Embed Size (px)
DESCRIPTION
Warfarin. Most used oral anticoagulant in the world. In some cases it has no alternative. Has many side effects. Careful monitoring and judicious titration of dose can make it best. Live long Warfarin.
Citation preview

Dr. Md. Arifur Rahman SazalMBBS, MD (Cardiology)
Clinical & Interventional Cardiologist National Institute of Cardiovascular Diseases
Dhaka, Bangladesh

WARFARIN

A brief history of warfarin
The discovery of oral anticoagulants is one of the most mysterious story in pharmaceutical
history.
It started with a hemorrhagic disease in cattle in the Midwest US in the 1920s. This was due to
ingestion of spoiled sweet clover. The substance responsible for bleeding was extracted and
identified as a coumarin by Karl Paul Link from University of Wisconsin.
In 1941 it used as a rat and mouse poison, but the survival of a man suffering from
thromboembolic disease after an attempted suicide by the use of a large amount of warfarin-
based rodenticide led to clinical trials of warfarin (Wisconsin Alumni Research
Foundation,WARF), which was approved for medical use in 1954.

Sweet clover sweet smell but bitter
taste
Systematic name
(RS)-4-hydroxy- 3-(3- oxo- 1-phenylbutyl)- 2H- chromen- 2-one

Mechanism of action

Routes Oral
Bioavailability 100%
Protein binding 99.5%
MetabolismHepatic: CYP2C9,
2C19, 2C8, 2C18, 1A2 and 3A4
Half-life 40 hours
Excretion Renal (92%)
Pregnancy cat. D
Pharmacokinetic data

Condition INR range
Preventing DVT (high risk patients, like those
who have had hip replacement) 2.0-3.0
Therapy after DVT or pulmonary embolism 2.0-3.0
Preventing systemic embolism
- Atrial fibrillation
-Valvular heart disease
-Tissue heart valves (first 3 months)
2.0-3.0
2.0-3.0
2.0-3.0
Bileaflet mechanical heart valve (aortic) 2.5-3.5
Mechanical prosthetic heart valve (high risk) 3.0-4.5
Thrombosis in antiphospholipid antibody
syndrome 3.0-4.5
Indication with target INR

Contraindication

Increased bleeding risk due to increased effect of warfarin: ➞ INR
Antiarrhythmics - amiodarone , propafenone
Antibiotics - amoxicillin , cephalosporins , fluoroquinolones, macrolides.
Anticonvulsants - phenytoin ,sodium valproate
Antidepressants -duloxetine ,venlafaxine, SSRI.
Antifungals- fluconazole , itraconazole , ketoconazole.
Antihyperlipidemics - Ezetimibe , fenofibrate ,Atorvastatin,
fluvastatin ,rosuvastatin
Decreased effect warfarin:➞INRAntibiotics - rifampin Antidepressants- trazodone Antiepileptics - carbamazepine , phenobarbitone ,phenytoin.
Drug interaction

Vegetables that include cauliflower,
kale, Brussels sprouts, asparagus,
spinach, alfalfa, turnip greens,
mustard greens and collard greens
Beverages such as herbal teas
(green tea) and coffee.
Vegetable oils that include soybean,
olive.
Peas and green onions
Dairy products such as yogurt
Vitamin K ,Foods to Avoid while on Warfarin

Complications of Warfarin
Hemorrhage- 2.7% (major- 1.1%-8.1%)
Warfarin Embryopathy -5% -30%
Warfarin necrosis- 0.02%
Osteoporosis- 0.1%
Purple toe syndrome-0.01%

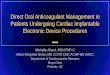
Warfarin Embryopathy (WE) -Di Sala syndrome
A specific pattern of congenital anomalies develop in children born to
mothers exposed to warfarin during the first trimester of pregnancy
(between the 6th and 12th weeks of gestation).
Classical features of WE-
Nasal hypoplasia
Chondrodysplasia punctata
(epiphyseal and vertebral bone
stippling)
Less frequent
malformations-Intraventricular hemorrhage
Hydrocephalus
Cervical spine myelopathy
Finger and toe defects

Calcifications and irregular ossification of lumbar and sacral vertebrae
Chondrodysplasia punctata

21-week stillborn with warfarin embryopathy, extreme nasal hypoplasia.

Nasal hypoplasia

Warfarin necrosis
The onset is usually within the first 2 to 5 days
of warfarin therapy, when the blood tends to
clot more than is normal.
Skin necrosis affects areas of the body with a
high fat content, such as breasts, thighs,
buttocks, hips and abdomen. .
It affects 1 in every 10,000 patients prescribed
warfarin.

D/D of Warfarin necrosis: Pyoderma gangrenosum ,,Necrotizing fasciitis.

Mechanism of Warfarin necrosis
Warfarin
Inhibition of protein C
( natural anticoagulant)
Coagulation factor imbalance
Paradoxical activation of coagulation
Thrombosis
Skin necrosis.

Purple toe syndrome
Warfarin cause violaceous painful discoloration of the toes
and the sides of the feet . This typically happens within the
first few weeks of starting warfarin
The problem appears to occur mostly in elderly people
and in people with underlying arteriosclerosis. bleeding
into atheromatous plaques in the blood vessel wall leads to
the release of cholesterol clumps that embolize to the
hands and feet, leading to obstruction of small arteries.

Purple toe syndrome

Osteoporosis and Warfarin
Warfarin indirectly weaken bones, because vitamin K is involved with the
protein osteocalcin, which is important for bone remineralization .

Warfarin in special situations

Warfarin in pregnancy Warfarin cross the placenta and should be avoided during the first and third
trimesters.
Treatment at 6-12 weeks gestation causes Warfarin embryopathy.
Later exposure is associated with central nervous system abnormalities.
Almost 5%- 30% of children (10 of 35) born to mothers with a prosthetic heart
valve were malformed .Heparins do not cross the placenta and do not cause these
problems.
It is safe to breastfeed during warfarin therapy as there is minimal excretion into
breast milk.

Warfarin in Prosthetic heart valves
The ACCP recommends
Bileaflet or tilting disc valves- INR -2.0-3.0 –life long.
Caged ball or disc- 2.5-3.5- life long.
Bioprosthetic (tissue) valve require three months of warfarin -
INR -2.0-3.0.
Combination of aspirin (100 mg/day) with warfarin reduces the
risk of systemic embolism.

Venous Thromboembolism ( DVT and PE )
Target INR of 2.5 (INR range, 2.0-3.0) for all treatment durations.
The duration of treatment is based on the indication as follows: For
patients with a DVT or PE secondary to a transient (reversible) risk
factor, treatment with warfarin for 3 months is recommended.
For patients with two episodes of unprovoked DVT or PE, long-term
treatment with warfarin is recommended

Warfarin in liver disease
Warfarin is associated with a 0.8% to 1.2% risk
of transaminase elevation >3 ULN .
Liver damage in Hepatitis C could be treated with
warfarin.
Warfarin reduces the scarring on the liver
caused by Hepatitis C.
In Hepatitis C, scarring of the liver accelerates in
those patients who are prone to form blood clots..
http://www.news-medical.net/news/2011/07/31/40407.aspx

Warfarin in Renal impairment
There is no evidence that response to Warfarin is altered in renal
impairment , thus dosage adjustments are generally not necessary.
However, patients with renal impairment may cause platelet defects and
may increase risk for bleeding.
Patients with CKD required on average a 25% reduction warfarin
dose.
Journal of the American Society of Nephrology (JASN). April 2009

Antithrombotic Therapy in Cardioversion for Atrial Fibrillation
Timing of cardioversion Anticoagulation
Early cardioversion in patients with AF
for < 48 hrs
Heparin during cardioversion period to achieve
PTT of 1.5 to2.5 times the baseline value
Early cardioversion in patients with AF
for > 48 hrs or an unknown duration, but
without documented atrial thrombi
Heparin during cardioversion period to achieve
PTT of 1.5 to 2.5 times the baseline value.
Warfarin for 4 weeks after cardioversion to
achieve target INR of 2.5 (range: 2.0 to 3.0)
Elective cardioversion in patients with AF
>48 hrs or an unknown duration
Warfarin for 3 weeks before and 4 weeks after
cardioversion to achieve target INR of 2.5 (range:
2.0 to 3.0)

CHADS2 score Condition Points
C Congestive heart failure 1
H Hypertension: blood pressure consistently above 140/90 mmHg (or treated hypertension on medication)
1
A Age ≥75 years 1
D Diabetes mellitus 1
S2 Prior Stroke or TIA 2
Total 6
Guidelines for the management of atrial fibrillation
Estimating the risk of stroke

CHA2DS2 VASc score
European Heart Journal (2010) 31, 2369–2429doi:10.1093/eurheartj/ehq278

Score RiskAnticoagulation
TherapyConsiderations
0 Low
No antithrombotic
therapy (or
Aspirin)
No antithrombotic therapy (or Aspirin 75-325mg
daily)
1 ModerateOral anticoagulant
(or Aspirin)
Oral anticoagulant, either new oral anticoagulant
drug Dabigatran or well controlled warfarin at INR
2.0-3.0 (or Aspirin 75-325mg daily.
2 or greater High Oral anticoagulant
Oral anticoagulant, using either a new oral
anticoagulant drug (Rivaroxaban or Dabigatran) or
well controlled warfarin at INR 2.0-3.0
Anticoagulation (CHA2DS2 VASc score)
European Heart Journal (2010) 31, 2369–2429doi:10.1093/eurheartj/ehq278

Warfarin monitoring- Recommended INR testing guidelines

Managing overdose and bleeding of warfarin therapy
Clinical setting Action
INR >5.0 but < 9.0 (no
bleeding)
Stop warfarin, 1-2.5mg vitamin K1, INR in 6-12 hours,
restart warfarin at reduced dose once INR is < 5.
INR ≥9.0 (no bleeding) Stop warfarin, 5mg vitamin K1, measure INR in 6-12
hours, restart warfarin at reduced dose once INR is < 5,
clotting factor replacement- if high risk of bleeding
Major bleeding (any
level of INR)
Stop warfarin, give 5mg vitamin K1, clotting factor
replacement, measure INR as required, assess need to
restart warfarin

Future challenges for Warfarin
?

Property Dabigatran Warfarin
Indication for AF Non-valvular atrial fibrillation Valvular or non-valvular atrial
fibrillation
Mechanism of action Direct inhibition of thrombin Reduced synthesis of
prothrombin and other clotting
factors
Administration Oral
Twice daily (for AF)
Oral
Once daily
Dosing Fixed dose, dependent on creatinine
clearance and age
Individualised to each patient
and target INR
Onset of action 0.5–2 hours 36–72 hours
Elimination half-life 12–14 hours 20–60 hours
Duration of action 24 hours 48–96 hours
Comparison of Dabigatran and Warfarin

Property Dabigatran Warfarin
Stable,
predictable
pharmacokinetics
Yes No
Interactions with
diet and alcohol
No Yes
Interactions with
medicines
Interactions largely unknown, clinical
experience over time likely to reveal more.
Known interaction with p-glycoprotein
inhibitors e.g. oral ketoconazole,
verapamil, amiodarone
Multiple
Monitoring No routine monitoring required. INR every one
to eight
weeks
depending on
clinical
situation
Comparison of dabigatran and warfarin

Property Dabigatran Warfarin
Risk of major
haemorrhage
Similar for both medicines
Major GI bleeding rates may be higher than with
warfarin, however, rates of intracranial haemorrhage
and life-threatening bleeding may be lower with
dabigatran.
Similar for both
medicines.
Other adverse
effects
Dyspepsia
Possibly increased risk of MI
Multiple reported,
however, in clinical
practice these are
relatively rare
Antidote None available but can be removed by dialysis Vitamin K
Fresh-frozen plasma
Cost Very expensive- 450 $/ month Very cheap- 30 $/ month
Comparison of dabigatran and warfarin

Trials designed to compare the new oral anticoagulants to prevent thromboembolism with warfarin in AF
Trial Study drug DosingNumber of
patientsDesign
RE-LY Dabigatran110 mg twice daily, 150
mg twice daily18,113
Randomized, open-label, noninferiority
Rocket-AF Rivaroxaban15 mg daily, 20 mg
daily14,000
Randomized, double blind, noninferiority
ARISTOTLE Apixaban 5 mg twice daily 15,000Randomized, double blind,
noninferiority
Engage AF Edoxaban30 mg daily, 60 mg
daily16,500
Randomized, double blind, noninferiority
Altman and Vidal Thrombosis Journal 2011 9:12 doi:10.1186/1477-9560-9-12

The evidence for dabigatran - RE-LY trial The Randomised Evaluation of Long-Term Anticoagulation Therapy Large,
randomised, non-inferiority clinical trial
Event % of incidents per year Significance (P ≥ 0.05)
Dabigatran
110 mg
Dabigatran
150 mgWarfarin
Stroke or systemic embolism
1.53 1.11 1.69D150 superior to WD110 not inferior to WD150 superior to D110
Myocardial infarction 0.72 0.74 0.53 W superior to D150
Intracranial haemorrhage 0.23 0.30 0.74D110 superior to WD150 superior to W
Life-threatening bleeding 1.22 1.45 1.80D110 superior to WD150 superior to W
Gastrointestinal bleeding 1.12 1.51 1.02W superior to D150D110 superior to D150
Death from vascular causes
2.43 2.28 2.69 D150 superior to W
Death from any causes 3.75 3.64 4.13 No difference

New hope Pharmacogenetics
based warfarin therapy

Pharmacogenetics based warfarin therapy

Pharmacogenetics based warfarin therapy

Mr. Shakil
64 inch
58 kg
03 .08. 69Dr. Tazkera
Mr. Atik

Pharmacogenetics based warfarin therapy

ConclusionWarfarin took more than 20 years to establish its existance as an
effective and adjustable anticoagulant .
Physicians has more than 40 years of experience to use it
It is now in good shape with vast knowledge of handling it
Furthermore Pharmacogenetics based warfarin therapy is getting
popularity.
Newer anticoagulants are in different phases of their trials .
Many more informations and results are still pending -so it will not be
so easy to replace warfarin by newer anticoagulants so early.

Live long Warfarin
Thank you
Dr.Arif