 no 5 pp 461ndash4682013
[47] I Atar D Konas S Acikel et al ldquoFrequency of atrial fibrillationand factors related to its development in dialysis patientsrdquoInternational Journal of Cardiology vol 106 pp 47ndash51 2006
[48] E Vazquez C Sanchez-Perales F Borrego et al ldquoInfluenceof atrial fibrillation on the morbido-mortality of patients onhemodialysisrdquo American Heart Journal vol 140 no 6 pp 886ndash890 2000
[49] S A Lubitz C Moser L Sullivan et al ldquoAtrial fibrillationpatterns and risks of subsequent stroke heart failure or deathin the communityrdquo Journal of the American Heart Associationvol 2 Article ID e000126 2013
[50] U S Renal DATA System USRDS 200520062007 AnnualData Report Atlas of End-Stage Renal Disease in the UnitedStates Bethesda National Institutes of Health NationalInstitute of Diabetes and Digestive and Kidney Diseaseshttpwwwusrdsorgarchiveaspx
[51] S Genovesi A Vincenti E Rossi et al ldquoAtrial fibrillation andmorbidity and mortality in a cohort of long-term hemodialysispatientsrdquoAmerican Journal of Kidney Diseases vol 51 no 2 pp255ndash262 2008
[52] J Olesen G Lip A L Kamper et al ldquoStroke and bleeding inatrial fibrillation with chronic kidney diseaserdquoTheNewEnglandJournal of Medicine vol 367 pp 625ndash635 2012
[53] W C Winkelmayer J Liu S Setoguchi and N K ChoudhryldquoEffectiveness and safety of warfarin initiation in olderhemodialysis patients with incident atrial fibrillationrdquo ClinicalJournal of the American Society of Nephrology vol 6 no 11 pp2662ndash2668 2011
[54] M J Elliott D Zimmerman and R M Holden ldquoWarfarinanticoagulation in hemodialysis patients a systematic review ofbleeding ratesrdquoAmerican Journal of Kidney Diseases vol 50 no3 pp 433ndash440 2007
The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

The Scientific World Journal 9
[55] R M Holden G J Harman M Wang D Holland and A GDay ldquoMajor bleeding in hemodialysis patientsrdquo Clinical Journalof the American Society of Nephrology vol 3 no 1 pp 105ndash1102008
[56] A C Y To M Yehia and J F Collins ldquoAtrial fibrillation inhaemodialysis patients do the guidelines for anticoagulationapplyrdquo Nephrology vol 12 no 5 pp 441ndash447 2007
[57] A J Rose E M Hylek A Ozonoff A S Ash J I ReismanandD R Berlowitz ldquoPatient characteristics associatedwith oralanticoagulation control results of the Veterans AffaiRs Study toImprove Anticoagulation (VARIA)rdquo Journal of Thrombosis andHaemostasis vol 8 no 10 pp 2182ndash2191 2010
[58] L J SchurgersHMH Spronk BAM Soute PM Schiffers JG R DeMey and C Vermeer ldquoRegression of warfarin-inducedmedial elastocalcinosis by high intake of vitamin K in ratsrdquoBlood vol 109 no 7 pp 2823ndash2831 2007
[59] R Koos A H Mahnken G Muhlenbruch et al ldquoRelation oforal anticoagulation to cardiac valvular and coronary calciumassessed by multislice spiral computed tomographyrdquo AmericanJournal of Cardiology vol 96 no 6 pp 747ndash749 2005
[60] H C Rayner R L Pisoni J Bommer et al ldquoMortality andhospitalization in haemodialysis patients in five Europeancountries results from the Dialysis Outcomes and PracticePatterns Study (DOPPS)rdquo Nephrology Dialysis Transplantationvol 19 no 1 pp 108ndash120 2004
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom